")
Back to Journals » Research and Reports in Urology » Volume 16
Experimental and New Approaches for Bladder Preservation in Intermediate and High-Risk Non-Muscle-Invasive Bladder Cancer (NMIBC)
Authors Avilez ND, Capibaribe DM, Reis LO
Received 29 November 2023
Accepted for publication 8 February 2024
Published 6 April 2024 Volume 2024:16 Pages 89—113
DOI https://doi.org/10.2147/RRU.S452377
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Panagiotis J Vlachostergios
Natália D Avilez,1 Diego M Capibaribe,1 Leonardo O Reis1,2
1UroScience, State University of Campinas, Unicamp, Campinas, São Paulo, Brazil; 2ImmunOncology, Pontifical Catholic University of Campinas, PUC-Campinas, São Paulo, Brazil
Correspondence: Leonardo O Reis, Rua Vital Brasil, 80, Cidade Universitária Zeferino Vaz, Campinas, São Paulo, CEP 13083-888, Brasil, Tel +55 19 3521-7481, Email [email protected]
Abstract: About 75% of bladder cancers are detected as non-muscle invasive. High-risk patients have high progression risk. Although the standard is transurethral resection of bladder tumor plus full dose intravesical BCG for one to 3 years, due to the high risk of progression, radical cystectomy may be considered in specific cases. Although radical cystectomy is still the best approach for high-grade NMIBC from an oncological perspective, its high morbidity and impact on quality of life motivate studies of new strategies that may reduce the need for cystectomy. We carried out a mini-review whose objectives were: 1 - to identify bladder-sparing alternatives that are being studied as possible treatment for patients with intermediate and high-risk NMIBC; 2 - understand the evidence that exists regarding success rate, follow-up, and side effects of different strategies. Several studies have sought alternatives for bladder preservation, including immunotherapy, intravesical chemotherapy, chemo-hyperthermia, antibody-drug conjugates, viral genetic therapy, and others with promising results. The selection of an optimal therapy for high-risk NMIBC that can reduce the need for cystectomy, with low toxicity and high efficacy, is of paramount importance and remains an issue, however, several known medications are being tested as bladder-preserving alternatives in this scenario and have shown promise in studies.
Keywords: high-grade, non-muscle-invasive bladder cancer, unfavorable, bladder preservation
Introduction
Bladder cancer (BC) is the tenth most reported cancer worldwide when both sexes are considered, and the standardized death rate (per 100,000 person-years) is 3.3 for men versus 0.86 for women.1
Approximately 75% of bladder cancers are detected as non-muscle invasive (NMIBCs).2 The European Urological Association (EAU) guidelines classify NMIBCs as low, intermediate, high, and very high risk based on the World Health Organization (WHO) 2004/2016 or WHO 1973 classification systems (Table 1). Patients diagnosed with high-risk NMIBC recurred in 2.6% to 5.7% in one year and 10% to 19% in ten years, while very high-risk patients experienced recurrence in 12% to 32% and 39% to 79% in one and ten years, respectively.3
 |
Table 1 EAU Risk Classification According to WHO 2004/2016/WHO 1973 Grading Classification Systems |
Standard treatment varies by risk. Low-risk NMIBCs are treated with transurethral resection of bladder tumor (TURBT) alone, while intermediate- and high-risk NMIBCs should be treated with TURBT plus full-dose intravesical BCG for 1 to 3 years. Due to the high risk of progression, immediate radical cystectomy (RC) should be discussed with patients, mainly in the very high-risk group. Early RC is strongly recommended in patients with tumors that are not BCG-responsive and should be considered in recurrent high-grade tumors.4
Although RC is the best approach from an oncological point of view, its high morbidity and impact on quality of life motivate studies of new strategies that may reduce the need for cystectomy.
The only conservative alternative treatment approved by the Food and Drug Administration (FDA) for BCG-unresponsive disease is pembrolizumab, but toxicity and durability of response are concerns. Other conservative treatments are being studied and may be a future alternative to bladder preservation.
New Strategies to Reduce the Need for Cystectomy
Immunotherapy
Recent studies found that intradermal BCG priming, prior to intravesical instillations, can be a promising alternative, as it has demonstrated the ability to expedite the migration of T lymphocytes into the bladder, thereby enhancing the local immune response.5 Table 2 summarizes the main studies.
 |
Table 2 Immunotherapy Studies |
Another immunotherapy that also has its role proven are PD-1/PD-L1 inhibitors, which are already included in the guidelines for metastatic and locally advanced bladder cancer. Recent studies have shown the role of this immune checkpoint blockade (ICB) also in NMIBC, showing it to be an important therapeutic target in BCG-unresponsive NMIBC.
One notable breakthrough has been the approval of Pembrolizumab by the FDA for treating BCG-unresponsive Carcinoma In Situ (CIS), based on the KEYNOTE-057 study. This study evaluated the efficacy of the PD-1 inhibitor Pembrolizumab in high-risk, BCG-unresponsive NMIBC and yielded impressive results, with a complete response in 40% of patients within three months, and 42% achieving complete response. Serious treatment-related adverse events occurred in eight (8%) patients.8 Another study evaluated the combination of BCG and intravesical pembrolizumab, the 1-year recurrence-free rates was 22% and 5 of 9 patients had progressed to muscle invasive bladder cancer (MIBC), one death occurred from myasthenia gravis that was deemed potentially related to treatment.6
The SWOG S1605 study examined the use of Atezolizumab in patients with CIS unresponsive to BCG, with promising results with 37.6% of complete response at 6 months. Despite the promising results of ICB, its systemic administration presents significant adverse effects, the most frequent AEs were fatigue (49.3%) and 12.3% patients presented grade 3–5 adverse effects including one treatment-related death.9 Intravesical administration of Durvalumab was also studied in patients with pT1 or higher (BCG-naïve) bladder cancer with modest reported activity.7
CD40 is another immune checkpoint under investigation expressed by several cell types in the myeloid cell lineage, such as dendritic cells, macrophages, monocytes, and B cells, that can be targeted for agonistic antibody treatment in bladder cancer.11 CD40 ligand stimulation produces a robust antitumor response, including activation of dendritic cells to engulf, process, and present tumor antigen to T cells and can initiate programmed cell death.12 However, systemic CD40 therapy was associated with immune-related adverse events such as cytokine release syndrome, thrombocytopenia, and liver toxicity.10
Intravesical Chemotherapy
Chemotherapy is another modality that has already proven its role in metastatic and muscle invasive bladder cancer and intravesical administration has been studied for NMIBC (summarized in Table 3). Several studies have been carried out with gemcitabine as monotherapy,13–27 as well as in association with several other medications, such as docetaxel,28,29 cabazitaxel and cisplatin,30 oral everolimus31 and mitomycin C (MMC).32,33
 |
Table 3 Intravesical Chemotherapy Studies |
Hurle et al studied gemcitabine monotherapy after BGC failure or intolerance, and 68.7% of patients had negative cystoscopy and urinary cytology after induction, although the result dropped to 31.6% after 24 months; overall survival (OS) was 77.9% and cancer-specific survival (CSS) was 80.68% after 24 months.34 Skinner et al had also good results with 47% of patients with negative cystoscopy, urinary cytology, and biopsy, after 3 months and 21% after 24 months.13
The gemcitabine’s potential has also been explored in combination with various other medications. Chevuru et al studied gemcitabine plus docetaxel with a 74% response at 3 months, and 50% and 30% high-grade recurrence-free survival (RFS) at 2 and 5 years, respectively, and 64% 5-year OS.28 Studying the same drug combination Steinberg et al29 and Milbar et al35 found high-grade RFS of 46% and 42% at 2 years, respectively.
