")
Back to Journals » Research and Reports in Urology » Volume 15
Hemorrhagic Cystitis: Making Rapid and Shrewd Clinical and Surgical Decisions for Improving Patient Outcomes
Authors Jefferson FA, Linder BJ
Received 18 March 2023
Accepted for publication 31 May 2023
Published 29 June 2023 Volume 2023:15 Pages 291—303
DOI https://doi.org/10.2147/RRU.S320684
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Panagiotis J Vlachostergios
Francis A Jefferson, Brian J Linder
Department of Urology, Mayo Clinic, Rochester, MN, USA
Correspondence: Brian J Linder, Email [email protected]
Abstract: Hemorrhagic cystitis (HC) can be one of the most challenging clinical scenarios for urologists to manage. It most commonly occurs as a toxicity of pelvic radiation therapy or in patients treated with the oxazaphosphorine class of chemotherapy. Successful management of HC necessitates a stepwise approach with a thorough understanding of the various treatment options. Once ensuring hemodynamic stability, conservative management includes establishing bladder drainage, manual clot evacuation, and continuous bladder irrigation through a large-bore urethral catheter. If gross hematuria persists, operative cystoscopy with bladder clot evacuation is often required. There are multiple intravesical options for treating HC, including alum, aminocaproic acid, prostaglandins, silver nitrate, and formalin. Formalin is an intravesical option that has caustic effects on the bladder mucosa and is most often reserved as a last-line intravesical treatment. Non-intravesical management tools include hyperbaric oxygen therapy and oral pentosan polysulfate. If needed, nephrostomy tube placement or superselective angioembolization of the anterior division of the internal iliac artery can be performed. Finally, cystectomy with urinary diversion is a definitive, albeit invasive, treatment option for refractory HC. While there is no standardized algorithm, treatment modalities typically progress from less to more invasive. Clinical judgement and shared decision-making with the patient are required when choosing therapies for managing HC, as success rates are variable and some treatments may have significant or irreversible effects.
Keywords: hemorrhagic cystitis, hematuria, cystectomy, formalin, bladder cancer, radiation
Introduction
Hemorrhagic cystitis (HC) is a sterile cystitis that results in persistent diffuse bleeding from the bladder mucosa with resultant gross hematuria. It is most common in patients treated with the oxazaphosphorine class of chemotherapy or secondary to pelvic radiation therapy (RT). The chemotherapy agents most commonly implicated include ifosfamide or cyclophosphamide in the setting of bone and soft tissue sarcoma or hematopoietic cell transplantation. It can also present as a late toxicity of pelvic RT when the bladder is within or near the radiation treatment field (eg prostate cancer, cervical cancer, etc.). Clinical presentations range from transient painless hematuria or irritative lower urinary tract symptoms to refractory acute bleeding necessitating transfusion and interventional measures.
Despite the availability of multiple treatment options, management of HC can be challenging, as treatment success rates vary and in some cases symptoms can be severe and persistent. The objective of this paper is to review the etiology, presentation, and management of HC, specifically in the context of the urologist’s role in workup and management. Our intention is not to review an exhaustive list of all agents and treatment modalities reported, but rather to describe a practical set of tools that the urologist can add to their armamentarium and apply as indicated depending on the presentation of HC.
Epidemiology
Gross hematuria accounts for approximately 27% of all urologic consultations and between 4% and 20% of inpatient urologic consultations.1,2 Regarding HC specifically, radiation cystitis accounts for 5–10% of gross hematuria cases.3 Among patients presenting to the emergency room for HC related to radiation for prostate cancer, roughly 50% subsequently undergo invasive procedures.4 In the largest series of patients undergoing cystectomy for refractory HC, radiation was identified as the etiology in 95% of patients.5
In addition, up to 40% of patients who receive the oxazaphosphorine class of chemotherapy (ie cyclophosphamide and ifosfamide) develop HC of various severity, though this rate decreases to less than 5% when preventive measures are taken.6–10 Prolonged and higher doses of these chemotherapeutic agents increase the risk of HC, such as in patients undergoing hematopoietic cell transplantation and those on chronic oral therapy for rheumatologic diseases.11
Etiology and Pathophysiology
The most common inciting factors for HC are chemotherapy and pelvic radiation therapy. While multiple chemotherapeutic agents can cause HC, those most often implicated are the oxazaphosphorine alkylating agents ifosfamide and cyclophosphamide.12,13 Ifosfamide and cyclophosphamide result in a proinflammatory cascade that can lead to HC. Hepatic metabolism of cyclophosphamide and ifosfamide generates the reactive unsaturated aldehyde, acrolein, which is renally filtered, excreted, and concentrated in the bladder.14,15 Acrolein leads to cell death by upregulating reactive oxygen species and nitric oxide, both of which produce downstream effects resulting in abnormal DNA repair and increased production of proinflammatory cytokines.16,17 Histologically, these molecular changes manifest as urothelial damage including bladder mucosal edema, ulceration, and hemorrhage.
The rate of hemorrhagic cystitis resulting from oxazaphosphorine chemotherapeutic agents is significantly reduced with the use of prophylactic mesna.8–10 Mesna is a thiol compound (2-mercaptoethane sulfonate) administered either subcutaneously or intravenously that inactivates acrolein in the urine. Mesna reduces the rate of HC with gross hematuria to less than 5%, though microscopic hematuria may still occur in up to 18% of patients.8–10 Likewise, hyperhydration at the time of chemotherapy treatment has been associated with decreased rates of HC.18,19
While RT can cause acute bladder inflammation leading to urinary symptoms, HC is typically a late complication of RT. Following full-dose, standard-fractionation pelvic RT for prostate or gynecologic cancer, HC occurs in 6.5% to 9% of patients, though it is classified as severe in less than 5%.20–23 It can occur months to years after radiation treatment, with the median latent period from pelvic radiation therapy to the development of radiation-related HC being 35 months.3,24,25 The initial response of the bladder to radiation therapy is edema and friability of the urothelium. Later, there is progressive endarteritis leading to obliteration of the suburothelial vasculature. This results in ischemia, reperfusion injury, and fibrosis of the mucosa and submucosa. Clinically, during cystoscopy, this presents itself as visibly dilated and friable vessels that bleed easily.26 Proposed measures to prevent radiation-related HC include hyperhydration, continuous bladder irrigation, sodium hyaluronate, and cranberry juice or extract; however, no definitive success with these interventions has been demonstrated, and therefore none are routinely recommended.3
Presentation
Clinically, patients with HC will often present with some degree of gross hematuria, ranging from mild hematuria to significant gross hematuria with clots, or even life-threatening hemorrhage. Notably, the intensity of red color change in the urine does not necessarily reflect the severity of the hematuria, since just 1 mL of blood per liter of urine can cause visible color change.27 Additional symptoms may include irritative lower urinary tract symptoms (urgency, frequency, and dysuria) as well as obstructive symptoms (sensation of incomplete bladder emptying), especially if there is clot obstruction.
