")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Evaluating Parents’ Concerns, Needs, and Levels of Satisfaction with the Services Provided for ASD Children in Saudi Arabia
Authors Al Awaji NN, Al-Taleb SM, Albagawi TO, Alshammari MT, Sharar FA, Mortada EM
Received 29 October 2023
Accepted for publication 20 December 2023
Published 8 January 2024 Volume 2024:17 Pages 123—146
DOI https://doi.org/10.2147/JMDH.S447151
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Nisreen Naser Al Awaji,1 Sumaih Mohammed Al-Taleb,1,* Teef Olayan Albagawi,1,* Maram Taleb Alshammari,1,* Fay Abdullah Sharar,1,* Eman M Mortada2
1Department of Health Communication Sciences, College of Health and Rehabilitation Sciences, Princess Nourah bint Abdulrahman University, Riyadh, 11671, Saudi Arabia; 2Health Sciences department, College of Health and Rehabilitation Sciences, Princess Nourah bint Abdulrahman University, Riyadh, 11671, Saudi Arabia
*These authors contributed equally to this work
Correspondence: Eman M Mortada, Health Sciences department, College of Health and Rehabilitation Sciences, Princess Nourah Bint Abdulrahman University, P.O Box 84428, Riyadh, 11671, Saudi Arabia, Email [email protected]
Background: Supporting children with autism spectrum disorder (ASD) and their parents is vital in improving their children’s abilities and their parents’ ability to care for them. Thus, parents’ perceptions of and levels of satisfaction with the services provided for their children must be assessed.
Aim: This study aimed to understand parents’ perceptions of and satisfaction with the speech–language services (SLS) provided for ASD children in different health facilities in Saudi Arabia.
Methods: This cross-sectional study included 109 parents of ASD children. The survey included five sections dealing with (1) general information about the child; (2) assessment of the child’s ASD characteristics (including their age when diagnosed, when they first noticed symptoms, and their speech, language, and communication abilities); (3) the reasons for enrollment in SLS sessions; (4) questions about SLS; and (5) parents’ perceptions of SLS, satisfaction with the service, descriptions of their children’s progress, and the respect and support they received.
Results: Parents’ satisfaction levels were significantly higher when they had easy access to SLS, sufficient information and support, proper training in applying therapy exercises at home, and perceived respect and support from speech and language pathologists (SLPs). The reasons for discontinuing SLS included high session costs, the need for initial behavioral sessions, the lack of qualified SLPs, the end of the sessions, the lack of improvement, the nonavailability of specialized centers, and parents’ dependence on home training only. They also sought opportunities for work and education, continuous and intensive SLS sessions, reduced costs, centers for adults with ASD, and accessible schools. Parents’ main concerns were their children’s poor speech and language skills, independence, and social acceptance.
Conclusion and Implications: The study highlighted the importance of understanding parents’ experiences with SLS, identifying the factors that enhance SLS use by ASD children, and improving parents’ satisfaction with such services.
Keywords: autism spectrum disorder, concerns, parents, perceptions, needs, speech language service
What This Paper Adds to the Literature
Parents’ experiences with speech and language therapy (SLT) can help identify areas for improvement. Financial challenges, limited specialized centers, the lack of therapists, and continuous communication sessions are common challenges faced by parents of ASD children. Sharing common experiences can enhance parents’ self-confidence, strength, and coping strategies. Multidisciplinary team-related school services for ASD children should also involve collaborative support from professionals in the fields of special education and speech, occupational, and physical therapy. Parents’ concerns include their children’s poor speech and language skills, independence, and social acceptance. Understanding their SLS experiences and addressing factors that enhance SLS use and improve parents’ satisfaction are crucial for improving the quality of care for children with ASD.
Introduction
Autism spectrum disorder (ASD) is a neurodevelopmental disorder that affects a child’s communication and language skills at any age. A child with ASD may have restricted and repetitive behaviors and a reduced ability to communicate with others. Each child’s condition will differ from those of other children in terms of understanding and using nonverbal and verbal language, facial expressions, and body language. In terms of speech and language development, several children with autism experience either linguistic challenges or strengths across all subsystems of language, including pragmatics, grammar, semantics, syntax, phonology, and morphology, both orally and in writing. Interestingly, some of these children may demonstrate exceptional language abilities, including linguistic creativity.
Furthermore, depending on the severity of the communication issue, some children may be verbal, while others may be minimally or not at all verbal. The symptoms of ASD are most often noticed at the age of 18 months or older, and the formal diagnosis can be made at the age of two years by a licensed specialist.2 However, in the Kingdom of Saudi Arabia (KSA), the median age of ASD diagnosis is three years3. According to a report by the General Authority for Statistics, Saudi Arabia has 49,016 children with ASD,4 which means that one in every 160 children in the country is diagnosed with ASD.5
Children with ASD receive services from psychiatrists, psychologists, occupational therapists, developmental educators, dieticians, social workers, behavior practitioners, disability support workers, and speech and language pathologists (SLPs).
Early interventions can improve ASD children’s communication skills due to the neuroplasticity of their brains at an early age.6 Children with ASD can face many challenges during their childhood years, in their school years, and later in life. Thus, parenting a child with ASD can be very challenging for parents, and this can significantly affect their parenting efficiency, increase parenting stress, and affect their emotional well-being and quality of life (QoL).7,8 The severity of a child’s social impairment is strongly linked to his/her parents’ concerns and burdens.7 Individuals with ASD contribute a significant financial burden to society as a whole. Specifically, many of these individuals require lifelong support and care in a variety of domains, including education, healthcare, and community services, resulting in significant costs for individuals with ASD, their families, public and private health insurance companies, and financial aid programs.9
Although there are no data available for the financial cost of ASD in Saudi Arabia, several studies have indicated that families of autistic children often incur substantial additional expenses, lost earnings, and increased care demands as a result of the child’s additional needs10–12 According to a national survey conducted in Ireland, families with autistic children spent on average €28,465 per year as a result of out-of-pocket expenses for private autism services, lost income, and informal care.13
A study conducted in Jordan reported that the average monthly cost of therapy sessions was between a quarter and a third of the total monthly family income14. In terms of the cost of therapy sessions for speech language services (SLS), a study conducted in Egypt showed that financial concerns are among the major difficulties faced by parents due to intense and costly sessions; therefore, some parents have to end their children’s SLS sessions.15 In general, children from families with a low socioeconomic status (SES) have greater unmet healthcare needs and poorer overall health outcomes than their peers from families with a higher SES.
