")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 10
Ganciclovir ophthalmic gel 0.15% for the treatment of acute herpetic keratitis: background, effectiveness, tolerability, safety, and future applications
Received 25 November 2013
Accepted for publication 14 February 2014
Published 20 August 2014 Volume 2014:10 Pages 665—681
DOI https://doi.org/10.2147/TCRM.S58242
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Timothy Y Chou, Bennett Y Hong
Department of Ophthalmology, Stony Brook University, Stony Brook, NY, USA
Abstract: Eye disease due to herpes simplex virus (HSV) is a leading cause of ocular morbidity and the number one infectious cause of unilateral corneal blindness in the developed parts of the globe. Recurrent keratitis can result in progressive corneal scarring, thinning, and vascularization. Antiviral agents employed against HSV have primarily been nucleoside analogs. Early generation drugs included idoxuridine, iododesoxycytidine, vidarabine, and trifluridine. While effective, they tended to have low bioavailability and measurable local cellular toxicity due to their nonselective mode of action. Acyclovir 0.3% ointment is a more selective agent, and had become a first-line topical drug for acute HSV keratitis in Europe and other places outside of the US. Ganciclovir 0.15% gel is the most recently approved topical treatment for herpes keratitis. Compared to acyclovir 0.3% ointment, ganciclovir 0.15% gel has been shown to be better tolerated and no less effective in several Phase II and III trials. Additionally, topical ganciclovir does not cause adverse systemic side effects and is therapeutic at lower concentrations. Based on safety, efficacy, and tolerability, ganciclovir 0.15% gel should now be considered a front-line topical drug in the treatment of dendritic herpes simplex epithelial keratitis. Topics of future investigation regarding other potential uses for ganciclovir gel may include the prophylaxis of recurrent HSV epithelial keratitis, treatment of other forms of ocular disease caused by herpesviruses and adenovirus, and ganciclovir gel as an adjunct to antitumor therapy.
Keywords: antiviral, herpes, Virgan, Zirgan, ganciclovir, keratitis, HSV
Herpes simplex virus ocular infection
Eye disease due to herpes simplex virus (HSV) is a leading cause of ocular morbidity and the number one infectious cause of unilateral corneal blindness in the developed parts of the world.1–8 Herpes simplex type 1 (HSV-1) is the most common herpes virus implicated in ocular infections. Herpes simplex type 2 (HSV-2) can also infect ocular tissues, but in such instances is more commonly seen in the neonatal setting.2
A recent survey revealed that nearly 60% of individuals in the US are seropositive for HSV-1, indicating that they had been exposed to the virus.9 Polymerase chain reaction testing of trigeminal ganglia in cadavers detected a greater presence of HSV with increasing age, reaching almost 100% by the age of 60 years.2 An estimated 400,000 to 500,000 individuals have experienced some form of ocular infection with HSV in the US.1,6,10–12 Incidence of HSV keratitis in the US and Europe ranges from 4.1 to 31.5 cases per 100,000 per year, of which 42% comprise new cases and 58% recurrent cases.4,5,13–15 In raw numbers, that represents some 48,000 to 59,000 episodes of ocular herpes diagnosed each year stateside, 20,000 to 24,000 of these being new primary cases.3,4,10,12,14 Across the globe, roughly one million new or recurrent cases of herpes simplex epithelial keratitis occur annually.16 Epithelial keratitis is the most prevalent form of ocular herpes simplex infection, comprising 50% to 80% of cases.16
The herpesviruses comprise a family of DNA viruses, eight of which are known to cause human disease.2,3,17 Herpesviruses have been implicated in numerous varied and, often, extremely serious diseases – several with ophthalmic manifestations. HSV-1, most commonly observed in the form of herpes labialis, is responsible for an estimated 98% of nonneonatal ocular infections.2,4,18,19 HSV-2 is the usual etiologic agent for genital and neonatal herpes infections; it can occasionally also infect ocular and orofacial structures through sexual transmission. The clinical appearance of keratitis from HSV-1 and HSV-2 is essentially the same.1 Neonatal herpes simplex infection, which can involve HSV-1 as well as HSV-2, is most frequently transmitted through the birth canal.2,4 Eighty percent of infected neonates with no central nervous system involvement develop keratitis, and 10% manifest conjunctivitis.7 Varicella-zoster virus is behind another consequential ocular infection - herpes zoster ophthalmicus. Epstein-Barr virus can cause acute mononucleosis and, along with it, a secondary keratitis. Cytomegalovirus (CMV) underlies a severe retinitis that can develop in immunoincompetent individuals, such as those with adult immune deficiency syndrome due to human immunodeficiency virus. The other human herpesviruses are: human herpesvirus 6, human herpesvirus 7, and human herpesvirus 8. The latter is associated with Kaposi’s sarcoma, lymphoma, and multicentric Castleman’s disease.17,20 The herpesviruses have in common an icosahedral coat and they reproduce by replicating double stranded DNA. Their virions invade living cells, establishing latency in the cell nuclei, where their linear genome is transformed into circularized episomes that are not integrated into the host DNA chromosome.17,21,22 During the replication process, host cellular machinery is recruited to aid in the transcription and production of virally-encoded proteins (including virally-encoded factors, DNA-dependent DNA polymerase, and transcription factors) that ultimately effect DNA replication and virion assembly.23
HSV-1 is typically transmitted through nonsexual contact in childhood.1,4 Primary ocular HSV infection may be undetectable or mild a majority of the time.2 It is estimated that as low as 1% to 6% of initially infected individuals exhibit actual clinical signs and symptoms.1,2,4 Following HSV exposure, there is an incubation period of 1 to 28 days.10 Primary HSV-1 disease may then manifest clinically as a nonspecific upper-respiratory-tract prodrome.24 A vesicular or ulcerative eruption develops over skin and mucus membranes innervated by the fifth cranial nerve such as the periorbital region, where it may present as blepharitis, acute follicular conjunctivitis, or epithelial keratitis.4,24–28 In a Rochester, Minnesota study that followed, for as long as 33 years, 122 patients who were diagnosed for the first time with ocular HSV, initial infections were found to be predominantly corneal.2,28 By contrast, a Moorfields hospital study following 108 patients with ocular HSV for up to 15 years found that most primary infections were located in the conjunctivae and palpebral regions.2,29 After the primary infection, the herpes virus enters a nonreplicating latent stage. It remains dormant indefinitely, typically in the trigeminal nerve ganglion, until such a time that it may reactivate, and then recurs clinically.1,3,7 The virus has been discovered in other spinal ganglia as well.30 Additionally, there is some evidence to suggest that the cornea itself may represent yet another site where latent herpes virus may reside.31,32 Herpes simplex viral DNA has been detected in the cornea through polymerase chain reaction and other means. Some debate whether this may represent low-level active infection rather than true latency.19 Regardless, current methods to detect infectious virus in tissue have limited sensitivity, and the validity of the corneal latency theory therefore has not been conclusively proven.19,33
HSV sometimes seems to reactivate in response to physical, hormonal, or emotional factors.34,35 Stress, ocular trauma, contact lens use, ultraviolet radiation, immune compromise, and hormonal changes have all been identified as possible triggers.2–4,7,10,26,36,37 Conversely, the Herpes Eye Disease Study Group looked at several of these factors, such as psychological stress, systemic infection, sunlight exposure, menstrual period, contact lens wear, and eye injury, and found no statistically significant association between any of them and the reactivation of ocular herpes disease.38 There may be additional external triggers for herpetic disease. For uncertain reasons, there is some predilection for ocular herpes to occur during the winter months.2,10 The incidence of HSV keratitis is increased up to six-fold after corneal transplant, when performed for nonherpetic conditions.2,39,40 Although some cases could be explained by possible activation of previously-unrecognized latent host disease,40 other occurrences after penetrating keratoplasty appear to be due to actual transmission of herpes virus from donor tissue to recipient.31,32 Corneal treatment with the excimer laser can predispose to recurrent herpes ocular disease, as well as stimulate viral shedding.26,41 Underlying local and systemic immunologic deficiency – such as the prior use of steroids and other immunosuppressives, atopic disease, malignancy, and human immunodeficiency virus infection – appears to promote the severity and frequency of infection.2,4 In summary, although the chain of events required to effect HSV reactivation have not been fully elucidated, they appear to be determined by a combination of host, virus, and environmental factors.
Recurrent herpes eye infection frequently presents as epithelial ulceration, which can be further described as dendritic or geographic in appearance (Figure 1). The latter may be a more severe version of the former. In deeper layers of the cornea, HSV can cause stromal keratitis and endotheliitis. Uveitis can sometimes accompany keratitis, or may occur independently. Patients with stromal disease and uveitis almost always have concomitant epithelial involvement, or have had a history of antecedent HSV epithelial keratitis.10 Additional ocular manifestations include blepharitis, canaliculitis, retinitis, and optic neuritis.7
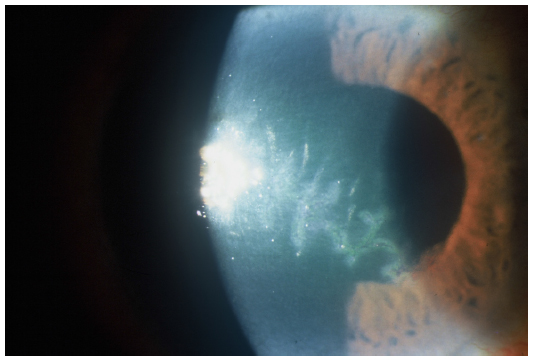 | Figure 1 Large epithelial dendrite due to Herpes simplex virus. |
Thirty-two percent of those who have an episode of primary HSV infection will go on to experience recurrences within 15 years.29 Previous episodes of herpetic eye disease, especially if stromal and multiple, predispose to subsequent recurrences.42 Dendritic keratitis was the most common form of recurrent disease in the previously cited Rochester, Minnesota study.28 In the Moorfields Hospital study, however, most recurrences were either conjunctival or palpebral, with only 9% exhibiting dendritic ulcers.29 Recurrences tend to present in the same general location as prior ocular HSV infection.28 Therefore, the differences in the location of recurrent disease for these two studies are probably directly related to differences in the location of the primary infections. With respect to keratitis specifically, prior ulcerative keratitis does not necessarily presage subsequent epithelial recurrences. However, an occurrence of stromal keratitis increases by tenfold the risk of future stromal episodes.42
Only half of herpetic corneal ulcers will heal spontaneously within 2 weeks.16 Untreated, or with inappropriate steroid administration, herpetic epithelial dendrites are more likely to progress to larger geographic and ameboid lesions.1,14 Children appear susceptible to developing more severe HSV keratitis, including geographic ulcers.2 Repeated occurrences of ulcerative disease as well as chronic stromal keratitis can result in progressive corneal scarring, thinning, and vascularization.3,14 Ultimately, visual acuity can be affected to the point where a patient is in need of corneal transplant. Starting at 15,000 per year in 1981, the number of penetrating keratoplasties performed in the United States reached a high of 36,000 per year by 1990.43,44 In 2004, penetrating keratoplasties in the US had dipped somewhat to 32,106, alongside 51,544 total grafts worldwide.44 According to several reports covering the past 30 years or so in the US and various other developed countries, somewhere around 5% (0.6% to 10%) of corneal transplants are for scarring due to HSV.2,43,45–53 HSV keratitis, however, can go on to recur in the graft itself, resulting in scarring, graft failure, and rejection.7,8 The presence of unrecognized latent HSV in recipient corneas may elevate the risk of primary graft failure as well as late endothelial failure.54,55 Evidence for HSV-1 within donor tissue has also been found, and felt to be a potential cause for primary graft failure.56 It is clear that the ability to treat and prevent recurrences of HSV keratitis is an important public health issue as it relates to vision, conservation of valuable limited resources (such as transplant tissue), and healthcare expenses. Effective therapy is highly desirable to lessen the morbidity of the infection, and in so doing, mitigating the corneal and visual consequences.
