")
Back to Journals » Advances in Medical Education and Practice » Volume 15
Health Care Clinical Preceptors’ Attitudes Towards Interprofessional Education in Saudi Arabia: A Cross-Sectional Study
Authors Al Nufaiei ZF , Bukhari AA, Abalkhail NA, Melebari RM, Alluhibi R, Al Zhranei RM , Allhadian F, Turkestani FA , Alsulami M , Alshamrani KM , Abdelrahman EI, Zipp GP
Received 8 December 2023
Accepted for publication 13 April 2024
Published 22 April 2024 Volume 2024:15 Pages 343—355
DOI https://doi.org/10.2147/AMEP.S451938
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Ziyad F Al Nufaiei,1– 3 Amr A Bukhari,1– 3 Nawaf A Abalkhail,1– 3 Raif M Melebari,1– 3 Reem Alluhibi,1– 3 Raid M Al Zhranei,1– 3 Fahad Allhadian,1– 3 Faisal A Turkestani,1– 3 Maher Alsulami,2– 4 Khalid M Alshamrani,2,3,5 Emad I Abdelrahman,6 Genevieve P Zipp7
1Department of Respiratory Therapy, College of Applied Medical Sciences, King Saud Bin Abdulaziz University for Health Sciences, Jeddah City, Saudi Arabia; 2King Abdullah International Medical Research Center, Jeddah City, Saudi Arabia; 3Ministry of the National Guard - Health Affairs, Jeddah City, Saudi Arabia; 4Department of Emergency Medical Services, College of Applied Medical Sciences, King Saud Bin Abdulaziz University for Health Sciences, Jeddah City, Saudi Arabia; 5Department of Radiological Sciences, College of Applied Medical Sciences, King Saud Bin Abdulaziz University for Health Sciences, Jeddah City, Saudi Arabia; 6Internal Medicine Department, Albayt Medical General Center, Mecca City, Saudi Arabia; 7Department of Interprofessional Health Sciences & Health Administration, School of Health and Medical Sciences, Seton Hall University, Nutley, NJ, USA
Correspondence: Ziyad F Al Nufaiei, RRT-NPS, CPFT Department of Respiratory Therapy, College of Applied Medical Sciences, King Saud Bin Abdulaziz University for Health Sciences, Jeddah City, Saudi Arabia, Email [email protected]
Introduction: IPE fosters a dynamic learning environment that may promote students’ knowledge, abilities, and collaborative approach towards addressing challenging clinical circumstances. While much has been reported in the literature regarding these diverse IPE learning environments, limited information exists regarding clinical preceptors’ attitude and perceptions of IPE, especially in Saudi Arabia. Given the impact clinical preceptors have on the formation of healthcare students exploring their perceptions, which may impact their actions is imperative.
Methodology: The study focused on understanding the attitudes and perceptions of clinical preceptors towards IPE in a healthcare setting in Saudi Arabia. The study was conducted in Saudi Arabia. Data was collected via Email letter of solicitation (LOS) which included a link to the Readiness for Interprofessional Learning Scale (RIPLS) survey. The LOS was sent to all the health care programs in Saudi Arabia.
Results: The study surveyed 182 clinical preceptors. The findings revealed consistent favorable opinions towards “Teamwork and Collaboration”. The majority of preceptors concurred that learning alongside other students would increase students’ efficiency on healthcare teams and deepen their comprehension of clinical issues. The “Roles and Responsibilities” category, however, obtained lower ranks in general from the preceptors. Not surprising, differences in rankings were greatest between preceptors who had and did not have IPE exposure, there were significant variations in views toward “Teamwork and Collaboration”, “Negative Professional Identity”, and “Roles and Responsibilities”. Preceptors exposed to IPE showed lower median ratings for “Negative Professional Identity” and “Roles and Responsibilities” and better median scores for “Teamwork and Collaboration”.
Conclusion: The attitudes and perceptions of preceptors who had experienced IPE were more favorable toward IPE and thus may foster it more effectively in the students they work with. Therefore, ensuring that all preceptors are aware of and have experience with IPE is important as we seek to promote person-centered care.
Keywords: interprofessional education, roles and responsibilities, interprofessional communication, teamwork, clinical preceptors, collaboration
Background
Person-centered care (PCC) has emerged as a hallmark of healthcare systems around the world.1 The provision of PCC focuses on providing interdisciplinary care that is “compassionate and collaborative” (CCC) for all persons.2 In the literature, interdisciplinary care is defined as “a partnership between a team of health professionals and a client in a participatory, collaborative, and coordinated approach to share decision-making around health issues”.3 Recognizing the impact of interdisciplinary care on the provision of person-centered care health professional program has expanded their curriculums to include interprofessional education opportunities,4,5 Interprofessional Education [IPE] IPE is characterized as circumstances when two or more professions participate in reciprocal learning to improve communication and the standard of service.6
IPE can prepare health professionals to address the demands of the population’s health and welfare, consider the difficulties brought on by fragmented cooperation in healthcare systems, by improving the communication among healthcare professionals and thereby directly affecting patient outcomes.6
According to Maharajan et al [2017], many health-care professional programs require interprofessional education in some format. IPE experiences necessitate the development of creative intellectual learning environments rooted in promoting meaningful social interactions and collaborations. Learning necessitates the identification and appreciation of the distinctive socialization, as well as the development of learning opportunities with constructive interaction.7
IPE, according to research, enables students from several disciplines to develop vital collaboration skills.8 It is strongly advised to create multidisciplinary team training programs that include simulations, virtual world learning experiences, paper cases, diverse team-building exercises, and instruction in verbal and nonverbal communication skills to improve Interprofessional Collaboration [IPC] in healthcare.8 In order to provide complete patient care, Chen et al [2016] underlined the crucial significance of IPE in training learners across healthcare occupations to work successfully as a member of integrated teams.9 For medical students to manage complex clinical circumstances cooperatively, high levels of competence, skills, and a professional attitude are crucial.8 All health profession students require effective skills in integrating information, teamwork, respecting all persons, and overall professional accountability, to promote person-centered care. However, the full potential of Interprofessional Education remains underutilized in many medical schools and health professional schools.
