")
Back to Journals » International Journal of General Medicine » Volume 17
Frequent Misdiagnosis of Scabies as Eczema in China: A Descriptive Study of 23 Cases
Received 10 January 2024
Accepted for publication 10 April 2024
Published 26 April 2024 Volume 2024:17 Pages 1615—1623
DOI https://doi.org/10.2147/IJGM.S458731
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sandul Yasobant
Xumei Wu,1,2 Feifei Yang,3 Ruina Zhang1
1Department of Dermatology, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Dermatology, Beijing Children’s Hospital, Capital Medical University, National Center for Children’s Health, Beijing, People’s Republic of China; 3Department of Dermatology, Tongzhou Maternal & Child Health Hospital of Beijing, Beijing, People’s Republic of China
Correspondence: Ruina Zhang, Department of Dermatology, Beijing Friendship Hospital, Capital Medical University, Beijing, 100050, People’s Republic of China, Tel +8613811708671, Email [email protected]
Objective: To outline the clinical manifestations observed in patients with scabies misdiagnosed as generalized eczema, analyse the factors contributing to these misdiagnoses and explore potential reasons for the resurgence of scabies.
Patients and Methods: A retrospective analysis was performed to investigate the patients with scabies misdiagnosed as generalized eczema.
Results: We included 23 patients, with twelve (52.17%) being male and eleven (47.83%) female. The illness duration ranged from 0.5 to 7 months. Among all patients, 12 (52.17%) were residents of nursing homes, 5 (21.74%) were staff members of these facilities, 4 (17.39%) were caregivers of long-term hospitalized relatives, 1 (4.35%) was a construction worker, and 1 (4.35%) had a history of tourism. The rash predominantly affected the trunk and extremities, 12 patients (52.17%) are each involved the perineum and fingers webbings. The presentations included erythema, papules, and nodules. The main complaint of all patients was nocturnal itch. Under direct microscopy, 5 patients (21.74%) tested positive for scabies mites, and 3 (13.04%) showed histopathological features consistent with scabies. All patients were initially misdiagnosed with generalized eczema.
Conclusion: Over half of all patients diagnosed with scabies either resided or worked in long-term care facilities. The lack of awareness of scabies among medical staff in long-term care facilities readily led to frequent misdiagnosis. Comprehensive measures should be implemented urgently to strengthen disease management.
Keywords: scabies, long-term care facilities, elderly, misdiagnose, pruritus
Introduction
Scabies is a contagious dermatosis caused by infestation with the parasite Sarcoptes scabiei var. hominis, which was first reported by Bonomo in 1687.1 It represents a global health concern that affects individuals of all ages, races, and social strata. Transmission occurs through direct skin-to-skin contact or contact with the fomites of infected patients. The morbidity rates vary significantly, ranging from 4% to 100% in low-income countries.2,3 The rash of scabies is symmetrically distributed, typically affecting the interdigital spaces, wrists, axillae, behind the ears, waist, ankles, feet, and buttocks. In men, the penis and scrotum are commonly affected, while in women, the areolae, nipples, and perineum are frequently involved.4 The clinical manifestations include disseminated inflammatory papules, accompanied by scratch marks, vesicles, and nodules. The characteristic feature of scabies is the burrow,5 which appears as tortuous, linear, grey-white tracks, typically 1–10 mm in length, but is rarely observed. Pruritus, a common symptom, intensifies at night or after a hot bath. Scabies tends to thrive in overcrowded areas with limited water resources, with higher incidence rates in closed environments, such as hospitals, prisons, and nursing homes. As an important public health concern, scabies was added to the World Health Organization’s list of neglected tropical diseases in 2017.6
Around the 1980s, China experienced a very high incidence of scabies. However, over the past two decades, the prevalence has greatly decreased, especially in economically developed urban areas, owing to societal progress, improved hygiene practice, and enhanced living standards. Despite this, a resurgence of scabies has been observed in the last two years, coinciding with the rapid development of long-term care facilities and inadequate sanitary management measures. Most subjects in the present study were elderly residing in nursing homes. Due to a lack of awareness of scabies among primary general practitioners, almost 100% of patients were misdiagnosed with dermatitis or eczema. Consequently, oral antihistamines and topical corticosteroid ointments were administered without improvement. This study collected data on 23 patients misdiagnosed with generalized eczema, with the aim of summarising their clinical manifestations, analysing the reasons for misdiagnosis and proposing potential solutions.
