")
Back to Journals » Open Access Surgery » Volume 16
Effectiveness of Leg-Elevation to Prevent Post-Spinal Hypotension in Elective Cesarean Section: A Systematic Literature Review of Randomized Controlled Trial
Authors Besha Desta A, Alemu B, Mossie A , Abebe M, Shiferaw A , Girma B, Ilala TT , Tamrat Yilma K, Mohamed K
Received 19 July 2023
Accepted for publication 26 September 2023
Published 9 October 2023 Volume 2023:16 Pages 61—68
DOI https://doi.org/10.2147/OAS.S426771
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Luigi Bonavina
Aschalew Besha Desta,1 Belete Alemu,1 Addisu Mossie,1 Minda Abebe,1 Adanech Shiferaw,1 Bizuwork Girma,2 Tajera Tageza Ilala,1 Kidanamariam Tamrat Yilma,1 Khalid Mohamed3
1Department of Anesthesia, College of Health Sciences and Medicine, Hawassa University, Hawassa, Ethiopia; 2Department of Anesthesia, College of Health Sciences and Medicine, Selale University, Fiche, Ethiopia; 3Department of Anesthesia, College of Health Sciences and Medicine, Bule Hora University, Bule Hora, Ethiopia
Correspondence: Aschalew Besha Desta, Anesthesia Department, College of Health Sciences and Medicine, Hawassa University, Hawassa, Ethiopia, Email [email protected]
Background: A typical side effect of spinal anaesthesia is post-spinal hypotension. Its overall incidence ranges between 25– 75% in the general population, and it is even higher in pregnant mothers who underwent a caesarean delivery. Post-spinal hypotension-related adverse effects can be prevented by having adequate evidence-based knowledge about their management and prevention. The objective of this review is to determine the effectiveness of leg elevation in preventing post-spinal induced hypotension during elective caesarean sections.
Methods: A comprehensive literature search was conducted in PubMed, the Medline database, the Cochrane Review, and Google Scholar from 1993 to 2023. Healthy women with full-term pregnancies who underwent elective caesarean delivery performed with spinal anaesthesia were included, and parturients with co-existing diseases, studies on other population, case reports studies written in non-English languages and studies contain abstract only were excluded. For both interventional and non-interventional research, the methodological strengths of the included studies were evaluated using the Cochrane risk of bias assessment tool.
Results: A total of 8158 articles from various electronic databases were found using the search method. After removing duplicates, 247 articles were chosen for screening; 13 were included for critical evaluation, and 6 were eliminated with justifications. The included publications are made up of 7 RCTs on 681 pregnant women in 5 different countries, and it was found that the leg elevated group had a lower incidence of post-spinal hypotension than the control group.
Conclusion: A majority of the evidence revealed that leg elevation following spinal anaesthesia in a caesarean delivery was effective in preventing post-spinal-induced hypotension. In addition to prevention, applying leg elevation following spinal anaesthesia is helpful in lowering the incidence of post-spinal hypotension, which is catastrophic. It reduces the requirement for vasopressors and also provides a non-invasive and reversible technique that does not call for any special equipment.