IPE is important because it helps students become active participants in interprofessional collaborations, which is essential for assuring patient safety and high-quality care.6–10 Despite the fact that IPE efforts have proliferated all over the world across all health professions, there is still a vacuum in our knowledge of the elements that contribute to successful learning through IPE. Various strategies for infusing IPE into health professions education have been reported on in the literature and include simulations, case studies, group activities, and rounds to name a few.7,10–12 Literature has also surfaced exploring the attitudes and perceptions of students and faculty regarding IPE practices across many health professions.7,8,10,12 However, limited data exists regarding the attitudes and perceptions of clinical preceptors who play a major role in the educational process of health professional students specific to their perceptions regarding the impact of IPE and its impact on healthcare.
Several conceptual lenses can be used to guide our understanding of the impact of IPE on clinical practice and healthcare. The Intergroup Communication Theory [ICT], which deals with learning with and about-groups, notes that learners must transcend bias, stereotyped beliefs, and hostility from the group to which they do not belong, thus enabling us to see the positive impact of learning with and from others.13 The Social Capital Theory supports the idea that forming sociable relationships among students from various professions during IPE activities leads to confidence in other professional groups during practice.14 Taken together, these conceptual frames offer a guiding lens that highlights the impact IPE can have on practice and care from a communications perspective.
Hayashi et al [2012] conducted a cross-sectional descriptive study to examine former students of an IPE program, to determine if they still had a positive attitude toward collaborative practices in their postgraduate clinical experiences. A section of current undergraduate students and former students was used to establish the difference in attitudes and perceptions between the two groups. The study established that the former students in the IPE program had a more positive attitude than current undergraduate students towards IPE. This was attributed to team efficacy and the fact that the former students spent more time with patients than the undergraduate students. Thereby, suggesting that actual work experience supported a positive attitude towards IPE.15 In general, then, one might infer that prior IPE experience has a positive effect on professional identities and attitudes toward collaboration.16 Recognizing that IPE interactions provide aspiring health professionals invaluable practice and help them develop the attitudes and skills necessary for future interprofessional cooperation, the infusion of IPE into professional health sciences programs has proliferated.17 However, since much of professional healthcare programs develop their student body via clinical engagement with the mentorship of clinical preceptors, understanding the attitudes and perceptions of clinical preceptors towards IPE and their overall readiness to engage in interprofessional care is imperative. Clinical preceptors function as role models, knowledge brokers and coaches, therefore understanding their readiness to key.18–20 Hudak et al, 2018 noted that clinical preceptors offer a conducive learning environment that supports the occurrence of desired interprofessional experiences across a wide variety of settings and disciplines.21 One would argue that professional practice requires clinical preceptors to have a clear understanding of and positive perception towards the practice of IPE.13 However, limited studies have explored the attitudes and perceptions of clinical preceptors towards IPE given their crucial role in the professional formation of healthcare professionals. Therefore, this study sought to understand the attitudes and perceptions of healthcare clinical preceptors towards Interprofessional Education with a major focus on clinical preceptors practicing in Saudi Arabia given the unique healthcare system surrounding Saudi Arabia. The authors specifically choose to look at clinical preceptors’ knowledge, skills, and attitudes regarding readiness to learn with other healthcare professionals via the Readiness for Interprofessional Learning Scale (RIPLS) given that if one is not ready themselves to learn interprofessional and employ the tenets associated with IPE we are left to question how they will be able to promote that in the students they are working with.
Methods
Study Design
The study adopted a cross-sectional research design, which was essential in investigating the attitudes and perceptions of healthcare clinical preceptors towards Interprofessional Education.
Study Participants and Area
The study focused on understanding the attitudes and perceptions of clinical preceptors towards IPE in a healthcare setting in Saudi Arabia. The study was conducted in Saudi Arabia particularly due to the diverse healthcare system in Saudi Arabia, which would limit data generalizability from other US or other global healthcare systems studied.
Sample Size
The minimum sample size for this study was calculated utilizing G-power software. Based on the effect size of 0.58 and a power of 0.80, which is required for the analysis of independent t test [two groups], the recommended number was 96. For the comparison between the two groups: those who were exposed to IPE and those who were not, the minimum sample size for each group was 48. Providentially, the recommended sample size was achieved in this study.