Methodology
In this single-center retrospective study, we collected data from 23 patients with scabies misdiagnosed with generalized eczema at the Dermatology Outpatient Clinic of Beijing Friendship Hospital from 2021 to 2023. Among these patients, 5 (21.74%) received a scabies diagnosis through microscopic examination, and 3 (13.04%) were supported by histopathological examination. All patients achieved a cure following treatment with 10% sulphur ointment. We recorded demographic characteristics, disease duration, contact history, lesion distribution, lesion morphology, and previous treatments for all included cases.
Statistical Analysis
Quantitative data are expressed as the mean ± standard deviation and qualitative data as the number and percentage of patients, n (%).
Results
General Information
The age of the 23 patients included in the study ranged from 40 to 90 years, with a median age of 65.96 years. The age distribution was as follows: 3 patients (13.04%) were aged 40–50 years, 5 patients (21.74%) were aged 51–60 years, 6 patients (26.09%) were aged 61–70 years, 6 patients (26.09%) were aged 71–80 years, and 3 patients (13.04%) were aged 81–90 years. The gender distribution was nearly equal, with 12 (52.17%) men and 11 (47.83%) women. The disease duration ranged from 0.5 to 7 months, with an average duration of 3.2 months (Table 1).
 |
Table 1 Sociodemographic Characteristics of the Study Population |
Lesion Distribute
In all 23 patients, the lesions were widespread, with 100% of cases involving the trunk, primarily the abdomen. Additionally, 22 patients (95.65%) exhibited lesions on the extremities, predominantly on the upper limbs. Twelve patients (52.17%) had lesions on their hands/fingers, and 12 (52.17%) on their genital areas (Table 2).
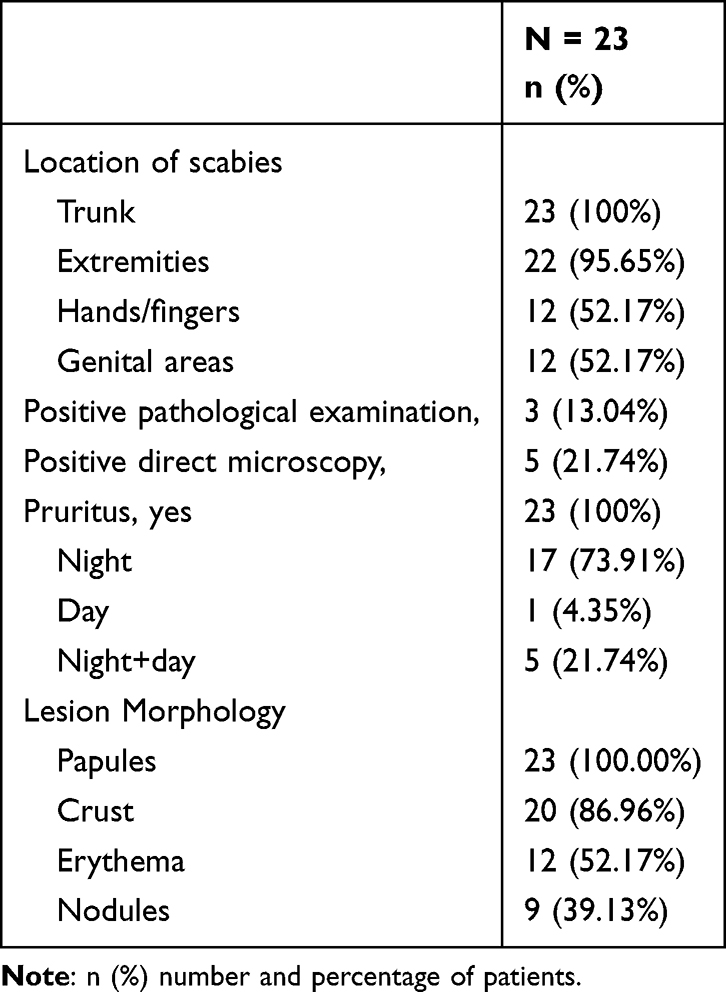 |
Table 2 Scabies Clinical Characteristics |
Pruritus Characteristics
All patients complained of pruritus, with 17 patients (73.91%) reporting more intense itching at night. One patient (4.35%) experienced worsening itching during the day, while 5 (21.74%) reported no considerable difference in itching between day and night (Table 2).