When HC is suspected, it is important to recall that cyclophosphamide or ifosfamide causes hematuria within 24 to 48 hr of administration of a single dose, which can last for approximately 5 days. In addition, these patients may be thrombocytopenic or have other bleeding disorders related to the underlying pathology that is being treated with chemotherapy. As previously discussed, HC resulting from RT can occur at any point after RT and is typically months to years later.3,24,25
Initial Evaluation and Management
Regardless of the etiology of gross hematuria, the initial evaluation in an acute setting should be focused on assessing hemodynamic stability and ensuring bladder drainage. This assessment includes vital signs, complete blood count, coagulation profiles, and intravascular volume repletion, including blood products, as indicated. Platelets should be repleted to maintain levels at >50,000/µL, and consideration should be given to holding of anticoagulation medications while weighing the risk of thromboembolic events. Physical exam should include abdominal exam and suprapubic palpation to assess bladder distention. Bladder drainage must be ensured immediately to prevent potential clot retention and the risk of subsequent bladder rupture. If there is gross hematuria with large clots, a large bore (≥22Fr) 3-way catheter should be placed, and manual irrigation performed for clot extraction. If urine is cleared with manual irrigation alone, monitoring bladder drainage and providing hydration may adequately control hematuria. However, if significant hematuria with passage of clots persists, continuous bladder irrigation with normal saline should be initiated. The initial evaluation and management of hematuria with clot retention is summarized in Figure 1. From there, it is essential to identify the likely underlying etiology for hematuria as well as any contributing factors to target further management.
 |
Figure 1 Initial evaluation and management of gross hematuria with clot retention. Reproduced with permission from: Linder BJ, Boorjian SA. Management of emergency bleeding, recalcitrant clots, and hemorrhagic cystitis. AUA Update Series. 2015;34 (Lesson 3).28 |
If HC secondary to chemotherapy or prior RT is suspected, the urologist must ensure other potential etiologies are ruled out, including malignancy (eg progression of primary malignancy or secondary malignancy from prior chemotherapy or radiation), urolithiasis, infection, traumatic injury, and upper urinary tract bleeding, among others. Once stabilized, the recommended diagnostic evaluation for gross hematuria includes urine cytology, cystoscopy, and upper tract cross-sectional imaging, preferably with CT urogram (as comorbidities allow).29
During initial evaluation and stabilization, if the clot burden is such that catheter irrigation alone is insufficient to control the hematuria or clear the clots from the bladder, then the patient should be taken to the operating room for cystoscopy and clot evacuation under anesthesia. This procedure is also an opportunity to fulgurate bleeding vessels, to manage any bleeding tumors accordingly, and to potentially establish a diagnosis of HC based on the appearance of the urothelium. Figure 2 If there is complete catheter obstruction with inability to drain the patient’s bladder, then this trip to the operating room should be treated as an emergency. In a series of 33 patients with HC from cyclophosphamide exposure or RT, cystoscopy with clot evacuation (with or without fulguration) resulted in resolution of hematuria without further need for treatment in 14 (42%) patients.30 Fulguration is typically performed with cautery, however reports of laser use have also demonstrated success.31 Attention must be paid to the depth of laser penetration, as bladder perforation and intestinal injury have been reported.32 Regardless of whether cystoscopy with clot evacuation is curative for HC, it is often a necessary step to clear the bladder of clot burden prior to administering intravesical therapy.
 |
Figure 2 Cystoscopic image of radiation cystitis demonstrating increased vascularity/telangiectasia. |
Interventions for Persistent Hemorrhagic Cystitis
If hematuria persists despite hydration, bladder irrigation, and cystoscopy with clot evacuation, then intravesical instillations should be considered. Our practice is to trial conservative management for 2–4 days (eg hydration and normal saline continuous bladder irrigation) if the patient’s clinical status allows and then proceed with cystoscopy and clot evacuation with or without fulguration. Pending findings and results, a transition to instillation of intravesical therapies may be needed if patients are not progressing. Care is taken to clear the bladder of all clots prior to intravesical instillation due to the difficulty associated with clot removal after clots interact with intravesical agents. Of note, data regarding the efficacy and safety of intravesical therapies are largely limited to case series. While there is no standardized treatment algorithm for HC, treatments typically progress from less invasive to more invasive and should be based on shared decision-making with the patient. For patients with symptoms refractory to less-invasive measures, interventional procedures and surgery are then utilized Figure 3.
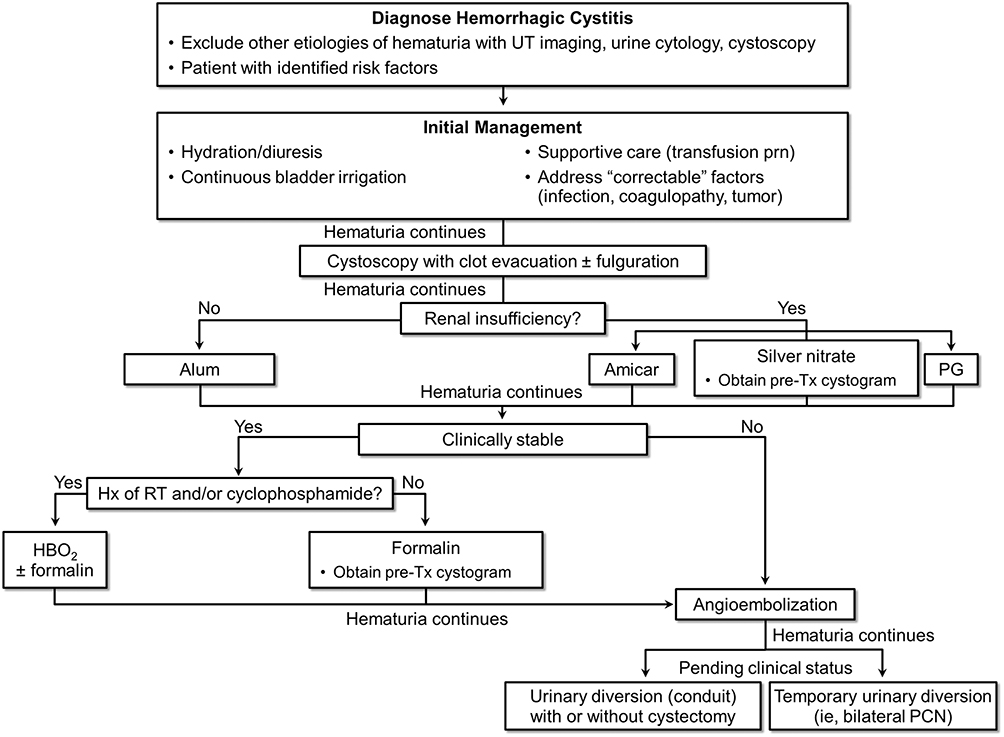 |
Figure 3 Algorithm for managing hemorrhagic cystitis. Reproduced with permission from: Linder BJ, Boorjian SA. Management of emergency bleeding, recalcitrant clots, and hemorrhagic cystitis. AUA Update Series. 2015;34 (Lesson 3).28 |
Alum
Given a favorable side effect profile and reasonable success rates, alum is commonly the first intravesical therapy utilized. Alum (aluminum ammonium sulfate or aluminum potassium sulfate) is an intravesical agent that induces hemostasis by causing protein precipitation, vasoconstriction, and decreased capillary permeability.33,34 Our practice is to irrigate the bladder with a 1% alum solution (50gm alum in 5L of sterile water) at a rate of 250 to 300 mL/hour once the bladder has been cleared of clots.33 This irrigation is done through a large-bore three-way catheter and can be initiated after clot evacuation, and treatment can be continued at the bedside without the need for anesthesia. The rate of alum treatment resulting in resolution of HC ranges from 66% to 100%.33,35 In the largest studied cohort of alum-treated patients (n=40), 60% did not require further treatment for HC prior to hospital discharge, and 33% did not require further treatment for HC at a median follow-up of 17 months.36 Furthermore, the median time to discharge was significantly shorter for patients who responded to alum than those who did not (3 days vs 13 days).36
Alum generally has a low-risk profile and is well tolerated. The most commonly reported adverse effects are irritative urinary symptoms such as bladder spasms, which occur in 35% and can be managed with anticholinergic or beta-3 agonist medications.35,36 Alum is renally cleared and should therefore be used with caution in patients with renal insufficiency who are at increased risk of systemic effects. Aluminum toxicity can manifest as mental status changes, malaise, speech disorder, and seizure.33,36,37 In patients with renal insufficiency, osteomalacia and anemia can also occur.35 If there is concern for aluminum toxicity, the alum irrigation should be stopped, and serum aluminum levels checked. In patients with normal renal function receiving alum, serum aluminum levels have been shown to increase from a mean baseline of 1.68 µmol/L to 3.36 µmol/L, while alum toxicity has been reported to occur at a mean aluminum level of 7.4 µmol/L.38–40
Aminocaproic Acid
Aminocaproic acid is a synthetic lysine that promotes hemostasis by competitively inhibiting plasminogen and plasmin, resulting in decreased fibrinolysis.35 It can be administered intravesically or orally, as approximately 80% is excreted in the urine unchanged.41 Intravesical dosing is 200 mg aminocaproic acid/L of 0.9% normal saline, while oral dosing is 100 to 150 mg/kg/day in divided doses. Both intravesical and oral routes of administration have demonstrated 92% to 100% effectiveness in resolving hemorrhagic cystitis, though these data are from small case series with no specific commenton durability of the treatment.42–44
Adverse events of aminocaproic acid are rare and most often associated with oral administration rather than intravesical. Such events include thrombotic complications, myopathy, and rhabdomyolysis.45,46 Importantly, a CT urogram or an equivalent study should be performed to rule out upper urinary tract hemorrhage prior to administration of oral aminocaproic acid, as upper tract clots can form and cause ureteral obstruction.47
