")
Back to Journals » International Journal of Nephrology and Renovascular Disease » Volume 16
Emerging Role of Sodium–Glucose Co-Transporter 2 Inhibitors for the Treatment of Chronic Kidney Disease
Authors Isidto R , Danguilan R, Naidas O , Vilanueva R, Arakama MH, Paraiso LM
Received 13 September 2022
Accepted for publication 24 December 2022
Published 21 February 2023 Volume 2023:16 Pages 43—57
DOI https://doi.org/10.2147/IJNRD.S387262
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Pravin Singhal
Rey Isidto,1 Romina Danguilan,2 Oscar Naidas,3 Russell Vilanueva,2 Mel-Hatra Arakama,2 Layla Marie Paraiso2
1HealthLink Medical, Surgical, Dental Clinics and Diagnostic Center, Iloilo City, Iloilo, Philippines; 2Department of Adult Nephrology, National Kidney and Transplant Institute, Quezon City, Manila, Philippines; 3Department of Adult Nephrology, St. Luke’s Medical Center, Quezon City, Manila, Philippines
Correspondence: Rey Isidto, HealthLink Medical, Surgical, Dental Clinics and Diagnostic Center, Iloilo City, Iloilo, Philippines, Tel +63 9178406232, Fax +63 33 3303863, Email [email protected]
Abstract: Chronic kidney disease is one of the leading causes of morbidity and mortality in the Philippines. It is associated with a growing health burden as many patients progress to end-stage renal disease. Until recently, therapeutic options for the management of chronic kidney disease were limited. Sodium–glucose co-transporter 2 inhibitors offer an alternative therapeutic approach for patients with chronic kidney disease. Several trials have shown renal benefits with sodium–glucose co-transporter 2 inhibitors in patients with cardiovascular disease with and without type 2 diabetes and across a range of estimated glomerular filtration rate levels. In the Philippines, the sodium–glucose co-transporter 2 inhibitors dapagliflozin and canagliflozin are approved for the prevention of new and worsening nephropathy in type 2 diabetes. With emerging treatment options, an urgent need exists for guidance on the management of chronic kidney disease within the Philippines. In this review, we focus on the putative renal-protective mechanisms of sodium–glucose co-transporter 2 inhibitors, including effects on tubuloglomerular feedback, albuminuria, endothelial function, erythropoiesis, uric acid levels, renal oxygen demand, and hypoxia. Furthermore, we discuss the findings of recent large clinical trials using sodium–glucose co-transporter 2 inhibitors in patients with chronic kidney disease and diabetic kidney disease, summarize safety aspects, and outline the practical management of patients with chronic kidney disease in the Philippines.
Keywords: chronic renal insufficiency, diabetic nephropathies, safety, sodium-glucose transporter 2 inhibitors
Introduction
Globally, chronic kidney disease (CKD) exerts a major patient and public burden, affecting almost 843.6 million individuals.1,2 Angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptor blockers (ARBs) are the predominant pharmacological interventions available for the treatment of diabetic kidney disease (DKD) and non-DKD, albeit with limitations.3,4 Concomitant treatment with an ACE inhibitor and ARB is associated with an increased risk of adverse events in patients with diabetic nephropathy.5 A meta-analysis of 22 randomized controlled trials reported that both ACE inhibitors and ARBs increased the risk of developing hyperkalaemia in patients with CKD stages 3–5 with a glomerular filtration rate (GFR) of <60 mL/min per 1.73 m2 and elevated serum creatinine levels.4 Only 52–81% of the patients with CKD stages 3–5 receive renin–angiotensin system (RAS) blockers.6
Despite available treatments, the global annual incidence of end-stage renal disease (ESRD) among patients with diabetes had increased from 375.8 to 1016.0 per million during 2000–2015, according to the latest published data.7 During this period, the incidence of ESRD increased dramatically in Southeast Asia, and this region was reported as having the second highest incidence of ESRD globally.7 Strict blood glucose with anti-diabetic therapies and blood pressure control by inhibition of angiotensin has been shown to be unable to stop disease progression to ESRD.8,9 Therefore, new alternative treatment strategies are needed to effectively treat patients with CKD.
Sodium–glucose co-transporter 2 (SGLT2) inhibitors have evolved from a novel hypoglycemic agent, to potent cardio- and renoprotective agent in type 2 diabetes (T2D), and recently, to an effective standalone therapeutic option for CKD regardless of the presence of diabetes mellitus (DM).9 SGLT-2 is predominantly expressed in the proximal renal tubule, and accounts for 90% of renal glucose reabsorption. By inhibiting SGLT2, the glucose and sodium reabsorption is decreased, the tubule-glomerular feedback is restored and the aforementioned damage is undone.10 Large-scale cardiovascular outcome trials investigating SGLT2 inhibitors have demonstrated that these therapies have renoprotective effects distinct from their glucose-lowering action, including the potential to reduce ESRD and acute kidney injury rates.11,12 Recent studies conducted in patients with moderate-to-severe CKD, SGLT2 inhibitors (canagliflozin, dapagliflozin) showed renoprotective effects.12,13 SGLT2 inhibitors therefore represent an alternative or adjunct to current treatment approaches in the management of CKD in patients with and without T2D. In the Philippines, dapagliflozin is approved for the prevention of new and worsening nephropathy in T2D, and canagliflozin is approved for use in patients with CKD and albuminuria.14,15 Due to the continuous increase in the number of patients progressing to ESRD from diabetes mellitus,7 an urgent need for guidance on the management of CKD within the Philippines exists, especially with emerging treatment options. The aim of this manuscript is to review the epidemiology of CKD in Philippines and recent large clinical-outcome trials of SGLT2 inhibitors in patients with CKD, putative renal-protective mechanisms of action of SGLT2 inhibitors, and the practical management of patients with CKD.
Epidemiology of CKD in the Philippines
The prevalence of CKD in Asia was estimated to be 434.3 million (95% confidence interval (CI) 350.2 to 519.7) in a recent systematic review and meta-analysis.16 The average prevalence of CKD stages 3–5 in Asia was 11.2%; the prevalence of CKD stages 3–5 varied among subregions (East Asia: 8.6%, South-East Asia: 12.0%, Western Asia: 13.1%, South Asia: 13.5%.17 In 2017, the prevalence of CKD in Southeast Asia was almost 70 million people.1 Asian patients with T2D have high rates of kidney disease,18,19 with 58.6% having microalbuminuria or macroalbuminuria.18 Furthermore, a higher proportion of Southeast Asian patients with T2D develop nephropathy and progressive kidney failure at a much younger age than their European counterparts.19 A study conducted in Manila reported a high prevalence (42%) of nephropathy among patients newly diagnosed with T2D.20 A recent retrospective study conducted by Crisostomo and Allyn Sy has also reported high nephropathy rate (about 40%) in patients with newly diagnosed with T2D.21 In 2017, the prevalence of CKD in the Philippines was 9,317,802, with 34,051 CKD-attributed deaths.1 In 2019, CKD was the fourth leading cause of mortality in the Philippines.22 According to a 2015 systematic review, the use of renal replacement therapy (RRT) in Asia is expected to rise sharply in the next decade.23
According to the latest World Health Organization data published in 2020 Kidney Disease Death rate in Philippines reached 51.96% or 5.84% of the total deaths.24 A database including current data on CKD is unavailable in the Philippines. CKD management in the Philippines is an important issue yet is limited by a paucity of published data on CKD. The Philippine Renal Disease Registry, with most recent data from 2016, for example, predominantly reports RRT data, underscoring the rising number of patients receiving dialysis but not including data on patients with CKD stages 1 to 4.25 According to Philippine Renal Disease Registry 2020 Annual report, in 2016, the incidence and prevalence of patients undergoing dialysis for ESRD in the Philippines was 21,535 and 37,280, respectively.25 By 2025, the number of patients with ESRD in the Philippines is expected to increase by 10–20%.26 According to a 2019 report, PhilHealth (a national health insurance program) spent over 10.6 billion Philippine pesos for 2,187,846 haemodialysis claims, which ranked first among the top 10 medical procedures.27 These data underscore the incredible burden of RRT and the need for treatments that can mitigate CKD progression, which could help offset the high costs of RRT.2
Data on Filipino patients with CKD are scarce, but a single-centre study on CKD education reported that among 299 financially disadvantaged patients with CKD, 60% were men, mean age was 49 years, and 37% were high-school graduates.28 A total of 30% of the patients had chronic glomerulonephritis as the primary renal disease, and 60% initially presented to the tertiary renal referral centre with CKD stage 5. When evaluated prior to consultation at the study site, 43.1% of the patients did not know about the seriousness of CKD, and 17.7% thought CKD was not serious.28 Overall, these data suggest a gap in the screening and diagnosis of CKD in the Philippines that warrants further study.
