")
Back to Journals » Risk Management and Healthcare Policy » Volume 17
Exploring Mental Health Literacy and Its Associated Factors: A National Cross-Sectional Study in Saudi Arabia, 2023
Authors BinDhim NF, Althumiri NA, Ad-Dab’bagh Y, Alqahtani MMJ , Alshayea AK, Al-Luhaidan SM , Al-Duraihem RA , Alhabeeb AA
Received 24 October 2023
Accepted for publication 13 February 2024
Published 20 February 2024 Volume 2024:17 Pages 355—363
DOI https://doi.org/10.2147/RMHP.S442425
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Nasser F BinDhim,1 Nora A Althumiri,1,2 Yasser Ad-Dab’bagh,3 Mohammed MJ Alqahtani,4 Ahmad Kassab Alshayea,5 Sulaiman Mohammed Al-Luhaidan,6 Rashed Abdullah Al-Duraihem,7 Abdulhameed Abdullah Alhabeeb7
1Research and Studies Department, Informed Decision-Making Research and Studies, Riyadh, Saudi Arabia; 2Research and Studies Department, Sharik Association for Research and Studies, Riyadh, Saudi Arabia; 3Mental Health Department, Neuroscience Center, King Fahad Specialist Hospital-Dammam, Dammam, Eastern Region, Saudi Arabia; 4Department of Psychology, King Khalid University, Abha, Saudi Arabia; 5Department of Psychology, King Saud University, Riyadh, Saudi Arabia; 6Studies and Information, National Committee for Narcotics Control, Riyadh, Saudi Arabia; 7National Centre for Mental Health Promotion, Riyadh, Saudi Arabi
Correspondence: Nora A Althumiri, Email [email protected]
Objective: The aim of this study is to examine, for the first time, the mental health literacy of the Saudi general population. Additionally, we aim to identify demographic factors associated with elevated mental health literacy scores.
Methods: A cross-sectional study using a phone interview survey with quota sampling was conducted for equal distribution of sexes, age and administrative regions. Mental health literacy was assessed by the previously validated mental health literacy scale (MHLS). The MHLS ranges from 35 to 160, and a higher score indicates greater level of mental health literacy.
Results: In this study, 4,547 (70.2%) agreed to complete the interview. The sample was equally distributed across Saudi Arabia’s 13 administrative regions with 50.1% female and mean age 35.9 (SD: ± 12.8). In terms of education, 55.1% have a bachelor’s degree or above. The nationally weighted score on the original MHLS was 110.75. the MHLS Saudi validation score was influenced by various variables including: marital status, healthcare-related job, sex, education level, and proximity to individuals with mental health issues.
Conclusion: The study offers data for the first time on Saudi Arabian mental health literacy status. The high MHLS score reflects good societal awareness and understanding of mental health related concepts and issues in the Saudi population. The results of this study set the baseline for mental health literacy in Saudi Arabia. Future research may focus on utilizing the validated MHLS and the method used in this study to explore the effect of other social and individual factors on mental health literacy.