In the KSA, services for individuals with ASD can be provided through the government or the private sector (specialized clinics, special needs centers, hospitals, and schools). While all government-provided ASD services are free, and some private institutions are charitable, not all children with ASD have access to these services.16 Financial support can be provided by the Ministry of Social Affairs (MSA) to individuals with disabilities, including ASD, under certain conditions. To receive such support, an applicant must be duly registered with the MSA and have their disability assessed. Then, for the disability to be considered eligible for the subsidy service, the following requirements must also be met: the family income should not exceed SAR 4000 per month, an individual should not be admitted to health and rehabilitation facilities at the government’s expense for more than six months, beneficiaries of the MSA’s care centers must reside permanently in the KSA, and a person must not be older than 45 when the disability occurs (MSA).17 Therefore, not all children with ASD can receive the services they need under government coverage.16 Furthermore, better services are provided in major cities, whereas fewer services are provided in smaller cities.18,19 These limitations can adversely affect the caregivers’ and the ASD children’s QoL, as evidenced by past studies,19,20 which reported low QoL levels among ASD children and their caregivers. Thus, the caregivers and the children with ASD must receive appropriate medical, psychological, and financial support. For example, to avoid unfavorable variations in healthcare services across cities, unified national centers with qualified staff can provide advanced healthcare services and affordable teaching and training sessions for caregivers.19
At present, major goals and plans in the healthcare sector have been set under Saudi Vision 2030 so that services can be expanded for all ASD children in the KSA. In recent years, the Saudi government has undertaken large-scale initiatives to improve the QoL of individuals with various health conditions and their professional careers. Related to this, it is also important to understand parents’ experiences of caring for their children with ASD to support the development of more responsive and effective services, including providing early diagnostic services, counseling parents, educating school-age children, and providing community living arrangements and leisure activities to adults.15
Several studies in different geographical areas have reported unmet service needs for individuals with ASD and their families,21,22 including a lack of the following services: medical, targeted therapy, school, job coaching, financial management, and services for young adults with ASD.23,24 Moreover, parents of children with ASD have expressed difficulties in communication,15 limited social support, and limited involvement in the SLT process.25,26 All these concerns may affect parents’ QoL.15,18,27
Communication is crucial in an individual’s ability to form relationships and function in society, which is especially important for children with autism. Therefore, the present study aims to create the foundation for a program that can enhance the perceptions of parents of children with ASD and their levels of satisfaction with the SLS provided in the KSA and, ultimately, to improve the available SLS services in the country. The main objectives of this study are as follows:
- To measure parents’ perceptions of and levels of satisfaction with the SLS provided, as well as their concerns, needs, and recommendations;
- To identify the potential reasons for their decision to discontinue the services for their children; and
- To compare the parents’ levels of satisfaction with the SLS provided on the basis of the characteristics of ASD children, the availability and use patterns of speech clinics, and the parents’ perceptions of SLS.
Methodology
Study Design and Setting
A cross-sectional study design was chosen for this study, as we considered it the most appropriate design to achieve the descriptive and analytical objectives of the study. The study was conducted from health facilities providing SLP services, including King Abdullah Bin Abdulaziz University Hospital, and at different centers, such as the Prince Nasser Bin Abdulaziz Center for Autism, Riyadh Specialized Rehabilitation Center, and the Basmat Qudrati Center. The data were collected from December 2022 to February 2023.
Sample Size and Sampling Technique
Based on the existing number of ASD children in Saudi Arabia (ie, 49,016),4 95% confidence interval (CI), degree of precision = 0.05 at 95% CI, and anticipated prevalence of satisfaction with SLS received = 50%, the required sample size for this study is 382 parents, which we calculated using the appropriate statistical package, namely, OpenEpi.28 The inclusion criteria were as follows: having an ASD child aged 2–10 years and a willingness to participate in the study. Those who gave incomplete responses were excluded from the study. Thus, out of 442 parents of ASD children who agreed to take part in the survey, only 109 completed the survey. The remaining 333 gave incomplete answers, so their data were excluded from the total number of responses. Thus, the final sample consisted of 109 parents.
Survey
The self-reported online Arabic survey was developed by the research team to measure the perceptions of parents of ASD children. This tool was originally developed in English and then translated into Arabic using a forward-backward translation process. The final version of the survey consisted of the following five main sections:
- This section involved questions extracting general information about the child, including his/her gender; age; area of residence; whether the child has any problems with speech, language, and communication; and whether the child has received SLS.
- This section included questions related to the child’s ASD characteristics, such as age at diagnosis of ASD, age when his/her caregiver first noticed ASD symptoms, and the child’s speech, language, communication, and social skills.
- This section involved questions related to the parents’ reasons for enrolling their children in speech, language, and/or communication sessions.
- This section included questions about SLS, such as the availability and accessibility of these services, whether the child is still receiving SLS or has discontinued receiving them, and information about the child’s condition.
- The final section was about the parents’ perceptions of SLS, which included their levels of satisfaction with the SLS provided, the progress they noted in their children’s conditions, and their perceptions of the respect and support they received. A 3-question satisfaction scale was used consisting of a 3-point scale with responses ranging from 0 (not satisfied) to 2 (satisfied). The total score ranged from 0 to 6 after summing the responses. Accordingly, the participants were dichotomized into those satisfied with the provided services (scores above the median > 4) and those who were not satisfied with the provided services (scores equal to or below the median 4). This section also collected information on the parents’ needs, concerns, difficulties, and recommendations, in which the following open-ended questions were asked: In general, what are your greatest needs and concerns related to your child with autism? What difficulties do you face related to speech, language, and/or communication services? Do you have any recommendations to improve current speech, language, and/or communication services for children with autism in Saudi Arabia? Regarding the open-ended questions, the data were analyzed quantitatively, as the answers were numerically coded and categorized.
Data Collection
A pilot test was conducted to assess the target group’s comprehension of the questionnaire items, the time required for data collection after pilot testing on a sample of 10 caregivers, and the internal consistency of the items. The questionnaire items were assessed in terms of their face validity and content validity by four experts who rated each item on a five-point Likert scale (1 = extremely irrelevant, 2 = irrelevant, 3 = slightly relevant, 4 = relevant, and 5 = strongly relevant). All items’ mean scores on the experts’ ratings were 3.5 or higher. The internal reliability and convergent validity of this scale were assessed through pilot testing on a sample of 10 caregivers who were excluded from the final analysis. The parents were asked questions related to their reasons for enrolling their children in speech, language, and/or communication sessions. In the last section about the parents’ perceptions of SLS, which included their levels of satisfaction with the SLS provided, the Cronbach’s alpha coefficient was 0.78. The Kuder–Richardson formula was used in the reliability analysis for questions about SLS, such as the availability and accessibility of these services, whether the child is still receiving SLS or has discontinued receiving them, and information about the child’s condition. The results showed that the subscale had a reliability of 0.81. Finally, the survey was distributed via different social media channels (Twitter, WhatsApp, and Telegram).
