")
Back to Journals » Open Access Surgery » Volume 16
Giant Cystic Hygroma with Complete Encasement of the Great Vessels of the Neck in an 18 Month Old Infant
Authors Abdulahi Z , Meseret G, Belachew A, Abera K
Received 2 June 2023
Accepted for publication 26 September 2023
Published 6 October 2023 Volume 2023:16 Pages 55—60
DOI https://doi.org/10.2147/OAS.S416166
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Luigi Bonavina
Zinedin Abdulahi,1 Girum Meseret,2 Anteneh Belachew,3 Kalkidan Abera4
1Department of Surgery, Pediatric Surgery Unit, Haramaya University, Hiwot Fana Comprehensive University Hospital, Harar, Ethiopia; 2Department of Surgery, Plastic and Reconstructive Surgery Unit, Haramaya University, Hiwot Fana Comprehensive University Hospital, Harar, Ethiopia; 3Department of Anatomical Pathology, Haramaya University, Hiwot Fana Comprehensive University Hospital, Harar, Ethiopia; 4Department of Clinical Radiology, Harar General Hospital, Harar, Ethiopia
Correspondence: Zinedin Abdulahi, Department of Surgery, Pediatric Surgery Unit, Haramaya University, Hiwot Fana Comprehensive University Hospital, Harar, Ethiopia, Email [email protected]
Background: Cystic hygroma is a benign condition of the lymphatic vessels. It is seen in 1 in 5000 live births. Generally lymphatic malformations are classified into microcystic and macrocystic. They commonly occur in the cervicofacial and axillary regions.
The Case: A 1 year and 6 month old female child presenting with progressive right side neck swellings with later development of voice change and air hunger which is positional. Contrast enhanced CT of the neck demonstrated cystic mass with encasement of the common carotid artery and jugular vein with the mass also extending to the submandibular gland and the base of skull. After a 48 hour course of dexamethasone the patient was operated on with complete excision of the mass. Intraoperatively we also encountered right hypoglossal nerve passing through the mid part of the mass. Patient developed post-operative facial palsy with progressive improvement.
Conclusion: Giant lymphatic malformations particularly in the neck region can involve great vessels and major nerves so extreme care is needed during operative interventions to avoid major operative injuries.
Keywords: giant cystic hygroma, common carotid artery, vagus nerve, hypoglossal nerve
Background
Lymphangiomas are the most common name given to lymphatic abnormalities, yet the term “malformation” is more accurate because the prefix “appendix-oma” suggests the hyperplastic and proliferative nature of tumors. The gross histology might range from a single giant cyst or macrocystic structure to numerous smaller cysts also called microcystic lymphatic malformations. These lesions can affect the tissue architecture locally or more extensively. Lymphatic malformations change in size as a result of injury or infection, and they may undergo fibrotic shrinking following recurring episodes of infections namely lymphangitis and cellulitis.1
About 1 in 6000 live births are affected with cystic hygroma. The posterior cervical triangle of the neck is the typical location for 70–80% of cystic hygromas while the remaining 20–30% are distributed across the axilla, superior mediastinum, chest wall, mesentery, retroperitoneal area, pelvis, and uterus. Cystic hygroma is known to present at birth in about 50% of the affected newborns and 90% present by age 2 years.2
ymphatic malformations may be treated with sclerotherapy, surgical resection, or both. Morbidity can be anticipated based on the anatomic location and extent. Resecting complex LM can be of significant benefit but often staging is needed. The operation is long and tedious, and requires meticulous dissection to preserve vital structures.3
Case Presentations
This case is an 18 month old female child who was delivered at a local health center with delivery being uneventful. The mother did not have ANC follow-up. Six months prior to her presentations the mother noticed right side neck swelling which gradually increased in size with progressive voice changes and difficulty in breathing particularly while she sleeps in supine or left lateral positions. At presentation she had moderate malnutrition and a 10 by 15 centimeter, nontender, and mobile mass without distended neck veins, as shown in Figure 1. Chest exam was non remarkable. Baseline lab works were sent and all were normal. Neck sonography demonstrated a right side multispeed fluid-containing cystic mass with some solid components and carotid artery was seen at the middle of the mass consistent with cystic hygroma. To further delineate the anatomy we did a CT scan with contrast of the neck which showed a 15 by 13 cm mass with common carotid artery and jugular vein encasement and tracheal shift to the left side. There was also mild narrowing of the common carotid artery (Figure 2).