Keywords: mental health literacy, literacy tool, Saudi Arabia, mental health, mental literacy
Background
Mental Health Literacy (MHL) is a relatively new term which refers to understanding and perceptions about mental disorders which might be beneficial for their recognition, management, and prevention.1 This term was coined by Jorm et al in 1997 who defined MHL as “knowledge and beliefs about mental disorders that may facilitate their recognition, management or prevention”.2,3 It encompasses the ability to recognize specific disorders, knowing how to seek mental health information, knowledge of risk factors and causes.3,4
The measurement of MHL in the general population / community has several benefits. It offers a baseline from which to evaluate the present mental health landscape, that is pertinent for policy-making and mental health planning.5 It identifies misconceptions about mental health and informs targeted interventions to correct these misconceptions.1,6 Additionally, better MHL could help with early detection and intervention to reduce the prevalence of mental health problems in the public.1,4,7
Condition-specific tools for measuring MHL typically measure knowledge and attitudes towards a specific mental health disorder such as depression or anxiety.8 These tools provide detailed insights into the understanding of specific conditions. On the other hand, assessments of MHL in general public offer a broader sample of societal knowledge and perceptions related to mental health.9 Such assessments may identify societal barriers to mental health care and guide interventions to improve MHL.10
O Connor and Casey developed the validated quantitative mental health literacy Scale (MHLS) for general population Mental Health Literacy assessment.11 The MHLS has 35 items in a statement form and shows good internal consistency, test-retest reliability, and validity in the original validation study.12 Within the validation sample, “the mean score for the scale was 127.38 (SD = 12.63, minimum 92.00, maximum 155.00)”.12 In general, the distribution of the scale was “approximately normal (skewness −0.115, kurtosis −0.231)”.12 This measure has been translated and validated for use in Saudi Arabia’s general population with good test retest reliability; “the intraclass correlation coefficient ICC was = 0.866, Cronbach’s (0.850) and McDonald’s (0.863) values are above 0.80 indicating very good reliability”.12,13 MHLS has also been translated and validated in other languages including Turkish, Slovenian, French, Chinese and Zambian.14–18 Thus, we used Saudi-validated MHLS for this national survey to assess mental health literacy in Saudi Arabia’s general population.13 A small study with university students using a non-validated version of MHLS in Saudi Arabia was also conducted.19
The aim of this study is to examine MHL of the Saudi general population. Additionally, we aim to identify demographic factors associated with elevated MHL scores.
Methods
Study Design
This research utilized a cross-sectional design and was carried out via computer-aided telephone interviews. The research methodology, formerly validated for its sensitivity, reliability, and adequacy in sample size, was borrowed from the established protocol for mental health surveillance in Saudi Arabia developed in 2020.20–22 This methodology allows for meaningful comparison with historical data in the future, while the results of this study serve as the baseline for the country. Just before conducting the actual interviews, trained interviewers who were experienced in doing telephone research underwent a series of training sessions to become familiar with the interview guidelines. The ZDataCloud system facilitated the collection and governance of research data, leading to a more efficient and well-organized data collection process.23,24 This study was granted ethical Approval by the Sharik Association for Research ethics committee (Approval no. (2023–8)).
Participants and Recruitment
For this study, adults aged 18 years and above, residing across all 13 administrative regions of Saudi Arabia, were selected at random using a systematically generated list of phone numbers. Each individual was contacted a maximum of three times via telephone. If there was no response, an attempt was made to reach out to another potential participant sharing similar demographics in terms of age, gender, and location. The interviewers obtained oral consent, which was acceptable and approved by the ethics committee at Sharik Association for Health Research, from the participants after explaining the study, the type of information to be collected, and the participants’ right to end the survey at any time, while assuring the anonymity and confidentiality of the data in accordance with research ethics standards and local laws. The consent was documented in the respective field within the data collection system. If consent was not provided or the participants did not answer 3 attempts, the process was repeated with another potential individual matching the same demographic profile. Thus, the non-respondents are matched demographically to their replacement which does not need further analysis to compare respondents with nonrespondents.
Sample Size
In accordance with the procedure for mental health surveillance in Saudi Arabia 2020, this research utilized a proportional quota sampling technique to achieve a balanced sample of participants. The quota within each region was based on gender (male and female) and two age groups (19–36 and 37–90). This age categorization was informed by the median age for adults provided by the Saudi Statistics Authority. This division led to 52 quotas for this national survey, thereby strengthening the diversity of the sample and mitigating potential biases from nonprobability sampling.
The size of the sample was determined by the level of sub-analysis required for different future requirements; This entailed the examination of age and gender distributions among various geographical areas. We employed a medium effect size of about 0.21, with a power of 80% and a confidence level of 95%.25 Consequently, it was recommended that each quota include 87 individuals, resulting in a combined total of 383 participants per region and a grand total of 4,524 individuals for the entire sample. Once the desired number of participants was reached in each quota, individuals sharing similar traits were deliberately excluded by the ZDataCloud system.
