")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Effect of Comprehensive Nursing on Pain Relief, Comfort and Burden of Family Care of Infantile Anal Fistula
Authors Wei Y, Wang YZ, Li Y, Liu L, Sui TT, Li Y
Received 27 September 2023
Accepted for publication 10 January 2024
Published 12 February 2024 Volume 2024:17 Pages 641—648
DOI https://doi.org/10.2147/JMDH.S442306
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ying Wei,1 Yan-Zhi Wang,2 Ying Li,1 Ling Liu,1 Ting-Ting Sui,2 Yuan Li1
1Department II of Anorectal Department, China-Japan Friendship Hospital, Beijing, 100029, People’s Republic of China; 2Department I of Anorectal Department, China-Japan Friendship Hospital, Beijing, 100029, People’s Republic of China
Correspondence: Ying Wei, Department II of Anorectal Department, China-Japan Friendship Hospital, No. 2, Sakura East Street, Chaoyang District, Beijing, 100029, People’s Republic of China, Tel +86-01053236548, Email [email protected]
Objective: To explore the effect of comprehensive nursing on pain relief, comfort and burden of family care of infantile anal fistula.
Methods: This was a randomized, double-blind, controlled clinical trial. A total of 106 cases of children with anal fistula from January 2021 to December 2021 were selected and divided into observation group and control group, there were 53 cases in each group. The control group were underwent with routine nursing intervention. The observation group were underwent with video health education, peer support, music relaxation training, physiotherapy and auricular point pressing on the basis of routine nursing therapy and other measures (comprehensive nursing). The wound healing time, comfort score, complication rate and family care burden of two groups were compared.
Results: After intervention, the scores of pain degree in the observation group were significantly lower than those in the control group (4.02 ± 0.85 vs 5.89 ± 2.36, p < 0.05), and the scores of comfort degree in the observation group were higher than those in the control group (70.23 ± 5.98 vs 46.88 ± 5.23, p < 0.05). After intervention, the wound healing time of the observation group was shorter than that of the control group (3.98 ± 0.63 vs 5.77 ± 1.02, p < 0.05), and the crying times of the observation group were less than that of the control group (1.22 ± 0.26 vs 4.02 ± 0.48, p < 0.05). After intervention, the total scores of family members’ care load in the observation group were significantly lower than those in the control group (37.26 ± 4.78 vs 55.99 ± 5.02, p < 0.05).
Conclusion: Comprehensive nursing can effectively promote wound healing in infantile anal fistula, reduce pain, prompt children’s comfort, reduce the number of children crying, and reduce the burden of care for children’s families.
Keywords: comprehensive nursing, infantile anal fistula, comfort, complications, family care burden
Introduction
Infantile anal fistula, a common acute purulent infection disease in childhood, is caused by the spread of the anal gland to the anorectal tissue after being infected by pathogenic bacteria.1 Characterized by acute onset, rapid progression, and spontaneous rupture, the disease puts children at risk of persistent anal fever, pain, and insomnia. If effective intervention is not available, it may progress to sepsis or septicemia, which will seriously threaten the life of children.2
In view of the rupture of tissues around the anus caused by infantile anal fistula and the resulting wound pain, children suffering from persistent pain will cry and resist treatment due to their young age and poor pain tolerance, which increases the care burden of their families.3 If effective measures are taken to reduce the pain of children, the adverse effects of pain on their bodies can not only be reduced, but also their comfort can be improved. This results in reduced crying frequency, improved treatment cooperation, and accelerated rehabilitation of children.4
On the basis of evidence-based nursing, comprehensive nursing, a high-quality nursing service, is developed to address clinical pain problems.5 There have been previous studies on the application of comprehensive nursing intervention in patients with hip replacement,6 hepatitis B,7 etc., all of which have proven the ideal analgesic effect of this intervention. However, there is no relevant report about whether comprehensive nursing can alleviate pain in children with infantile anal fistula and improve their comfort. Comprehensive nursing is based on routine nursing, more standardized and reasonable targeted services for patients, fundamentally improve the quality of nursing. The intervention measure of this study - comprehensive nursing, is based on the routine nursing treatment of video health education, peer support, music relaxation training, physical therapy and auricular acupoint compression and other measures. By comparing the effects of comprehensive nursing and routine nursing on pain relief, comfort and family nursing burden of children with anal fistula, this study aims to explore better intervention methods and provide guidance for clinical nursing of children with anal fistula.