Lesion Morphology
The cases were primarily characterized by erythema, papules, nodules, and crusts. Papules were observed in all patients, erythema in 12 (52.17%), nodules in 9 (39.13%), and crusts in 20 (86.96%). None of the patients showed burrows or secondary pyogenic infections in their lesion morphology (Table 2).
Contact History
Of the 23 patients, 12 (52.17%) were long-term residents of nursing homes, 5 (21.74%) were nursing home staff, 4 (17.39%) were caregivers for long-term hospitalized relatives, 1 (4.35%) was a construction worker and 1 (4.35%) had a travel history.
Misdiagnosis
All patients were initially misdiagnosed with generalized eczema. Before the correct diagnosis, 22 patients (95.65%) had taken oral antihistamines, 1 (4.34%) had received unidentified traditional Chinese medicine orally, 18 (78.26%) had used topical corticosteroids, 2 (8.69%) had received intramuscular injections of compound betamethasone and 7 (30.43%) had externally used traditional Chinese medicine ointments.
Management of Scabies
After scabies was suspected, all 23 patients underwent treatment with 10% sulphur ointment topically applied twice daily for three consecutive days, covering the entire body except the face, with special attention to the webbings of the fingers, wrists, elbows, armpits, groin, and genital areas. On the fourth day, the patients changed their clothes, bed linens and took a bath. This constituted one treatment course. All patients were cured after three consecutive regular treatments and showed no recurrence upon re-examination at two weeks after drug withdrawal (Figures 1–2).
 |
Figure 1 Scrotal scabies of a 66-year-old nursing home resident. (A) Multiple nodules in size 0.3–0.5mm on the scrotuma before treatment; (B) One week after the initiation of treatment with 10% sulphur ointment; (C) Two weeks after the initiation of treatment. (D) Three weeks after the initiation of treatment. |
 |
Figure 2 Scabies of a 71-year-old nursing home resident. (A) Showing multiple papules and plaque with crust and scale before treatment; (B) One week after the initiation of treatment with 10% sulphur ointment; (C) Two weeks after the initiation of treatment. |
Discussion
Scabies is a global infectious skin disease that is often neglected.7 The WHO estimates that approximately 300 million people are affected by scabies annually, with approximately 130 million suffering from the condition at any given time.8 Although scabies is not fatal and is treatable, it can have deleterious effects, particularly on the elderly residing in nursing homes who often have underlying conditions such as hypertension, diabetes, and weakened immune systems. Among the cases we studied, a 58-year-old patient with Down syndrome (Figure 3) and other comorbidities including hypertension, diabetes, Parkinson’s disease, Alzheimer’s disease, polymorphic undifferentiated sarcoma, chronic glomerulonephritis, and depression. Grodner et al suggested that Down syndrome is a high-risk factor for the development of crusted scabies.9 Itching is a hallmark symptom of scabies, seriously affecting sleep and mental well-being.10 Scabies can also lead to secondary bacterial infections such as Staphylococcus aureus and post-streptococcal glomerulonephritis.11 It impacts the quality of life, as demonstrated in a study by A Jin-gang et al, indicating that scabies has a moderate impact on the patients’ quality of life.12 Scabies often occurs in confined places such as nursing homes, hospitals, nurseries, and prisons.13 So patients with scabies can also affect the people around them and the reputation of nursing homes, leading to panic among other residents.14
 |
Figure 3 Scabies of a 58-year-old patient with Down syndrome. (A) Erythematous papules with scale at interdigital areas of the fingers. (B and C) One week and two weeks after the initiation of treatment at interdigital areas of the fingers. (D) Erythematous papules with scale located at genitals and extended to the abdomen and bilateral thigh. (E and F) One and two weeks after the initiation of treatment with 10% sulphur ointment at genitals, abdomen and bilateral thigh. |
With the ongoing development of societies, the ageing of the global population has become a prevalent trend. United Nations statistics reveal a considerable increase in the global population aged ≥65 years, from 160 million in 1950 to 720 million in 2020. China, being the most populous country is experiencing a rapid increase in the number of its elderly population. A cross-sectional analysis of the 2015 Global Burden of Disease Study identified China as the second-highest country for scabies incidence, following Indonesia, East Timor, Vanuatu, and Fiji.15 Beijing, as the capital of China, is also facing challenges owing to its aging population. As of 2022, among Beijing’s permanent residents, 4.651 million individuals are aged ≥60 years, constituting 21.3% of the total population. In response to this demographic shift, elderly care facilities have proliferated under policy guidance and societal demand. Before 1990, Beijing had only 68 government-run elderly care facilities. Since 2006, the number of such institutions has consistently grown, reaching 795 institutions with 116,629 beds by 2023, expanding at an annual rate of approximately 10%. This rapid development introduces challenges, including insufficient sanitary management and a lack of scabies knowledge among staff, resulting in outbreaks of infectious skin diseases. The residents of these institutions are often elderly individuals with various underlying diseases and cognitive impairments like Alzheimer’s and dementia, making scabies more prevalent and readily transmitted. In our study, 12 out of 23 cases were nursing home residents, and 5 were staff, with 73.9% related to elder care institutions, emphasizing the urgent need for improved sanitary management. It is imperative to enhance the hygiene management mechanism in nursing homes. Staff members should wear long gowns and gloves when interacting with different residents to prevent potential transmission between staff and residents, as previously mentioned.16 Moreover, there is a need to promote education and awareness of scabies among nursing home management personnel and staff through activities, such as knowledge dissemination and training. General practitioners and dermatologists should possess a comprehensive understanding of the clinical characteristics of scabies. Recognizing atypical presentations in elderly patients is crucial. During patient visits, healthcare professionals should diligently inquire about the patient’s history of scabies exposure, conduct thorough examinations, and strive to improve the accurate diagnosis rate of scabies among elderly patients.