Antiviral therapy
The antiviral agents employed against HSV have primarily been nucleoside analogs. They function by competitive inhibition, becoming incorporated into viral DNA within infected cells. Viral DNA synthesis in this manner is interrupted by the irreversible binding of viral DNA polymerase.7,57 Early generation drugs included idoxuridine, iododesoxycytidine, vidarabine, and trifluridine. They tended to have low bioavailability and measurable local toxicity.3,14,58,59 Idoxuridine, an analog of the pyrimidine thymidine, was the first effective agent, introduced in 1962. Its efficacy was limited by ocular surface toxicity and poor hydrosolubility.60 It eventually fell out of use in the early 1990s in favor of more effective and better-tolerated topical medications.5 Vidarabine, a purine analog, exhibits somewhat fewer side effects than idoxuridine, but still not-insignificant local toxicity.3,7,59 Formulated as an ointment, vidarabine is poorly soluble like idoxuridine, limiting effective corneal penetration.7,8,60 At least in part for these reasons, vidarabine is considered less preferable than trifluridine and acyclovir, and has generally fallen out of use.61 Trifluridine, a synthetic pyrimidine nucleoside, was approved by the US Food and Drug Administration (FDA) as a 1% solution for treatment of HSV keratitis in 1980.5 It is administered every 2 hours while awake, up to nine times a day. It has become the most widely used topical antiviral agent for treatment of HSV keratitis in the United States.3,14 Toxic local side effects, however, have been described as particularly severe.3,4
The aforementioned topical agents have proven to be effective in reducing the duration of infection, as well as decreasing scarring and other pathologic consequences of ulcerative HSV keratitis. At the same time, the drugs are also generally nonselective in their activity against DNA synthesis. Although they shut down viral processes, they will interrupt cellular function just as readily by being incorporated into human cellular DNA.3 In so doing, they inhibit DNA replication of both normal and viral-infected cells.4,5 Consequently, these agents have tended to exhibit cellular toxicity. Prolonged use has manifested itself in adverse side effects, mostly involving ocular surface toxicity. These effects include: epithelial keratitis, ulceration, and dysplasia; delayed wound healing; follicular and cicatricial conjunctivitis; and punctal and canalicular stenosis.5,7,8,14,60,62–64
Acyclovir is another purine nucleoside analog, but with selective inhibitory activity against HSV DNA polymerase.7,14,59 It is able to inhibit viral DNA synthesis without concomitantly interrupting cellular processes of uninfected host cells.1 In Europe, acyclovir is available as a 3% ointment. It has been demonstrated to be effective against HSV ulcerative keratitis, reducing healing time and adverse visual consequences. Local toxicity is less than that of the nonselective agents.14,60 Acyclovir is poorly soluble in water, however, requiring formulation in a polyethylene glycol base. The ointment can cause some discomfort as well as blurred vision, which in turn can affect patient compliance.1,3,6,14,65 Nevertheless, acyclovir 3% ointment came to be the first-line topical treatment for HSV epithelial keratitis in Europe and other countries outside of the US. Oral acyclovir, as well as other oral agents such as valacyclovir, appears to have similar efficacy to that of the topical form.15,16,65–69 The few studies that compared oral plus topical antiviral therapy to topical treatment alone found the combined regimen to be as efficacious as, but not more so, than topical antiviral therapy only.16,68,70 Oral acyclovir has been shown to be useful for prevention of recurrent HSV eye disease in its various manifestations.71–74 Once discontinued, however, reactivation of HSV eye disease returns to pretreatment rates, as the latent form of the virus is not eradicated by this virustatic medication.57,75
Ganciclovir
Metabolism and antiviral action
Ganciclovir, like acyclovir, is a synthetic purine nucleoside, and an analog of guanosine. Its chemical structure is 9-[[2-hydroxy-1-(hydroxymethyl)ethoxy]methyl] guanine (CAS number 82410-32-0), with empirical formula C9H13N5O4 and molecular weight 255.23.2–4,7,76 Ganciclovir is phosphorylated by viral thymidine kinases of the herpesvirus family and other viruses, and by protein kinase of CMV, into ganciclovir monophosphate.1 Within virus-infected cells, both viral and cellular thymidine kinases catalyze further phosphorylation of ganciclovir monophosphate into ganciclovir triphosphate, the active metabolite.1,3–5 Ganciclovir triphosphate accumulates in virus-infected host cells, interfering with viral replication in two ways: 1) it is directly incorporated into viral strand primer DNA, inducing DNA single- and double-strand breaks, and resulting in viral DNA chain termination;14,77 and 2) being a derivative of 2′-deoxyguanosine, it competes with deoxyguanosine triphosphate for binding to viral DNA-polymerase, interrupting new viral DNA synthesis.1,3,14,76 Ganciclovir’s potent genotoxic effects are irreversible.78 HSV-infected cells become rapidly apoptotic, resulting in cell death.77,79 Because ganciclovir is not recognized as a substrate by human thymidine kinase within healthy human cells, the active metabolite does not build up in uninfected cells.5 Consequently, while strongly inhibiting viral replication in cells infected with HSV, it does not damage DNA or interfere with DNA polymerization in healthy cells.3,57,80 The effects of ganciclovir are thus limited to HSV-infected cells, resulting in less potential host toxicity.5
Indications
Systemic ganciclovir is administered in intravenous, oral, and vitreous implant forms. It is FDA-approved for treatment of CMV retinitis in immunocompromised individuals (including those with acquired immunodeficiency syndrome), and for prevention of CMV disease in bone marrow and solid organ transplant recipients at risk for CMV disease.4,7,8 Off-label uses include prevention of recurrent CMV retinitis and treatment of CMV pneumonitis, CMV neurological disease, progressive outer retinal necrosis caused by varicella-zoster virus, and certain human herpesvirus 8 diseases.20 Ganciclovir, both systemic and topical, has also been used with some success in treatment of CMV endothelitis.81–84 It is considered to be a first-line choice of therapy for these sight- and life-threatening CMV infections.85 Ganciclovir has a broad spectrum of activity against a variety of viruses, including all human herpesviruses (including HSV-1, HSV-2, varicella-zoster virus, Epstein-Barr virus, CMV, and human herpesvirus 6) and adenovirus.1,3–5,14,65 The drug appears to have equal or greater potency against the herpesviruses, with the exception of CMV, than does acyclovir.3,78,85,86 CMV does not have an exact thymidine kinase gene homologue; instead, the CMV UL97 gene, with putative thymidine kinase activity, phosphorylates ganciclovir.87 Although it slows replication of CMV DNA, ganciclovir (unlike acyclovir) is not an absolute chain terminator in this case, and small subgenomic fragments of CMV DNA continue to be synthesized.88 Nonetheless, its superiority to acyclovir in inhibiting CMV replication lies in its tenfold greater intracellular concentration.3,89 As a virustatic agent, ganciclovir does not eradicate virus in the latent phase, and so maintenance therapy may be required to prevent recurrences.85 When administered systemically, it exhibits hematologic toxicity, although effects are usually reversible.3,7,8,85 Systemic ganciclovir has been associated with granulocytopenia, thrombocytopenia, anemia, azoospermia, and a rise in serum creatinine.89
While not available commercially, oral ganciclovir was shown in one study to be efficacious in relieving symptoms and shortening the clinical course of herpes stromal keratitis and endotheliitis. In a single-blind prospective trial carried out from 2008 to 2009 at a Fudan University hospital, Wang et al compared two therapeutic regimens involving ganciclovir for the symptomatic relief and cure of herpes stromal keratitis and corneal endotheliitis.86 They demonstrated that oral ganciclovir, when added to a regimen of ganciclovir 0.15% ophthalmic gel and fluorometholone eye drops, was found to be superior to treatment consisting of only ganciclovir gel and fluorometholone. Nevertheless, since ganciclovir is poorly absorbed in the gastrointestinal tract, its potential use as an oral agent in the future remains unclear.90
Dosage formulations
Ganciclovir is now approved as a topical antiviral agent for treatment of acute herpes simplex epithelial dendritic ulcerative keratitis, in the form of a 0.15% aqueous gel. It is marketed in Europe under the trade name Virgan® (Spectrum Théa Pharmaceuticals, Macclesfield, UK) and has been available outside of the United States since 1996. Ganciclovir gel 0.15% was more recently approved by the FDA in the United States, since September 2009, as Zirgan® (Bausch and Lomb Incorporated, Rochester, NY, USA). With a pH of 7.4, each gram of the gel contains 1.5 mg of active ganciclovir in a hydrophilic polymer base, carbomer 974P.88 Benzalkonium chloride 0.0075% is used as a preservative. Dosing schedules for both Zirgan® and Virgan® are for use in the affected eye, one drop five times per day (about every 3 hours while awake) until the corneal ulcer heals, then one drop three times a day for 7 additional days. The medication appears most effective when used early in the course of the infection.78 Patients are warned not to wear contact lenses while using ganciclovir gel for treatment of active herpes keratitis due to the potential link between herpes keratitis recurrence and contact lens use.37,76 Several clinical trials have shown ganciclovir 0.15% ophthalmic gel to be both safe and effective; the topical formulation is well tolerated, nontoxic to the ocular surface, and does not cause adverse systemic side effects.7,8,14,65,92,93
Ocular pharmacokinetics
Both acyclovir and ganciclovir topical forms demonstrate effective penetration in and through the cornea to achieve therapeutic levels in deeper structures, including the aqueous humor.7,8,59 Its hydrophilic base allows ganciclovir to be solubilized as an aqueous gel. This, in turn, enhances drug resorption, permitting equivalent therapeutic effects at far lower concentrations than that of acyclovir 3% ointment.59 The effective median dose of ganciclovir in vitro against clinical ocular isolates of herpes simplex virus is 0.23 μg/mL.14,65 A single drop of ganciclovir gel, instilled on the ocular surface, can produce tissue concentrations (Cmax [maximal concentration]) in the cornea (17 μg/g), conjunctiva (160 μg/g), aqueous humor (1 μg/g), and iris and ciliary body (4 μg/g), which surpass the effective concentrations for HSV-1 and HSV-2 for over 4 hours.91 This capacity to concentrate in ocular tissues and fluids could be related to ongoing drug absorption over time, as the gel formulation permits extended drug contact on the ocular surface.5,59,94 Indeed, ganciclovir gel has often been described as “galenic”, after the ancient physician Galen, implying a medication designed with maximal absorption properties in mind.14,59 Ganciclovir is a relatively small-sized molecule with high lipophilicity and high cellular affinity.59 Its lipophilic nature causes ganciclovir to be poorly soluble in water; this is likely the reason that, for topical use, it was not formulated as an aqueous solution.59 At the same time, however, increased lipophilicity has been shown to enhance permeability through the corneal epithelium by improving absorption into the lipoidal corneal epithelial cells.3,95 The presence of an epithelial defect enhances corneal absorption even more by eliminating one of the primary barriers to absorption (ie, the epithelium).59,96,97 Hence, one would expect better passage of topical ganciclovir through the cornea in earlier stages of an infection when the ulceration is presumably at its largest. Topical ganciclovir appears to primarily pass through the cornea by means of passive diffusion.98 This method is by no means inefficient as measurable levels of ganciclovir can be found within the anterior chamber of rabbit eyes within 5 minutes of administration.97
Preclinical studies
Preclinical studies have examined topical ganciclovir’s effects on animal models, particularly rabbit corneas, and demonstrated efficacy in decreasing the severity of herpes keratitis.59,96,99 Castela et al examined the effects of ganciclovir gel 0.2%, 0.0125%, and 0.05% in comparison with acyclovir 3% ointment in a rabbit model of HSV keratitis.4,59 Corneal ulcer size, clouding, and vascularization were all significantly reduced in all drug-treated groups compared with placebo (P<0.05). Acyclovir 3% ointment was not significantly different than ganciclovir 0.05% gel in clinical efficacy, but was significantly better than the 0.2% and 0.0125% gels. HSV-1 was cultured from pooled tear samples to determine duration of infectivity. Viral shedding was eliminated after 12 days with the 0.2% and 0.05% ganciclovir gels – faster than the 14 days required using placebo, but not as rapidly as for the group receiving acyclovir ointment (10 days). The differences in viral eradication between the ganciclovir 0.05% gel and the acyclovir 3% ointment groups, however, were not statistically significant. Corneal penetration was good: the mean corneal concentrations were high with the 0.2%, 0.05%, and 0.0125% gels being nine, 1.5, and three times higher, respectively, than the effective median dose (0.20–32 μg/mL) of the in vitro HSV strain. Castela et al discovered, in their study, mild to very high levels of ganciclovir in several cellular tissues: cornea and chorio–retina for all three gel concentrations, and iris for all but the 0.0125% formulation.59 By contrast, the mean concentrations of ganciclovir in ophthalmic fluids and plasma were generally very low. This difference might be explained by ganciclovir’s comparatively poor water solubility. There was, nevertheless, still a detectable presence of therapeutic levels of ganciclovir in the aqueous humor 4 hours after the last topical administration of the 0.2% gel. The authors postulated that this could be related to slow diffusion of the drug into the aqueous humor from the cornea. No ocular or systemic toxicity was expected or noted in the study.59
There is some degree of dose–response relationship in this study. Rabbits exhibited a faster ulcer healing time with ganciclovir 0.05% than with the other two concentrations. Only the 0.05% gel was equivalent to acyclovir 3% gel in efficacy. The 0.2% gel achieved the higher drug levels in cornea, iris, and aqueous humor compared to the less concentrated formulations. Paradoxically, the 0.0125% gel achieved somewhat higher corneal concentrations than the 0.05% gel; however, this did not seem to translate into faster clinical healing or duration of viral shedding.59
Trousdale et al demonstrated the clinical efficacy of ganciclovir ointment prepared in different concentrations.96 They treated experimental HSV-1 keratitis in rabbit eyes with ganciclovir 1%, ganciclovir 0.1%, acyclovir 3%, idoxuridine 1%, and placebo. All antiviral groups were superior to placebo; the two concentrations of ganciclovir showed no difference and were, along with acyclovir, superior to idoxuridine. In another animal investigation, Shiota et al found that ganciclovir 0.3%, prepared as an ointment, was more effective than acyclovir 3% and idoxuridine 0.5% ointments after 4 days of therapeutic use against herpetic ulcers in rabbit eyes.100 The results of these different preclinical studies suggested that the optimal concentration for topical ganciclovir was likely to be greater than 0.0125% but less than 1%.