Materials and Methods
Clinical Data
A randomized, double-blind, controlled clinical trial was designed. One hundred and six children with infantile anal fistula admitted from January 2021 to December 2021 were recruited. The inclusion criteria were as follows: ① children who met the diagnostic criteria for infantile anal fistula in the “Consensus of Chinese Experts on the Diagnosis and Treatment of Anal Fistula”;8 ② those who were clearly diagnosed as infantile anal fistula by extrusion method and anoscopy; ③ those aged 6 months to 6 years; and ④ parents or legal guardians of children with knowledge and consent to the specific matters of this study, and signed the informed consent. The exclusion criteria were as follows: ① children with tuberculous anal fistula; ② those with other anal or rectal diseases; ③ patients who dropped out for various reasons. All recruited children were divided into two groups using a random number table: the observation group and the control group, with 53 cases in each group.
Methods
Conventional Nursing (Control Group)
Patients included in the control group will receive conventional nursing after admission, which mainly includes health education, defecation guidance, urination guidance and dressing change nursing. Specific implementation measures are as follows:
(1) Health education: After admission, knowledge education on infantile anal fistula was conducted for children and their families by the primary nurses, who were asked to avoid pressing the wound while assisting the children to turn over.
(2) Defecation guidance: The family members were instructed to prepare honey water for the children every morning, add fruit paste for supplementary food, and massage the abdomen of the children to promote defecation and avoid them eating cold, irritating and spicy food.
(3) Urination guidance: A warm water bag was placed on the abdomen of the children, and the bottom and anterior wall of their bladder were gently massaged to relax the urethral sphincter and relieve the spasm of the bladder sphincter.
(4) Dressing change nursing: Dressing change was strictly carried out according to the steps of defecation–sitz bath–microwave therapy–dressing change, etc. Before taking a sitz bath, the children’s wounds were cleaned by the primary nurses, and the sitz bath temperature was adjusted to about 35°C. Afterwards, the wounds were deeply flushed with metronidazole and hydrogen peroxide, the granulation tissue that grew higher than the surface of the wounds was trimmed, and the dressing was changed gently.
Comprehensive Nursing (Observation Group)
A pain intervention team was formed by the head nurse and three nurses with experience in anorectal care. The head nurse shall supervise and correct any errors; Organize nursing training regularly, and nursing staff should conduct standardized perianal training once every six months. They were responsible for consulting domestic and foreign literature, collecting relevant information and formulating comprehensive intervention measures. Comprehensive nursing is an addition to conventional nursing. Video health education, peer support, music relaxation training, physiotherapy and auricular point pressing therapy were used to care patients in the observation group. The specific measures were as follows:
(1) Video health education: After admission, centralized video health education was organized for the children and their families by the primary nurses so that the children and their families could watch videos related to the treatment of infantile anal fistula. The content of the video included the causes, treatment methods, prognosis scenarios, precautions during treatment, pain management methods and so on. The video education lasted for 30 min. After watching the video, the primary nurses asked the children and their families questions and gave small gifts to those who answered correctly as a token of encouragement.
(2) Peer support: During hospitalization, children who had been treated for infantile anal fistula in our hospital and had an ideal prognosis, together with their family members, were invited to the ward by the primary nurses to make a presentation for the children, and encouraged the children to actively cooperate with the treatment. Meanwhile, they explained to the children about the relevant countermeasures when the pain occurred, in order to enhance the children’s ability to cope with the disease.
