")
Back to Journals » Risk Management and Healthcare Policy » Volume 17
Gender and the Relationship Between Knowledge, Self-Efficacy, and Behaviors for Cardiovascular Health Among Adults – The Effects of Conditional Process Modeling
Authors Wiraszka O , Włodarczyk D
Received 9 November 2023
Accepted for publication 17 February 2024
Published 26 February 2024 Volume 2024:17 Pages 365—374
DOI https://doi.org/10.2147/RMHP.S447839
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gulsum Kubra Kaya
Oliwia Wiraszka,1,* Dorota Włodarczyk2,*
1Faculty of Health Sciences, Medical University of Warsaw, Warsaw, Poland; 2Department of Health Psychology, Medical University of Warsaw, Warsaw, Poland
*These authors contributed equally to this work
Correspondence: Oliwia Wiraszka, Faculty of Health Sciences, Medical University of Warsaw, Warsaw, Poland, Tel +48 798 664 227, Email [email protected]
Background: Cardiovascular diseases are the main causes of morbidity and premature mortality among men and women in most industrialized and many developing countries. Cardiovascular health (CVH) is a relatively new term that focuses on maintaining good health not only on the prevention of cardiovascular diseases.
Purpose: To demonstrate gender differences in selected elements regarding CVH, such as cardio-protection knowledge, behaviors for CVH, and self-efficacy and in the relationships between them.
Methods: In this cross-sectional study, a convenience sample of 157 respondents (70% women) aged 20– 60 was included. The research tool consisted of four parts: the List of Health Behaviors – CVH version, the Test of Cardio-protection Knowledge, the Generalized Self-Efficacy Scale (GSES), and a sociomedical survey. To estimate the direct and indirect effects between the variables, a bootstrapping procedure was adopted, as recommended for small- and medium-sized samples.
Results: There were no gender differences in cardio-protection knowledge, but the groups differed in the levels of behaviors for CVH and self-efficacy. Women generally declared a higher level of healthy behaviors, whereas men demonstrated a higher level of self-efficacy. Women reported more healthy activities related to diet. Men more frequently practiced resistance exercise. The relationships between cardio-protection knowledge, self-efficacy, and behaviors for CVH were different in men and women.
Conclusion: Further research should focus more on gender differences in mechanisms underlying health behaviors. Health-promoting programs should give more attention than before to how to differentiate the messages sent to men and women.
Keywords: self-efficacy, cardiovascular health, health behaviors
Introduction
Due to the fact that cardiovascular diseases (CVDs) are the main cause of morbidity and premature mortality among men and women in most industrialized and many developing countries,1 the topic of cardiovascular (or cardiac or heart) health (CVH) is attracting increasing interest. It grew out of preventive cardiology, which in turn evolved from cardiology.2 The term “CVH” emphasizes a new focus on maintaining good health, going beyond simply the prevention of cardiovascular diseases. Nowadays, it is increasingly used not only by cardiologists but also by experts in healthcare, health policy, and health economics focused on promoting and preserving high levels of CVH from childhood to middle age and beyond.3
Key recommendations on how to reduce and even prevent the incidence of cardiovascular diseases originate from preventive cardiology and are based on findings from landmark studies like the Framingham Study4 and the Seven Countries Study.5 Thanks to them, scientists have acquired a basic knowledge about the occurrence of heart diseases and factors predisposing to their occurrence. Currently, recommendations are developed by large institutions and associations uniting specialists dealing with problems of the heart and vascular diseases, such as the American Heart Association and the European Society of Cardiology.6,7
The main recommended behaviors encompass a healthy diet (a Mediterranean diet or another similar one), optimizing lifestyle by reducing the amount of time spent sitting, engaging in physical activity, maintaining a healthy body weight, quitting smoking, caring about mental health, and reducing stress.7 However, to maintain a proper level of CVH in the population, knowledge about recommended behaviors and their actual implementation (action in accordance with recommendations) play a key role. Studies on the level and in the scope of such knowledge may be helpful in determining further directions in promoting CVH.
