")
Back to Journals » Clinical Ophthalmology » Volume 16
Early Outcomes of Two Treatment Modes of PresbyLASIK: Monocular vs. Micro-Monovision
Authors Agarwal S, Thornell E
Received 1 August 2022
Accepted for publication 19 September 2022
Published 1 November 2022 Volume 2022:16 Pages 3597—3606
DOI https://doi.org/10.2147/OPTH.S384553
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Smita Agarwal,1,2 Erin Thornell1
1Wollongong Eye Specialists, Wollongong, Australia; 2Graduate School of Medicine, University of Wollongong, Wollongong, Australia
Correspondence: Erin Thornell, Tel +61 2 4223 6388, Fax +61 2 4263 0511, Email [email protected]
Purpose: To report the visual, refractive and subjective outcomes of presbyLASIK for the correction of presbyopia.
Methods: Monocular (20 eyes) or micro-monovision (12 eyes) presbyLASIK was performed on a total of 32 eyes in 16 patients (50% female, average age 55± 4.6 years) using the Zeiss VisuMax 400Hz femtosecond and Schwind Amaris 1050RS excimer laser platform. Predictability, safety and efficacy were assessed and compared at 4– 6 weeks, 3 months and 6 months. Results were considered significant if P < 0.05.
Results: For monocular treatments, average postoperative spherical equivalent (SE) was 0.1± 0.1 D and − 0.86± 0.5 D at 4– 6 weeks postoperatively for distance and near eyes respectively; 90% eyes achieved SE ± 1.0 D of the target. Postoperative binocular uncorrected distance (UDVA), intermediate (UIVA) and near visual acuity (UNVA) were − 0.03± 0.1 LogMAR (20/20), 0.09± 0.26 LogMAR (N4) and 0.29± 0.11 LogMAR (N6) respectively with 90% patients achieving binocular UDVA of 20/20 or better. For micro-monovision treatments, average postoperative SE was − 0.33± 0.51 D and − 1.60± 0.78 D at 4– 6 weeks postoperatively for distance and near eyes respectively; 100% eyes achieved SE ± 1.0 D of the target. Postoperative binocular UDVA, UIVA and UNVA were 0.05± 0.16 LogMAR (20/20), − 0.02± 0.10 LogMAR (N3) and 0.23± 0.08 LogMAR (N5) respectively with 67% patients achieving binocular UDVA of 20/20 or better.
Conclusion: Monocular and micro-monovision presbyLASIK are both effective options for the treatment of presbyopia. Monocular treatments are more likely to be well tolerated by patients who prefer to preserve exceptional distance vision, while micro-monovision treatments may be better suited to patients who can tolerate compromises in distance vision in order to attain greater intermediate vision function.
Keywords: refractive surgery, presbyopia, presbyLASIK
Introduction
There is predicted to be 1.782 billion presbyopes globally by 2050.1 High demand for spectacle independence has led to surgical technologies that can correct refractive error while simultaneously adding depth of focus (DOF) to partially restore near and intermediate vision.
PresbyLASIK is a refractive laser procedure developed to treat presbyopia. Similar to conventional laser in situ keratomileusis (LASIK), the procedure involves cutting a flap and reshaping the underlying stromal tissue to correct refractive errors. To improve functional vision in the near to intermediate range, the non-dominant eye is corrected for an intermediate vision target (i.e., micro-monovision), and spherical aberration (SA) is introduced to steepen the central cornea and extend DOF into the intermediate vision range. This essentially forms a bi-aspheric multifocal cornea whereby the central cornea is optimised for near vision and the peri-central cornea for distance vision with a transition zone in between that provides intermediate vision.
The presbyMAX treatment system developed by Schwind offers three treatment options; monocular, micro-monovision and hybrid which differ in the amount of DOF (i.e., amount of SA) induced in each eye and therefore preserves distance, near or intermediate vision respectively. Characteristics of monocular and micro-monovision treatment modes are described in Table 1. Briefly, both treatment groups receive similar refractive targets, i.e., a distance target (generally plano) in their dominant eye and an intermediate target (e.g., −1.5 D) in their non-dominant eye, but differing amounts of ADD power, or DOF. DOF is calculated using an algorithm built in to the PresbyMAX software. For monocular treatments, distance-corrected eyes receive no added DOF and the near-corrected eye receives 0.9 D DOF. For micro-monovision treatments, both the distance- and near-corrected eyes receive 0.9 D DOF. Monocular treatments therefore retain exceptional distance vision while micro-monovision compromises some distance vision to restore some functional intermediate vision. The mode of treatment is selected based on patient preference and lifestyle.