Clinical studies
Phase I studies
During Phase I investigations, ganciclovir gel 0.15% was administered to healthy human volunteers. In one randomized double-masked study, ten volunteers received ganciclovir gel 0.15% in one eye and its vehicle gel in the other eye five times per day for 7 days.3,4,94,101 Eyes were examined before, during, and after the treatment period; examination findings were unchanged between visits. The gels were generally well tolerated, producing no side effects deemed to be clinically significant by either subjects or investigators.4,94 Blurred vision, however, was noted by eighty percent of the participants after topical administration of the gels.94 In a second masked trial, six male subjects were dosed with ganciclovir gel 0.15% in each eye every 3 hours over a 12 hour study period, totalling four instillations.3,4,94,102 This represented about 0.04% and 0.1%, respectively, of the typical daily oral and intravenous doses of ganciclovir, assuming full systemic absorption of the gel.3 Tear samples were collected using Schirmer’s strips, and their ganciclovir concentrations assayed. Measurements were taken initially to obtain control levels, and then 2 hours, 45 minutes following each instillation of ganciclovir gel. Mean tear ganciclovir levels among study participants varied from 0.92 to 6.86 μg/mL, exceeding the mean effective concentration of HSV-1 by at least fivefold.4,94 Systemic levels of ganciclovir (11.5±3.7 ng/mL) were negligible.3,4,101,102 Apart from irritation from the paper strips, patients did not experience any additional discomfort from the topical medication.4,102
Phase II and III studies
There have been four key multinational multicenter controlled randomized single-masked open-label studies – three Phase IIb and one Phase III – comparing ganciclovir 0.15% gel to acyclovir 3% ointment, which is considered the gold standard internationally for topical treatment of HSV epithelial keratitis.3,5,14,65,92,93 Patients with herpetic ulcers, designated as dendritic or geographic, with no antiviral therapy in the previous 14 days, were eligible for inclusion; those with severe stromal disease, keratouveitis, previous keratoplasty, and immune deficiency were excluded. Phase II subjects were ≥2 years of age, while Phase III participants were age 18 and above.1 Ganciclovir gel was demonstrated to be, at a minimum, as effective as acyclovir ointment, actually healing ulcers more rapidly and at a higher rate. The 0.15% gel also proved to have better tolerability, causing fewer treatment-related adverse side effects than the 3% ointment.14,103
Phase II studies examined the optimal concentration and dosing schedule for subjects ≥2 years old with active herpes epithelial keratitis, considering efficacy as well as adverse effects.1 Topical ganciclovir gel 0.15% was compared against topical acyclovir ointment 3%. The clinical trials lasted 15 to 25 months and enrolled 213 total patients, with all studies being completed by May 1992.3 Study one was conducted in Africa, involving 67 eyes of 66 patients, and study two was from Europe, with 37 participants from four study centers in France, Switzerland, and England.3,14,92 A third Phase II study (study three) from Pakistan compared ganciclovir and acyclovir on 36 and 38 subjects, respectively.5,93 For studies one and three, there was also a ganciclovir 0.05% treatment arm.5,14,93 Study four was the largest of the clinical studies, involving 164 subjects ≥18 years of age with herpes keratitis from 28 study centers in France, England, Ireland, Mali, Tunisia, and Madagascar.1,65 Patients were followed for 2 years between September 1992 and September 1994 in this Phase III trial.57,65,104 The four studies are summarized in Table 1.
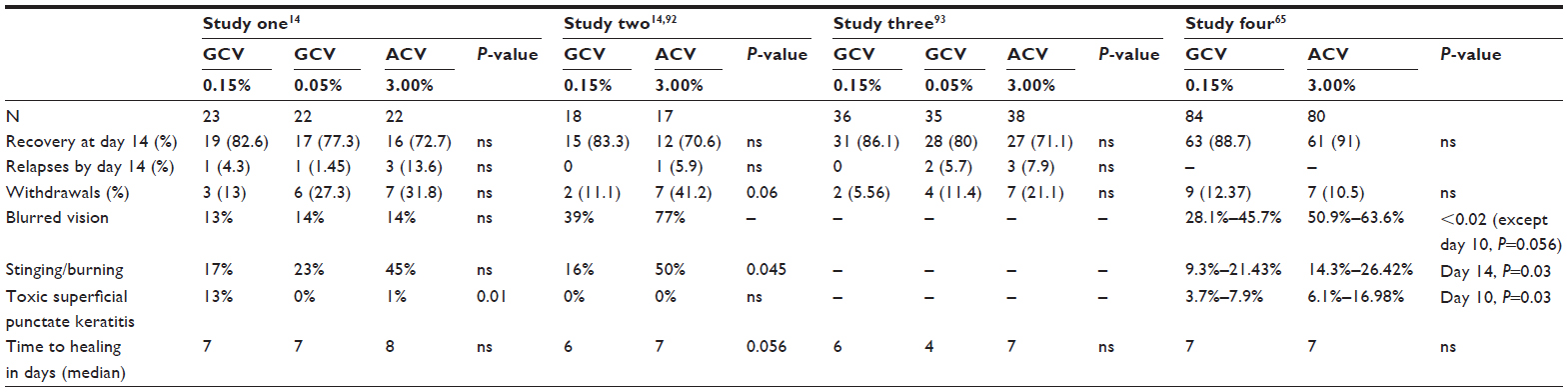 | Table 1 Phase II and III clinical studies |
In a retrospective pooled analysis of the three Phase IIb clinical trials, ganciclovir 0.15% gel was found to be noninferior to acyclovir 3% ointment in healing dendritic HSV ulcers.1,11 Median healing time for ulcers was 6–10 days.1 Seventy-two percent of patients who were administered ganciclovir gel demonstrated clinical resolution at day 7 in comparison to 69% of those treated with acyclovir ointment (difference 2.5%; 95% confidence interval –15.6% to 20.9% [numbers derived from pooled data]).11 In addition, 81% of dendritic ulcers resolved at day 10 and 89% at day 14. Median time to recovery in the three Phase II studies (pooled) was 6–7 days for ganciclovir gel and 7–8 days for acyclovir ointment. In the per protocol population of study two, the median time to healing for the ganciclovir group (6 days) was somewhat less than, but not significantly different from, the median healing time for the acyclovir group (7 days) (P=0.056).4,92 Recovery rates at 14 days in the same cohort were higher for topical ganciclovir (83.3%) than for acyclovir ointment (70.6%), but again without achieving statistical significance.4,14,92 Sahin and Hamrah have additionally pooled the data from the three Phase II studies, looking specifically at the intent-to-treat study participants. The authors calculated a statistically significant difference in proportion of ulcers resolved at trial endpoint after ganciclovir gel treatment (85%) compared to treatment with acyclovir ointment (71%) (P=0.04).3,4
The Phase III multicenter randomized prospective study compared ganciclovir 0.15% gel and acyclovir 3% ointment for the treatment of herpes simplex epithelial keratitis, both dendritic and geographic.65 Dendritic corneal ulcerations were of less than 7 days’ duration. Patients were randomized to receive ganciclovir gel or acyclovir ointment, with each drug being administered five times per day until healing of the ulcer, followed by three times daily for an additional 3 days. The two topical antiviral medications demonstrated comparable efficacy with no significant adverse effects. Following 7 days of treatment in the Phase III trial, 77% of patients on ganciclovir gel achieved clinical resolution of dendritic ulcers, versus 72% of those taking acyclovir 3% ointment (difference 5.8%; 95% confidence interval -9.6% to 18.3%); after 14 days, healing rates increased to 86% and 89%, respectively.1,5,11,76 These differences in healing time between the two groups were not statistically significant. Overall recovery rate over the entire duration of the Phase III treatment trial was 89% for recipients of ganciclovir gel and 91% for those receiving acyclovir ointment.1,5,65 Median time to recovery from dendritic ulcers was 7 days for both the ganciclovir gel and acyclovir ointment treatment groups, as well as for geographic ulcers treated with acyclovir. Although median healing time was 9 days for geographic ulcers treated with ganciclovir gel, there were overall too few patients with geographic ulcers to derive meaningful statistical analysis.4 As a result, since ganciclovir gel could not be demonstrated with statistical certainty to be noninferior to acyclovir ointment for treatment of geographic herpetic ulcers, ganciclovir 0.15% gel has not been approved in the US for this indication.1 For the treatment of dendritic ulcers, however, ganciclovir 0.15% gel was established to be noninferior to acyclovir 3% ointment. When data is further pooled from all four major studies, including the Phase III trial, ganciclovir 0.15% gel continues to prove at least as effective as acyclovir 3% ointment in the treatment of herpes simplex dendritic epithelial keratitis.1,3,4
The Phase II and III studies were not originally designed to ascertain noninferiority; noninferiority and comparable efficacy were confirmed through subsequent retrospective analysis.1,57 The trials initially held time-to-healing as the primary endpoint, and reported on efficacy data for day 14 of treatment. Treatment continued for a maximum period of 21 days for dendritic ulcers, and 35 days for geographic ones. For FDA approval, however, the primary endpoint needed to be redefined as the proportion of patients exhibiting clinical healing by day 7.1,57 The differences in median healing time for dendritic ulcers were not statistically significant for the different topical treatments in any of the four major studies.1,57
Investigators kept track of relapses occurring by day 14. Relapses developed in 0%–4% of ganciclovir-treated patients in the four clinical studies, and in 0%–14% of patients who received acyclovir. This actually amounted to only zero to two patients who relapsed for either drug in any one of the individual studies. Because of this small number of actual relapses, the percentage differences were not statistically significant.1,4,5,14,57
Tolerability and adverse effects
