")
Back to Journals » Medical Devices: Evidence and Research » Volume 16
Efficacy of Flowable Collagen Hemostat Evaluated in Preclinical Models of Liver Injury and Spinal Cord Exposure
Authors Lake SP, Bradbury K , Gagne DH, Deeken CR , Badhwar A , Bohnen A
Received 29 March 2023
Accepted for publication 29 May 2023
Published 5 June 2023 Volume 2023:16 Pages 123—132
DOI https://doi.org/10.2147/MDER.S411735
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Spencer P Lake,1 Kasia Bradbury,2 Darcy H Gagne,2 Corey R Deeken,3 Amit Badhwar,2 Angela Bohnen4
1Department of Mechanical Engineering & Materials Science, Washington University in St. Louis, St. Louis, MO, USA; 2Becton, Dickinson and Company, Warwick, RI, USA; 3Covalent Bio, LLC, St. Louis, MO, USA; 4Neurosurgery One, Littleton, CO, USA
Correspondence: Amit Badhwar, Becton, Dickinson and Company (BD), 100 Crossings Boulevard, Warwick, RI, 02886, USA, Tel +1 401 825-8514, Fax +1 401 825-8762, Email [email protected]
Introduction: Excessive bleeding in trauma and surgical settings leads to increased operative time, reoperation rates, and overall healthcare costs. A wide range of hemostatic agents have been developed to control bleeding that can vary considerably in type of hemostatic action, ease of application, cost, risk of infection, and dependence on patient coagulation. Microfibrillar collagen-based hemostatic materials (MCH) have yielded beneficial results in a variety of applications.
Methods: A new flowable collagen product, containing a modified MCH flour, but in a more convenient flowable delivery system, was evaluated for hemostatic efficacy in preclinical models of solid organ injury and spinal cord exposure. The primary objective of this study was to compare the hemostatic potential and local tissue responses to this novel, flowable collagen-based hemostatic agent to the original flour formulation to confirm that the new method of delivery did not interfere with the hemostatic properties of the MCH flour.
Results: When observed visually, the flowable MCH flour mixed with saline (FL) provided more precise application and uniform coverage to injured tissues compared to the dry MCH flour alone (F0). All of the treatments (FL, F0, and gauze) exhibited comparable Lewis bleed grade at all three time points evaluated in the capsular resection liver injury model (bleed grade: 1.0– 1.3; p> 0.05 in all cases). FL and F0 exhibited comparable 100% acute hemostatic efficacy and similar long-term histomorphological properties (up to 120 days) in a capsular resection liver injury in pigs, while gauze resulted in significantly lower rates of acute hemostatic efficacy (8– 42%, p< 0.05 in all cases). In an ovine model of dorsal laminectomy and durotomy, FL and F0 again exhibited comparable results without any neurological effects.
Conclusion: Flowable microfibrillar collagen was shown to yield favorable short- and long-term outcomes in two representative applications where hemostatic efficacy is critical to surgical success.
Keywords: hemostatic agent, bleeding, microfibrillar collagen, liver injury, spine surgery
Introduction
Bleeding is a common challenge in surgical settings and can lead to severe health complications. Nearly 30% of surgical patients suffer from bleeding-related complications.1 Surgical specialties with high rates of bleeding include cardiac (47%), solid organ (28.5%) and spine (15%) among others.1 Uncontrolled bleeding during surgery can impair wound healing, increase infection rates and risk of organ failure, and impact mortality rates.2,3 Such complications exert significant impact on the healthcare system by increasing medical cost, exemplified by increased surgical times, increased need for post-operative monitoring, advance specialist consultation, longer hospital stays, and increased intensive care needs.1,2
The ability to control bleeding quickly and thoroughly in trauma conditions or during surgical procedures is critical. Hemostasis is important for providing hemodynamic stability, maintaining visibility of the operative field, and reducing blood loss and associated blood transfusions.4,5 Blood transfusions are often performed to combat uncontrolled blood loss in the operating room, but are a limited and expensive resource, increase risk of infection, and are associated with increased morbidity and mortality.6,7 Thus, elimination of unneeded transfusions would provide significant benefit. Effective hemostatic agents that control bleeding could reduce the number of transfusions, decrease time in the operating room, reduce reoperation rates, improve recovery times, and reduce overall healthcare costs.6,8
The selection of hemostatic agents can be challenging due to the large range of products that are available (see below). The optimal product for each specific application will depend on the type of surgical procedure, severity and location of bleeding, coagulation status, extent of patient comorbidities (eg, hypertension, diabetes) and other procedure- or patient-specific considerations (eg, religious/cultural beliefs regarding human/animal derived products). As much as 40% of inadequate hemostasis could be due to inappropriate use of hemostatic agents.1 Thus, it is imperative to select the hemostatic agent that optimizes patient outcomes, rather than select products based on surgeon familiarity/preference, availability, ease of use or speed of application (although each of these factors can be beneficial in appropriate circumstances).