 |
Table 1 Description of Treatment Patterns of presbyLASIK |
PresbyMAX has been reported to be a safe, reliable and predictable treatment for presbyopia.2,3 Reversal of a presbyMAX treatment to remove induced multifocality in the case of intolerance of ametropia has been reported,4 although long term data is scarce due to the low incidence of reversal. While some studies have reported regression resulting from central corneal flattening and latent hyperopia,5–7 long term results of presbyLASIK appear stable although data is scarce. Studies of visual quality have previously relied on objective data and have reported a transient loss in image quality as measured by objective scattering index (OSI) and modulation transfer function (MTF).8 Subjective visual quality following presbyMAX presbyLASIK has been poorly reported. This study compares postoperative results achieved by monocular and micro-monovision presbyLASIK in a group of 16 patients with a focus on subjective quality of vision.
Materials and Methods
This retrospective cohort study reports refractive, visual and subjective outcomes of presbyLASIK performed at a private refractive surgical clinic on the South Coast of NSW, Australia, for the treatment of presbyopia. This study was conducted according to the tenets of the Declaration of Helsinki. Ethics approval was not required as per University of Wollongong HREC recommendations due to the retrospective nature of the study. Patient data was anonymised and kept confidential.
Screening and Patient Selection
Retrospective analysis was performed on 32 eyes from 16 patients that had undergone either monocular (20 eyes) or micro-monovision (12 eyes) presbyLASIK (50% female, average age 55±4.6 years) between January 1st and December 31st, 2019 at a private refractive clinic on the South Coast of NSW, Australia.
Patients were screened preoperatively to determine suitability for presbyLASIK and were deemed suitable if their photopic pupil was 2.5–3.5 mm and their scotopic pupil was >4.5 mm, if their thinnest corneal thickness was >500 micron, and their preoperative refraction was < ±2.5 D sphere and < ±1.5 D cylinder. Topography (Pentacam HR; Oculus; Irvine, USA) and macular optical coherence tomography (OCT; Cirrus HD 500; Zeiss; Oberkochen, Germany) were performed to exclude the presence of corneal or retinal pathology. Dominance was determined using the hole test and tolerance to monovision was tested using trial frames with their distance correction and either +1.5 D or +1.75 D ADD in their non-dominant eye. Near ADD selection was based on the patient’s lifestyle and visual expectations. Patients were assigned to a treatment group, i.e., monocular or micro-monovision treatment group, according to their lifestyle preferences and expectations; patients were assigned to the monocular group if they did not want any compromise in distance vision and the micro-monovision group if they could tolerate compromising distance vision in order to have better near vision. Patients were excluded from the study if they had concomitant ocular pathologies that may affect visual outcomes or history of prior kerato-refractive procedures. Informed written consent was received before commencing any procedure.
Procedure
Keratoscopy and aberrometry (Peramis; Schwind; Kleinostheim, Germany) were performed preoperatively under mesopic conditions and asymmetric monocular or micro-monovision presbyLASIK treatments were planned using the PresbyMAX module of the CAM Amaris software (Schwind; Kleinostheim, Germany). Briefly, both treatment groups received a plano±0.25 D target in their dominant eye and either −1.0 to −1.5 D in their non-dominant eye depending on their tolerance of anisotropia. DOF was calculated automatically using an algorithm built in to the PresbyMAX software. For monocular treatments, distance-corrected eyes received no added DOF and near-corrected eyes received 0.9 D DOF. For micro-monovision treatments, both the distance- and near-corrected eyes received 0.9 D DOF. All surgeries were performed by one surgeon (SA) at a single site.