Data Collection
All healthcare sciences program directors in Saudi Arabia received an Email requesting that they forward the provided study letter of solicitation (LOS) to their clinical preceptors for their consideration. The LOS included details about the study, participants inclusion and exclusion criteria, and a link to the study survey housed via Qualtrics. The data collection was conducted from November 2021 to February 2022. The survey required approximately 10 minutes to complete. This study was approved by the Institutional Review Board of King Abdullah International Medical Research Center, study number: SP21J/387/08. All participants gave electronic informed consent, including publication of anonymized responses before completing the survey. The participants were informed about their right to withdraw at any time, anonymity, and confidentiality and that the guidelines outlined in the Declaration of Helsinki were followed.
Study Tool
The study utilized the “Readiness for Interprofessional Learning Scale (RIPLS)”, for data collection. RIPLS was developed by Parsell and Bligh in 1999 and allows study participants to focus on different aspects of Interprofessional Education; hence, it is effective in evaluating the perceptions and attitudes of clinical preceptors towards IPE.22 Parsell and Bligh popularized the word “Readiness for Interprofessional Learning” as a rating method in which students eligible to engage in IPE are evaluated on four dimensions: teamwork awareness and skills, self and others’ roles and responsibilities, patient benefits, practice and personal development, and values. The survey has 19 questions divided into four sections: “teamwork and partnership”, “negative professional identity”, “positive professional identity”, and “roles and responsibilities”. On a 5-point Likert scale, participants showed their degree of agreement: “strongly disagree, disagree, neutral, Agree, or strongly agree”.22
The RIPLS consists of 19 items measured through 5-point Likert scales. Parsell and Bligh22 constructed the RIPLS to test readiness for teamwork and collaboration, professional identity and roles and responsibilities. In the literature, the reliability of this instrument has been questioned, thus leading to a four-factor model being proposed by McFadyen et al.23 The four-factor model appears to be more reliable than the original three-factor construct.23 The four-factor construct represented the following dimensions: teamwork and collaboration (items 1–9), positive professional identity (items 13–16), negative professional identity (items 10–12), and roles and responsibility (17–19). Answers to the 19 items were given on 5-point Likert scales (1 = strongly disagree, 2 = Disagree, 3 = neutral, 4 = agree, and 5 = strongly agree). For items 1–9 and 13–16 representing the domains of teamwork and collaboration and positive professional identity, respectively, with higher scores indicating readiness for IPE. The answers for items 10–12 and 17–19 were given on 5-point Likert scales too and reverse scored as was done by McFadyen et al23 (1 = Strongly agree, 2 = agree, 3 = neutral, 4 = disagree, 5 = Strongly disagree). Descriptive statistics for individual items will be presented using the original scaling. Higher scores for the reverse coded items reflect greater readiness towards IPE.
The RIPLS tool was embedded in a questionnaire that gathered additional information on the demographics of the participants and explored three open-ended questions developed by the principal investigator. The open-ended questions were utilized to evaluate clinical preceptors’ thoughts regarding the impact of IPE on the students they engaged with in clinic. The open-ended questions allowed the clinical preceptors to share their perspectives regarding the differences on the four domains between those students who have participated in IPE during their educational programs and those that did not.
The first open-ended question asked, “During your experience as clinical preceptor, which groups of students (those exposed to IPE during their education program or those who were not exposed) were more effective during the clinical rotation and why?” The second question asked, “Could you please rank the following domains: Values/Ethics, Roles/Responsibilities, Interprofessional Communication, and Teams and Teamwork, from the most noticed (1) to the least noticed (4) among your students who were exposed to IPE during their educational program”. The third question asked, “Could you please rank the following domains: Values/Ethics, Roles/Responsibilities, Interprofessional Communication, and Teams and Teamwork, from the most noticed (1) to the least noticed (4) among your students who were not exposed to IPE during their educational program”. Three health-care educators’ experts reviewed the demographic profile and open-ended questions for content clarity using the Delphi Review Process. Eighty-five percent consensus was achieved after two rounds of review on each open-ended question and the demographics question.
Data Analysis
Data collected using the RIPLS were analyzed using the Statistical Package for Social Sciences (SPSS) version 28. First, the principal investigator (PI) analyzed the data to examine general participants’ characteristics. Second, the PI explored the attitude and perceptions of healthcare clinical preceptors towards IPE. Third, the PI compared clinical preceptors who were exposed to IPE in their educational programs to those who were not using an independent t-test to explore the influence of IPE. Statistically, Shapiro Wilk test was used to examine data normality. Then, Mann–Whitney U nonparametric test was used to examine difference between two groups: exposed to IPE and not exposed to IPE. The statistical significance of the results was considered at p < 0.05.
