")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 15
Factors Influencing ART Adherence Among Persons Living with HIV Enrolled in Community Client-Led Art Delivery Groups in Lira District, Uganda: A Qualitative Study
Authors Isabirye R, Opii DJ , Opio Ekit S, Kawomera A, Lokiru L , Isoke R , Ssenkaali J, Puleh SS
Received 30 March 2023
Accepted for publication 9 June 2023
Published 15 June 2023 Volume 2023:15 Pages 339—347
DOI https://doi.org/10.2147/HIV.S414971
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Rogers Isabirye,1 Didan Jacob Opii,1 Sharon Opio Ekit,2 Alice Kawomera,2 Luke Lokiru,3 Robert Isoke,1 Joachim Ssenkaali,4 Sean Steven Puleh3
1Department of Midwifery and Nursing, Faculty of Health Sciences, Lira University, Lira, Uganda; 2Department of Psychiatry, Faculty of Medicine, Lira University, Lira, Uganda; 3Department of Epidemiology and Biostatistics, Faculty of Public Health, Lira University, Lira, Uganda; 4Department of Physiology, Faculty of Medicine, Lira University, Lira, Uganda
Correspondence: Sean Steven Puleh, Department of Epidemiology and Biostatistics, Faculty of Public Health, Lira University, P.O Box 1035, Lira City, Uganda, Email [email protected]
Background: Community client-led ART delivery groups (CCLADs) were introduced as one of the strategies to better serve individual needs and reduce unnecessary burdens on the health system. However, limited data adequately explained the factors influencing ART adherence among HIV/AIDS patients in CCLAD’s model of care. The study aimed to assess the factors influencing ART adherence among HIV-positive patients attending CCLADs in Lira District, Uganda.
Materials and Methods: We employed a qualitative method of data collection recruiting 25 study participants (expert clients) between July and August 2020. The study purposefully chose 25 participants to participate in with HIV/AIDS patients enrolled in community-based HIV care models. The interviews were recorded on audiotape, transcribed, and translated verbatim. We used a thematic approach to analyze the data.
Results: Our study shows that social support among group members, patient self-motivation, counselling, and guidance were the major facilitators of adherence. From the analysis of results, our study found the following themes: Lack of food, stigma, forgetfulness, stress, unfair staff at the hospital, and socio-cultural beliefs were among the major barriers identified in this study.
Conclusion: The study emphasizes that CCLADs improve ART adherence for HIV-positive clients by providing a supportive environment and medication access. Peer influence on alternative medicine usage hinders adherence. We recommend that continued support, funding, and education are necessary to address misconceptions and sustain CCLADs’ effectiveness.
Keywords: community client-led ART delivery, barriers, facilitators, HIV/AIDS
Background
Globally, 38.4 million [33.9 million–43.8 million] people are reported living with HIV in 2021.1 CCLADs according to this study are community-based models of care that empower HIV-positive clients to form peer-led groups where they collectively support and assist each other in various aspects of HIV treatment and care. The initiative plays a crucial role in achieving the UNAIDS 95-95-95 target, which aims to ensure that 95% of the persons living with HIV are enrolled into care and virally suppressed by 2030.1 According to the Uganda Aids Commission (2022) fact sheet report, 1.4 million people in Uganda were living with HIV and AIDS.2 In the same year, 96% of people living with HIV (PLWHIV) were on treatment, but only 92% were virally suppressed.2 Full ART adherence is central to good treatment outcomes; however, it still remains a challenge among HIV positive patients to date.3
In Uganda, ART service delivery puts a lot of pressure on the health system, which translates into higher cost, congestions, and long waiting times due to the long waiting lines.4 The World Health Organization (WHO) and major donors recommended differentiated HIV service delivery as a novel evidenced based strategy to promote meaningful involvement of PLWHIV, and to enhance patients’ self-management.5 The CCLADs have been implemented as one of the differentiated service delivery (DSD) model since 2017 by the Ministry of Health.6,7
The CCLADs are thought to bring treatment closer to patients, best serving the increasing number of HIV patients while decreasing undue burden on the HIV treatment system8 and improving adherence. According to this study adherence refers to the extent to which individuals living with HIV consistently follow their prescribed ART regimen. Each CCLAD group consists of between 4 and 6 HIV positive patients who come from the same community. An expert client is identified by group members and made the group leader. An expert client refers to an individual living with HIV who has received training and support to provide peer-based services and support to other individuals living with HIV.9 The collection of ART regiments at each refill for all the group members from the facility is done by only one member who then distributes to the others. However, there is limited information on how well CCLADs have addressed the critical issues in improving adherence as a method aimed at improving treatment outcomes. In addition, HIV differentiated care might be influenced by many factors such as complexity around patient’s preferences among others.5,6,9 It is against this background that this study assessed the factors influencing ART adherence among persons living with HIV/AIDS in Lira District, Uganda. A preprint has previously been published in research Gate.10