De Castro et al reported a few encouraging cases combining gemcitabine with cabazitaxel and cisplatin with 64% 2-year RFS.30 The combination of intravesical gemcitabine and oral everolimus demonstrated 20% RFS at 12 months but was not well tolerated.31 Docetaxel alone showed 25% RFS at 3 years.37 Other associations such as MMC,32,33 paclitaxel, nab-paclitaxel,16,17,36 valrubicin and doxorubicin15,22 have been described with conflicting results.
Chemo Hyperthermia (CTH)
While hyperthermia in the temperature range of 40°C to 45°C exerts direct cytotoxic effects, disrupting metabolism, causing DNA damage, impairing cell function, and promoting apoptosis in tumor cells, chemo hyperthermia increases cell membrane permeability and modifies blood perfusion, improving drug penetration in the urothelium, with potential to increase chemotherapy effectiveness.38–40 This is achieved through external or internal (integrated into a catheter) microwave-generated heating devices or by a conductive system that externally heats the chemotherapy solution before intravesical administration and can also be combined with radiotherapy to enhance treatment efficacy.41,42
Colombo et al compared CHT and MMC in patients with intermediate and high-risk NMIBC with 17.1% and 57.5% recurrence rates, respectively.43 An update of this study showed 15% and 53% disease-free survival (DFS) and a bladder preservation rate of 86% and 79% for thermochemotherapy and chemotherapy alone, at 10 years, respectively.44
Another trial studying intermediate- and high-risk NMIBC patients showed 24-month RFS of 78.1% and 64.8% in the CHT with MMC and BCG group, respectively; the progression rate was <2% in both groups.45 Nativ et al treated 111 NMBC patients that failed BCG with CHT and found 56% 24-month DFS. Recurrence rate was 61% at 2 years vs 39% in those with maintenance treatment.46
Intravesical electromotive drug delivery is another approach involving the application of an electrical current across the urothelium to enhance drug movement. In a prospective study, Di Stasi et al evaluated patients with high-risk NMIBC, treated with conventional BCG, passive MMC, and electromotive MMC, with 64%, 31% and 58%, after 6 months, respectively, although 20 patients underwent cystectomy and 19 died of disseminated bladder cancer.47 The main studies on CTH are in Table 4.
 |
Table 4 Chemo Hyperthermia (CTH) Studies |
Target Therapy
Table 5 shows studies on target therapy. Sunitinib acts by inhibiting the vascular endothelial growth factor receptor (VEGFR) and, thus, inhibits tumor activity. A phase II study offered Sunitinib to patients with NMIBC who progressed after BCG and found 44% remission at 12 weeks and 22% PFS after 12 months. Grades 3 and 4 toxicity was noted in 68% of patients.48
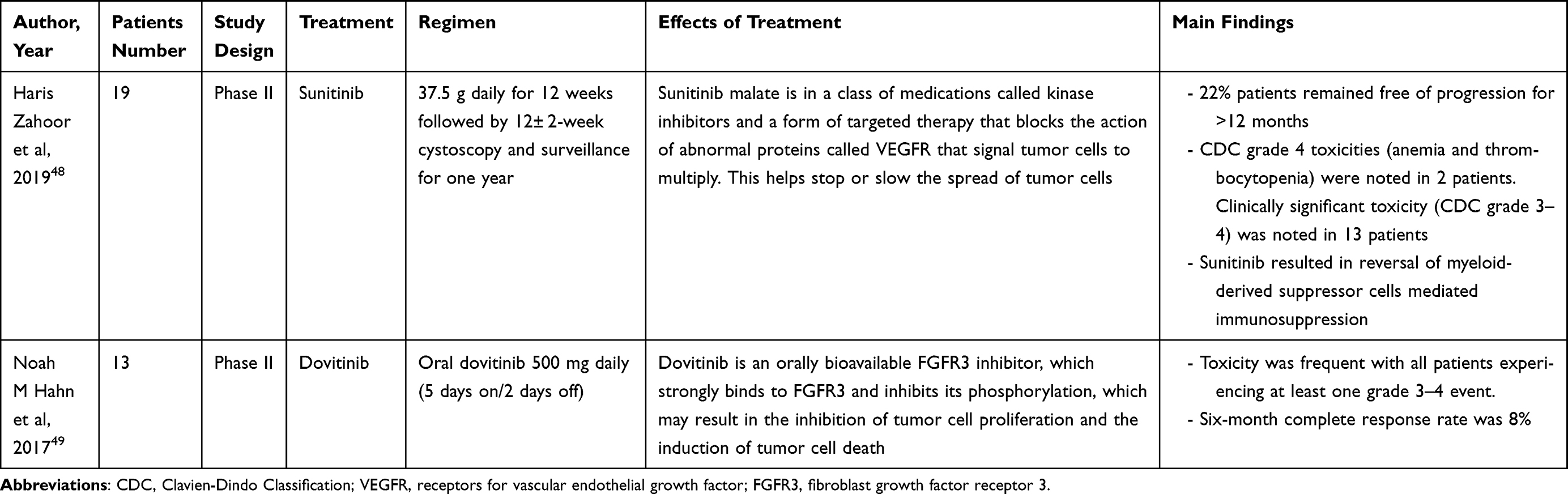 |
Table 5 Target Therapy Studies |
Another phase II study evaluated NMIBC patients unresponsive to BCG with altered FGFR3 expression treated with oral dovitinib and found 33% complete response in patients with FGFR3 mutation, however also with high toxicity.49
Viral Gene Therapy
Other therapies are also being tested based on studies that show that genotypic and phenotypic alterations can favor tumor invasion and the development of tumor escape mechanisms (summarized in Table 6).