Using open-ended questions, respondents were asked to qualitatively express their opinion. Data were analyzed through open coding, in-vivo coding as described by Miles.24 All 3 investigators independently coded the first 2 surveys open-ended question responses, then met and compared codes and analytic memos to ensure consistency. Thirteen additional surveys open-ended question responses (every 5th survey was reviewed) were conducted and individually coded, and the investigators met again to discuss codes and memos, resolve discrepancies at which time the investigators unanimously agreed that saturation was met for a total of 15 interviews.24 The investigators then individually collapsed codes into categories and then met to establish agreement on thematic analysis statements derived from categories. Before the study and throughout data collection and analysis, the investigators openly discussed their positionality related to this research.
Results
Demographic Data
A total of 208 participants responded to the survey, 26 were excluded as they did not complete all survey questions. A total of 182 clinical preceptors completed the entire survey. Socio-demographic characteristics of the 182 participants are shown in Table 1. Almost half of the participants were males and about two-third were below 40 years old. Eight percent of the participants had a Diploma, 33% had a bachelor’s degree, and 37% held a master’s degree, while 21% were doctorly prepared. More than half of the participants had been practicing for more than five years [60%]. The majors of the participants included Medicine [21%], Nursing [22%], Respiratory therapy [12%], and Dentistry [8%], Radiology [8%], in addition to other majors as shown in [Table 1].
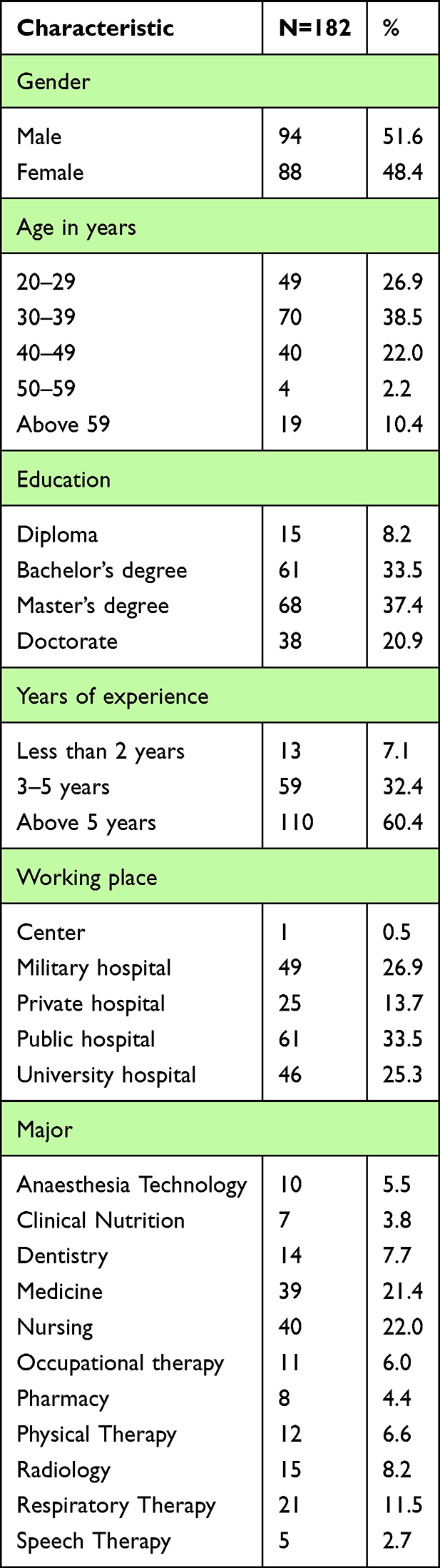 |
Table 1 Demographic Characteristics of Participants [N = 182] |
Participants’ Exposure to IPE
Overall, 48% [87/182] of the clinical preceptors had been exposed to IPE experiences during their academic programs [Figure 1]. Among these, 46% received a separate IPE academic course, while 34% experienced it embedded in an existing course, 9% had a one-time event, and only 10% had an IPE simulation experience [Figure 2]. Moreover, about two-third of these experiences occurred throughout their entire academic program [68%], while one-third were placed in the first and second clinical years [13%, 19%, respectively].
 |
Figure 1 IPE experiences in academic program. |
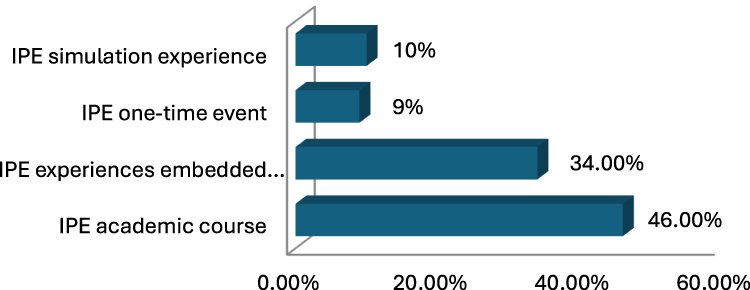 |
Figure 2 Types of IPE experiences. |
Participants Attitude and Perception Towards IPE
The reliability of the scale was determined by calculating Cronbach’s alpha for the 19-item RIPLS [0.828]. Responses of the participants are shown in [Table 2]. A high median score on the items from Q1-to Q9 [median = 5] indicates a strongly positive attitude of the participants towards the “Teamwork and Collaboration” concept, with nearly 0% disagreement. Participants' responses regarding “Negative Professional Identity” were ranging from neutral to agree, while responses toward “Positive Professional Identity” were predominately positive, and almost 80% of the participants agreed to all the 4 items. The median value was 4 in Q17 and Q19, which indicate an agreement toward both items, while participants reported a neutral response toward Q18 with median value equal to 3.