(3) Music relaxation training: A quiet and comfortable conference room was selected as the intervention place. Under the guidance of the primary nurses, the children were placed in a supine position, and soft music with a soothing rhythm was played for them. The soft language was used to guide the children to meditate, imagining that they were on the vast grassland and feeling the breath of nature. Besides, the children were instructed to adjust their breathing in order to meditate on running on the grassland after recovery and were encouraged to express their inner feelings at the moment. This method was followed for 20 min every day.
(4) Physiotherapy: The family members of the children were instructed to apply hot compresses on the perianal area of the children with dried lemon towels soaked in warm water at 35–40°C every morning, noon and evening to reduce the pain and swelling of the children.
(5) Auricular point pressing therapy:9 The children were placed in a supine or seated position with their heads tilted to one side, and their skin area to be operated on was cleaned with a wet towel. Shenmen point, sympathetic point, anus point, rectum point, subcortical point, etc. were selected as the main points, and lung, liver and spleen were selected as the matching points. After the acupuncture points were determined, auricular plaster therapy was performed. A piece of tape was cut into squares of about 0.5 cm × 0.5 cm, and the vaccaria seed was placed in the center. The auricle was fixed with one hand, and with the other hand, the tape with the vaccaria seeds on it was aligned with the relevant acupuncture points and pressed. When pressing, the pressing force was adjusted according to the children’s own feelings, the family members of the children were instructed to press 3 to 5 times when the children felt obvious pain, and each acupoint was pressed for 30s/time. The pressing force was appropriate for the children to feel local acid swelling pain, and the above operations were carried out alternately on the two ears. The tape was replaced every 3 days to prevent it from getting wet during the indwelling period.
Observation Indicators
The two groups were compared in terms of wound healing time, comfort score, daily crying frequency, pain score and family care burden. (1) The wound healing time is the time required for the wound to grow from ulcer to granulation. (2) Comfort score: Kolcaba’s General Comfort Questionnaire (GCQ)10 was used to evaluate patients’ comfort. The questionnaire involves four dimensions, including physiology, environment, psychology and social culture, with a total of 28 items. Each item was assigned 1–4 points, and the total score was 28–112 points, with a higher score indicating greater patient comfort. (3) Crying frequency per day: each crying is defined as continuous crying for more than 1 min. (4) Pain score: The Children’s Visual Analogue Scale11 was used for pain evaluation. The total score of the scale was 0–10 points, with a higher score indicating more obvious pain. (5) Family care burden: The Zarit Caregiver Burden Inventory (ZBI)12 was applied to evaluate family care burden. The scale includes five aspects of caregivers’ health status (5 items), economic conditions (5 items), mental state (4 items), relationship with patients (4 items) and social life (4 items), with a total of 22 items. Each aspect was assigned a score of 0 to 4, with a total score of 0 to 88, with a higher score indicating a heavier caregiver load. The Cronbach’s α coefficient of the scale was 0.812–0.869, and the reliability coefficient was 0.822–0.869, indicating ideal scale reliability and validity.
Evaluation Method
The wound healing time and daily crying frequency of the two groups were recorded by the primary nurses. The pain degree, comfort degree and care burden of the two groups were evaluated by questionnaire in the children’s ward before and after the intervention. Prior to the investigation, the investigation purpose and matters needing attention were explained to the children’s family members to mobilize their enthusiasm for participating in the investigation. During the study period, 106 questionnaires were sent out and all were effectively recovered, with a total recovery rate of 100%.
Quality Control
For a scientific, reliable and valid study, a random number table was used to divide the recruited children into the experimental group and the control group to reduce systematic bias between the two groups. When we included the study samples, clear inclusion and exclusion criteria were adopted to ensure the consistency of the subjects. Clinical experimenters, raters and subjects were not aware of their treatment group status. In addition, the data collection process was carried out by trained primary nurses to ensure the consistency and accuracy of the data.
Statistical Analysis
SPSS 21.0 was used to make a statistical analysis of the data in this study. The measurement data was tested for normality. If normality was met, it was expressed as mean ± standard deviation ( ), otherwise, it was expressed as the median and interquartile range (M, P25–P75). Counting data was expressed as the number of cases and percentages (n, %). T test was utilized to compare the measurement data between groups, and χ2 test was employed to compare the counting data between groups. A P value < 0.05 indicates a statistically significant difference.
