")
Back to Journals » Patient Preference and Adherence » Volume 18
Fatalism as a Mediator of the Association Between Family Resilience and Self-Management Among Patients with Chronic Wounds in China
Authors Qiu Y , Fan S , Fu Q, Yang M, Zhu L
Received 3 November 2023
Accepted for publication 29 December 2023
Published 9 January 2024 Volume 2024:18 Pages 53—67
DOI https://doi.org/10.2147/PPA.S446219
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Yuhuan Qiu,1,2 Shujun Fan,1 Qiuyan Fu,1 Minlie Yang,2 Lihong Zhu2
1Wuxi School of Medicine, Jiangnan University, Wuxi, People’s Republic of China; 2Department of Burn and Plastic Surgery, Affiliated Hospital of Jiangnan University, Wuxi, People’s Republic of China
Correspondence: Minlie Yang, Department of Burn and Plastic Surgery, Affiliated Hospital of Jiangnan University, No. 1000 Hefeng Road, Binhu District, Wuxi, 214122, People’s Republic of China, Email [email protected]
Purpose: The purpose of this study was to examine how fatalism acts as a mediator in the correlation between family resilience and self-management among patients with chronic wounds in China.
Participants and Methods: This study used a cross-sectional research design. A total of 269 adult patients (18– 94 years old) with chronic wounds residing in Wuxi, China participated in this study. Participants completed the Chinese version of the Walsh Family Resilience Questionnaire, 16-item Chinese version of the Fatalism Scale, and Self-Management Scale of Chronic Wound Patients. We conducted correlation and mediation analyses using SPSS 27.0 and PROCESS 4.0.
Results: The results indicated family resilience was a significant positive predictor of self-management (β = 0.7101, p < 0.0001), and the pathway between family resilience and self-management was partially mediated by fatalism (Effect = 0.1432, 95% confidence interval [0.0625, 0.2341]).
Conclusion: The results indicated that incorporating spiritual interventions into future person-centered self-management programs could align with the motivation of patients with chronic wounds and their families, and reduce the negative impact of fatalism on health outcomes.
Keywords: chronic wounds, fatalism, family resilience, self-management, mediation
Introduction
In clinical practice, chronic wounds (CW), which are caused by various factors, are wounds that fail to progress toward healing within four weeks of applying standard care,1 such as diabetic foot ulcers, arterial or venous leg ulcers, and pressure injuries.2 With the increase in the aging population, obesity, diabetes, and other medical conditions, the incidence of chronic wounds has shown a concomitant increase. In China, compared with the results of an epidemiological investigation on chronic wounds in 1998, the current study3 showed that the average age of patients with CW has increased by 15.8 years, and the composition ratio of patients with chronic wounds during the years 2013–2017 was 2.4–3.9‰, which was higher than the global prevalence rate of 2.21‰ estimated by Martinengo et al.4 Chronic wounds are often complicated by comorbidities and varying etiologies leading to complex wound management and a prolonged course of treatment, which results in decreased quality of life and substantial economic and psychosocial costs.5,6
There is a consensus that care for chronic wounds needs to be simplified so that it can be patient-administered or provided by the family, and self-management has become an increasingly important part of the long-term management of chronic wounds since the start of the pandemic.1,7 Managing oneself is essential for the successful treatment of chronic diseases8 and is defined as the ability of a patient to control the symptoms of a disease through their own behavior, thereby reducing the impact of the disease on their health, psychosocial status, and lifestyle.9 Proper self-care can decrease instances of medical attention and cut down on medical costs, while also allowing patients to become more independent and enhance their overall wellbeing and health literacy.10–12 Previous research has indicated that individuals suffering from chronic wounds have various gaps in self-care knowledge and practice, and their self-management behaviors are often insufficient.13,14 Qualitative and quantitative studies have revealed that the self-care capacity of individuals with CW is linked to demographic factors (eg, age), physical factors (eg, wound size), psychological factors (eg, disgust), socioeconomic factors (eg, access to services and resources), and spiritual factors (eg, beliefs).8,15–18 Studies have also underscored the significance of family support in ensuring treatment compliance and concordance with self-care behaviors in individuals with CW.19,20
Family resilience, which is the capacity, procedure, and adaptation of a family to confront hardship, is considered an important factor in facilitating family caregivers’ implementation of long-term care for patients with chronic diseases.21,22 The concept of family resilience has its roots in the exploration of individual psychological resilience. However, more and more researchers were recognizing that the process of dealing with adversity on an individual level could apply to a process that involves the entire family system, which was reflected in their increasing emphasis on the importance of family support in disease management. Therefore, the research perspective gradually expanded from the individual level to the family level.23,24 For patients with CW, the primary dilemmas they confront are the direct and indirect repercussions of disease symptoms, treatment, and management, including ulcer and treatment-related pain; stigma and social isolation due to odor and exudate; activity restrictions (physical and social recreational activities) due to skin ulceration and wound dressing; dependence on family due to reduced self-care ability; anxiety about non-healing wounds; and fear of amputation.25–27 Although no previous studies have explored the family resilience of patients with CW, relevant studies on family support of patients with CW suggest that family resilience has an impact on self-management of patients with CW, because family resilience has been conceptualized as shared beliefs and support, strong family organization and positive interactions, and utilization of social resources, which are indicative of family support.28 Wantonoro et al19 concluded that strengthening the family support system for the management of diabetic ulcer care, such as improving family caregivers’ knowledge and self-efficacy through interdisciplinary education, can positively affect the self-care of patients with wounds both physically and psychologically. A recent systematic review by Huang et al29 suggested that home-based patient or informal caregivers’ interventions in managing chronic wounds at home can be effective in improving patient outcomes and changing self-care behavior. Hence, a connection exists between family factors and self-management in individuals with CW, and the impact of family resilience on the self-management among patients with CW needs further quantitative research investigation.