Materials and Methods
Study Design/Setting
We conducted a qualitative study to explore the perspectives of PLWHIV in CCLADs regarding factors influencing ART adherence between July and August 2020. We conducted the study at Lira City and district, northern Uganda. Lira Regional Referral Hospital located in Lira City was used as the entry point because they have all the records of the clients in CCLADs. Lira Regional Referral Hospital; has 12,275 HIV/AIDS clients currently on HAART and 219 HIV positive patients in 36 CCLAD groups.11 To qualify as an expert client, a person must have at least 24 months of ART experience, excellent adherence (virally suppressed at or below 1000 copies/mL of blood), and training in basic psychosocial support for other patients. Lira is located approximately 340 kilometers from Kampala by road, the capital city of Uganda. The Lira district is part of the Lango sub-region. The district is bordered to the northeast by Otuke district, to the north by Pader district, to the southeast by Dokolo district, to the east by Alebtong district, to the southwest by Kwania district, and to the west by Kole district.
Study Population and Sample Size Estimation
We studied adult HIV positive patients referred to as expert clients receiving ART in the CCLAD models at LRRH. Expert Clients are cadres of HIV-positive persons who use their own personal experience living with HIV to help others overcome the many challenges that come with an HIV-positive diagnosis to improve adherence.12 The information saturation principle was used to estimate a sample size of 25 participants for a thorough understanding of the phenomenon. Interviews were conducted until a complete range of responses was obtained, and additional interviews yielded no new information.13 The expert clients were recruited in the study if they were at least one adult aged 18 years or older and agreed to provide informed consent for the interviews. The expert clients were excluded if they were sick and unable to be interviewed.
Sampling Criteria
We chose LRRH on purpose because it contained records for all PLWHIV receiving care through CCLADs in Lira district, northern Uganda. The expert clients were purposefully chosen as participants based on characteristics or qualities that will allow for a thorough understanding of factors influencing ART adherence among PLWHIV in CCLADs. The key characteristic considered in this study was because they have a wealth of information about their experiences receiving services through the CCLAD model. Expert clients according to this study are HIV-positive men and women who use their own experiences living with HIV to help others overcome the many challenges that come with being HIV-positive. The participants were contacted by phone, and an appointment to meet with them in the community was set up. Those who met the eligibility requirements were chosen.
Data Collection, Tools and Method
The study research assistants of social sciences training were recruited. They were trained on the study protocol, as well as tools for one day. The research assistants conducted interviews among people living with HIV in their homes in private, in the Lango language, for an average of 30 minutes. The interviewers took the time to get to win the trust of the respondents so they could open up about their experiences. The interviewers asked the questions while observing the participants’ body language. Key informant interview guide was used to collect data from the respondents. The interviews were conducted with the participants, and the audio was recorded, and additional fieldnotes taken during the interviews. The interviews were conducted in the language best understood by the respondents (English or Luo). The interviews took an average of 30 minutes each.
Data Management and Analysis
The qualitative data was recorded in audio recorders during interviews and was transcribed in the respective languages. Those in the local language Langi were then translated into English. The transcripts were read multiple times for data familiarization.14 The data were coded manually, and the codes were merged following consensus from the authors of the study, then summarized into themes. Thematic analysis was done based on major themes that emerged from the responses obtained during the interviews.
