")
Back to Journals » Research and Reports in Urology » Volume 15
Giant Pyonephrosis in an Ectopic Kidney: A Case Report
Authors Ahmed MM , Adem MB, Mideksa AG , Huluka TY
Received 13 June 2023
Accepted for publication 27 August 2023
Published 1 September 2023 Volume 2023:15 Pages 409—414
DOI https://doi.org/10.2147/RRU.S412100
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Panagiotis J Vlachostergios
Mensur Mohammed Ahmed,* Mubarek Bargicho Adem,* Adugna Getachew Mideksa,* Tolesa Yadeta Huluka
Department of Surgery Urology Division, Saint Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia
*These authors contributed equally to this work
Correspondence: Mensur Mohammed Ahmed, Tel +251978191741, Email [email protected]
Abstract: Pyonephrosis is characterized by infective hydronephrosis accompanied by suppurative destruction of the renal parenchyma, resulting in partial or complete impairment of renal function. Patients present with wide range of symptoms, they can be asymptomatic in 15% but most of them present with septic features like fever, chills, and flank pain. Urinary tract infections, functional and anatomic obstruction, and anatomic anomalies such as pelvic and horseshoe kidneys are common etiologic factors. We report a 30 years old female patient with giant pyonephrosis in an ectopic kidney. She presented with acute toxic symptoms after she has been experiencing progressive abdominal swelling and pain for a couple of years. Simple nephrectomy was done four weeks after she has been initially treated with percutaneous drainage of the pus and intravenous antibiotics.
Keywords: giant pyonephrosis, ectopic kidney, percutaneous nephrostomy, simple nephrectomy
Introduction
Giant hydronephrosis is considered when the renal pyelocalyceal system contains more than 1000cc of fluid or radiologically as the kidney is occupying hemiabdomen with midline crossing and/or that equals the height of five vertebral bodies.1
Giant pyonephrosis is an uncommon urological condition. It is rare in the adult population, and diagnosis may be difficult to achieve. It is identified based on the patient’s clinical signs and symptoms, blood and urine tests, and imagings like ultrasound (USG), computed tomography (CT) urography, and magnetic resonance imaging (MRI). Giant pyonephrosis in an ectopic kidney represents a rare and intriguing clinical entity that demands attention due to its distinctive presentation and challenging management.
Pyonephrosis coupled with the presence of an ectopic kidney makes the clinical scenario more complex. This paper delves into a compelling case study of a patient with a massive infected cystic mass of an ectopic kidney, exploring the diagnostic intricacies, therapeutic interventions, and postoperative outcomes. Through this investigation, we aim to shed light on the diagnostic and therapeutic considerations when confronting such an exceptional presentation of pyonephrosis in the context of an ectopic kidney.
Case Report
A 30 years old female patient complains of right lower flank and abdominal pain for two years associated with gradually progressive abdominal swelling of the same duration. She presented to our hospital with worsening of abdominal and flank pain at the same site associated with vomiting, fever, chills and rigor, and bilateral leg swelling for one week. She has no comorbidities such as Diabetes Mellitus or Hypertension. Her pulse rate was 120, BP 100/60, and temperature 38.8°C, and on abdominal examination there was firm to soft abdominopelvic mass to the level of umbilicus and bilateral grade two pitting edema. Examination of the other systems was normal. On the comprehensive metabolic panel test, the white blood count was 7.2k with a neutrophil percentage of 78%, hemoglobin was 11.2 g/dl, creatinine was 1.03 and serum electrolytes were in normal ranges. The urine analysis revealed leukocytes and other findings that were consistent with infection.
Abdominopelvic ultrasound showed a huge septated cystic mass filled with echo debris content, no renal parenchyma was detected, and the kidney was absent in the right renal fossa. Abdominopelvic Ct-scan revealed normal left kidney and absent kidney in the right renal fossa but a huge (22 cm x 18 cm) cystic mass which is lobulated with thin septations and immeasurable parenchymal thickness, no solid component, homogeneously filled with fluid content with density of 30 Hounsfield Unit in the right iliac fossa extending to the left kidney and pelvis pushing bowel and uterus laterally (Figures 1 and 2).