The impact of family resilience on self-management among patients with CW may not be immediate but could also have an indirect effect through fatalism. Accompanied by chronic diseases, patients and their families, in the long-term coping process, infer a variety of beliefs, cognitions, and understandings that are embedded in the family background. In the face of similar chronic diseases and different family patterns, the path of resilience often is not simply in response to the disease but indicates the cultural and social metaphors behind certain strategies to cope with distress.30 With changes in the medical model, psychological and social support for patients have gained increased attention, and researchers began focusing on patients’ perspectives, beliefs, and autonomy, and recommending the construction of patient-centered holistic care.31,32 Atkin et al33 noted that the major driver of success in managing chronic wounds was that patients followed the agreed upon care path with their health care professionals. In other words, health professionals must fully understand the patient’s belief system to tailor the plan in a way that they believe will be effective.
Fatalism is a common worldview in society, and fatalistic individuals believe life is the result of fate and that what happens in life is not controlled by personal behavior.34 They are often inactive, tend to have a negative outlook on future occurrences, and are more likely to disregard preventive measures.35 A sense of fatalism may develop with disease progression and have an impact on patients’ self-management behaviors. For example, Kamath et al36 found that fatalism was a negative determinant of self-care behavior among individuals suffering from chronic heart failure. Rustveld et al37 conducted focus groups with Latino men with diabetes on their belief systems and attitudes related to diabetes self-care. The participants expressed a strong sense of fatalism regarding the course of their disease, lacked motivation to adhere to self-care behaviors especially for long-term dietary control, and had strong negative attitudes toward changing their traditional dietary patterns. Their findings imply that fatalism, as a culturally influenced belief that could be embedded in family-level understandings of illness, may affect the self-care behaviors of patients with CW and be supported by the family. Masson et al38 pointed out that when implementing a patient-centered care plan for patients with CW, it is necessary to track the fatalism that may arise in patients from poor wound healing. However, there is a dearth of studies investigating the correlation between fatalism and self-management in individuals with CW, and no studies have examined whether fatalism plays a role in the relationship between family resilience and self-management among individuals with CW.
Social cognitive theory posits there is a dynamic interaction between one’s behavior, cognitions, and environment in which individual cognition is the core of the interaction.39 Therefore, this study aimed to elucidate the relationships between family resilience (environment), fatalism (cognition), and self-management (behavior) among patients with CW from the perspective of social cognitive theory. The results of the study would contribute to the development of self-management interventions for patients with CW consistent with a person-centered holistic care plan.
Based on the above, we examined the following hypotheses.
H1: Family resilience would be positively related to self-management. H2: Family resilience would be negatively related to fatalism. H3: Fatalism would be negatively related to self-management. H4: The relationship between family resilience and self-management would be mediated by fatalism.
Materials and Methods
Participants and Procedures
This study was designed as a cross-sectional survey. A total of 269 inpatients and outpatients with chronic wounds in the Burn and Trauma Treatment Center of the Affiliated Hospital of Jiangnan University in Wuxi, China participated in the study. Patients were recruited from April 2023 to September 2023 using convenience sampling. The inclusion criteria were as follows: meet the diagnostic criteria for chronic wounds in the Guidelines for the Diagnosis and Treatment of Chronic Wounds (revised 2011),40 including diabetic foot ulcers, traumatic wounds, arterial leg ulcers, venous leg ulcers, pressure injuries, and Infectious wounds; over 18 years old; able to communicate effectively; and able to complete the questionnaire independently or with the help of the investigator. The exclusion criteria were patients with mental illness, cognitive impairment, hearing dysfunction, or speech dysfunction. The research protocol was approved by the Jiangnan University Medical Ethics Committee (approval number: JNU20221201IRB16) and conducted in compliance with the ethical guidelines of the Declaration of Helsinki.
Data Collection
First, wound care nurses in the clinic, primary nurses on the ward, and three nursing graduate students were trained by the head nurse of the burn and trauma treatment center on patient recruitment. They were instructed on the inclusion and exclusion criteria and the consistent format to use when presenting the purpose of the study and content of the questionnaire to patients. Second, using the convenience sampling method, upon their first visit to the burn and trauma treatment center, patients who agreed to participate were assessed by one of the investigators on the team for inclusion in the study without filling the survey again in the future. The purpose of the study was communicated to each patient, and if the patient met the criteria, written informed consent was obtained at that time. Then, the participant completed the questionnaire under the guidance of the investigator. The investigator responded to any questions that the participant had regarding the questionnaire items or study. Third, after the exclusion of questionnaires that had missing or incomplete responses, three nursing graduate students input the data into EpiData Software 3.0 and double-checked the questionnaires to ensure the correctness of all data entry.
Measures and Variables
The survey instrument covered four primary sections: participant sociodemographic and clinical data, family resilience, fatalism, and self-management of chronic wounds. A questionnaire created by the investigator was utilized to acquire sociodemographic and clinical information, which comprised of gender, age, marital status, education level, religion, occupation, household, number of children, residence, monthly household income, smoking status, drinking status, number of comorbidities, type of wounds, number of wounds, wound size, wound duration, and Visual Analogue Scale (VAS) score.
The Walsh Family Resilience Questionnaire (WFRQ)41,42 was used to assess family resilience. We used the Chinese version of the WFRQ (WFPQ-C) which was translated by Wang et al.28 This scale has 26 items that comprise three dimensions: family belief system; organization, communication, and problem solving; and utilization of external resources. Items are responded to using a 5-point Likert scale, with a total score range of 26–130. Higher total scores reflect greater family resilience. Wang et al43 reported a Cronbach’s α of 0.97, of 0.962 in this study.
The 16-item Chinese version of the Fatalism Scale43 was used to measure fatalism. The translated scale is based on the Multidimensional Fatalism Scale for General Life Events, which was developed by Shen et al44 and revised by Piña-Watson et al.45 This 5-point Likert scale has 16 items and assesses the three dimensions of predetermination, luck, and pessimism, with higher ratings signifying a higher level of fatalism. The scale demonstrated good reliability (α = 0.84) and validity in the original study.44 The Cronbach’s α was 0.921 in our study.
