")
Back to Journals » Research and Reports in Urology » Volume 15
Efficacy Analysis of Physical Therapy in Treating Chronic Prostatitis: Unblocking Obstructed Glandular Ducts Could Be a Novel Treatment Strategy
Received 2 October 2023
Accepted for publication 28 November 2023
Published 18 December 2023 Volume 2023:15 Pages 553—561
DOI https://doi.org/10.2147/RRU.S442844
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Guglielmo Mantica
Weiguang Lin,1,2 Yunlong Wang,1,2 Yanxiong Chen1,2
1Department of Urology, Renhui Clinic, Jiangmen, 529099, People’s Republic of China; 2Department of Urology, Renhui Frontline Clinic, Shenzhen, 518038, People’s Republic of China
Correspondence: Yanxiong Chen, Department of Urology, Renhui Clinic, Jiangmen, 529099, People’s Republic of China, Email [email protected]
Objective: This study investigates the efficacy of physical therapy in treating chronic prostatitis grounded on the glandular duct blockage theory.
Methods: The study includes patients who were diagnosed and treated for chronic prostatitis between November 2022 and July 2023 at Renhui clinic in Jiangmen, Guangdong and Renhui frontline clinic in Shenzhen Guangdong. The recorded data includes the frequency of physical therapies including prostate massages, rectal probe high-frequency vibration treatment, and low-intensity extracorporeal shockwave therapy (Li-ESWT). Post-treatment urine sediment was collected for microscopic examination, and the scores of each patient on the National Institutes of Health Chronic Prostatitis Symptom Index (NIH-CPSI) and the Premature Ejaculation Diagnostic Tool (PEDT) were recorded pre- and post-treatment in order to calculate the effectiveness rate.
Results: The study involved a total of 48 patients, of which 26 were diagnosed with premature ejaculation. On average, each patient received 2.1 prostate massages, underwent 4.1 rectal probe high-frequency vibration treatments, and 8.3 Li-ESWT sessions. Following treatment, the initial microscopic examination of the urine sediment revealed aged white blood cell clusters, prostate calculi clusters, and inactive sperm clusters, all appearing in the shape of glandular tubes. The mean NIH-CPSI scores pre- and post-treatment were 27.2± 6.9 and 18.0± 6.6, respectively, indicating an effectiveness rate of 81.3%. The average PEDT scores pre- and post-treatment were 14.5± 3.5 and 10.5± 4.2, respectively, with an effectiveness rate of 53.8%.
Conclusion: Unblocking obstructed glandular ducts might provide a novel therapeutic strategy for treating chronic prostatitis.
Keywords: chronic prostatitis, low-intensity extracorporeal shockwave therapy, physical therapy, glandular duct
The prostate consists of 70% glands and 30% fibromuscular interstitium. The glandular part is primarily made up of 30–50 complex tubuloalveolar glands, with the main function of secreting prostatic fluid.1 The glandular tissue comprises three sections. The mucosal gland, being the smallest, resides within the urethral mucosa and directly opens into the urethra. The submucosal gland is positioned under the mucosal layer, and the main gland makes up the majority of the gland structure.2 The glandular duct is an essential part of the prostate. The main gland’s duct is the longest and has a winding route. There are many types of prostatitis,1,3 when the gland becomes inflamed, various inflammatory substances can cause tissue congestion and edema. This glandular enlargement may lead to the narrowing of the duct, subsequently resulting in ductal obstruction.4 As the duct remains obstructed, exudation from the inflamed prostate tissue occurs, and the size of the prostate enlarges compared to its previous state.4 The swollen prostate exerts pressure inwards onto the urethra. Simultaneously, different inflammatory agents irritate the urethra, resulting in symptoms like frequent urination, urgency, and incomplete emptying. Around the prostate is a mesh-like distribution of the pelvic nerve plexus. These plexuses are mainly visceral sensory nerves and those responsible for controlling erection and ejaculation. Inflammation within the prostate tissue can also cause exudation that irritates the pelvic nerve plexus. Furthermore, the swollen prostate can press outwards on the nearby pelvic nerve plexus, possibly resulting in symptoms like pelvic pain and disorders in sexual function.5–7 Based on the aforementioned glandular duct obstruction theory, prostate massage has been a primary treatment method for chronic prostatitis (CP) since the early 20th century.1 Extracorporeal shock wave therapy has been used in clinical practice for nearly 50 years. Since low-intensity extracorporeal shockwave therapy (Li-ESWT) was reported for the treatment of CP, its safety and efficacy have been confirmed by numerous studies.8–10 In this research, we adopted a treatment method combining prostate massage with Li-ESWT for CP, which showed promising results. Herein we report the details.