Patients were advised to commence lubricating eye drops (Systane PF; Alcon; Geneva, Switzerland) QID for 7 days prior to surgery and to use 0.1% dexamethasone (Maxidex; Alcon; Geneva, Switzerland) and ofloxacin (Ocuflox; Allergan; Irvine, USA) drops from the morning of surgery, using 1 drop of each in each eye twice. Flaps were created centered on the visual axis using the VisuMax 400 Hz femtosecond laser (Carl Zeiss; Oberkochen, Germany) with the following settings: flap thickness of 120 micron, flap diameter of 7.9 mm, hinge position at 90° (superior), side cut angulation of 90°, energy offset of 34 for the flap and side cut, track distance of 4.2 micron for the flap and 2.0 micron for the flap cut, and spot distance of 4.2 micron for the flap and 2.0 micron for the side cut. Treatment was performed using a Schwind Amaris 1050RS excimer laser (Schwind; Kleinostheim, Germany) using optical zones between 6.5 and 6.8 mm according to scotopic pupil size. A refractive target of plano±0.25 DS was used for distance (dominant) eyes and −1.0 to −1.5 DS was used for near (non-dominant) eyes after assessing them preoperatively for their visual needs and acceptance. Following treatment, one drop each of 0.1% dexamethasone (Maxidex; Alcon; Geneva, Switzerland) and ofloxacin (Ocuflox; Allergan; Irvine, USA) and a bandage contact lens (BCL) was applied to each eye to help reduce postoperative pain and discomfort, and to aid in healing of the flap. The BCL was removed 1 day following surgery and patients were advised to use 0.1% dexamethasone (Maxidex; Alcon; Geneva, Switzerland) and ofloxacin (Ocuflox; Allergan; Irvine, USA) drops QID for 1 week and TDS for another week, and lubricating drops QID for 3 months.
Postoperative Follow Up and Statistics
Predictability, safety and efficacy were assessed and compared at 4–6 weeks, 3 months and 6 months, and spectacle independence at 3 months following surgery.
Monocular and binocular UDVA was measured using a Snellen chart (VistaVision) at 6 metres, and UIVA and UNVA were measured using a near vision chart (Sussex Vision) at 1 metre and 40 cm respectively under photopic conditions (i.e., clinical setting with the room light on). Low light vision was measured using the same charts and distances under mesopic lighting (i.e., clinical setting with the room light off). Corrected binocular contrast sensitivity (CS) was measured using a Pelli Robson chart (VistaVision) under mesopic conditions at a distance of 6 metres. Spherical equivalent (SE) and corrected distance visual acuity (CDVA) was measured using manifest refraction based on autorefraction (ARK-1a; Nidek; Gamagori, Japan). Corneal OCT, pachymetry (Cirrus HD 500; Zeiss; Oberkochen, Germany) and topography (Pentacam HR; Oculus; Irvine, USA) were performed to monitor for postoperative corneal thinning or ectasia. Subjective symptoms were recorded via informal interviews and patient reports of symptoms.
Change in SE and VA was compared preoperatively to 6 months postoperatively, and 4–6 weeks to 6 months postoperatively using two-tailed t-test assuming unequal variances. Association between treatment groups and incidence of postoperative visual complaints was tested for using a χ2 test of independence. All statistical analysis was performed in Excel (Microsoft Office; Microsoft Corporation; Redmond, USA) using the Analysis ToolPak add in. Results were considered statistically different if P < 0.05 and correlation was considered significant if χ crit < χ2.
Results
Retrospective analysis was performed for 32 eyes from 16 patients that had undergone either monocular (20 eyes) or micro-monovision (12 eyes) presbyLASIK (50% female, average age 55±4.6 years). One eye was myopic preoperatively and the remaining 31 eyes were hyperopic. Partial suction loss was encountered for one eye which required partial cutting of the flap with corneal scissors at the 6–8 o’clock position. No other intra- or postoperative complications were experienced and no eyes required refractive enhancement. There was no significant difference in age (P = 0.25), or preoperative sphere (P = 0.96), cylinder (P = 0.91), SE (P = 0.96), UDVA (P = 0.99), UNVA (P = 0.17), CDVA (P = 0.95) or CNVA (P = 0.77) between the groups. Preoperative measurements are summarised in Table 2.
 |
Table 2 Preoperative Baseline Parameters |
All patients attended their 6-week postoperative follow up appointment. Nine patients attended their 3-month (5 monocular and 4 micro-monovision) follow up and ten patients attended their 6-month follow up (6 monocular and 4 micro-monovision).