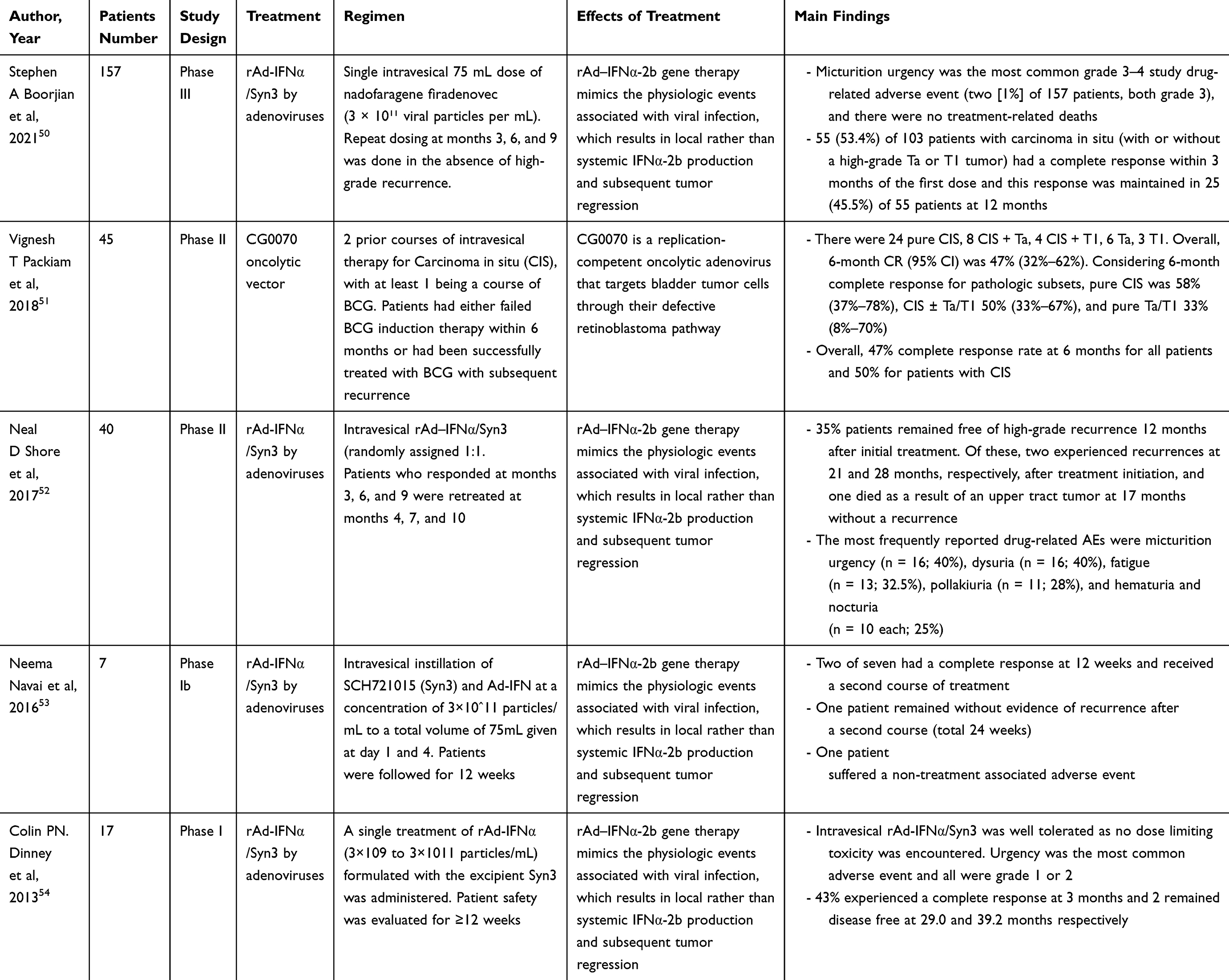 |
Table 6 Viral Gene Therapy Studies |
Nadofaragene firadenovec (rAd-IFNα/Syn3) is a promising contender, comprises rAd-IFNα, a non-replicating recombinant adenovirus vector-based gene therapy agent, which introduces a copy of the human IFNα-2b gene into the urothelial cell wall.55,56
Syn3, a polyamide surfactant, complements this by enhancing viral transduction of the urothelium.57 In a phase II trial involving 40 patients with BCG-unresponsive high-grade NMIBC, the RFS after 12 months was 35%; no grade four or five adverse events occurred.52 Encouraged by these results, Boorjian et al conducted a multicenter phase III clinical trial in the USA, with 151 patients who did not respond to BCG and found that in patients with CIS, a complete response rate of 53.4% at 3 months and 45.5% of the response was maintained at 12 months.50 The rAd-IFNα/Syn3 has undergone evaluation in 4 single-arm cohort trials,50,52–54 revealing complete response rates ranging from 29% to 60% at 3 months and from 29% at 3 months to 35% at 12 months.
Complete response rate of 47% at 6 months, 30% at 12 months, with lower rates in the subgroup with concomitant CIS, was reported in a phase II study of 45 “BCG-exposed” NMIBC patients with or without CIS who refused RC and received intravesical CG0070 with n-dodecyl-BD-maltoside (a transduction enhancer).51
Other oncolytic viruses with relevance include intravesical talimogene laherparepvec, a herpes simplex 1 virus with ICP47 deletion that incorporates the human GM-CSF gene, diphtheria toxin A, and intravesical V937 (Cavatak, Coxsackievirus A21).58
Antibody-Drug Conjugates (ADCs)
ADCs are a new therapeutic approach that combines the high specificity of monoclonal proteins with cytotoxic agents. In recent years, ADCs have emerged as an innovative therapeutic tool that can take advantage of tumor-specific molecular characteristics (the main studies are found in Table 7).