Reports revealed gender as a factor differentiating levels of knowledge and behaviors for CVH. For example, a study in six European countries revealed social inequalities in CVD awareness.8 CVDs were recognized as the main health problem by less than 20% of surveyed men and 4% of women, while 50% of male respondents identified heart disease as the leading cause of death, compared to 16.5% of female respondents. Regardless of gender, only about 15% were able to identify the symptoms accompanying a myocardial infarction other than chest pain. For both sexes, the most common risk factor for developing CVD was exposure to stress (63% of respondents). Men more often pointed to smoking, drinking alcohol, and not taking up physical activity, whereas women more frequently mentioned obesity. Female respondents more often than men declared going to doctor’s appointments and self-monitoring in terms of blood pressure measurements, as well as following a diet containing a large amount of fruit and vegetables. Men, on the other hand, highlighted better coping with stressful situations, maintaining a healthy weight, and quitting smoking.8 Other studies also confirmed that as well as factors such as place of residence and level of education, gender is another one determining the level of knowledge about CVD risk factors. Women are more knowledgeable about it and also more willing to participate in health-related studies, which may impact their results.9 In addition to the above, women are also more aware of the harmful effects of inappropriate habits or lifestyle. Obese women were more likely than obese men to believe that their diet was harmful. Similarly, more female than male smokers perceived their addiction as harmful.10 Other studies found that women and men had similar Framingham CVD risk scores, however women perceived their risk to be significantly higher.11 In the nationwide multicenter epidemiological WOBASZ study conducted in Poland in the years 2003–2005, respondents (over 13,500) were asked to suggest ways of reducing the incidence of CVD, excluding medication.12 Twenty percent of the respondents were unable to give any example; most of them were men. In the question on the consequences of untreated hypertension, 20% of the total population could not give any correct answer, and again the majority of this group were men. Extensive knowledge in this area was shown by only 2.2% of the respondents, among whom the group of women was twice as large as that of men.13
According to the most prominent health behavior theories, self-efficacy is an important factor involved in the implementation of healthy action. It is defined as “the belief in one’s capabilities to organize and execute the course of action required for producing given attainments”.14 It may be of a more general nature or refer to a specific area like sedentary behaviors.15 Self-efficacy encompasses cognitions that determine whether a change in health behavior will be initiated, how it will be performed, and for how long it will be sustained in the face of adversities.16 Its role in lifestyle change was confirmed in many studies.17 Therefore, findings on factors and conditions that are conducive to increasing self-efficacy would also be of special importance in the field of CVH. It seems that proper cardio-protection knowledge (set of options that could be used) would affect self-efficacy beliefs in one’s own capabilities to act (the “can-do cognition”18) and in the aftermath change behaviors for CVH. However, in the light of the data showing gender differences in attitudes towards health, it is not clear whether the above relationships are similar in men and women.
The Aims of the Study and Hypotheses
There were two main aims of the study: 1) to examine gender differences in cardio-protection knowledge, behaviors for CVH, and self-efficacy; and 2) to verify the role of gender in the relationship between cardio-protection knowledge and behaviors for CVH with self-efficacy as an intervening variable (Figure 1). In this study, we used terminology suggested by Preacher and Hayes19 and focused on an indirect effect (but not a mediated effect) and moderation (Hayes, 2012).20
 |
Figure 1 The conceptual model tested in the study: gender as a moderator of the relationship between cardio-protection knowledge and behaviors for CVH through self-efficacy as an intervening variable (ab – indirect pathway; c’ - direct pathway). |
In this model, it is postulated that cardio-protection knowledge affects behaviors for CVH directly and indirectly through self-efficacy as an intervening variable. In the indirect effect (the product of paths a and b), cardio-protection knowledge is assumed to affect self-efficacy beliefs (path a), and this results in a change in behaviors for CVH (path b). The direct effect is an effect of cardio-protection knowledge on behaviors for CVH after controlling for self-efficacy. It is also hypothesized that gender moderates both the relationship between cardio-protection knowledge and self-efficacy (path a) and the direct effect between cardio-protection knowledge and behaviors for CVH (path c’ – the relationship between cardio-protection knowledge and behaviors for CVH after controlling for self-efficacy as an intervening variable). Based on the results of correlation analyses we may expect these relationships to be different in women and men (gender as a moderator).
Method
Participants and Procedure
In this cross-sectional study, the sample consisted of 157 respondents, including 109 women (69%), 47 men (30%), and one person describing their gender as different (1%).
The inclusion criteria were as follows: adults aged 18–60, with non-medical professional/academic activities, without diagnosed or treated cardiovascular disease (CVD), and consent to participate in the study. Among the entire group of respondents, four people confirmed having CVD, and they were excluded from further analyses. The study was conducted from September 2022 to January 2023. Paper questionnaires with the instructions for the procedure were disseminated among workers in the selected public administration offices after getting permission from their management. Next, the surveys were collected at the time agreed beforehand. Thus, 82 (out of 120; 70% response rate) anonymously completed surveys were collected. Additionally, the link to the online survey was made available to the group of extramural students of non-medical faculties and 75 of them completed the survey. The method of assessment did not differentiate the levels of key variables in the study. Statistical analysis was performed using SPSS version 24. The study was approved by the Bioethics Committee of the institution (Medical University of Warsaw, no. AKBE/211/2022, issued on September 12, 2022).