Materials and Methods
Data were collected from Renhui Clinic in Jiangmen City, Guangdong Province, and Renhui Frontline Clinic in Shenzhen City from November 2022 to July 2023. This data was based on patient interviews, rectal finger examinations, expressed prostatic secretion (EPS) tests, previous color Doppler ultrasound results, EPS and post-massage urine culture results, and scores from the National Institutes of Health Chronic Prostatitis Symptom Index (NIH-CPSI) to confirm a diagnosis of CP. Inclusion criteria: 1. Ages between 18 and 50; 2. Main clinical manifestation of perineal or lower abdominal pain persisting for over 3 months, possibly with symptoms of the lower urinary tract and sexual dysfunction; 3. NIH-CPSI score of more than 10. Exclusion criteria: 1. Perineal skin damage or infection; 2. Suffering from bleeding disorders or currently on anticoagulant therapy; 3. Cases with a history of bladder, prostate, or rectal surgeries not suitable for prostate massage; 4. Cases with incomplete follow-up information. This study was approved by the Ethics Committee of Baiyun District Maternal and Child Health Hospital (NO.20230518), and informed consent was obtained from all cases.
Every patient underwent physical therapy which contains three therapeutic methods: prostate massage, rectal probe high-frequency vibration treatment (RPHFVT), Li-ESWT. The procedure for prostate massage involves the patient assuming a chest-knee lying position, the doctor inserts the index finger into the patient’s anus, and massages from both sides of the prostate towards the central groove three times each, finally massaging the central groove from top to bottom three times. This sequence is repeated for approximately 3 minutes. RPHFVT uses a prostate treatment device (TRM-2Z(B), produced by Wuhan Fairfun Technology Co., Ltd., see Figure 1). Patients are placed in a lateral decubitus position with bent knees, after lubricating the anus, the probe is inserted, where its angle and depth are adjusted ensuring the probe surface is closely aligned with the central groove, then the vibration amplitude is fine-tuned, and the operational duration is set for 30 minutes. Li-ESWT uses an extracorporeal shock wave therapy device (LGT-2500S, produced by Guangzhou Longest Technology Co., Ltd., see Figure 2). The device parameters are set with an energy density of 0.25mJ/mm2, a frequency of 8HZ, and 3000 shock wave pulses. Patients are instructed to assume a chest-knee lying position, the shock wave probe is aligned with the patient’s perineal area for treatment, during the shock wave treatment, a doctor's finger is simultaneously inserted into the rectum for prostate massage, the doctor’s finger can be used inside the rectum for palpation, guiding the direction of the shock waves, ensuring comprehensive shock wave treatment across the entire prostate area, while also focusing on harder localized regions for intensive therapy. The doctor arranges the treatment plan based on each patient’s schedule, ensuring that each patient receives at most two treatments daily, with an interval of more than 3 hours between treatments. Normally, each patient first receives RPHFVT 2–4 times to open up the outlet of the glandular duct. The follow-up treatments are mainly Li-ESWT. The patient is scheduled to have a prostate massage after every 3–5 Li-ESWT sessions. If prostate fluid is seen emanating from the urethral orifice after each treatment, it is sampled for microscopic examination, and every time, the sediment from the post-therapy urine is also taken for microscopic analysis. Each patient is assessed using the NIH-CPSI and premature ejaculation diagnostic tool (PEDT) scores before starting the treatment. Scoring with NIH-CPSI and PEDT is also done two weeks post-treatment completion, Comparisons are made between the two sets of scores, an NIH-CPSI reduction of at least 6 points is deemed indicative of effective treatment, a PEDT score of ≥11 indicates the existence of premature ejaculation, scores between 9 and 10 suggest potential premature ejaculation, while scores of ≤8 indicate no premature ejaculation. Patients who had (or were suspected to have) premature ejaculation before treatment and transitioned to no premature ejaculation post-treatment are considered effectively treated, and the treatment efficacy rate is then compiled.