 |
Table 2 Participants Attitude and Perception Toward IPE [N = 182] |
Attitude Differences by the Exposure to IPE
Attitude differences [measured by the median of each scale] versus exposure to IPE is shown in [Figure 3]. In order to detect the statistical significance of the difference in attitude of the participants who had prior exposure to IPE compared to those who never received IPE, we ran Mann–Whitney U-test as shown in [Table 3]. Analysis revealed a statistically significant difference overall [p-value=0.00], additionally there was a statistically significant difference in “Teamwork and Collaboration” “Negative Professional Identity” and “Roles and Responsibilities” with p-value = 0.00. On the other hand, difference between exposed and non-exposed group regarding “Positive Professional Identity” was not significant [p = 0.082].
 |
Table 3 Attitude Differences by the Exposure to IPE |
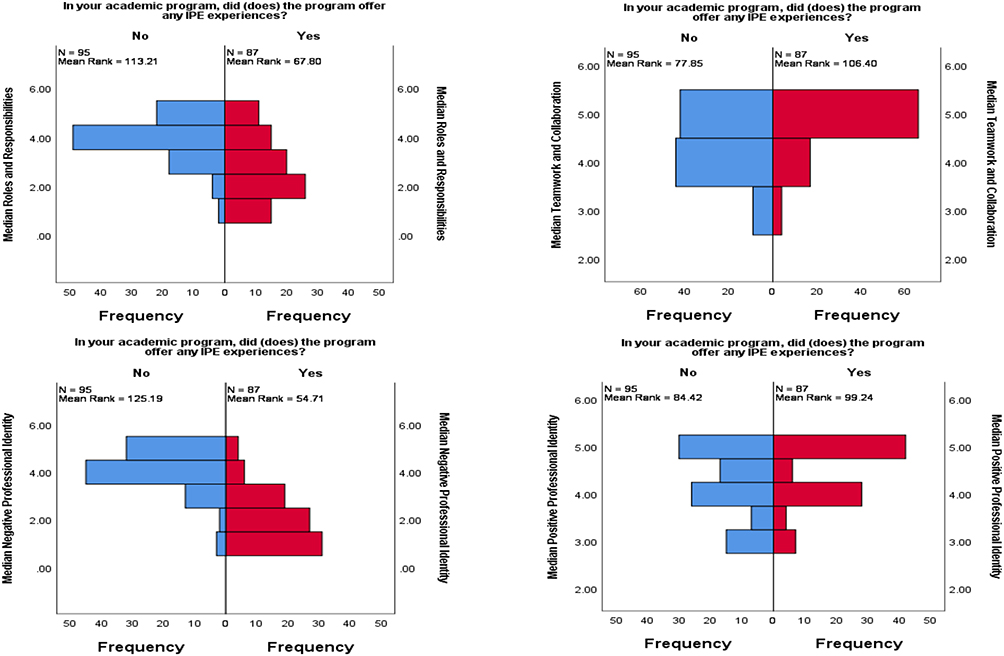 |
Figure 3 Attitude differences toward each scale in exposed vs non exposed group. |
Qualitative Data Analysis
The three open-ended questions were designed to explore the clinical participants’ perception about the importance of IPE. A total of 182 participants answered the first open-ended question, which asked, “During your experience as clinical preceptor, which groups of students, those who were exposed to IPE during their program or those who were not, was more effective during the clinical rotation and why?” Most responses indicated that students who were exposed to IPE during their program of study were more effective than those not exposed. In addition, their responses supported those students exposed to IPE had a sense of responsibility, good understanding of other roles, and communication skills in comparison to those who did not have IPE experience [Table 4].
 |
Table 4 Participants’ Responses to the First Open-Ended Question |
A total of 182 participants answered the second and third open-ended question, which asked, “Could you please list the following domains: values/Ethics, Roles/Responsibilities, Interprofessional Communication, and Teams and Teamwork, from the most noticed to the least one among your students who were exposed to IPE during their study, and Could you please list the following domains: values/Ethics, Roles/Responsibilities, Interprofessional Communication, and Teams and Teamwork, from the most noticed to the least one among your students who were not exposed to IPE during their study”, respectively. The order of importance for students exposed to IPE during their studies according to the clinical preceptors’ perceptions is as follows: Roles/Responsibilities, Interprofessional Communication, Teams and Teamwork, and Values/Ethics [Table 5]. In contrast, the clinical preceptors have ranked the students who did not have any exposure to Interprofessional Education (IPE) during their studies according to the following order of importance: Teams and Teamwork, Values/Ethics, Roles/Responsibilities, and Interprofessional Communication [Table 6].