Keywords: leg elevation, prevention, hypotension, spinal anesthesia, cesarean section
Introduction
Caesarean sections are becoming more prevalent around the world, with rates rising in both developed and developing countries. According to the situation and timing of the mother and foetus, it can be performed electively or urgently.1
Regional anaesthesia also aligns with the most popular caesarean delivery technique due to its ease of usage, quick start, and benefits to both the mother and the foetus. Despite its simplicity and safety compared to general anaesthesia, it is associated with different adverse effects, of which post-spinal hypotension is the most common.2
Hypotension is frequently described as a systolic blood pressure less than 100 mm Hg or a drop of 20% or more from the patient’s baseline. Because of physiological changes associated with pregnancy, including compression of the inferior vena cava by the enlarged uterus and sympathetic inhibition from neuraxial blockage, which significantly lowers parturients’ blood pressure, the incidence of post spinal hypotension is 80% in pregnancy, which is higher than the general population’s 25% to 75%.3,4
Post-spinal hypotension (PSH) is the most common problem in caesarean delivery. Since prevention and management of PSH have been extensively researched, the major goals of these treatments are to increase vascular tone and venous return, which can be accomplished by using vasopressors, fluid administration, and positioning techniques.5
Potential risk factors for post-spinal hypotension include a history of hypertension, body mass index, the height of the sensory block, the time between spinal induction and the delivery of the foetus, the urgency of the surgery, spinal additives, the length of the crystalloid load, a high gravid uterus, and the rate of injection. Finding these indicators is crucial in an area with limited resources for monitoring key organs and also for assisting clinicians in making treatment decisions for moms who are at risk of hypotension.6
Additionally, compared to parasympathetic activity, sympathetic activity is more prominent in pregnant women. Since parasympathetic activity predominates and peripheral vasodilatation is increased by sympathetic activity, venous return and cardiac preload are decreased, which causes bradycardia, nausea, and vomiting. Systemic hypotension is the outcome of the decreased pre-load, which also causes decreased cardiac output (CO). Aortocaval compression aggravates this condition even further. The same sympathetic blockade achieved with epidural anaesthesia but with a lower incidence and severity of hypotension may be explained by the sudden onset of sympathetic blockade, which leaves little time for cardiovascular compensation and frequently causes maternal hypotension. Higher sympathetic block correspondingly raises the danger of cardio-inhibitory responses like the Bezold-Jarisch reflex and, ultimately, cardiac arrest and mortality by decreasing the occurrence of compensatory mechanisms through baroreceptors.7
Since uterine blood flow has been demonstrated to be reduced after blood pressure has been recovered, prevention of PSH is preferable rather than treatment. According to their findings, volume expansion with crystalloid, a frequent clinical practise, is not always successful in lowering the incidence of maternal hypotension following spinal anaesthesia for caesarean delivery. Although colloid administration is more reliable, there are also higher costs. Although it was assumed that vasopressors such as phenylephrine would lessen uterine arterial blood flow and foetal umbilical arterial PH, they were also beneficial in normalizing maternal blood pressure. Although mechanical methods to increase central blood volume appear to be similarly effective, they are not commonly used.8–10
The best way to prevent hypotension during caesarean section is still up for debate, despite the fact that many measures have been reported for its prevention and management. As a result, this review also aims to find evidence for physical prophylactic measures such as leg elevation in preventing PSH, as it is a straightforward and affordable management protocol applied with little experience and has a less adverse effect.11 The main objective of this review is to determine the effects of leg elevation to prevent post-spinal-induced hypotension in women having elective caesarean delivery under spinal anaesthesia.
Objective
The objective of this review is to summarize evidence on the effectiveness of leg elevation in preventing post-spinal-induced hypotension in elective caesarean sections.
Review Questions
We were conducting this review to have the common understanding on identifying post-spinal hypotension prevention strategies, selecting preferable techniques on prevention of PSH and effectiveness applying lower leg elevation during CS for reducing maternal hypotension following SA.
Methods and Materials
Protocol
The method of reporting the review used is preferred reporting of systematic review and meta-analysis (PRISMA).
Eligibility Criteria
Inclusion Criteria
All randomized controlled trials reporting the effectiveness of leg elevation for PSH in elective cesarean section from 1993 to 2023 were covered.
Exclusion Criteria
Parturients with co-existing diseases, studies on other population, case reports studies written in non-English languages and studies contain abstract only were excluded.
Search Strategy
Electronic databases, including the Cochrane Library, PubMed/Medline, and Google Scholar, were all thoroughly searched. The goal of the search approach was to examine all randomised controlled trials on the prevention of PSH in pregnant patients having an elective caesarean section under spinal anaesthesia, both published and unpublished. The Cochrane Library and PubMed/Medline were used for a thorough initial search. A second search was conducted using PICO words [leg elevation OR leg lifting AND spinal anaesthesia OR intrathecal injection AND hypotension OR low blood pressure AND caesarean section OR operational delivery] and a combination of free text words and indexed terms with Boolean operators. All discovered articles’ reference lists were used in the third search to look for new studies. Finally, Google Scholar was used to conduct an extra search for grey literature. All 7 retrieved studies were assessed for inclusion in the systematic literature review based on the eligibility criteria after the duplicates were eliminated using EndNote’s reference manager. Each article’s title and abstract were first reviewed, and any citations that did not fit the inclusion requirements or were only abstracts were removed. The remaining citations’ full texts were acquired and examined. The PRISMA flowchart below provides a summary of the search strategy’s findings (Figure 1).