Ethical Considerations
The study complies with the Declaration of Helsinki. Ethical concerns were duly considered before conducting the study. First, ethical approval was secured from the Internal Review Board (IRB) of Princess Nourah bint Abdulrahman University (IRB Approval No. 22–993), and consent forms were provided to the parents, in which they indicated their willingness to participate in the study. They were assured of the confidentiality of their information.
Statistical Data Analysis
The collected data were analyzed using the Statistical Package for the Social Sciences version 28. The data analysis included frequency distributions for each measure of the sample. A graphical presentation of the data was created to organize them. This was followed by their classification into six major categories using a fishbone diagram and a Pareto chart created with MS Excel, using the data obtained from the parents’ reasons for either enrolling their children in SLS outside their cities or for discontinuing the sessions. In addition, Pearson’s chi-square test and likelihood ratios were used for all categorical variables to test for relationships in proportions across the questions. The results were considered statistically significant at p ≤ 0.05.
Results
General Characteristics of the Participants
Table 1 shows the general characteristics of children with ASD, as reported by their parents. The majority of the children were boys and lived in the central region of the KSA (78.9% and 60.6%, respectively). Most of them (46.8%) were in the age group of 8–10 years old. Table 1 also presents the ASD characteristics of the children, as reported by their parents. Most parents indicated that their children were diagnosed with ASD and that autistic behaviors were noticed for the first time at ages younger than four years (66.1% and 51.9%, respectively).
 |
Table 1 Characteristics of Children with Autism According to Their Parents (n = 109) |
Reasons Parents Use SLS
Only 22.1% of the respondents went outside their cities to attend other SLS clinics. Additionally, 46.8% of the parents reported that their children’s SLT sessions had already ended (Table 2). Based on the analysis of data, the parents’ primary reasons for enrolling their children in SLS were as follows: language delay (n = 103, 94.5%), no words used or use of only a few words (n = 90, 82.6%), communication issues (n = 83, 76.1%), and behavioral problems (n = 80, 73.5%; Table 3). Furthermore, most of the parents (79.8%) stated that their cities offered SLS.
 |
Table 2 Availability and Use of Speech Clinics According to the Parents (n = 109) |
 |
Table 3 Main Reasons for the Children’s Attendance at Speech Language Services (n = 109) |
When asked about their reasons for allowing their children to attend SL sessions outside their cities, the 25 parents who said they did so had the following reasons: a lack of SLS in their cities, a desire for higher-quality services, moving to a new neighborhood, and a desire for services other than speech and language. Service unavailability was the most frequently reported reason (44%), as shown in Figure 1.
 |
Figure 1 Parents’ reasons for letting their children attend speech language sessions outside their cities (n = 25). |
 |
Figure 2 Pareto chart ranking the reasons for the discontinuation of the children’s communication sessions (n = 51). |
Reasons for Discontinuing SLS
Table 4 and figure 2 present the reasons for discontinuing the SLS, as reported by the parents of the ASD children. The highlighted rows present the most significant reasons for the discontinuation of SLS. The high costs of the sessions, the need for initial behavioral sessions, the lack of qualified and specialized SLPs, the end of the sessions, a lack of improvement in the child, a lack of specialized centers, and the parents’ dependence on home training only accounted for 78% of all reasons for discontinuing the sessions. The remaining reasons (ie, nonavailability of services after the age of 10, long travel distance, and delay in the sessions) comprised the remaining 22%.
 |
Table 4 Percentage Values of the Reasons for Discontinuing Communication Sessions: Pareto Analysis |
The parents who reported that they had stopped receiving SLS sessions for their children were asked about the reasons for discontinuing them. As shown in the Pareto chart, among all the perceived causes for halting communication sessions, long distance had the highest cumulative percentage (Figure 3). The fishbone diagram also depicts the parents’ reasons for the discontinuation of the SLS sessions. These variables were divided into six main groups: child, parent, personnel, place, policy, and process (Figure 3).
 |
Figure 3 Fishbone diagram illustrating the different factors contributing to the end of the children’s communication sessions. |
Parents’ Satisfaction with the Provided SLS
Upon analyzing the levels of the parents’ satisfaction with the provided SLS on the basis of the characteristics of their ASD children, a statistically significant level of satisfaction was found in the group of parents of children aged 6–8 years [χ2 (6) = 12.86, p = 0.046]. Their satisfaction levels were significantly higher than those of parents of ASD children in the age group of less than 4 years [χ2 (8) = 12.25, p = 0.05]. However, neither the level of satisfaction nor the remaining characteristics of the ASD children showed statistical significance (p values >0.05; Table 5).
 |
Table 5 Parents’ Levels of Satisfaction with the Speech and Language Services Provided on the Basis of the Characteristics of Children with Autism (n = 109) |
Next, the parents’ levels of satisfaction with the SLS provided on the basis of the availability and use of speech clinics were analyzed. Those with children receiving SLS reported statistically significant levels of satisfaction [χ2 (2) = 6.92, p = 0.031]. Similarly, parents whose children attended SLS twice a week reported considerably better satisfaction levels [χ2 (10) = 15.86, p = 0.05]. Furthermore, significant levels of satisfaction were observed in two groups of parents: those who did not stop SLS sessions for their ASD children until the behavioral therapy sessions were completed [χ2 (4) = 12.01, p = 0.017] and those who had their children trained at home using the exercises used in the clinic [χ2 (4) = 11.733, p = 0.019; Table 6].
 |
Table 6 Parents’ Levels of Satisfaction with the Speech and Language Services Provided on the Basis of the Availability and Use Patterns of Speech Clinics (n = 109) |
Table 7 shows the parents’ levels of satisfaction with the SLS provided. A statistically significant level of satisfaction was observed in parents who were provided with sufficient information about their children’s conditions by the SLPs [χ2 (2) = 33.578, p < 0.001]. Similarly, their satisfaction levels were significantly higher [χ2 (2) = 40.313, p < 0.001] when they received sufficient information from the speech therapists on how to train their children with autism.
 |
Table 7 Parents’ Levels of Satisfaction with the SLS Received (n = 109) |
Moreover, those parents who trained their children at home using the exercises applied in the clinics and parents who believed that meeting with others going through the same experiences would encourage them to allow their children to continue attending the SLS sessions were more satisfied with the services provided [χ2 (4) = 11.733, p = 0.019 and χ2 (1) = 11.88, p =0.03, respectively].