Background on SGLT2 Inhibitors
In healthy individuals, the kidneys play an important role in glucose homeostasis through gluconeogenesis and the active reabsorption of nearly all the glucose filtered by the glomerulus.29 Sodium–glucose co-transporters significantly contribute to renal glucose reabsorption. SGLT1 is a high-affinity, low-capacity transporter responsible for a small proportion of the renal glucose reabsorption; it is primarily located in the small intestine but is also found in the S3 segment of the renal proximal tubule (PT) and other tissues.30–33
SGLT2 is a low-affinity, high-capacity transporter responsible for most of the renal glucose reabsorption; it is located in the S1 and S2 segments of the renal PT.31–34 When initially approved, SGLT2 inhibitors were contraindicated in patients with estimated glomerular filtration rate (eGFR) <60 mL/min per 1.73 m2 because of their decreased glucose-lowering efficacy with decreasing kidney function, reflecting their mode of action.35 Since then, numerous trials have demonstrated renal benefits with various SGLT2 inhibitors in patients with T2D with and without CKD and with various types of cardiovascular disease (CVD), supporting their use in patients with eGFR ≥30 mL/min per 1.73 m2.13,36 In the Philippines, dapagliflozin was recently approved for the prevention of new or worsening nephropathy in patients with T2D with eGFR ≥45 mL/min per 1.73 m2.14
Various American (eg, American Diabetes Association,37 American College of Cardiology38), European (eg, European Society of Cardiology, European Association for the Study of Diabetes39), and global (eg, Kidney Disease: Improving Global Outcomes40) guidelines recommend the use of SGLT2 inhibitors in patients with CKD and T2D. Given the very recent publication of some large clinical-outcome trials of SGLT2 inhibitors (Table 1), some guidelines remain to be updated based on the results of those trials, particularly for patients with CKD without T2D. For example, the latest CKD guidelines from the European Renal Association—European Dialysis and Transplant Association are from 2016.41 There is increasing activity aimed at developing local guidelines in Asia (Japan, China, Korea, the Philippines, and Indonesia).42 The Asian Pacific Society of Nephrology Clinical Practice Guideline on Diabetic Kidney Disease recommends the use of SGLT2 inhibitors in adults with T2D and eGFR ≥30 mL/min per 1.73 m2 who have DKD or CVD.43 In the completed clinical-outcome trials, renal benefits of SGLT2 inhibitors were demonstrated at decreasing levels of baseline kidney dysfunction (as reflected by varying levels of eGFR and albuminuria), independent of the glucose-lowering effects of SGLT2 inhibitors, the presence of T2D, or the use of RAS blockers.13,44–47
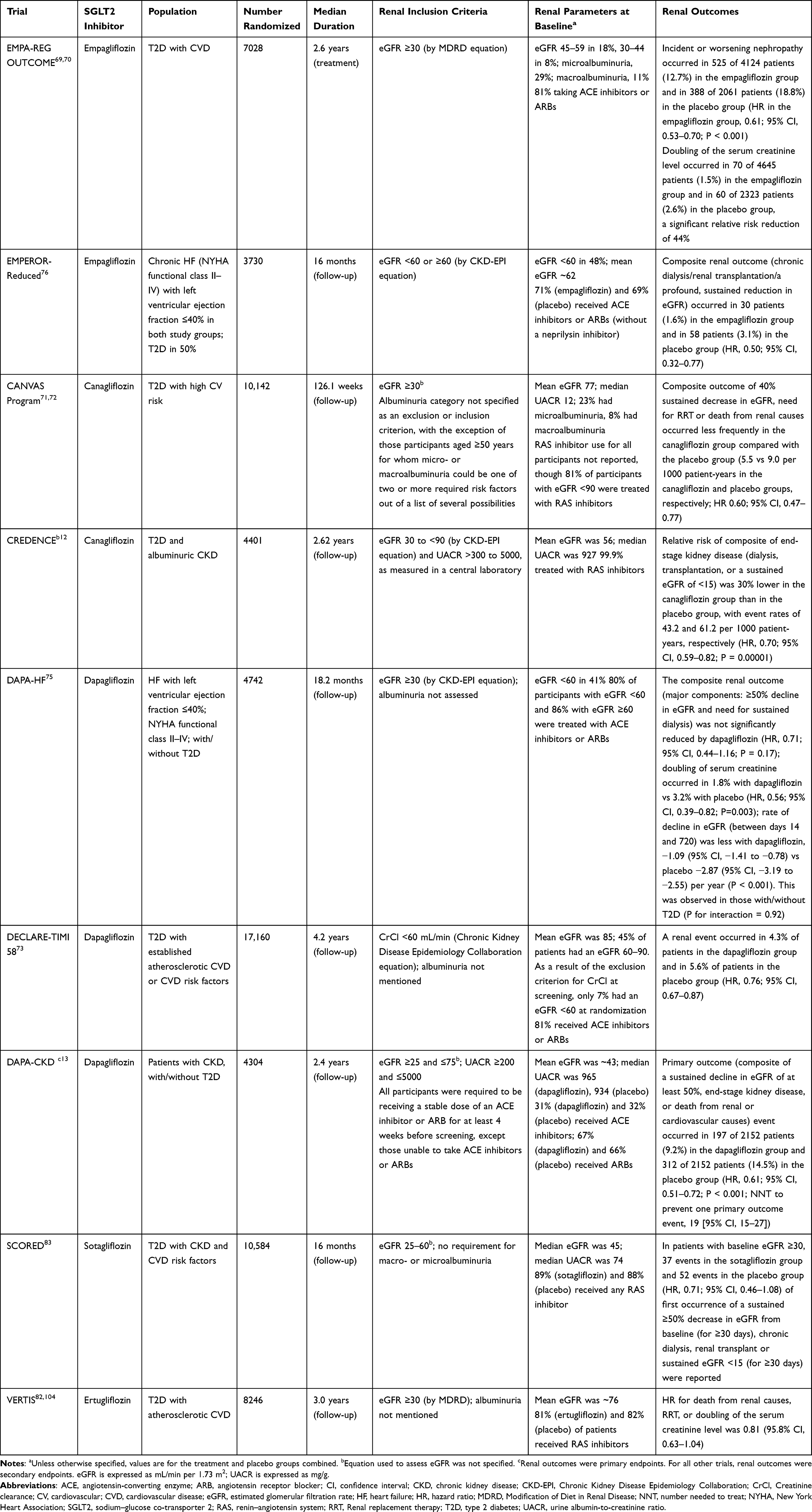 |
Table 1 Randomized, Double-Blind Clinical Trials of SGLT2 Inhibitors with Renal Outcomes |
Potential Renal-Protective Mechanisms of SGLT2 Inhibitors
Various mechanisms that could explain the beneficial renal effects of SGLT2 inhibitors have been postulated and reviewed.30,48 Although clinical trial data support the existence of renal-protective mechanisms with SGLT2 inhibition, given the complexity and number of potential mechanisms involved, caution should be exercised in attributing the beneficial renal effects of SGLT2 inhibitors to any single mechanism. The proposed mechanisms, which include direct effects on renal physiology and anti-inflammatory, anti-hypertensive, and anti-fibrotic effects,48 may work synergistically, with some mechanisms contributing to a greater extent under certain clinical settings. The schematic diagram on potential renal-protective mechanisms of SGLT2 inhibitors is presented in Figure 1.49
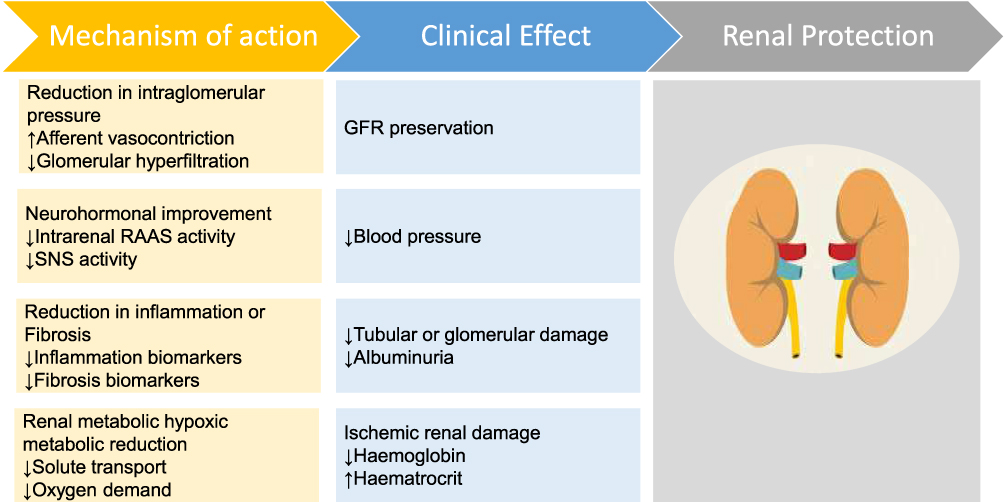 |
Figure 1 Schematic diagram on potential renal-protective mechanisms of SGLT2 inhibitors. Abbreviations: GFR, glomerular filtration rate; RAAS, renin–angiotensin–aldosterone system; SNS, sympathetic nervous system. Notes: The up and down arrows in white boxes indicate an increase and decrease, respectively. Adapted from Leoncini G, Russo E, Bussalino E, Barnini C, Viazzi F, Pontremoli R. SGLT2is and renal protection: from biological mechanisms to real-world clinical benefits. Int J Mol Sci. 2021;22(9):4441. doi:10.3390/ijms22094441.49 |
Insight into some of the mechanisms of SGLT2 inhibition was provided by the randomized, placebo-controlled, multicentre DIAMOND study, which examined the effects of 6 weeks of treatment with dapagliflozin on proteinuria in patients with non-diabetic CKD and residual proteinuria.50 Dapagliflozin did not reduce glycated haemoglobin, proteinuria, or fasting plasma glucose and did not affect urine adenosine or other vasoactive mediators. The 6-week timeframe of DIAMOND was probably too short for the reduced glomerular pressure caused by SGLT2 inhibition to affect proteinuria.50 Dapagliflozin did affect body weight and haemoconcentration biomarkers, and reduced measured GFR, which was completely reversible within 6 weeks of drug discontinuation.50 This suggests SGLT2 inhibition ameliorates kidney function, independent of its glycaemic effects. Further mechanistic research is anticipated, especially given the important differences in pathogenic mechanisms between DKD and non-DKD.51