Prostaglandins
Intravesical prostaglandins include carboprost tromethamine and prostaglandin F2-alpha. These agents lead to vascular smooth muscle constriction and platelet aggregation.35,48 One regimen for intravesical prostaglandin administration is 50 mL of 4 to 8 mg/L carboprost tromethamine instilled in the bladder for 1 hr followed by bladder drainage and then by another 50 mL of the solution for another hour. The solution is again drained, and the bladder is irrigated with normal saline. This can be repeated four times daily for a maximum of 400 mL of carboprost tromethamine administered within 8 hr. The concentration can be increased to 10 mg/L if there is no improvement. In addition, continuous bladder irrigation using 8 to 10 mg/L solution of carboprost tromethamine at 100 mL/hour for 10 hr can also be tried.35 The efficacy of intravesical prostaglandins in managing HC appears similar to that of alum, with successful control of HC in 60% of patients in a prospective randomized case series of 19 patients.36,48 While adverse effects of prostaglandins are limited to bladder spasms, notable drawbacks include higher cost, specific storage requirements, and lower availability.35,48 It is therefore considered an alternative if other agents are unsuccessful or unavailable.
Silver Nitrate
Silver nitrate induces chemical cauterization of hemorrhagic urothelium as it converts to to nitric acid upon bladder instillation. Silver nitrate must be mixed with water, as mixture with saline causes precipitation. Solution concentrations of 0.01% to 1% can be used, though instillation of concentrations 0.5% or higher can be painful and require general or spinal anesthesia.49 The available evidence regarding the efficacy of intravesical silver nitrate is limited, with fewer than 20 reported cases of successful HC control.50–52 The most recent report found that intravesical instillation did not result in resolution of hematuria for the nine patients studied, and all patients required additional interventions and red blood cell transfusions.49 Overall, there appears to be a limited role for intravesical silver nitrate in the management of HC. Of note, silver salts can precipitate during silver nitrate instillation, which can cause obstruction of upper urinary tracts; therefore, a cystogram should be performed prior to instillation to rule out vesicoureteral reflux.53
Pentosan Polysulfate Sodium
Pentosan polysulfate sodium (PPS) is a heparin analog that is well studied as an oral agent in the treatment of interstitial cystitis/bladder pain syndrome; it is used off-label for patients with HC.54 It has both anticoagulant and fibrinolytic properties, but the proposed mechanism of action of PPS is repair of the protective glycosaminoglycan lining of the urothelium. Several small case series have reported successful treatment of HC resulting from radiation and chemotherapy-induced HC with the use of oral PPS.55–59 The largest such report included 51 patients treated with 100 mg oral three times per day, 31 (61%) of whom were able to stop PPS or take a reduced dose without recurrence of hematuria.56 Similar success was noted in a cohort of 14 patients, with HC following RT, where 10 (71%) of patients achieved complete resolution of HC following PPS.55 Adverse effects of PPS include headache, nausea, diarrhea, and hepatic dysfunction; however, most concerning is the potential for maculopathy associated with chronic PPS use. Additionally, there appears to be an increased risk of maculopathy with higher cumulative exposure to PPS.60 Significant associations between PPS and maculopathy develop after 3 to 5 years of daily exposure to PPS.60–62 This risk led the United States Food and Drug Administration to issue a statement in the United States Prescribing Information for PPS capsules describing the risk of maculopathy and the need to conduct annual retinal examinations in patients on chronic PPS.63
Formalin
Intravesical formalin is reserved as a last-line intravesical intervention for recalcitrant HC when other agents have failed. Formalin is a 37% aqueous solution of formaldehyde that causes protein hydrolysis, resulting in capillary occlusion and coagulation of the bladder mucosa.33,35 It is usually administered initially as a 1% to 2% solution for 10 to 15 min under gravity instillation (<15 cm H2O), and dosing can be escalated if the initial treatment is unsuccessful; concentrations as high as 10% have been reported.35 Notably, the recommended dosing refers to formalin concentration, not formaldehyde concentration.33 Instillation is done in the operating room under spinal or general anesthesia due to significant discomfort associated with instillation of this solution. It is essential to perform a cystogram prior to instillation of formalin to rule out vesicoureteral reflux and bladder perforation, as reflux of formalin into the ureters could cause ureteral stricture. If reflux is present, occlusive ureteral catheters can be placed prior to instillation to limit ureteral exposure.64 If bladder perforation is identified, formalin instillation should not be performed due to the risk of intraperitoneal injury.65,66
When performing formalin instillation, the urethral catheter should be placed on light tension during instillation to limit urethral exposure, and all exposed skin surfaces should be covered with a combination of plastic adhesive surgical drapes and copious petroleum jelly. In female patients, vaginal packing should be placed. Prior to instillation, patients should be counseled on the risk of long-term bladder changes including fibrosis with decreased compliance and capacity, which can lead to significant voiding symptoms. Other documented complications of intravesical formalin include ureteral stenosis with resultant hydroureteronephrosis, bladder neck contracture, vesicovaginal fistula, and vesicorectal fistula.66–68
There has been a rare case reporting systemic formalin absorption resulting in death.69,70 Of note, this case was with formalin instillation at a higher concentration (4%) and with longer dwell times than in contemporary practices (30 min). Additionally, an animal model (dog) demonstrated that increasing concentrations were associated with higher absorption rates.70 A previous review found similar results, with higher concentrations and longer dwell times being associated with a greater risk of complications.71
Contemporary original research regarding the efficacy of intravesical formalin in treating HC is scarce. In the 1990’s, a cohort of 35 patients with hemorrhagic radiation cystitis refractory to conservative measures and clot evacuation were treated with 1% to 4% concentrations of intravesical formalin.66 While there was an initial complete response of 89% after a single instillation, hematuria recurred in 23% of these patients at a median follow-up of 7 months. Also of note, 31% of patients experienced major complications including bilateral ureteral stenosis, vesicovaginal fistula, and decreased bladder capacity, ultimately requiring urinary diversion. One patient died from formalin toxicity and hemorrhage. A more recent study reported longer-term outcomes in a similar cohort of eight patients (over a 14-year timeframe) with recalcitrant hemorrhagic radiation cystitis undergoing treatment with 1% to 4% intravesical formalin.67 At 8 months, 75% (6/8) had a resolution of hematuria, though 33% (2/6) of these patients ultimately required cystectomy, one for recurrent HC and one for end-stage bladder dysfunction. Similarly, successful resolution of HC has been reported as high as 88% at follow-up of 4 months in another older study.68
Tacrolimus
Tacrolimus is a calcineurin inhibitor that has been studied as an agent to treat hemorrhagic cystitis due to its potent anti-inflammatory effects and ability to induce acute arteriole vasoconstriction.72 Liposomal-encapsulated tacrolimus has been shown in rat models to decrease symptoms of radiation cystitis, decrease inflammatory histologic changes associated with radiation damage to the urothelium, and limit systemic absorption of tacrolimus.72–74 Clinical studies on the use of intravesical tacrolimus are limited, though success has been reported in one case report of refractory radiation-induced hemorrhagic cystitis.75 Intravesical tacrolimus for hemorrhagic cystitis is not used routinely and remains investigational.