All parents who felt respected and supported by their SLPs were satisfied with the services provided [χ2 (4) = 80.21, p < 0.001]. Furthermore, parents who found improvements in their children’s condition after receiving SLS (85.0%) were also satisfied with the services provided [χ2 (4) = 61.31, p < 0.001; Table 7].
Parents’ Needs, Concerns, and Perceived Difficulties Regarding the Provided SLS
Table 8 presents the needs reported by the parents of ASD children. The highlighted rows represent the most significant needs, which, if addressed, can enable parents to meet the majority of their needs. The following were the needs reported: methods for their children to express their needs, academic and employment opportunities, continuous and intensive sessions, reduced session costs, centers for adults with ASD, and accessible schools for children with ASD. These reasons constituted 79% of all identified needs. The remaining needs accounted for only 21% of the reported needs.
 |
Table 8 Percentage Values of the Reported Needs by the Parents: Pareto Analysis |
In the Pareto chart (Figure 4) ranking the perceived needs of parents with autistic children, accessible schools for their children had the highest cumulative percentage among all needs reported by the parents. Table 9 lists all the concerns reported by the parents of ASD children. The highlighted rows are the major concerns reported by the parents: child growing up with poor language and speech skills, lack of independence, child’s future, social interactions, and social acceptance. These constituted 79.59 (80%) of all reported concerns, and the remaining concerns accounted for only 20% of the total. Furthermore, in the Pareto chart (Figure 5) ranking the perceived concerns of parents with ASD children, being socially acceptable had the highest cumulative percentage among all concerns reported by the parents.
 |
Table 9 Percentage Values of the Reported Concerns by the Parents: Pareto Analysis |
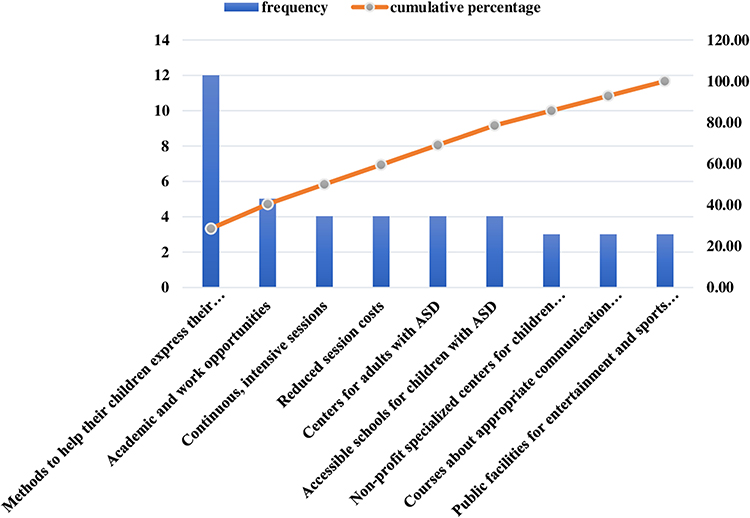 |
Figure 4 Pareto chart ranking the perceived needs of the parents of children with autism (n = 42). |
 |
Figure 5 Pareto chart ranking the concerns of the parents of children with autism (n = 49). |
Table 10 shows the difficulties reported by the parents of children with ASD. The highlighted rows indicate the most significant difficulties they encountered, including high session costs, shortage of services, shortage of experienced SLPs, irregular sessions, child’s refusal to attend the sessions, and short session durations, altogether constituting 78% of all the difficulties encountered by the parents. The remaining difficulties accounted for only 22% of the total. In Figure 6, the short duration of the sessions shows the highest cumulative percentage among all difficulties reported by the parents. Meanwhile, in Figure 7, the launch of new specialized ASD centers has the highest cumulative percentage among the reported recommendations by the parents.
 |
Table 10 Percentage Values of the Reported Difficulties by the Parents: Pareto Analysis |
 |
Figure 6 Pareto chart ranking the perceived difficulties of the parents of children with autism (n = 86). |
 |
Figure 7 Pareto chart ranking the recommendations of the parents of children with autism (n = 86). |
Table 11 lists the recommendations proposed by parents of ASD children. The highlighted rows present the most significant recommendations made by the parents: increasing the number of sessions, reducing session costs, and launching new specialized ASD clinics, which constituted 76% of all the reported recommendations. The remaining concerns accounted for 24% of the total.
 |
Table 11 Percentage Values of the Recommendations Made by the Parents: Pareto Analysis |
Discussion
This study explored the perceptions of parents of ASD children and their levels of satisfaction with the SLS provided in Saudi Arabia. This work also examined the potential reasons for parents’ discontinuation of SLS, along with their needs and concerns for their children. All these topics were investigated in this study to determine the relevant target areas for supporting parents of ASD children in the KSA.
Factors Associated with Parents’ Levels of Satisfaction with the SLS Provided
In this study, almost two-thirds of the parents reported that their children were diagnosed with ASD at an average age of less than 4 years, matching the findings of different studies.29,30 This age is considered early compared with those found in other studies31–33. Notably, parents who received an early diagnosis of ASD for their children (less than 4 years old) had significantly higher levels of satisfaction with the SLS provided than those whose children were diagnosed at later ages. It is possible that an early ASD diagnosis can enable a child to receive more healthcare services, thus reducing the severity of symptoms and improving the QoL of both the child and the caregiver34–36. Likewise, an early diagnosis can significantly influence parents’ responses and enable them to better cope with their children’s conditions.37,38
Similarly, the parents of children who had attended two SLT sessions per week reported considerably better satisfaction levels, which could be attributed to the improvements noted in their children’s conditions—a finding consistent with that of Adib et al.31 In a study conducted on ASD children who have speech sound disorders, the greatest improvement was observed when the children received an average of 2.57 SL sessions per week for a period of 6 weeks.39 Intensive interventions can also improve communication and daily social skills, thereby resulting in ASD children’s improved social behaviors.40
Parents’ involvement is essential for effective SLT.41 For children, caregiver involvement can lead to better interventions and language outcomes.42,43 For parents, participation in interventions can improve their parenting skills, reduce stress and conflict, and promote positive family interactions.44,45 Therefore, SLPs must provide parents with sufficient information and support on how to implement different intervention strategies at home and ensure that parents understand what they are doing.46 In the current study, the parents’ levels of satisfaction were significantly higher when they had easier access to SLS, higher perceived helpfulness of information obtained, greater training received on how to apply therapy exercises at home, and greater perceived respect and support from SLPs. Therefore, satisfaction can also be determined by the quality of the relationship between ASD children’s parents and SLPs.47
The availability of support groups can also reduce social isolation for the parents of ASD children, provide them access to relevant information, foster meaningful interactions with other parents of ASD children, and allow them to learn advocacy skills and gain confidence in their roles as parents.31,48,49 The parents in the current study reported that meeting with other people whose children had the same conditions facilitated the continuation of SLS sessions for their children and increased their levels of satisfaction with such services. This support group is also important in increasing awareness of ASD, thus helping parents and healthcare providers with the early detection of the disorder.29
Reported Difficulties and Potential Reasons for Discontinuing SLS and/or Seeking Services Outside the City
A Pareto chart was used to determine the main causes of discontinuing SLS so that necessary improvements could be made.50 Interestingly, the difficulties experienced by the parents in the current study seemed to be associated in one way or another with their tendency to discontinue receiving SLS for their children.