Measures
The research tool consisted of four parts, with three of them being developed for the purpose of the study. The first part was a sociomedical survey in which respondents were asked to provide, among other things, their age, gender, health status, etc.
The second part was the List of Health Behaviors – CVH version, consisting of 15 statements describing behaviors for CVH developed on the basis of the contemporary recommendations. This part starts with the question: “In the last year, how often have you performed the following activities?” Examples of these behaviors include: at least 150–300 minutes of aerobic exercise of moderate intensity per week; a diet consisting of plants and products rich in fiber; and caring about experiencing positive emotions in one’s life. The participants responded using a five-point Likert scale from 1 – almost never to 5 – always or almost always/several times a week (depending on the type of behavior). The total score of behaviors for CVH was calculated as a sum of responses to all items. The reliability of the scale was satisfactory with a Cronbach’s alpha of 0.79.
The third part was the Test of Cardio-protection Knowledge. It consisted of 15 statements developed on the basis of contemporary knowledge, for example: Maintaining a healthy weight reduces the risk of heart diseases; good relationships with people promote heart health; for health reasons, a better choice is to limit meat consumption, especially processed meat. The respondents assessed whether the statement was true (1) or false (0) according to their knowledge. Due to the ambiguous wording, one of the statements was excluded. The total score of knowledge was calculated as a sum of 14 responses. The reliability of this scale measured by the Kuder-Richardson formula-20 was 0.60, with a mean proportion of correct answers of 0.85.
The level of self-efficacy was measured by means of the Polish adaptation of the Generalized Self-Efficacy Scale (GSES) by R. Schwarzer et al.21 It contains 10 statements on various personal characteristics relevant to performing action and achieving one’s goals, for example: “I can always solve difficult problems if I just try hard enough”. The respondents assessed to what extent they agreed with them using a four-point scale from 1 = no to 4 = yes. The total score was calculated as a sum of all responses. The Cronbach’s alpha coefficient was 0.86.
In all questionnaires, higher total scores indicated higher levels of frequency of behavior for CVH, cardio-protection knowledge, and self-efficacy.
Statistical Analysis
The violation of normal distribution of variables was verified with the Kolmogorov–Smirnov test. It showed that except for behavior index, they were not normally distributed (p < 0.05). Thus, to analyze the differences between groups we used the nonparametric Mann–Whitney test (including for single-question results). To compare the groups with respect to descriptive statistics, we used a chi-square test (for frequencies) and analysis of variance (for interval and ratio scales; in cases where the assumption of variance homogeneity was not met, we applied the Brown-Forsythe correction).22
To estimate the direct and indirect effects between the variables in the conceptual model, a regression-based path analysis approach was adopted, as proposed by Preacher and Hayes19,20 together with the PROCESS macro (available at www.processmacro.org). PROCESS uses a bootstrapping procedure, which is recommended when there are asymmetries and other forms of nonnormality in the sampling distribution of the statistic, especially in small- and medium-sized samples.23 Two models from a versatile computational tool were used: Model 4 (to establish indirect and direct effects in a total sample) and Model 8 (to establish conditional indirect and direct effects, specific to each gender).20 In the analyses, 5000 bootstrap resamples and 95% confidence intervals (CI) were used, with values of low and upper levels of CI (LLCI and ULCI, respectively). All the statistical analyses were conducted using SPSS 26 software. A value of 0.05 was used as the significance level.
Results
Sociomedical Characteristics of the Group by Gender
The mean age of the sample was 34.90±10.96 years (range from 20 to 60). The mean body weight of the subjects was 73.28±16.99 kg (range from 45 to 130), and the mean height was 171.10±9.007 (range from 153 to 195). Based on the body weight and height of the subjects, the average BMI was calculated, where the mean 24.86±4.52 kg/m2 (min–max 16.94–37.25).
Men and women differed in their occupational status (x² = 6.63; p = 0.04). Women were more frequently professionally active (79% versus 60%), whereas among men there were more students (40% versus 21%). Women also reported more stressful situations in their lives (Z=−3.71; p < 0.001). The groups did not differ in age (Z = −1.54; p = 0.123), the number of diseases under treatment (x² = 1.40; p = 0.85), the frequency of blood pressure measurements last month and lipid profile last year (x² = 2.39; p = 0.30 and x² = 0.94; p = 0.62, respectively), and the frequency of smoking (x² = 4.46; p = 0.35). Men and women did not differ in their subjective health status (Z = −1.39; p = 0.16) and familiarity with the term “cardiovascular health” (x² = 3.50; p = 0.48). Half of the group had never met this term, 15% had heard the term but they did not know what it meant, and 35% declared that they had come across this term and they knew what it meant.