 |
Figure 1 Showing 25 by 20 centimeter right-sided lymphatic mass extending from lower neck to mandibular area and the mass also extends to the left side. |
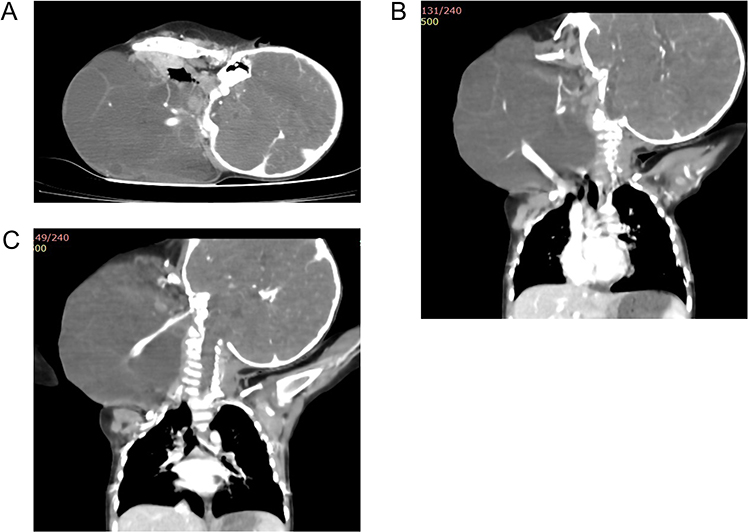 |
Figure 2 Note that there is a well-defined lobulated multiseptated cystic lesion on the right cervical region measuring 14 by 10.5 by 12.5 cm. It has enhancing solid components and septa (A). The mass extends from the right maxillary region to the suprascapular area with minimal extensions to the thoracic inlet and involves the anterior and the posterior cervical regions. The mass surrounded and pushed the right carotid artery and the internal jugular vein anterolateral with minimal caliber changes and no filling defects seen. The sternocleidomastoid muscle is stretched and lost its fat plane at the dorsomedial side. The right submandibular gland is infiltrated with the mass and there is clear fat plane with right thyroid lobe (B and C). |
Because of the size of the mass and the complexity of the planned operation we prepared an ICU bed and gave her dexamethasone for 48 hours and proceeded to surgery. With central line secured we made a right side reverse J incision to expose the mass. First we made a proximal control of the common carotid artery, the internal jugular vein and the vagus nerve and proceeded upwards and all the neurovascular structures were freed by careful combination of blunt and sharp dissections (Figure 3). We also encountered the right hypoglossal nerve passing in the mass to submental space. The mass was inseparable from the right submandibular gland so we removed the gland. There was iatrogenic entry to the floor of the mouth and pharynx both of which were repaired in two layers. Finally we removed the whole tumor with no major neurovascular injury, as shown in Figure 4. Surgery took about eight and a half hours. We then transferred the intubated patient to ICU. Later on she was extubated after 5 days but there was significant stridor so a tracheostomy was performed. The patient also developed right side facial weakness but this is improving so we have considered facial nerve strain only. Steroid was tapered over three weeks. After nutritional rehabilitation the patient was discharged home with tracheostomy weaning process started. Because of the limitations we could not do genetic screening but we have subjected the specimen for pathology and the conclusion is of lymphatic malformations, as shown in Figure 5.
 |
Figure 3 (A) The internal jugular vein, common carotid artery and vagus nerve are exposed and controlled with loop; (B) shows on further mobilizations of the mass the internal jugular vein is seen passing through the mid portion of the mass. |
 |
Figure 4 (A) Shows a complete excision of the mass with freed great vessels and vagus. Also note the hypoglossal nerve passing anterior to the bifurcation of the common carotid artery; (B) final appearance after completion of the surgery; (C) resected specimen. |
 |
Figure 5 Histologic section shows lymphatic spaces lined by attenuated endothelium and separated by thin fibrous stroma containing lymphocytes. |
Discussions
We report a neck-based large cystic hygroma with a neurovascular encasement.
Most lymphatic abnormalities are discovered postnatally and become clinically apparent at an early age; more than 65% of diagnoses are made at birth, and over 90% by the age of 2 years.2 There is no known pathophysiology for LMs but the lymphatic sac’s inability to connect with the systemic venous system is ascribed as the cause of neck and axillary LMs. Peripheral lesions could be explained by lymphatic bud sequestration.4 Understanding lymphatic embryology allows one to appreciate the tendency of postnatal lymphatic abnormalities to occur in lymphatic-rich regions of ontogeny.5,6 The cervicofacial region (75%) and the axillary region (20%) are the most frequent anatomical sites, followed by the mediastinum and the retroperitoneum.