Ethics Approval and Consent to Participate
The authors confirm that the approvals were sought from appropriate institutions and that all methods in this study were performed in accordance with the relevant guidelines and regulations. The study protocol was reviewed and cleared by the Gulu University Research Ethics Committee (GUREC-048-20). The protocol was further cleared for collection of data in Uganda by the national research regulator, the Uganda National Council of Science and Technology (RESCLEAR/01). Administrative clearance for this study was obtained from the district health officer of Lira district and the hospital administration of LRRH. Written informed consent was obtained from all study participants according to the Declaration of Helsinki for interviews, audio recording and publication of anonymised responses. None of the participants were below 18 years of age.
Results
Characteristics of Respondents
In our study, of the 25 group heads of CCLADs, majority, 64% (16/25), of the respondents are males and 64% (16/25) were married. In addition, the majority, 60% (15/25), of those who participated only had completed primary education and 76% (19/25) were dependent on subsistence farming (Table 1).
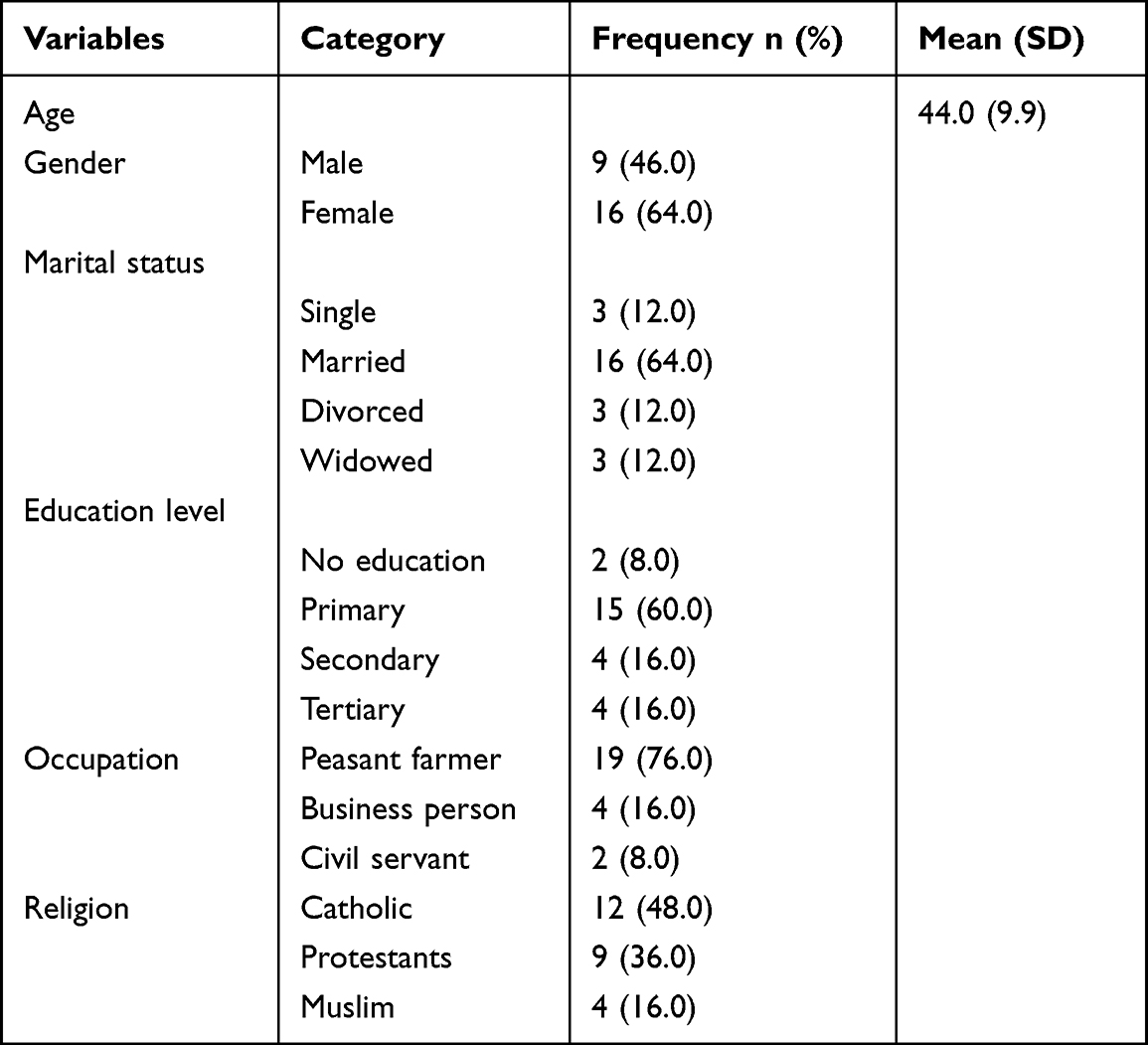 |
Table 1 The Socio-Demographic Characteristics of the Participants in CCLADs in Lira (n = 25) |
ART Adherence Among HIV-Positive Clients in CCLAD in Lira District
Majority of the participants reported that CCLADs improved ART adherence since there is group support. Accordingly, CCLADs had many benefits, although some participants narrated some challenges related to being in care while in the CCLAD-differentiated model of care. These are presented as a mixed narrative of the factors influencing ART adherence from the themes that emerged from the data. Enablers are defined in this study as benefits qualified by those in the CCLAD groups that may directly result in increased ART adherence. The barriers are considered as factors that negatively affect adherence among the members of the CCLADs.
Healthcare Worker–Client Relationship
Majority of the respondents reported mixed feelings about how they were treated by health workers. During drug refills and clinical appointments, the majority of respondents said they got along well with the health workers. Some reported that health workers treated them unfairly, which may discourage them from remaining in care. Some had the following to say regarding treatment by the health workers:
……. Medical personnel who could follow me up because at that time they could really care for those with HIV. I could shed tears whenever I see that nurse. It was a Dr. who convinced me and I started again and I realized I could live again and I continued till now. (Female, R02, 45 years)
It is that nurse I got in …………. who helped me because she took me by hand to the clinical room and gave me my medication. (Female, R15, 34 Years)
Some of the KIs pointed out that they were being mistreated such as being shouted at by the health workers. One of the respondents had the following to say….
When I started taking ARVs, I did not want to continue because I found a nurse who shouted at me in the presence of my daughter and I left taking it for one year. And yet I had to pick drugs from my friends. (Female, R02, 45 years)
Saving Transport Cost
Most of the participants reported that adherence to ART has numerous benefits. The majority of the key informants had similar views that CCLADs have enabled clients to access the drugs conveniently, saving them transport cost. The clients further reported that, by pooling resources, clients can share the cost of transportation, making it more affordable for everyone. Some of the views have been shared as quoted below;