The Self-Management Scale of Chronic Wound Patients developed by Chen15 has 26 items and five dimensions: wound management, nutrition management, life management, basic disease management, and emotion management. Items are responded to using a 5-point Likert scale, with 1 = none and 5 = always. Total scores range from 26–130, with higher scores indicating higher levels of self-management ability. The original instrument yielded a Cronbach’s α value of 0.899.15 Cronbach’s α was 0.950 in our study.
Statistical Analysis
Statistical analysis was performed using SPSS 27.0. Descriptive statistics were employed to analyze all data and scale scores. The chronic wound self-management level by diverse characteristics was assessed using a one-way ANOVA or t-test. After controlling for covariates, a partial correlation analysis was conducted to examine the correlations among the target variables. The prediction of self-management was investigated through the implementation of hierarchical multiple regression analysis, focusing on the impact of family resilience and fatalism. Ultimately, a bias-corrected bootstrapping analysis (5000 resamples) utilizing the PROCESS 4.0 was carried out to verify the mediating effect of fatalism.46 As shown in Figure 1, three regression models were performed to verify the mediating effect. Model 1 (path c) is the effect of family resilience, excluding fatalism, on self-management. Model 2 (path a) is the effect of family resilience on fatalism. Model 3 (paths b and c’) is the effect of fatalism and family resilience on chronic wound self-management. The mediating effect (path a*b, also known as the indirect effect) was deemed statistically significant if the 95% bootstrap confidence interval (CI) of the indirect effect did not exhibit a value of zero.47,48 Statistical significance was determined by a p-value < 0.05.
 |
Figure 1 Diagram of paths in the mediation model. |
Results
Participants’ Characteristics and Self-Management
Table 1 displays the descriptive statistics pertaining to participant sociodemographic and clinical characteristics. The participants ages ranged from 18–94 and included 169 (62.8%) men and 100 (37.2%) women. Most participants were older adults (≥60 years old, 76.6%), married (88.5%), and irreligious (88.8%). Almost half (46.5%) reported having a primary school education or below. There were significant differences in self-management according to age, education level, occupation, number of children, residence, household, monthly household income, number of comorbidities, type of wounds, wound size, wound duration, and VAS score (Table 1). No significant differences in self-management were observed according to gender, marital status, religion, smoking status, drinking status, and the number of wounds.
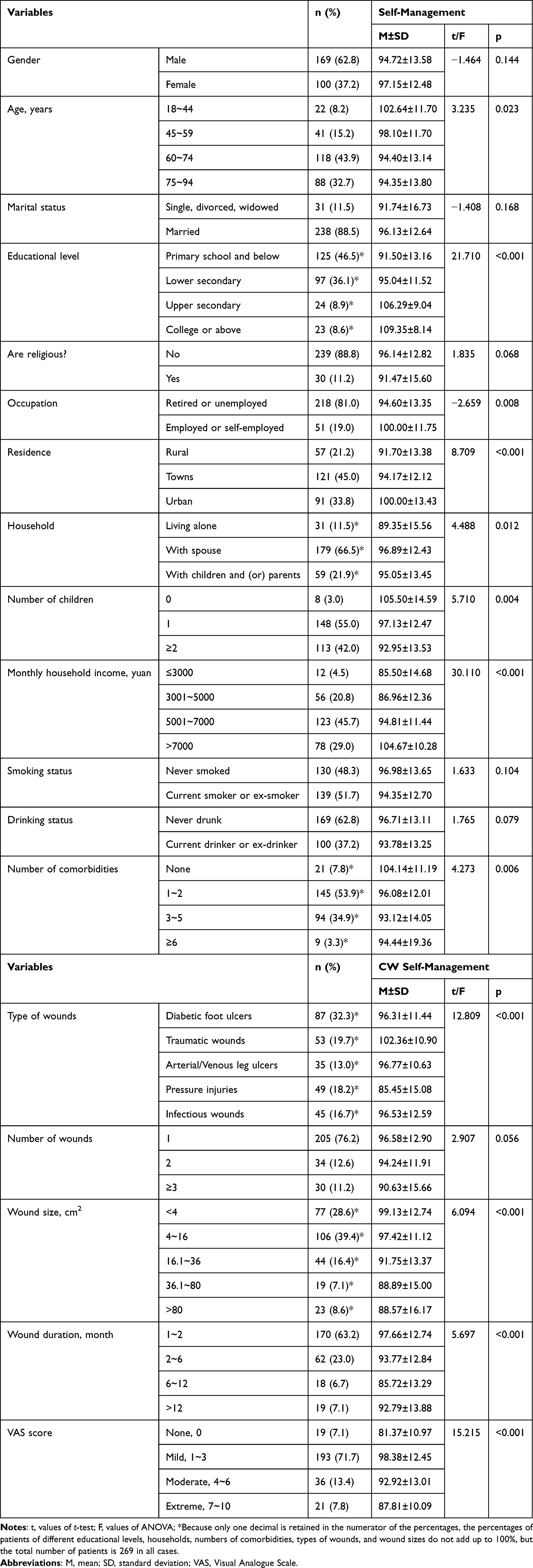 |
Table 1 Participant Sociodemographic and Clinical Characteristics, Differences in Self-Management by Characteristics (N=269) |
Descriptive Characteristics and Correlations Among the Target Variables
Descriptive statistics and correlations among the target variables are shown in Table 2. The mean score on the WFPQ-C was 91.53 ± 14.50 with a mean item score of 3.52 ± 0.56 (range is 1–5), indicating a medium level of family resilience. The mean Fatalism Scale score was 43.10 ± 10.36 with a mean item score of 2.69 ± 0.65 (range is 1–5), indicating a low to medium level of fatalism. The mean score on the Self-Management Scale of Chronic Wound Patients was 95.62 ± 13.21. The mean item score was 3.68 ± 0.51 (range is 1–5), indicating a medium level of self-management ability.