), otherwise, it was expressed as the median and interquartile range (M, P25–P75). Counting data was expressed as the number of cases and percentages (n, %). T test was utilized to compare the measurement data between groups, and χ2 test was employed to compare the counting data between groups. A P value < 0.05 indicates a statistically significant difference.
Results
Basic Information of the Two Groups
In the observation group, there were 28 male children and 25 female children, aged 6 months to 6 years old, with an average of (3.89±0.78) years; The course of disease was 2–12 d, with an average of (6.42±1.12) d; The types of space abscess included 24 cases of low infantile anal fistula, 16 cases of ischiorectal space abscess, 10 cases of postanorectal space abscess and 3 cases of pelvic and rectal space abscess. In the control group, there were 27 male children and 26 female children, aged 6 months to 6 years old, with an average age of (3.92±0.87) years; The course of the disease was 2–10 d, with an average of (6.62±1.08) d; The types of space abscess included 23 cases of low infantile anal fistula, 17 cases of ischiorectal space abscess, 8 cases of postanorectal space abscess and 5 cases of pelvic and rectal space abscess. No significant statistical significance was observed in the clinical data of the two groups (P > 0.05), which was comparable. See Table 1 for details.
 |
Table 1 Basic Information of the Two Groups |
Comparison of Pain Degree Scores and Comfort Degree Scores Between the Two Groups Before and After the Intervention
Before the intervention, no significant statistical significance was observed in the pain degree scores of the observation group and the control group (7.98±1.20 vs 8.02±1.85, P = 0.895), while after the intervention, the pain degree scores of the observation group were significantly lower than those of the control group (4.02±0.85 vs 5.89±2.36, P < 0.05). Before the intervention, no statistical significance was observed in the comfort degree scores of the observation group and the control group (38.25±4.98 vs 38.69±4.75, P = 0.642), while after the intervention, the comfort degree scores of the observation group were significantly higher than those of the control group (70.23±5.98 vs 46.88±5.23, P < 0.05). See Table 2 for details.
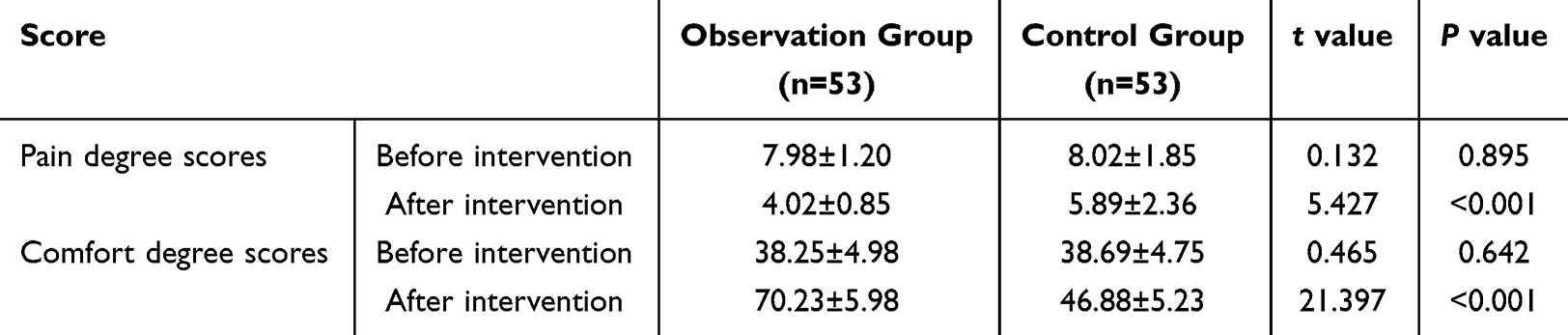 |
Table 2 Comparison of Pain Degree Scores and Comfort Degree Scores Between the Two Groups Before and After the Intervention ( |

Comparison of Wound Healing Time and Daily Crying Frequency Between the Two Groups
After the intervention, the wound healing time and the daily crying frequency were evaluated. The results showed that the wound healing time in the observation group was shorter than that in the control group (3.98±0.63 vs 5.77±1.02, P < 0.05), and the daily crying frequency in the observation group was less than that in the control group (1.22±0.26 vs 4.02±0.48, P < 0.05). See Table 3 for details.