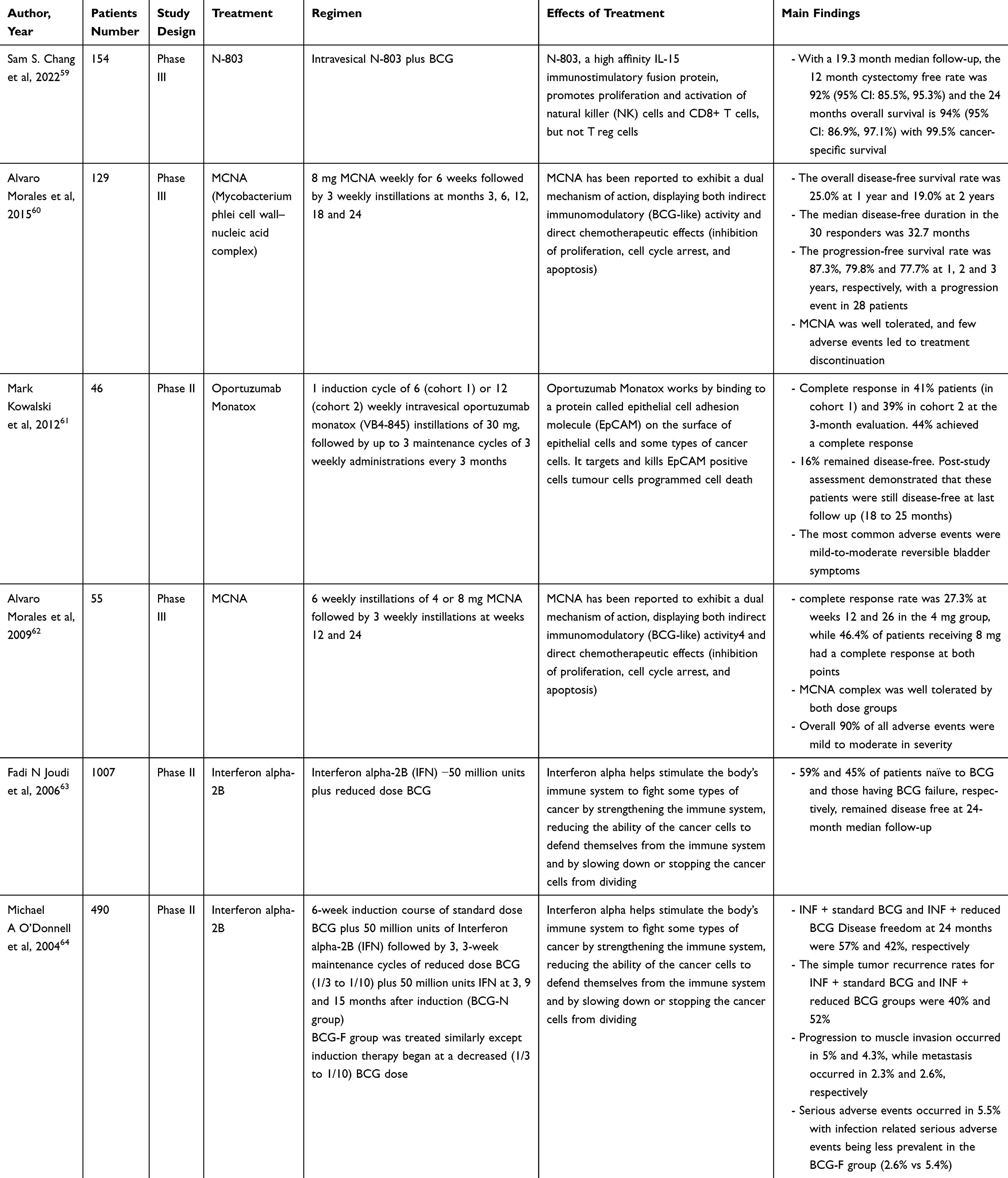 |
Table 7 Antibody-Drug Conjugates (ADCs) |
The enfortumab vedotin is an antibody–drug conjugate directed against Nectin-4, which is highly expressed in luminal subtypes of bladder cancer.65 It was recently approved by the FDA for the treatment of metastatic patients, and a multicenter study is evaluating the safety and response in BCG-unresponsive NMIBCs.66
Vicinium (oportuzumab monatox) is a recombinant fusion protein that ingeniously combines a humanized single-chain anti-EpCAM (epithelial cell adhesion molecule) antibody with Pseudomonas exotoxin A. Kowalsky et al studied it in patients with NMIBC unresponsive to BCG with concomitant CIS and found a 44% response rate, and in 16% this response was maintained until the end of the follow-up period (18–25 months), with minimal adverse effects.61
A phase II trial studying a combination of BCG with interleukins achieved a 24-month OS of 94% with minimal adverse effects.59 Other studies tested interferon (IFN)α2b action. O’Donnell et al compare INF + standard BCG and INF + reduced BCG Disease freedom at 24 months were 57% and 42%, respectively.64 Joudi et al got promising results comparing INF in patients naïve to BCG and those having BCG failure with 59% and 45% patients disease free at 24-month median follow-up, respectively.63
An immunomodulatory and antineoplastic compound derived from Mycobacterium phlei60,62 was also tested in a phase III trial with overall disease-free survival of 19% at 2 years and few adverse events.60
Photodynamic Therapy (PDT)
Photodynamic Therapy (PDT) involves the administration of a photosensitizing agent activated by light at a specific wavelength. PDT outcomes are based on limited patient series in the context of NMIBC and are therefore considered experimental (the main studies are found in Table 8).
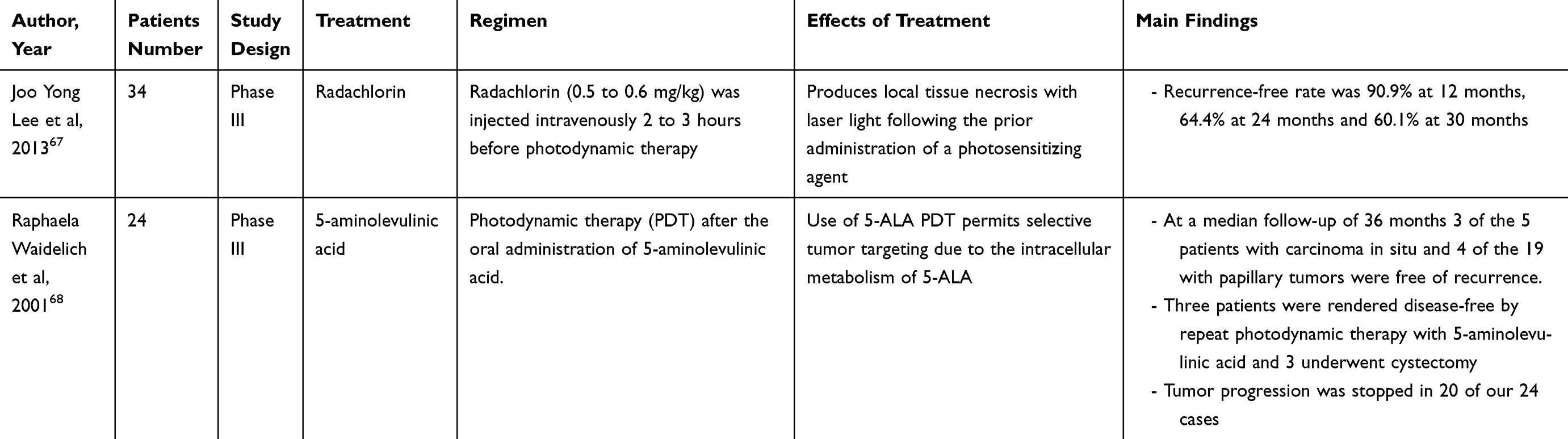 |
Table 8 Photodynamic Therapy (PDT) Studies |
Still, it is an incipient and experimental treatment, of which there are only small series described. Waidelich et al studied PDT with oral 5-aminolevulinic acid in patients with BCG-refractory NMIBC with a complete remission in 100% of patients with CIS and 79.2% patients with papillary tumors, and after 3 years 60% of CIS patients and 21% of papillary patients remained disease-free.68
Lee et al investigated the PDT with intravenous radachlorin in 34 patients with a high-grade T1 disease, with or without concomitant CIS, and none of the patients had evidence of disease after 12 weeks. RFS was 60.1% at 30 months. Adverse events observed were mainly lower urinary tract symptoms and hematuria.67
Discussion
In the realm of bladder cancer, Non-Muscle Invasive Bladder Cancer (NMIBC) presents a significant challenge, with a prevalence of 75%. This condition is categorized into three risk groups, with the high-risk category exhibiting a notably low recurrence-free survival (RFS) rate of just 23%. Patients with high-grade NMIBC face a substantial risk of recurrence and progression, nearly 50% in some cases, often necessitating invasive and burdensome surgical interventions.69 Therefore, any therapeutic approach that can reduce the necessity for cystectomy while demonstrating reduced toxicity and high efficacy, is of paramount importance. Bacillus Calmette-Guérin (BCG) therapy has been the cornerstone treatment for NMIBC for decades. However, its failure rate (40%) and progression rate (15%) necessitate alternative strategies and novel treatment advancements.70
The Food and Drug Administration (FDA) has recognized the urgency for new treatments in cases of BCG failure, as evidenced by their acceptance of single-arm studies.71,72 However, the lack of uniformity in these studies, particularly in aspects such as tumor multifocality, size, maintenance therapy, prior recurrence rates, and cystoscopy evaluation methods, weakens the robustness of the data and complicates its interpretation.