Hyperbaric Oxygen Therapy
If intravesical agents are not successful in controlling hematuria, hyperbaric oxygen therapy (HBOT) is an effective option for managing HC from both RT and chemotherapy, though most data come from RT-induced HC. Patients are placed in a pressurized chamber and subjected to 100% inhalational oxygen at a pressure of 2 to 3 atmospheres. Multiple, usually 20–60, treatment sessions ranging from 90 to 120 min each are required.76–83 The mechanism of action is increased oxygen tension and tissue oxygenation at the level of the urothelium, which promotes angiogenesis and wound healing.78,84–86
In several smaller case series, partial or complete resolution of hematuria in patients with at least 12 months of follow-up occurred in 80% to 90%.87 Several studies reported reconstitution of normal bladder mucosa confirmed cystoscopically following completion of HBOT.77,78,83 In addition, these studies suggested that response to HBOT was more favorable when patients were treated within 6 months of hematuria onset.77,78,83,88
Larger randomized trials evaluating HBOT for HC demonstrate mixed results. In one study, 36 patients were randomized to either HBOT (100% oxygen at 2.5 atm for 60 min daily, 7 days per week for 30 days) or intravesical instillation of hyaluronic acid (40 mg of hyaluronic acid instilled in the bladder for at least 20 min weekly for 1 month and then monthly for the following 2 months).89 At a follow-up of 12 months, no significant differences between the HBOT and intravesical hyaluronic acid groups were detected, with a complete response of 50% (10/20 patients) versus 75% (12/16 patients) and a partial response of 35% (7/20 patients) versus 19% (3/16 patients), respectively.
In contrast, HBOT was shown to offer some benefit over the control group in a randomized controlled trial of 87 patients with radiation cystitis who completed pelvic RT at least 6 months prior.90 Patients were randomized to either HBOT (100% oxygen at 2.4 to 2.5 atm for 80 to 90 min per session for 30 to 40 sessions) or to a control group that received no interventions. The primary endpoint was a change in Expanded Prostate Index Composite (EPIC) score, a validated patient-reported outcomes measure.91–93 Notably, patients with hematuria requiring ongoing transfusion were excluded.90 Patients were followed for 4 to 6 months after completion of RT (6 to 8 months post randomization), at which point 73% of patients randomized to HBOT demonstrated clinically significant improvement, of which 23% had no change, and 5% worsened according to EPIC score. In the control group, 34% improved, 54% had no change, and 11% worsened. Longer term outcomes were not described.
In general, multi-year follow-up of HBOT is limited, though recurrence rates have been reported from 25% to 73% at 5 years.84,88 Data is more limited on HBOT to treat cyclophosphamide-associated HC, but small case series do support a high degree of efficacy at up to 1 year of follow-up.94,95
Approximately 40% of patients receiving HBOT may experience adverse events associated with HBOT including otalgia and barotrauma, which may require placement of tympanostomy tubes.79 In addition, hyperoxia-induced transient myopia with visual changes has been reported in up to 12%.90 Other ocular complications such as cataract formation are a known risk of HBOT due to oxidative damage.96,97
Selective Angioembolization
In patients who are hemodynamically unstable because of gross hematuria and in those with refractory HC despite intravesical agents and HBOT, one may consider selective iliac artery angioembolization. During this procedure, an interventional radiologist places an occlusive agent (ie coil or gel foam) in the anterior branch of the internal iliac artery.98,99 Resolution of hematuria following embolization has been reported in up to 100% in some case series and has been shown to be effective in managing HC resulting from chemotherapy and radiation.100–103 More recently, superselective vesical artery embolization, in which only the vesical artery is embolized, has been described, which can result in resolution of gross hematuria within 48 hr.100 After superselective vesical artery embolization, recurrence has been reported in 11% to 17% of patients, with follow-up ranging from 11 to 14.5 months; most recurrences were managed conservatively, while others required repeat angioembolization. Notably, no patients reported bladder or sexual dysfunction with a median follow-up of 14.5 months.100,104 Risks of selective angioembolization include occlusion of the posterior branch of the internal iliac artery, which could compromise the superior gluteal artery and lead to gluteal pain.105 Although rare, another notable risk is bladder necrosis.106
Urinary Diversion
In cases of HC refractory to the previously listed treatment modalities, urinary diversion may be necessary. Success with diversion via percutaneous nephrostomy tubes is limited to small series.107,108 A more definitive intervention comes in the form of a cystectomy with urinary diversion, which is typically a treatment of last resort given its invasive nature. This can typically be done with a simple cystectomy and an ileal or transverse colon conduit, taking care to choose bowel that is unaffected by prior radiation in those with a history of RT.5,109,110 Alternatively, patients who are not candidates for intestinal urinary diversion can undergo cystectomy with either cutaneous ureterostomies or ureteral ligation with percutaneous nephrostomy tube drainage. The largest available series on cystectomy for HC included 21 patients, 81% of whom had radiation as the underlying etiology.5 Severe complications (Clavien III–V) occurred in 42% of cases, with a 90-d mortality rate of 16%. As such, this treatment remains a last resort for patients with emergency hemorrhage from the bladder.