 |
Table 5 The Order of Importance for IPE Exposure |
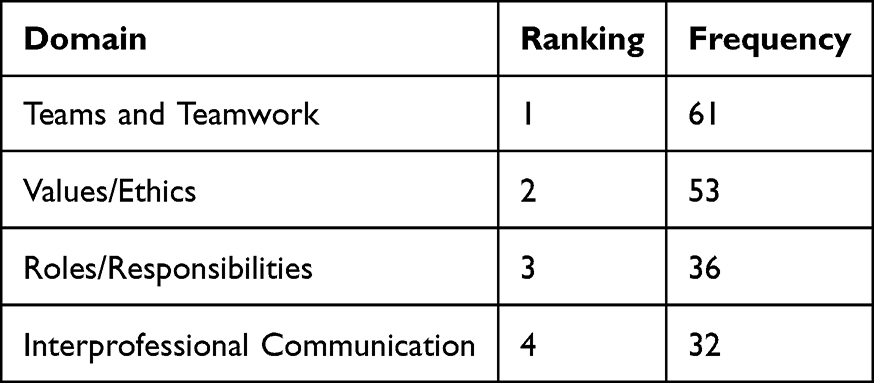 |
Table 6 The Order of Importance for Students Who Did Not Have IPE Exposure |
Discussion
The aim of this study was to explore attitudes and perceptions of healthcare clinical preceptors towards Interprofessional Education and how they will be able to promote that in the students they are working with. In this study, all the clinical preceptors who understand purpose of IPE and those who did not know had a strong positive attitude towards the “Teamwork and Collaboration”. They agreed that students learning with other students would help them become more effective members of a healthcare team and that shared learning with other healthcare students would increase their ability to understand clinical problems. In fact, their perceptions towards roles and responsibilities category received the lowest rankings. Some studies report that in current professional settings, certain jobs are considered as being more important than others. In the context of comprehensive patient treatment, doctors are frequently seen as team leaders. In order to provide effective and efficient patient care, healthcare teams must be guided by leaders with authority and competence.1–8,25
This study reports that clinical preceptors in Saudi Arabia have an overall positive attitude towards IPE. This study finding with Saudi Arabia's clinical preceptors is in accordance with multiple studies conducted in other professions to determine the attitude towards IPE. A study conducted revealed positive attitude towards IPE among pharmacy academics, with a majority recognizing the importance of IPE.17 Through the inclusion of IPE in courses, both staff members and students reported having a better awareness of team responsibilities and communication. These findings also support the study of Rodger et al (2010), which found that healthcare workers had favorable opinions of IPE.26 In the few research endeavors conducted in the Middle Eastern very slight variations in IPE-related healthcare professional services were found and more importantly they yielded similar results in that IPE was regarded with great importance.27–30
An important finding from this research is that the clinical preceptors who had been exposed to IPE during their academic programs experienced different ways of delivering IPE. Thus, there is no apparent consistency present in how IPE is being delivered currently. Exploring the different approaches to infusing IPE and determining which is more effective long term is imperative if we want to make impactful changes. A study evaluated the effects of IPE stimulation training on medical and nursing students’ Medical Task Performance and Teamwork Behavior Performance [TBP]. The MTP and TBP were improved by both IPE and Single-Professional Education [SPE] simulations. Between the two groups, there were, however, no appreciable differences.29 The creation of an IPE program aimed at medical and nursing students, encouraging learning across personal, professional, and interprofessional elements, is one of the study’s strong points.29 Indeed, the current evidence in the literature clearly demonstrates that exposure to IPE during academic programs leads to improved outcomes in terms of patient-centered care.29,30
The perceptions of clinical preceptors towards IPE varied between the two groups (exposed to IPE vs not exposed) in terms of “Teamwork and Collaboration”, “Negative Professional Identity”, and “Roles and Responsibilities”. However, there was no difference between the exposed and non-exposed groups regarding “Positive Professional Identity”. One potential reason for the clinical preceptor’s fewer positive attitudes could be attributed to the impact of their curriculum and/or clinical training sessions on their scores.16,19,21 Ultimately, to fully understand these observed differences in subscales additional research is required.
The perceptions of clinical preceptors have a significant impact on the performance of students. These perceptions are affected by the preceptors’ own views and may also be influenced by the students’ exposure to IPE. Our open-ended questions provide additional valuable insights. As a result of their exposure to IPE, preceptors perceived students understanding of “Roles and Responsibilities” and “Interprofessional Communication” were higher than those of “Teams and Teamwork”, “Values/Ethics”, and other domains. “Teams and Teamwork”, on the other hand, were identified as the most noticeable domain by students who were not exposed to IPE, followed by values/ethics, roles/responsibilities, and interprofessional communication. Thus, clinical preceptors perceived IPE influenced students’ perceptions of roles, communication, and cooperation in healthcare settings in a favorable way.22–24 As students learn how to cooperate effectively in a collaborative setting, this exposure aids in the development of their effective communication and cooperation skills. IPE exposure fosters a shared concept of patient care and breaks down professional silos, improving collaboration among healthcare providers and improving patient outcomes.31–34
Finally, IPE is of importance in educating students for the modern, collaborative, and dynamic healthcare environment. Several suggestions may be put into practice to build IPE in health sciences courses efficiently. First, interdisciplinary activities and simulations should be incorporated into curriculum design to give students chances to study and work with peers from diverse healthcare professions. Second, faculty development initiatives should be started to give facilitators the abilities and information required to lead IPE experiences. Thirdly, the effect of IPE will be increased by developing conditions for interprofessional learning that promote honest dialogue, respect for one another, and appreciation for each profession’s distinctive contributions. Encouraging ongoing assessment and feedback systems will guarantee the efficacy of IPE programs in developing future healthcare professionals who excel at collaboration and patient-centeredness. Finally, providing clinical preceptors who work with health science professional students, prior to graduation, must continue to build upon the tenants of IPE promoted in the student’s coursework and foster IPE learning experiences during their clinical. However, to do so they must be informed themselves.