 |
Table 2 Descriptive Statistics and Correlations Among the Target Variables (N=269) # |
The correlation analysis showed that family resilience had a positive correlation with self-management (r = 0.823, p < 0.01) and a negative correlation with fatalism (r = −0.796, p < 0.01). Fatalism also negatively related to self-management (r = −0.775, p < 0.01). The regression analysis results are presented in Table 3. Family resilience was a significant positive predictor of self-management, making up 36.5% of the variance. Fatalism was a significant negative predictor of self-management, explaining an extra 1.7% of the variance. The findings suggested that fatalism was as a partial mediator and the association between family resilience and self-management decreased from 0.710 to 0.553 when fatalism incorporated into the model.
 |
Table 3 The Hierarchical Multiple Regression Analyses of Self-Management (N=269) |
Mediation Analyses
The results of the mediation analysis are shown in Table 4. Age, education level, occupation, number of children, residence, household, monthly household income, number of comorbidities, type of wounds, wound size, wound duration, and VAS score were covariates in the models. In Model 1, family resilience positively predicted self-management (β = 0.7101, p < 0.0001). In Model 2, family resilience negatively predicted fatalism (β = −0.6757, p < 0.0001). Model 3 revealed a strong correlation between self-management and both family resilience and fatalism, with the standardized regression coefficient for family resilience dropping to 0.5530.
 |
Table 4 Mediating Effects of Fatalism on the Relationship Between Family Resilience and Self-Management (N=269) # |
The findings of the mediating effect are presented in Table 5. The bootstrapped 95% CI for the indirect path was [0.0625, 0.2341], thereby validating the notion that the influence of family resilience, mediated by fatalism, had an indirect impact of 0.1432. 22.13% of the variance in the relationship between family resilience and self-management was due to fatalism. These findings corroborate our hypothesis that the relationship between family resilience and self-management would be mediated by fatalism. The final mediation model, along with the standardized path coefficients (a, b, c, c’), is displayed in Figure 2.
 |
Table 5 Mediating Model Examination by Bootstrap |
 |
Figure 2 Proposed models that investigate mediated effects. Notes: ***The correlation is significant at 0.001 (p<0.001). |
Discussion
The findings of this study indicated that the participants had a medium level of self-management ability, which is similar to the mean score reported in Zhang12 but lower than the mean reported in Chen.15 Thus, the self-management ability of patients with CW in our study needs to be improved. Since the pandemic, the self-management of patients with CW has gradually become the preferred model of care with some patients being required to perform self-management passively under limited resources; however, many patients have not qualified for self-care, which suggests an urgent need for adjustment and innovation in the model of care.11 There is a consensus that self-management models need to be patient-centered, making decisions with the patient to better fit the definition of positive health and empower the patients to face physical, mental, and social challenges.9 Therefore, we explored the internal and external factors that influence the level of self-management in patients with CW, consistent with previous qualitative and quantitative studies.17,49
The findings of this study indicated that patients with CW who had attained a higher level of education were more likely to possess greater self-management ability. It is possible that the disparity is due to the fact that more educated patients have higher levels of health literacy in processing, understanding, and acquiring health information for successful self-management.50 Furthermore, those with a higher level of education tend to have a greater sense of self-efficacy, and therefore may be more confident in self-management and the pursuit of independence.7 Some other internal factors that affected self-management were age, comorbidity, and wound condition. With regard to external factors, socioeconomic circumstances were associated with the ability of patients to take care of themselves to attain health outcomes. For instance, a prior research revealed that individuals residing in rural regions encountered transportation difficulties with relatively little access to wound care services, resulting in a postpone engagement in proper self-care.17 Our study confirmed the association of different places of residence with level of self-management ability. Additionally, family factors, such as living status, number of children, and monthly household income, were shown to be associated with self-management among patients with CW in our study.
The mean score for family resilience suggested a medium level of family resilience in our sample, slightly lower than the mean reported by Wang et al28 for Chinese community residents. With the development of positive psychology, family resilience as a family trait or a dynamic process that helps families relieve stress provides a new perspective for studying chronic diseases at the family level. Despite the lack of consensus among academics on the concept of family resilience, it is generally interpreted from three different angles. The competence-based perspective refers to the characteristics or ability of the family to adapt to stress and cope with a crisis.51,52 The process perspective concerns the dynamic process by which families use resources to cope with adversity and to adapt and develop.41,53 The outcome perspective focuses on the effects of family coping with a crisis and stress, manifested as the improvement of family relationships and abilities after experiencing adversity.54 Several core characteristics of family resilience theory can be summarized as follows: (1) threatened by stressful events or crises (2) the use of strengths and resources, (3) having a positive outlook in the face of adversity or crisis, and (4) empowerment of the family in the ability to repair itself and grow from adversity.55 We elucidated the result of an existing correlation between family resilience and self-management by resource utilization, positive perceptions, and empowerment. In terms of resource utilization, patients in families with high levels of resilience tend to be more able to utilize potential strengths and resources, including individual (eg, health literacy), family (eg, family support), and social (eg, leg clubs) resources.56–58 In terms of positive perceptions, family resilience guides family cognition and behavior patterns,55 and positive beliefs and family characteristics are protective factors in coping with stress.21 Patients who possess strong strengths of family resilience tend to receive greater emotional support from family members, cope with the disease with a more optimistic attitude, and adopt more active and effective self-management behaviors.59 In terms of empowerment, high-resilience families tend to have the knowledge and confidence to identify and establish family-friendly resources and utilize adaptive coping strategies,55 and contribute to self-efficacy and posttraumatic growth.19,60
The goal of most family resilience interventions implemented by nurses for patients with CW is to assist empowerment,19,61 that is, to promote family coping with the disease by providing external resources to enhance family well-being, support family functioning, and adjust family relationships. Family resilience is not only affected by the ability of family members, the availability of family resources and the strength of social support, but is also affected by macrosystems such as ethnic culture and beliefs.62 The phenomenological study of Hassani et al63 found that fatalism existed in the cognition of resilience among chronic patients, who believed that patience and trust in God was equal with resilience. The findings of this research indicated a significant negative association between family resilience and fatalism. The family can be an important natural support system, and family resilience can positively affect the cognitive style and emotional experience of family members,59 while the emergence of fatalism is closely related to the living environment and cognitive emotions of patients.64 Studies have shown that family resilience is significantly negatively correlated with anxiety and depression;45,65 consequently, family resilience may have an effect on the formation of fatalism by influencing anxiety and depression in patients with CW.