Conclusions
HC remains one of the most challenging clinical scenarios for urologists to manage. While there are multiple treatment options, it is important to bear in mind several practical points. First, for significant gross hematuria with blood clots, the patient is at risk of clot obstruction. Therefore, once the patient is initially stabilized, ensuring adequate bladder drainage is crucial. When considering intravesical options, one should consult with pharmacy personnel to determine which agents are available, as this varies by institution. In addition, clinical judgement is required to make the decision to escalate interventions, and one must factor in the patient’s overall clinical and functional status. For example, one must avoid the pitfall of prolonging the inpatient course with subsequent functional and clinical decline with undue delay in management with therapies if they are not improving the hematuria.
In general, for patients who are hemodynamically stable, our practice is to begin with aggressive manual bladder irrigation to remove clots followed by initiation of continuous bladder irrigation. If hematuria continues despite 48 to 72 hr of bladder irrigation, then we proceed to the operating room for cystoscopy and clot evacuation; we will then start intravesical instillation of alum in the operating room at the conclusion of the case. We typically use alum since this is readily available at our institution and our personnel have experience using it. If hematuria persists despite these measures, we participate in shared decision-making, with the patient regarding options of trialing another non-formalin intravesical agent, hyperbaric oxygen therapy, or returning to the operating room for formalin instillation. Beyond this, we discuss proceeding to procedural interventions such as nephrostomy tube placement, selective angioembolization, or cystectomy with urinary diversion.
Funding
No funding was received for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Antoniewicz AA, Zapala L, Poletajew S, Borowka A. Macroscopic hematuria-a leading urological problem in patients on anticoagulant therapy: is the common diagnostic standard still advisable? ISRN Urol. 2012;2012:710734. doi:10.5402/2012/710734
2. Mariani AJ, Mariani MC, Macchioni C, Stams UK, Hariharan A, Moriera A. The significance of adult hematuria: 1000 hematuria evaluations including a risk-benefit and cost-effectiveness analysis. J Urol. 1989;141(2):350–355. doi:10.1016/S0022-5347(17)40763-4
3. Payne H, Adamson A, Bahl A, et al. Chemical- and radiation-induced haemorrhagic cystitis: current treatments and challenges. BJU Int. 2013;112(7):885–897. doi:10.1111/bju.12291
4. Lee V, An Y, Park HS, Yu JB, Kim SP, Jairam V. Emergency department visits for radiation cystitis among patients with a prostate cancer history. BJU Int. 2022;130(2):208–216. doi:10.1111/bju.15650
5. Linder BJ, Tarrell RF, Boorjian SA. Cystectomy for refractory hemorrhagic cystitis: contemporary etiology, presentation and outcomes. J Urol. 2014;192(6):1687–1692. doi:10.1016/j.juro.2014.06.030
6. Creaven PJ, Allen LM, Cohen MH, Nelson RL. Studies on the clinical pharmacology and toxicology of isophosphamide (NSC-109724). Cancer Treat Rep. 1976;60(4):445–449.
7. Van Dyk JJ, Falkson HC, Van der Merwe AM, Falkson G. Unexpected toxicity in patients treated with iphosphamide. Cancer Res. 1972;32(5):921–924.
8. Kemeny N, Reichman B, Dougherty J, Lipperman R, Cheng E. Phase II trial of ifosfamide and mesna in advanced colorectal cancer. Cancer Treat Rep. 1987;71(6):663–664.
9. Scheulen ME, Niederle N, Bremer K, Schutte J, Seeber S. Efficacy of ifosfamide in refractory malignant diseases and uroprotection by mesna: results of a clinical Phase II-study with 151 patients. Cancer Treat Rev. 1983;10(Suppl A):93–101. doi:10.1016/S0305-7372(83)80013-9
10. Nobile MT, Rosso R, Brema F, Cinquegrana A, Santi L. Phase II study of ifosfamide combined with Mesna uroprotection in advanced non-small-cell lung carcinoma and other solid tumors. Tumori. 1984;70(5):433–437. doi:10.1177/030089168407000508
11. Brade WP, Herdrich K, Varini M. Ifosfamide--pharmacology, safety and therapeutic potential. Cancer Treat Rev. 1985;12(1):1–47. doi:10.1016/0305-7372(85)90011-8
12. Efros MD, Ahmed T, Coombe N, Choudhury MS. Urologic complications of high-dose chemotherapy and bone marrow transplantation. Urology. 1994;43(3):355–360. doi:10.1016/0090-4295(94)90079-5
13. Ilhan O, Koc H, Akan H, et al. Hemorrhagic cystitis as a complication of bone marrow transplantation. J Chemother. 1997;9(1):56–61. doi:10.1179/joc.1997.9.1.56
14. Cox PJ. Cyclophosphamide cystitis and bladder cancer. A hypothesis. Eur J Cancer. 1979;15(8):1071–1072. doi:10.1016/0014-2964(79)90296-2
15. Philips FS, Sternberg SS, Cronin AP, Vidal PM. Cyclophosphamide and urinary bladder toxicity. Cancer Res. 1961;21:1577–1589.
16. Korkmaz A, Oter S, Deveci S, et al. Involvement of nitric oxide and hyperbaric oxygen in the pathogenesis of cyclophosphamide induced hemorrhagic cystitis in rats. J Urol. 2003;170(6 Pt 1):2498–2502. doi:10.1097/01.ju.0000085593.31396.d8
17. Korkmaz A, Topal T, Oter S. Pathophysiological aspects of cyclophosphamide and ifosfamide induced hemorrhagic cystitis; implication of reactive oxygen and nitrogen species as well as PARP activation. Cell Biol Toxicol. 2007;23(5):303–312. doi:10.1007/s10565-006-0078-0
18. Shepherd JD, Pringle LE, Barnett MJ, Klingemann HG, Reece DE, Phillips GL. Mesna versus hyperhydration for the prevention of cyclophosphamide-induced hemorrhagic cystitis in bone marrow transplantation. J Clin Oncol. 1991;9(11):2016–2020. doi:10.1200/JCO.1991.9.11.2016
19. Ballen KK, Becker P, Levebvre K, et al. Safety and cost of hyperhydration for the prevention of hemorrhagic cystitis in bone marrow transplant recipients. Oncology. 1999;57(4):287–292. doi:10.1159/000012062
20. Mendenhall WM, Henderson RH, Costa JA, et al. Hemorrhagic radiation cystitis. Am J Clin Oncol. 2015;38(3):331–336. doi:10.1097/COC.0000000000000016
21. Smit SG, Heyns CF. Management of radiation cystitis. Nat Rev Urol. 2010;7(4):206–214. doi:10.1038/nrurol.2010.23
22. Levenback C, Eifel PJ, Burke TW, Morris M, Gershenson DM. Hemorrhagic cystitis following radiotherapy for stage Ib cancer of the cervix. Gynecol Oncol. 1994;55(2):206–210. doi:10.1006/gyno.1994.1278
23. Eifel PJ, Levenback C, Wharton JT, Oswald MJ. Time course and incidence of late complications in patients treated with radiation therapy for FIGO stage IB carcinoma of the uterine cervix. Int J Radiat Oncol Biol Phys. 1995;32(5):1289–1300. doi:10.1016/0360-3016(95)00118-I
24. Corman JM, McClure D, Pritchett R, Kozlowski P, Hampson NB. Treatment of radiation induced hemorrhagic cystitis with hyperbaric oxygen. J Urol. 2003;169(6):2200–2202. doi:10.1097/01.ju.0000063640.41307.c9
25. Denton AS, Clarke NW, Maher EJ. Non-surgical interventions for late radiation cystitis in patients who have received radical radiotherapy to the pelvis. Cochrane Database Syst Rev. 2002;2002(3):CD001773. doi:10.1002/14651858.CD001773
26. Suresh UR, Smith VJ, Lupton EW, Haboubi NY. Radiation disease of the urinary tract: histological features of 18 cases. J Clin Pathol. 1993;46(3):228–231. doi:10.1136/jcp.46.3.228
27. Phadke KD, Vijayakumar M, Sharma J, Iyengar A; Indian Pediatric Nephrology G. Consensus statement on evaluation of hematuria. Indian Pediatr. 2006;43(11):965–973.