High SLS session costs were one of the most reported reasons to discontinue receiving the services, consistent with the literature investigating financial constraints as barriers to accessing different rehabilitation services.51–53 This financial concern is valid, as the average monthly cost of therapy sessions is reported to be between a quarter and a third of a family’s total monthly income in Jordan.14 A study conducted in the US found that the overall cost of raising a child with ASD across his/her lifespan is over USD1 million.10 Thus, families who have children with ASD are more likely to experience financial difficulties, require additional income to cover the costs of their children’s care, reduce their work hours because of their children’s conditions, and spend more than 10 hours per week providing or coordinating care compared with families whose children have other diagnoses.14,54,55
In the KSA, greater efforts have been directed toward improving the quality of healthcare services and facilities for all people with special needs, including ASD, consistent with Saudi Vision 2030. As previously mentioned, financial support is provided to ASD children through the MSA under certain conditions. Some, but not all, children receive services in private centers with full government sponsorship.16 Thus, families that do not receive government support tend to spend more funds enrolling in private centers to help their children (Khan et al, 2020). If no insurance is available, they must bear full treatment costs.56
Another reason reported by the parents for discontinuing their children’s SLS sessions and/or seeking services outside the city was the nonavailability of specialized centers, possibly in nonmajor cities; this could be the reason families travel to major cities, even outside the KSA, to receive ASD-specific services.57 In turn, this may increase treatment costs for children with ASD. The parents also reported insufficient education, knowledge, and skills among healthcare professionals, a finding consistent with the literature.16,57 The SLP educational program for undergraduate and graduate students in the KSA does not have a course that focuses solely on ASD; rather, ASD is just one of the topics within the course.58 This might have contributed to the insufficient knowledge and skills of SLPs regarding ASD.
Another reason reported by parents for discontinuing services was the irregular schedules of the SLS sessions, which can be attributed to the significant shortage of ASD services in the KSA.18 In addition, there is a shortage of SLPs working in health centers in the KSA, thus contributing to the high demand for SLS.59 It is recommended that all of the abovementioned issues should be taken into consideration by policymakers.
Required Support for Parents of Children with ASD
All parents want the best possible future for their children, but the parents of ASD children seem doubtful of the opportunities that the future can bring for their children. This is not surprising, as different studies have noted a lack of available support for parents and limited socialization, employment, and housing options for families with ASD children, especially those most affected by this disorder.60,61 A Pareto chart was used to analyze the data from 42 parents who expressed the most important forms of support that they needed.
One of the needs reported by the parents was having a method for their children to express their needs. The importance of communication for parents is probably linked to their fear that without language, their children will not be able to address their needs, particularly around strangers, or that, as parents, they may not know that their children have safety concerns, such as bullying.62 Nevertheless, the parents in the current study repeatedly mentioned the high costs of SLS and the need for frequent and consistent sessions, both of which were previously reported as the main reasons why parents discontinued SLS for their children. This issue is not surprising because, all over the world, families of children with ASD bear significant financial burdens. If this problem is not solved, the burden will spill over to society.63
Adults with ASD should have the same opportunities and rights as other people. However, because of the difficulties they encounter in terms of communication, social interactions, and sensory issues, they may experience challenges in the future. Unfortunately, as children with ASD become older, the use of rehabilitation services, including speech therapy, decreases.10,64,65 Therefore, centers for adults with ASD are needed, as reported by the parents in the current study. Training and support must also be provided for individuals with ASD so that they can later have jobs and participate meaningfully in society.66–68
The need for future employment opportunities for their ASD children has been reported by parents in Middle Eastern countries.69 This undertaking requires government assistance. The proper educational placement and future college lives of children with ASD must also be considered, because they require special educational support (ie, social, communication, and organizational support) and academic modifications.70 In this regard, government funds should be directed toward providing educational opportunities for children with ASD.71 Based on the findings above, a possible recommendation to meet most of the parents’ needs is to consider the provision of multidisciplinary team-related school services for ASD children. These involve the collaborative support of SLT, occupational therapy, physical therapy, and special education.
The parents in the present study also expressed other concerns. While many of these concerns faced by families caring for ASD children have been known for some time,72,73 the same concerns related to uncertainties about the continuity of care in the future,74,75 being independent and living a normal social life,74,76 and fear of bullying77,78 were expressed by the parents in the current study.
These needs and concerns highlight the importance of expanding the services provided to parents and their ASD children across the lifespan of the latter. Evidently, a high level of parents’ unmet needs can be resolved by the provision of optimal and affordable SLS and educational services. Therefore, greater financial, social, and emotional support could help parents better tailor the interventions and services provided to children with ASD in the future.
Moving on to other recommendations suggested by the parents in this study, the major suggestions were as follows: increased number of sessions, reduced session costs, and the launch of new specialized clinics. All these recommendations were previously reported as either concerns or difficulties. Therefore, healthcare providers (ie, SLPs) must determine parents’ needs, concerns, and challenges and then work toward meeting the former’s expectations so that the continuation of the desired care can be ensured.29 Furthermore, acceptable and sustained access to the necessary services in various health care settings must also be provided,79 including SLS, as this would eventually affect parents’ levels of satisfaction with the services provided.
Limitations and future research directions
While the current study provides valuable insights, several limitations should be considered. The first one is the small sample size, which limits the generalizability of the study to the KSA population. Furthermore, more parents living in other rural areas must be included to gain better knowledge of the difficulties and service restrictions they face.80 Second, this study used a self-reported questionnaire, which means that reporting bias can also be a limitation of this study. Thus, future research should consider the use of integrative techniques, such as mixed-method approaches (a combination of quantitative and qualitative studies). Furthermore, the inclusion of a specific age group in the current study might have accounted for non-response to the self-rating questionnaires, which must have influenced the high rate of non-completion of the survey. Finally, the study included only parents of ASD children from a younger age group. Future research should explore the difficulties and other challenges faced by parents of adolescents and adults with autism.