Data Collection
The quota sampling methodology, facilitated by the ZDataCloud data collection platform, is an automated process that minimizes human intervention and consequently reduces sampling bias.23 The system automatically closes quotas upon reaching the pre-determined sample size. However, due to concurrent phone call attempts, there were instances where more than one participant passed the eligibility criteria simultaneously. This situation, in some cases, led to slightly larger sample sizes than initially planned for certain quotas.
To improve data quality and reduce bias in this national survey, the following steps were taken: (1) All data collectors were trained on the interview guide and research ethics; (2) all data were collected using ZDataCloud, a research data quality and governance system that has various functions, including testing participants’ eligibility, controlling sample size within each dataset to prevent human bias, and allow the researcher to add data integrity checks (eg Age must be at least 18).;24 (3) Data integrity checks were conducted after data collection was completed, with no concerns found.
Study Variables and Outcome Measures
The study is segmented into various parts, including participant demographics, historical mental health data, and familiarity, as well as the Mental Health Literacy Scale (MHLS) composed of 35 individual items. Participants in this study were asked to rate each of the MHLS item on a scale of “1 to 4, with 1 signifying (Very unlikely = I am certain that it is NOT likely) to 4 (Very Likely = I am certain that it IS very likely) (for instance, “If someone became extremely nervous or anxious in one or more situations with other people (e.g., a party) or performance situations (e.g., presenting at a meeting) in which they were afraid of being evaluated by others and that they would act in a way that was humiliating or feel embarrassed, then to what extent do you think it is likely they have Social Phobia”) or in some other items a five-point scale that ranges from 1 (Strongly Disagree) to 5 (Strongly agree). (for example, ‘Seeing a mental health professional means you are not strong enough to manage your own difficulties”)
12,13 The MHLS score fluctuates between 35 and 160, wherein a higher score implies a better understanding of mental health literacy. All details regarding the MHLS’s psychometric properties in Saudi population, such as its validity and reliability, have been previously published (MHLS SA Validation).13
Statistical Analysis
Descriptive statistics were utilized to elaborate on demographic variables, mental health history, and familiarity. Both the original MHLS scale and the Saudi Validation version, along with their factors, were presented in total score and full descriptive analysis, encompassing range, mean, median, kurtosis, skewness, and percentiles. Since the MHLS score is a continuous variable, multiple linear regression analysis was performed, incorporating all nine variables, to explore the association with the total MHLS Saudi Validation score. In the multiple linear regression categorical variables were converted into dummy variables. This is a standard and widely accepted practice in statistical analysis.26–28
Results
Of the 6,468 individuals contacted via telephone, 4,547 (70.2%) responded and agreed to finish the interview, with identical distribution among the thirteen administrative regions of Saudi Arabia as designed in the quota sampling. Of the entire sample, 50.1% were female, the mean age was 35.9 ± 12.8 SD (range = 18 89; median 36.0), and 55.0% had a bachelor’s degree level or above (Table 1).