The most common adverse and toxic side effects, as determined from pooled data from all four major studies, were blurred vision (ganciclovir 57.8%, acyclovir 71.3%), eye irritation (ganciclovir 25.6%, acyclovir 46.2%), punctate keratitis (ganciclovir 8.8%, acyclovir 16%), and conjunctival hyperemia (ganciclovir 5.6%, acyclovir 5%).5 Bausch and Lomb Incorporated, in their full prescribing information for Zirgan® 0.15% ophthalmic gel, reported similar common side effects, with just slightly different percentages: blurred vision (60%), eye irritation (20%), punctate keratitis (5%), and conjunctival hyperemia (5%).76 Ganciclovir 0.15% gel was generally better tolerated than acyclovir 3% ointment, virtually across the board, except for conjunctival hyperemia. There were fewer complaints of blurred vision, and discomfort such as burning and stinging in the ganciclovir group than in the acyclovir group.4 Systemic absorption was low, and there were no adverse hematologic effects.14 No adverse events were categorized as serious.1,65
Blurred vision and irritation
Eight out of the 10 study subjects in the first Phase I investigation reported blurred vision after ganciclovir gel adminisstration.94 In each of the four subsequent key clinical studies, fewer patients reported blurred vision or eye irritation from ganciclovir gel than from acyclovir ointment.3,5 In Phase II, study two, the proportion of patients experiencing blurred vision after 1 week of therapy with ganciclovir gel (58%) was nearly one-third less than the proportion of patients with blurring after acyclovir ointment (89%); when it occurred, blurred vision also tended to last longer (>5 minutes) with acyclovir ointment than with ganciclovir gel.3,14,57 At the same time, incidence of burning or stinging was nearly reduced threefold in ganciclovir (17%) versus acyclovir (50%).14,57 The Phase III trial, study four, found incidence of visual disturbances to be significantly less with ganciclovir gel than with acyclovir ointment on day 7 (P<0.05).57,65,104 Furthermore there were significantly fewer complaints of stinging, tingling, and burning among ganciclovir recipients compared to those who received acyclovir ointment (P<0.05).1,3,57 Hoh et al from England, Ireland, and France, in their portion of the Phase III report, indicated that 83.2% of subjects taking ganciclovir gel and 86.8% of those on acyclovir ointment noted blurred vision, ranging from mild to severe.65 The visual disturbances lasted longer after topical instillation of acyclovir than ganciclovir, persisting an average of 32.9 and 22 minutes, respectively. The tonicity and pH of ganciclovir 0.15% gel are physiologic, a factor that likely plays at least a part in its overall tolerability.59 Another aspect is its aqueous formulation, which appears for most patients to be preferable to, and more comfortable to administer than, an ointment-based medication.3,7,8,14,57
Surface toxicity
In study one, a slightly higher percentage of patients on ganciclovir (13%) than on acyclovir (9%) exhibited toxic superficial punctate keratopathy (SPK) by day 14.5,14 Conversely in study four, toxic SPK was twice as prevalent in the acyclovir 3% ointment group than in the ganciclovir 0.15% gel group (P=0.03 at day 10) during treatment of dendritic ulcers.65 No punctate keratitis was seen at all among the 13 patients with geographic ulcers who were placed on ganciclovir 0.15% gel during the fourth major clinical trial; by contrast, in the same trial, 15%–43% of 13 geographic ulcer patients exhibited SPK at various stages of follow-up during their treatment with acyclovir 3% ointment.3,5,57,65,104 Punctate keratitis also remained nearly twice as prevalent among patients administered topical acyclovir compared to topical ganciclovir when data from all of the four pivotal studies were pooled.5 Ching et al reviewed 88 trials of topical antiviral medications and found that 40 of them had data about adverse reactions. The median percentage of eyes exhibiting superficial punctate keratopathy for the following specific antivirals was: acyclovir, 10%; ganciclovir, 4%; trifluridine, 4%; and brivudine, 0%.16
As with all topical drugs, use of ganciclovir gel conceivably carries a risk of local hypersensitivity reactions. Dermatological side effects have been noted with other antivirals; however, contact hypersensitivity of the skin or conjunctiva was not observed in any of the clinical studies of ganciclovir gel.14,16,65,90,92,93,105 Only one case study reports an occurrence of generalized cutaneous rash and splinter hemorrhages, and that was from systemic ganciclovir use.106
Subjective tolerability
In studies one, two, and four, both patients and investigators were asked to subjectively rate the local tolerability of administered antiviral medications.3,14,65,92 Seventy-five point four percent of subjects rated the tolerability of ganciclovir 0.15% gel as excellent, compared to 40.4% of those who received acyclovir 3% ointment. Investigators similarly rated ganciclovir 0.15% gel as having excellent tolerability more frequently than for acyclovir 3% gel: 81.8% versus 44.7%, respectively. The difference in patient ratings in study two, as well as both patient and investigator ratings in study four, were statistically significant (P<0.001).5,57,65,104 Based on these results, the major advantage of ganciclovir gel over acyclovir ointment appears to be its tolerability, with less blurred vision and ocular irritation. Patient withdrawals due to disease exacerbation, poor tolerance, or other complications were fewer among those given ganciclovir (11.2%) than those treated with acyclovir ointment (19.7%) (pooled data for the four major studies).4,5
Ganciclovir compared to other antivirals
Various topical antiviral agents have generally demonstrated similar efficacy in the treatment of HSV epithelial keratitis. In 52 studies reviewed for the Preferred Practice Pattern® monograph published by the American Academy of Ophthalmology, trifluridine, acyclovir, brivudine, and ganciclovir were all similar, helping 90% of total corneas to heal within 2 weeks.16 Wilhelmus conducted a review of literature from 1950 to 2010 encompassing 106 comparative trials and 5,872 patients.61 Acyclovir, ganciclovir, vidarabine, brivudine, and trifluridine, on meta-analysis, all appeared superior to idoxuridine; additionally, trifluridine and acyclovir, while themselves equally effective, were both superior to vidarabine; brivudine and ganciclovir were at least as effective as acyclovir and trifluridine.61
Adverse local reactions have been frequently observed to varying degrees after use of any and all of the topical antiviral eyedrops. These side effects include stinging upon instillation, allergic blepharoconjunctivitis, superficial keratopathy, and toxoallergic follicular conjunctivitis.16 Oral acyclovir appears to be equally effective as the topical antivirals, but without the local side effects.61
Topical trifluridine 1% has been hitherto the only topical antiviral agent commercially available for use against dendritic herpes simplex keratitis in the United States. Despite this fact, ganciclovir gel 0.15% has not been directly compared to trifluridine 1% in human studies. At the 2008 Annual Meeting of the Association for Research in Vision and Ophthalmology, Varnell and Kaufman reported on their study comparing ganciclovir ophthalmic gel 0.15% and trifluridine ophthalmic solution 1% in the treatment of experimental herpetic keratitis.107 Rabbits were infected with McRae strain of HSV-1 and then treated with one of the two antivirals. The two drugs demonstrated clinical equivalency. In a separate masked trial focused on toxicity, uninfected rabbits with intact corneas and corneal epithelial defects were administered either topical trifluridine drops or ganciclovir gel.108 Those with intact epithelium or small epithelial defects did not demonstrate toxicity after 14 days’ treatment. However, rabbits with total epithelial defects exhibited more conjunctival inflammation and corneal edema after 20 days of treatment with trifluridine drops than after ganciclovir gel (P<0.0001).5,108 This finding suggests that topical ganciclovir may be slightly less toxic than trifluridine, especially during more extended therapy.103 Gordon et al looked at the antiherpetic effects of ganciclovir, the cyclic ganciclovir derivative 2′-nor-cGMP, and trifluridine in BALB/c mice inoculated with HSV-1.109 The two forms of ganciclovir were found to be significantly more effective than trifluridine in reducing ocular HSV titers and improving epithelial keratitis in the mice (P=0.0001). With respect to reducing stromal keratitis, all three drugs were clinically equivalent, and also significantly more effective than balanced salt solution. It is important to note that no trials have been performed to directly compare these effects in a clinical setting.