Conclusion
To the best of our knowledge, this is the first research in the KSA to investigate parents’ levels of satisfaction with SLS, the support structures, and their needs and concerns for their ASD children. Parents with ASD children reported increased satisfaction with early diagnosis, two weekly SLT sessions, adequate information and training, support from SLPs, and improved communication skills. They also sought opportunities for work and education, continuous and intensive SLS sessions, reduced costs, centers for adults with ASD, and accessible schools. The parents’ main concerns involved their children’s poor speech and language skills, independence, and social acceptance. However, difficulties such as high therapy session costs, shortages of specialized personnel, and irregular sessions hindered their children’s ability to continue receiving SLS.
The current study also highlighted the importance of understanding the experiences of parents with SLS, addressing the major factors that enhance the use of SLS by ASD children and improving their parents’ satisfaction with such services. The information obtained from the parents’ experiences can help SLPs and policymakers identify important areas for improvement. In the study, the parents repeatedly drew attention to the financial challenges they faced, in addition to other difficulties mostly related to limited specialized centers, the lack of SLPs, and the need for intensive and continuous SLS sessions throughout their children’s lives. The study further proposes the conduct of multidisciplinary team-related research and the provision of evidence-based school services that involve the collaborative support of special education and SL, occupational, and physical therapy specialists so that a holistic approach can be provided intensively and consistently for ASD children.
Acknowledgments
Our gratitude goes out to Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2024R126), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Funding
This research was funded by Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2024R126), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ibrahimagic A, Patkovic N, Radic B, Hadzic S. Communication and language skills of autistic spectrum disorders in children and their parents’ emotions. Materia Socio Medica. 2021;33(4):250. doi:10.5455/msm.2021.33.250-256
2. Lord C, Risi S, DiLavore PS, Shulman C, Thurm A, Pickles A. Autism from 2 to 9 years of age. Arch Gen Psychiatry. 2006;63(6):694–701. doi:10.1001/archpsyc.63.6.694
3. Alnemary FM, Alnemary FM, Simon-Cereijido G, et al. Factors associated with age of diagnosis of autism spectrum disorder among children in Saudi Arabia: new insights from a cross-sectional study. BMC Res Notes. 2022;15(1). doi:10.1186/s13104-022-06035-x
4. Stats. King Salman center for disability research. Available from: https://www.kscdr.org.sa/en/stats.
5. Health Days 2022. World autism awareness day. Available from: https://www.moh.gov.sa/en/HealthAwareness/HealthDay/2022/Pages/HealthDay-.
6. Park H, Park HY, Yoo E, Han A, Galeoto G. Impact of family-centered early intervention in infants with autism spectrum disorder: a single-subject design. Occup Ther Int. 2020;2020:1–7. doi:10.1155/2020/1427169
7. Kheir NM, Ghoneim OM, Sandridge AL, Hayder SA, Al-Ismail MS, Al-Rawi F. Concerns and considerations among caregivers of a child with autism in Qatar. BMC Res Notes. 2012;5(1):1–7. doi:10.1186/1756-0500-5-290
8. Karst JS, van Hecke AV. Parent and family impact of autism spectrum disorders: a review and proposed model for intervention evaluation. Clin Child Fam Psychol Rev. 2012;15(3):247–277. doi:10.1007/s10567-012-0119-6
9. Rogge N, Janssen J. The economic costs of autism spectrum disorder: a literature review. J Autism Dev Disord. 2019;49(7):2873–2900. doi:10.1007/s10803-019-04014-z
10. Buescher AVS, Cidav Z, Knapp M, Mandell DS. Costs of autism spectrum disorders in the United Kingdom and the United States. JAMA Pediatr. 2014;168(8):721–728. doi:10.1001/jamapediatrics.2014.210
11. Hussain SA, Ortendahl JD, Bentley TGK, et al. The economic burden of caregiving in epilepsy: an estimate based on a survey of US caregivers. Epilepsia. 2020;61(2):319–329. doi:10.1111/epi.16429
12. Järbrink K, McCrone P, Fombonne E, Zandén H, Knapp M. Cost-impact of young adults with high-functioning autistic spectrum disorder. Res Dev Disabil. 2007;28(1):94–104. doi:10.1016/j.ridd.2005.11.002
13. Tinelli MM, Roddy A, Knapp M, et al. Economic evaluation of anti-epileptic medicines for autistic children with epilepsy. J Autism Dev Disord. 2023. doi:10.1007/s10803-023-05941-8
14. Masri AT, Nasir AK, Irshaid AG, et al. Autism services in low-resource areas. Neurosciences. 2023;28(2):116–122. doi:10.17712/nsj.2023.2.20220098
15. Gobrial E. The lived experiences of mothers of children with the autism spectrum disorders in Egypt. Soc Sci. 2018;7(8):133. doi:10.3390/socsci7080133
16. Al-Dakroury WA, Alnemary FM, Alnemary F. Autism in the Kingdom of Saudi Arabia: current situation and future perspectives for services and research. Perspect ASHA Spec Interest Groups. 2022;7(6):2104–2109. doi:10.1044/2022_persp-22-00087
17. Human Resources and Social Development. Financial subsidy service for people with disability. Available from: https://www.hrsd.gov.sa/en/ministry-services/services/69895.