 |
Figure 1 Prostate treatment device (TRM-2ZB), produced by Wuhan Fairfun Technology Co., Ltd.). |
 |
Figure 2 Extracorporeal shock wave therapy device (LGT-2500S, produced by Guangzhou Longest Technology Co., Ltd.). |
Results
A total of 48 patients were studied, of which 26 were diagnosed with premature ejaculation. Each patient received three treatment modalities of physical therapy, the average number of prostate massages administered was 2.1, underwent RPHFVT 4.1 times, and received Li-ESWT 8.3 times. Post-treatment, microscopic examination of the prostatic fluid showed the release of ductal obstructions, such as aged white blood cell clusters that took the shape of glandular ducts (Figure 3), formations of prostate calculi (Figure 4), and groups of inactive sperms (Figure 5). Following the treatment, strip-like urinary sediments could be observed in the initial urine (Figure 6), The collected urinary sediment, when pipetted onto a slide, revealed white strip-like formations (Figure 7). Upon microscopic examination, it revealed aged white blood cell clusters that had the appearance of glandular ducts (Figure 8), alongside old white blood cell clusters and prostate calculi both exhibiting the glandular duct shape (Figures 9 and 10), and clusters of prostate calculi taking on a glandular duct shape (Figure 11), and inactive sperm clusters also resembling glandular ducts (Figure 12). Efficacy rates for CPSI and PEDT are shown in Table 1.
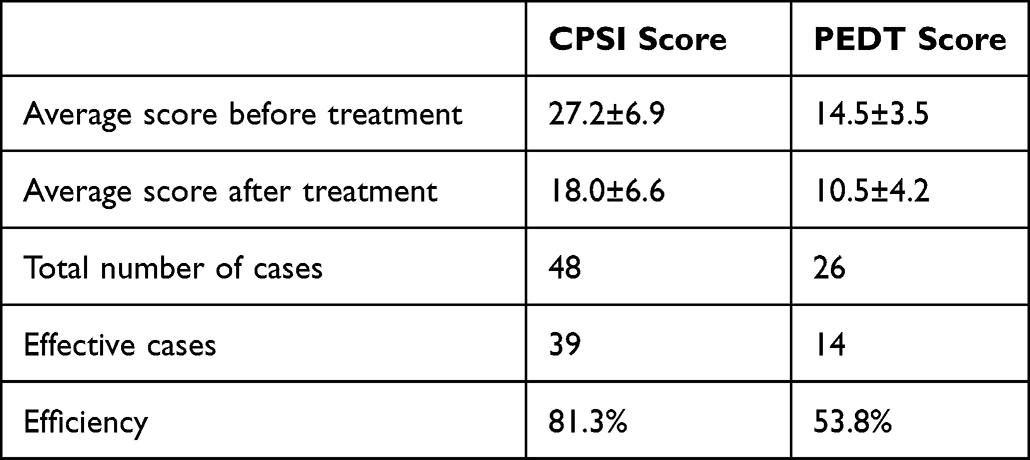 |
Table 1 Results of Physical Therapy |
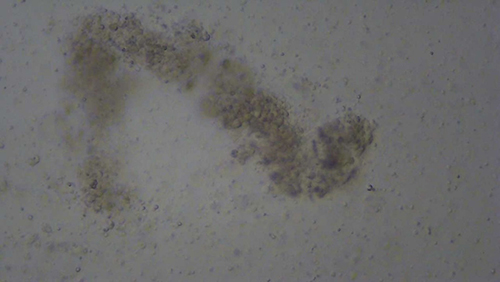 |
Figure 3 Aged white blood cell clusters in the shape of glandular tubes are visible in the prostatic fluid (magnified 500x under microscopy). |
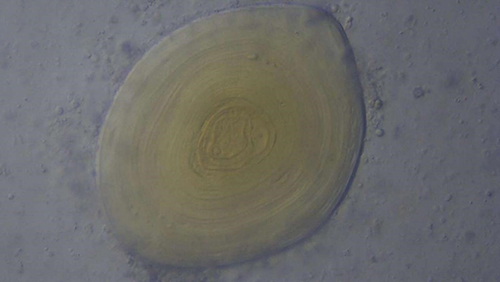 |
Figure 4 Prostate calculi is visible in the prostatic fluid (magnified 500x under microscopy). |
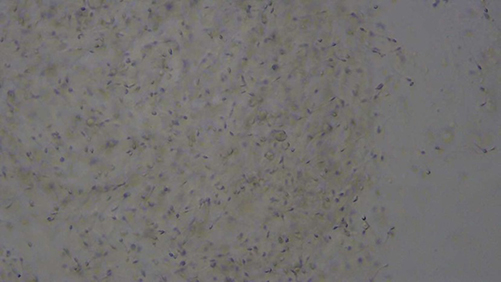 |
Figure 5 Inactive sperms are visible in the prostatic fluid (magnified 500x under microscopy). |
 |
Figure 6 Strip-shaped urinary sediments are visible in the post-treatment urine (the strip-shaped sediments are pointed out by the red arrow). |
 |
Figure 7 The strip-shaped urinary sediment is aspirated and placed on a slide (the strip-shaped sediments are pointed out by the red arrow). |
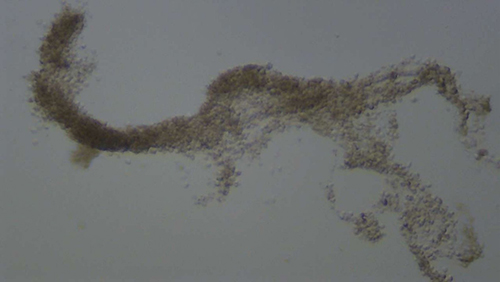 |
Figure 8 Branched glandular-shaped aged white cell clumps (magnified 200x under microscopy). |
 |
Figure 9 Glandular-shaped old white cell clumps and prostate calculi (magnified 500x under microscopy). |
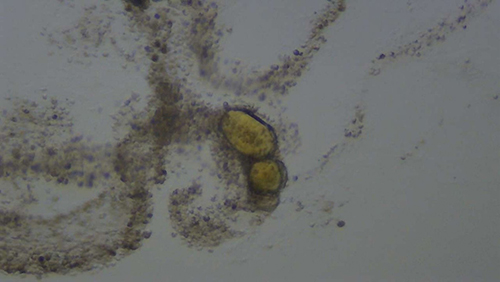 |