Visual and Refractive Outcomes
At 6 weeks postoperatively, SE was −0.06±0.47 for distance eyes and −1.14±0.69 for near eyes (Table 3), with 93.7% eyes achieving within ±1.0 D and 59.4% achieving within ±0.5 D of the target (Figure 1A). All eyes achieved within ±1.0 D of the target astigmatism; 75% and 75% achieved within ±0.5 D of target astigmatism for the monocular and micro-monovision groups respectively (Figure 1B). There was a slight trend for overcorrection of distance eyes using micro-monovision treatments (y = 1.2984x – 0.0272; R2 = 0.9607) (Figure 1C) and of under-correction of reading eyes using monocular treatments (y = 0.8635x - 0.4884; R2 = 0.6379) (Figure 1C). Refraction remained stable over 6 months of the study for distance and near eyes and for both treatment groups (P = 0.51 for monocular distance eyes, P = 0.49 for monocular near eyes, P = 0.22 for micro-monovision distance eyes and P = 0.31 for micro-monovision near eyes) (Figure 1D). There was no difference between CS or binocular UDVA, UIVA or UNVA outcomes for monocular and micro-monovision treatments (P = 0.93, 0.31, 0.26 and 0.26 respectively) (Table 3).
 |
Table 3 Postoperative Outcomes at 6 Weeks Following Monocular or Micro-Monovision presbyLASIK. Binocular Uncorrected Visual Acuity is Recorded in LogMAR |
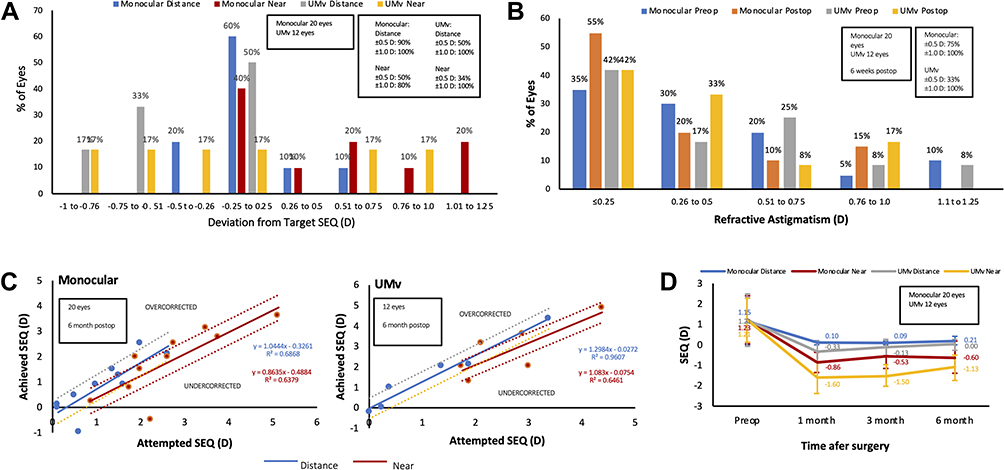 |
Figure 1 Refractive outcomes of monocular or micro-monovision presbyLASIK in eyes corrected for distance and near vision presented as (A) deviation of postoperative SEQ from target refraction, (B) post-refractive atsigmatism, (C) attempted correction versus achieved SEQ, and (D) refractive stability. Abbreviations: SEQ, refractive spherical equivalent; UMv, micro-monovision. |
UDVA was similar under photopic and mesopic conditions (P = 0.53), however UIVA and UNVA were reduced under mesopic conditions compared to photopic conditions (P<0.001) (Table 3). Under photopic conditions, 81.2% patients achieved 0.0 LogMAR (equivalent to 20/20) or better for binocular UDVA and 81.2% achieved N6 (equivalent to 20/40) or better for binocular UNVA (Figure 2A). At 4–6 weeks postoperatively, 59.4% of total eyes experienced a loss of one or more lines of CDVA while 40.6% experienced no change in CDVA. Of those that attended their 6-month appointment (10 patients, total of 20 eyes), 20% eyes experienced a loss of 1 or more lines of CDVA, with 65% experiencing no change and 15% experiencing a gain of 1 line. Neither distance eyes in the monocular group nor near eyes in the micro-monovision group experienced a loss in lines, while 1 (25%; N = 4) distance eye in the micro-monovision group lost 1 line and 4 (67%; N = 6) near eyes in the monocular group lost 1 or more lines (Figure 2B). Two patients (12.5%; N = 16) required spectacles for reading fine print following surgery.