Elderly patients with scabies are frequently misdiagnosed as having eczema or other common dermatosis. In a study by Skayem et al, half of 95 severe scabies cases were initially misdiagnosed, with the most common misdiagnosis being eczema.17 In our study, almost all patients received one or multiple misdiagnosis of eczema, with 22 patients receiving antihistamines and 18 using topical glucocorticoids as treatments. The use of glucocorticoids in scabies can exacerbate or mask the manifestations, increasing the risk of infection or severe scabies. In pig models, systemic corticosteroids (oral dexamethasone at a dose of 0.2 mg/kg/day) increased the intensity and duration of scabies infestation.18 Pigs treated with corticosteroids developed severe, especially crusted scabies.19 Misdiagnosis often arises due to the profuse distribution of scabies lesions, resembling generalized eczema. In our study, nearly all patients had symmetrically distributed lesions on the extremities and back, in addition to the abdominal area. Although the presentations in interdigital spaces or genital areas are diagnostically significant, in our study, only approximately 50% of patients had lesions in these areas. When ambulatory clinics do not perform close scrutiny, an eczema diagnosis is often established.
Inadequate differentiation of pruritic dermatological diseases by physicians is another factor contributing to the misdiagnosis of scabies. Various skin conditions, including eczema, atopic dermatitis, nodular prurigo, xerosis, and pruritus, present with itching and can be challenging to distinguish clinically.20 Understanding the following characteristics of scabies can aid in its differentiation from other skin disorders with pruritus. Firstly, scabies is contagious, with most patients having a history of contact with the person who has the similar symptoms like roommates or family members, necessitating a thorough medical history review. Secondly, in patients with scabies, papules, vesicles, and burrows are distributed on the softer parts of the skin such as scrotum and interdigital areas of the fingers. Thirdly, scabies itching typically intensifies at night due to increased mite activity. In our study, all patients reported itching, with 5 patients showing no significant difference between day and night, 1 experiencing more severe itching during the day, and 17 reporting increased itching at night—aligning with typical clinical observations.
Over the past two to three decades, as the living conditions have improved, the number of scabies cases has greatly reduced. As a result, young medical professionals often lack awareness of scabies, relying heavily on textbook knowledge and lacking practical clinical experience, which diminishes their vigilance. Recognizing this, especially among first-contact physicians, could substantially decrease the misdiagnosis rate and enhance clinical diagnostic accuracy.
The diagnosis of scabies mainly relies on skin dermatoscopy and reflectance confocal microscopy, during which a brownish triangular contour (kite sign, corresponding to the head and breastplate of the mite), in connection with the aircontaining intracorneal burrow system (“wake sign”).5 Alternatively, scraping scales from the lesion with a blunt scalpel and mixing them with mineral oil for microscopic examination can reveal scabies mites, eggs, fecal pellets, and other metabolites. Skin biopsy may also be employed to identify scabies mites. Additionally, the utilization of the newly developed quantitative polymerase chain reaction (qPCR) detection, combined with the employment of alternative non-invasive swab sampling techniques could augment the diagnostic rate of scabies.21 However, these techniques exhibit lower sensitivity in cases of common scabies with sparse mite infestation. Among the 23 patients mentioned, only 5 underwent scabies microscopy, yielding positive results for scabies mites. Skin biopsy was performed in 3 patients, revealing dermal infiltration of eosinophils, supporting the diagnosis of scabies when mites are not visible (Figure 4). Therefore, empirical treatment becomes particularly crucial, especially when encountering patients presenting with eczematous lesions, accompanied by rashes in the interdigital spaces or genital areas, residing in nursing homes or having a history of hospitalization. Vigilance should be heightened, and empirical acaricidal therapy should be promptly administered if conventional treatments are ineffective to avoid delays in managing the condition.