 |
Figure 1 Prisma Flow chart. |
Data Extraction
Two separate reviewers used a customized Excel sheet to extract the data, and any discrepancies or conflicts were settled through consensus or another method. The information that was gathered from the patient population includes information on their age, place of origin, sample size, study design, year of publication, primary outcome, and complications related to interventions, and length of surgery.
Data Synthesis and Quality Assessment
All the eligible studies were included in the synthesis during the systematic review. P.05 was considered statistically significant for all outcomes. To assess the methodological quality and risk of bias of each included study, the Cochrane Collaboration and ROBIN’s risk of bias assessment tool were used. The tool is used to evaluate the quality of studies in two dimensions: external validity (assessing the target population, sampling frame, and sampling method) and internal validity (assessing the data collection method, case definition, study instrument, and mode of data collection). The risk of bias was evaluated by the researcher.
Critical Appraisal
Using the Cochrane Collaboration’s risk of bias assessment technique for RCT trials, the risk of bias was evaluated.12 By using the ROB tool, which has components for selection bias (random sequence generation and allocation concealment), performance bias (blinding of participants and personnel), detection bias (blinding of outcome assessment), attrition bias (incomplete outcome data), reporting bias (selective reporting), and other bias, the methodological quality of all seven RCT studies was evaluated (as shown in Table 1 below). Our systematic review’s quality was rated as being of a high standard, and it was reported in accordance with AMSTAR 2 criteria.13
 |
Table 1 Risks of Bias Assessments (ROB) |
Result
A total of 8158 items were found using a thorough search approach across various electronic databases. After duplications were eliminated using the EndNote reference manager, 247 articles were chosen for screening; 13 papers were then included for critical evaluation, and 6 articles were discarded with justifications. Seven RCT studies are presented in the selected papers. Among the 7 studies included in the review are 2 from Turkey, 2 from Egypt and 1 each from India, Great Britain, and Ethiopia, respectively. All seven included RCTs were comparative intervention studies between leg elevation and placebo for the prevention of PSH. The PRISMA flow chart includes a list of the study selection procedures. The table below (Table 2) provides an overview of the studies.
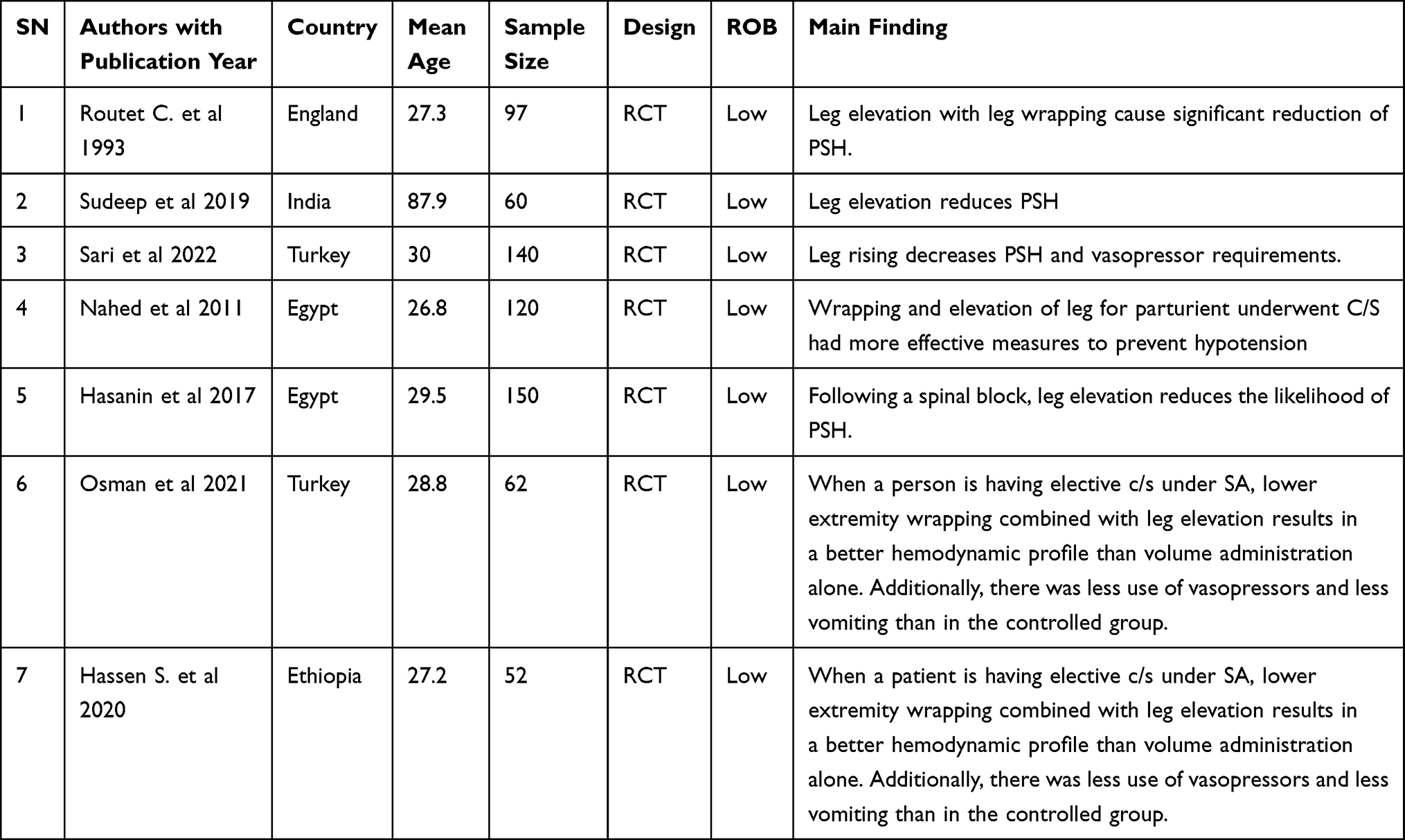 |
Table 2 Description of Included Study in the Review |
Additional Characteristics of the Studies
Most trials were performed in a diverse array of countries, but reports in English were selected for this review: Most of the selected studies used 45-degree leg elevation as the study group compared to placebo (flat supine) during caesarean section delivery under spinal anaesthesia. One study used a level of elevation of 40–45 degrees, while another used a level of elevation of 30 degrees.
Discussion
For elective or emergency Caesarean sections, spinal anaesthesia is frequently chosen. The benefits include ease of use, quick onset, dense motor block, and avoidance of any potential airway issues that could arise from general anaesthesia. The incidence of hypotension following spinal anaesthesia for a Caesarean section is reported to be as high as 80%.14