 |
Figure 2 Visual outcomes of monocular or micro-monovision presbyLASIK in eyes corrected for distance and near vision presented as (A) cumulative binocular UDVA and UNVA at 6 weeks and (B) change in monocular CDVA at 6 months. Abbreviations: UDVA, uncorrected distance visual acuity; UNVA, uncorrected near visual acuity; CDVA, corrected distance visual acuity; UMv, micro-monovision. |
Subjective Visual Acuity
There was no statistical association between treatment and incidence of postoperative visual complaints at any time point (χ2 = 0.26, χ crit = 12.59 at 4–6 weeks; χ2 = 0.40, χ crit = 11.07 at 3 months; χ2 = 0.39, χ crit = 11.07 at 6 months). For both treatments, the most common complaint was blurred UNVA which had largely resolved by 6 months for the micro-monovision group (from 50% to 17%; Table 4). Early reports of blurred UDVA and other dry eye symptoms (e.g., grittiness, fluctuating vision, etc.) were largely resolved by 6 months postoperative. Photopic symptoms (i.e., haloes, starbursts) were only reported in the monocular group, but resolved in 50% of cases (1 patient) by 6 months (Table 4).
 |
Table 4 Visual Complaints 3 and 6 Months Following Monocular or Micro-Monovision presbyLASIK |
Discussion
This study reports the refractive and visual outcomes of an Australian cohort following monocular or micro-monovision presbyopic correction using the PresbyMAX suite. This procedure provides safe and effective correction for presbyopia with potentially fewer visual complaints than lens based surgical options that that use diffractive multifocal lenses.
Efficacy
Previous studies of hyperopic eyes undergoing presbyopic correction using the PresbyMAX program have reported between 60–90% of eyes achieving within ±0.5 D of the target refraction,9–11 with a higher proportion of distance eyes within ±0.5 D than reading eyes.11 This study reports a higher proportion of eyes in the monocular group achieving within ±0.5 D of target compared to the micro-monovision group (Figure 1A). In the micro-monovision group there was a trend towards slight under-correction for near-corrected eyes (less myopic result) and slight over-correction for distance eyes (more myopic result) (Figure 1C). The monocular treatment group had better outcomes for UDVA compared to the micro-monovision treatment group with more patients achieving 20/25 or better, while the micro-monovision group had better outcomes for UNVA with more patients achieving 20/40 or better (equivalent to N6 or J3) (Figure 2A). Previous studies have reported between 70–100% achieving 20/20 or better for UDVA and between 80–90% of patients achieving 20/40 or better for UNVA9–12, similar to the outcomes presented here. When assessing suitability, it is important to consider patient preference and lifestyle; monocular treatments may be better suited to patients who prefer to maintain distance vision (i.e., those with outdoor lifestyles) as UDVA is better preserved and any under-correction is likely to be well tolerated. Similarly, patients who prefer to have better near vision (i.e., those who have a lot of screen time) are likely to tolerate some over-correction and may be better suited to micro-monovision treatments. Induced DOF is calculated automatically by the PresbyMAX software based on the treatment mode selected (i.e., −0.9 D for reading eyes), however inducing greater amounts of DOF may also help enhance reading vision for patients wishing greater spectacle independence.