 |
Figure 4 Scabies on the Hip of a 90-year-old patient. (A) Showing multiple nodules and hyperpigmentation on the Hip. (B) Histopathological examination of nodule on the Hip: a large number of inflammatory cells infiltrated in the superficial and middle dermis (HE, 200×). (C) showing a large number of eosinophils and lymphocytes in the dermis (HE, 400×). |
The primary approach to scabies treatment involves the use of insecticides to eliminate the mites and relieve itching. In countries, such as the United States, the United Kingdom, and France, permethrin is the preferred treatment for scabies. Lindane ointment, owing to its neurotoxic side effects, is currently less commonly used.22 Oral ivermectin, an antibiotic with potent acaricidal effects, can be used for the treatment of crusted scabies and prophylactic treatment of scabies.23 Ivermectin is only acaricidal and not ovicidal; thus, repeated treatment after 7 to 14 days is necessary, so that all larvae that were still unhatched at the time of the initial treatment can be killed before at taining reproductive maturity.5 Over the past few years, reports from around the world about the use of ivermectin for scabies in humans have suggested that this drug could be used as an alternative oral therapy, especially in Western countries. In China, because of lack of ivermectin, the most commonly used treatments are 10% sulphur ointment or crotamiton cream. Sulphur ointment is cost-effective and readily available.12 In our studied cases, all 23 patients were treated with 10% sulphur ointment topically, achieving a cure after three courses. No serious adverse reactions occurred, with only 1 patient experiencing localized irritant dermatitis.
The limitations of this study include the collection of cases from a single center only, with a small number of cases. In the future, it is necessary to validate the conclusions through a population-based studies with a larger sample size to explain the reason related to the rise and fall and rise again of scabies in China.
Conclusion
The rapid expansion of long-term care facilities underscores the urgency of implementing robust health management systems and augmenting staff awareness of hygiene to curtail the transmission of various infectious diseases, including scabies. To address scabies resurgence, training programs in scabies knowledge for primary general practitioners and specialists should be intensified. Equipping them with a comprehensive understanding of the clinical characteristics of scabies is crucial for reducing the misdiagnosis rates, enhancing diagnostic accuracy and enabling timely disease control. When there is diagnostic uncertainty, it may be worth a trial of scabies treatment in patients with unexplained pruritus.
Data Sharing Statement
Data generated and analysed during the study are available from the corresponding authors.
Ethics Statement
This study was conducted in accordance with the principles of the Declaration of Helsinki. Ethical clearance was obtained from the Ethical Review Committee of Beijing Friendship Hospital (2023-P2-094-01). Informed consent was acquired from each participant included in the study and the patients in the images provided written informed consent for the images to be published.
Acknowledgment
We are very grateful to the unit in charge for their administrative approval and support. We also thank the cooperation of all the patients in our study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Ramos-E-Silva M. Giovan cosimo bonomo (1663–1696): discoverer of the etiology of scabies. Int J Dermatol. 1998;37(8):625–630. doi:10.1046/j.1365-4362.1998.00400_1.x
2. Meinking TL, Burkhart CG, Burkhart CN. Ectoparasitic diseases in dermatology: reassessment of scabies and pediculosis. Adv Dermatol. 2000;15:67–108.
3. Burkhart CG, Burkhart CN, Burkhart KM. An epidemiologic and therapeutic reassessment of scabies. Cutis. 2000;65(4):233–240.