 |
Table 3 Comparison of Wound Healing Time and Daily Crying Frequency Between the Two Groups ( |

Comparison of Care Burden Scores of Children’s Family Members Between the Two Groups
Before the intervention, no significant statistical significance was observed between the observation group and the control group in terms of the five dimensions, namely, family members’ health status, economic conditions, mental state, relationship with patients and social life (P > 0.05), and the total score of family members’ care burden between the two groups was not significantly different (70.37±5.98 vs 69.98±6.12, P = 0.741). After the intervention, no significant statistical significance was observed between the observation group and the control group in terms of the five dimensions of family members’ care burden (P < 0.05), and the total score of family members’ care burden in the observation group was significantly lower than that in the control group (37.26±4.78 vs 55.99±5.02, P < 0.05). See Table 4 for details.
 |
Table 4 Comparison of Care Burden Scores of Children’s Family Members Between the Two Groups ( |

Discussion
Infantile anal fistula, one of the common diseases in anorectal department, causes perianal tissue ulcers and ulceration, resulting in obvious pain in children. Children suffering from infantile anal fistula are prone to crying, anxiety, depression and other emotions during treatment due to their young age and poor pain tolerance. Thus, it affects the degree of cooperation and rehabilitation of children in treatment, and increases the care burden of their families.13 For this reason, reasonable and effective nursing measures need to be adopted to assist in the treatment process. Comprehensive nursing intervention measures play a significant role in improving the nursing effect. Comprehensive nursing intervention is a measure based on conventional nursing that strengthens intervention in the aspects of observation and targeted treatment of children’s condition, maintenance of inpatient environment, health education, psychological counseling, dietary guidance, discharge guidance, etc., aiming to ensure more comprehensive nursing. It can effectively alleviate the pain of children with infantile anal fistula, improve their comfort, soothe their crying mood, and reduce the care burden for their families.
To relieve the pain of children with infantile anal fistula, comprehensive nursing measures were implemented in this study on the basis of evidence-based theory. The results showed that the comfort scores of the observation group were significantly higher than that of the control group after the intervention (P < 0.05), indicating the prominent role of comprehensive nursing in effectively reducing the pain of children with anal fistula and soothing their negative emotions. Previous studies have pointed out14 that negative emotions are the source of stress response, which will lead to an increase in the excitability of the sympathetic–adrenal medulla–hypothalamus–pituitary–adrenocortical axis. As a result, the body secretes a large amount of catecholamines and epinephrine, which increases the pain of children. In response to this, health education, peer support, and music relaxation for children in the comprehensive nursing can effectively reduce anxiety and depression in children, thus achieving an analgesic effect.15 There are three reasons for this. First, health education can improve children’s cognition of diseases and reduce the negative emotions caused by wrong cognition; Secondly, peer support provides children with a better understanding of the disease, enhances their confidence in dealing with it, and reduces their anxiety and fear when facing it; Finally, music relaxation therapy can effectively divert children’s attention, avoid them from paying too much attention to the impact of pain on the body, and alleviate their pain.16 In addition to placing a high premium on the influence of the psychological state on pain, a series of measures were also taken in this study to reduce the influence of physiological factors on children. For example, hot compress around the anus can relax the blood vessels around the anus and reduce the pain caused by perianal edema.17 Auricular plaster therapy, a traditional Chinese medicine syndrome differentiation nursing therapy, plays the role of relieving pain and stopping bleeding, promoting the flow of qi and blood circulation, tranquilization and sedation by pressing acupoints such as subcortical point, sympathetic point, Shenmen point, anus points, and rectum points, thus effectively alleviating the pain of