Preference for one race or sexual orientation is not seen in this malformations. Several imaging modalities may be required, depending on the intricacy of the anatomy and any potential extension or field effects of the anomaly.7 LMs may swell in response to a systemic viral or bacterial infection which is not seen in other vascular abnormalities. Usually, this passive engorgement has no negative effects. Antibiotics (oral or intravenous, depending on severity) should be started when regional edema, tightness, erythema, and systemic indications of infection appear suddenly.
The indications for LM treatment vary with the extent and location of the lesions. Some of the indications for ablation or resection are recurrent complications with infection, cosmesis, deformity, dysfunction, airway obstructions and leakage into body cavities or from the skin.8
Sclerotherapy, surgical resection, or a combination of the two may be used to treat LMs.
Sclerotherapy is effective for treating macrocytic LMs and frequently results in unnoticeable lesions. Typical sclerosants that are commonly used are sodium tetradecyl sulfate, pure ethanol, and doxycycline.
The sole option for a permanent LM cure is surgical excision. Resection for complex LM can also be of significant benefit, but staging is often needed. Particularly cervicofacial LMs often require staged procedures. Tracheostomy may be needed in cases of oropharyngeal and airway obstruction, and should precede attempts at sclerotherapy for cervicofacial LM.8 Typically the operation takes a long time and is tedious, and often requires meticulous dissection to preserve vital structures. The use of nerve stimulators decreases the chance of injury to major nerves.8,9
Conclusions
We have operated on a mass of this complexity in a resource-limited setting without the aid of nerve stimulations and in a single stage. We avoided sclerotherapy in this particular patient because the common carotid artery and the jugular veins were entrapped within the mass. Operations close to these important structures can be tiring and time-consuming so one has to be meticulous, patient, and careful while performing such procedures. Proximal control of neurovascular structures is of paramount importance while operating on such complex masses. We have followed the child for one and a half years and there is no recurrence.
Abbreviation
LMs refers to lymphatic malformations.
Ethics Informed Consent
Informed consent was obtained from the guardians of the patient to publish the case and use of both preoperative and intraoperative images. Institutional approval is not acquired to publish this report.
Acknowledgment
To the families of the girl for their willingness for the case to be reported and to Dr. Fisseha Temesegen (consultant General and Pediatric surgeon at Tikur Anbessa Specialized University Hospital, Addis Abeba University) for the valuable advice that he has given us during the surgical planning.
Funding
No support or funding was obtained for this report.
Disclosure
The authors report there is no known competing financial interest or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Mulliken JB. Vascular malformations of the head and neck. In: Mulliken JB, Young AE, editors. Vascular Birthmarks, Hemangiomas and Malformations. Philadelphia: WB Saunders; 1988:301.
2. Dahnert W. Radiology Review Manual.
3. Upton J, Coombs CJ, Mulliken JB, et al. Vascular malformations of the upper limb: a review of 270 patients. J Hand Surg Am. 1999;24(5):1019–1035. doi:10.1053/jhsu.1999.1019
4. Brouillard P, Vikkula M. Genetic causes of vascular malformations. Hum Mol Genet. 2007;16(Spec No. 2):R140–9. doi:10.1093/hmg/ddm211
5. Sabin FR. The lymphatic system in human embryos with a consideration of the morphology of the system as a whole. Am J Anta. 1909;9(1):43. doi:10.1002/aja.1000090104
6. Sabin FR. On the origin of the lymphatic system from the veins and the development of the lymph heart and thoracic duct in the pig. Am J Anat. 1901;1(3):367. doi:10.1002/aja.1000010310
7. Bill AH, Summer DS. A unified concept of lymphangiomas and cystic hygroma. Surg Gynecol Obstet. 1965;120:79.
8. Fonkalsrud EW. Congenital malformations of the lymphatic system. In: Gans SL, Grosfeld JL, editors. Seminars in Pediatric Surgery. Vol. 3. Orlando, FL: WB Saunders; 1994:62.
9. Alqahtani A, Nguyen LT, Flageole H, et al. 25 years’ experience with lymphangiomas in children. J Pediatr Surg. 1999;34(7):1164–1168. doi:10.1016/S0022-3468(99)90590-0
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.