Antiviral resistance
Most HSV isolates have been found to be sensitive to acyclovir and ganciclovir while exhibiting more variable sensitivity to idoxuridine and vidarabine.110 As has been observed with antimicrobials, the effectiveness of antiviral agents may be limited by emerging pathogen resistance.14,111–113 Resistance to acyclovir has already been observed.114 Since it has a similar structure and mechanism of action to acyclovir, ganciclovir might be expected to face viral cross-resistance.6 HSV resistance to nucleoside analogues such as ganciclovir, however, is not extremely common, with a relatively low 0.1%–0.7% prevalence among immunocompetent individuals.1,5,115 It turns out that viruses that become resistant to acyclovir may remain sensitive to ganciclovir.78 The molecular mechanisms that underlie ganciclovir activity – namely, the appropriation of the virus’ own thymidine kinase activity – hinder the ready development of viral resistance.5 Nevertheless, resistance may be conferred by mutations in viral thymidine kinase that render the virus unable to phosphorylate the nucleoside analog drugs.78,89,116 Hlinomazová et al found 14% of patients with polymerase chain reaction-proven HSV-1 keratitis and keratouveitis to be clinically acyclovir-resistant. Patients not responding to acyclovir were all subsequently treated successfully with topical ganciclovir gel 0.15%.6 Duan et al examined 173 isolates from patients with HSV-1 keratitis. Eleven isolates (6.4%) were acyclovir resistant in vitro, and nine of the eleven were refractory to acyclovir treatment. Five of eleven were additionally cross resistant to ganciclovir.116 Drug-resistant herpes simplex viruses that enter latency may retain resistance after subsequent reactivation.117 Host immunologic deficiency appears to promote HSV drug-resistance: 4% to 7% of HSV isolates taken from immunocompromised patients have been found to be resistant to nucleoside analogs such as acyclovir.1,115,118 HSV cross-resistance to acyclovir, ganciclovir, and idoxuridine may also be observed in patients with atopic disease or in those who have taken topical corticosteroids.119
Post-marketing surveys
In Phase IV post-marketing surveys of Zirgan conducted by Bausch and Lomb Incorporated, there have been occasional reports of eye irritation and injection, but they have been rare.5 The same evaluations, however, have identified no unlabeled or unexpected adverse events that would be considered serious.120 Often, symptoms of minor eye burning, tingling, and visual blurring were not severe enough to require discontinuation of the medication.91 Seventy-five percent of patients queried after a full course of treatment for herpes simplex dendritic keratitis reported excellent, 22% good, and only 3% poor tolerability of the ganciclovir 0.15% gel.65
Systemic toxicity
Systemic absorption of topical ganciclovir has been measured and found to be minimal.5,59 Under the standard initial dosing regimen for HSV dendritic keratitis of one drop five times per day, the estimated maximum daily dose of ganciclovir 0.15% gel is 0.375 mg. Even assuming complete systemic absorption, this represents only about 0.04% of the maintenance dose for oral valganciclovir (900 mg/day) and just 1% of the daily dose for intravenous ganciclovir (5 mg/kg/day, assuming 75 kg weight).76 When patients with ulcerative herpes simplex keratitis instilled ganciclovir gel 0.15% five times daily for 11–15 days, plasma levels averaged 0.013 μg/mL. That level is 640-times lower than the Cmax (8.0 μg/mL) achieved after administration of 5 mg/kg of ganciclovir intravenously.91 Because topical ganciclovir is absorbed systemically in such small amounts, its topical use would not be expected to produce systemic side effects.7,59,79 Consistent with this expectation, none of the known hematological side effects of systemic ganciclovir have been observed with use of the gel formulation.7 Drugs that inhibit rapidly replicating cell populations such as skin, bone marrow, and gastrointestinal mucosa may demonstrate additive toxicity when administered along with systemic ganciclovir. Interactions of this kind have not been documented in association with topical ganciclovir. Nevertheless, warnings remain in place for prescribers to take caution and to only use these drugs concomitantly when the benefits are felt to outweigh potential risks.91
Ganciclovir gel is indicated for topical use only.76 Accidental oral overdose of ganciclovir gel has not been reported. Spectrum Théa Pharmaceuticals, the manufacturer of Virgan®, believes that, even if inadvertent ingestion were to occur, significant systemic toxicity would be highly improbable.91 There is only 7.5 mg of ganciclovir in a typical 5 g tube of the medication. The oral bioavailability of ganciclovir gel when taken with food is only 6%. By contrast, the daily intravenous therapeutic dose of ganciclovir is 500–1,000 mg. The drug is primarily excreted in unchanged form through glomerular filtration, with a systemic clearance rate of 3.64 mL/minute/kg.91
Pediatric use
Oral acyclovir may be the preferred antiviral medication for therapy of HSV keratitis in the pediatric age group; it is especially convenient in younger children or infants since it can be administered as a liquid suspension.121,122 Oral valacyclovir or famciclovir are acceptable alternatives in older children.121 The pediatric use of topical trifluridine, vidarabine, and acyclovir ointment has also been described.121,123,124 There have been no reports to date on the use of topical ganciclovir specifically in children, although Phase II studies included children ≥2 years of age. Ganciclovir gel 0.15% has not been tested in pediatric patients under 2 years of age; its utility and safety in that age group has therefore not been established.76
Safety in pregnancy and nursing; teratogenicity; effects on fertility
Similarly, ganciclovir gel’s safety for pregnant women and nursing mothers is unknown. For this reason it falls under Pregnancy Category C. Observations of adverse effects in animals have included carcinogenesis, mutagenesis, suppression of fertility, and maternal/fetal toxicity. Rabbits and mice were intravenously administered ganciclovir up to 17,000× the daily human ocular dose of 6.25 μg/kg/day. The drug in these high doses caused maternal toxicity, teratogenic effects, fetal growth retardation, and embryo death in rabbits. In mice, maternal toxicity, including decreased mating behavior and fertility, fetal toxicity, teratogenesis, and embryo lethality, were similarly observed. Oral and intravenous administration of ganciclovir to male mice and dogs, amounting to 30–1,600× the human daily ocular dose, also caused decreased fertility due to hypospermatogenesis.76,91 Spermatogenesis is inhibited reversibly at lower doses of systemic ganciclovir, but irreversibly using higher doses. Similarly, female infertility may also be permanent. In vivo tests were conducted, exposing mouse cells to ganciclovir, at levels exceeding the plasma levels of patients on ganciclovir gel treatment by 24,000× and 80,000×. Genetic point mutations and chromosomal damage were produced under these conditions.91
The safety of ganciclovir gel for use in nursing mothers is unknown; there is no current information on whether the drug might be absorbed from ocular tissues in sufficient amounts to be detectable in breast milk. However, in a precautionary note, ganciclovir has been found to be secreted in the milk of laboratory animals; adverse effects were subsequently observed in the offspring.3
Carcinogenesis
Ganciclovir was carcinogenic to mice at daily oral doses of 20 and 1,000 mg/kg/day – approximately 3,000× and 160,000×, respectively, the human ocular dose of 6.25 μg/kg/day. No carcinogenic effects, however, were observed in mice that ingested 1 mg/kg/day, representing 160× the daily human ocular dose. There was a small increase in tumor occurrence when plasma levels of ganciclovir in these animals reached about 50× the levels measured in humans after topical ganciclovir treatment.11,91
Based on this preclinical safety data, the drug is not recommended in pregnant and lactating females, and should be considered potentially carcinogenic and teratogenic.91
Future applications and directions
HSV ocular disease
Ganciclovir gel may have several future applications beyond its current indication. Currently, ganciclovir ophthalmic gel 0.15% is not approved for use in the US in patients with geographic ulcers as a result of insufficient data to establish noninferiority to acyclovir.1,4 Further delineating its effectiveness against geographic ulcers might be a logical next step.
The third Herpetic Eye Disease Study Group study demonstrated a trend toward oral acyclovir being beneficial for herpetic iridocyclitis, but numbers were insufficient to achieve statistical significance.125 There may be value in examining whether topical ganciclovir might also be useful in the management and treatment of this common manifestation of ocular herpes simplex. After topical administration, ganciclovir appears to reach therapeutic levels not only in the cornea but also the aqueous humor, although at lower concentrations in the latter location.3,7,8,57,65 Initial studies of topical ganciclovir in rabbit eyes inoculated with HSV have demonstrated improvement of not only epithelial ulceration, but also of conjunctivitis, iritis, and corneal clouding.96 It is unknown, of course, whether iridocyclitis would be treated with a similar dosing regimen as that used for HSV epithelial keratitis; higher doses of topical ganciclovir may be required.59
In the second Herpetic Eye Disease Study, the question of oral acyclovir’s usefulness against necrotizing HSV keratitis was left unanswered due to insufficient numbers of patients with that condition recruited into the study.67 If a study could recruit enough patients to achieve sufficient statistical power, it might answer whether antivirals such as topical ganciclovir are helpful against this uncommon form of herpes keratitis. In the meantime, it is more likely that information will trickle out over time through anecdotal reports.
Ganciclovir gel appears to have some capability to protect against recurrent herpes ulcerative keratitis, including after penetrating keratoplasty.7,8 Hlinomazová et al observed that, in patients with acyclovir-resistant HSV-1 keratitis and keratouveitis, the average relapse rate decreased from four to less than one per 12 months following a single 4-week period of ganciclovir gel therapy.6 Ganciclovir ointment, used five times per day for 2 days, even at a concentration of just 0.03%, was effective in preventing HSV epithelial lesions in rabbit corneas.100 Tabbara reported on 16 consecutive patients with history of recurrent herpetic keratitis who had undergone corneal transplantation due to ocular sequelae of the disease. In an open nonrandomized study, the patients applied ganciclovir 0.15% gel four times daily in the first week after penetrating keratoplasty, and then two times each day for a period of 1 year. Long term prophylaxis with topical ganciclovir gel afforded protection against recurrence of HSV keratitis in these subjects.7,8 Currently, oral acyclovir is the only antiviral medication that has been demonstrated to reduce the risk of recurrent HSV eye disease.71 Ganciclovir gel may hold some potential as an alternative for HSV prophylaxis. The exact clinical setting, along with dosing frequency and length of treatment, still require further elucidation.4,7,8
Adenoviral conjunctivitis
Some investigators have demonstrated evidence that ganciclovir gel may be useful against adenovirus – another DNA virus.4,5,103,126–128 Epidemic keratoconjunctivitis (EKC) due to adenovirus is a significant public health nuisance that accounts for countless days lost from work and school, significant patient discomfort and inconvenience, and even long term ocular consequences, such as chronic keratitis, corneal scarring with decreased vision, and conjunctival scarring. Furthermore, 4.3% of patients with EKC can be coinfected with HSV-1;129 15.2% of patients with HSV-1 infection may have coincident adenovirus present.6 In vitro, ganciclovir inhibits adenoviral replication, including that of serotypes 8 and 19 – the most commonly encountered serotypes in EKC.91 Trousdale et al, in studies of cotton rat eyes inoculated with adenovirus, found that topical ganciclovir, in a higher 3% dose, seemed to reduce incidence, titer, and duration of viral shedding.130 Epstein et al examined the anti-adenovirus activity of ganciclovir 0.15% gel in a rabbit model. They found that active virions were cleared significantly faster in rabbits’ eyes that received the antiviral gel than in control eyes that did not receive the active agent. However, symptomatic improvement was not found to be statistically significant.128
Outside of anecdotal reports, there have been a couple of small studies that have looked at the usefulness of ganciclovir gel for clinical EKC in humans. Vérin et al treated 36 patients at the onset of culture-proven adenovirus type 8 conjunctivitis with ganciclovir 0.15% gel four times a day. Ocular discomfort was reportedly relieved in 1 week, and no patients went on to develop keratitis. The investigators emphasized the importance of initiating therapy as early as possible in the clinical course.131
Tabbara and Jarade conducted an investigation on 18 study patients with adenoviral keratoconjunctivitis. Subjects were randomized to receive either ganciclovir 0.15% gel or artificial tears four times per day. Mean recovery time for the ganciclovir gel group was 7.7 days compared to a mean of 18.5 days for the control group. Only two patients given ganciclovir developed subepithelial opacities, while seven of nine patients developed them using artificial tears. The difference was statistically significant (P<0.05). The authors concluded that ganciclovir 0.15% gel appears to be a safe and effective treatment for adenoviral keratoconjunctivitis.126
Yabiku et al conducted a double-blind prospective trial to evaluate the efficacy and toxicity of ganciclovir 0.15% gel in the treatment of adenoviral conjunctivitis. Thirty-three patients with clinical adenovirus conjunctivitis were divided into ganciclovir-gel treatment and artificial-tear control groups. Patients in the treatment group experienced a statistically significant improvement of pain, itching, and photophobia symptoms during the 10 day course of their therapy. There were some trends toward both better and faster improvement of signs and symptoms in the ganciclovir group compared to controls (P=0.26). There was also a trend toward less household transmission in the ganciclovir-treated group (P=0.16). None of these trends, though, was statistically significant. Lastly, ocular complications after conjunctivitis were compared and found not to be significantly different between the two groups.127
As of this writing, there are two ongoing trials assessing the efficacy of ganciclovir gel in the treatment of adenovirus conjunctivitis (ClinicalTrials.gov identification: NCT01533480132 and NCT01600365133).
Other herpesvirus eye diseases
Three cases of superficial and epithelial CMV keratitis have been reported: 1) in a patient who received a cardiac transplant; 2) in a patient after penetrating keratoplasty; and 3) spontaneous occurrence in a patient with AIDS.134–136 Excision of the diseased corneal button was reported to be curative in the patient who had acquired CMV keratitis after the keratoplasty.135 In the patient with AIDS, antiviral therapy with oral acyclovir, oral famciclovir, topical foscarnet, topical trifluridine, and topical acyclovir were all ineffective; however, the patient expired before additional treatment options could be explored.136 As noted previously in this review, some patients with CMV endotheliitis have responded to topical ganciclovir therapy.81,83 It is certainly conceivable that the antiviral gel might also have potential for use against the more superficial form of CMV keratitis.
Aggarwal et al recently reported on four immunocompromised patients with herpes zoster ophthalmicus-related pseudodendrites, unresponsive to oral valacyclovir. Each patient was administered ganciclovir 0.15% gel five times per day, and each had successful healing of their corneal lesions within 7 days. The gel drops were tapered to twice a day after the patients showed improvement; total duration of ganciclovir therapy ranged from 1 week to 2 months. In three of the four patients, topical prednisolone 1% was used concomitantly alongside ganciclovir gel. Visual acuity as well as corneal sensation improved in three out of the four patients.137
Antitumor effects
Finally, ganciclovir may have potential as an antitumor drug. While ganciclovir cannot be phosphorylated by healthy mammalian cells, it can be phosphorylated by murine cells that contain the gene for herpes simplex thymidine kinase.89 These transformed cells are easily killed by ganciclovir.138 A similar inhibitory effect by ganciclovir is seen in murine melanoma cells transfected with the herpes simplex thymidine kinase gene.138,139 If tumor cells can be selectively transformed with a herpes simplex thymidine kinase gene, they may become susceptible to ganciclovir’s effects on their DNA replication.89 This theory has already been shown to have clinical promise in the treatment of pediatric retinoblastoma patients with vitreous seeds. Eight patients had resolution or reduction of vitreous seeds after suicide gene therapy involving intravitreal injection of adenoviral vector containing herpes thymidine kinase gene, followed by administration of ganciclovir.140 It is possible that topical ganciclovir might have potential to similarly inhibit neoplastic conjunctival and ocular surface cells, if gene therapy technology could be developed to deliver viral thymidine kinase gene into those cells. Topical drugs such as interferon alpha 2b, mitomycin C, and retinoic acid have already been used as both primary and adjuvant therapy for treatment of ocular surface squamous neoplasia, including conjunctival/corneal intraepithelial neoplasms.141–143 These agents have also been shown to have antitumor activity against conjunctival melanoma, as well as primary acquired melanosis with atypia.144–146 We are not aware of research being presently conducted to examine whether topical ganciclovir gel might play any similar role against ocular surface neoplasms.