Fatalism, as a world view affecting patients’ cognition and coping behaviors with diseases, has been shown to be related to a variety of negative behaviors and adverse health outcomes.43 The results of this study showed that fatalism was significantly negatively related to self-management. An ethnographic study by Sari et al66 showed that Javanese patients were influenced by Islamic culture in their practice of diabetes self-management, believing that everything that happened was God’s will and that diabetes was a trial from God, which reflected the predetermination dimension of the Fatalism Scale. This disease perception can lead patients to have a negative attitude toward medical treatment and doubt the value of self-management in managing disease symptoms. Stiffler et al67 highlighted that self-management skills are not solely derived from the information provided, but rather from motivation and the aspiration to achieve better outcomes. Thus, it is crucial to take into account the internal motivation of patients with CW to uphold optimal self-management practices and prevent further complications when strategizing care for this demographic.17 Spiritual beliefs are thought to be a buffer or coping strategy that can help people change their fatalism.68 Studies have shown that spiritual interventions can reduce an individual’s fatalism.69,70 Thus, when developing a self-management plan for patients with CW, it is important to consider their cultural beliefs, such as fatalism, which could promote their motivation for self-management and improve their health outcomes.71
Innovation and Limitations
This is the first study to find that fatalism plays a partial mediating role in the relationship between family resilience and self-management in patients with CW using a quantitative methodology. With the development of positive psychology, many studies have identified the benefits of enhancing psychological resilience in chronic disease management;72 however, most studies have focused on individual psychological resilience.73,74 Based on the dynamic interaction between the individual’s behavior, cognitions, and environment posited in social cognitive theory,39 this study considered the environmental factor of family-centered self-management of patients with CW,29 focusing on family resilience, and analyzed the relationships between family resilience, fatalism, and self-management. Additionally, patients with CW have varied perceptions and beliefs about self-care that influence their self-care practices,31,75 and identifying patient motivation and cultural context may improve the consistency of their self-management behaviors.20 Therefore, we focused on fatalism as an individual cognition and variable for analysis. This research broadened our comprehension of fatalism and its association with the management of chronic illnesses, and provide new ideas for constructing person-centered self-management programs for patients with CW.
This study has certain limitations. First, this study utilized convenience sampling instead of random sampling, and the survey was only conducted in Wuxi, China where most residents were Han and had no religious affiliation. Thus, the generalizability of the results is limited. Second, the family resilience of patients’ informal caregivers was not assessed. As family resilience has been found to be positively associated with the support of relatives,76 the influence of informal caregivers on chronic disease management and their burden of long-term care cannot be ignored.7 Future investigations should include the informal caregivers of patients with CW. Moreover, the adaptation of patients with CW to their disease seems to be a dynamic process of coping with fluctuating life changes, and the cross-sectional design of the study does not allow for investigation of how coping behaviors influenced by fatalism change over time. While there are studies suggesting that fatalism is an attitude that leads to negative health outcomes,77 there are also some studies that have provided evidence of fatalism acting as a protective factor, helping individuals cope with illness in the context of specific cultural beliefs or resource constraints, and alleviating self-blame and other negative emotions.71,77 For example, in the context of Chinese culture, patients may develop fatalistic voluntarism in their long-term adaptation to disease, helping them to reduce or avoid guilt caused by events beyond their control, cope with stressful situations, and bolster an optimistic perspective to pursue a brighter future.78 However, the specific demographic and geographic focus of our study limited its generalizability due to China’s ethnic diversity and variations in cultural beliefs across different regions. Future researches should consider conducting longitudinal studies with diversified samples from multiple regions to enhance our understanding of the correlation between fatalism and self-management in patients with CW and their families.
Conclusion
Patients with CW had a moderate level of self-management ability. There was a positive relationship between family resilience and self-management and a negative relationship between fatalism and self-management, and family resilience indirectly influenced self-management through fatalism. Treatment of patients with CW should involve considering the cultural and religious context of the patient, reducing the negative impact of their fatalism on health outcomes through spiritual interventions, and developing person-centered self-management programs consistent with the motivation of the patient and their family.
Abbreviations
CW, chronic wounds; VAS, Visual Analogue Scale; WFRQ-C, the Chinese version of the Walsh Family Resilience Questionnaire.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author.
Ethics and Consent
The ethical consent was approved by the Jiangnan University Medical Ethics Committee (Approval number: JNU20221201IRB16). We confirm that a written informed consent was obtained from the study participants. The guidelines outlined in the Declaration of Helsinki were also followed.
Acknowledgments
We are very grateful to the people who gave help to this study. The participation of patients with chronic wounds in this study is gratefully acknowledged.