There are many different hemostatic products currently available for clinical use, which are often classified into four general categories: mechanical, biologically active, flowable agents, and sealants.2,9–11 Mechanical hemostats (eg, bone wax, gelatin sponges, oxidized regenerated cellulose), which are generally more affordable and easier to apply than other products, use physical means to limit bleeding and/or help activate the extrinsic coagulation cascade by serving as a scaffold for clot formation. These products are most successful in treating minimal bleeds in patients with intact coagulation systems and adequate space for access.9 Biologically active hemostats (eg, bovine, human or recombinant thrombin) reduce bleeding by activating clotting factors, aiding in conversion of fibrinogen into fibrin for clotting, and promoting platelet aggregation and adherence. These products are typically useful for local or diffuse bleeding and are beneficial for patients with impaired coagulative abilities, but are moderately priced and can have minor risk for disease transmission and/or inciting an immune response. Flowable hemostats seek to stop bleeding by combining two mechanisms: a hemostatic material (eg, gelatin) provides a mechanical tamponade effect and an active component (eg, thrombin) initiates the clotting response. These products are generally easy to deliver and can conform to variable wound sites, but do require reconstitution prior to use and are generally more expensive than other approaches. Sealants are absorbable dressings that seal tissue and close active sources of bleeding like blood vessels and lymphatics. These products can be composed of biologic (eg, lyophilized fibrinogen and thrombin) or synthetic materials (eg, cyanoacrylates), are designed to be fast acting, and useful for patients with limited coagulation/clotting.
Mechanical hemostatic materials based on microfibrillar collagen (eg, AviteneTM) have shown beneficial results in a variety of applications12 and offer additional benefits beyond those of a typical mechanical hemostat due to the inclusion of collagen. As the predominant structural protein of the extracellular matrix, collagen-based mechanical hemostats promote platelet aggregation and reinforce clotting in a way that is not possible with a purely mechanical hemostat.13 Other advantages include ease of storage and delivery and long shelf life. Microfibrillar collagen is available as a flour (ie, microsalt collagen powder), compressed sheets, or sponges,11 which enables product use in various anatomical settings and surgical applications. These biologically-based, absorbable microfibrillar collagen hemostatic materials can control bleeding when conventional procedures are ineffective. However, one limitation when attempting to deliver this product to variable or non-uniform wounds; sheets/sponges may not be appropriate for uneven sites, and flour products can be difficult to deliver in areas with limited access (ie minimally invasive surgery).
A new device (AviteneTM Flowable Collagen Hemostat; BD, Warwick, RI), combines the benefits of hemostasis provided by microfibrillar collagen in a more convenient, flowable delivery system that is intended to overcome the challenges associated with anatomical space limitations and offering a wider range of potential uses. Specifically, an MCH flour is mixed with saline and then delivered in controlled amounts via syringe to the bleeding site. The primary objective of this study was to compare the hemostatic potential and local tissue responses to this novel, flowable collagen-based hemostatic agent to the original flour formulation to confirm that the new method of delivery did not interfere with the hemostatic properties of the MCH flour. To this end, flowable collagen was evaluated in large animal models of representative injuries where hemostatic products can have a significant clinical impact, namely solid organ (ie, liver) bleeding and neurosurgery (ie, spine surgery and spinal cord exposure).
Methods
Materials
This study evaluated the hemostatic ability of AviteneTM Flowable Collagen Hemostat (BD, Warwick, RI), which is produced by combining a modified version of AviteneTM MCH flour (dry, sterile, 100% purified bovine corium collagen) with sterile saline (0.9% sodium chloride solution). AviteneTM products are absorbable hemostatic agents indicated for use in surgical procedures to control bleeding. To prepare the test product, 1 gram of MCH flour was modified through additional and modified milling processes to increase the solubility of the base flour and then mixed with 7 mL of saline in a polycarbonate syringe. The resulting flowable mixture was applied as AviteneTM Flowable Collagen Hemostat (designated as FL). As a control group comparison, 1 gram of AviteneTM Microfibrillar Collagen Hemostat Flour (ie, dry, 0 mL saline, designated F0) was provided in a cup and applied to the injury sites. In addition, for the long-term solid organ assessment, sterile woven gauze sponges (USP Type VII, Medline, Northfield, IL) were also considered and compared to the collagen-based products. All of the protocols for this project were reviewed and approved by the Institutional Animal Care and Use Committee of CBSET, Inc. (Lexington, MA) prior to the commencement of experiments (IACUC protocol # I00310), and all procedures complied with the National Institutes of Health (NIH) guidelines for animal welfare.