……. we always have turns for each person to collect our medication from the hospital. So, if it is your turn, we collect 500/= shillings each to give a person going to collect our medication. However, for other people, I do not know how it can prevent them because am always at my home here and if it is my turn of going to the hospital, I just go and pick drugs for all and we save money. (Female, R14, 31 years)
Some people had started to fear going to the hospital because of covid-19 lockdown but I would like to thank the hospital for making the ARV refill near us. This was really a problem to us because we could go and if not having a mask would be a challenge. (Female, R7, 33 years)
Benefits of ART Adherence
The majority of participants stated that adhering to ART has numerous advantages. The majority of key informants agreed that CCLADs had helped clients stick to treatment. A significant number of respondents stated that the drugs are brought to the clients’ homes and they rarely miss taking them, resulting in better adherence. Here are a few examples of quotes:
I realized the goodness of this drug because it was making me stronger and healthier. The drugs are brought nearer and I keep on taking ARVs because it is making me able to live, pay school fees, and farm. (Male, R3, 53 years)
The support I get from the group makes HIV medication easy. When we meet, we remind each other about the importance of taking the drugs…….it has made me happy since it has given me a longer life. I never liked this drug in the beginning because I did not know that I was HIV positive. (Female, R9, 37 years)
Religious Influence
In addition, the influence of the religious leaders was also reported by some of the participants. A number of participants reported that religious leaders are very strong pillars in their lives. Some of the respondents reported that they would consult religious leaders with the hopes of getting healed. One of the participants was quoted as follows:
Sometimes our group go to the pastor to pray for us with belief we shall get healed or God can make it easy to live with AIDS. At first, we abandoned taking the drugs with hopes of getting healed and one of us nearly died when she got very sick. (Female, R13, 54 years)
Peer Influence to Use of Alternative Medicine
A number of HIV-positive patients in CCLADs reported that group members influenced them to use alternative medicine (traditional herbs) to cure HIV as a belief and practice that impeded consistent ART adherence. Some of the participants died as a result of using alternative medicine. This view was reported by some of the respondents as quoted below;
There was a friend of mine in the group who said they are not supposed to take a particular drug for so long, and she went to an herbalist and started taking herbs, abandoning ARVs, and she died. (Female, R6, 53 years)
Another respondent said those without knowledge of treatment options in the group still use the harmful traditional methods to cure HIV which can negatively influence ART adherence. He reported
…………. Still stuck on cultural ways and beliefs such as using traditional herbs for curing HIV which can discourage him/her from taking their ARVs. (Male, R22, 45 years)
Stigma
However, some of the clients in the CCLADs pointed out that being in groups leads to stigma. Some participants reported that there are affiliates in the group who share groupmate’s status with other members of the community. Then, everyone will get to know that you are living positively which can increase stigma. Some of the quotations are as shown below.