Tubuloglomerular Feedback
In diabetes, increased glucose and sodium reabsorption in the renal PT leads to increased adenosine triphosphate (ATP) and oxygen demand.45,52 Adenosine is an important signalling factor for tubuloglomerular feedback (TGF) at the macula densa (MD).53 Excessive sodium reabsorption in the renal PT also leads to decreased sodium delivery to the MD.54 This decreases the adenosine production due to reduced consumption of ATP at the MD, and therefore reduces TGF, leading to increased glomerular pressure or RAS activity. SGLT2 inhibition increases sodium delivery to the MD,54 thereby increasing the ATP consumption and adenosine production.55 The increase in adenosine causes vasoconstriction of the afferent arteriole, leading to a reduction in intraglomerular hypertension and a decrease in eGFR.30,35,54–56 Overall, by promoting specific intrarenal haemodynamic changes, SGLT2 inhibitors may protect glomeruli from barotrauma.45,48
Albuminuria
Reductions in albuminuria may also offer protection against renal damage. Adding dapagliflozin to ACE inhibitor or ARB therapy in hypertensive patients with T2D reduced albuminuria as early as 4 weeks from treatment initiation.57 However, SGLT2 inhibitors’ renal benefits independent of baseline albuminuria, as seen in large clinical trials, suggest that non–albuminuria-lowering mechanisms additionally account for the renal benefits.47
Endothelial Function
Endothelial cells are important in not only the vasculature but also the kidney, given the endothelial cells’ exposure to the circulation and any toxins. Increased sodium levels can have undesirable effects on vascular contractility by damaging the glycocalyx lining of the endothelial vascular walls and stiffening the vessels.58,59 SGLT2 inhibition, by lowering blood glucose and sodium levels, reduces aortic stiffness and improves endothelial function, conduit arterial function, and vascular tone.60,61 Mechanistic studies in patients with T2D demonstrate a direct beneficial effect on the vasculature associated with a decline in markers of oxidative stress.61 The mechanisms and the extent to which these renal benefits are exerted in patients with CKD without T2D remain to be elucidated.
Erythropoiesis
Treatment with SGLT2 inhibitors transiently increases erythropoietin levels.56 Mechanisms beyond haemoconcentration, such as reverse renal remodelling, could contribute to the effect on erythropoietin.62 The increase in haematocrit associated with SGLT2 inhibition may be due to the normalization of renal cortical oxygenation resulting in the normalization of erythropoietin-producing cell function.62 Further studies are needed to investigate the degree to which the increased haematocrit reported with SGLT2-inhibitor treatment is a safety or efficacy signal.
Uric Acid Levels
Increased serum uric acid levels are associated with high risk for renal diseases and all-cause mortality.63,64 Hyperuricaemia may trigger proinflammatory cytokines, resulting in vascular and tubulointerstitial lesions, which eventually promote the development of CKD.65 Additionally, hyperuricaemia induces hypertension by activating the RAS and inhibiting nitric oxide synthesis, promoting endothelial dysfunction, vascular smooth-muscle cell proliferation, and sodium reabsorption. SGLT2 inhibition reduces serum uric acid levels,66 possibly indirectly via modulation of glucose transporter 9.63 However, subgroup analyses of a meta-analysis did not show a serum uric acid–lowering effect in patients with CKD.66
Renal Oxygen Demand and Hypoxia
Sodium reabsorption drives renal oxygen consumption.67 SGLT1 and SGLT2 inhibition in diabetic rats has been shown to improve the partial pressure of oxygen in the renal cortex.68 By inhibiting sodium transport, SGLT2 inhibitors in these rats reduced the workload of the renal PTs and improved tubulointerstitial hypoxia by decreasing the excess renal oxygen requirement,68 effects that can be potentially extrapolated to humans.
Clinical Trials of SGLT2 Inhibitors in Patients with CKD and DKD
Large, randomized, double-blind, placebo-controlled, cardiovascular-outcome trials in patients with T2D, such as EMPA-REG OUTCOME,69,70 CANVAS,71,72 and DECLARE-TIMI 58,73 initially provided evidence for the renal benefits of various SGLT2 inhibitors (Table 1). In EMPA-REG OUTCOME, empagliflozin slowed the progression of kidney disease, lowered the risk of serum creatinine doubling, and RRT compared with placebo.69 CANVAS demonstrated a lack of effect modification by baseline eGFR.72 In DECLARE-TIMI 58, dapagliflozin lowered the rate of progression of renal disease in patients who had or were at risk for atherosclerotic CVD.73 In a post hoc analysis of this trial, dapagliflozin reduced the risk of hospitalization for heart failure and renal-specific composite outcomes in patients with multiple risk factors for atherosclerotic CVD, suggesting beneficial effects in a broad primary-prevention population.74 Although these trials showed renal benefits, few patients were at high risk of kidney failure and the studies did not have renal endpoints as the primary outcome.