Conclusion
Based on safety, efficacy, and tolerability, ganciclovir gel 0.15% should now be considered a front-line topical antiviral drug for the treatment of dendritic herpes simplex epithelial keratitis.4,57,147 The gel poses less toxicity and requires a simpler dosing regimen than one of the main topical alternatives: trifluridine.14,61,65,92,93 Additionally, the American Academy of Ophthalmology concluded, in their Preferred Practice Pattern® monograph on HSV epithelial keratitis, that the use of ganciclovir was associated with a better outcome overall than acyclovir topical ointment, despite similar healing rates found at 7 days.16 This assessment is likely more related to ganciclovir gel’s favorable side effect and tolerability profile. The actual clinical efficacy of the various current antiviral choices have not been shown to be significantly different. As a result, the cost of treatment may turn out, more often than not, to be the deciding factor in which therapeutic option to choose. At a representative local pharmacy near our institution in Stony Brook, New York, the recent costs of a 2 week treatment course for the three drugs – Zirgan® 0.15% gel (1× 5 g tube), oral acyclovir (70× 400 mg tablets), and generic trifluridine 1% eye drops (1× 8 mL bottle) – were $273.62, $41.88, and $164.46, respectively (Centereach Walmart Store #2286, telephone communication, Jan, 2014). Prices may vary due to insurance policies and pharmacy location. The average wholesale prices for the three are $283.04, $216.97 (per 100 tablets), and $178.28, respectively. According to Bausch and Lomb Incorporated (HH DeCory, written communication, Jan, 2014), the wholesale acquisition cost for Zirgan® 0.15% gel is $235.87.
There exist several potential topics of interest for future examination and research. These include ganciclovir gel’s usefulness against HSV geographic ulcers, necrotizing keratitis, and iridocyclitis. Additionally there may be possible therapeutic applications for topical ganciclovir adenoviral keratoconjunctivitis, CMV keratitis including endotheliitis, and herpes zoster ophthalmicus pseudodendritic keratitis. Another intriguing question that may merit further investigation is whether ganciclovir gel may play any adjunctive role in the treatment of certain ocular surface tumors. The full spectrum of clinical applications for this newest of approved topical antiviral agents, therefore, remains to be determined.
Disclosure
The authors report no conflicts of interest in this work.
References
Croxtall JD. Ganciclovir ophthalmic gel 0.15%: in acute herpetic keratitis (dendritic ulcers). Drugs. 2011;71(5):603–610. | |
Liesegang TJ. Herpes simplex virus epidemiology and ocular importance. Cornea. 2001;20(1):1–13. | |
Sahin A, Hamrah P. Acute Herpetic Keratitis: What is the Role for Ganciclovir Ophthalmic Gel? Ophthalmol Eye Dis. 2012;4:23–34. | |
Colin J. Ganciclovir ophthalmic gel, 0.15%: a valuable tool for treating ocular herpes. Clin Ophthalmol. 2007;1(4):441–453. | |
Kaufman HE, Haw WH. Ganciclovir ophthalmic gel 0.15%: safety and efficacy of a new treatment for herpes simplex keratitis. Curr Eye Res. 2012;37(7):654–660. | |
Hlinomazová Z, Loukotová V, Horáčková M, Šerý O. The treatment of HSV1 ocular infections using quantitative real-time PCR results. Acta Ophthalmol. 2012;90(5):456–460. | |
Tabbara KF, Al Balushi N. Topical ganciclovir in the treatment of acute herpetic keratitis. Clin Ophthalmol. 2010;4:905–912. | |
Tabbara KF. Treatment of herpetic keratitis. Ophthalmology. 2005; 112(9):1640. | |
Xu F, Sternberg MR, Kottiri BJ, et al. Trends in herpes simplex virus type 1 and type 2 seroprevalence in the United States. JAMA. 2006;296(8):964–973. | |
Liesegang TJ. Epidemiology and natural history of ocular herpes simplex virus infection in Rochester, Minnesota, 1950–1982. Trans Am Ophthalmol Soc. 1988;86:688–724. | |
Zirgan® [patient’s guide]. Rochester: Bausch and Lomb Incorporated; 2012. Available from: http://www.zirgan-info.com/healthcare_professionals/flipbooks/zirgan_detail_aid_fb/index.html. | |
Lairson DR, Begley CE, Reynolds TF, Wilhelmus KR. Prevention of herpes simplex virus eye disease: a cost-effectiveness analysis. Arch Ophthalmol. 2003;121(1):108. | |
Young RC, Hodge DO, Liesegang TJ, Baratz KH. Incidence, recurrence, and outcomes of herpes simplex virus eye disease in Olmsted County, Minnesota, 1976–2007: the effect of oral antiviral prophylaxis. Arch Ophthalmol. 2010;128(9):1178–1183. | |
Colin J, Hoh HB, Easty DL, et al. Ganciclovir ophthalmic gel (Virgan; 0.15%) in the treatment of herpes simplex keratitis. Cornea. 1997;16(4):393–399. | |
Labetoulle M. [The latest in herpes simplex keratitis therapy]. J Fr Ophtalmol. 2004;27(5):547–557. | |
Ching SST, Feder RS, Hindman HB, Wilhelmus KR, Mah FS. Herpes Simplex Virus Epithelial Keratitis, Preferred Practice Pattern® Clinical Questions. American Academy of Ophthalmology. 2012:1–8. | |
Morissette G, Flamand L. Herpesviruses and chromosomal integration. J Virol. 2010;84(23):12100–12109. | |
Robinet-Combes A, Colin J. Atteintes herpétiques du segment antérieur. Paris, France: Editions Techniques; 1993. Encycl Med Chir, Ophtalmol, 21-200 D-20 (7 p). | |
Farooq AV, Shukla D. Corneal latency and transmission of herpes simplex virus-1. Future Virol. 2011;6(1):101–108. | |
Drugs: Ganciclovir. AIDSinfo Drug Database: US Department of Health and Human Resources; 2013. | |
Mellerick DM, Fraser NW. Physical state of the latent herpes simplex virus genome in a mouse model system: evidence suggesting an episomal state. Virology. 1987;158(2):265–275. | |
Deshmane SL, Fraser NW. During latency, herpes simplex virus type 1 DNA is associated with nucleosomes in a chromatin structure. J Virol. 1989;63(2):943–947. | |
Herpesviruses. In: Brooks GF, Carroll KC, Butel JS, Morse SA, Mietzner TA, editors. Jawetz, Melnick, and Adelberg’s Medical Microbiology, 26e. New York: McGraw-Hill; 2013. Available from: http://accessmedicine.mhmedical.com.ezproxy.hsclib.sunysb.edu/content.aspx?bookid=504&Sectionid=40999955. Accessed February 7, 2014. | |
Suthpin JE, Dana MR, Florakis GJ, Hammersmith K, Reidy JJ, Lopatynsky M, Basic and Clinical Science Course, External Disease and Cornea section 8. San Francisco: American Academy of Ophthalmology. 2006;14:324. | |
Toma HS, Murina AT, Areaux RG Jr, et al. Ocular HSV-1 latency, reactivation and recurrent disease. Semin Ophthalmol. 2008;23(4):249–273. | |
Asbell PA. Valacyclovir for the prevention of recurrent herpes simplex virus eye disease after excimer laser photokeratectomy. Trans Am Ophthalmol Soc. 2000;98:285–303. | |
Darougar S, Wishart MS, Viswalingam ND. Epidemiological and clinical features of primary herpes simplex virus ocular infection. Br J Ophthalmol. 1985;69(1):2–6. | |
Liesegang TJ, Melton LJ 3rd, Daly PJ, Ilstrup DM. Epidemiology of ocular herpes simplex. Incidence in Rochester, Minn, 1950 through 1982. Arch Ophthalmol. 1989;107(8):1155–1159. | |
Wishart MS, Darougar S, Viswalingam ND. Recurrent herpes simplex virus ocular infection: epidemiological and clinical features. Br J Ophthalmol. 1987;71(9):669–672. | |
Obara Y, Furuta Y, Takasu T, et al. Distribution of herpes simplex virus types 1 and 2 genomes in human spinal ganglia studied by PCR and in situ hybridization. J Med Virol. 1997;52(2):136–142. | |
Zheng X. Reactivation and donor-host transmission of herpes simplex virus after corneal transplantation. Cornea. 2002;21(Suppl 7):S90–S93. | |
Remeijer L, Maertzdorf J, Doornenbal P, Verjans GM, Osterhaus AD. Herpes simplex virus 1 transmission through corneal transplantation. Lancet. 2001;357(9254):442. | |
Kennedy DP, Clement C, Arceneaux RL, Bhattacharjee PS, Huq TS, Hill JM. Ocular herpes simplex virus type 1: is the cornea a reservoir for viral latency or a fast pit stop? Cornea. 2011;30(3):251–259. | |
Du T, Zhou G, Roizman B. Modulation of reactivation of latent herpes simplex virus 1 in ganglionic organ cultures by p300/CBP and STAT3. Proc Natl Acad Sci U S A. 2013;110(28):E2621–E2628. | |
Chida Y, Mao X. Does psychosocial stress predict symptomatic herpes simplex virus recurrence? A meta-analytic investigation on prospective studies. Brain Behav Immun. 2009;23(7):917–925. | |
Ludema C, Cole SR, Poole C, Smith JS, Schoenbach VJ, Wilhelmus KR. Association between unprotected ultraviolet radiation exposurev and recurrence of ocular herpes simplex virus. Am J Epidemiol. 2014;179(2):208–215. | |
Mucci JJ, Utz VM, Galor A, Feuer W, Jeng BH. Recurrence rates of herpes simplex virus keratitis in contact lens and non-contact lens wearers. Eye Contact Lens. 2009;35(4):185–187. | |
No authors listed. Psychological stress and other potential triggers for recurrences of herpes simplex virus eye infections. Herpetic Eye Disease Study Group. Arch Ophthalmol. 2000;118(12):1617–1625. | |
Remeijer L, Doornenbal P, Geerards AJ, Rijneveld WA, Beekhuis WH. Newly acquired herpes simplex virus keratitis after penetrating keratoplasty. Ophthalmology. 1997;104(4):648–652. | |
Borderie VM, Meritet JF, Chaumeil C, et al. Culture-proven herpetic keratitis after penetrating keratoplasty in patients with no previous history of herpes disease. Cornea. 2004;23(2):118–124. | |
Levy J, Lapid-Gortzak R, Klemperer I, Lifshitz T. Herpes simplex virus keratitis after laser in situ keratomilieusis. J Refract Surg. 2005;21(4):400–402. | |
No authors listed. Predictors of recurrent herpes simplex virus keratitis. Herpetic Eye Disease Study Group. Cornea. 2001;20(2):123–128. | |
Ghosheh FR, Cremona FA, Rapuano CJ, et al. Trends in penetrating keratoplasty in the United States 1980–2005. Int Ophthalmol. 2008;28(3):147–153. | |