Because of fear of stigma, some men living with HIV who are not in CCLADs avoid refilling their ARVs. As a result, they begin to share ARVs with their wives in CCLADs. This causes these women to miss taking their ARVs because the medications run out before their refill dates. (Female, R15, 34 Years)
Sometimes people can point out to us that we are taking HIV medication, and this can anger us. (Female, R11, 52 years)
Conflict in the Group
Some participants reported bad conversations among group members, which can lead to poor adherence. A good personal focus on treatment was reported as a strategy to ensure group members’ adherence and to take medications as an essential part of their daily lives. This viewpoint was shared by some of the respondents as quoted below:
The people in the group I interact with talk bad about each other, but cannot stop me, but encourage me. That is how I have been living because I don’t even take alcohol. (Male, R1, 45 years)
However, on the other hand, some of the respondents reported being infuriated by others in the group. It was reported that when the group members lack understanding amongst themselves it leads to conflicts which affect adherence to the drugs. A huge number of the respondents reported being infuriated by the associates in the group due to negative talk. Some of the participants had the following to say:
My thoughts prevented me from taking my medication in the past because if you are upset by someone in the group and you are also sick, you can be annoyed and easily stop taking your medication and offer to die. (Male, R25, 62 years)
Discussion
The study revealed important findings regarding ART adherence among HIV-positive clients in CCLADs in Lira district. Participants reported that CCLADs improve adherence through group support, but challenges such as healthcare worker–client relationships, peer influence, religious leaders, conflicts, and stigma hinder adherence.
The benefits of being in a community client-led ART delivery group in low-resource settings are numerous. Our results in this study show that community client-led ART delivery groups (CCLADs) can improve adherence to treatment, retention in care, and reduce healthcare costs. An earlier study found that CCLADs significantly reduced costs associated with HIV care.9 First, these groups provide a support system for PLHIV who may face stigma and discrimination in their communities. Our results further show that being a part of a group of people who share similar experiences can help reduce the isolation and loneliness that PLHIV may feel. Similar studies have shown that adherence rates were higher in groups where clients were involved in the distribution and administration of ART drugs than in those where healthcare providers were responsible for the entire process.8,15,16
In low-resource settings, where access to healthcare is limited, community-led ART delivery groups can provide a supportive environment for PLHIV and improve their overall health outcomes. Being part of a supportive community can positively influence health, adherence to ART, and overall health outcomes of people living with HIV (PLHIV). Several studies have highlighted the benefits of community-based interventions. The result from this study is consistent with other evidence highlighting the importance of social support in community client-led ART delivery groups and suggests that such groups can facilitate social support among PLWHIV.17,18 These findings underscore the importance of developing and supporting community client-led ART delivery groups in low resource settings.