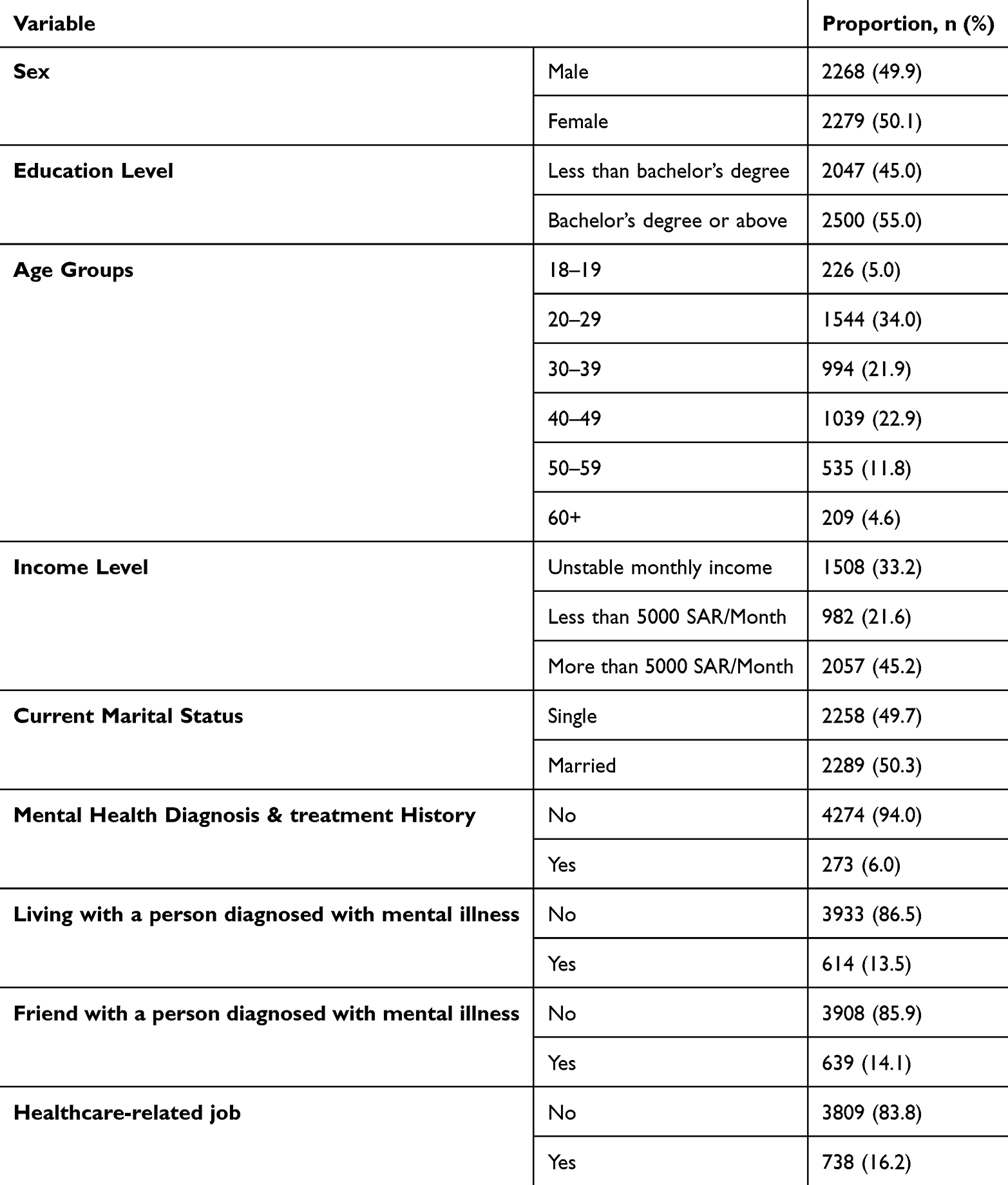 |
Table 1 Study Sample Characteristics |
As shown in Table 2, the results of MHLS in this study are normally distributed.