Darlington JK, Adrean SD, Schwab IR. Trends of penetrating keratoplasty in the United States from 1980 to 2004. Ophthalmology. 2006;113(12):2171–2175. | |
Liu E, Slomovic AR. Indications for penetrating keratoplasty in Canada, 1986–1995. Cornea. 1997;16(4):414–419. | |
Lindquist TD, McGlothan JS, Rotkis WM, Chandler JW. Indications for penetrating keratoplasty: 1980–1988. Cornea. 1991;10(3):210–216. | |
Yahalom C, Mechoulam H, Solomon A, Raiskup FD, Peer J, Frucht-Pery J. Forty years of changing indications in penetrating keratoplasty in Israel. Cornea. 2005;24(3):256–258. | |
Sano FT, Dantas PE, Silvino WR, et al. [Trends in the indications for penetrating keratoplasty]. Arq Bras Oftalmol. 2008;71(3):400–404. Portuguese. | |
Robin JB, Gindi JJ, Koh K, et al. An update of the indications for penetrating keratoplasty. 1979 through 1983. Arch Ophthalmol. 1986;104(1):87–89. | |
Inoue Y, Shimomura Y, Fukuda M, et al. Multicentre clinical study of the herpes simplex virus immunochromatographic assay kit for the diagnosis of herpetic epithelial keratitis. Br J Ophthalmol. 2013;97(9):1108–1112. | |
Edwards M, Clover GM, Brookes N, Pendergrast D, Chaulk J, McGhee CN. Indications for corneal transplantation in New Zealand: 1991–1999. Cornea. 2002;21(2):152–155. | |
Williams KA, Lowe MT, Bartlett CM, Kelly L, Coster DJ, editors. The Australian Corneal Graft Registry 2007 Report. 2007. | |
Patel NP, Kim T, Rapuano CJ, Cohen EJ, Laibson PR. Indications for and outcomes of repeat penetrating keratoplasty, 1989–1995. Ophthalmology. 2000;107(4):719–724. | |
Aydemir O, Turkcuoglu P, Bulut Y, Kalkan A. The relationship of graft survival and herpes simplex virus latency in recipient corneal buttons. Clin Ophthalmol. 2007;1(2):127–131. | |
De Kesel RJ, Koppen C, Ieven M, Zeyen T. Primary graft failure caused by herpes simplex virus type 1. Cornea. 2001;20(2):187–190. | |
Biswas S, Suresh P, Bonshek RE, Corbitt G, Tullo AB, Ridgway AE. Graft failure in human donor corneas due to transmission of herpes simplex virus. Br J Ophthalmol. 2000;84(7):701–705. | |
Foster CS. Ganciclovir gel – a new topical treatment for herpetic keratitis. US Ophthalmic Rev. 2007;3:52–56. | |
Shearer DR, Bourne WM. Severe ocular anterior segment ischemia after long-term trifluridine treatment for presumed herpetic keratitis. Am J Ophthalmol. 1990;109(3):346–347. | |
Castela N, Vermerie N, Chast F, et al. Ganciclovir ophthalmic gel in herpes simplex virus rabbit keratitis: intraocular penetration and efficacy. J Ocul Pharmacol. 1994;10(2):439–451. | |
Lass JH, Langston RH, Foster CS, Pavan-Langston D. Antiviral medications and corneal wound healing. Antiviral Res. 1984;4(3):143–157. | |
Wilhelmus KR. Antiviral treatment and other therapeutic interventions for herpes simplex virus epithelial keratitis. Cochrane Database Syst Rev. 2010(12):CD002898. | |
Udell IJ. Trifluridine-associated conjunctival cicatrization. Am J Ophthalmol. 1985;99(3):363–364. | |
Lass JH, Thoft RA, Dohlman CH. Idoxuridine-induced conjunctival cicatrization. Arch Ophthalmol. 1983;101(5):747–750. | |
Maudgal PC, Van Damme B, Missotten L. Corneal epithelial dysplasia after trifluridine use. Graefes Arch Clin Exp Ophthalmol. 1983;220(1):6–12. | |
Hoh HB, Hurley C, Claoue C, et al. Randomised trial of ganciclovir and acyclovir in the treatment of herpes simplex dendritic keratitis: a multicentre study. Br J Ophthalmol. 1996;80(2):140–143. | |
Guess S, Stone DU, Chodosh J. Evidence-based treatment of herpes simplex virus keratitis: a systematic review. Ocul Surf. 2007;5(3):240–250. | |
Collum LM, Akhtar J, McGettrick P. Oral acyclovir in herpetic keratitis. Trans Ophthalmol Soc U K. 1985;104(Pt 6):629–632. | |
Wilhelmus KR. The treatment of herpes simplex virus epithelial keratitis. Trans Am Ophthalmol Soc. 2000;98:505–532. | |
Sozen E, Avunduk AM, Akyol N. Comparison of efficacy of oral valacyclovir and topical acyclovir in the treatment of herpes simplex keratitis: a randomized clinical trial. Chemotherapy. 2006;52(1):29–31. | |
Barron BA, Gee L, Hauck WW, et al. Herpetic Eye Disease Study. A controlled trial of oral acyclovir for herpes simplex stromal keratitis. Ophthalmology. 1994;101(12):1871–1882. | |
No authors listed. Acyclovir for the prevention of recurrent herpes simplex virus eye disease. Herpetic Eye Disease Study Group. N Engl J Med. 1998;339(5):300–306. | |
No authors listed. Oral acyclovir for herpes simplex virus eye disease: effect on prevention of epithelial keratitis and stromal keratitis. Herpetic Eye Disease Study Group. Arch Ophthalmol. 2000;118(8):1030–1036. | |
Simon AL, Pavan-Langston D. Long-term oral acyclovir therapy. Effect on recurrent infectious herpes simplex keratitis in patients with and without grafts. Ophthalmology. 1996;103(9):1399–1404; discussion 1395–1404. | |
Uchoa UB, Rezende RA, Carrasco MA, Rapuano CJ, Laibson PR, Cohen EJ. Long-term acyclovir use to prevent recurrent ocular herpes simplex virus infection. Arch Ophthalmol. 2003;121(12):1702–1704. | |
O’Brien WJ, Segundo AP, Guy J, Dorn EM, Taylor JL. Herpetic stromal disease: response to acyclovir/steroid therapy. Acta Ophthalmol Scand. 1996;74(3):265–270. | |
Zirgan® [prescribing information] Rochester: Bausch and Lomb Incorporated; 2010. Available from: http://www.bausch.com/-/m/BL/United%20States/Files/Package%20Inserts/Pharma/zirganpackageinsert.pdf. Accessed April 16, 2014. | |
Tomicic MT, Bey E, Wutzler P, Thust R, Kaina B. Comparative analysis of DNA breakage, chromosomal aberrations and apoptosis induced by the anti-herpes purine nucleoside analogues aciclovir, ganciclovir and penciclovir. Mutation Research/Fundamental and Molecular Mechanisms of Mutagenesis. 2002;505(1):1–11. | |
Cheng YC, Huang ES, Lin JC, et al. Unique spectrum of activity of 9-[(1,3-dihydroxy-2-propoxy)methyl]-guanine against herpesviruses in vitro and its mode of action against herpes simplex virus type 1. Proc Natl Acad Sci U S A. 1983;80(9):2767–2770. | |
Shaw MM, Gurr WK, Watts PA, Littler E, Field HJ. Ganciclovir and penciclovir, but not acyclovir, induce apoptosis in herpes simplex virus thymidine kinase-transformed baby hamster kidney cells. Antivir Chem Chemother. 2001;12(3):175–186. | |
Chun YS, Park NH. Effect of ganciclovir [9-(1,3-dihydroxy-2-propoxymethyl)guanine] on viral DNA and protein synthesis in cells infected with herpes simplex virus. Antimicrob Agents Chemother. 1987;31(2):349–351. | |
Chee SP, Jap A. Treatment outcome and risk factors for visual loss in Cytomegalovirus endotheliitis. Graefes Arch Clin Exp Ophthalmol. 2012;250(3):383–389. | |
Kandori M, Inoue T, Takamatsu F, et al. Prevalence and features of keratitis with quantitative polymerase chain reaction positive for cytomegalovirus. Ophthalmology. 2010;117(2):216–222. | |
Su CC, Wang IJ, Chen WL, Lin CP, His B, Hu FR. Topical ganciclovir treatment in patients with cytomegalovirus endotheliitis receiving penetrating keratoplasty. Clin Experiment Ophthalmol. 2013;41(4):339–347. | |
Wang SC, Tsai IL, Lin HC, Kuo LL, Tsai CY, Liou SW. Recurrent cytomegalovirus corneal endotheliitis after penetrating keratoplasty. Eur J Ophthalmol. March–April 2010;20(2):457–459. | |
Faulds D, Heel RC. Ganciclovir. A review of its antiviral activity, pharmacokinetic properties and therapeutic efficacy in cytomegalovirus infections. Drugs. 1990;39(4):597–638. | |
Wang X, Xu JJ, Le QH, Wang Y, Wang WT. [Clinical assessment of oral ganciclovir capsules on the treatment of herpes simplex keratitis]. Zhonghua Yan Ke Za Zhi. 2010;46(11):994–999. Chinese. | |
Sullivan V, Talarico CL, Stanat SC, Davis M, Coen DM, Biron KK. A protein kinase homologue controls phosphorylation of ganciclovir in human cytomegalovirus-infected cells. Nature. 1992;358(6382):162–164. | |
Hamzeh FM, Lietman PS. Intranuclear accumulation of subgenomic noninfectious human cytomegalovirus DNA in infected cells in the presence of ganciclovir. Antimicrob Agents Chemother. 1991;35(9):1818–1823. | |
Crumpacker CS. Ganciclovir. N Engl J Med. 1996;335(10):721–729. | |
Leibowitz HM, Waring GO. Corneal Disorders: Clinical Diagnosis and Management. Philadelphia, PA: Saunders; 1998:599–600, 746–748. | |
Virgan® [summary of product characteristics]. Macclesfield: Spectrum Théa Pharmaceuticals; 2003. | |
Transphyto. 1993b. Etude clinique comparative multicentrique de l′effet del′instillation de GV 550 dans l’herpes corne´en superficiel. Clermont- Ferrand, France: Rapport clinique No 44.GV 550/12.90-46.GV 550/07.90. Dossier d′AMM. | |
Transphyto. 1993c. Etude clinique comparative randomisée en simple insu de l′effet de l′instillation de ganciclovir gel ophtalmique dans le traitement de l′herpes cornéen superficiel. Clermont-Ferrand, France: Rapport clinique No 47.GV 550/09.90. Dossier d′AMM. | |
Pouliquen P, Elena PP, Malecaze F, Luyckx J, Lanoue A, Goldschmidt P. Assessment of the safety and local pharmacokinetics of 0.15% gel of ganciclovir (Virgan®) in healthy volunteers. ARVO meeting 1996; Fort Lauderdale, FL, USA. Invest Ophthalmol Vis Sci. 1996;37:S313, abstract 1431. | |
Tirucherai GS, Dias C, Mitra AK. Corneal permeation of ganciclovir: mechanism of ganciclovir permeation enhancement by acyl ester prodrug design. J Ocul Pharmacol Ther. 2002;18(6):535–548. | |
Trousdale MD, Nesburn AB, Willey DE, Taaid H. Efficacy of BW759 (9-[[2-hydroxy-1-(hydroxymethyl) ethoxy] methyl] guanine) against herpes simplex virus type 1 keratitis in rabbits. Curr Eye Res. 1984;3(8):1007–1015. | |
Lowe E, Jiang S, Proksch JW. Rapid ocular penetration of ganciclovir with topical administration of Zirgan® to rabbits. Poster presented at: 2008 Annual Meeting of the Association for Research in Vision and Ophthalmology; April 30–May 5, 2011; Fort Lauderdale, FL. | |