Treatment of Liver Injury
The objective of this procedure was to evaluate short- and long-term responses when using a flowable microfibrillar collagen product to stop bleeding in a porcine model of a solid organ (liver) injury. Following intra-operative capsular resection liver injury, animals were treated with one of three different devices and observed until sacrifice at 30, 90 or 120 days (n=12/group).
Female Yorkshire swine (Sus scrofa domesticus; n=36; 4–5 months of age; 39.0–59.4 kg) were fasted prior to surgery but allowed water ad libitum. Pre-operatively, buprenorphine (0.03 mg/kg, intramuscular), carprofen (2.2 mg/kg, oral or intramuscular) and tiletamine-zolazepam (4 mg/kg, intramuscular) were administered as analgesia, non-steroidal anti-inflammatory, and pre-anesthetic, respectively. Isoflurane anesthesia (delivered in 100% oxygen) was used for sedation. The animals were placed in dorsal recumbency, and body temperature was maintained while under anesthesia. After induction of anesthesia, access was made in a carotid artery via cut-down for direct arterial blood pressure monitoring. Mean arterial pressure (MAP) was maintained at levels similar to human (ie, 80–100 mmHg); when MAP adjustment was needed, phenylephrine HCl was administered via intravenous drip (0.06–0.6 μg/kg/min) or bolus (0.02–0.04 mg). A baseline activated clotting time (ACT) test and hematocrit were measured to ensure there were no obvious pre-existing clotting issues. ACT levels were measured approximately every 30±5 minutes, with final hematocrit and ACT collected prior to closure. To induce the liver injury, a ~30 cm ventral midline laparotomy incision was made to expose the abdominal cavity. Bleeding sites were prepared by creating 1 cm × 1 cm square capsular resection injuries in the liver. Each injury was allowed to bleed freely for 30 seconds to collect blood into pre-weighed gauze to determine the volume of blood lost from each injury site. The severity of bleeding was scored using the Lewis bleeding severity scale:14 0 = no bleeding, 1 = mild, 2 = moderate, 3 = severe, and 4 = life threatening. Only injuries that scored a 1 (mild) or 2 (moderate) on the Lewis scale were utilized for treatments. If an injury did not produce sufficient bleeding, an additional injury was created, or the site was further manipulated to create more bleeding. Each animal was treated with one type of hemostat device: 3 mL of a mixture of 1 g modified AviteneTM flour combined with 7 mL saline (FL), 0.33 g dry AviteneTM Flour (F0), or woven gauze sponge (“gauze”). Wound appropriate pressure was applied for 3 minutes followed by visual observation for up to 10 minutes to evaluate hemostatic efficacy by determining the percentage of wounds that had reached hemostasis. If hemostasis was not achieved after the first 3 minutes or if bleeding was observed during the observation period, additional 1-minute pressure cycles were applied. Clinical observations were performed daily for the first 14 post-operative days and then weekly thereafter. Following sacrifice at 30, 90 and 120 days (± 2 days) via intravenous overdose of potassium chloride solution, the original wounds were exposed, and several features were assessed including hemorrhage and extent of peritoneal tissue attachments (0 = no attachments, 1 = loose only, 2 = firm with minimal vascularity, 3 = firm with extensive vascularity, 4 = firm with extensive vascularity and fibrosis, 5 = firm attachments directly to visceral organs). In addition, tissues were fixed in 10% neutral buffered formalin (NBF), processed, and embedded in paraffin wax. Histological sections were evaluated for presence or absence of hemostatic material, inflammation, fibrosis, and mineralization using a four-point semi-quantitative scale: 0 = no response/not present, 1 = minimal/focal/barely detectable, 2 = mild/focal or rare multifocal/slightly detectable, 3 = moderate/multifocal to confluent/easily detectable, and 4 = marked/diffuse/overwhelming presence.