Funding
This work was supported by grants from the Top Talent Support Program for young and middle-aged doctor of Wuxi Health Committee (BJ2020046).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Eriksson E, Liu PY, Schultz GS, et al. Chronic wounds: treatment consensus. Wound Repair Regen. 2022;30(2):156–171. doi:10.1111/wrr.12994
2. Frykberg RG, Banks J. Challenges in the treatment of chronic wounds. Adv Wound Care. 2015;4(9):560–582. doi:10.1089/wound.2015.0635
3. Chen C, Yao Z, Chen K, Chen B. Epidemiological investigation on clinical characteristics of 801 inpatients with chronic wounds. Chin J Burns. 2020;36(5):388–394. doi:10.3760/cma.j.cn501120-20191231-00477
4. Martinengo L, Olsson M, Bajpai R, et al. Prevalence of chronic wounds in the general population: systematic review and meta-analysis of observational studies. Ann Epidemiol. 2019;29:8–15. doi:10.1016/j.annepidem.2018.10.005
5. Sen CK. Human wound and its burden: updated 2020 compendium of estimates. Adv Wound Care. 2021;10(5):281–292. doi:10.1089/wound.2021.0026
6. Jones RE, Foster DS, Longaker MT. Management of Chronic Wounds-2018. JAMA. 2018;320(14):1481–1482. doi:10.1001/jama.2018.12426
7. Bolton Saghdaoui L, Lampridou S, Racaru S, Davies AH, Wells M. Healthcare interventions to aid patient self-management of lower limb wounds: a systematic scoping review. Int Wound J. 2023;20(4):1304–1315. doi:10.1111/iwj.13969
8. Chen Z, Jiang Y, Chen M, Baiyila N, Nan J. Resilience as a mediator of the association between spirituality and self-management among older people with chronic obstructive pulmonary disease. Healthcare. 2021;9:12. doi:10.3390/healthcare9121631
9. van Riel P, Zuidema RM, Vogel C, Rongen-van Dartel SAA. Patient self-management and tracking: a European experience. Rheum Dis Clin North Am. 2019;45(2):187–195. doi:10.1016/j.rdc.2019.01.008
10. Callender LF, Johnson AL, Pignataro RM. Patient-centered education in wound management: improving outcomes and adherence. Adv Skin Wound Care. 2021;34(8):403–410. doi:10.1097/01.ASW.0000753256.29578.6c
11. Brown A. Managing chronic wounds in the community: should we be promoting self-care? Br J Healthcare Manage. 2022;28(5):138–140. doi:10.12968/bjhc.2022.0059
12. Zhang L Application Research of self-management strategy based on the King’s Theory of Goal Attainment in the outpatient chronic wound patients [dissertation]. Soochow University; 2022.
13. Manickum P, Mashamba-Thompson T, Naidoo R, Ramklass S, Madiba T. Knowledge and practice of diabetic foot care - A scoping review. Diabetes Metab Syndr. 2021;15(3):783–793. doi:10.1016/j.dsx.2021.03.030
14. Chin YF, Huang TT, Hsu BR, Weng LC, Wang CC. Factors associated with foot ulcer self-management behaviours among hospitalised patients with diabetes. J Clin Nurs. 2019;28(11–12):2253–2264. doi:10.1111/jocn.14822
15. Chen M The study of impact factor of Chronic Wound Patients’Selfmanagement [dissertation]. Jinan University; 2015.
16. Gaind S, Clarke A, Butler PE. The role of disgust emotions in predicting self-management in wound care. J Wound Care. 2011;20(7):346–350. doi:10.12968/jowc.2011.20.7.346
17. Costa IG, Tregunno D, Camargo-Plazas P. I cannot afford off-loading boots: perceptions of socioeconomic factors influencing engagement in self-management of diabetic foot ulcer. ANS Adv Nurs Sci. 2020;43(4):322–337. doi:10.1097/ans.0000000000000328
18. Zhu X, Lee M, Chew EA, Goh LJ, Dong L, Bartlam B. “When nothing happens, nobody is afraid!” beliefs and perceptions around self-care and health-seeking behaviours: voices of patients living with diabetic lower extremity amputation in primary care. Int Wound J. 2021;18(6):850–861. doi:10.1111/iwj.13587
19. Wantonoro W, Komarudin K, Imania DR, Harun S, Nguyen TV. The influence of 6-month interdisciplinary accompaniment on family caregivers’ knowledge and self-efficacy regarding diabetic wound care. SAGE Open Nurs. 2023;9:23779608231167801. doi:10.1177/23779608231167801
20. Bullen B, Young M, McArdle C, Ellis M. Overcoming barriers to self-management: the person-centred diabetes foot behavioural agreement. Foot. 2019;38:65–69. doi:10.1016/j.foot.2019.01.004
21. Kuang Y, Wang M, Yu NX, et al. Family resilience of patients requiring long-term care: a meta-synthesis of qualitative studies. J Clin Nurs. 2023;32(13–14):4159–4175. doi:10.1111/jocn.16500
22. Sorayyanezhad A, Nikpeyma N, Nazari S, Sharifi F, Sarkhani N. The relationship of caregiver strain with resilience and hardiness in family caregivers of older adults with chronic disease: a cross-sectional study. BMC Nurs. 2022;21(1):184. doi:10.1186/s12912-022-00966-3
23. Henry CS, Morris AS, Harrist AW. Family resilience: moving into the third wave. Fam Relat. 2015;64(1):22–43. doi:10.1111/fare.12106
24. McCubbin HI, McCubbin MA, Thompson AI, Thompson EA. Resiliency in ethnic families: a conceptual model for predicting family adjustment and adaptation. In: Resiliency in Native American and Immigrant Families Resiliency in Families Series. Vol. 2. Sage Publications, Inc; 1998:3–48.
25. Alves de Araújo W, Couto Assis W, Benemérita Alves Vilela A, Narriman Silva de Oliveira Boery R, Palmarella Rodrigues V, Montargil Rocha R. Meanings of living with a chronic wound: a meta-synthesis study. Significados de vivir con una herida crónica. 2020;18:1–13. doi:10.30886/estima.v18.936_IN
26. Phillips P, Lumley E, Duncan R, et al. A systematic review of qualitative research into people’s experiences of living with venous leg ulcers. J Adv Nurs. 2018;74(3):550–563. doi:10.1111/jan.13465
27. Ma L, Chen J, Sun Y, Feng Y, Yuan L, Ran X. The perceptions of living with diabetic foot ulcers: a systematic review and meta-synthesis of qualitative studies. J Tissue Viability. 2023;32(1):39–50. doi:10.1016/j.jtv.2022.11.005
28. Wang A, Lu J. Validation of the Chinese version of the Walsh family resilience questionnaire. Fam Process. 2023;62(1):368–386. doi:10.1111/famp.12751
29. Huang Y, Hu J, Xie T, et al. Effects of home-based chronic wound care training for patients and caregivers: a systematic review. Int Wound J. 2023. doi:10.1111/iwj.14219
30. Feng Y, Yang L. Family resilience and cultural consonance study. Hua Dong Li Gong Da Xue Xue Bao She Hui Ke Xue Ban. 2018;33(06):10–17.