28. Linder BJ, Boorjian SA. Management of emergency bleeding, recalcitrant clots, and hemorrhagic cystitis. AUA Updat Ser. 2015;34(3):1.
29. Barocas DA, Boorjian SA, Alvarez RD, et al. Microhematuria: AUA/SUFU guideline. J Urol. 2020;204(4):778–786. doi:10.1097/JU.0000000000001297
30. Kaplan JR, Wolf JS Jr. Efficacy and survival associated with cystoscopy and clot evacuation for radiation or cyclophosphamide induced hemorrhagic cystitis. J Urol. 2009;181(2):641–646. doi:10.1016/j.juro.2008.10.037
31. Pascoe C, Christidis D, Manning TG, Lamb BW, Murphy DG, Lawrentschuk N. Photoselective vaporization of the bladder for the management of radiation cystitis-technique and initial outcomes. Urology. 2019;123:295. doi:10.1016/j.urology.2018.04.030
32. Vicente Rodriguez J, Farina LA. Perforación intestinal tras tratamiento de cistitis rádica con laser de neodimio:YAG [Intestinal perforation after treatment of radiation cystitis using the neodymium:YAG laser]. Actas Urol Esp. 1991;15(5):459–461. Spanish.
33. Choong SK, Walkden M, Kirby R. The management of intractable haematuria. BJU Int. 2000;86(9):951–959. doi:10.1046/j.1464-410x.2000.00900.x
34. Thompson IM, Teague JL, Mueller EJ, Rodriguez FR. Intravesical alum irrigation for intractable bleeding secondary to adenocarcinoma of the prostate. J Urol. 1987;137(3):525–526. doi:10.1016/S0022-5347(17)44098-5
35. Abt D, Bywater M, Engeler DS, Schmid HP. Therapeutic options for intractable hematuria in advanced bladder cancer. Int J Urol. 2013;20(7):651–660. doi:10.1111/iju.12113
36. Westerman ME, Boorjian SA, Linder BJ. Safety and efficacy of intravesical alum for intractable hemorrhagic cystitis: a contemporary evaluation. Int Braz J Urol. 2016;42(6):1144–1149. doi:10.1590/s1677-5538.ibju.2015.0588
37. Perazella M, Brown E. Acute aluminum toxicity and alum bladder irrigation in patients with renal failure. Am J Kidney Dis. 1993;21(1):44–46. doi:10.1016/S0272-6386(12)80719-0
38. Goswami AK, Mahajan RK, Nath R, Sharma SK. How safe is 1% alum irrigation in controlling intractable vesical hemorrhage? J Urol. 1993;149(2):264–267. doi:10.1016/S0022-5347(17)36051-2
39. Roberts NB, Williams P. Serum aluminium measurement by DC plasma emission spectrometry. Ann Clin Biochem. 1988;25(Pt 2):169–175. doi:10.1177/000456328802500207
40. Fleming LW, Stewart W, Fell GS, Halls DJ. The effect of oral aluminium therapy on plasma aluminium levels in patients with chronic renal failure in an area with low water aluminium. Clin Nephrol. 1982;17(5):222–227.
41. McNicol FA, Alkjaersig N, Sherry S. The absorption, distribution, and excretion ofϵ-aminocaproic acid following oral or intravenous administration to man. J Lab Clin Med. 1962;59(1):1.
42. Stefanini M, English HA, Taylor AE. Safe and effective, prolonged administration of epsilon aminocaproic acid in bleeding from the urinary tract. J Urol. 1990;143(3):559–561. doi:10.1016/S0022-5347(17)40018-8
43. Singh I, Laungani GB. Intravesical epsilon aminocaproic acid in management of intractable bladder hemorrhage. Urology. 1992;40(3):227–229. doi:10.1016/0090-4295(92)90479-G
44. Kaye JD, Smith EA, Kirsch AJ, Cerwinka WH, Elmore JM. Preliminary experience with epsilon aminocaproic acid for treatment of intractable upper tract hematuria in children with hematological disorders. J Urol. 2010;184(3):1152–1157. doi:10.1016/j.juro.2010.05.020
45. Manjunath G, Fozailoff A, Mitcheson D, Sarnak MJ. Epsilon-aminocaproic acid and renal complications: case report and review of the literature. Clin Nephrol. 2002;58(1):63–67. doi:10.5414/CNP58063
46. Kane MJ, Silverman LR, Rand JH, Paciucci PA, Holland JF. Myonecrosis as a complication of the use of epsilon amino-caproic acid: a case report and review of the literature. Am J Med. 1988;85(6):861–863. doi:10.1016/S0002-9343(88)80037-8
47. Geltzeiler J, Schwartz D. Obstruction of solitary kidney due to epsilon-aminocaproic-acid-induced fibrin clot formation. Urology. 1984;24(1):64–66. doi:10.1016/0090-4295(84)90390-x
48. Praveen BV, Sankaranarayanan A, Vaidyanathan S. A comparative study of intravesical instillation of 15(s) 15 Me alpha and alum in the management of persistent hematuria of vesical origin. Int J Clin Pharmacol Ther Toxicol. 1992;30(1):7–12.