Treatment of Spinal Cord Injury
The objective of this procedure was to evaluate the ability of a flowable microfibrillar collagen product to provide hemostatic function when applied directly to the spinal cord in an ovine model of dorsal laminectomy and durotomy, without causing any damaging neurological or tissue effects. Adult castrated male (n=26) and nulliparous females (n=11) sheep (Ovis Aries; 7–53 months of age; 50.1–85.5 kg) were subjected to a hemi-laminectomy of the L2 and L3 vertebrae, followed by an incision in the dura mater to expose the spinal cord. Animals were randomly assigned to receive treatment with either modified AviteneTM flour combined with 7 mL saline (FL) or dry AviteneTM Flour (F0) and then evaluated after 45, 90 or 120 days (n=6–7 animals/treatment/time point). Sheep were fasted prior to surgery, then given buprenorphine (0.01–0.03 mg/kg) and banamine (1.0 mg/kg) prior to intubation. Anesthesia with inhalant anesthetic (Isoflurane 1–5%) was administered throughout the procedure. A 20–25 cm dorsal midline incision was made over the upper lumbar vertebrae and an L2/L3 laminectomy performed to expose the dura mater. After collecting 1 mL of cerebrospinal fluid, a 1-cm incision was made in the dura mater to expose the spinal cord. One of the two products (FL or F0) was then applied directly to the spinal cord and observed for 10 minutes to determine the ability to target the injury site. The surgical incision was closed with multiple layers of absorbable sutures and tissue glue was applied to the skin (if needed). Following the procedure, animals had health checks regularly and incision site observation for 7 days (or until complete healing). Neurological examinations were performed daily for 7 days, then on days 14, 30, and the day of sacrifice (45, 90 or 120 ± 3 days) to assess acute and progressive deficits in the central nervous system. Euthanasia was performed under anesthesia with 1 mL/4.5 kg euthasol or sodium pentobarbital and 2 mEq/kg potassium chloride administered intravenously. Treated areas of spinal cord were harvested, fixed in 10% NBF and prepared for histological evaluation. Paraffin-embedded sections were stained with hematoxylin and eosin and scored semi-quantitatively on a 0–4 scale (see previous section). Evaluated parameters included measures of inflammation (treatment site inflammation, leptomeningeal inflammation, histiocytes, giant cells, lymphocytes), hemostatic product (hemorrhage, presence and infiltration of treatment material), and impact to host tissues (spinal cord compression, axon sheath swelling, axonal degeneration, neuronal degeneration).
Statistical Analysis
For hemostatic efficacy, the number of injuries that passed/failed at each evaluation time point was compared using Fisher’s exact test. Statistical results with p<0.05 were considered statistically significant. Semi-quantitatively scored metrics (ie, bleed grade, histological measures, peritoneal tissue attachment severity) were not compared statistically but instead were compared qualitatively.
Results
Treatment of Liver Injury
The surgical procedure was able to create consistent and repeatable square capsular resection injuries in porcine liver tissue (Figure 1). Visual observation of the injuries shows differences in acute responses following treatment with the flowable (FL) and flour (F0) collagen microfibrillar materials or with gauze (Figure 1). While both collagen materials filled the wound sites, the flowable formulation was more cohesive and solid-like, while the collagen flour was looser and more granular. In contrast, temporary application with gauze left the wound appearance similar to the untreated case. The creation of capsular resection liver injuries led to consistent levels of bleeding as assessed by Lewis severity scores, with average values ranging between 1.0–1.3 and no significant differences between wounds assigned to the 30-, 90- or 120-day groups (Figure 2A). While the application of woven gauze resulted in hemostasis at a low rate of 8–42%, the use of either FL or F0 led to 100% hemostatic efficacy for all wounds (Figure 2B). Thus, both collagen products were much more effective at stopping acute bleeding than can be achieved through the use of gauze alone. For the long-term evaluation, animals recovered well and there was no mortality throughout the study. Semi-quantitative histological scores demonstrated mostly consistent results for the three products at 30, 90 and 120 days (Figure 3). Specifically, there was no hemorrhage detected for any product at any time point. Residual hemostatic material was only observed at 30 days in the organs treated with flowable material (FL, F0). Inflammation and fibrosis scores were similar between groups and gradually improved with time. Mineralization was observed in all three groups at 30 days, then only minimally in the gauze-treated livers at 90 and 120 days. Lastly, average peritoneal tissue attachment severity scores were relatively consistent at all three time points, with no significant differences between treatment groups (Figure 4).