Gender and Cardio-Protection Knowledge and Behaviors for Cardiovascular Health, and Self-Efficacy
Descriptive statistics of the main variables were as follows: for behaviors for CVH, the scores ranged from 5 to 56 (mean 36.27±10.44); for cardio-protection knowledge, the scores ranged from 5 to 14 (median = 12, mean 11.87±1.83); for self-efficacy, the scores ranged from 10 to 40 (median = 30, mean 29.33±4.51).
There were no gender differences in cardio-protection knowledge but the groups differed in the levels of cardio-protection behaviors and self-efficacy (Table 1). Women declared a higher level of healthy behaviors, whereas men demonstrated a higher level of self-efficacy.
 |
Table 1 Gender Differences in Total Scores of Cardio-Protection Knowledge, Behaviors for CVH, and Self-Efficacy |
The analysis of specific cardio-protection behaviors revealed that women and men differed in six behaviors out of the 15 included in the study (Table 2). Women declared more healthy activities related to diet: a diet based on vegetables and fruits, wholegrain cereal products and low-fat dairy products, replacement of saturated fats with unsaturated ones, introduction of fiber products, limitation of alcohol consumption to 100g/week, and replacing meat with oily fish at least once a week. Men more frequently practiced resistance (strength) exercise at least twice a week.
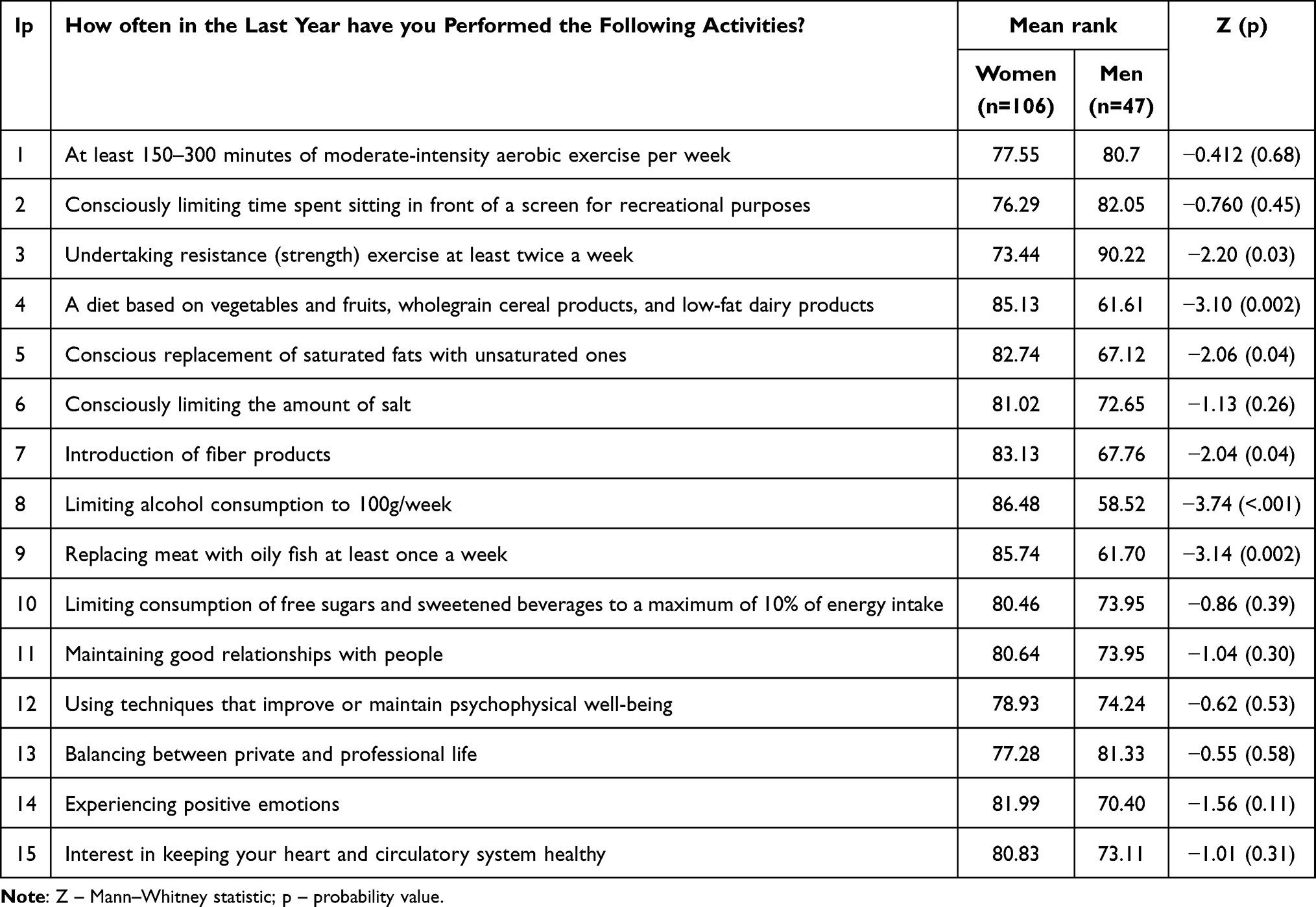 |
Table 2 Specific Cardio-Protection Behaviors by Gender |
The Relationships Between Cardo-Protection Knowledge, Self-Efficacy, and Behaviors for CVH – the Role of Gender
As shown in Table 3, the coefficients of correlations in the total sample have a different character compared to gender groups. In the total sample, cardio-protection knowledge was significantly connected with behaviors for CVH (weak correlation). Both knowledge and behaviors were related to self-efficacy, but the relationship between self-efficacy and behaviors only approached statistical significance. It turned out that the relationships between knowledge and behaviors and between behaviors and self-efficacy were only significant in women. At the same time, there was a noticeable connection between knowledge and self-efficacy in men, which in women only approached statistical significance.