The primary disadvantage of spinal anaesthesia in patients having elective CS is post-spinal hypotension. The mother is not only put at risk for the negative effects of hypotension due to the drop in blood pressure, but it also causes placental hypoperfusion, which can result in foetal acidosis and, in severe cases, foetal bradycardia and cardiovascular collapse. The principal factor causing the hypotension that follows spinal anaesthesia is the decreased arterial and venous tonus brought on by the sympathetic block.15
Previous research has examined a range of prophylactic measures to counter the hypotension brought on by spinal block. Intravenous fluid administration prior to spinal anaesthesia is one of the most extensively studied strategies for avoiding hypotension. In spite of its questionable effectiveness, fluid management in obstetric anaesthesia is nevertheless often used, according to a new study on the treatment of spinal-induced hypotension in patients scheduled for caesarean delivery.16 Crystalloids may not be sufficient to prevent hypotension during spinal anaesthesia, according to a recent Cochrane analysis. Contrarily, multiple studies have shown that post-spinal hypotension occurs less frequently in women who receive colloids compared to women who receive crystalloids. But the primary goal of conducting this review is to summarize the research on the effectiveness of leg elevation in preventing PSH following a caesarean section.5
The cardiac output and preload are both raised as a result of the auto-transfusion of blood brought on by LE from the lower limbs into the heart. In a prior study using radio-labelled erythrocytes, counts from the radio-labelled intravascular space of the calves after LE were found to be reduced by 34.4%, or roughly 150 mL. We believe that leg elevation, despite the relatively small volume that is transported, is quite effective in reducing the incidence of PSH for two reasons: 1. Receiving a transfusion within a brief time 2: Not being regular fluids and being blood.17,18 Assali and Prystowsky wrote one of the first studies demonstrating the effectiveness of limb elevation. The studies on patients undergoing CS under spinal anaesthesia showed that raising the legs to 90 degrees or wrapping them to keep them out of the systemic circulation could prevent hypotension brought on by spinal blocking.19 According to Pernoll et al, the most effective way to avoid hypotension is to elevate the legs to a straight-up position simultaneously with shifting the left uterus. The volume sensitive to auto transfusion is confined, according to some writers; hence, it cannot significantly change blood pressure.20
The literature contains a very small number of studies on the use of LE in pregnant women. Rout et al initial study on this topic involved 97 pregnant women and was conducted in 1993. In this study, the patients were split into three groups: the control group, the Esmarch bandage group, and the LE group. The incidence of hypotension was observed to be lower in the group wearing an Esmarch bandage than in the control group (15% vs 53%, p = 0.004). Although the incidence of hypotension was lower in the group administered with a 30-degree