 |
Figure 1 Images of capsular resection liver injury: (A) (untreated) or 10 minutes after application of treatment using (B) FL, (C) F0, or (D) Gauze (scale bar = 1 cm). |
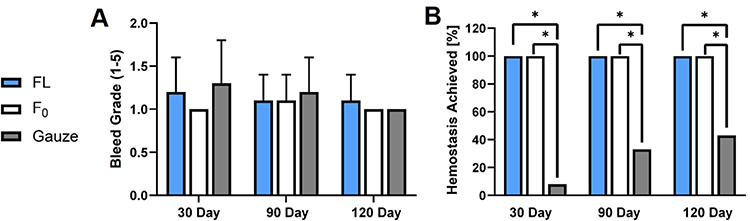 |
Figure 2 Acute response to capsular resection liver injury: (A) Bleed grade (mean ± standard deviation) and (B) Hemostatic efficacy (% of wounds with hemostasis) 10 minutes after applying FL, F0 or gauze (n=12/group; *For p<0.05). |
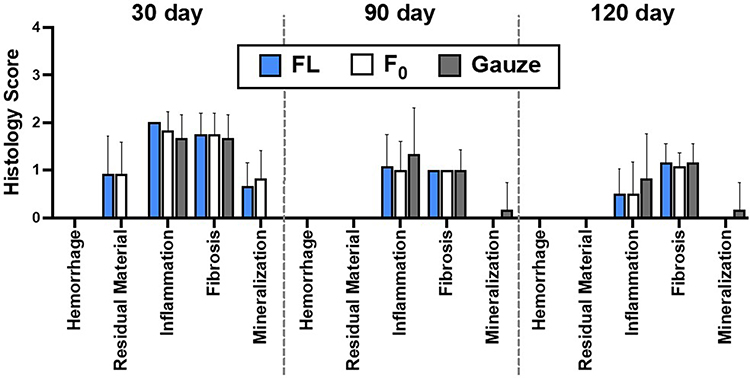 |
Figure 3 Semi-quantitative histological scores 30, 90 and 120 days after treating capsular resection liver injury with FL, F0 or gauze (mean ± standard deviation (SD); n=12/group). |
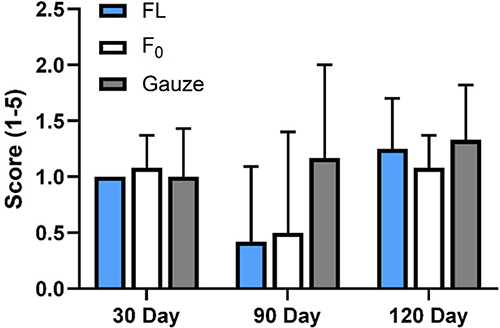 |
Figure 4 Peritoneal tissue attachment severity scores 30, 90 and 120 days after treating capsular resection liver injuries using FL, F0 or gauze (mean ± standard deviation (SD); n=12/group). |
Treatment of Spinal Cord Injury
In an ovine model of dorsal laminectomy and durotomy, direct spinal cord application of flowable collagen material was associated with favorable tissue responses (comparable to the application of a hemostatic flour product) and lack of any additional neurological effects. Some macroscopic differences were visually apparent following application of flowable (FL) or flour (F0) hemostatic products (Figure 5). Specifically, flowable collagen provided a smoother coating of material and more extensive coverage than the flour immediately after application; this effect was particularly evident at the 10-minute time point. All animals survived to predetermined endpoints; there was no mortality and no abnormal macroscopic observations noted. H&E-stained sections taken from the anatomical region posterior to (but including) the spinal cord showed the long-term biological response to treatment using the evaluated products (Figure 6). Visible in these sections are the edges of the laminectomy and the location of the applied collagen material. When scored histologically, measures of the inflammatory response were mostly consistent between the two groups and at each time point (Figure 7). Specifically, treatment site inflammation was mild for both groups at 45 days (average scores of 1.67–1.8) and minimal (<1) at later time points. Minimal leptomeningeal inflammation was detected at 45 and 90 days but was not observed at 120 days. Inflammatory cells (histiocytes, giant cells and lymphocytes) were minimally to slightly detectable at 45 days, absent at 90 days, then absent to barely detectable levels at 120 days. Other observations were made for the histological sections related to persistent hemostatic material and the impact on local tissues (Figure 8). For FL, minimal hemorrhage was evident at 30 days, but not at subsequent time points. Hemorrhage was present at low levels for F0-treated animals at all time points. The highest overall scoring metrics in this study were for the presence and infiltration of the treatment material, with average scores ranging from 1.33–3.67 at 45 days for the two products; however, both measures decreased to low or undetectable levels at 90 and 120 days. Lastly, all semi-quantitative measures of the tissue response (ie, spinal cord compression, axon sheath swelling, axonal degeneration, neuronal degeneration) were observed to be mild or not present at all time points and not different between groups.