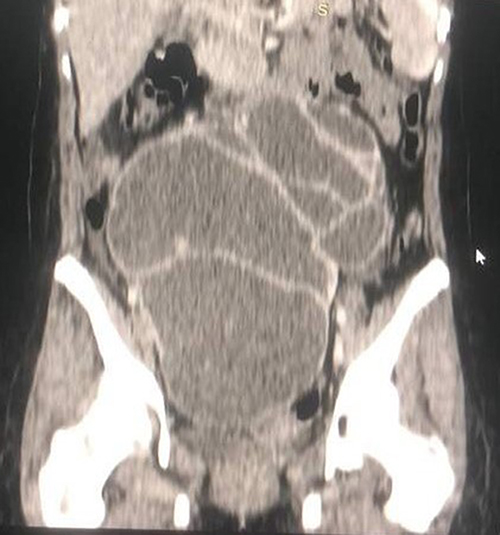 |
Figure 1 Coronal CT scan image of the giant ectopic hydronephrotic right kidney. |
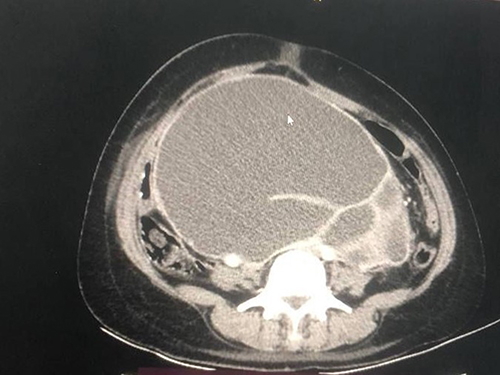 |
Figure 2 Axial CT scan image of the giant ectopic hydronephrotic right kidney. |
Based on the aforementioned clinical findings, the patient was started on empiric intravenous antibiotics, and the pyonephrosis was drained with a percutaneous nephrostomy tube. The output was 3000 mL frank pus over the first 15 min; subsequently, 2600 mL of pus drained over the next couple of days, and the output decreased significantly (Figures 3–5). The patient was admitted and administered intravenous antibiotics for ten days. After four weeks, simple nephrectomy was performed on an elective basis (Figure 6). The nephrectomy sample was sent for histopathologic examination and showed a thinned-out renal parenchyma with thyroidisation change and dense interstitial chronic inflammation, but no features of malignancy. The patient experienced an uneventful postoperative period. The patient was doing well on the subsequent follow-up.
 |
Figure 3 Distended abdomen and PCN tube in situ draining frank pus. |
 |
Figure 4 Flat abdomen an hour after PCN insertion. |
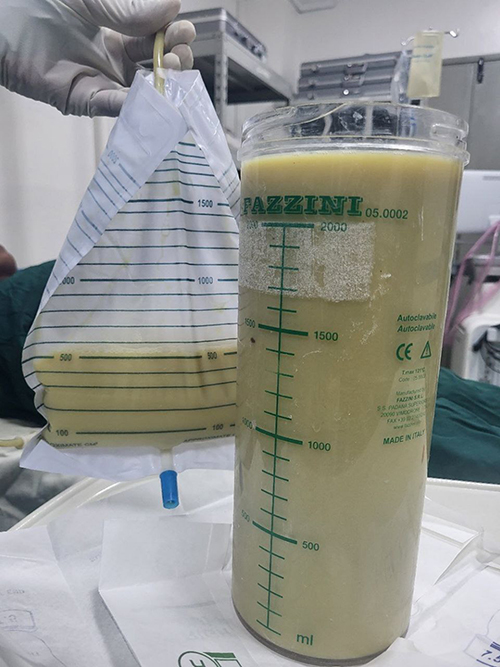 |
Figure 5 The 3000 mL frank pus drained within 15 minutes of PCN insertion. |
 |
Figure 6 Morphological appearance of nephrectomy specimen. |
Discussion
The presence of pus distinguishes pyonephrosis, a suppurative infection of the pelvicalyceal system, from infected hydronephrosis. It usually results in persistent pyelonephritis, parenchymal damage, and impaired renal function.2 Urinary tract infections, functional and anatomic obstruction, and anatomic anomalies such as pelvic and horseshoe kidneys are etiologic factors.3 Ureteric obstruction is the primary anatomical factor in the etiopathogenesis of pyonephrosis. At least 70% of patients with pyonephrosis have stones as the primary cause.4 E. coli, Enterococcus, Klebsiella, Proteus, and Pseudomonas are the most common etiologic microorganisms found in pyonephrosis.2
Giant hydronephrosis is defined as the presence of more than 1000 cc of fluid in the pelvicalyceal system. It has also been described radiologically as an enlarged kidney occupying half of the abdomen with midline crossing and/or measuring the height of five vertebral bodies.5 We found two cases of giant hydronephrosis reported a couple of years ago from our same institution: the first case is 46 years old male patient, and simple nephrectomy was performed with 22 liters of coffee ground colored fluid content, and the second case is 32 years old female patient with a similar case and 9 liters of urine containing hydronephrotic kidney found intraoperatively. Both cases of giant hydronephrosis were due to pelviureteral junction obstruction, and nephrectomy was performed on elective bases (4) and (5). We report a 30 years old female patient diagnosed with giant pyonephrosis in an ectopic kidney that poses both diagnostic and treatment challenges.