In the context of Immune Checkpoint Blockade (ICB), only two-phase II trials have been notable. These trials have shown encouraging results in BCG-unresponsive patient cohorts with Carcinoma In Situ (CIS) or concurrent papillary tumors. The first trial, led by Balar et al,6 evaluated Pembrolizumab and, despite a small patient cohort, yielded promising outcomes with only 13% of patients experiencing significant treatment-related adverse events. Intravesical administration of Pembrolizumab may mitigate certain adverse events and elicit a CD4+T cell response. Interestingly, the drug was detectable in urine but not in blood samples in a small phase I study. The second trial investigated Atezolizumab but failed to meet the efficacy threshold.9 The success of ICB in Muscle-Invasive Bladder Cancer (MIBC) has already been incorporated into treatment guidelines and may soon extend to earlier stages of the disease. The FDA has already approved its use in the NMIBC BCG unresponsive CIS scenario, although data on toxicity and complication rates in NMIBC post-BCG failure remain limited.
Sunitinib, an early targeted agent and an endothelial growth factor receptor inhibitor, showed potential in bladder cancer (BC). However, a phase II trial by Zahoor et al involving 19 BCG-failure patients indicated that while relatively safe, Sunitinib did not improve outcomes. Dovitinib achieved biologically active concentrations in the urothelium and inhibited pFGFR3 pharmacodynamically but was associated with frequent high-grade toxicities.49
Intravesical chemotherapy is a familiar approach in clinical practice. For BCG-naïve patients, a Randomized Controlled Trial (RCT) demonstrated that the combination of Mitomycin C (MMC) and BCG was more effective than BCG alone in terms of recurrence-free interval and progression rate reduction.73 In BCG-unresponsive cases, various agents such as Valrubicin, Gemcitabine, MMC, and Docetaxel have been extensively studied, with Gemcitabine emerging as a favorable option due to its efficacy and patient acceptability, particularly in BCG-resistant cases.
Microwave-induced hyperthermia has shown to enhance the efficacy of MMC in high-risk tumors, as evidenced by a single-center study with a 10-year follow-up and an RCT indicating superior outcomes compared to BCG in intermediate and high-risk cases.74 However, further head-to-head studies are required for a definitive conclusion.
Chemohyperthermia, combining hyperthermia with chemotherapy, has shown promise in enhancing treatment outcomes but comes with several challenges. It can increase both local and systemic toxicity, complicate treatment delivery due to the need for specialized equipment and expertise and pose risks of bladder damage. Additionally, it incurs higher costs and resource utilization, and there is a lack of long-term data on its efficacy and safety.
The exploration of immunotherapy and anti-inflammatory agents in NMIBC is an active area of research. While promising results have been observed, further validation of their safety and efficacy is necessary. Advances in immunotherapy are poised to revolutionize NMIBC treatment, but patient-specific factors must guide treatment selection.
Gene therapy, although in its nascent stages, shows great promise for NMIBC treatment. Ongoing research aims to overcome challenges in gene delivery, immune response regulation, and targeted gene expression. Current clinical trials are assessing the safety and efficacy of gene therapy for NMIBC.
Photodynamic therapy, despite being studied for decades, has a limited presence in literature with less than 30 single-arm studies. However, the outcomes have been largely positive, with most complications being mild and transient. Future high-quality research is essential to further establish its efficacy.
Enfortumab vedotin (EV), an antibody–drug conjugate targeting Nectin-4, is currently being evaluated in a Phase 1 trial (EV-104, NCT05014139) presented by Kamat et al at ASCO 2023. This study aims to assess the safety, tolerability, and anti-tumor activity of intravesical EV in BCG-unresponsive NMIBCs and is actively recruiting participants.
Nadofaragene firadenovec has demonstrated tolerability without dose-limiting toxicity or significant treatment-related side effects. A single dose was sufficient to achieve measurable urine IFNα, indicating its potential efficacy.74
Conclusion
The selection of an optimal therapy for intermediate and high-risk NMIBC that can reduce the need for cystectomy, with reduced toxicity and high efficacy, is of paramount importance and remains an issue; however, several bladder-preserving alternatives are being tested in this scenario and have shown promise, pending long-term oncological results and larger methodologically robust trials.
Pembrolizumab is still the only drug approved by the FDA, but other ICBs also show promise, as do intravesical chemotherapy and ADCs, recently approved by the FDA for metastatic treatment, which are also being pulled to earlier stages.
Acknowledgment
To the involved institution(s), the patients, and those that provided and cared for study patients. Heveline Roesch has helped address the reviewers’ and editors’ comments.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Reis LO, National Council for Scientific and Technological Development – CNPq, Research Productivity: 304747/2018-1 and 310135/2022-2. The funder was not involved in study design, data collection, data analysis, manuscript preparation, and/or publication decisions.
Disclosure
The authors report no conflicts of interest.
References
1. IARC, Cancer Today. Estimated number of new cases in 2020, worldwide, both sexes, all ages; 2021. Available from: https://gco.iarc.fr/today/en.