18. Babatin AM, Alzahrani BS, Jan FM, Alkarimi EH, Jan MM. The availability of services for children with autism spectrum disorder in a Saudi population. Neurosciences. 2016;21(3):223–226. doi:10.17712/nsj.2016.3.20150597
19. Al-Jabri BA, Abualhamael RM, Al Hazza MT, Bahabri SA, Alamri YM, Alghamdi BM. Quality of life of caregivers of autistic children in Saudi Arabia: cross-sectional study. Neurosciences. 2022;27(3):150–155. doi:10.17712/nsj.2022.3.20210141
20. Asiri F, Tedla JS, Sangadala DR, et al. Quality of Life among Caregivers of Children with Disabilities in the Kingdom of Saudi Arabia: a Systematic Review. J Disabil Res. 2023;2(2). doi:10.57197/jdr-2023-0016
21. Chiri G, Warfield ME. Unmet need and problems accessing core health care services for children with autism spectrum disorder. Matern Child Health J. 2012;16(5):1081–1091. doi:10.1007/s10995-011-0833-6
22. Kogan MD, Strickland BB, Blumberg SJ, Singh GK, Perrin JM, Van Dyck PC. A national profile of the health care experiences and family impact of autism spectrum disorder among children in the United States, 2005–2006. Pediatrics. 2008;122(6):2005–2006. doi:10.1542/peds.2008-1057
23. Taylor JL, Henninger NA, Mailick MR. Longitudinal patterns of employment and postsecondary education for adults with autism and average-range IQ. Autism. 2015;19(7):785–793. doi:10.1177/1362361315585643
24. Kamenov K, Mills JA, Chatterji S, Cieza A. Needs and unmet needs for rehabilitation services: a scoping review. Disabil Rehabil. 2019;41(10):1227–1237. doi:10.1080/09638288.2017.1422036
25. Auert EJ, Trembath D, Arciuli J, Thomas D. Parents’ expectations, awareness, and experiences of accessing evidence-based speech-language pathology services for their children with autism. Int J Speech Lang Pathol. 2012;14(2):109–118. doi:10.3109/17549507.2011.652673
26. Siklos S, Kerns KA. Assessing need for social support in parents of children with autism and Down syndrome. J Autism Dev Disord. 2006;36(7):921–933. doi:10.1007/s10803-006-0129-7
27. Dardas LA, Ahmad MM. For fathers raising children with autism, do coping strategies mediate or moderate the relationship between parenting stress and quality of life? Res Dev Disabil. 2015;36:620–629. doi:10.1016/j.ridd.2014.10.047
28. Dean AG. OpenEpi: open Source Epidemiologic Statistics for Public Health; 2007. Available from: http://www.openepi.com/Menu/OE_Menu.htm.
29. Chamak B, Bonniau B, Oudaya L, Ehrenberg A. The autism diagnostic experiences of French parents. Autism. 2011;15(1):83–97. doi:10.1177/1362361309354756
30. Linnsand P, Gillberg C, Nilses Å, Hagberg B, Nygren G. A High Prevalence of Autism Spectrum Disorder in Preschool Children in an Immigrant, Multiethnic Population in Sweden: challenges for Health Care. J Autism Dev Disord. 2021;51(2):538–549. doi:10.1007/s10803-020-04563-8
31. Adib NAN, Ibrahim MI, Rahman AA, et al. Predictors of caregivers’ satisfaction with the management of children with autism spectrum disorder: a study at multiple levels of health care. Int J Environ Res Public Health. 2019;16(10):1–18. doi:10.3390/ijerph16101684
32. Lamba N, Van Tonder A, Shrivastava A, Raghavan A. Exploring challenges and support structures of mothers with children with Autism Spectrum Disorder in the United Arab Emirates. Res Dev Disabil. 2022;120:104138. doi:10.1016/j.ridd.2021.104138
33. van’t Hof M, Tisseur C, van Berckelear-Onnes I, et al. Age at autism spectrum disorder diagnosis: a systematic review and meta-analysis from 2012 to 2019. Autism. 2021;25(4):862–873. doi:10.1177/1362361320971107
34. Lord C, Brugha TS, Charman T, et al. Autism spectrum disorder. Nat Rev Dis Primers. 2020;6(1). doi:10.1038/s41572-019-0138-4
35. Malhi P, Prasad KVD, Suthar R. Satisfaction with the Journey of Receiving a Diagnosis of Autism: experiences of Indian Parents. Indian J Soc Psychiatry. 2023;39(2):168–174. doi:10.4103/ijsp.ijsp_331_20
36. Zwaigenbaum L, Bauman ML, Choueiri R, et al. Early Intervention for children with autism spectrum disorder under 3 years of age: recommendations for practice and research. Pediatrics. 2015:136:S60–S81. doi:10.1542/peds.2014-3667E
37. Lappé M, Lau L, Dudovitz RN, Nelson BB, Karp EA, Kuo AA. The diagnostic odyssey of autism spectrum disorder. Pediatrics. 2018;141(Supplement 4):S272–S279. doi:10.1542/peds.2016-4300C
38. Legg H, Tickle A. UK parents’ experiences of their child receiving a diagnosis of autism spectrum disorder: a systematic review of the qualitative evidence. Autism. 2019;23(8):1897–1910. doi:10.1177/1362361319841488
39. Beiting M, Maas E. Autism-centered therapy for childhood apraxia of speech (Act4cas): a single-case experimental design study. Am J Speech Lang Pathol. 2021;30(3s):1525–1541. doi:10.1044/2020_AJSLP-20-00131
40. Potter CA. Father involvement in the care, play, and education of children with autism. J Intellect Dev Disabil. 2017;42(4):375–384. doi:10.3109/13668250.2016.1245851
41. National Research Council. Educating Children with Autism. National Academies Press; 2001.
42. Green J, Charman T, McConachie H, et al. Parent-mediated communication-focused treatment in children with autism (PACT): a randomised controlled trial. Lancet. 2010;375(9732):2152–2160. doi:10.1016/S0140-6736(10)60587-9
43. Hampton LH, Kaiser AP. Intervention effects on spoken-language outcomes for children with autism: a systematic review and meta-analysis. J Intellectual Disability Res. 2016;60(5):444–463. doi:10.1111/jir.12283
44. Kuravackel GM, Ruble LA, Reese RJ, Ables AP, Rodgers AD, Toland MD. COMPASS for Hope: evaluating the effectiveness of a parent training and support program for children with ASD. J Autism Dev Disord. 2018;48(2):404–416. doi:10.1007/s10803-017-3333-8
45. Laxman DJ, McBride BA, Jeans LM, et al. Father involvement and maternal depressive symptoms in families of children with disabilities or delays. Matern Child Health J. 2015;19(5):1078–1086. doi:10.1007/s10995-014-1608-7
46. Flippin M, Hahs-Vaughn DL. Parent couples’ participation in speech-language therapy for school-age children with autism spectrum disorder in the United States. Autism. 2020;24(2):321–337. doi:10.1177/1362361319862113
47. Moh TA, Magiati I. Factors associated with parental stress and satisfaction during the process of diagnosis of children with autism spectrum disorders. Res Autism Spectr Disord. 2012;6(1):293–303. doi:10.1016/j.rasd.2011.05.011
48. Ludlow A, Skelly C, Rohleder P. Challenges faced by parents of children diagnosed with autism spectrum disorder. J Health Psychol. 2012;17(5):702–711. doi:10.1177/1359105311422955
49. Perreault M, Rousseau M, Provencher H, Roberts S, Milton D. Predictors of caregiver satisfaction with mental health services. Community Ment Health J. 2012;48(2):232–237. doi:10.1007/s10597-011-9403-z
50. Claire L What Is a Pareto Chart? Definition & Examples; 2019. Available from: https://tulip.co/blog/what-is-a-pareto-chart-definition-examples/.