Furthermore, participants in this study had similar views that CCLADs have enabled them to access the drugs conveniently and saving them in transport cost. This is due to the fact that transport costs can be a significant barrier to accessing healthcare services in many low-income countries.8 Especially in rural and remote areas, clients may have to travel long distances to reach health facilities, which can be expensive. Our results are in agreement with evidence from elsewhere, where patients participating in the CCLAD model valued the opportunity to share the burden of ART refill pick-up transportation costs from facilities.7,19
Our results show that, CCLADs save clients time and other resources which have ability to improve adherence. Our findings are in agreement with a study that found that CCLADs reduce patient travel time and costs associated with receiving care.18 Additionally, congestion and long waiting times at points of care can also lead to missed appointments and poor follow-up care, further exacerbating the negative impact on patient outcomes. Similar findings were echoed in a study conducted elsewhere and in Uganda which found that congestion and long waiting times were common challenges faced by community client-led ART delivery groups.17,20 The study found that these challenges led to frustration and dissatisfaction among patients, which could potentially lead to poor adherence to ART and subsequent treatment failure. A possible reason could be due to the context in which these studies were conducted.
Our findings revealed that some PLWHIV in CCLADs seek treatment from religious leaders and alternative medicine in the hope of being healed. The findings are similar to those of another study, which discovered that some respondents believed that prayer can indeed heal HIV.21 Furthermore, another study identified religious leaders as key stakeholders in the HIV/AIDS fight, despite their role being limited by a lack of training, inadequate equipment, and facilitation to carry out HIV prevention programs.22 This could be due to the similarity of the population and the context. The role of the religious leaders and key individuals in the group who may have influence can negatively impact on adherence to ART. Nonetheless, most antiretroviral treatment (ART) programs in this region continue to struggle with poor adherence to therapy due to client factors such as religious beliefs.23 Furthermore, evidence from elsewhere also suggests that some individuals have preference for traditional medication (herbs) which have the potential to compromise the adherence to ART.24
Community client-led ART delivery groups can reduce stigma is by providing a safe and supportive environment for people to share their experiences and challenges with HIV/AIDS and take control of their treatment. In our study, we found that CCLADs remarkably reduced stigma. A possible reason could be that community client-led ART delivery groups provide a safe and supportive environment for peer support and education, empowering individuals living with HIV/AIDS. Our finding is consistent with the result from a study where individuals recognize the fact that the model improves their medication devotion and enhances their capacity to be productive workers and considers taking responsibility for their families.25 However, the study conducted elsewhere found that fear of stigma was one of the barriers to adherence.26
While community client-led groups can be effective in reducing transport costs and improving access to healthcare, conflicts can arise within these groups. Our finding shows that conflict in community client-led ART delivery groups can have negative consequences for both the group and the clients they serve. This could be due to difference in priorities/interest within group members or an unhealthy dynamic, where certain individuals exert disproportionate control or influence over decision-making processes. Similar findings were found in a study which showed that some clients voiced a lack of unity among individuals, as well as some patients are hesitant to form CCLAD groups as they may not know one another at first and are afraid of conflicting in the society.18 By addressing conflicts early on and promoting collaboration and shared decision-making, community client-led groups can continue to serve their clients effectively and promote equitable access to healthcare services.
Strengths and Limitations of the Study
The current study had some strengths. The study identified several facilitators of CCLADs, including positive relationships with healthcare workers and social support from group members. Participants reported that good treatment by healthcare workers encourages them to adhere to their medication, while social support from group members creates a strong support network that provides various benefits, including cost-sharing and access to drugs during COVID-19 lockdowns. Religious leaders were also identified as influential in some cases, while peer influence to use of alternative medicine was reported as a significant barrier to ART adherence. Our study had some limitations. This study was only conducted on CCLADs in one health facility, which could affect the generalizability of the findings. There is a potential impact of interviewer bias on participant responses, but we believe it is minor in comparison to the knowledge generated in this article.
Conclusion
Overall, the study underscores the importance of CCLADs as a model of care for HIV-positive clients in improving ART adherence. The findings suggest that a supportive environment and access to medication are crucial enablers of adherence, while peer influence to use of alternative medicine poses a significant barrier. The study highlights the need for continued support and funding for CCLADs, as well as ongoing education to address misconceptions about HIV treatment and the use of alternative medicine.