2. Compérat E, Larré S, Roupret M, et al. Clinicopathological characteristics of urothelial bladder cancer in patients less than 40 years old. Virchows Arch. 2015;466:589–594. doi:10.1007/s00428-015-1739-2
3. Sylvester RJ, Rodríguez O, Hernández V, et al. European Association of Urology (EAU) Prognostic Factor Risk Groups for Non-muscle-invasive Bladder Cancer (NMIBC) incorporating the WHO 2004/2016 and WHO 1973 classification systems for grade: an update from the EAU NMIBC guidelines panel. Eur Urol. 2021;79:480–488. doi:10.1016/j.eururo.2020.12.033
4. Psutka SP, Barocas DA, Catto JWF, et al. Staging the host: personalizing risk assessment for radical cystectomy patients. Eur Urol Oncol. 2018;1:292–304. doi:10.1016/j.euo.2018.05.010
5. Tse J, Singla N, Ghandour R, Lotan Y, Margulis V. Current advances in BCG-unresponsive non-muscle invasive bladder cancer. Expert Opin Investig Drugs. 2019;28:757–770. doi:10.1080/13543784.2019.1655730
6. Meghani K, Cooley LF, Choy B, et al. First in-human intravesical delivery of pembrolizumab identifies immune activation in bladder cancer unresponsive to Bacillus Calmette-Guérin. Eur Urol. 2022;82:602–610. doi:10.1016/j.eururo.2022.08.004
7. Moe A, Liow E, Redfern A, et al. A phase I open label dose-escalation study to evaluate the tolerability, safety and immunological efficacy of sub-urothelial durvalumab injection in adults with muscle-invasive or high-risk non-muscle-invasive bladder cancer (SUBDUE-1, SUB-urothelial DUrvalumab injection-1 study): clinical trial protocol. BJU Int. 2021;128(Suppl 1):9–17. doi:10.1111/bju.15365
8. Balar AV, Kamat AM, Kulkarni GS, et al. Pembrolizumab monotherapy for the treatment of high-risk non-muscle-invasive bladder cancer unresponsive to BCG (KEYNOTE-057): an open-label, single-arm, multicentre, Phase 2 study. Lancet Oncol. 2021;22:919–930. doi:10.1016/S1470-2045(21)00147-9
9. Black PC, Tangen C, Singh P, et al. Phase II trial of atezolizumab in BCG-unresponsive non-muscle invasive bladder cancer: SWOG S1605 (NCT #02844816). J Clin Oncol. 2020;38(15 Suppl):5022. doi:10.1200/JCO.2020.38.15_suppl.5022
10. Vonderheide RH, Flaherty KT, Khalil M, et al. Clinical activity and immune modulation in cancer patients treated with CP-870,893, a novel CD40 agonist monoclonal antibody. J Clin Oncol. 2007;25:876–883. doi:10.1200/JCO.2006.08.3311
11. Mangsbo SM, Broos S, Fletcher E, et al. The human agonistic CD40 antibody ADC-1013 eradicates bladder tumors and generates T-cell–dependent tumor immunity. Clin Cancer Res. 2015;21:1115–1126. doi:10.1158/1078-0432.CCR-14-0913
12. Bennett SR, Carbone FR, Karamalis F, Flavell RA, Miller JF, Heath WR. Help for cytotoxic-T-cell responses is mediated by CD40 signalling. Nature. 1998;393:478–480. doi:10.1038/30996
13. Skinner EC, Goldman B, Sakr WA, et al. SWOG S0353: phase II trial of intravesical gemcitabine in patients with nonmuscle invasive bladder cancer and recurrence after 2 prior courses of intravesical Bacillus Calmette-Guérin. J Urol. 2013;190:1200–1204. doi:10.1016/j.juro.2013.04.031
14. Sternberg IA, Dalbagni G, Chen LY, Donat SM, Bochner BH, Herr HW. Intravesical gemcitabine for high risk, nonmuscle invasive bladder cancer after Bacillus Calmette-Guérin treatment failure. J Urol. 2013;190:1686–1691. doi:10.1016/j.juro.2013.04.120
15. Steinberg GD, Smith ND, Ryder K, Strangman NM, Slater SJ. Factors Affecting valrubicin response in patients with Bacillus Calmette-Guérin-refractory bladder carcinoma in situ. Postgrad Med. 2011;123:28–34. doi:10.3810/pgm.2011.05.2281
16. McKiernan JM, Barlow LJ, Laudano MA, Mann MJ, Petrylak DP, Benson MC. A phase I trial of intravesical nanoparticle albumin-bound paclitaxel in the treatment of Bacillus Calmette-Guérin refractory nonmuscle invasive bladder cancer. J Urol. 2011;186:448–451. doi:10.1016/j.juro.2011.03.129
17. Bassi PF, Volpe A, D’Agostino D, et al. Paclitaxel-hyaluronic acid for intravesical therapy of Bacillus Calmette-Guérin refractory carcinoma in situ of the bladder: results of a phase I study. J Urol. 2011;185:445–449. doi:10.1016/j.juro.2010.09.073
18. Di Lorenzo G, Perdonà S, Damiano R, et al. Gemcitabine versus bacille Calmette-Guérin after initial bacille Calmette-Guérin failure in non-muscle-invasive bladder cancer: a multicenter prospective randomized trial. Cancer. 2010;116:1893–1900. doi:10.1002/cncr.24914
19. Perdonà S, Di Lorenzo G, Cantiello F, et al. Is gemcitabine an option in BCG-refractory nonmuscle-invasive bladder cancer? A single-arm prospective trial. Anticancer Drugs. 2010;21:101–106. doi:10.1097/CAD.0b013e3283324d83
20. Laudano MA, Barlow LJ, Murphy AM, et al. Long-term clinical outcomes of a phase I trial of intravesical docetaxel in the management of non-muscle-invasive bladder cancer refractory to standard intravesical therapy. Urology. 2010;75:134–137. doi:10.1016/j.urology.2009.06.112
21. Addeo R, Caraglia M, Bellini S, et al. Randomized phase III trial on gemcitabine versus mytomicin in recurrent superficial bladder cancer: evaluation of efficacy and tolerance. J Clin Oncol. 2010;28:543–548. doi:10.1200/JCO.2008.20.8199
22. Ignatoff JM, Chen YH, Greenberg RE, Pow-Sang JM, Messing EM, Wilding G. Phase II study of intravesical therapy with AD32 in patients with papillary urothelial carcinoma or Carcinoma In Situ (CIS) refractory to prior therapy with Bacillus Calmette-Guerin (E3897): a trial of the Eastern Cooperative Oncology Group. Urol Oncol. 2009;27:496–501. doi:10.1016/j.urolonc.2008.05.004
23. Mohanty NK, Nayak RL, Vasudeva P, Arora RP. Intravesicle gemcitabine in management of BCG refractory superficial TCC of urinary bladder-our experience. Urol Oncol. 2008;26:616–619. doi:10.1016/j.urolonc.2007.10.016
24. Gunelli R, Bercovich E, Nanni O, et al. Activity of endovesical gemcitabine in BCG-refractory bladder cancer patients: a Translational Study. Br J Cancer. 2007;97:1499–1504. doi:10.1038/sj.bjc.6604074
25. Dalbagni G, Russo P, Bochner B, et al. Phase II trial of intravesical gemcitabine in bacille Calmette-Guérin-refractory transitional cell carcinoma of the bladder. J Clin Oncol. 2006;24:2729–2734. doi:10.1200/JCO.2005.05.2720
26. Bartoletti R, Cai T, Gacci M, et al. Intravesical gemcitabine therapy for superficial transitional cell carcinoma: results of a phase II Prospective Multicenter Study. Urology. 2005;66:726–731. doi:10.1016/j.urology.2005.04.062