Study Strengths and Limitation
As with any study, there are limitations that must be addressed. Firstly, assessing IPE is not an easy procedure because different types of pedagogy from programs to others, therefore, exploring different or many tools would be more effective. Secondly, although the participants were explicitly reassured that the research was independent of regular courses, they might have given socially desirable answers. Finally, the principal investigator collected data at a single point in time, therefore, the potential of inherent biases was not controlled which may dramatically influence the participants’ responses.
Conclusion
The study surveyed 182 clinical preceptors in Saudi Arabia regarding their knowledge, skills, and attitudes regarding readiness to learn with other healthcare professionals. One might question the relevance of asking clinical preceptors about their readiness, but we would argue that as adult learners in healthcare, we must always be ready to employ interprofessional practice for the care of our patients and to promote interprofessional practice skills in the students we mentor in the clinic. Therefore, understanding the readiness, attitudes, and perceptions towards IPE using the Readiness for Interprofessional Learning Scale (RIPLS) and several open-ended questions afford valuable insights that must be addressed moving forward. First, given that not all preceptors had been introduced to IPE in your educational programs and we expect them to promote IPP in our students, we must address this gap possibly with continuing education training. Second, most preceptors concurred that learning alongside other professions will increase their efficiency in healthcare teams and deepen their comprehension of clinical issues and the importance of “Teamwork and Collaboration”. However, with the “Roles and Responsibilities” category, obtaining lower ranks, we must begin to explore alternate means by which to expose students to this information.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ekman I, Swedberg K, Taft C, et al. Person-Centered Care — ready for Prime Time. Eur J Cardiovasc Nurs. 2011;10(4):248–251. doi:10.1016/j.ejcnurse.2011.06.008
2. Lown BAMD, McIntosh SMHA, Gaines MEJD, et al. Integrating Compassionate, Collaborative Care (the “Triple C”) Into Health Professional Education to Advance the Triple aim of Health Care. Acad Med. 2016;91(3):310–316. doi:10.1097/ACM.0000000000001077
3. Orchard CA, Curran V, Kabene S. Creating a Culture for Interdisciplinary Collaborative Professional Practice. Med Educ Online. 2005;10(1):1. doi:10.3402/meo.v10i.4387
4. Macdonald MB, Bally JM, Ferguson LM, Lee murray B, Fowler-Kerry SE, Anonson JM. Knowledge of the professional role of others: a key interprofessional competency. Nurse Educ Practice. 2010;10(4):238–242. doi:10.1016/j.nepr.2009.11.012
5. Rotegård AK, Moore SM, Fagermoen MS, Ruland CM. Health assets: a concept analysis. Int j Nursing Studies. 2010;47(4):513–525. doi:10.1016/j.ijnurstu.2009.09.005
6. El-Awaisi A, Sheikh Ali S, Abu Nada A, Rainkie D, Awaisu A. Insights from healthcare academics on facilitating interprofessional education activities. J Interprof Care. 2021;35(5):760–770.
7. Maharajan MK, Rajiah K, Khoo SP, et al. Attitudes and Readiness of Students of Healthcare Professions towards Interprofessional Learning. PloS one. 2017;2–13.
8. Lash DB, Barnett MJ, Parekh N, Shieh A, Louie MC, l TTT. Perceived Benefits and Challenges of Interprofessional Education Based on a Multidisciplinary Faculty Member Survey. American Journal of Pharmaceutical Education. 2014;78(10). doi:10.5688/ajpe7810180
9. Chen AK, Rivera J, Rotter N, Green E, Kools S. Nurse Education in Practice Interprofessional education in the clinical setting: a qualitative look at the preceptor’ s perspective in training advanced practice nursing students. Nurse Educ Pract. 2016;21:29–36. doi:10.1016/j.nepr.2016.09.006
10. Alahmari MD. Interprofessional Education. Saudi Health Students’ Attitudes Toward Shared Learning. 2019.
11. King J, Beanlands S, Fiset V, et al. using interprofessional simulation to improve collaborative competences for nursing, physiotherapy, and respiratory therapy students. J Interprof Care. 2016;30(5):599–605. doi:10.1080/13561820.2016.1189887
12. Klima D, Hinderer KA, Freda K, Winter D, Joyner R. Interprofessional collaboration between two rural institutions: a simulated teaching laboratory paradigm. Respir Care Educ Annual. 2014;23:45–48.
13. Gallois C, Watson BM, Giles H. Intergroup Communication: identities and Effective Interactions Intergroup Communication. Identities Effective Interactions. 2018.