The DAPA-HF trial, in patients with heart failure with reduced ejection fraction with and without T2D, found that dapagliflozin treatment slowed the rate of eGFR decline, regardless of T2D status or baseline eGFR level.75 EMPEROR-Reduced, which used a different composite renal outcome and had more renal events than DAPA-HF, also showed a slower rate of eGFR decline, as well as a lower risk of serious renal outcomes, in empagliflozin-treated versus placebo-treated patients.76 Randomized-controlled-trial evidence for renal benefits with SGLT2-inhibitor treatment was substantiated by the global CVD-REAL 3 observational trial, involving more than 65,000 patients with T2D; compared with other glucose-lowering drugs, treatment with SGLT2 inhibitors was associated with a slower rate of kidney function decline and lower risk of major kidney events.77
CREDENCE, the first clinical trial of an SGLT2 inhibitor with a primary renal endpoint, included only patients with T2D and albuminuric CKD on an ACE inhibitor or ARB treatment background and demonstrated a lower risk of kidney failure versus placebo after a median follow-up of 2.62 years (the trial was stopped early because of indications of substantial efficacy).12
Given SGLT2 inhibitors’ mechanisms of action involving salutary effects on glomerular haemodynamics and not just metabolic parameters, their beneficial renal effects were predicted to extend to patients with CKD that is non-DKD.78 This hypothesis was substantiated by the DAPA-CKD trial, which was stopped early because of indications of substantial efficacy after a median follow-up of 2.4 years. DAPA-CKD is the only large, completed clinical trial to date that enrolled patients with CKD with and without T2D (N=4304, including 115 patients from the Philippines). Patients receiving dapagliflozin had a decreased risk of worsening kidney function (defined as ≥50% sustained decline in eGFR), ESRD, or death from renal or cardiovascular causes versus placebo.13 A greater reduction in eGFR was observed during the first 2 weeks of treatment with dapagliflozin than with placebo. This was followed by a smaller annual change in the mean eGFR. Importantly, renal protection was demonstrated in patients with baseline eGFR as low as 25 mL/min per 1.73 m2.13 Given the broad range of countries represented, the results of DAPA-CKD demonstrated that dapagliflozin produces similar beneficial effects on renal outcomes regardless of patients’ race and geographic region.79
Overall, several meta-analyses have substantiated the benefits of SGLT2 inhibitors on various renal outcomes. A meta-analysis of six trials (EMPA-REG OUTCOME, the two trials of the CANVAS Program, DECLARE-TIMI 58, CREDENCE, and VERTIS CV) suggests favourable effects of SGLT2 inhibitors on kidney disease progression with moderate heterogeneity across trials.36 Another meta-analysis of data from EMPA-REG OUTCOME, the CANVAS Program, DECLARE-TIMI 58, and CREDENCE further substantiated the reduced risk of dialysis, transplantation, and death due to kidney disease, as well as protection against acute kidney injury (AKI).47 In a recent network meta-analysis of 764 trials (CKD and/or albuminuria: 37 trials; high risk of cardiovascular or kidney disease: 10 trials) undertaken in patients with T2D, SGLT2 inhibitors reduced kidney failure (which was generally defined as eGFR <15 mL/min per 1.73 m2 or start of RRT).80 A meta-analysis of 12 large trials (T2D: 9 trials including EMPA-REG OUTCOME, CANVAS Program, DAPA-HF, and CREDENCE; without T2D: 3 trials) suggested that the beneficial effects of SGLT2 inhibitors on clinical kidney outcomes were not restricted to patients with T2D.81 However, whether the beneficial nephroprotective effects extend to all SGLT2 inhibitors remains to be established. Evidence suggests heterogeneity among different SGLT2 inhibitors; for example, the VERTIS CV trial82 of ertugliflozin and the SCORED trial83 of sotagliflozin did not find significant differences between SGLT2-inhibitor treatment and placebo on the composite renal outcome. However, multiple factors could have caused these negative results. Heterogeneity among outcomes across the different SGLT2 inhibitors could be attributed to different populations included in the trials, different baseline renal risk, and/or differences in outcome definitions (Table 1).
The varying levels of eGFR and albuminuria in the completed SGLT2-inhibitor trials provide robust evidence supporting their renal benefits across a wide range of types and degrees of kidney dysfunction (Table 1). Although stopping trials early could lead to overestimation of treatment benefits,84 the confirmatory results across most trials suggest that the beneficial renal-protective effects of SGLT2 inhibition are genuine. EMPA-KIDNEY (NCT03594110)85 is being conducted in patients with CKD without T2D. Estimated to complete by the end of 2022, it has a composite primary endpoint of time to first occurrence of kidney disease progression or cardiovascular death. The results of EMPA-KIDNEY may support the results of DAPA-CKD and DECLARE-TIMI 58 and will add to the evidence base on the use of SGLT2 inhibitors in patients with CKD.
The Safety of SGLT2 Inhibitors and Practical Management of Patients with CKD
Current criteria for diagnosis of CKD in adults (irrespective of age) include persistent signs of renal damage (for at least 3 months), such as a eGFR <60 mL/min per 1.73 m2 or increased urine albumin-to-creatinine ratio.86 This approach has been critiqued, because it the threshold for diagnosis of CKD is less accurate particularly in older people.87,88 Older people with eGFR 45 to 59 mL/min/1.73 m2 are not necessarily at low risk of CKD complications.88 A large meta-analyses conducted (2,051,244 participants) to evaluate association between the age and eGFR and albuminuria indicated that the eGFR threshold above which the risk of mortality is increased is not consistent across all ages.89 Among younger individuals, mortality is increased at eGFR <75 mL/min per 1.73 m2, whereas in elderly people it is increased at levels <45 mL/min per 1.73 m2.89
Different clinical trials used different eGFR thresholds for inclusion of participants (Table 1). The lowest approved eGFR to start canagliflozin and empagliflozin treatment is ≥30 mL/min per 1.73 m2 and ≥45 mL/min per 1.73 m2, respectively.15,90 In DAPA-CKD, dapagliflozin was prescribed in 979 (45.5%) patients with eGFR 30 to <45 mL/min per 1.73 m2, and in 293 (13.6%) patients with eGFR <30 mL/min per 1.73 m2.13 In CREDENCE, 119 (5.4%) patients with eGFR between 30 and <45 mL/min per 1.73 m2 received canagliflozin.12 We therefore recommend further evaluation of the appropriate eGFR threshold for which SGLT2 inhibitors can be used.