Abbreviations
CCLAD, Community Client-Led Art Delivery; HIV, Human immunodeficiency virus; AIDs, Acquired immunodeficiency syndrome; LRRH, Lira Regional Referral Hospital; ART, Anti-retroviral treatment.
Data Sharing Statement
We can confirm that the datasets used and/or analyzed during the current study will be available from the corresponding author on reasonable request.
Acknowledgments
We are grateful to the study participants for volunteering their time during the study. We are grateful to the project administration of the Health Professional Education Partnership Initiative – Transforming Ugandan Institutions Training Against HIV/AIDS for doing an outstanding job in making our research vision a reality. Furthermore, we would like to thank the staff at the LRRH ART clinic, particularly Dr. Luka Joshua, who guided us through the entire respondent recruitment process. Finally, we are grateful to Dr. Moses Ocan for his expertise and guidance throughout the manuscript writing process.
Author Contributions
All authors contributed significantly to the conception and design, data acquisition, or data analysis and interpretation; took part in drafting the article or critically revising this for important content; agreed to submit it to the current journal; gave final approval for the version to be published; and agreed to be accountable for all aspects of the work.
Funding
Research reported in this publication was supported by the Fogarty International Center (US Department of State’s Office of the US Global AIDS Coordinator and Health Diplomacy [S/GAC] and the President’s Emergency Plan for AIDS Relief [PEPFAR]) of the National Institutes of Health under Award Number R25TW011210. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. UNAIDS. Factsheet.; 2022. Available from: https://www.unaids.org/en/resources/fact-sheet?_gl=1*a0tnrh*_ga*MTczNjAwNTEyNC4xNjg2Njg4ODg2*_ga_T7FBEZEXNC*MTY4NjY4ODg4Ni4xLjEuMTY4NjY4ODg5Mi41NC4wLjA.
2. UNAIDS. Facts on HIV and Aids in Uganda in 2022; 2022.
3. Ridgeway K, Dulli LS, Murray KR, et al. Interventions to improve antiretroviral therapy adherence among adolescents in low- and middle-income countries: a systematic review of the literature. PLoS One. 2018;13(1):e0189770. doi:10.1371/journal.pone.0189770
4. Geng EH, Holmes CB. Research to improve differentiated HIV service delivery interventions: learning to learn as we do. PLoS Med. 2019;16(5):e1002809. doi:10.1371/journal.pmed.1002809
5. Grimsrud A, Bygrave H, Doherty M, et al. Reimagining HIV service delivery: the role of differentiated care from prevention to suppression. J Int AIDS Soc. 2016;19(1):21484. doi:10.7448/IAS.19.1.21484
6. Roy M, Bolton Moore C, Sikazwe I, et al. A review of differentiated service delivery for HIV treatment: effectiveness, mechanisms, targeting, and scale. Curr HIV/AIDS Rep. 2019;16(4):324–334. doi:10.1007/s11904-019-00454-5
7. Zakumumpa H, Makobu K, Ntawiha W, et al. A mixed-methods evaluation of the uptake of novel differentiated ART delivery models in a national sample of health facilities in Uganda. PLoS One. 2021;16(7):e0254214. doi:10.1371/journal.pone.0254214
8. Kasande M, Taremwa M, Tusimiirwe H, et al. Experiences and perceptions on community client-led ART delivery (CCLADS) model of antiretroviral (ART) delivery: patients’ and providers’ perspectives in south western Uganda. HIV AIDS. 2022;14:539–551. doi:10.2147/HIV.S387190
9. Barker C, Dutta A, Klein K. Can differentiated care models solve the crisis in HIV treatment financing? Analysis of prospects for 38 countries in sub-Saharan Africa. J Int AIDS Soc. 2017;20(4):21648. doi:10.7448/IAS.20.5.21648
10. Isabirye R, Puleh SS, Opii DJ, et al., Barriers and facilitators of art adherence among Hiv Positive patients in community client-led art delivery groups at lira regional referral hospital; 2021.