49. Montgomery BD, Boorjian SA, Ziegelmann MJ, Joyce DD, Linder BJ. Intravesical silver nitrate for refractory hemorrhagic cystitis. Turk J Urol. 2016;42(3):197–201. doi:10.5152/tud.2016.38445
50. Kumar AP, Wrenn EL Jr, Jayalakshmamma B, Conrad L, Quinn P, Cox C. Silver nitrate irrigation to control bladder hemorrhage in children receiving cancer therapy. J Urol. 1976;116(1):85–86. doi:10.1016/S0022-5347(17)58690-5
51. Diamond DA, Jeffs RD, Marshall FF. Control of prolonged, benign, renal hematuria by silver nitrate instillation. Urology. 1981;18(4):337–341. doi:10.1016/0090-4295(81)90384-8
52. Jerkins GR, Noe HN, Hill DE. An unusual complication of silver nitrate treatment of hemorrhagic cystitis: case report. J Urol. 1986;136(2):456–458. doi:10.1016/S0022-5347(17)44907-X
53. Raghavaiah NV, Soloway MS. Anuria following silver nitrate irrigation for intractable bladder hemorrhage. J Urol. 1977;118(4):681–682. doi:10.1016/S0022-5347(17)58154-9
54. Chermansky CJ, Guirguis MO. Pharmacologic management of interstitial cystitis/bladder pain syndrome. Urol Clin North Am. 2022;49(2):273–282. doi:10.1016/j.ucl.2022.01.003
55. Hampson SJ, Woodhouse CR. Sodium pentosan polysulphate in the management of haemorrhagic cystitis: experience with 14 patients. Eur Urol. 1994;25(1):40–42. doi:10.1159/000475245
56. Sandhu SS, Goldstraw M, Woodhouse CR. The management of haemorrhagic cystitis with sodium pentosan polysulphate. BJU Int. 2004;94(6):845–847. doi:10.1111/j.1464-410X.2004.05044.x
57. Toren PJ, Norman RW. Cyclophosphamide induced hemorrhagic cystitis successfully treated with pentosanpolysulphate. J Urol. 2005;173(1):103. doi:10.1097/01.ju.0000146626.78180.83
58. Duthie G, Whyte L, Chandran H, Lawson S, Velangi M, McCarthy L. Introduction of sodium pentosan polysulfate and avoidance of urethral catheterisation: improved outcomes in children with haemorrhagic cystitis post stem cell transplant/chemotherapy. J Pediatr Surg. 2012;47(2):375–379. doi:10.1016/j.jpedsurg.2011.11.037
59. Hatch RV, Freyer CW, Carulli A, et al. Pentosan polysulfate for the treatment of hemorrhagic cystitis after allogeneic hematopoietic cell transplant. J Oncol Pharm Pract. 2022;28(7):1609–1612. doi:10.1177/10781552221105295
60. Vora RA, Patel AP, Melles R. Prevalence of maculopathy associated with long-term pentosan polysulfate therapy. Ophthalmology. 2020;127(6):835–836. doi:10.1016/j.ophtha.2020.01.017
61. Hanif AM, Shah R, Yan J, et al. Strength of association between pentosan polysulfate and a novel maculopathy. Ophthalmology. 2019;126(10):1464–1466. doi:10.1016/j.ophtha.2019.04.024
62. Jain N, Li AL, Yu Y, VanderBeek BL. Association of macular disease with long-term use of pentosan polysulfate sodium: findings from a US cohort. Br J Ophthalmol. 2020;104(8):1093–1097. doi:10.1136/bjophthalmol-2019-314765
63. National Institutes of Health. ELMIRON- pentosan polysulfate sodium capsule, gelatin coated; 2022. Available from: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=f0ba651e-3d8a-11df-8fbe-119855d89593.
64. Bright JF, Tosi SE, Crichlow RW, Selikowitz SM. Prevention of vesicoureteral reflux with Fogarty catheters during formalin therapy. J Urol. 1977;118(6):950–952. doi:10.1016/S0022-5347(17)58259-2
65. Capen CV, Weigel JW, Magrina JF, Masterson BJ. Intraperitoneal spillage of formalin after intravesical instillation. Urology. 1982;19(6):599–601. doi:10.1016/0090-4295(82)90007-3
66. Dewan AK, Mohan GM, Ravi R. Intravesical formalin for hemorrhagic cystitis following irradiation of cancer of the cervix. Int J Gynaecol Obstet. 1993;42(2):131–135. doi:10.1016/0020-7292(93)90626-8
67. Ziegelmann MJ, Boorjian SA, Joyce DD, Montgomery BD, Linder BJ. Intravesical formalin for hemorrhagic cystitis: a contemporary cohort. Can Urol Assoc J. 2017;11(3–4):E79–E82. doi:10.5489/cuaj.4047
68. Vicente J, Rios G, Caffaratti J. Intravesical formalin for the treatment of massive hemorrhagic cystitis: retrospective review of 25 cases. Eur Urol. 1990;18(3):204–206. doi:10.1159/000463910
69. Rao MS, Singhal PC, Bapna BC, et al. Fatal complication of intravesical formalin during control of intractable hemorrhage from radiation cystitis. Urology. 1978;11(6):588–590. doi:10.1016/0090-4295(78)90008-0
70. Eickenberg HU, Adcock R. Vascular absorption of intravesical formalin in cyclophosphamide induced haemorrhagic cystitis. Urol Res. 1976;4(1):5–8. doi:10.1007/BF00256128
71. Godec CJ, Gleich P. Intractable hematuria and formalin. J Urol. 1983;130(4):688–691. doi:10.1016/S0022-5347(17)51405-6
72. Rajaganapathy BR, Janicki JJ, Levanovich P, et al. Intravesical liposomal tacrolimus protects against radiation cystitis induced by 3-beam targeted bladder radiation. J Urol. 2015;194(2):578–584. doi:10.1016/j.juro.2015.03.108
73. Chuang YC, Tyagi P, Huang HY, et al. Intravesical immune suppression by liposomal tacrolimus in cyclophosphamide-induced inflammatory cystitis. Neurourol Urodyn. 2011;30(3):421–427. doi:10.1002/nau.20981
74. Nirmal J, Tyagi P, Chancellor MB, et al. Development of potential orphan drug therapy of intravesical liposomal tacrolimus for hemorrhagic cystitis due to increased local drug exposure. J Urol. 2013;189(4):1553–1558. doi:10.1016/j.juro.2012.10.123
75. Dave CN, Chaus F, Chancellor MB, Lajness M, Peters KM. Innovative use of intravesical tacrolimus for hemorrhagic radiation cystitis. Int Urol Nephrol. 2015;47(10):1679–1681. doi:10.1007/s11255-015-1098-6
76. Weiss JP, Boland FP, Mori H, et al. Treatment of radiation-induced cystitis with hyperbaric oxygen. J Urol. 1985;134(2):352–354. doi:10.1016/S0022-5347(17)47166-7
77. Mathews R, Rajan N, Josefson L, Camporesi E, Makhuli Z. Hyperbaric oxygen therapy for radiation induced hemorrhagic cystitis. J Urol. 1999;161(2):435–437. doi:10.1016/S0022-5347(01)61914-1
78. Chong KT, Hampson NB, Corman JM. Early hyperbaric oxygen therapy improves outcome for radiation-induced hemorrhagic cystitis. Urology. 2005;65(4):649–653. doi:10.1016/j.urology.2004.10.050
79. Oliai C, Fisher B, Jani A, et al. Hyperbaric oxygen therapy for radiation-induced cystitis and proctitis. Int J Radiat Oncol Biol Phys. 2012;84(3):733–740. doi:10.1016/j.ijrobp.2011.12.056
80. Oscarsson N, Arnell P, Lodding P, Ricksten SE, Seeman-Lodding H. Hyperbaric oxygen treatment in radiation-induced cystitis and proctitis: a prospective cohort study on patient-perceived quality of recovery. Int J Radiat Oncol Biol Phys. 2013;87(4):670–675. doi:10.1016/j.ijrobp.2013.07.039