Pyonephrosis was identified based on the patients’ signs and symptoms, blood and urine examination, and imaging using ultrasound and Ct-scan. The patients are usually toxic with high fever, chills, loin pain, and tenderness. However, occasionally, a patient may only complain of fever and vague gastrointestinal symptoms. Patients commonly report previous urolithiasis, urinary tract infections or surgery. Urine analysis may not reveal signs of infection in case of obstructed upper urinary tract. MRI, CT, and USG are common imaging modalities used for the diagnostic evaluation of pyonephrosis. To diagnose pyonephrosis, determine the causes, evaluate renal function, and evaluate perinephric inflammation and complications, such as perinephric abscess and emphysematous pyelonephritis, a Contrast enhanced ct-scan is very sensitive.2,6 CT can also help to differentiate pyonephrosis from infected hydronephrosis. In fact, suppurative renal parenchyma destructive lesions and peri-nephritis are absent in infected hydronephrosis.
The pelvicalyceal system is usually significantly dilated during ultrasound scanning in pyonephrosis, however collecting system wall thickening and/or contraction may be the only sonographic finding. Low-level echoes from the pus and debris can be in the infected pelvicalyceal system, but you might need to increase the gain to view them. Sonographic findings of focal areas of reduced echogenicity within the hydronephrotic parenchyma are suggestive of pyonephrosis.7
Pyonephrosis can be treated with percutaneous drainage, retrograde ureteral stenting, or nephrectomy. In cases of pyonephrosis, conservative treatment with antibiotics alone is ineffective; surgical intervention is usually needed. Percutaneous nephrostomy (PCN) is a minimally invasive and efficient way to drain the pelvicalyceal system (PCS), hence it is commonly used as the initial treatment for obstructed urinary systems and to monitor ipsilateral urine production, especially when they are septic.2 Pyonephrosis is treated with percutaneous nephrostomy for both diagnostic and therapeutic advantages. Percutaneous nephrostomy is favored as the initial step in the surgical management of pyonephrosis because it drains pus from the renal cavities, which decreases renal distension and severity of subsequent peri nephritis. The surgical procedure of choice is nephrectomy if the contralateral kidney is healthy; if a nephrostomy is inserted on an emergency basis, nephrectomy can be performed once the patient’s overall health has improved, often after two weeks.2,3
Some cases of giant pyonephrosis have been reported previously from different countries; however, this is the first case reported in our country, if not from Africa, and a case of giant pyonephrosis measuring 13 cm × 24 cm × 34 cm (7 litres of pus) caused by an obstructed stone. They performed a simple nephrectomy through a large midline incision, and a similar case of giant pyonephrosis from the same country was reported four years later and treated with simple nephrectomy.3,8 An open nephrectomy was used to treat a case of giant pyonephrosis measuring 23 cm × 30 cm × 27.9 cm which was caused by urolithiasis and diabetes, as reported by Hasigov et al.9 Rupesh Gupta et al had reported a case of giant pyonephrosis of size 30 cm × 26 cm × 20 cm (12 liters of pus) due to Ureteropelvic Junction Obstruction and they have done nephrectomy through subcostal incision.9 Niang et al recently reported a case of giant pyonephrosis containing 10 liters of pus and spontaneously ruptured in the adjacent muscles and the treatment was an aspiration followed by a nephrectomy by laparotomy.10 In our case, we initially managed her with percutaneous drainage of pus and stabilized with hydration and intravenous antibiotics, followed by simple nephrectomy on an elective basis. The patient had an uneventful postoperative course and follow up.