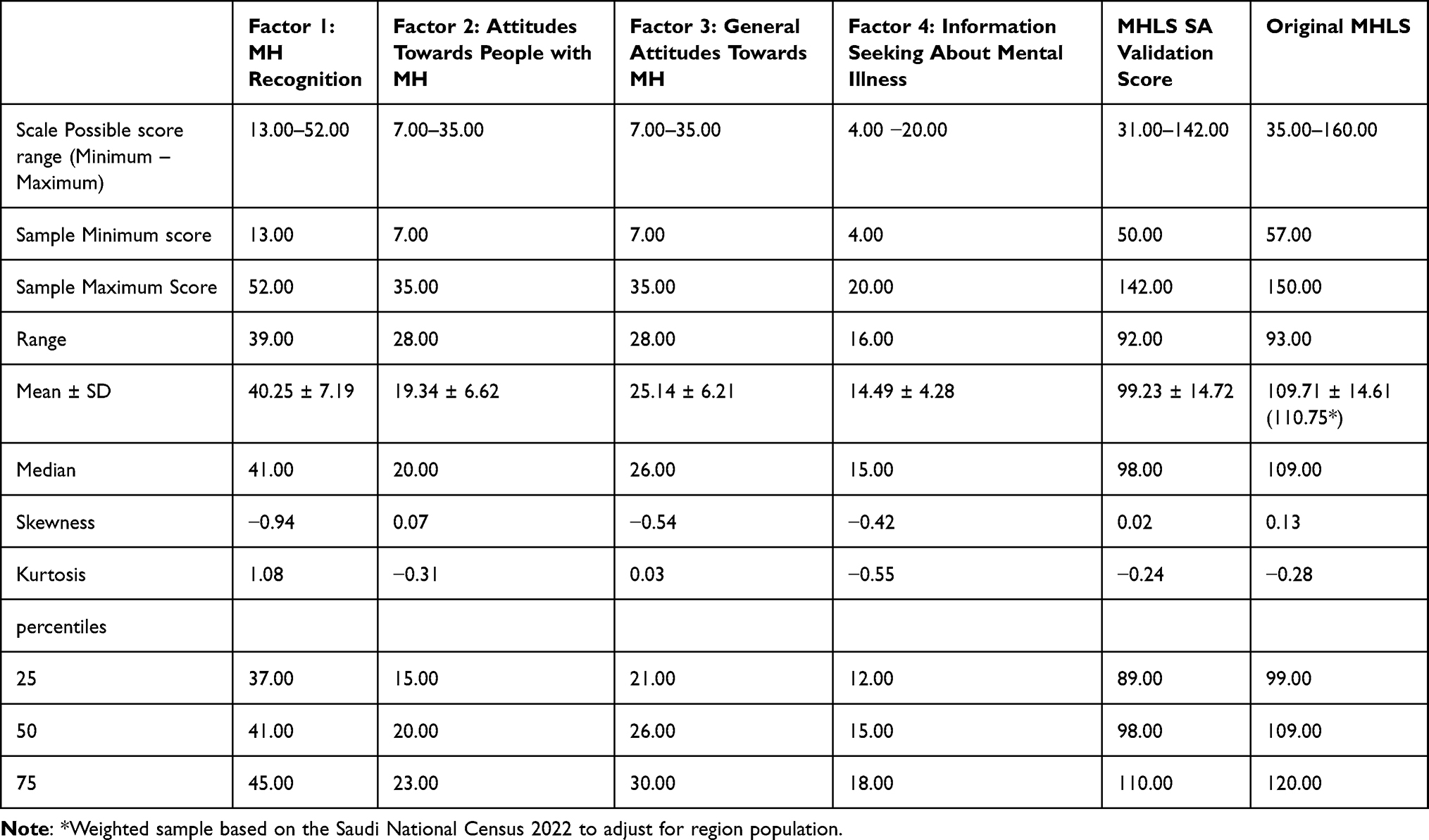 |
Table 2 Descriptive Analysis and Percentiles of MHLS in the Sample |
 |
Table 3 Mean Scores for MHL by Demographic Characteristics in the Sample |
 |
Table 4 Multiple Linear Regression Analysis to Explore the Association Between MHL SA Validation Score and Sociodemographic |
Table 3 showed the mean scores for MHL by the sample demographic characteristics.
Table 4 showed that the MHLS Saudi validation score is influenced significantly by factors like marital status, healthcare-related job, sex, education level, and one’s proximity to individuals diagnosed with mental health issues. Income level and personal mental health diagnosis history, although included in the model, did not show a significant impact on the total score.