Figure 10 Glandular-shaped old white cell clumps and prostate calculi (magnified 200x under microscopy). |
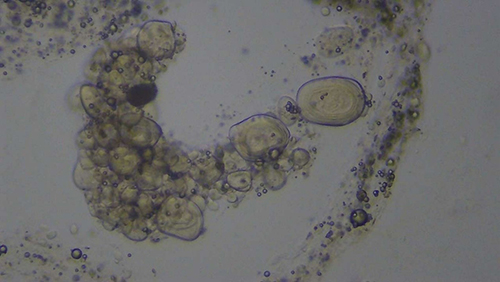 |
Figure 11 Prostate calculi clusters arranged in a glandular shape (magnified 500x under microscopy). |
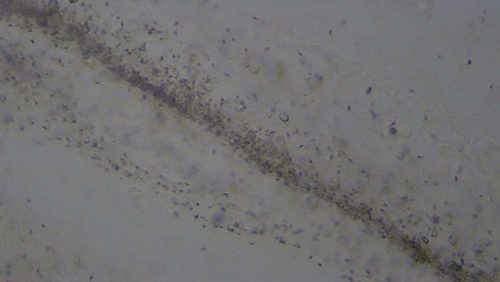 |
Figure 12 Inactive sperms arranged in a glandular shape (magnified 500x under microscopy). |
Discussion
CP is regarded as a complex disease in urology, currently, the predominant treatment strategy for CP largely relies on drug-based comprehensive regimens.11,12 The range of drugs includes antibiotics, alpha-receptor blockers, psychotropic medications, and botanical preparations,13,14 but the therapeutic effects of these medications have been less than satisfactory.15,16 Prostate massage has been a principal treatment for CP since the early 20th century.1 Currently, as drugs often prove ineffective for the stubborn symptoms of CP, prostate massage has regained favor. Prostate massage aids in expelling obstructions from the glandular ducts, facilitating the clearance of blocked ducts and enhancing peripheral blood flow around the prostate.1 The probe is inserted into the rectum and placed closely against the central groove of the prostate. High-frequency vibrations can facilitate the expulsion of obstructions from the glandular ducts, functioning on the same principle as prostate massage. The effectiveness and safety of Li-ESWT for treating CP have been confirmed in multiple studies.9,10,17 There are four reaction phases on tissue: physical, physicochemical, chemical, and biological reactions. It can break down calcium salt deposits in tissues, while promoting cell proliferation, neovascularization, and protein synthesis in the treated area, thereby enhancing the function of damaged tissues.18,19 Li-ESWT offers hope to patients with prostatitis due to its role in alleviating urinary symptoms and relieving pain.20–23
Based on the aforementioned theories, we conducted this research. Every patient kept their first urine sample after treatment, often, the urine appeared turbid to the naked eye, with a significant amount of sediment present. We examined the urine sediment under a microscope, and frequently observed prostate calculi. Research suggests that inflammation of the prostate is a significant factor in the formation of prostate calculi.4 When there is chronic inflammation in the prostate tissue, the narrowing of the glandular duct results in poor drainage of prostatic fluid, leading to the accumulation of prostatic fluid and calcium salts, thereby causing the formation of prostate calculi. However, after the formation of prostate calculi, the blockage of the glandular duct becomes more severe, and the inflammatory response intensifies, creating a vicious cycle. Physical therapy aims to break this cycle. Once prostate calculi is expelled, the glandular duct is unblocked, and the inflammatory response is alleviated.