A common phenomenon from the clinical trials that should not be mistaken for an adverse event (and that does not signify an increased risk of an adverse event) is the slight reduction in eGFR (the “eGFR dip”) that occurs within the first few weeks of initiation of SGLT2-inhibitor treatment.44 The eGFR dip, typically between 4 and –6 mL/min per 1.73 m2,48 is transient and reversible within a few weeks of treatment discontinuation,50 even after ~3 years of treatment.69 Rather than an indication of lack of efficacy, the eGFR dip is generally thought to signify that the medication is working; it reflects acute haemodynamic effects, marked by initial reduction in hyperfiltration, and, in the long term, preservation of kidney structure and improved renal clinical outcomes.44 The eGFR dip has been seen across many large clinical trials, indicating a class-wide effect and one independent of the presence of T2D or severity of baseline kidney dysfunction.44 A post hoc analysis of the EMPA-REG OUTCOME trial found that patients with T2D and more advanced kidney disease and/or diuretic therapy at baseline had a greater chance of having an initial eGFR dip >10%, which occurred in 28.3% of the patients on empagliflozin and 13.4% of the patients on placebo.91 Additionally, a post hoc analysis of the CREDENCE trial reported that significantly more patients with T2D and CKD experienced an eGFR dip >10% in the canagliflozin (45%) than in the placebo group (21%).92 However, large, prolonged fluctuations in serum creatinine warrant evaluation for AKI.93 SGLT2 inhibitors induce a natriuretic response, which may restore TGF and reduce intraglomerular pressure.30
SGLT2 inhibitors have been shown to be generally safe, although they confer a higher risk of mycotic genital infections and diabetic ketoacidosis (DKA) compared with placebo.36 The risk of mycotic genital infections can be reduced with appropriate hygiene.94 A meta-analysis did not find an increased risk of AKI, DKA, urinary tract infection, or fracture compared with active comparators or placebo.95 Indeed, in a network meta-analysis, SGLT2 inhibitors were associated with a lower risk of AKI compared with placebo and active comparators.96 Although reports of AKI were initially a concern with SGLT2-inhibitor treatment, current evidence supports a renal-protective effect.47,97,98 In the DAPA-CKD trial, there were no cases of definite or probable DKA in the dapagliflozin group versus 2 cases in the placebo group.13 Severe hypoglycaemia—characterized by severe impairment in consciousness or behaviour and the need for external assistance and intervention to treat hypoglycaemia—was observed in half the number of patients in the dapagliflozin group compared with those in the placebo group (14 vs 28), but was not observed in patients with non-diabetic CKD.13 At low plasma glucose levels, the efficacy of SGLT2 inhibitors to increase urinary glucose excretion is attenuated, resulting in a low risk of hypoglycaemia.30 However, a multicentre cohort study undertaken in the United Kingdom and Canada in patients with T2D compared dipeptidyl peptidase-4 inhibitors with SGLT2 inhibitors and found the latter to be associated with almost a threefold greater risk of DKA.99 DKA is a medical emergency and when associated with SGLT2-inhibitor treatment can present with euglycaemia, which could delay diagnosis.100 The occurrence of euglycaemia depends on the balance between endogenous glucose production and renal glucose clearance. DKA symptoms include nausea, vomiting, abdominal pain, thirst, polyuria, fever, and confusion.100 To prevent SGLT2 inhibitor–mediated DKA, SGLT2-inhibitor treatment should be stopped during excessive alcohol intake, dehydration, acute illness, ~3 days before surgery, or in situations associated with volume depletion such as diarrhoea and vomiting, and insulin omission or inappropriate dose reduction should be avoided.100 The Asian Pacific Society of Nephrology Clinical Practice Guideline on Diabetic Kidney Disease recommends that screening for blood ketone levels be performed in individuals taking SGLT2 inhibitors during starvation, excessive alcohol intake, acute illness, or inappropriate insulin dose reduction.43 Patient education to recognize the symptoms and signs of DKA, volume depletion, orthostatic hypotension, and genital mycotic infection is recommended,101,102 and patients should be encouraged to maintain sufficient hydration and carbohydrate intake.103
Conclusions
With the rising burden of CKD and related complications in the Philippines, management strategies with newer treatment options are warranted. Globally, SGLT2 inhibitors have shown renoprotective benefits in patients with CKD, with and without T2D. Large clinical outcome trials support the beneficial renal effects of SGLT2 inhibitor treatment across a range of eGFR levels and albuminuria with tolerable safety. Several international guidelines also recommend initiating SGLT2 inhibitors in patients with stage 3 or higher CKD, irrespective of T2D status. Considering the efficacy and safety profile, SGLT2 inhibitors should be routinely prescribed in this patient population in Philippines to reduce progression of CKD. There is also an urgent need to incorporate SGLT2 inhibitors in local guidelines in Philippines to enable appropriate patient selection for use of SGLT2 inhibitors in routine clinical practice in the Philippines.
Data Sharing Statement
The data sets used and/or analysed during the current study are available from the corresponding author on reasonable formal request.
Acknowledgments
The authors would like to thank Steven Tresker for medical writing support and Suchita Nath-Sain, PhD, for editorial assistance, both from Cactus Life Sciences (part of Cactus Communications) in accordance with GPP 2022 guidelines. Editorial and post-submission support was provided by Prajakta Nachane from Labcorp Scientific Services and Solutions Private Limited.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The preparation of this manuscript and funding of the journal’s article processing charges was supported by AstraZeneca Pharmaceuticals (Phils), Inc, Philippines.
Disclosure
Dr. Rey Isidto was the national lead investigator for the DAPA CKD clinical trial. He has received honoraria for speaking engagements from Astra Zeneca, Servier, Corbridge Group and Zydus Healthcare and LG Life Sciences. Romina A. Danguilan reports honoraria, advisory fees, and research grants from Astellas, AstraZeneca, Corbridge, Multi-Product Line, Novartis, and Philippine Council for Health, Research and Development. Oscar Naidas reports honoraria and lecture fees from AstraZeneca and Boehringer Ingelheim. Russell Villanueva reports honorarium for module development and/or speaking engagements from Astellas, Astra Zeneca, Boerhinger Ingelheim, Globo Asiatico, Merck, Nestle Health Science, Novartis Sanofi Aventis and Servier. Layla Paraiso received honorarium from Fibrogen and GlaxoSmithKlein. The authors report no other conflicts of interest in this work.
References
1. Bikbov B, Purcell CA, Levey AS, et al. Global, regional, and national burden of chronic kidney disease, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2020;395(10225):709–733. doi:10.1016/S0140-6736(20)30045-3
2. Levin A, Tonelli M, Bonventre J, et al. Global kidney health 2017 and beyond: a roadmap for closing gaps in care, research, and policy. Lancet Lond Engl. 2017;390(10105):1888–1917. doi:10.1016/S0140-6736(17)30788-2
3. Rhee JJ, Jardine MJ, Chertow GM, Mahaffey KW. Dedicated kidney disease-focused outcome trials with sodium-glucose cotransporter-2 inhibitors: lessons from CREDENCE and expectations from DAPA-HF, DAPA-CKD, and EMPA-KIDNEY. Diabetes Obes Metab. 2020;22:46–54. doi:10.1111/dom.13987
4. Zhang Y, He D, Zhang W, Xing Y, Guo Y, Wang F. ACE inhibitor benefit to kidney and cardiovascular outcomes for patients with non-dialysis chronic kidney disease stages 3–5: a network meta-analysis of randomised clinical trials. Drugs. 2020;80:797–811. doi:10.1007/s40265-020-01290-3
5. Fried LF, Emanuele N, Zhang JH, Brophy M, Conner TA, Duckworth W. Combined angiotensin inhibition for the treatment of diabetic nephropathy. N Engl J Med. 2013;369:1892–1903. doi:10.1056/NEJMoa1303154
6. Stengel B, Muenz D, Tu C, Speyer E, Pinho N, Combe C. Adherence to the kidney disease: improving global outcomes CKD Guideline in nephrology practice across countries. Kidney Int Rep. 2021;6:437–448. doi:10.1016/j.ekir.2020.11.039
7. Cheng HT, Xu X, Lim PS, Hung KY. Worldwide epidemiology of diabetes-related end-stage renal disease, 2000–2015. Diabetes Care. 2021;44:89–97. doi:10.2337/dc20-1913
8. Diabetic nephropathy: challenges in pathogenesis, diagnosis, and treatment. Available from: https://www.hindawi.com/journals/bmri/2021/1497449/.
9. Cardiovascular Diabetology Full Text. Renoprotection with SGLT2 inhibitors in type 2 diabetes over a spectrum of cardiovascular and renal risk. Available from: https://cardiab.biomedcentral.com/articles/10.1186/s12933-020-01163-9.
10. SGLT2 inhibitors in chronic kidney disease: from mechanisms to clinical practice. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9598622/.
11. Mosenzon O, Wiviott SD, Cahn A, et al. Effects of dapagliflozin on development and progression of kidney disease in patients with type 2 diabetes: an analysis from the DECLARE-TIMI 58 randomised trial. Lancet Diabetes Endocrinol. 2019;7(8):606–617. doi:10.1016/S2213-8587(19)30180-9
12. Perkovic V, Jardine MJ, Neal B, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med. 2019;380(24):2295–2306. doi:10.1056/NEJMoa1811744
13. Heerspink HJL, Stefánsson BV, Correa-Rotter R, et al. Dapagliflozin in patients with chronic kidney disease. N Engl J Med. 2020;383(15):1436–1446. doi:10.1056/NEJMoa2024816
14. FARXIGA® (dapagliflozin). Prescribing Information. AstraZeneca Pharm LP; 2020. Available from: https://medicalinformation.astrazeneca-us.com/home/prescribing-information/farxiga-pi.html.