4. Hay RJ, Steer AC, Engelman D, et al. Scabies in the developing world--its prevalence, complications, and management. Clin Microbiol Infect. 2012;18(4):313–323. doi:10.1111/j.1469-0691.2012.03798.x
5. Sunderkötter C, Wohlrab J, Hamm H. Scabies: epidemiology, diagnosis, and treatment. Dtsch Arztebl Int. 2021;118(41):695–704. doi:10.3238/arztebl.m2021.0296
6. Martin D, Wiegand R, Goodhew B, et al. Impact of ivermectin mass drug administration for lymphatic filariasis on scabies in eight villages in kongwa district, Tanzania. Am J Trop Med Hyg. 2018;99(4):937–939. doi:10.4269/ajtmh.18-0018
7. Claire Fuller L. Epidemiology of scabies. Curr Opin Infect Dis. 2013;26(2):123–126. doi:10.1097/QCO.0b013e32835eb851
8. Sharaf MS, Othman AA, Abdel-Ghaffar AE, et al. Crusted scabies in a rabbit model: a severe skin disease or more? Parasit Vectors. 2023;16(1):413. doi:10.1186/s13071-023-05995-8
9. Grodner C, Miquel J, Hadj-Rabia S, et al. Crusted scabies in children in France: a series of 20 cases. Eur J Pediatr. 2022;181(3):1167–1174. doi:10.1007/s00431-021-04251-4
10. Thomas CT, Coates SJ, Engelman D, et al. Ectoparasites: scabies. J Am Acad Dermatol. 2020;82(3):533–548. doi:10.1016/j.jaad.2019.05.109
11. Shmidt E, Levitt J. Dermatologic infestations. Int J Dermatol. 2012;51(2):131–141. doi:10.1111/j.1365-4632.2011.05191.x
12. Jin-gang A, Sheng-xiang X, Sheng-bin X, et al. Quality of life of patients with scabies. J Eur Acad Dermatol Venereol. 2010;24(10):1187–1191. doi:10.1111/j.1468-3083.2010.03618.x
13. Scheinfeld N. Controlling scabies in institutional settings: a review of medications, treatment models, and implementation. Am J Clin Dermatol. 2004;5(1):31–37. doi:10.2165/00128071-200405010-00005
14. De Beer G, Miller MA, Tremblay L, et al. An outbreak of scabies in a long-term care facility: the role of misdiagnosis and the costs associated with control. Infect Control Hosp Epidemiol. 2006;27(5):517–518. doi:10.1086/504365
15. Karimkhani C, Colombara DV, Drucker AM, et al. The global burden of scabies: a cross-sectional analysis from the Global Bruden of Disease Study 2015. Lancet Infect Dis. 2017;17(12):1247–1254 doi:10.1016/S1473-3099(17)30483-8
16. Andersen BM, Haugen H, Rasch M, et al. Outbreak of scabies in Norwegian nursing homes and home care patients: control and prevention. J Hosp Infect. 2000;45(2):160–164. doi:10.1053/jhin.1999.0716
17. Skayem C, Majda A, Gary C, et al. Severe scabies: a French multi-centre study involving 95 patients with crusted and profuse disease and review of the literature. Acta Derm Venereol. 2023;103:adv00878. doi:10.2340/actadv.v103.5351
18. Mounsey KE, Murray HC, Bielefeldt-Ohmann H, et al. Prospective study in a porcine model of Sarcoptes scabiei indicates the association of th2 and th17 pathways with the clinical severity of scabies. PLoS Negl Trop Dis. 2015;9(3):e0003498. doi:10.1371/journal.pntd.0003498
19. Murakonda P, Yazdanbaksh K, Dharmarajan TS. Scabies in the nursing home, misdiagnosis means costs, and embarrassment: story of a centenarian smitten by scabies! J Am Med Dir Assoc. 2014;15(1):74–75. doi:10.1016/j.jamda.2013.11.002
20. Berger TG, Shive M, Harper GM. Pruritus in the older patient: a clinical review. JAMA. 2013;310(22):2443–2450. doi:10.1001/jama.2013.282023
21. Chng L, Holt DC, Field M, et al. Molecular diagnosis of scabies using a novel probe-based polymerase chain reaction assay targeting high-copy number repetitive sequences in the Sarcoptes scabiei genome. PLoS Negl Trop Dis. 2021;15(2):e0009149. doi:10.1371/journal.pntd.0009149
22. Salavastru CM, Chosidow O, Boffa MJ, et al. European guideline for the management of scabies. J Eur Acad Dermatol Venereol. 2017;31(8):1248–1253. doi:10.1111/jdv.14351
23. Panahi Y, Poursaleh Z, Goldust M. The efficacy of topical and oral ivermectin in the treatment of human scabies. Ann Parasitol. 2015;61(1):11–16.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.