Microscopic examination of urinary sediment frequently reveals aged clusters of white blood cells arranged in a pattern resembling glandular ducts. The production of white blood cells may not be due to a bacterial infection, but rather, after the ducts are obstructed, the body’s immune system naturally secretes white blood cells into the glandular ducts. However, the white blood cells are ineffective in addressing the obstruction in the ducts. They gradually accumulate in the ducts, eventually forming tube-like clusters. These tubular clusters of white blood cells eventually intensify the blockage and level of inflammation in the ducts. Physical therapy facilitates the expulsion of the blocked white blood cell clusters, ultimately clearing the glandular ducts.
Microscopic examination of urinary sediment also found inactivated sperm, The ejaculatory duct traverses the prostate and merges into the urethra, Blockage of the prostatic duct can compress the ejaculatory duct, leading to obstruction of semen expulsion or reflux into the surrounding prostatic ducts. Sperm that accumulates in the prostatic duct for a prolonged period will become inactivated, Physical therapy can expel sperm trapped in the duct, clearing the glandular duct.
During Li-ESWT combined with prostate massage, finger examination often finds that the obstructed glandular duct area is relatively hard, and there is pain upon pressing. With the mechanotransduction of Li-ESWT, the blockages inside the glandular duct start to loosen, and the blocked area starts to soften, fingers can then smoothly push out the obstruction, the softened prostate tissue can also be maneuvered by the finger, thereby separating the adhesion between the prostate and surrounding pelvic tissues, and relieving the compression of the prostate on the surrounding nerve bundles. Normally, each patient first receives RPHFVT 2–4 times to open up the outlet of the glandular duct. The follow-up treatments are mainly Li-ESWT, because it can conduct energy to the depth of the gland. The patient is scheduled to have a prostate massage after every 3–5 Li-ESWT sessions. Prostate massage can push out the blockage of the glandular duct from the depth of the glandular duct.