15. INVOKANA® (canagliflozin). Prescribing Information. Janssen; 2019. https://www.janssenlabels.com/package-insert/product-monograph/prescribing-information/INVOKANA-pi.pdf.
16. Liyanage T, Toyama T, Hockham C, et al. Prevalence of chronic kidney disease in Asia: a systematic review and analysis. BMJ Glob Health. 2022;7(1):e007525. doi:10.1136/bmjgh-2021-007525
17. Suriyong P, Ruengorn C, Shayakul C, Anantachoti P, Kanjanarat P. Prevalence of chronic kidney disease stages 3–5 in low- and middle-income countries in Asia: a systematic review and meta-analysis. PLoS One. 2022;17(2):e0264393. doi:10.1371/journal.pone.0264393
18. Wu AYT, Kong NCT, Leon FA, Pan CY, Tai TY, Yeung VTF. An alarmingly high prevalence of diabetic nephropathy in Asian type 2 diabetic patients: the MicroAlbuminuria Prevalence (MAP) Study. Diabetologia. 2005;48(1):17–26. doi:10.1007/s00125-004-1599-9
19. Chandie Shaw PK, Baboe F, van Es LA, et al. South-Asian type 2 diabetic patients have higher incidence and faster progression of renal disease compared with Dutch-European diabetic patients. Diabetes Care. 2006;29(6):1383–1385. doi:10.2337/dc06-0003
20. Fojas MC, Lantion-Ang FL, Jimeno CA, Santiago D, Arroyo M, Laurel A. Complications and cardiovascular risk factors among newly-diagnosed type 2 diabetics in Manila. Philipp J Intern Med. 2009;47:99–105.
21. Journal of the ASEAN Federation of Endocrine Societies. Prevalence of microvascular complications among newly_diagnosed type 2 diabetes mellitus patients in Ospital Ng Makati outpatient department. Available from: https://asean-endocrinejournal.org/index.php/JAFES/article/view/1957.
22. Institute for Health Metrics and Evaluation (IHME) data on the Philippines; 2020. Available from: http://www.healthdata.org/philippines.
23. Liyanage T, Ninomiya T, Jha V, et al. Worldwide access to treatment for end-stage kidney disease: a systematic review. Lancet. 2015;385(9981):1975–1982. doi:10.1016/S0140-6736(14)61601-9
24. Kidney Disease in Philippines. World Life Expectancy. Available from: https://www.worldlifeexpectancy.com/philippines-kidney-disease.
25. Philippine Renal Disease Registry: PRDR Annual Report. Renal Disease Control Program (REDCOP), National Kidney and Transplant Institute (NKTI) and Epidemiology Bureau of the Department of Health (DOH); 2020.
26. Sahay M, Jasuja S, Tang SCW, Alexander S, Jha V, Vachharajani T. Aetiology, practice patterns and burden of end-stage kidney disease in South Asia and South-East Asia: a questionnaire-based survey. Nephrol Carlton. 2021;26:142–152. doi:10.1111/nep.13825
27. Stats and Charts 2019. PhilHealth. Available from: https://www.philhealth.gov.ph/about_us/statsncharts/snc2019_r1.pdf.
28. Danguilan R, Cabanayan-Casasola CB, Evangelista NN, Pelobello MLF, Equipado CD, Lucio-Tong ML. An education and counseling program for chronic kidney disease: strategies to improve patient knowledge. Kidney Int Suppl. 2013;3:215–218. doi:10.1038/kisup.2013.17
29. Gerich JE. Role of the kidney in normal glucose homeostasis and in the hyperglycaemia of diabetes mellitus: therapeutic implications. Diabet Med. 2010;27(2):136–142. doi:10.1111/j.1464-5491.2009.02894.x
30. Heerspink HJL, Perkins BA, Fitchett DH, Husain M, Cherney DZI. Sodium glucose cotransporter 2 inhibitors in the treatment of diabetes mellitus. Circulation. 2016;134(10):752–772. doi:10.1161/CIRCULATIONAHA.116.021887
31. Hediger MA, Rhoads DB. Molecular physiology of sodium-glucose cotransporters. Physiol Rev. 1994;74:993–1026. doi:10.1152/physrev.1994.74.4.993
32. Liu JF, Matulonis UA. Bevacizumab in newly diagnosed ovarian cancer. Lancet Oncol. 2015;16(8):876–878. doi:10.1016/S1470-2045(15)00064-9
33. Vrhovac I, Balen Eror D, Klessen D, Burger C, Breljak D, Kraus O. Localizations of Na(+)-D-glucose cotransporters SGLT1 and SGLT2 in human kidney and of SGLT1 in human small intestine, liver, lung, and heart. Pflugers Arch. 2015;467:1881–1898. doi:10.1007/s00424-014-1619-7
34. Nair S, Wilding JP. Sodium glucose cotransporter 2 inhibitors as a new treatment for diabetes mellitus. J Clin Endocrinol Metab. 2010;95:34–42. doi:10.1210/jc.2009-0473
35. Fioretto P, Zambon A, Rossato M, Busetto L, Vettor R. SGLT2 inhibitors and the diabetic kidney. Diabetes Care. 2016;39(Suppl 2):S165–S171. doi:10.2337/dcS15-3006
36. McGuire DK, Shih WJ, Cosentino F, Charbonnel B, Cherney DZI, Dagogo-Jack S. Association of SGLT2 inhibitors with cardiovascular and kidney outcomes in patients with type 2 diabetes: a meta-analysis. JAMA Cardiol. 2021;6:148–158. doi:10.1001/jamacardio.2020.4511
37. American Diabetes Association. 11. Microvascular complications and foot care: standards of Medical Care in Diabetes-2020. Diabetes Care. 2020;43(Suppl 1):S135–S151. doi:10.2337/dc20-S011
38. Das ESR. Expert consensus decision pathway on novel therapies for cardiovascular risk reduction in patients with type 2 diabetes: a report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2020;76:1117–1145. doi:10.1016/j.jacc.2020.05.037
39. Cosentino F, Grant PJ, Aboyans V, Bailey CJ, Ceriello A, Delgado V. ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J. 2019;41:255–323.