Majumdar S, Tirucherai GS, Pal D, Mitra AK. Functional differences in nucleoside and nucleobase transporters expressed on the rabbit corneal epithelial cell line (SIRC) and isolated rabbit cornea. AAPS PharmSci. 2003;5(2):72–85. | |
Naito T, Nitta K, Kinouchi Y, Shiota H, Mimura Y. Effects of 9-(1,3-dihydroxy-2-propoxymethyl) guanine (DHPG) eye drops and cyclosporine eye drops in the treatment of herpetic stromal keratitis in rabbits. Curr Eye Res. 1991;10 Suppl:201–203. | |
Shiota H, Naito T, Mimura Y. Anti-herpes simplex virus (HSV) effect of 9-(1,3-dihydroxy-2-propoxymethyl) guanine (DHPG) in rabbit cornea. Curr Eye Res. 1987;6(1):241–245. | |
Clirophta. Evaluation de la tolérance locale chez le volontaire sain, après instillations multiples d’un gel ophtalmique de ganciclovir 0,15%, Virgan. Nice, France: Rapport clinique Virgan/F-94-01. Dossier d’AMM; 1994. | |
Clirophta. Cinétique du ganciclovir dans les larmes, après instillations multiples d’un gel ophtalmique de ganciclovir 0,15%, Virgan, chez le volontaire sain. Nice, France: Rapport clinique Virgan/F-94-02. Dossier d’AMM; 1994. | |
Kaufman HE. Data from Trials Evaluating Ganciclovir Ophthalmic Gel 0.15% and Acyclovir Ophthalmic Ointment 3.0% for Herpetic Keratitis. AAO Annual Meeting, Atlanta, GA, USA. November 9, 2008. P0054. | |
Traugott, K. National Drug Monograph: Ganciclovir Ophthalmic Gel 0.15% (Zirgan™). VA Pharmacy Benefits Management Services. May 2010. | |
Holdiness MR. Contact dermatitis from topical antiviral drugs. Contact Dermatitis. 2001;44(5):265–269. | |
Lorenzi S, D’Antuono A, Iorizzo M, Tosti A. Skin rash and splinter hemorrhages from ganciclovir. J Dermatolog Treat. 2003;14(3):177–178. | |
Varnell ED, Kaufman HE. Comparison of Ganciclovir Ophthalmic Gel and Trifluridine Drops for the Treatment of Experimental Herpetic Keratitis. Invest Ophthalmol Vis Sci. 2008;49:E-Abstract 2491. | |
Varnell ED, Kaufman HE. Comparison of ganciclovir ophthalmic gel and trifluridine drops for the treatment of experimental herpes keratitis. Paper presented at: 2011 Annual Meeting of the Association for Research in Vision and Ophthalmology; April 30 to May 5, 2011; Fort Lauderdale, FL. | |
Gordon YJ, Capone A, Sheppard J, Gordon A, Romanowski E, Araullo-Cruz T. 2′-nor-cGMP, a new cyclic derivative of 2′NDG, inhibits HSV-1 replication in vitro and in the mouse keratitis model. Curr Eye Res. 1987;6(1):247–253. | |
Charles SJ, Gray JJ. Ocular herpes simplex virus infections: reduced sensitivity to acyclovir in primary disease. Br J Ophthalmol. 1990;74(5):286–288. | |
Lee SY. Herpes simplex virus ocular infections. Drugs Today (Barc). 1998;34(3):241–249. | |
Laibson PR. Resistant herpes simplex keratitis. Clin Experiment Ophthalmol. 2010;38(3):227–228. | |
Superti F, Ammendolia M, Marchetti M. New advances in anti-HSV chemotherapy. Current medicinal chemistry. 2008;15(9):900–911. | |
Choong K, Walker NJ, Apel AJ, Whitby M. Aciclovir-resistant herpes keratitis. Clin Experiment Ophthalmol. 2010;38(3):309–313. | |
Levin MJ, Bacon TH, Leary JJ. Resistance of herpes simplex virus infections to nucleoside analogues in HIV-infected patients. Clin Infect Dis. 2004;39 Suppl 5:S248–S257. | |
Duan R, de Vries RD, Osterhaus AD, Remeijer L, Verjans GM. Acyclovir-resistant corneal HSV-1 isolates from patients with herpetic keratitis. J Infect Dis. 2008;198(5):659–663. | |
Duan R, de Vries RD, van Dun JM, et al. Acyclovir susceptibility and genetic characteristics of sequential herpes simplex virus type 1 corneal isolates from patients with recurrent herpetic keratitis. J Infect Dis. 2009;200(9):1402–1414. | |
Bacon TH, Levin MJ, Leary JJ, Sarisky RT, Sutton D. Herpes simplex virus resistance to acyclovir and penciclovir after two decades of antiviral therapy. Clin Microbiol Rev. 2003;16(1):114–128. | |
Yao YF, Inoue Y, Kase T, Uchihori Y, Mori Y, Ohashi Y. Clinical characteristics of acyclovir-resistant herpetic keratitis and experimental studies of isolates. Graefes Arch Clin Exp Ophthalmol. 1996; 234 Suppl 1:S126–S132. | |
Drugs; Guidance, Compliance, and Regulatory information; Surveillance. US Food and Drug Administration; updated 11/13/2012. Available from: http://www.fda.gov/drugs/guidancecomplianceregulatoryinformation/surveillance/ucm324693.htm. Accessed April 16, 2014. | |
Liu S, Pavan-Langston D, Colby KA. Pediatric herpes simplex of the anterior segment: characteristics, treatment, and outcomes. Ophthalmology. 2012;119(10):2003–2008. | |
Schwartz GS, Holland EJ. Oral acyclovir for the management of herpes simplex virus keratitis in children. Ophthalmology. 2000;107(2):278–282. | |
Hsiao C-H, Yeung L, Yeh L-K, et al. Pediatric herpes simplex virus keratitis. Cornea. 2009;28(3):249–253. | |
Chong E-M, Wilhelmus KR, Matoba AY, Jones DB, Coats DK, Paysse EA. Herpes simplex virus keratitis in children. Am J Ophthalmol. 2004;138(3):474–475. | |
No authors listed. A controlled trial of oral acyclovir for iridocyclitis caused by herpes simplex virus. The Herpetic Eye Disease Study Group. Arch Ophthalmol. 1996;114(9):1065–1072. | |
Tabbara KF, Jarade EF. Ganciclovir effects in adenoviral keratoconjunctivitis. Invest Ophthalmol Vis Sci. 2001;42:4. | |
Yabiku ST, Yabiku MM, Bottós KM, Araújo AL, Freitas Dd, Belfort R Jr. [Ganciclovir 0.15% ophthalmic gel in the treatment of adenovirus keratoconjunctivitis]. Arq Bras Oftalmol. 2011;74(6):417–421. Portuguese. | |
Epstein SP, Fernandez KB, Carter BM, Abdou SA, Gadaria N, Asbell PA. Safety and efficacy of ganciclovir ophthalmic gel for treatment of adenovirus keratoconjunctivitis utilizing cell culture and animal models. Inv Ophthalmol Vis Sci. 2012;(Suppl)53(4):6203. | |
Uchio E, Takeuchi S, Itoh N, Matsuura N, Ohno S, Aoki K. Clinical and epidemiological features of acute follicular conjunctivitis with special reference to that caused by herpes simplex virus type 1. Br J Ophthalmol. 2000;84(9):968–972. | |
Trousdale MD, Goldschmidt PL, Nóbrega R. Activity of ganciclovir against human adenovirus type-5 infection in cell culture and cotton rat eyes. Cornea. 1994;13(5):435–439. | |
Vérin P, Mortemousque B, Barach D. Ganciclovir 0.15% gel, a new treatment in epidemic keratoconjunctivitis (EKC). Ophthalmic Res. 1997;29(Suppl 1):12–27. | |
Lifelong Vision Foundation. A Placebo Controlled Comparison of Topical Zirgan Versus Genteal Gel for the Treatment of Adenovirus Conjunctivitis. In: ClinicalTrials.gov [website on the Internet]. Bethesda, MD: US National Library of Medicine; 2012 [updated February 10, 2012]. Available from http://clinicaltrials.gov/ct2/show/NCT01533480?term=NCT01533480&rank=1. NLMidentifier:NCT01533480. Accessed March 5, 2014. | |
Adapt Produtos Oftalmológicos Ltda. Evaluate the Use of Ganciclovir Gel 0.3% for the Treatment of Conjunctivitis Caused by Adenovirus. In: ClinicalTrials.gov [website on the Internet]. Bethesda, MD: US National Library of Medicine; 2011 [updated May 15, 2012]. Available from http://clinicaltrials.gov/ct2/show/NCT01600365?term=NCT01600365&rank=1. NLMidentifier:NCT01600365. Accessed March 5, 2014. | |
Yee RW, Sigler SC, Lawton AW, Alderson GL, Trinkle JK, Lum CT. Apparent cytomegalovirus epithelial keratitis in a cardiac transplant recipient. Transplantation. 1991;51(5):1040–1043. | |
Wehrly SR, Manning FJ, Proia AD, Burchette JL, Foulks GN. Cytomegalovirus keratitis after penetrating keratoplasty. Cornea. 1995;14(6):628–633. | |
Wilhelmus KR, Font RL, Lehmann RP, Cernoch PL. Cytomegalovirus keratitis in acquired immunodeficiency syndrome. Arch Ophthalmol. 1996;114(7):869–872. | |
Aggarwal S, Cavalcanti BM, Pavan-Langston D. Treatment of pseudodendrites in herpes zoster ophthalmicus with topical ganciclovir 0.15% gel. Cornea. 2014;33(2):109–113. | |
Oliver S, Bubley G, Crumpacker C. Inhibition of HSV-transformed murine cells by nucleoside analogs, 2′-NDG and 2′-nor-cGMP: mechanisms of inhibition and reversal by exogenous nucleosides. Virology. 1985;145(1):84–93. | |
Vile RG, Hart IR. Use of tissue-specific expression of the herpes simplex virus thymidine kinase gene to inhibit growth of established murine melanomas following direct intratumoral injection of DNA. Cancer Research. 1993;53(17):3860–3864. | |
Chévez-Barrios P, Chintagumpala M, Mieler W, et al. Response of retinoblastoma with vitreous tumor seeding to adenovirus-mediated delivery of thymidine kinase followed by ganciclovir. J Clin Oncol. 2005;23(31):7927–7935. | |
Sturges A, Butt AL, Lai JE, Chodish J. Topical interferon or surgical excisio for the management of primary ocular surface squamous neoplasia. Ophthalmology. 2008;115(8):1297–1302. | |
Gupta A, Muecke J. Treatment of ocular surface squamous neoplasia with Mitomycin C. Br J Ophthalmol. 2010;94(5):555–558. | |
Krilis M, Tsang H, Coroneo M. Treatment of conjunctival and corneal epithelial neoplasia with retinoic acid and topical interferon alpha-2b: long-term follow-up. Ophthalmology. 2012;119(10):1969–1973. | |
Westekemper H, Freistuehler M, Anastassiou G, et al. Chemosensitivity of conjunctival melanoma cell lines to single chemotherapeutic agents and combinations. Br J Ophthalmol. 2012;96(4):591–596. | |
Herold TR, Hintschich C. Interferon alpha for the treatment of melanocytic conjunctival lesions. Graefes Arch Clin Exp Ophthalmol. 2010;248(1):111–115. | |
Finger PT, Sedeek RW, Chin KJ. Topical interferon alpha in the treatment of conjumctival melanoma and priimary acquired melanosis complex. Am J Ophthalmol. 2008;145(1):124–129. | |
McDonald MB, Hardten DR, Mah FS, et al. Management of epithelial herpetic keratitis: An evidence-based algorithm. Report from the Ad-Hoc Committee for the Management of Epithelial Herpetic Keratitis. November 11, 2012. Available from: http://www.optometricmanagement.com/content/bl/2/b-l_treament-finalnb.pdf. Accessed April 16, 2014. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.