31. Gethin G, Probst S, Stryja J, Christiansen N, Price P. Evidence for person-centred care in chronic wound care: a systematic review and recommendations for practice. J Wound Care. 2020;29(Sup9b):S1–s22. doi:10.12968/jowc.2020.29.Sup9b.S1
32. Fearns N, Heller-Murphy S, Kelly J, Harbour J. Placing the patient at the centre of chronic wound care: a qualitative evidence synthesis. J Tissue Viability. 2017;26(4):254–259. doi:10.1016/j.jtv.2017.09.002
33. Atkin L, Bućko Z, Conde Montero E, et al. Implementing TIMERS: the race against hard-to-heal wounds. J Wound Care. 2019;23(Sup3a):S1–s50. doi:10.12968/jowc.2019.28.Sup3a.S1
34. Peng YS, Wang CC. Fatalism of urinary bladder. Neurourol Urodyn. 2020;39(1):470–471. doi:10.1002/nau.24199
35. Valenti GD, Faraci P. Identifying predictive factors in compliance with the COVID-19 containment measures: a mediation analysis. Psychol Res Behav Manag. 2021;14:1325–1338. doi:10.2147/prbm.S323617
36. Kamath DY, Bhuvana KB, Salazar LJ, et al. A qualitative, grounded theory exploration of the determinants of self-care behavior among Indian patients with a lived experience of chronic heart failure. PLoS One. 2021;16(1):e0245659. doi:10.1371/journal.pone.0245659
37. Rustveld LO, Pavlik VN, Jibaja-Weiss ML, Kline KN, Gossey JT, Volk RJ. Adherence to diabetes self-care behaviors in English- and Spanish-speaking Hispanic men. Patient Prefer Adherence. 2009;3:123–130. doi:10.2147/ppa.s5383
38. Masson R, Vuagnat H, Uçkay I, Toutous-Trellu L, Prendki V. Infection of chronic wounds in elderly patients. Rev Med Suisse. 2017;13(582):1938–1944.
39. Graf AS, Cohn TJ, Syme ML. Social cognitive theory as a theoretical framework to predict sexual risk behaviors among older adults. Clin Gerontol. 2021;44(3):331–344. doi:10.1080/07317115.2020.1825584
40. Repair committee group TSoCMA. Guidelines for the Diagnosis and Treatment of Chronic Wounds (Revised 2011). Repair committee group TSoCMA; 2011.
41. Walsh F. Family resilience: a framework for clinical practice. Fam Process. 2003;42(1):1–18. doi:10.1111/j.1545-5300.2003.00001.x
42. Walsh F. Applying a family resilience framework in training, practice, and research: mastering the art of the possible. Fam Process. 2016;55(4):616–632. doi:10.1111/famp.12260
43. Zhang X, Zuo B, Zhao Y. Revision of the Chinese version of fatalism scale. Zhongguo Lin Chuang Xin Li Xue Za Zhi. 2018;26(05):914–917. doi:10.16128/j.cnki.1005-3611.2018.05.017
44. Shen L, Condit CM, Wright L. The psychometric property and validation of a fatalism scale. Psychol Health. 2009;24(5):597–613. doi:10.1080/08870440801902535
45. Piña-Watson B, Abraído-Lanza AF. The intersection of Fatalismo and pessimism on depressive symptoms and suicidality of Mexican descent adolescents: an attribution perspective. Cultur Divers Ethnic Minor Psychol. 2017;23(1):91–101. doi:10.1037/cdp0000115
46. Hayes AF, Rockwood NJ. Regression-based statistical mediation and moderation analysis in clinical research: observations, recommendations, and implementation. Behav Res Ther. 2017;98:39–57. doi:10.1016/j.brat.2016.11.001
47. Mackinnon DP, Warsi G, Dwyer JH. A simulation study of mediated effect measures. Multivariate Behav Res. 1995;30(1):41. doi:10.1207/s15327906mbr3001_3
48. Preacher KJ, Hayes AF. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav Res Methods Instrum Comput. 2004;36(4):717–731. doi:10.3758/bf03206553
49. Nasirin C, Lionardo A, Nurzani A. Effectiveness of self-concept management of patients with depression in diabetic ulcer. Curr Diabetes Rev. 2022;18(7):e211221199215. doi:10.2174/1573399818666211221150345
50. Weller CD, Team V, Probst S, et al. Health literacy in people with venous leg ulcers: a protocol for scoping review. BMJ Open. 2021;11(5):e044604. doi:10.1136/bmjopen-2020-044604
51. Mccubbin MA, Mccubbin HI. Resiliency in families: a conceptual model of family adjustment and adaptation in response to stress and crises. Fam Assess. 1996;1:64.