When the prostate stones, white blood cell clusters, and inactive sperm trapped inside the glandular duct are expelled, the duct becomes unobstructed again, the volume of the prostate will also reduce compared to its previous size, the compression and inflammatory irritation exerted by the prostate on the urethra and surrounding nerve bundles will lessen, Urination, pelvic pain and symptoms of sexual dysfunction all exhibit different levels of improvement. As the number of treatments increases, the glandular ducts will further unblock, and the effectiveness may improve. Medication alone was often ineffective in treating refractory prostatitis.24 Multidisciplinary treatment of CP is necessary.25,26 When the glandular ducts of the prostate are unblocked, drugs can more easily penetrate into the gland. Physical therapy combined with medication may improve the effectiveness of the treatment of chronic prostatitis.
This research initially shows that physical therapy can unblock obstructed glandular ducts to alleviate symptoms of prostatitis, however, this study has its limitations, with a small number of cases and the absence of a control group and multi-disciplinary treatment, and further research will be carried out in the future.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Baiyun District Maternal and Child Health Hospital (NO.20230518). All procedures performed in the study involving human participants were in accordance with the 1964 Declaration of Helsinki, and informed consent was obtained from all cases.
Acknowledgments
We very much appreciate the help of Professor Hu Li of Baiyun District Maternal and Child Health Hospital for his technical guidance.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received.
Disclosure
The authors declare that they have no competing interests.
References
1. Wein AJ. Campbell-Walsh Urology.
2. Lpgjl H. Concise. Histology: Saunders; 2011.
3. Crocetto F, Barone B, De Luca L, Creta M. Granulomatous prostatitis: a challenging differential diagnosis to take into consideration. Future Oncol. 2020;16(13):805–806. doi:10.2217/fon-2020-0185
4. Hyun JS. Clinical significance of prostatic calculi: a review. World J Mens Health. 2018;36(1):15–21. doi:10.5534/wjmh.17018
5. Chung SD, Keller JJ, Lin HC. A case-control study on the association between chronic prostatitis/chronic pelvic pain syndrome and erectile dysfunction. BJU Int. 2012;110(5):726–730. doi:10.1111/j.1464-410X.2011.10807.x
6. Cai T, Pisano F, Magri V, et al. Chlamydia trachomatis infection is related to premature ejaculation in chronic prostatitis patients: results from a cross-sectional study. J Sex Med. 2014;11(12):3085–3092. doi:10.1111/jsm.12699
7. Tran CN, Shoskes DA. Sexual dysfunction in chronic prostatitis/chronic pelvic pain syndrome. World J Urol. 2013;31(4):741–746. doi:10.1007/s00345-013-1076-5
8. Franco JVA, Turk T, Jung JH, et al. Non-pharmacological interventions for treating chronic prostatitis/chronic pelvic pain syndrome: a Cochrane systematic review. BJU Int. 2019;124(2):197–208. doi:10.1111/bju.14492
9. Mykoniatis I, Pyrgidis N, Sokolakis I, et al. Low-intensity shockwave therapy for the management of chronic prostatitis/chronic pelvic pain syndrome: a systematic review and meta-analysis. BJU Int. 2021;128(2):144–152. doi:10.1111/bju.15335
10. Kernesiuk MN, Prouza O. Experience of the use of extracorporeal shock wave therapy in the treatment of category III B chronic prostatitis. Urologiia. 2013;6): 36:8–9.