40. de Boer IH, for the DCCT/EDIC Research Group. Kidney disease and related findings in the diabetes control and complications trial/epidemiology of diabetes interventions and complications study. Diabetes Care. 2013;37(1):24–30. doi:10.2337/dc13-2113
41. Farrington K, Covic A, Aucella F, Clyne N, Vos L, Findlay A. Clinical Practice Guideline on management of older patients with chronic kidney disease stage 3b or higher. Nephrol Dial Transplant. 2016;31:66. doi:10.1093/ndt/gfw356
42. Tsukamoto Y. Implication of global nephrology guidelines in Asia and “Asian CKD Best Practice Guidelines.”. Nephrol Carlton. 2010;2:43–44. doi:10.1111/j.1440-1797.2010.01310.x
43. Liew A, Bavanandan S, Prasad N, et al. Asian pacific society of nephrology clinical practice guideline on diabetic kidney disease. Nephrology. 2020;25(S2):12–45. doi:10.1111/nep.13785
44. De Nicola L, Gabbai FB, Garofalo C, Conte G, Minutolo R. Nephroprotection by SGLT2 inhibition: back to the future? J Clin Med. 2020;9(2243). doi:10.3390/jcm9072243
45. Dekkers CCJ, Gansevoort RT. Sodium-glucose cotransporter 2 inhibitors: extending the indication to non-diabetic kidney disease? Nephrol Dial Transpl. 2020;35(Suppl 1):i33–i42. doi:10.1093/ndt/gfz264
46. Heerspink HJ, Desai M, Jardine M, Balis D, Meininger G, Perkovic V. Canagliflozin slows progression of renal function decline independently of glycemic effects. J Am Soc Nephrol. 2017;28:368–375. doi:10.1681/ASN.2016030278
47. Neuen BL, Young T, Heerspink HJL, Neal B, Perkovic V, Billot L. SGLT2 inhibitors for the prevention of kidney failure in patients with type 2 diabetes: a systematic review and meta-analysis. Lancet Diabetes Endocrinol. 2019;7:845–854. doi:10.1016/S2213-8587(19)30256-6
48. Heerspink HJL, Kosiborod M, Inzucchi SE, Cherney DZI. Renoprotective effects of sodium-glucose cotransporter-2 inhibitors. Kidney Int. 2018;94:26–39. doi:10.1016/j.kint.2017.12.027
49. Leoncini G, Russo E, Bussalino E, Barnini C, Viazzi F, Pontremoli R. SGLT2is and renal protection: from biological mechanisms to real-world clinical benefits. Int J Mol Sci. 2021;22(9):4441. doi:10.3390/ijms22094441
50. Cherney DZI, Dekkers CCJ, Barbour SJ, Cattran D, Abdul Gafor AH, Greasley PJ. Effects of the SGLT2 inhibitor dapagliflozin on proteinuria in non-diabetic patients with chronic kidney disease (DIAMOND): a randomised, double-blind, crossover trial. Lancet Diabetes Endocrinol. 2020;8:582–593. doi:10.1016/S2213-8587(20)30162-5
51. Anders HJ, Huber TB, Isermann B, Schiffer M. CKD in diabetes: diabetic kidney disease versus nondiabetic kidney disease. Nat Rev Nephrol. 2018;14:361–377. doi:10.1038/s41581-018-0001-y
52. Hesp AC, Schaub JA, Prasad PV, Vallon V, Laverman GD, Bjornstad P. The role of renal hypoxia in the pathogenesis of diabetic kidney disease: a promising target for newer renoprotective agents including SGLT2 inhibitors? Kidney Int. 2020;98:579–589. doi:10.1016/j.kint.2020.02.041
53. Oyarzún C, Garrido W, Alarcón S, Yáñez A, Sobrevia L, Quezada C. Adenosine contribution to normal renal physiology and chronic kidney disease. Mol Asp Med. 2017;55:75–89. doi:10.1016/j.mam.2017.01.004
54. Cherney DZI, Perkins BA, Soleymanlou N, Maione M, Lai V, Lee A. Renal hemodynamic effect of sodium-glucose cotransporter 2 inhibition in patients with type 1 diabetes mellitus. Circulation. 2014;129:587–597. doi:10.1161/CIRCULATIONAHA.113.005081
55. Rajasekeran H, Lytvyn Y, Bozovic A, Lovshin JA, Diamandis E, Cattran D. Urinary adenosine excretion in type 1 diabetes. Am J Physiol Ren Physiol. 2017;313:F184–F191. doi:10.1152/ajprenal.00043.2017
56. Lambers HJ, de Zeeuw D, Wie L, Leslie B, List J. Dapagliflozin a glucose-regulating drug with diuretic properties in subjects with type 2 diabetes. Diabetes Obes Metab. 2013;15:853–862. doi:10.1111/dom.12127
57. Heerspink HJL, Johnsson E, Gause-Nilsson I, Cain VA, Sjöström CD. Dapagliflozin reduces albuminuria in patients with diabetes and hypertension receiving renin-angiotensin blockers. Diabetes Obes Metab. 2016;18:590–597. doi:10.1111/dom.12654
58. Kusche-Vihrog K, Schmitz B, Brand E. Salt controls endothelial and vascular phenotype. Pflugers Arch. 2015;467:499–512. doi:10.1007/s00424-014-1657-1
59. Oberleithner H. Vascular endothelium: a vulnerable transit zone for merciless sodium. Nephrol Dial Transpl. 2014;29:240–246. doi:10.1093/ndt/gft461
60. Shigiyama F, Kumashiro N, Miyagi M, Ikehara K, Kanda E, Uchino H. Effectiveness of dapagliflozin on vascular endothelial function and glycemic control in patients with early-stage type 2 diabetes mellitus: DEFENCE study. Cardiovasc Diabetol. 2017;16:84. doi:10.1186/s12933-017-0564-0
61. Solini A, Giannini L, Seghieri M, Vitolo E, Taddei S, Ghiadoni L. Dapagliflozin acutely improves endothelial dysfunction, reduces aortic stiffness and renal resistive index in type 2 diabetic patients: a pilot study. Cardiovasc Diabetol. 2017;16:138. doi:10.1186/s12933-017-0621-8
62. Sano M, Takei M, Shiraishi Y, Suzuki Y. Increased hematocrit during sodium-glucose cotransporter 2 inhibitor therapy indicates recovery of tubulointerstitial function in diabetic kidneys. J Clin Med Res. 2016;8:844–847. doi:10.14740/jocmr2760w
63. Chino Y, Samukawa Y, Sakai S, Nakai Y, Yamaguchi J, Nakanishi T. SGLT2 inhibitor lowers serum uric acid through alteration of uric acid transport activity in renal tubule by increased glycosuria. Biopharm Drug Dispos. 2014;35:391–404. doi:10.1002/bdd.1909
64. Odden MC, Amadu AR, Smit E, Lo L, Peralta CA. Uric acid levels, kidney function, and cardiovascular mortality in US adults. In: National Health and Nutrition Examination Survey (NHANES) 1988–1994 and 1999–2002. American journal of kidney diseases; 2016.