11. Puleh SS, Ikwara EA, Namutebi S, et al. Knowledge and perceptions of primary healthcare providers towards integration of antiretroviral therapy (ART) services at departmental levels at selected health facilities Lira district, Uganda. BMC Health Serv Res. 2023;23(1):394. doi:10.1186/s12913-023-09388-6
12. Ahmed CV, Weissinger G, Teitelman A, et al. Expert client service delivery practices among adolescents living with HIV in Eswatini: a thematic analysis. Child Youth Serv Rev. 2022;132:106309. doi:10.1016/j.childyouth.2021.106309
13. Hennink M, Kaiser BN. Sample sizes for saturation in qualitative research: a systematic review of empirical tests. Soc Sci Med. 2021;292:114523. doi:10.1016/j.socscimed.2021.114523
14. Miles MB, Huberman AM. Qualitative Data Analysis: An Expanded Sourcebook.
15. Mukumbang FC, Ndlovu S, van Wyk B. Comparing patients’ experiences in three differentiated service delivery models for HIV treatment in South Africa. Qual Health Res. 2022;32(2):238–254. doi:10.1177/10497323211050371
16. Miyingo C, Mpayenda T, Nyole R, et al. HIV treatment and care of adolescents: perspectives of adolescents on community-based models in northern Uganda. HIV AIDS. 2023;15:105–114. doi:10.2147/HIV.S405393
17. Kintu TM, Ssewanyana AM, Kyagambiddwa T, et al. Exploring drivers and barriers to the utilization of community client-led ART delivery model in South-Western Uganda: patients’ and health workers’ experiences. BMC Health Serv Res. 2021;21(1):1129. doi:10.1186/s12913-021-07105-9
18. Kizito O, Sabiti L. Factors associated with uptake of community client-led ART delivery model at Mulago adult HIV clinic _ mulago national referral hospital. Cogent Med. 2021;8. doi:10.1080/2331205X.2021.1896427
19. Prust ML, Banda CK, Nyirenda R, et al. Multi-month prescriptions, fast-track refills, and community ART groups: results from a process evaluation in Malawi on using differentiated models of care to achieve national HIV treatment goals. J Int AIDS Soc. 2017;20(4):21650. doi:10.7448/IAS.20.5.21650
20. McCarthy EA, Subramaniam HL, Prust ML, et al. Quality improvement intervention to increase adherence to ART prescription policy at HIV treatment clinics in Lusaka, Zambia: a cluster randomized trial. PLoS One. 2017;12(4):e0175534. doi:10.1371/journal.pone.0175534
21. Zou J, Yamanaka Y, John M, et al. Religion and HIV in Tanzania: influence of religious beliefs on HIV stigma, disclosure, and treatment attitudes. BMC Public Health. 2009;9:75. doi:10.1186/1471-2458-9-75
22. Murungi T, Kunihira I, Oyella P, et al. The role of religious leaders on the use of HIV/AIDS prevention strategies among young people (15–24) in Lira district, Uganda. PLoS One. 2022;17(10):e0276801. doi:10.1371/journal.pone.0276801
23. Azia I, Mukumbang FC, Shernaaz C, et al. Role of religious beliefs on antiretroviral treatment adherence among Pentecostal Christians in sub-Saharan Africa: a scoping review protocol. BMJ Open. 2022;12(4):e052750. doi:10.1136/bmjopen-2021-052750
24. Nyogea D, Mtenga S, Henning L, et al. Determinants of antiretroviral adherence among HIV positive children and teenagers in rural Tanzania: a mixed methods study. BMC Infect Dis. 2015;15:28. doi:10.1186/s12879-015-0753-y
25. Mukumbang FC. Leaving no man behind: how differentiated service delivery models increase men’s engagement in HIV care. Int J Health Policy Manag. 2021;10(3):129–140. doi:10.34172/ijhpm.2020.32
26. Biadgilign S, Deribew A, Amberbir A, et al. Barriers and facilitators to antiretroviral medication adherence among HIV-infected paediatric patients in Ethiopia: a qualitative study. J Soc Aspects HIV/AIDS. 2009;6(4):148–154. doi:10.1080/17290376.2009.9724943
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.