children and relieving local swelling. It can effectively alleviate the pain of children, improve their comfort, and prevent them from crying and uncooperative treatment due to physical discomfort, thereby reducing the care burden of their families.18,19 Acupoint stimulation is an auxiliary therapy that originated in ancient China and is based on the theory of main lateral channel.20 It has been regarded by the World Health Organization (WHO) as an effective intervention to deal with various health issues.21 The mechanism of intervention can be explained by institutional function. In the human ear, there are multipotent cells that contain information for the entire body, and in the auricle area, the innervation and blood supply of the viscera. This part of the body has relationships with energy meridians, organs and internal organs according to Chinese medicine theory.22 Research by Corrêa et al pointed out that auricular therapy can be applied clinically by trained nurses to provide effective auxiliary treatment.23
Comprehensive nursing is a nursing mode that centers on the health needs of people and communities and provides patients with holistic options. Rohwer et al emphasized that comprehensive nursing is cost-effective.24 It was shown in this study that the wound healing time of the observation group was shorter than that of the control group, and the daily crying frequency was also less than that of the control group, fully demonstrating that comprehensive nursing with the modern nursing service concept of “people-oriented” as the core can improve the clinical treatment effect through comprehensive intervention. Cui et al also pointed out that comprehensive nursing intervention is beneficial to improving symptoms and nutritional status, controlling the incidence of malnutrition, reducing anxiety and depression, and assisting surgery.25
Nonetheless, there are some limitations in this study. First of all, insufficient samples are included in this study, which may lead to biased statistical analysis results. Secondly, the single-center design is adopted in this study, and the promotion scope of the findings may be limited by geographical and institutional particularities. Moreover, the assessment of family members’ care burden after infantile anal fistula surgery mainly relies on questionnaires, which may be affected by the subjective factors of the respondents.
Conclusion
To sum up, comprehensive nursing can effectively promote wound healing, relieve pain, improve comfort in children with anal fistula, reduce crying frequency and relieve the care burden for family members. Comprehensive nursing plays a positive role in improving the comfort of infantile anal fistula and reducing the burden of family care. In the future, medical institutions can provide comprehensive nursing for children by adjusting nursing plans, so as to achieve more ideal therapeutic effects and reduce the burden on their family members.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of China-Japan Friendship Hospital.
Written informed consent was obtained from all participants’ parent or legal guardian.
Funding
This study did not receive any funding in any form.
Disclosure
All of the authors had no any personal, financial, commercial, or academic conflicts of interest separately.
References
1. Ding W, Sun YR, Wu ZJ. Treatment of perianal abscess and fistula in infants and young children: from basic etiology to clinical features. Am Surg. 2021;87(6):927–932. doi:10.1177/0003134820954829
2. Sun Y, Hao S, Zhang X, et al. A systematic review and meta-analysis of comparing drainage alone versus drainage with primary fistula treatment for the perianal abscess in children. Eur J Pediatr Surg. 2023. doi:10.1055/a-2070-3613
3. Qiang Z, Jingen L, Hongtao L. Advance in the diagnosis and treatment of anal abscess and anal fistula of infants. Chin Med Herald. 2018;15(16):34–37.
4. Jun L, Rong Y, Yun’e Z. Effect of entire nursing intervention on patients undergoing one-time radical surgery of infantile anal fistula. Journal of Qilu Nursing. 2020;26(4):110–113.
5. Hopman P, de Bruin SR, Forjaz MJ, et al. Effectiveness of comprehensive care programs for patients with multiple chronic conditions or frailty: a systematic literature review. Health Policy. 2016;120(7):818–832. doi:10.1016/j.healthpol
6. Cun Z. Construction of Evidence-Based Nursing for Pain Assessment of Patients Undergoing Total Hip Replacement. Lanzhou University; 2020.
7. Chen F, Pang X, Dai X. Effect of comprehensive nursing on the pain, anxiety and malnutrition of hepatitis B patients. Am J Transl Res. 2021;13(5):4656–4665.