65. Ponticelli C, Podestà MA, Moroni G. Hyperuricemia as a trigger of immune response in hypertension and chronic kidney disease. Kidney Int. 2020;98:1149–1159. doi:10.1016/j.kint.2020.05.056
66. Zhao Y, Xu L, Tian D, Xia P, Zheng H, Wang L. Effects of sodium-glucose co-transporter 2 (SGLT2) inhibitors on serum uric acid level: a meta-analysis of randomized controlled trials. Diabetes Obes Metab. 2018;20:458–462. doi:10.1111/dom.13101
67. Lassen NA, Munck O, Thaysen JH. Oxygen consumption and sodium reabsorption in the kidney. Acta Physiol Scand. 1961;51:371–384. doi:10.1111/j.1748-1716.1961.tb02147.x
68. O’Neill J, Fasching A, Pihl L, Patinha D, Franzén S, Palm F. Acute SGLT inhibition normalizes O2 tension in the renal cortex but causes hypoxia in the renal medulla in anaesthetized control and diabetic rats. Am J Physiol Ren Physiol. 2015;309:F227–F234. doi:10.1152/ajprenal.00689.2014
69. Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and progression of kidney disease in type 2 diabetes. N Engl J Med. 2016;375(4):323–334. doi:10.1056/NEJMoa1515920
70. Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373:2117–2128. doi:10.1056/NEJMoa1504720
71. Neal B, Perkovic V, Mahaffey KW, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med. 2017;377(7):644–657. doi:10.1056/NEJMoa1611925
72. Neuen BL, Ohkuma T, Neal B, Matthews DR, Zeeuw D, Mahaffey KW. Cardiovascular and renal outcomes with canagliflozin according to baseline kidney function. Circulation. 2018;138:1537–1550. doi:10.1161/CIRCULATIONAHA.118.035901
73. Wiviott SD, Raz I, Bonaca MP, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2019;380(4):347–357. doi:10.1056/NEJMoa1812389
74. Cahn A, Raz I, Leiter LA, et al. Cardiovascular, renal, and metabolic outcomes of dapagliflozin versus placebo in a primary cardiovascular prevention cohort: analyses from DECLARE-TIMI 58. Diabetes Care. 2021;44(5):1159–1167. doi:10.2337/dc20-2492
75. Jhund PS, Solomon SD, Docherty KF, Heerspink HJL, Anand IS, Böhm M. Efficacy of dapagliflozin on renal function and outcomes in patients with heart failure with reduced ejection fraction: results of DAPA-HF. Circulation. 2021;143:298–309. doi:10.1161/CIRCULATIONAHA.120.050391
76. Packer M, Anker SD, Butler J, et al. Cardiovascular and renal outcomes with empagliflozin in heart failure. N Engl J Med. 2020;383(15):1413–1424. doi:10.1056/NEJMoa2022190
77. Heerspink HJL, Karasik A, Thuresson M, et al. Kidney outcomes associated with use of SGLT2 inhibitors in real-world clinical practice (CVD-REAL 3): a multinational observational cohort study. Lancet Diabetes Endocrinol. 2020;8(1):27–35. doi:10.1016/S2213-8587(19)30384-5
78. Wheeler DC, Stefansson BV, Batiushin M, et al. The dapagliflozin and prevention of adverse outcomes in chronic kidney disease (DAPA-CKD) trial: baseline characteristics. Nephrol Dial Transplant. 2020;35(10):1700–1711. doi:10.1093/ndt/gfaa234
79. Vart P, Correa-Rotter R, Hou FF, Jongs N, Chertow GM, Langkilde AM. Efficacy and safety of dapagliflozin in patients with chronic kidney disease across major geographic regions. Kidney Int Rep. 2022;7(4):699–707. doi:10.1016/j.ekir.2022.01.1060
80. Palmer SC, Tendal B, Mustafa RA, Vandvik PO, Li S, Hao Q. Sodium-glucose cotransporter protein-2 (SGLT-2) inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists for type 2 diabetes: systematic review and network meta-analysis of randomised controlled trials. BMJ. 2021;372:m4573. doi:10.1136/bmj.m4573
81. Kang A, Jardine MJ. SGLT2 inhibitors may offer benefit beyond diabetes. Nat Rev Nephrol. 2021;17:83–84. doi:10.1038/s41581-020-00391-2
82. Cannon CP, Pratley R, Dagogo-Jack S, et al. Cardiovascular outcomes with ertugliflozin in type 2 diabetes. N Engl J Med. 2020;383(15):1425–1435. doi:10.1056/NEJMoa2004967
83. Bhatt DL, Szarek M, Pitt B, et al. Sotagliflozin in patients with diabetes and chronic kidney disease. N Engl J Med. 2021;384(2):129–139. doi:10.1056/NEJMoa2030186
84. Guyatt GH, Briel M, Glasziou P, Bassler D, Montori VM. Problems of stopping trials early. BMJ. 2012;344:e3863. doi:10.1136/bmj.e3863
85. ClinicalTrialsgov. EMPA-KIDNEY (the study of heart and kidney protection with empagliflozin; 2020. Available from: https://clinicaltrials.gov/ct2/show/NCT03594110.
86. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. National Kidney foundation. Available from: https://kdigo.org/wp-content/uploads/2017/02/KDIGO_2012_CKD_GL.pdf.
87. Delanaye P, Jager KJ, Bökenkamp A, et al. CKD: a call for an age-adapted definition. J Am Soc Nephrol JASN. 2019;30(10):1785–1805. doi:10.1681/ASN.2019030238
88. Lees JS, Shlipak MG. Age-adapted eGFR thresholds underestimate the risks beyond kidney failure associated with CKD in older populations. J Am Geriatr Soc. 2022;70(12):3660–3664. doi:10.1111/jgs.18046
89. Hallan SI, Matsushita K, Sang Y, et al. Age and association of kidney measures with mortality and end-stage renal disease. JAMA. 2012;308(22):2349–2360. doi:10.1001/jama.2012.16817
90. JARDIANCE® (empagliflozin). Prescribing Information. Boehringer Ingelheim Pharma GmbH & Co. KG; 2019. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/204629s008lbl.pdf.
91. Kraus BJ, Weir M, Bakris G, Mattheus M, Cherney D, Sattar N. Kidney implications of the initial eGFR response to SGLT2 inhibition with empagliflozin: the ‘eGFR dip’ in EMPA-REG OUTCOME. Nephrol Dial Transpl. 2020;35(Suppl 3):LB005. doi:10.1093/ndt/gfaa146.LB005
92. Oshima M, Jardine MJ, Agarwal R, Bakris G, Cannon CP, Charytan DM. Insights from CREDENCE trial indicate an acute drop in estimated glomerular filtration rate during treatment with canagliflozin with implications for clinical practice. Kidney Int. 2021;99:999–1009. doi:10.1016/j.kint.2020.10.042
93. Kellum JA, Lameire N; Group KDIGOAKIGW. Diagnosis, evaluation, and management of acute kidney injury: a KDIGO summary (Part 1. Crit Care. 2013;17(204). doi:10.1186/cc11454
94. Williams SM, Ahmed SH. Improving compliance with SGLT2 inhibitors by reducing the risk of genital mycotic infections: the outcomes of personal hygiene advice. Diabetes. 2019;68(Suppl 1):1224. doi:10.2337/db19-1224-P
95. Donnan GJR, Grandy CA, Chibrikov E. Comparative safety of the sodium glucose co-transporter 2 (SGLT2) inhibitors: a systematic review and meta-analysis. BMJ Open. 2019;9:e022577. doi:10.1136/bmjopen-2018-022577
96. Zhao M, Sun S, Huang Z, Wang T, Tang H. Network meta-analysis of novel glucose-lowering drugs on risk of acute kidney injury. Clin J Am Soc Nephrol. 2020;16:70–78. doi:10.2215/CJN.11220720
97. Iskander C, Cherney DZ, Clemens KK, Dixon SN, Harel Z, Jeyakumar N. Use of sodium-glucose cotransporter-2 inhibitors and risk of acute kidney injury in older adults with diabetes: a population-based cohort study. CMAJ. 2020;192:E351–E360. doi:10.1503/cmaj.191283
98. Rampersad C, Kraut E, Whitlock RH, Komenda P, Woo V, Rigatto C. Acute kidney injury events in patients with type 2 diabetes using SGLT2 inhibitors versus other glucose-lowering drugs: a retrospective cohort study. Am J Kidney Dis. 2020;76:471–479. doi:10.1053/j.ajkd.2020.03.019
99. Douros A, Lix LM, Fralick M, Dell’Aniello S, Shah BR, Ronksley PE. Sodium-glucose cotransporter-2 inhibitors and the risk for diabetic ketoacidosis: a multicenter cohort study. Ann Intern Med. 2020;173:417–425. doi:10.7326/M20-0289
100. Goldenberg RM, Berard LD, Cheng AYY, Gilbert JD, Verma S, Woo VC. SGLT2 inhibitor-associated diabetic ketoacidosis: clinical review and recommendations for prevention and diagnosis. Clin Ther. 2016;38(2654–2664):2651. doi:10.1016/j.clinthera.2016.11.002
101. Tuttle KR, Brosius FC, Cavender MA, et al. SGLT2 inhibition for CKD and cardiovascular disease in type 2 diabetes: report of a scientific workshop sponsored by the national kidney foundation. Am J Kidney Dis. 2021;77(1):94–109. doi:10.1053/j.ajkd.2020.08.003
102. Lupsa BC, Inzucchi SE. Use of SGLT2 inhibitors in type 2 diabetes: weighing the risks and benefits. Diabetologia. 2018;61(10):2118–2125. doi:10.1007/s00125-018-4663-6
103. Qiu H, Novikov A, Vallon V. Ketosis and diabetic ketoacidosis in response to SGLT2 inhibitors: basic mechanisms and therapeutic perspectives. Diabetes Metab Res Rev. 2017;33(5):e2886. doi:10.1002/dmrr.2886
104. Cannon CP, McGuire DK, Pratley R, Dagogo-Jack S, Mancuso J, Huyck S. Design and baseline characteristics of the eValuation of ERTugliflozin effIcacy and Safety CardioVascular outcomes trial (VERTIS-CV. Am Heart J. 2018;206:11–23. doi:10.1016/j.ahj.2018.08.016
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.