Discussion
The results of the study indicate that out of the 6,468 individuals contacted, 4,547 (70.2%) responded and agreed to complete the interview. The sample was evenly distributed among the 13 administrative regions of Saudi Arabia, with 50.1% of the respondents being female and a mean age of 35.9 ± 12.8. The majority of the respondents (55.0%) had a bachelor’s degree or higher. The nationally weighted score on the original MHLS was determined to be 110.75, with the MHLS Saudi validation score being influenced significantly by factors such as marital status, healthcare-related job, sex, education level, and proximity to individuals diagnosed with mental health issues.
First, this study obtained a sample size of 4547 and conducted phone interviews at a national level. On the other hand, it was determined that the MHLS has been applied in four other countries using a self-administered online questionnaire.12,15,16,18 Sample sizes in these countries ranged from 330 in Australia to 1189 in Slovenia, and total scores from 90.52 in France to 127.38 in Australia.12,15,16 The overall score of 110.75 on the original MHLS reflects relatively high mental health literacy in the Saudi population. This is higher compared to scores found in other countries including France but lower compared to Australia. This suggests that even though the general public in Saudi Arabia is well informed on mental health problems, there’s still some room for improvement in comparison to countries like Australia.12 Thus, the cross country comparisons are important not only to benchmark but to understand the baseline or cutoff needed for societies to reach and sustain for MHL to make a real difference.
This study results show that demographic characteristics of the population have a moderate impact on the score of MHL in Saudi Arabia, which in turn provides insights into mental health literacy. The significant association observed between factors such as marital status, healthcare occupation, gender, as well as educational attainment together with the MHL score indicates that demographic variables play a role in influencing mental health literacy. This aligns with earlier studies that have shown how demographic factors can affect one’s overall knowledge of mental health.4 However, there is a need to explore the associations between MHL and other social and behavioral variables to extend the understanding of the factors that strongly impact MHL.
Moreover, proximity to mental health patients also influenced the MHLS score. This indicates that either direct or indirect experience with mental health patients might improve mental health literacy. This is consistent with earlier research which discovered personal experience of mental health is able to boost understanding, knowledge and attitudes.1,4 There are many straightforward strategies, or “nudges”, that can serve as interventions to leverage this knowledge. For example, volunteering at mental health facilities or participating in a mental health support groups, both of which can create an experience to improve MHL.
Income level and personal mental health diagnosis history were included in the multiple linear regression model but did not moderate the total score. The lack of statistical significance indicates that the two factors might have effects on specific behaviors and attitudes concerning mental health but have low impact on general MHL.
To explain the high national MHL score in this study. First, the National Center for Mental Health Promotion (NCMH)29 was established in 2019 to develop national and regional programs for mental health promotion and to support the community and population groups that are mostly vulnerable to mental disorders.30 Its board of directors is headed by the Minister of Health and comprises representatives from several governmental and private sector organizations as well as NGOs. The center aims to provide mental health awareness and education programs, improve the quality of psychological services, and develop preventive programs for mental health.30 In addition, the NCMH has a national good practice and ethics committee to monitor mental health claims, myths, and malpractices in the media and social media as well as generate quick decisions, awareness reports, and guidelines related to these malpractices.31 Such recent reforms place mental health promotion in a unique position, which is independent of mental health care and services, while concurrently being part of the overall mental health efforts at the national level. They empower mental health promotion to act freely in order to expand and implement mental health promotion and prevention initiatives, and simultaneously coordinate with other entities to embed mental health promotion activities within other mental health-related domains.
This is the first nation-wide study in Saudi Arabia to measure mental health literacy (MHL) and in Arabic-speaking countries. Not many countries have measured MHL at a national level. Measuring MHL nationally is the first step toward developing and introducing interventions to improve it and allows for future comparisons. This study’s findings provide a baseline for many future studies that aim to measure the effect of mental health promotion campaigns. They may also offer insights regarding sociocultural differences when compared with other countries.