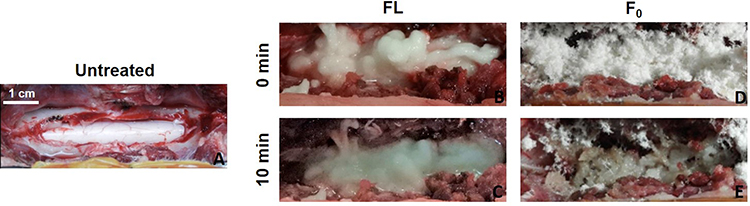 |
Figure 5 Images of spinal cord injury: (A) Without treatment (left) or 0 and 10 minutes after treatment using FL (middle (B and C)) or F0 (right (D and E)) (scale bar = 1 cm). |
 |
Figure 6 (left) Hematoxylin and eosin (H&E; scale bar = 2 mm) stained sections 45, 90 and 120 days after treating spinal cord injury with FL (A–C) and F0 (D–F); the 120-day F0 section is labeled with spinal cord (SC), edges of laminectomy (LM) and implanted material (MA) as an example; (Far right G)) photograph of representative spine specimen with dotted box showing the approximate location of stained sections in the vicinity of the spinal cord (scale bar = 1 cm). |
 |
Figure 7 Semi-quantitative inflammatory histological scores 45, 90 and 120 days after treating spinal cord injury with FL and F0 (mean ± standard deviation (SD); n=5–6/group). |
 |
Figure 8 Semi-quantitative general histological scores 45, 90 and 120 days after treating spinal cord injury with FL and F0 (mean ± standard deviation (SD); n=5–6/group). |
Among the dorsal laminectomy/durotomy groups, two animals did not complete the study: one 45-day F0 animal and one 120-day FL animal. Both animals that were lost to the study exhibited progressive hind limb ataxia and paresis after surgery. Veterinarian-recommended euthanasia was performed on day 10 and 3, respectively. For the 45-day F0 animal, assessment following necropsy revealed evidence of local hemorrhage unrelated to the device but associated with the surgical procedure and marked dorsoventral spinal cord compression that was consistent with the clinical presentation. For the 120-day FL animal, the treatment site exhibited mild dorsoventral compression (consistent with clinical deficits), mild hemorrhage, and notable treatment material presence without any evidence of adverse tissue response (eg, necrosis, excessive inflammation); thus, the outcome was attributed to the surgical laminectomy model and not device-related. Due to experimental constraints, only the latter could be replaced with an additional animal. Thus, each group included 12 (45- and 90-day) or 13 (120-day) animals, with a total of 37 sheep used.
Discussion
The primary objective of this study was to compare the hemostatic potential and local tissue responses to a novel, flowable collagen-based hemostatic agent to the original flour formulation to determine whether the method of delivery interfered with the hemostatic properties of the MCH flour. Comparable results were obtained for both formulations of microfibrillar collagen hemostatic material – flour and flowable – in representative animal models of solid organ (liver) injury and spine injury. For the flowable product, results demonstrated that there was no loss of hemostatic effect with the addition of saline pre-application (Figure 2B). Furthermore, the flowable material presented more uniform coverage and appearance (Figures 1 and 4) with precise application to injured tissues. The positive implementation of the flowable microfibrillar collagen formulation in these two preclinical models builds upon a long history of clinical success of the flour product.12
For the immediate response, capsular resection injury led to consistent levels of bleeding (~1.0–1.3; Figure 2A). After applying FL or F0, hemostasis was achieved in 100% of capsular resection injuries after 10 minutes (Figure 2B), indicating that both microfibrillar collagen products were effective at providing acute hemostasis following liver injury and significantly better than a comparison product (gauze).
For the long-term studies, treatment with the two microfibrillar collagen products (flour or flowable) yielded similar results in most of the outcome measures. For example, hemorrhage was not observed at any time points for liver injuries (Figure 3) and only minimally observed for spinal cord injuries (Figure 8), but with no apparent differences between groups. Moderate inflammation (average scores range 1.67–2.00) was observed at early time points (30 or 45 days) in both injuries, but then was minimally detected or absent at later times. In the case of the laminectomy and durotomy animals, leptomeningeal inflammation was not a prominent feature at any time for either treatment, while inflammatory cells (ie, histiocytes, giant cells, lymphocytes) mildly present at 45 days were reduced at 90 and 120 days (Figure 7). Thus, a mild inflammatory response observed initially was muted at later time points, consistent with a typical healing response following injury, and not noticeably affected by use of microfibrillar hemostatic material.
In the capsular resection liver injury, implanted hemostatic material was observed to interact with the adjacent peritoneal tissue via some loose attachments (score = 1) and firm attachments with minimal vascularity (score = 2); while there was some variability in these data (average values range 0.42–1.33), there were no significant differences between treatment groups or time points (Figure 4). In a similar manner, the extent of fibrosis, which represents the presence of extracellular matrix (ie, collagen), was observed to be consistent throughout with scores between 1–2 for all groups (Figure 3). At each evaluation point, fibrosis scores were very similar for FL, F0 and gauze groups, suggesting that fibrosis may reflect the general healing response in this injury model rather than a response to a particular biomaterial.