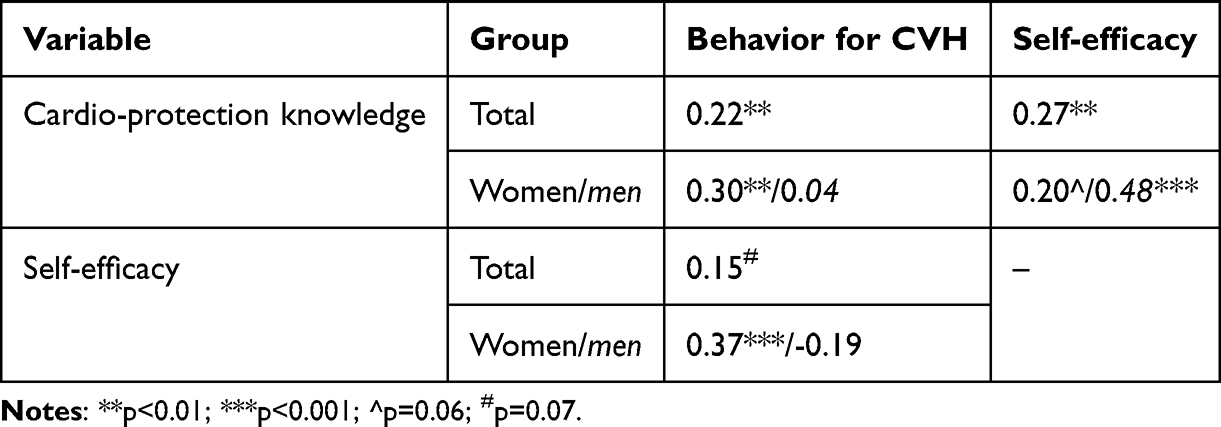 |
Table 3 Correlation Coefficients Between Cardio-Protection Knowledge, Self-Efficacy, and Behaviors for CVH in Total Sample and Gender Groups |
As shown in Table 4, both direct and indirect effects in the model of simple mediation (Model 4), without taking into account gender, were not significant. In the model of moderated mediation (Model 8), after controlling for self-efficacy, the direct relationship between cardio-protection knowledge and behaviors for CVH exists only in women. At the same time, the indirect effect of knowledge on behaviors for CVH through self-efficacy exists only in men. In men, cardio-protection knowledge is more strongly related to self-efficacy than in women, whereas the relationship between self-efficacy and behaviors for CVH is stronger in women. The effect size was stronger in men than in women (0.58 versus 0.28), however the pairwise contrast between conditional indirect effects was equal to −0.30 with a 95% CI between −1.06 and 0.39 and was insignificant.
 |
Table 4 Direct and Indirect Effects in Simple and Conditional Process Modeling |
Discussion
The study aimed to analyze selected elements regarding cardiac health, such as cardio-protection knowledge, behaviors for CVH, and self-efficacy, as well as gender differences in this area. It included a convenience group of adults not undergoing treatment for cardiac diseases, the majority of whom were women.