While our study provides valuable insights into the topic at hand, it is not without its limitations. First, the survey-based nature of our research inherently carries the risk of self-reporting bias, as respondents may not always accurately recall or honestly report their experiences or perceptions. Additionally, the cross-sectional research design of our study only offers a snapshot in time or one single observation, making it difficult to infer causality or track changes over time. Moreover, our research did not account for certain potentially influential variables, which may have impacted the results. Lastly, although comprehensive interviewer training was provided, interviewer bias can be a limitation for such a study. Despite these limitations, we believe our study offers a significant contribution to the existing body of knowledge and provides a foundation for future research related to mental health literacy in Saudi Arabia.
Conclusions
In conclusion, the study provides some new insights into the level of mental health literacy in Saudi Arabia and the factors that influence it. The findings can inform targeted interventions to improve mental health literacy, particularly among demographic groups that are less likely to have high mental health literacy.
Funding
This national survey is funded by “The National Center for Mental Health Promotion”.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jorm AF. Mental health literacy: empowering the community to take action for better mental health. Am Psychologist. 2012;67(3):231. doi:10.1037/a0025957
2. Jorm AF, Korten AE, Jacomb PA, et al. Mental health literacy: a survey of the public’s ability to recognise mental disorders and their beliefs about the effectiveness of treatment. Med j Aust. 1997;166(4):182–186. doi:10.5694/j.1326-5377.1997.tb140071.x
3. Chimoriya R, Mohammad Y, Thomson R, et al. Mental illness stigma and associated factors among Arabic-speaking refugee and migrant populations in Australia. Intl J Mental Health Sys. 2023;17(1):11. doi:10.1186/s13033-023-00580-z
4. Kutcher S, Wei Y, Coniglio C. Mental health literacy: past, present, and future. Can J Psychiatry. 2016;61(3):154–158. doi:10.1177/0706743715616609
5. Mendenhall E, De Silva MJ, Hanlon C, et al. Acceptability and feasibility of using non-specialist health workers to deliver mental health care: stakeholder perceptions from the PRIME district sites in Ethiopia, India, Nepal, South Africa, and Uganda. Soc sci med. 2014;118:33–42. doi:10.1016/j.socscimed.2014.07.057
6. Corrigan PW, Druss BG, Perlick DA. The impact of mental illness stigma on seeking and participating in mental health care. Psychol Sci Public Interes. 2014;15(2):37–70. doi:10.1177/1529100614531398
7. Jorm AF, Griffiths KM. The public’s stigmatizing attitudes towards people with mental disorders: how important are biomedical conceptualizations? Acta Psyc Scand. 2008;118(4):315–321. doi:10.1111/j.1600-0447.2008.01251.x
8. Brohan E, Gauci D, Sartorius N, et al. Self-stigma, empowerment and perceived discrimination among people with bipolar disorder or depression in 13 European countries: the GAMIAN–Europe study. J Affective Disorders. 2011;129(1–3):56–63. doi:10.1016/j.jad.2010.09.001
9. Reavley NJ, Jorm AF. Stigmatizing attitudes towards people with mental disorders: findings from an Australian National survey of mental health literacy and Stigma. Austr New Zealand J Psy. 2011;45(12):1086–1093. doi:10.3109/00048674.2011.621061
10. Corrigan PW, Morris SB, Michaels PJ, et al. Challenging the public stigma of mental illness: a meta-analysis of outcome studies. Psychiatric Serv. 2012;63(10):963–973. doi:10.1176/appi.ps.201100529
11. Riebschleger J, Grové C, Cavanaugh D, et al. Mental health literacy content for children of parents with a mental illness: thematic analysis of a literature review. Brain Sci. 2017;7(11):141. doi:10.3390/brainsci7110141
12. O’Connor M, Casey L. The Mental Health Literacy Scale (MHLS): a new scale-based measure of mental health literacy. Psychiatry Res. 2015;229(1–):511–516. doi:10.1016/j.psychres.2015.05.064
13. BinDhim NF, Althumiri NA, Ad-Dab’bagh Y, et al. Validation and psychometric testing of the Arabic version of the mental health literacy scale among the Saudi Arabian general population. Intl J Mental Health Sys. 2023;17(1):42. doi:10.1186/s13033-023-00615-5
14. Kesgin MT, Pehlivan S, Uymaz P. Study of validity and reliability of the mental health literacy scale in Turkish/ruh sagligi okuryazarligi olceginin turkce uyarlamasi: gecerlilik ve guvenilirlik calismasi. Anadolu Psikiyatri Dergisi. 2020;21(S2):5–14.