51. Noori F, Tiwari S, Padickaparambil S, Pothiyil DI. Parenting challenges and reasons for not availing rehabilitation services among families of adolescents with autism spectrum disorder: a qualitative study. Indian J Psychol Med. 2023;45(3):263–270. doi:10.1177/02537176221096769
52. Roddy Á, O’Neill C. Predictors of unmet needs and family debt among children and adolescents with an autism spectrum disorder: evidence from Ireland. Health Policy. 2020;124(3):317–325. doi:10.1016/j.healthpol.2020.01.005
53. Subramanyam AA, Mukherjee A, Dave M, Chavda K. Clinical practice guidelines for autism spectrum disorders. Indian J Psychiatry. 2019;61(8):S254–S269. doi:10.4103/psychiatry.IndianJPsychiatry_542_18
54. Mandak K, Light J. Family-centered services for children with ASD and limited speech: the experiences of parents and speech-language pathologists. J Autism Dev Disord. 2018;48(4):1311–1324. doi:10.1007/s10803-017-3241-y
55. Saunders BS, Tilford JM, Fussell JJ, Schulz EG, Casey PH, Kuo DZ Families, Systems, & Health; 2015.
56. Khan A, AlGhadeer H, Al-Qassimi A, Al-Jubran T, Al-Momen H, Al-Nazzal M. Autism in Saudi Arabia, a challenge to Saudi families: a cross-sectional study. Int J Med Diabetes Dev Ctries. 2020;4:1453–1458. doi:10.24911/ijmdc.51-1595277794
57. Alnemary FM, Aldhalaan HM, Simon-Cereijido G, Alnemary FM. Services for children with autism in the Kingdom of Saudi Arabia. Autism. 2017;21(5):592–602. doi:10.1177/1362361316664868
58. Beverly BL, Mathews LA. Speech-language pathologist and parent perspectives on speech-language pathology services for children with autism spectrum disorders. Focus Autism Other Dev Disabl. 2021;36(2):121–132. doi:10.1177/1088357620954380
59. Alakeel AI. The practice of speech-language pathology in Saudi Arabia. Arab Journal of Applied Linguistics. 2022;7(1):86–98.
60. Gray DE. Autism and the Family: Problems, Prospects, and Coping with the Disorder. 2600 South First Street, Springfield, IL 62704; tele: Charles C Thomas Publisher, Ltd; 1998.
61. Mastropieri MA, Scruggs TE. Decreasing inappropriate behaviors for adolescents with autism spectrum disorders using modified social stories. Educ Train Autism Dev Disabil. 2009;44(1):91–104.
62. DuBay M, Watson LR, Zhang W. In search of culturally appropriate autism interventions: perspectives of latino caregivers. J Autism Dev Disord. 2018;48(5):1623–1639. doi:10.1007/s10803-017-3394-8
63. The financial side of autism: private and public costs. A Comprehensive Book on Autism Spectrum Disorders. 2011.
64. Mire SS, Raff NS, Brewton CM, Goin-Kochel RP. Age-related trends in treatment use for children with autism spectrum disorder. Res Autism Spectr Disord. 2015;15–16:29–41. doi:10.1016/j.rasd.2015.03.001
65. Shivers CM, Sonnier-Netto L, Lee GK. Needs and experiences of family caregivers of individuals with autism spectrum disorders across the Lifespan. J Policy Pract Intellect Disabil. 2019;16(1):21–29. doi:10.1111/jppi.12272
66. Mawhood L, Howlin P. The outcome of a supported employment scheme for high-functioning adults with autism or Asperger syndrome. Autism. 1999;3(3):229–254. doi:10.1177/1362361399003003003
67. Simone R. Asperger’s on the Job: must-have advice for people with Asperger’s or high functioning autism, and their employers, educators, and advocates. Future Horizons; 2010.
68. Thomas KC, Ellis AR, McLaurin C, Daniels J, Morrissey JP. Access to care for autism-related services. J Autism Dev Disord. 2007;37(10):1902–1912. doi:10.1007/s10803-006-0323-7
69. Olsen PM. Raising a Child with Autism: Perspectives from Arab-Muslim Mothers. The Chicago School of Professional Psychology; 2016.
70. VanBergeijk E, Klin A, Volkmar F. Supporting more able students on the autism spectrum: college and beyond. J Autism Dev Disord. 2008;38(7):1359–1370. doi:10.1007/s10803-007-0524-8
71. Alyami HS, Naser AY, Alyami MH, Alharethi SH, Alyami AM. Knowledge and Attitudes toward Autism Spectrum Disorder in Saudi Arabia. Int J Environ Res Public Health. 2022;19(6):3648. doi:10.3390/ijerph19063648
72. Howlin P, Goode S, Hutton J, Rutter M. Adult outcome for children with autism. J Child Psychol Psychiatr. 2004;45(2):212–229. doi:10.1111/j.1469-7610.2004.00215.x
73. Hastings RP, Kovshoff H, Brown T, Ward NJ, Espinosa FD, Remington B. Coping strategies in mothers and fathers of preschool and school-age children with autism. Autism. 2005;9(4):377–391. doi:10.1177/1362361305056078
74. Desai MU, Divan G, Wertz FJ, Patel V. The discovery of autism: indiaN parents’ experiences of caring for their child with an autism spectrum disorder. Transcult Psychiatry. 2012;49(4):613–637. doi:10.1177/1363461512447139
75. Ravindran N, Myers BJ. Beliefs and practices regarding autism in Indian families now settled abroad: an internet survey. Focus Autism Other Dev Disabl. 2013;28(1):44–53. doi:10.1177/1088357612458970
76. Shu BC, Lung FW, Tien AY, Chen BC. Executive function deficits in non-retarded autistic children. Autism. 2001;5(2):165–174. doi:10.1177/1362361301005002006
77. An S, Chan CK, Kaukenova B. Families in transition: parental perspectives of support and services for children with autism in Kazakhstan. Intl J Disabil Dev Educ. 2020;67(1):28–44. doi:10.1080/1034912X.2018.1499879
78. Ha VS, Whittaker A, Whittaker M, Rodger S. Living with autism spectrum disorder in Hanoi, Vietnam. Soc Sci Med. 2014;120:278–285. doi:10.1016/j.socscimed.2014.09.038
79. Russell S, McCloskey CR. Parent perceptions of care received by children with an autism spectrum disorder. J Pediatr Nurs. 2016;31(1):21–31. doi:10.1016/j.pedn.2015.11.002
80. Malik-Soni N, Shaker A, Luck H, et al. Tackling healthcare access barriers for individuals with autism from diagnosis to adulthood. Pediatr Res. 2022;91(5):1028–1035. doi:10.1038/s41390-021-01465-y
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.