27. Bassi P, De Marco V, Tavolini IM, et al. Pharmacokinetic study of intravesical gemcitabine in carcinoma in situ of the bladder refractory to Bacillus Calmette-Guérin therapy. Urol Int. 2005;75:309–313. doi:10.1159/000089164
28. Chevuru PT, McElree IM, Mott SL, Steinberg RL, O’Donnell MA, Packiam VT. Long-term follow-up of sequential intravesical gemcitabine and docetaxel salvage therapy for non-muscle invasive bladder cancer. Urol Oncol. 2023;41:148.e1–148.e7. doi:10.1016/j.urolonc.2022.10.030
29. Steinberg RL, Thomas LJ, Brooks N, et al. Multi-institution evaluation of sequential gemcitabine and docetaxel as rescue therapy for nonmuscle invasive bladder cancer. J Urol. 2020;203:902–908. doi:10.1097/JU.0000000000000688
30. DeCastro GJ, Sui W, Pak JS, et al. A Phase I trial of intravesical cabazitaxel, gemcitabine and cisplatin for the treatment of nonmuscle invasive Bacillus Calmette-Guérin unresponsive or recurrent/relapsing urothelial carcinoma of the bladder. J Urol. 2020;204:247–253. doi:10.1097/JU.0000000000000919
31. Dalbagni G, Benfante N, Sjoberg DD, et al. Single Arm Phase I/II Study of everolimus and intravesical gemcitabine in patients with primary or secondary carcinoma in situ of the bladder who failed Bacillus Calmette Guerin (NCT01259063). Bladder Cancer. 2017;3:113–119. doi:10.3233/BLC-170095
32. Cockerill PA, Knoedler JJ, Frank I, Tarrell R, Karnes RJ. Intravesical gemcitabine in combination with mitomycin C as salvage treatment in recurrent non-muscle-invasive bladder cancer. BJU Int. 2016;117:456–462. doi:10.1111/bju.13088
33. Lightfoot AJ, Breyer BN, Rosevear HM, Erickson BA, Konety BR, O’Donnell MA. Multi-institutional analysis of sequential intravesical gemcitabine and mitomycin C chemotherapy for non-muscle invasive bladder cancer. Urol Oncol. 2014;32:35.e15–35.e19. doi:10.1016/j.urolonc.2013.01.009
34. Hurle R, Casale P, Morenghi E, et al. Intravesical gemcitabine as bladder-preserving treatment for BCG unresponsive non-muscle-invasive bladder cancer. Results from a Single-Arm, Open-Label Study. BJUI Compass. 2020;1:126–132. doi:10.1002/bco2.28
35. Milbar N, Kates M, Chappidi MR, et al. Oncological outcomes of sequential intravesical gemcitabine and docetaxel in patients with non-muscle invasive bladder cancer. Bladder Cancer. 2017;3:293–303. doi:10.3233/BLC-170126
36. Robins DJ, Sui W, Matulay JT, et al. Long-term survival outcomes with intravesical nanoparticle albumin-bound paclitaxel for recurrent non-muscle-invasive bladder cancer after previous Bacillus Calmette-guérin therapy. Urology. 2017;103:149–153. doi:10.1016/j.urology.2017.01.018
37. Barlow LJ, McKiernan JM, Benson MC. Long-term survival outcomes with intravesical docetaxel for recurrent nonmuscle invasive bladder cancer after previous Bacillus Calmette-Guérin therapy. J Urol. 2013;189:834–839. doi:10.1016/j.juro.2012.10.068
38. Hendricksen K. Device-assisted intravesical therapy for non-muscle invasive bladder cancer. Transl Androl Urol. 2019;8:94–100. doi:10.21037/tau.2018.09.09
39. Van der Heijden AG, Verhaegh G, Jansen CF, et al. Effect of hyperthermia on the cytotoxicity of 4 chemotherapeutic agents currently used for the treatment of transitional cell carcinoma of the bladder: an in vitro study. J Urol. 2005;173:1375–1380. doi:10.1097/01.ju.0000146274.85012.e1
40. Paroni R, Salonia A, Lev A, et al. Effect of local hyperthermia of the bladder on mitomycin C pharmacokinetics during intravesical chemotherapy for the treatment of superficial transitional cell carcinoma. Br J Clin Pharmacol. 2001;52:273–278. doi:10.1046/j.0306-5251.2001.01449.x
41. Liem EIML, Crezee H, de la Rosette JJ, de Reijke TM. Chemohyperthermia in non-muscle-invasive bladder cancer: an overview of the literature and recommendations. Int J Hyperth. 2016;32:363–373. doi:10.3109/02656736.2016.1155760
42. Longo TA, Gopalakrishna A, Tsivian M, et al. A systematic review of regional hyperthermia therapy in bladder cancer. Int J Hyperthermia. 2016;32:381–389. doi:10.3109/02656736.2016.1157903
43. Colombo R, Da Pozzo LF, Salonia A, et al. Multicentric study comparing intravesical chemotherapy alone and with local microwave hyperthermia for prophylaxis of recurrence of superficial transitional cell carcinoma. J Clin Oncol. 2003;21(23):4270–4276. doi:10.1200/JCO.2003.01.089
44. Colombo R, Salonia A, Leib Z, et al. Long-term outcomes of a randomized controlled trial comparing thermochemotherapy with mitomycin-C alone as adjuvant treatment for non-muscle-invasive bladder cancer (NMIBC). BJU Int. 2011;107(6):912–918. doi:10.1111/j.1464-410X.2010.09654.x
45. Arends TJ, Nativ O, Maffezzini M, et al. Results of a Randomised controlled trial comparing intravesical chemohyperthermia with Mitomycin C versus Bacillus Calmette-Guerin for adjuvant treatment of patients with intermediate- and high-risk non-muscle-invasive bladder cancer. Eur Urol. 2016;69:1046–1052. doi:10.1016/j.eururo.2016.01.006
46. Nativ O, Witjes JA, Hendricksen K, et al. Combined thermo-chemotherapy for recurrent bladder cancer after Bacillus Calmette-Guerin. J Urol. 2009;182(4):1313–1317. doi:10.1016/j.juro.2009.06.017
47. Di Stasi SM, Giannantoni A, Stephen RL, et al. Intravesical electromotive mitomycin C versus passive transport mitomycin C for high-risk superficial bladder cancer: a prospective randomized study. J Urol. 2003;170(3):777–782. doi:10.1097/01.ju.0000080568.91703.18
48. Zahoor H, Mir MC, Barata PC, et al. Phase II trial of continuous treatment with sunitinib in patients with high-risk (BCG-refractory) non-muscle invasive bladder cancer. Investig New Drugs. 2019;37:1231–1238. doi:10.1007/s10637-018-00716-w
49. Hahn NM, Bivalacqua TJ, Ross AE, et al. A Phase II trial of dovitinib in BCG-unresponsive urothelial carcinoma with FGFR3 mutations or overexpression: Hoosier cancer research network trial HCRN 12-157. Clin Cancer Res. 2017;23:3003–3011. doi:10.1158/1078-0432.CCR-16-2267
50. Boorjian SA, Alemozaffar M, Konety BR, et al. Intravesical nadofaragene firadenovec gene therapy for BCG-unresponsive non-muscle-invasive bladder cancer: a single-arm, open-label, repeat-dose clinical trial. Lancet Oncol. 2021;22:107–117. doi:10.1016/S1470-2045(20)30540-4