The results regarding the first research question indicate that women and men did not differ in terms of cardio-protection knowledge, but women had a higher rate of declared behaviors for CVH and a lower level of self-efficacy. A previous study showed that women usually have higher and/or broader knowledge of CVD risk factors and cardio-protection behaviors than men. A similar result was observed in a study regarding analysis of the level of knowledge in this area.9 In the WOBASZ study, among people who were unable to provide any examples of ways to reduce the incidence of CVD and the consequences of untreated hypertension, the majority were men. The small group of people who knew the answers were predominantly women.13 Unfortunately, due to the adoption of different tools for examining this area of knowledge, it can be difficult to compare the results. We adopted the test of knowledge, which allowed us to calculate a total number of correct answers. The questions encompass knowledge on recommended behaviors and the role of selected classic risk factors (hypertension, diabetes, cholesterol) and other risk factors, such as air pollution, social interactions, and depression. The reliability of the tool was slightly below the expected level, and the mean proportion of correct answers was quite high. Thus, this test could be too easy for this group and not potent enough to reveal the differences between groups. It seems that further development of the tool properly measuring cardio-protection knowledge with an easy way to update its questions according to the newest empirical results is necessary, both for clinical practice and scientific purposes.
Women declared a higher level of behaviors for CVH in the form of a global score. Specifically, they practiced five out of 15 behaviors more frequently than men. These activities referred mainly to the diet: higher intake of vegetables and fruits, wholegrain cereal products and low-fat dairy products, replacement of saturated fats with unsaturated ones, introduction of fiber products, and limiting salt and alcohol consumption. Men more frequently declared undertaking resistance exercise at least twice a week. These results are similar to other studies and confirm some specific patterns of health behaviors among men and women. Women are usually much more focused on diet (often in the context of their obesity or the prevention of obesity), whereas men are more focused on physical activity (often in the context of maintaining a proper weight and physical fitness). These differences seem to be related to culture and social conditions, like social roles and expectations. Men are noticeably less likely to use heart health behaviors despite having a similar level of knowledge as women.24,25 Research has shown that the differences determining physical activity by women and men include aspects such as the element of competitiveness, victory, appearance, and physical condition.26–28 In our study, the groups did not differ in their frequency of smoking and performing blood pressure measurements last month and lipid profile last year. This is not in line with previous research, as it also showed a specific pattern of gender differences: women being more willing to consult doctors and self-monitor (for example, in terms of blood pressure measurements) and men being more focused on quitting smoking.8
Women in our study revealed lower self-efficacy than men, understood as the belief in one’s ability to sustain an action required for achieving goals in the face of adversities. Additionally, women in our sample reported more stressful situations in their lives than men. These two findings are very important in the light of data showing that up to 25% of women experience depressive symptoms during their lives, which has been recognized as a new risk factor for cardiovascular diseases. People with depressive disorder are more prone to develop acute myocardial infarction, heart failure or stroke.29–31 There is increasing evidence of differences between women and men, including in epidemiology, pathophysiology, clinical management, and outcomes related to heart disease. The literature indicates that women are twice as likely to die from cardiovascular diseases and are more likely to suffer from diseases such as stroke, angina, heart failure, and peripheral artery disease than men.32 The basic mechanisms explaining the relationship between depression and CVD are based on behavioral and biological factors. Thus, a higher level of distress in women combined with lower coping resources in the form of self-efficacy, and especially self-efficacy specific for CVH, may constitute an additional risk of comorbidity and mortality among women.
The second research question concerned the role of gender in relationships between cardio-protection knowledge and behaviors for CVH, with self-efficacy as an intervening variable. The result showed that these relationships differ in men and women. In men, cardio-protection knowledge is not directly related to behaviors for CVH but can be important if it relates to self-efficacy. This would suggest that promoting behaviors for CVH in men only by increasing cardio-protection knowledge would be rather ineffective. However, if cardio-protection knowledge increases the sense ofself-efficacy, it may contribute to more frequent behaviors for CVH. In women, both cardio-protection knowledge and self-efficacy were related directly to behaviors for CVH, but cardio-protection knowledge was not related to self-efficacy. This could mean that in women, cognitive factors (like knowledge) are not critical for increasing self-efficacy. It is possible that women are more sensitive to emotional (for example, anxiety about yourself or your children and loved ones or benefits resulting from a given behavior) or practical and experiential aspects (for example, encouragement to act, tips on how to do it, experience or advice of others). At the same time, strengthening self-efficacy in women seems very important as it is positively related to a higher level of behaviors for CVH. These findings suggest that further research should focus more on gender differences in mechanisms underlying the performance of health behaviors. It is probably the case that health-promoting programs should pay more attention than before to how to differentiate the messages sent to men and women. The correlation analysis showed that in men, the relationship between self-efficacy and behaviors for CVH, although insignificant, was negative. This observation is rather confusing and would be difficult to explain. It could possibly occur in the case of overestimation of one’s own capabilities and leads to the loss of motivation as a result of this. However, this finding should be verified in further study with a bigger sample and different study groups.