15. Krohne N. Slovenian Validation of the Mental Health Literacy Scale (S-MHLS) on the general population: a four-factor Model. INQUIRY. J Health Care Organ. 2022;59:00469580211047193.
16. Montagni I, González Caballero JL. Validation of the mental health literacy scale in French university students. Behav Sci. 2022;12(8):259. doi:10.3390/bs12080259
17. Korhonen J, Axelin A, Grobler G, et al. Content validation of Mental Health Literacy Scale (MHLS) for primary health care workers in South Africa and Zambia─ a heterogeneous expert panel method. Global Health Action. 2019;12(1):1668215. doi:10.1080/16549716.2019.1668215
18. Wang A, Jia S, Shi Z, et al. Validation and psychometric testing of the Chinese version of the mental health literacy scale among nurses. Front Psych. 2022;12:791883. doi:10.3389/fpsyg.2021.791883
19. Almanasef M. Mental health literacy and help-seeking behaviours among undergraduate pharmacy students in Abha, Saudi Arabia. Risk Manage Health Pol. 2021;Volume 14:1281–1286. doi:10.2147/RMHP.S289211
20. Althumiri NA, Basyouni MH, BinDhim NF. Consistency and sensitivity evaluation of the Saudi Arabia Mental Health Surveillance System (MHSS): hypothesis generation and testing. JMIR Format Res. 2022;6(2):e23965. doi:10.2196/23965
21. BinDhim NF, Althumiri NA, Basyouni MH, et al. Saudi Arabia Mental Health Surveillance System (MHSS): mental health trends amid COVID-19 and comparison with pre-COVID-19 trends. Eur J Psych. 2021;12(1):1875642. doi:10.1080/20008198.2021.1875642
22. Alhabeeb AA. National screening for anxiety and depression in Saudi Arabia. Front Public Health. 2023;2022:11.
23. ZDataCloud: research data governance & quality system; 2023. Available from: https://zdatacloud.com.
24. Methodologists. ZDataCloud: revolutionizing research data governance with ISO 37000 principles; 2023. Available from: https://methodologists.net/Empowering-Universities-with-ZDataCloud:-IDMs-ISO-37000-Based-Solution-for-Research-Data-Governance-and-Quality-Management.
25. Cohen J. Statistical Power Analysis for the Behavioral Sciences. Academic press; 2013.
26. Zhang Z, McDonnell KT, Zadok E, et al. Visual correlation analysis of numerical and categorical data on the correlation map. IEEE Trans Visual Comput Graph. 2014;21(2):289–303. doi:10.1109/TVCG.2014.2350494
27. Hayes AF, Montoya AK. A tutorial on testing, visualizing, and probing an interaction involving a multicategorical variable in linear regression analysis. Commun Method Meas. 2017;11(1):1–30. doi:10.1080/19312458.2016.1271116
28. Sun Y. Multiple regression: methodology and applications. Highlights in science. Eng Technol. 2023;49:542–548.
29. BinDhim NF. Cultural adaptation and validation of the mental illness associated stigma scale for Arabic-speaking population in Saudi Arabia. Front Psyc. 2024;24:14.
30. NCMH. About the national center for mental health promotion; 2020. Available from: https://ncmh.org.sa/view/16/3th.
31. Saudi Gazette. Minister of health forms committee to monitor ethical practices in mental health sector; 2022. Available from: https://saudigazette.com.sa/article/623542/SAUDI-ARABIA/Minister-of-Health-forms-committee-to-monitor-ethical-practices-in-mental-health-sector.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.