In terms of the temporal persistence of product, residual hemostatic material was detected in histological sections at early time points, particularly for the F0-treated spinal cord injury (average score of 2.6) compared to FL-treated spinal cord (1.33) or application of either material for liver injuries (0.92). Furthermore, the infiltration of treatment material, which is an indication of how much the hemostatic product is observed to spread into host tissue, was prevalent in spine tissues at 45-days. At later time points, residual material was not observed or only minimally present for both injuries; as expected, material infiltration was also greatly decreased at subsequent periods.
In treating bleeding of spinal tissues, a particular concern is the degree to which hemostatic materials swell. Anatomical spaces around the spinal elements are tight, and even moderate swelling of introduced materials could have functional consequences on neural function if neurological tissues are compressed. In this study, axonal sheath swelling was observed to be only moderate in the worst case, but then decreased over time. Temporal results for the flowable and flour products were similar, although F0 demonstrated slightly higher scores (ie, more swelling) at each time point compared to FL. Thus, collagen microfibrillar products – and flowable formulations in particular – may be well-suited for hemostatic applications in surgical regions where access and swelling may be a concern, for example, in spinal surgery. For the spinal cord injury, several metrics were never present to a meaningful degree for either treatment, including spinal cord compression, axonal degeneration, and neuronal degeneration; thus, these aspects of healing are not anticipated to play a major role in the biological response.
This study was not without limitations. First, only one product was included as a comparison group (gauze). However, the purpose of the study was not to compare the AviteneTM products to all available hemostat materials; instead, the objective was to compare a flowable form of the microfibrillar collagen product to the well-established flour formulation and determine short- and long-term outcomes in two representative tissue applications. Second, while three time points were considered for the long-term evaluation of the liver and spinal cord injuries (between 30–120 days), data acquired at earlier (<30 days) and/or later (>120 days) times would perhaps yield additional insights into the short- and long-term tissue response after using these products. Third, only one ratio of solid product to saline volume was evaluated (1 g flour with 7 mL saline); while other ratios would alter the relative viscosity of the flowable product, preliminary data using other volumes of saline (not shown) indicated an optimal flowability for the 7 mL formulation. Future studies should assess a variety of flowable hemostatic agents in head-to-head studies to elucidate the clinical relevance of the various formulations that have been utilized in neurosurgical applications to date, including the novel Avitene™ Flowable product described here.15–18Additionally, a number of other novel, flowable hemostatic agents have recently been reported in the published literature and could also be evaluated in future studies.19–21
Funding
This project was funded by Becton, Dickinson, and Company (BD).
Disclosure
Dr. Bradbury, Mrs. Gagne and Dr. Badhwar are employees of BD. Dr. Lake is a consultant for and Dr. Deeken is the owner of Covalent Bio, LLC, which received funding from BD for this project. Dr. Bohnen is a consultant for BD. Dr. Deeken reports consulting fees from BD for manuscript preparation, during the conduct of the study; she also reports consulting fees for unrelated projects from BD, Medtronic, SurgiMatrix, Tissium, Surgical Innovation Associates, Osteogenics, Polynovo, MedSkin Solutions, Aran Biomedical, Ethicon (Johnson & Johnson), Americas Hernia Society Quality Collaborative, Colorado Therapeutics, and TELABio, outside the submitted work; In addition, Dr. Deeken has patents in bionanocomposite materials broadly related to the field of hernia repair (patent numbers: 2009293001, 2334257 2,334,257UK 602009046407.8, 2,334,257FR, 16/043,849, 2,737,542) issued to University of Missouri. The authors report no other conflicts of interest in this work.