The results of the study should be treated with caution as it has some limitations. The study included the convenience sample with broad inclusion criteria. The sample size was relatively small, and despite the use of advanced statistical methods (bootstrapping), this constitutes a significant limitation. Additionally, the gender ratio was not sufficiently balanced. The study was of a preliminary character and was focused on the key aspects of cardiovascular health treated as an element of health promotion rather than disease prevention. Thus, the number of factors potentially influencing cardiovascular health (potential confounders) was also limited. However, gender differences were studied not only in relation to the levels of key variables (cardio-protection knowledge, behaviors for CVH, and self-efficacy) but also to mutual relationships between them.
Conclusions and Practical Implications
Women and men did not differ in terms of cardio-protection knowledge, but women had a higher rate of declared behaviors for CVH and a lower level of self-efficacy. The relationships between cardio-protection knowledge, self-efficacy, and behaviors for CVH differed in men and women. Further research should focus more on gender differences in mechanisms underlying health behaviors. Health-promoting programs should give more attention than before to how to differentiate the messages sent to men and women.
Abbreviations
CVD(s), cardiovascular disease(s); CVH, cardiovascular health.
Data-Sharing Statement
The data analyzed in this study are available from the corresponding author on reasonable request.
Ethics Approval
The study was approved by the Bioethics Committee of the institution (Medical University of Warsaw, no. AKBE/211/2022, issued on September 12, 2022). The study was conducted in accordance with the Declaration of Helsinki.
Author Contributions
Both authors contributed equally to the work reported in the conception, study design, acquisition of data, and analysis and interpretation, and took part in drafting, revising, or critically reviewing the article; approved the final version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was supported by the Medical University of Warsaw (grant no. Z/MG/13/22).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cardiovascular diseases. WHO, Health topics, Cardiovascular diseases. Available from: https://www.who.int/health-topics/cardiovascular-diseases#tab=tab_1.
2. Labarthe DR, Kubzansky LD, Boehm JK, Lloyd-Jones DM, Berry JD, Seligman MEP. Positive cardiovascular health a timely convergence. J Am Coll Cardiol. 2016;68(8):860–867. doi:10.1016/j.jacc.2016.03.608
3. Labarthe DR. From cardiovascular disease to cardiovascular health: a quiet revolution? Circ Cardiovasc Qual Outcomes. 2012;5(6):86–92. doi:10.1161/CIRCOUTCOMES.111.964726
4. Cybulska B, Kłosiewicz-Latoszek L. Landmark studies in coronary heart disease epidemiology. the Framingham Heart Study after 70 years and the seven countries study after 60 years. Kardiol Pol. 2019;77(2):173–180. doi:10.5603/KP.a2019.0017
5. Seven Countries Study. homepage on the Internet. Available from: https://www.sevencountriesstudy.com.
6. Donna K, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA Guideline on the primary prevention of cardiovascular disease: a report of the American college of cardiology/American heart association task force on clinical practice guidelines. Circulation. 2019;140(11):596–646.
7. Visseren FLJ, Mach F, Smulders YM, et al. ESC Guidelines on cardiovascular disease prevention in clinical practice. Kardiol Pol. 2022;29:5–115.
8. Daponte-Codina A, Knox EC, Mateo-Rodriguez I, et al. Gender and social inequalities in awareness of coronary artery disease in European Countries. Int J Environ Res Public Health. 2022;19(3):1388. doi:10.3390/ijerph19031388
9. Koziński Ł, Krzymińska-Stasiuk E, Głogowska A, Raczak G. Analysis of the level of knowledge about the basic risk factors of cardiovascular diseases, taking into account socio-demographic relationships: a survey. [Analiza poziomu wiedzy o podstawowych czynnikach ryzyka chorób układu sercowo- -naczyniowego z uwzględnieniem zależności społeczno-demograficznych — badanie ankietowe]. Folia Cardiol Excerp. 2012;7(3):170–176.
10. Silagy C, Muir J, Coulter A, Thorogood M, Roe L. Cardiovascular risk and attitudes to lifestyle: what do patients think? BMJ. 1993;19(6893):1657–1660. doi:10.1136/bmj.306.6893.1657
11. Homko CJ, Santamore WP, Zamora L, et al. Cardiovascular disease knowledge and risk perception among underserved individuals at increased risk of cardiovascular disease. J Cardiovasc Nurs. 2008;23(4):332–337. doi:10.1097/01.JCN.0000317432.44586.aa
12. Drygas W, Bielecki W, Kozakiewicz K, et al. Multi-center National Population Health Survey – WOBASZ. [Wieloośrodkowe Ogólnopolskie Badanie Stanu Zdrowia Ludności – WOBASZ]. In: Epidemiology and Prevention of Circulatory Diseases [Epidemiologia I Prewencja Chorób Krążenia]. Medycyna Praktyczna; 2015:41–55.