LR than in the control group (39% vs 53%, p > 0.05), it was not statistically significant. The study was conducted in 1993. In this study, the patients were split into three groups: the control group, the Esmarch bandage group, and the LE group. The incidence of hypotension was observed to be lower in the group wearing an Esmarch bandage than in the control group (15% vs 53%, p = 0.004). Although the incidence of hypotension was lower in the group administered with a 30-degree LR than in the control group (39% vs 53%, p > 0.05), it was not statistically significant.21
Contrary to Rout and the other study by Assen et al 2020, the incidence of hypotension was found to be lower in the group treated with a 45-degree LR in the horizontal plane than the control group (33.3% vs 62.5%, p = 0.02).22 In addition, the experimental group was shown to have a considerably lower incidence of hypotension than the group given a 40-degree LR in the horizontal plane (34.7% vs 58.7%, p = 0.005). This finding is consistent with the findings of the study performed by Hasanin et al23 The incidence of hypotension was lower in the LR group than in the control group in the study by Mustafa Deniz Sari et al, similar to Hasanin and Assen, applying LR at an angle of 30 degrees with the horizontal plane (41.4% vs 77.1%, p = 0.001).24
In contrast to the control group, the leg elevation group had a decreased incidence of post-spinal hypotension. This randomised controlled experiment shows that, with a P value of 0.05, the incidence of post-spinal hypotension is 26 (34.7%) in the leg elevation group and 44 (58.7%) in the control group. Leg elevation reduced relative risk by 40.9% with a 95% confidence interval (CI) of 0.193–0.724, and this study reduced relative risk by 47%, which is statistically significant.25 According to Naheed F.’s study, there was a substantial difference between the groups, with legs (wrapping and elevation) having a higher MAP, a lower percentage of women with late-onset hypotension, and a lower percentage of babies who had poor outcomes. Excellent and similar neonatal outcomes were seen in both groups.14
Sudeep’s study concluded that elevation of the lower limb just after spinal anaesthesia is an effective method to prevent hypotension, as the rate of hypotension in Group A (leg wrapped) is 10%, whereas in Group B (leg not wrapped) it is 66.66%.26 In Osman Asen’s study, systolic, diastolic, and mean blood pressures in the wrapping group were considerably higher than those in the control group from the second minute of intrathecal injection to the 20th–30th minute of intrathecal injection. The control group received a median dose of ephedrine that was considerably larger than the wrapping group [15 (0–40) mg vs 5 (0–30) mg, p = 0.007]. Additionally, control individuals vomited more frequently than those who had their lower extremities wrapped and their legs elevated (18% vs 0%, p = 0.024).17 In general, the pooled effect of this review favours the efficacy of leg elevation in reducing PSH, as only one study found that leg elevation to 30° after spinal anaesthesia reported no significant decrease in the incidence of hypotension, whereas a larger study found a similar numerical reduction in hypotension that reached statistical significance. The LE group showed a lower incidence of PSH (31.4% vs 60.7%, P = 0.005) compared to the control.