Cystic intra-abdominal masses that resemble giant hydronephrosis have a list of differential diagnoses, including ovarian cysts, hepatobiliary cysts, renal cell carcinoma (RCC), retroperitoneal tumors, pseudomyxoma, splenomegaly, and ascites.11 Especially in female patients and pelvic ectopic kidney presenting with an abdominopelvic cystic mass, the diagnostic challenge remains difficult, and it is wise to consider pyonephrosis as a diagnosis and act promptly.
Conclusion
Accurate diagnosis and prompt management are required in patients with pyonephrosis. Female patients presenting with abdominopelvic cystic masses pose difficulty in diagnosis. Contrast-enhanced CT has high sensitivity in the detection of pyonephrosis and helps to identify etiologic factors, assess anatomic and physiologic renal function, evaluate complications, and rule out other differential diagnoses. Management of giant pyonephrosis with initial percutaneous drainage of pus followed by simple nephrectomy, if the contralateral kidney is healthy after the patient is stabilized, has the best outcome. The exceptional anatomical variation introduced by the ectopic kidney adds a layer of complexity to the diagnosis, treatment, and postoperative care. The successful resolution of this case underscores the importance of meticulous preoperative evaluation, prompt intervention, and comprehensive postoperative monitoring.
Data Sharing Statement
All data about the patient are available from the corresponding author upon request.
Consent
A written informed consent has been obtained from the patient to have the case details and any accompanying images published. No institutional review board approval was required to publish the case details.
Acknowledgments
We appreciate the patient’s permission to publish this case.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No specific grant from funding organizations in the public, private, or nonprofit sectors was given to this manuscript.
Disclosure
No authors have disclosed any conflicts of interest.
References
1. Dino MS, Hassen SM, Tufa TH, Morhason-Bello I. Unilateral giant hydronephrosis secondary to ureteropelvic junction obstruction in a middle-aged woman. Case Rep Urol. 2021;2021:1–4. doi:10.1155/2021/9900560
2. Lezin MS, Hofmann R, Stoller ML. Pyonephrosis: diagnosis and Treatment. Br J Urol. 1992;70(4):360–363. doi:10.1111/j.1464-410X.1992.tb15788.x
3. Selvi I, Ihsan Arik A, Basay MS. An unusual case: adult giant pyonephrosis. Surg Rehabil. 2018;2(4). doi:10.15761/SRJ.1000147
4. Rabii R, Joual A, Rais H, et al. Pyonéphrose : diagnostic et traitement : à propos de 14 cas [Pyonephrosis: diagnosis and treatment: report of 14 cases]. Ann Urol. 2000;34(3):161–164. French.
5. Gupta R, Gupta S, Choudhary A, Basu S. Giant pyonephrosis due to ureteropelvic junction obstruction: a case report. J Clin Diagn Res. 2017;11(8):D17–D18.
6. Fultz PJ, Hampton WR, Totterman SMS. Computed tomography of pyonephrosis. Abdom Imaging. 1993;18(1):82–87. doi:10.1007/BF00201709
7. Allan PL. Infectious diseases of the kidney. In: Clinical Ultrasound. Elsevier; 2011:460–466.
8. Erol A, Çoban S, Tekin A. A giant case of pyonephrosis resulting from nephrolithiasis. Case Rep Urol. 2014;2014:1–3. doi:10.1155/2014/161640
9. Hasigov A, Engbang JPN, Fidarov F. Giant pyonephrosis due to urolithiasis and diabetes: a case report. Open J Urol. 2016;06(07):122–125. doi:10.4236/oju.2016.67021
10. Niang FG, Faye I, Ndong A, Thiam I, Diop AN. Spontaneous rupture of a giant pyonephrosis: a case report. Radiol Case Rep. 2022;17(4):1225–1227. doi:10.1016/j.radcr.2022.01.056
11. Kaura KS, Kumar M, Sokhal AK, et al. Giant hydronephrosis: still a reality! Turk J Urol. 2017;43(3):337–344. doi:10.5152/tud.2017.78379
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.