52. Patterson JM. Understanding family resilience. J Clin Psychol. 2002;58(3):233–246. doi:10.1002/jclp.10019
53. Hawley DR, DeHaan L. Toward a definition of family resilience: integrating life-span and family perspectives. Fam Process. 1996;35(3):283–298. doi:10.1111/j.1545-5300.1996.00283.x
54. Black K, Lobo M. A conceptual review of family resilience factors. J Fam Nurs. 2008;14(1):33–55. doi:10.1177/1074840707312237
55. Yao J, Qiu S. Theoretical dispute, practical evolution and realistic mirror of family resilience. J Humanit. 2018;11:116–128. doi:10.15895/j.cnki.rwzz.2018.11.015
56. Wang D, Sun X, He F, Liu C, Wu Y. The mediating effect of family health on the relationship between health literacy and mental health: a national cross-sectional survey in China. Int J Soc Psychiatry. 2023;69(6):1490–1500. doi:10.1177/00207640231166628
57. Reyes J, Tripp-Reimer T, Parker E, Muller B, Laroche H. Factors influencing diabetes self-management among medically underserved patients with type II diabetes. Glob Qual Nurs Res. 2017;4:2333393617713097. doi:10.1177/2333393617713097
58. Abu Ghazaleh H, Artom M, Sturt J. A systematic review of community leg clubs for patients with chronic leg ulcers. Prim Health Care Res Dev. 2018;
59. Hou Y, Yang L, Zhang B, Han Y, Zhang Y, Zhao Q. Study on the mediating effect of fatalism in family resilience and self-management of lung neoplasms patients undergoing chemotherapy. Chin J Prac Nurs. 2022;38(36):2830–2837. doi:10.3760/cma.j.cn211501-20220126-00262
60. Park JH, Lee JS. Predictors of post-traumatic growth in young adult burn survivors. Burns. 2022;48(4):744–752. doi:10.1016/j.burns.2021.08.018
61. Subrata SA, Phuphaibul R, Grey M, Siripitayakunkit A, Piaseu N. Improving clinical outcomes of diabetic foot ulcers by the 3-month self- and family management support programs in Indonesia: a randomized controlled trial study. Diabetes Metab Syndr. 2020;14(5):857–863. doi:10.1016/j.dsx.2020.05.028
62. Ye M, Zhou L, Zhang W. Research progress on influencing factors of patients’ family resilience and its implications to nursing research. Chin Nurs Manag. 2021;21(09):1423–1427. doi:10.3969/j.issn.1672-1756.2021.09.030
63. Hassani P, Izadi-Avanji FS, Rakhshan M, Majd HA. A phenomenological study on resilience of the elderly suffering from chronic disease: a qualitative study. Psychol Res Behav Manag. 2017;10:59–67. doi:10.2147/prbm.S121336
64. Sukkarieh-Haraty O, Egede LE, Abi Kharma J, Bassil M. Diabetes fatalism and its emotional distress subscale are independent predictors of glycemic control among Lebanese patients with type 2 diabetes. Ethn Health. 2019;24(7):767–778. doi:10.1080/13557858.2017.1373075
65. Nabors LA, Graves ML, Fiser KA, Merianos AL. Family resilience and health among adolescents with asthma only, anxiety only, and comorbid asthma and anxiety. J Asthma. 2021;58(12):1599–1609. doi:10.1080/02770903.2020.1817939
66. Sari Y, Yusuf S, Kusumawardani LH, Sumeru A, Sutrisna E. The cultural beliefs and practices of diabetes self-management in Javanese diabetic patients: an ethnographic study. Heliyon. 2022;8(2):e08873. doi:10.1016/j.heliyon.2022.e08873
67. Stiffler D, Cullen D, Luna G. Diabetes barriers and self-care management: the patient perspective. Clin Nurs Res. 2014;23(6):601–626. doi:10.1177/1054773813507948
68. Franklin MD, Schlundt DG, McClellan LH, et al. Religious fatalism and its association with health behaviors and outcomes. Am J Health Behav. 2007;31(6):563–572. doi:10.5555/ajhb.2007.31.6.563
69. Hamilton JB, Worthy VC, Moore AD, Best NC, Stewart JM, Song MK. Messages of hope: helping family members to overcome fears and fatalistic attitudes toward cancer. J Cancer Educ. 2017;32(1):190–197. doi:10.1007/s13187-015-0895-z
70. Kestenbaum A, Shields M, James J, et al. What impact do chaplains have? A pilot study of spiritual AIM for advanced cancer patients in outpatient palliative care. J Pain Symptom Manage. 2017;54(5):707–714. doi:10.1016/j.jpainsymman.2017.07.027
71. Berardi V, Bellettiere J, Nativ O, Ladislav S, Hovell MF, Baron-Epel O. Fatalism, diabetes management outcomes, and the role of religiosity. J Relig Health. 2016;55(2):602–617. doi:10.1007/s10943-015-0067-9
72. Kim GM, Lim JY, Kim EJ, Park SM. Resilience of patients with chronic diseases: a systematic review. Health Soc Care Community. 2019;27(4):797–807. doi:10.1111/hsc.12620
73. Jin Y, Bhattarai M, Kuo WC, Bratzke LC. Relationship between resilience and self-care in people with chronic conditions: a systematic review and meta-analysis. J Clin Nurs. 2023;32(9–10):2041–2055. doi:10.1111/jocn.16258
74. Kuang D, Gu DF, Cao H, et al. Impacts of psychological resilience on self-efficacy and quality of life in patients with diabetic foot ulcers: a prospective cross-sectional study. Ann Palliat Med. 2021;10(5):5610–5618. doi:10.21037/apm-21-967
75. Oni D. Foot self-care experiences among patients with diabetes: a systematic review of qualitative studies. Wound Manag Prev. 2020;66(4):16–25. doi:10.25270/wmp.2020.4.1625
76. Li X, Li H. Reliability and validity of the Chinese version of the revised Walsh family resilience questionnaire. Ann Palliat Med. 2021;10(8):8709–8717. doi:10.21037/apm-21-1152
77. Keeley B, Wright L, Condit CM. Functions of health fatalism: fatalistic talk as face saving, uncertainty management, stress relief and sense making. Sociol Health Illn. 2009;31(5):734–747. doi:10.1111/j.1467-9566.2009.01164.x
78. Cheng H, Sit JW, Twinn SF, Cheng KK, Thorne S. Coping with breast cancer survivorship in Chinese women: the role of fatalism or fatalistic voluntarism. Cancer Nurs. 2013;36(3):236–244. doi:10.1097/NCC.0b013e31826542b2
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.