8. Zhongdai DU, Yingxiang J, Li X, et al. Exchange of clinical experience in anal abscess and fistula of infants. Chin J Surg Inte Trad West Med. 2020;26(6):1174–1176.
9. Morais BX, Ongaro JD, Almeida FO, et al. Auriculotherapy and reducing chronic musculoskeletal pain: integrative review. Rev Bras Enferm. 2020;73(s6):e20190394. doi:10.1590/0034-7167-2019-0394
10. Suhong L, Xuehui H, Rongqin L. Kolcaba K’s comfort theory and its practical application. Hebei Medl J. 2012;34(21):3312–3314.
11. Lin Z, Xianlan Z, Qiao S, et al. Research progress of children’s pain assessment. Chin Gen Pract. 2019;17(25):3098–3101.
12. Rui Z, Qiongling L, Xiangzhi C. Research progress on care load of caregivers of chronic diseases. J Guang Med Coll. 2014;32(2):239–241.
13. Jinghua W, Xiuhong L, Bin Z, et al. Comparative the children’s postoperative pain nursing score and the self-assessed results of resting pain and active pain. Nurs Prac Res. 2020;17(10):104–106.
14. Yimei H, Wang Q, Jie Z, et al. Application of multi-mode preemptive analgesia in the perioperative care of children with knee arthroscopy. Chin Gen Pract. 2020;18(23):3024–3028.
15. Feng W, Rong Y, Lihong L, et al. Effects of evidence-based problems nursing model on rehabilitation and psychological status of patients with perianal abscess after operation. Med Innova China. 2020;17(31):96–100.
16. Huifei C, Meiling Z. Effect of comprehensive intervention on relieving wound pain and dressing change pain after perianal surgery. Zhejiang J Trauma Sur. 2017;22(2):407–408.
17. Wenting Z, Xiaona S. Effect of comfort nursing intervention on alleviating postoperative pain of patient with crissum abscess. J Clinical Nur Prac. 2017;3(4):38–40.
18. Jing L, Minhui K, Yuxiu C. Analysis of the effect of TCM pain nursing on improving the quality of life of patients with infantile anal fistula. Fujian Med J. 2018;40(6):164–166.
19. Ying X. Effect of pain nursing on dressing change after anorectal surger. Guide Chin Med. 2019;17(4):174–175.
20. Tao WW, Jiang H, Tao XM, et al. Effects of acupuncture, tuina, tai chi, qigong, and traditional Chinese medicine five-element music therapy on symptom management and quality of life for cancer patients: a meta-analysis. J Pain Symptom Manage. 2016;51(4):728–747. doi:10.1016/j.jpainsymman
21. Wei W, Huang X, Zhu J. Effect of acupoint therapies on postoperative sleep quality: a narrative review. Med Sci Monit. 2023;10(29):e938920. doi:10.12659/MSM.938920
22. Vieira A, Hinzmann M, Silva K, et al. Clinical effect of auricular acupuncture in anxiety levels of students prior to the exams: a randomized controlled trial. Eur J Int Med. 2018;20:188–192. doi:10.1016/j.eujim.2018.05.012
23. Corrêa HP, Moura CC, Azevedo C, et al. Effects of auriculotherapy on stress, anxiety and depression in adults and older adults: a systematic review. Rev Esc Enferm USP. 2020;54:e03626. doi:10.1590/S1980-220X2019006703626
24. Rohwer A, Toews I, Uwimana-Nicol J, et al. Models of integrated care for multi-morbidity assessed in systematic reviews: a scoping review. BMC Health Serv Res. 2023;23(1):894. doi:10.1186/s12913-023-09894-7
25. Cui X, Shan T, Qiao L. Effect of self-transcendence theory combined with comprehensive nursing intervention under tumor nutrition education on symptom improvement, nutritional status, and positive psychology of elderly patients with gastric cancer. Contra Media Mol Imaging. 2022;2022:6084732. doi:10.1155/2022/6084732
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.