81. Yoshida T, Kawashima A, Ujike T, Uemura M, Nishimura K, Miyoshi S. Hyperbaric oxygen therapy for radiation-induced hemorrhagic cystitis. Int J Urol. 2008;15(7):639–641. doi:10.1111/j.1442-2042.2008.02053.x
82. Mougin J, Souday V, Martin F, Azzouzi AR, Bigot P. Evaluation of hyperbaric oxygen therapy in the treatment of radiation-induced hemorrhagic cystitis. Urology. 2016;94:42–46. doi:10.1016/j.urology.2016.04.015
83. Dellis A, Papatsoris A, Kalentzos V, Deliveliotis C, Skolarikos A. Hyberbaric oxygen as sole treatment for severe radiation - induced haemorrhagic cystitis. Int Braz J Urol. 2017;43(3):489–495. doi:10.1590/s1677-5538.ibju.2016.0451
84. Del Pizzo JJ, Chew BH, Jacobs SC, Sklar GN. Treatment of radiation induced hemorrhagic cystitis with hyperbaric oxygen: long-term followup. J Urol. 1998;160(3 Pt 1):731–733. doi:10.1016/S0022-5347(01)62770-8
85. Neovius EB, Lind MG, Lind FG. Hyperbaric oxygen therapy for wound complications after surgery in the irradiated head and neck: a review of the literature and a report of 15 consecutive patients. Head Neck. 1997;19(4):315–322. doi:10.1002/(SICI)1097-0347(199707)19:4<315::AID-HED10>3.0.CO;2-8
86. Cianci P, Sato R. Adjunctive hyperbaric oxygen therapy in the treatment of thermal burns: a review. Burns. 1994;20(1):5–14. doi:10.1016/0305-4179(94)90099-X
87. Degener S, Pohle A, Strelow H, et al. Long-term experience of hyperbaric oxygen therapy for refractory radio- or chemotherapy-induced haemorrhagic cystitis. BMC Urol. 2015;15:38. doi:10.1186/s12894-015-0035-4
88. Pereira D, Ferreira C, Catarino R, et al. Hyperbaric oxygen for radiation-induced cystitis: a long-term follow-up. Actas Urol Esp. 2020;44(8):561–567. doi:10.1016/j.acuro.2020.03.010
89. Shao Y, Lu GL, Shen ZJ. Comparison of intravesical hyaluronic acid instillation and hyperbaric oxygen in the treatment of radiation-induced hemorrhagic cystitis. BJU Int. 2012;109(5):691–694. doi:10.1111/j.1464-410X.2011.10550.x
90. Oscarsson N, Muller B, Rosen A, et al. Radiation-induced cystitis treated with hyperbaric oxygen therapy (RICH-ART): a randomised, controlled, Phase 2–3 trial. Lancet Oncol. 2019;20(11):1602–1614. doi:10.1016/S1470-2045(19)30494-2
91. Wei JT, Dunn RL, Litwin MS, Sandler HM, Sanda MG. Development and validation of the expanded prostate cancer index composite (EPIC) for comprehensive assessment of health-related quality of life in men with prostate cancer. Urology. 2000;56(6):899–905. doi:10.1016/S0090-4295(00)00858-X
92. Gil KM, Pugh SL, Klopp AH, et al. Expanded validation of the EPIC bowel and urinary domains for use in women with gynecologic cancer undergoing postoperative radiotherapy. Gynecol Oncol. 2019;154(1):183–188. doi:10.1016/j.ygyno.2019.04.682
93. Umbehr MH, Bachmann LM, Poyet C, et al. The German version of the Expanded Prostate Cancer Index Composite (EPIC): translation, validation and minimal important difference estimation. Health Qual Life Outcomes. 2018;16(1):36. doi:10.1186/s12955-018-0859-1
94. Kaur D, Khan SP, Rodriguez V, Arndt C, Claus P. Hyperbaric oxygen as a treatment modality in cyclophosphamide-induced hemorrhagic cystitis. Pediatr Transplant. 2018;22(4):e13171. doi:10.1111/petr.13171
95. Ajith Kumar S, Prasanth P, Tripathi K, Ghosh P. Hyperbaric oxygen-A new horizon in treating cyclophosphamide-induced hemorrhagic cystitis. Indian J Urol. 2011;27(2):272–273. doi:10.4103/0970-1591.82849
96. Palmquist BM, Philipson B, Barr PO. Nuclear cataract and myopia during hyperbaric oxygen therapy. Br J Ophthalmol. 1984;68(2):113–117. doi:10.1136/bjo.68.2.113
97. McMonnies CW. Hyperbaric oxygen therapy and the possibility of ocular complications or contraindications. Clin Exp Optom. 2015;98(2):122–125. doi:10.1111/cxo.12203
98. Palandri F, Bonifazi F, Rossi C, et al. Successful treatment of severe hemorrhagic cystitis with selective vesical artery embolization. Bone Marrow Transplant. 2005;35(5):529–530. doi:10.1038/sj.bmt.1704818
99. Ward JF, Velling TE. Transcatheter therapeutic embolization of genitourinary pathology. Rev Urol. 2000;2(4):236–252.
100. Mohan S, Kumar S, Dubey D, Phadke RV, Baijal SS, Kathuria M. Superselective vesical artery embolization in the management of intractable hematuria secondary to hemorrhagic cystitis. World J Urol. 2019;37(10):2175–2182. doi:10.1007/s00345-018-2604-0
101. Han Y, Wu D, Sun A, et al. Selective embolization of the internal iliac arteries for the treatment of severe hemorrhagic cystitis following hematopoietic SCT. Bone Marrow Transplant. 2008;41(10):881–886. doi:10.1038/bmt.2008.4
102. Gine E, Rovira M, Real I, et al. Successful treatment of severe hemorrhagic cystitis after hemopoietic cell transplantation by selective embolization of the vesical arteries. Bone Marrow Transplant. 2003;31(10):923–925. doi:10.1038/sj.bmt.1703954
103. De Berardinis E, Vicini P, Salvatori F, Sciarra A, Gentile V, Di Silverio F. Superselective embolization of bladder arteries in the treatment of intractable bladder haemorrhage. Int J Urol. 2005;12(5):503–505. doi:10.1111/j.1442-2042.2005.01074.x
104. Zhou C, Zhou CG, Wang B, Liu XL, Shi HB, Liu S. Superselective vesical artery embolization for intractable hemorrhagic cystitis following hematopoietic stem cell transplantation: a single-center retrospective study in 26 patients. Cardiovasc Intervent Radiol. 2021;44(6):943–951. doi:10.1007/s00270-021-02786-5
105. Yasumura K, Ikegami K, Kamohara T, Nohara Y. High incidence of ischemic necrosis of the gluteal muscle after transcatheter angiographic embolization for severe pelvic fracture. J Trauma. 2005;58(5):985–990. doi:10.1097/01.TA.0000162625.63241.12
106. Sieber PR. Bladder necrosis secondary to pelvic artery embolization: case report and literature review. J Urol. 1994;151(2):422. doi:10.1016/S0022-5347(17)34969-8
107. Farhan A, Lyons GR. Clinical outcomes following percutaneous urinary diversion for hemorrhagic cystitis. J Vasc Interv Radiol. 2022;33(7):841–844. doi:10.1016/j.jvir.2022.03.605
108. Sneiders A, Pryor JL. Percutaneous nephrostomy drainage in the treatment of severe hemorrhagic cystitis. J Urol. 1993;150(3):966–967. doi:10.1016/S0022-5347(17)35663-X
109. Noe HN, McSwain HM. Management of severe reflux in the patient with cyclophosphamide cystitis. J Urol. 1983;130(4):769–771. doi:10.1016/S0022-5347(17)51451-2
110. Marsh FP, Vince FP, Pollock DJ, Blandy JP, Blandy JP, Chir. M. Cyclophosphamide necrosis of bladder causing calcification, contracture and reflux; treated by colocystoplasty. Br J Urol. 1971;43(3):324–332. doi:10.1111/j.1464-410X.1971.tb12049.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.