References
1. Stokes ME, Ye X, Shah M, et al. Impact of bleeding-related complications and/or blood product transfusions on hospital costs in inpatient surgical patients. BMC Health Serv Res. 2011;11:135. doi:10.1186/1472-6963-11-135
2. Schreiber MA, Neveleff DJ. Achieving hemostasis with topical hemostats: making clinically and economically appropriate decisions in the surgical and trauma settings. AORN J. 2011;94(5):S1–S20. doi:10.1016/j.aorn.2011.09.018
3. Zimmerman LH. Causes and consequences of critical bleeding and mechanisms of blood coagulation. Pharmacotherapy. 2007;27(9 Pt 2):45S–56S. doi:10.1592/phco.27.9part2.45S
4. Overbey DM, Jones EL, Robinson TN. How hemostatic agents interact with the coagulation cascade. AORN J. 2014;100(2):148–159. doi:10.1016/j.aorn.2013.12.012
5. Burks S, Spotnitz W. Safety and usability of hemostats, sealants, and adhesives. AORN J. 2014;100(2):160–176. doi:10.1016/j.aorn.2014.01.026
6. Ozawa S. Patient blood management: use of topical hemostatic and sealant agents. AORN J. 2013;98(5):461–478. doi:10.1016/j.aorn.2013.08.014
7. Marik PE, Corwin HL. Efficacy of red blood cell transfusion in the critically ill: a systematic review of the literature. Crit Care Med. 2008;36(9):2667–2674. doi:10.1097/CCM.0b013e3181844677
8. DeAndra JA, Elefteriades JA, Hasaniya NW, Lattouf OM, Lazzara RR. Improving outcomes through the use of surgical sealants for anastomotic sealing during cardiovascular surgery. J Card Surg. 2009;24(3):325–333. doi:10.1111/j.1540-8191.2009.00809.x
9. Shander A, Kaplan LJ, Harris MT, et al. Topical hemostatic therapy in surgery: bridging the knowledge and practice gap. J Am Coll Surg. 2014;219(3):570–579 e574. doi:10.1016/j.jamcollsurg.2014.03.061
10. Schonauer C, Mastantuoni C, Somma T, de Falco R, Cappabianca P, Tessitore E. Topical hemostatic agents in neurosurgery, a comprehensive review: 15 years update. Neurosurg Rev. 2022;45(2):1217–1232. doi:10.1007/s10143-021-01684-1
11. Roberto Giammalva G, Brunasso L, Costanzo R, et al. The role of hemostatic devices in neurosurgery. A systematic review. J Clin Neurosci. 2021;89:151–157. doi:10.1016/j.jocn.2021.05.016
12. Cziperle DJ. Avitene microfibrillar collagen hemostat for adjunctive hemostasis in surgical procedures: a systematic literature review. Med Devices. 2021;14:155–163. doi:10.2147/MDER.S298207
13. Achneck HE, Sileshi B, Jamiolkowski RM, Albala DM, Shapiro ML, Lawson JH. A comprehensive review of topical hemostatic agents: efficacy and recommendations for use. Ann Surg. 2010;251(2):217–228. doi:10.1097/SLA.0b013e3181c3bcca
14. Lewis KM, Li Q, Jones DS, et al. Development and validation of an intraoperative bleeding severity scale for use in clinical studies of hemostatic agents. Surgery. 2017;161(3):771–781. doi:10.1016/j.surg.2016.09.022
15. Ereth M, Sibonga J, Oliver W, Nuttall G, Henderson J, Dekutoski M. Microporous polysaccharide hemospheres do not inhibit bone healing compared to bone wax or microfibrillar collagen. Orthopedics. 2008;31(3):222.
16. Guo D, Li D, Li J, et al. Topical application of the hematostatic agent Surgiflo(R) could attenuate brain injury in experimental TBI mice. Neurol Res. 2017;39(9):830–836. doi:10.1080/01616412.2017.1330815
17. Gazzeri R, Galarza M, Alfier A. Safety biocompatibility of gelatin hemostatic matrix (Floseal and Surgiflo) in neurosurgical procedures. Surg Technol Int. 2012;22:49–54.
18. Landi A, Gregori F, Marotta N, Delfini R. Efficacy, security, and manageability of gelified hemostatic matrix in bleeding control during thoracic and lumbar spine surgery: floSeal versus surgiflo. J Neurol Surg a Cent Eur Neurosurg. 2016;77(2):139–143. doi:10.1055/s-0035-1558413
19. Chen Z, Yao J, Zhao J, Wang S. Injectable wound dressing based on carboxymethyl chitosan triple-network hydrogel for effective wound antibacterial and hemostasis. Int J Biol Macromol. 2023;225:1235–1245. doi:10.1016/j.ijbiomac.2022.11.184
20. Wang T, Yi W, Zhang Y, et al. Sodium alginate hydrogel containing platelet-rich plasma for wound healing. Colloids Surf B Biointerfaces. 2023;222:113096. doi:10.1016/j.colsurfb.2022.113096
21. Xu X, Zeng Y, Chen Z, et al. Chitosan-based multifunctional hydrogel for sequential wound inflammation elimination, infection inhibition, and wound healing. Int J Biol Macromol. 2023;235:123847. doi:10.1016/j.ijbiomac.2023.123847
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.