Strengths
The prevention of PSH in parturients having elective CS was the emphasis of the current literature included in this review, and nearly all of the studies are randomised control trials with high-quality evidence. This evaluation also discusses various other adjuncts and combined strategies for preventing PSH.
Limitations
A few of the included studies had tiny sample sizes and questionable methodology. There was not sufficient research focusing on obstetric populations, despite the fact that the goal of this review was to assess the usefulness of leg elevation in the prevention of PSH after caesarean section. The majority of research concentrated on prevention via prophylactic administration of several vasopressor medication groups and hydration control. This restricts our review to specifically achieving its goal for the preventative component.
Conclusion
In C/S surgeries, hypotension is unavoidably experienced following spinal anaesthesia. Although it was unable to completely prevent PSH, we discovered that LE application in C/S was useful in lowering the incidence of hypotension. Additionally, this approach reduced the use of vasopressors. Leg raising is a useful, non-invasive technique that needs no special equipment. In a setting with limited resources, it will be helpful in the anaesthetic management of C/S procedures under spinal anaesthesia.
Abbreviations
CS, Cesarean section; PSH, Post- Spinal Hypotension; LE, Leg Elevation; LR, Leg Raise; RCT, Randomized Controlled Trial; SA, Spinal Anesthesia; PRISMA, Preferred Reporting of Systematic Review and Meta-Analysis; ROBINS, Risk of Bias in non-randomized studies.
Disclosure
The authors report no conflicts of interest in this work.
References
1. KlÖHR S, Roth R, Hofmann T, Rossaint R, Heesen M. Definitions of hypotension after spinal anaesthesia for caesarean section: literature search and application to parturients. Acta Anaesthesiol Scand. 2010;54(8):909–921. doi:10.1111/j.1399-6576.2010.02239.x
2. Hyderally H. Complications of spinal anesthesia. Mt Sinai J Med. 2002;69(1–2):55–56.
3. Lee JE, George RB, Habib AS. Spinal-induced hypotension: incidence, mechanisms, prophylaxis, and management: summarizing 20 years of research. Best Pract Res Clin Anaesthesiol. 2017;31(1):57–68. doi:10.1016/j.bpa.2017.01.001
4. Higuchi H, Hirata J-I, Adachi Y, Kazama T. Influence of lumbosacral cerebrospinal fluid density, velocity, and volume on extent and duration of plain bupivacaine spinal anesthesia. J Am Soc Anesthesiol. 2004;100(1):106–114.
5. Chooi C, Cox JJ, Lumb RS, et al. Techniques for preventing hypotension during spinal anaesthesia for caesarean section. Cochrane Database Syst Rev. 2017;8(8). doi:10.1002/14651858.CD002251.pub3
6. Brenck F, Hartmann B, Katzer C, et al. Hypotension after spinal anesthesia for cesarean section: identification of risk factors using an anesthesia information management system. J Clin Monit Comput. 2009;23:85–92. doi:10.1007/s10877-009-9168-x
7. Prashanth A, Chakravarthy M, George A, Mayur R, Hosur R, Pargaonkar S. Sympatho-vagal balance, as quantified by ANSindex, predicts post spinal hypotension and vasopressor requirement in parturients undergoing lower segmental cesarean section: a single blinded prospective observational study. J Clin Monit Comput. 2017;31:805–811. doi:10.1007/s10877-016-9906-9
8. Shaker EH, El Sabeeny WY. Crystalloids versus colloids versus hypertonic saline co-load during spinal anesthesia: which is more effective? Anaesth Pain Intensive Care. 2020;24(3):320–329. doi:10.35975/apic.v24i3.1277
9. Ralston DH, Shnider SM, deLorimier AA. Effects of equipotent ephedrine, metaraminol, mephentermine, and methoxamine on uterine blood flow in the pregnant ewe. J Am Soc Anesthesiol. 1974;1974:1.