51. Packiam VT, Lamm DL, Barocas DA, et al. An open label, single-arm, phase II Multicenter Study of the Safety and Efficacy of CG0070 oncolytic vector regimen in patients with BCG-unresponsive non-muscle-invasive bladder cancer: interim results. Urol Oncol. 2018;36:440–447. doi:10.1016/j.urolonc.2017.07.005
52. Shore ND, Boorjian SA, Canter DJ, et al. Intravesical RAd-IFNα/Syn3 for patients with high-grade, Bacillus Calmette-Guerin-refractory or relapsed non-muscle-invasive bladder cancer: a Phase II Randomized Study. J Clin Oncol. 2017;35:3410–3416. doi:10.1200/JCO.2017.72.3064
53. Navai N, Benedict WF, Zhang G, et al. Phase 1b trial to evaluate tissue response to a second dose of intravesical recombinant adenoviral interferon A2b formulated in Syn3 for failures of Bacillus Calmette-Guerin (BCG) therapy in nonmuscle invasive bladder cancer. Ann Surg Oncol. 2016;23:4110–4114. doi:10.1245/s10434-016-5300-6
54. Dinney CPN, Fisher MB, Navai N, et al. Phase I trial of intravesical recombinant adenovirus mediated interferon-A2b formulated in syn3 for Bacillus Calmette-Guérin failures in nonmuscle invasive bladder cancer. J Urol. 2013;190:850–856. doi:10.1016/j.juro.2013.03.030
55. Benedict WF, Tao Z, Kim CS, et al. Intravesical Ad-IFNalpha causes marked regression of human bladder cancer growing orthotopically in nude mice and overcomes resistance to IFN-alpha protein. Mol Ther. 2004;10:525–532. doi:10.1016/j.ymthe.2004.05.027
56. Connor RJ, Anderson JM, Machemer T, Maneval DC, Engler H. Sustained intravesical interferon protein exposure is achieved using an adenoviral-mediated gene delivery system: a study in rats evaluating dosing regimens. Urology. 2005;66:224–229. doi:10.1016/j.urology.2005.02.015
57. Yamashita M, Rosser CJ, Zhou JH, et al. Syn3 provides high levels of intravesical adenoviral-mediated gene transfer for gene therapy of genetically altered urothelium and superficial bladder cancer. Cancer Gene Ther. 2002;9:687–691. doi:10.1038/sj.cgt.7700488
58. Chu C, Pietzak E. Immune mechanisms and molecular therapeutic strategies to enhance immunotherapy in non-muscle invasive bladder cancer: invited review for special issue ”seminar: treatment advances and molecular biology insights in urothelial carcinoma”. Urol Oncol. 2023;41:398–409. doi:10.1016/j.urolonc.2022.05.013
59. Chang SS, Chamie K, Gonzalgo ML, et al. Positive efficacy and safety Phase 3 results in both CIS and papillary cohorts BCG-unresponsive nonmuscle invasive bladder cancer (NMIBC) after IL-15RFc superagonist N-803 (Anktiva) and BCG infusion. J clin oncol. 2022;40:431. doi:10.1200/JCO.2022.40.6_suppl.431
60. Morales A, Herr H, Steinberg G, et al. Efficacy and safety of MCNA in patients with nonmuscle invasive bladder cancer at high risk for recurrence and progression after failed treatment with Bacillus Calmette-Guérin. J Urol. 2015;193:1135–1143. doi:10.1016/j.juro.2014.09.109
61. Kowalski M, Guindon J, Brazas L, et al. A phase II study of oportuzumab monatox: an immunotoxin therapy for patients with noninvasive urothelial carcinoma in situ previously treated with Bacillus Calmette-Guérin. J Urol. 2012;188:1712–1718. doi:10.1016/j.juro.2012.07.020
62. Morales A, Phadke K, Steinhoff G. Intravesical mycobacterial cell wall-DNA complex in the treatment of carcinoma in situ of the bladder after standard intravesical therapy has failed. J Urol. 2009;181:1040–1045. doi:10.1016/j.juro.2008.11.019.
63. Joudi FN, Smith BJ, O’Donnell MA. Final results from a national multicenter Phase II trial of combination Bacillus Calmette-Guérin plus interferon alpha-2B for reducing recurrence of superficial bladder cancer. Urol Oncol. 2006;24:344–348. doi:10.1016/j.urolonc.2005.11.026
64. O’Donnell MA, Lilli K, Leopold C. Interim results from a national multicenter Phase II trial of combination Bacillus Calmette-Guerin plus interferon Alfa-2b for superficial bladder cancer. J Urol. 2004;172:888–893. doi:10.1097/01.ju.0000136446.37840.0a
65. Chu CE, Sjöström M, Egusa EA, et al. Heterogeneity in NECTIN4 expression across molecular subtypes of urothelial cancer mediates sensitivity to enfortumab vedotin. Clin Cancer Res. 2021;27:5123–5130. doi:10.1158/1078-0432.CCR-20-4175
66. Kamat AM, Steinberg GD, Inman BA, et al. Study EV-104: phase 1 study of intravesical enfortumab vedotin for treatment of patients with Non-Muscle Invasive Bladder Cancer (NMIBC)—trial in progress. J Clin Oncol. 2023;41:TPS582. doi:10.1200/JCO.2023.41.6_suppl.TPS582
67. Lee JY, Diaz RR, Cho KS, et al. Efficacy and safety of photodynamic therapy for recurrent, high grade nonmuscle invasive bladder cancer refractory or intolerant to bacille Calmette-Guerin immunotherapy. J Urol. 2013;190:1192–1199.
68. Waidelich R, Stepp H, Baumgartner R, et al. Clinical experience with 5-aminolevulinic acid and photodynamic therapy for refractory superficial bladder cancer. J Urol. 2001;165:1904–1907. doi:10.1016/S0022-5347(05)66239-8
69. Ritch CR, Velasquez MC, Kwon D, et al. Use and validation of the AUA/SUO risk grouping for nonmuscle invasive bladder cancer in a contemporary cohort. J Urol. 2020;203(3):505–511. doi:10.1097/JU.0000000000000593
70. Zuiverloon TCM, Zwarthoff EC. Predicting response to intravesical Bacillus Calmette-Güerin immunotherapy: are we moving forward? Eur Urol. 2016;69:201–202. doi:10.1016/j.eururo.2015.07.010
71. Kamat AM, Sylvester RJ, B€ohle A, et al. Definitions, end points, and clinical trial designs for non-muscle-invasive bladder cancer: recommendations from the International Bladder Cancer Group. J Clin Oncol. 2016;34:1935–1944. doi:10.1200/JCO.2015.64.4070
72. Lerner SP, Dinney C, Kamat A, et al. Clarification of bladder cancer disease states following treatment of patients with intravesical BCG. Bladder Cancer. 2015;1:29–30.
73. Cui J, Wang W, Chen S, et al. Combination of intravesical chemotherapy and Bacillus Calmette-Guerin versus Bacillus Calmette-Guerin monotherapy in intermediate- and high-risk nonmuscle invasive bladder cancer: a systematic review and meta-analysis. Medicine. 2016;95:e2572. doi:10.1097/MD.0000000000002572
74. Arends TJ, van der Heijden AG, Witjes JA. Combined chemohyperthermia: 10-year single center experience in 160 patients with nonmuscle invasive bladder cancer. J Urol. 2014;192:708–713. doi:10.1016/j.juro.2014.03.101
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.