11. Krakhotkin DV, Chernylovskyi VA, Bakurov EE, Sperl J. Evaluation of influence of the UPOINT-guided multimodal therapy in men with chronic prostatitis/chronic pelvic pain syndrome on dynamic values NIH-CPSI: a prospective, controlled, comparative study. Ther Adv Urol. 2019;11:1756287219857271. doi:10.1177/1756287219857271
12. Polackwich AS, Shoskes DA. Chronic prostatitis/chronic pelvic pain syndrome: a review of evaluation and therapy. Prostate Cancer Prostatic Dis. 2016;19(2):132–138. doi:10.1038/pcan.2016.8
13. Hiramatsu I, Tsujimura A, Soejima M, et al. Tadalafil is sufficiently effective for severe chronic prostatitis/chronic pelvic pain syndrome in patients with benign prostatic hyperplasia. Int J Urol. 2020;27(1):53–57. doi:10.1111/iju.14122
14. Abdel-Meguid TA, Mosli HA, Farsi H, et al. Treatment of refractory category III nonbacterial chronic prostatitis/chronic pelvic pain syndrome with intraprostatic injection of onabotulinumtoxinA: a prospective controlled study. Can J Urol. 2018;25(2):9273–9280.
15. Franco JVA, Turk T, Jung JH, et al. Pharmacological interventions for treating chronic prostatitis/chronic pelvic pain syndrome: a Cochrane systematic review. BJU Int. 2020;125(4):490–496. doi:10.1111/bju.14988
16. Hu M, Wazir J, Ullah R, et al. Phytotherapy and physical therapy in the management of chronic prostatitis-chronic pelvic pain syndrome. Int Urol Nephrol. 2019;51(7):1081–1088. doi:10.1007/s11255-019-02161-x
17. Daneshwar D, Nordin A. Treatment of prostatitis with low-intensity extracorporeal shockwave therapy (LI-ESWT). Int Urol Nephrol. 2023;55(12):3133–3145. doi:10.1007/s11255-023-03616-y
18. Simplicio CL, Purita J, Murrell W, Santos GS, Dos santos RG, Lana J. Extracorporeal shock wave therapy mechanisms in musculoskeletal regenerative medicine. J Clin Orthop Trauma. 2020;11(Suppl 3):S309–S18. doi:10.1016/j.jcot.2020.02.004
19. Liu Y, Chen X, Guo A, Liu S, Hu G. Quantitative assessments of mechanical responses upon radial extracorporeal shock wave therapy. Adv Sci. 2018;5(3):1700797. doi:10.1002/advs.201700797
20. Guu SJ, Geng JH, Chao IT, et al. Efficacy of low-intensity extracorporeal shock wave therapy on men with chronic pelvic pain syndrome refractory to 3-as therapy. Am J Mens Health. 2018;12(2):441–452. doi:10.1177/1557988317736585
21. Zhang ZX, Zhang D, Yu XT, Ma YW. Efficacy of radial extracorporeal shock wave therapy for chronic pelvic pain syndrome: a nonrandomized controlled trial. Am J Mens Health. 2019;13(1):1557988318814663. doi:10.1177/1557988318814663
22. Pajovic B, Radojevic N, Dimitrovski A, Vukovic M. Comparison of the efficiency of combined extracorporeal shock-wave therapy and triple therapy versus triple therapy itself in category III B chronic pelvic pain syndrome (CPPS). Aging Male. 2016;19(3):202–207. doi:10.1080/13685538.2016.1197899
23. Rayegani SM, Razzaghi MR, Raeissadat SA, et al. Extracorporeal shockwave therapy combined with drug therapy in chronic pelvic pain syndrome: a randomized clinical trial. Urol J. 2020;17(2):185–191. doi:10.22037/uj.v0i0.4673
24. Barone B, Mirto BF, Falcone A, et al. The efficacy of flogofilm((r)) in the treatment of chronic bacterial prostatitis as an adjuvant to antibiotic therapy: a randomized prospective Trial. J Clin Med. 2023;12(8):2784. doi:10.3390/jcm12082784
25. Magri V, Boltri M, Cai T, et al. Multidisciplinary approach to prostatitis. Arch Ital Urol Androl. 2019;90(4):227–248. doi:10.4081/aiua.2018.4.227
26. Centemero A, Rigatti L, Giraudo D, et al. The role of the multi-disciplinary team and multi-disciplinary therapeutic protocol in the management of the chronic pelvic pain: there is strenght in numbers! Arch Ital Urol Androl. 2021;93(2):211–214. doi:10.4081/aiua.2021.2.211
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.