10. Xu C, Liu S, Huang Y, Guo X, Xiao H, Qi D. Phenylephrine vs ephedrine in cesarean delivery under spinal anesthesia: a systematic literature review and meta-analysis. Int J Surg. 2018;60:48–59. doi:10.1016/j.ijsu.2018.10.039
11. Caille V, Jabot J, Belliard G, Charron C, Jardin F, Vieillard-Baron A. Hemodynamic effects of passive leg raising: an echocardiographic study in patients with shock. Intensive Care Med. 2008;34:1239–1245. doi:10.1007/s00134-008-1067-y
12. Higgins JP, Altman DG, Gøtzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928–d5928. doi:10.1136/bmj.d5928
13. Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358. doi:10.1136/bmj.j4008
14. Nahed F, Maternity K. Preventive measures to reduce post-spinal anesthesia hypotension for elective cesarean delivery. J Am Sci. 2011;7(2):634–640.
15. Yilkal D. Of hypotension in obstetrics after spinal anesthesia developing country; 2019.
16. Kee WDN. Prevention of maternal hypotension after regional anaesthesia for caesarean section. Curr Opin Anaesthesiol. 2010;23(3):304–309. doi:10.1097/ACO.0b013e328337ffc6
17. Esen O, Balci C, Sargin MA, Erdivanli B. Impact of leg wrapping in combination with leg elevation on postspinal hypotension in subjects undergoing elective cesarean section under spinal anesthesia; 2021.
18. Rutlen DL, Wackers F, Zaret B. Radionuclide assessment of peripheral intravascular capacity: a technique to measure intravascular volume changes in the capacitance circulation in man. Circulation. 1981;64(1):146–152. doi:10.1161/01.CIR.64.1.146
19. Assali N, Prystowsky H. Studies on autonomic blockade. II. Observations on the nature of blood pressure fall with high selective spinal anesthesia in pregnant women. J Clin Invest. 1950;29(10):1367–1375. doi:10.1172/JCI102374
20. Thomas D, Robson S, Redfern N, Hughes D, Boys R. Randomized trial of bolus phenylephrine or ephedrine for maintenance of arterial pressure during spinal anaesthesia for Caesarean section. Br J Anaesth. 1996;76(1):61–65. doi:10.1093/bja/76.1.61
21. Rout C, Rocke D, Gouws E. Leg elevation and wrapping in the prevention of hypotension following spinal anaesthesia for elective caesarean section. Anaesthesia. 1993;48(4):304–308. doi:10.1111/j.1365-2044.1993.tb06948.x
22. Assen S, Jemal B, Tesfaye A. Effectiveness of leg elevation to prevent spinal Anesthesia-induced hypotension during cesarean delivery in the resource-limited area: open randomized controlled trial. Anesthesiol Res Pract. 2020;2020:1–8. doi:10.1155/2020/5014916
23. Hasanin A, Mokhtar AM, Badawy AA, Fouad R. Post-spinal anesthesia hypotension during cesarean delivery, a review article. Egypt J Anaesth. 2017;33(2):189–193. doi:10.1016/j.egja.2017.03.003
24. Sari MD, Ozyurt E. Does leg raising prevent spinal-induced hypotension in elective cesarean sections? A randomized controlled study. J Anesth. 2022;30(3):1.
25. Hasanin A, Aiyad A, Elsakka A, et al. Leg elevation decreases the incidence of post-spinal hypotension in cesarean section: a randomized controlled trial. BMC Anesthesiol. 2017;17:1–6. doi:10.1186/s12871-017-0349-8
26. Singh K, Payal Y, Sharma J, Nautiyal R. Evaluation of hemodynamic changes after leg wrapping in elective cesarean section under spinal anesthesia. Int J Obstet Anesth Crit Care. 2014;4(1):23. doi:10.4103/2249-4472.132818
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.