13. Bielecki W, Kaczmarczyk-Chałas K, Piwońska A, et al. Awareness of the principles of preventing cardiovascular diseases in the adult population of Poland. Results of the WOBASZ program. [Świadomość zasad zapobiegania chorobom układu krążenia w populacji dorosłych mieszkańców Polski. Wyniki programu WOBASZ]. Kardiol Pol. 2005;63:4.
14. Bandura A. Self-Efficacy: The Exercise of Control. New York: W.H. Freeman and Company; 1997.
15. Blom V, Drake E, Kallings LV, Ekblom MM, Nooijen CFJ. Nooijen CF. The effects on self-efficacy, motivation and perceived barriers of an intervention targeting physical activity and sedentary behaviours in office workers: a cluster randomized control trial. BMC Public Health. 2021;21(1):1048. doi:10.1186/s12889-021-11083-2
16. Luszczynska A, Schwarzer R. Social cognitive theory. In: Conner M, Norman P, editors. Predicting Health Behaviour.
17. Affendi I, Nor Asiah M, Normi M, et al. Association between self-efficacy and health behaviour in disease control: a systematic review. Glob J Health Sci. 2018;10(1):18–36.
18. Warner LM, Schwarzer R. Self-efficacy and health. In: The Wiley Encyclopedia of Health Psychology: Volume II, the Social Bases of Health Behavior. New York: Wiley-Blackwell; 2020:605–613.
19. Preacher KJ, Hayes AF. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav Res Methods Instrum Comput. 2004;36(4):717–731. doi:10.3758/BF03206553
20. Hayes AF. PROCESS: a versatile computational tool for observed variable mediation, moderation, and conditional process modelling; 2012. Available from: http://www.afhayes.com/public/process2012.pdf.
21. Schwarzer R, Jerusalem M, Juczyński Z. GSES Generalized Self-Efficacy Scale [GSES Skala Uogólnionej Własnej Skuteczności]. In: Measurement Tool for Health Psychology Promotion [Narzędzie Pomiaru w Promocji Psychologii Zdrowia]. Warszaw: Pracownia Testów Psychologicznych PTP; 2001.
22. Field A. Discovering Statistics Using SPSS.
23. Levy JA, Landerman LR, Davis LL, et al. Advances in mediation analysis can facilitate nursing research. Nurs Res. 2011;60(5):333–339. doi:10.1097/NNR.0b013e318227efca
24. Domosławska-żylińska K, Włodarczyk D, Krysińska-Pisarek M. Cardiovascular disease threat and perceived efficacy of selected preventive behaviors among Polish men: an analysis based on the extended parallel process model. Front Public Health. 2023;11. doi:10.3389/fpubh.2023.1244302
25. Hildt-Ciupińska K, Pawłowska-Cyprysiak K. Positive health behaviors and their determinants among men active on the labor market in Poland. Am J Mens Health. 2020;14(1):1–10. doi:10.1177/1557988319899236
26. Molanorouzi K, Khoo S, Morris T. Motives for adult participation in physical activity: type of activity, age, and gender. BMC Public Health. 2015;15:66. doi:10.1186/s12889-015-1429-7
27. Egli T, Bland HW, Melton BF, Czech DR. Influence of Age, Sex, and race on college Students’ exercise motivation of physical activity. J Am Coll Health. 2011;59(5):399–406. doi:10.1080/07448481.2010.513074
28. Morgan C, McKenzie T, Sallis J, Broyles S, Zive M, Nader P. Personal, social, and environmental correlates of physical activity in a Bi-ethnic sample of adolescents. Pediatr Exerc Sci. 2003;15(3):288–301. doi:10.1123/pes.15.3.288
29. Bucciarelli V, Caterino AL, Bianco F, et al. Depression and cardiovascular disease: the deep blue sea of women’s heart. Trends Cardiovasc Med. 2020;30(3):170–176. doi:10.1016/j.tcm.2019.05.001
30. Goldstein BI, Carnethon MR, Matthews KA, et al. Major depressive disorder and bipolar disorder predispose youth to accelerated atherosclerosis and early cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2015;132(10):965–986. doi:10.1161/CIR.0000000000000229
31. Lichtman JH, Froelicher ES, Blumenthal JA, et al. Depression as a risk factor for poor prognosis among patients with acute coronary syndrome: systematic review and recommendations: a scientific statement from the American Heart Association. Circulation. 2014;129(12):1350–1369. doi:10.1161/CIR.0000000000000019
32. Martelli E, Zamboni M, Sotgiu G, et al. Sex-related differences and factors associated with peri-procedural and 1 year mortality in chronic limb-threatening ischemia patients from the CLIMATE Italian registry. J Pers Med. 2023;13(2):316. doi:10.3390/jpm13020316
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.