14. Hean S, Halloran CO, Craddock D, Hammick M, Pitt R. Testing theory in interprofessional education: social capital as a case study Testing theory in interprofessional education: social capital as a case study. J Interprofessional Care. 2012.
15. Hayashi T, Shinozaki H, Makino T, et al. Changes in attitudes toward interprofessional health care teams and education in the first-and third-year undergraduate students. J Interprof Care. 2012;26(2):100–107. doi:10.3109/13561820.2011.644355
16. Al-Eisa E, Alderaa A, AlSayyad A, et al. The perceptions and readiness toward interprofessional education among female undergraduate health-care students at King Saud University. J Phys Ther Sci. 2016;28(4):1142–1146. doi:10.1589/jpts.28.1142
17. Alshamrani KM, Ghulam EM, Alattas M, et al. Transition to remote/ hybrid learning during the COVID-19 pandemic among Saudi students of the College of Applied Medical Sciences: a cross-sectional study. Front Med. 2023;10:1257589. doi:10.3389/fmed.2023.1257589
18. Zechariah S, Ansa BE, Johnson SW, Gates AM, Leo G. Interprofessional Education and Collaboration in Healthcare: an Exploratory Study of the Perspectives of Medical Students in the United States. InHealthcare. 2014:1–11.
19. Maldonado AQ, Bray BS, Woodard LJ, et al. Impact of Participation on a Solid Organ Transplant Team on Student Pharmacists. Perceptions Interprofessional Roles. 2013;77(4):1–6.
20. Hall S, Goeckel C. An Exploratory Study on Perceptions of (IPE) Towards Interprofessional Practice in Athletic Training. Int J Med. 2018.
21. Hudak NM, Melcher B, Everett CM. Preceptors’ Perceptions of Interprofessional Practice, Student Interactions, and Strategies for Interprofessional Education in Clinical Settings. The Journal of Physician Assistant Education: the Official Journal of the Physician Assistant Education Association. 2018;29(1):39–42. doi:10.1097/JPA.0000000000000184
22. Parsell G, Bligh J. The development of a questionnaire to assess the readiness of health care students for interprofessional learning (RIPLS). Medical Education. 1999;33(2):95–100. doi:10.1046/j.1365-2923.1999.00298.x
23. McFadyen AK, Webster VS, Maclaren WM. The test-retest reliability of a revised version of the Readiness for Interprofessional Learning Scale (RIPLS). J Interprofessional Care. 2006;20(6):633–639. doi:10.1080/13561820600991181
24. Mile MB, Huberman AM, Saldana J. Qualitative Data Analysis: A Methods of Sourcebook. London: Sage; 2014.
25. Vafadar Z, Vanaki Z, Ebadi A. The Readiness of Postgraduate Health Sciences Students for Interprofessional Education in Iran. Glob J Health Sci. 2015;7(4):190. doi:10.5539/gjhs.v7n4p190
26. Rodger S, Hoffman J. Where in the world is interprofessional education? A global environmental scan. J Interprof Care. 2010;24(5):479–491. doi:10.3109/13561821003721329
27. Wilbur K, Hasnani-Samnani Z, Kelly I. Interprofessional Education Activity Among Undergraduate Nursing and Pharmacy Students in the Middle East. Nurse Educ. 2015;40(4):163–164. doi:10.1097/NNE.0000000000000135
28. Al-Eisa E, Alderaa A, Alsayyad A, et al. The perceptions and readiness toward interprofessional education among female undergraduate health-care students at King Saud University. J Phys Ther Sci. 2016;28(4):1142–1146. doi:10.1589/jpts.28.1142
29. Chen HW, O’donnell JM, Chiu YJ, et al. Comparison of learning outcomes of interprofessional education simulation with traditional single-profession education simulation: a mixed-methods study. BMC Med Educ. 2021.
30. Bally JMG, Spurr S, Hyslop S, Hodgson-Viden H, McNair ED. Using an interprofessional competency framework to enhance collaborative pediatric nursing education and practice. BMC Nurs. 2022;21(1). doi:10.1186/s12912-022-00932-z
31. Neill M, Hayward KS, Peterson T. Students’ perceptions of the interprofessional team in practice through the application of servant leadership principles. J Interprof Care. 2007;21(4):425–432. doi:10.1080/13561820701443512
32. Yune SJ, Park KH, Min YH, Ji E. Perception of interprofessional education and educational needs of students in South Korea: a comparative study. PLoS One. 2020;15(12):e0243378. doi:10.1371/journal.pone.0243378
33. Teuwen C, van der Burgt S, Kusurkar R, Schreurs H, Daelmans H, Peerdeman S. How does interprofessional education influence students’ perceptions of collaboration in the clinical setting? A qualitative study. BMC Med Educ. 2022;22(1):1–10. doi:10.1186/s12909-022-03372-0
34. Al Nufaiei ZF, Zipp GP. Interprofessional Education Towards Interprofessional Practice: a Mixed-Methods Exploration of Respiratory Care Students and Therapists’ Perceptions. Eur J Health Sc. 2022;7(1):13–22. doi:10.47672/ejhs.926
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.