A previous concern of presbyLASIK was postoperative refractive drift resulting from progressive flattening of the cornea and latent hyperopia. Previous studies have reported hyperopic drift of up to 0.1–0.4 D per year following PresbyMAX.5,7 While refraction remained stable with no statistically significant change over the 6 month follow up period, micro-monovision treatments trended towards more hyperopic drift (+0.33 D for distance and +0.47 D for near eyes) compared to monocular treatments (+0.11 D for distance and +0.26 D for near eyes). Near-corrected eyes (i.e., non-dominant eyes) also showed a trend towards more hyperopic drift compared to distance-corrected eyes (Figure 1D). While using cycloplegic refraction helps to reduce the risk of regression due to uncorrected latent hyperopia, it has also been reported that larger corrections are at more risk of regression following hyperopic LASIK.6 Preoperative SE for this study ranged from 0 D to 3.375 D; the inclusion of large corrections in this study group could explain the higher rate of regression compared to similar studies, and could also explain the higher risk of regression for near-corrected eyes as hyperopic near-corrected eyes require a larger treatment. Increasing the ablation zone6 and application of 0.02% mitomycin C may help reduce the risk of regression and scarring.13
Safety
Previous studies have reported between 10–50% of eyes losing 1 or more lines of CDVA9–12 following presbyLASIK, similar to that reported here. At 6 months postoperative, approximately 50% of patients who had lost lines of CDVA at 3 months had recovered. Due to the transient nature of the reduction in CDVA, it is likely to be due to dry eyes which is reported in up to 95% of cases following LASIK,14 usually resolving over the following months. As it has been reported that hyperopic presbyLASIK induces corneal higher order aberrations (HOAs) to a larger extent than standard hyperopic LASIK,5 it is also possible that stabilization of the HOAs may also be a contributing factor to the delayed recovery in vision. At 6 months, loss of lines of CDVA was only reported in distance-corrected eyes from the micro-monovision group and near-corrected eyes from the monocular group (Figure 2B). As CDVA was preserved in the preferred eye for each group (i.e., distance eye for the monocular group and the near eye for the micro-monovision group), it was considered likely that any loss of CDVA would be well tolerated by the patients. In fact, the patient from the micro-monovision group who lost 1 line of CDVA in their distance-corrected eye did not report any visual complaints and was satisfied with their vision. Of the patients from the monocular group who lost lines of CDVA in their near-corrected eyes, one patient lost 1 line of CDVA and initially complained of poor reading vision, possibly due to higher expectations, but was satisfied following counselling. One patient lost 2 lines of CDVA and complained of mild eye strain but was otherwise satisfied. This patient was under-corrected (postoperative SE +0.625 D versus a target of −1.5 D) and experienced an increase in horizontal coma (−0.934 micron postoperatively compared to −0.042 micron preoperatively). Horizontal coma is generally compensated for by the crystalline lens but has been reported to correlate with double vision following LASIK.15 As the patient did not report symptoms of double vision, the mild eye strain reported by the patient was likely a result of under-correction of the near-corrected eye possibly due to latent hyperopia. Another patient in the monocular group lost 3 lines of CDVA and complained of poor vision in the near-corrected eye. Notably, this eye experienced partial suction loss during the procedure which necessitated partial manual cut of the flap. The flap appeared normal postoperatively and did not require further intervention. Total HOAs remained similar for this eye postoperatively, however there was increase in with-the-rule (WTR) astigmatism compared to preoperative levels (−0.791 micron postoperatively compared to −0.042 micron preoperatively). It has been reported that with WTR astigmatism results in better UDVA outcomes in emmetropic post-LASIK eyes compared to against-the-rule (ATR) astigmatism16 while ATR astigmatism helps improve near vision in myopic eyes.17 It is possible that the postoperative WTR astigmatism compromised his near vision in the affected eye. Although the postoperative SE was close to target (−0.875 D vs. a −1.0 D target), it is also possible that the patient may have benefited from a more myopic target or more comprehensive preoperative counselling. Despite this, the majority of patients were satisfied with their vision and no patients required refractive enhancement.
Visual Quality
PresbyLASIK offers an alternative to standard multifocal or extended DOF (EDOF) lenses which have been associated with reduction in CS, reduced low light vision and the induction of visual artefacts such as haloes and glare.18–20 It also helps to provide spectacle independence in presbyopic patients who are considered too young for lens-based procedures and do not want to lose stereopsis or have any photopic symptoms. Most previous studies have compared multifocal to monofocal lens implantation, generally reporting a reduction of CS between 0.06–0.09 for eyes that receive multifocal lenses compared to the eye that receive monofocal lenses.19,21 Studies that have assessed postoperative CS following LASIK or presbyLASIK are sparser and are often inconsistent. Epstein et al compared CS following LASIK or presbyLASIK and reported similar CS for both treatments5 while Pinelli et al reported a decrease in CS at higher spatial frequencies compared to preoperative values for patients that had undergone laser presbyopia correction, postulating that this may be due to an increase in postoperative coma.22 Schlote et al reported a postoperative CS of 1.83±0.18 for a group treated for presbyopia using the Supracor suite, within the normal population range.23 Importantly, a Cochrane review reported that changes in CS following presbyLASIK appear to be dependent on the CS testing method used, with charts that utilize sinusoidal gratings being more sensitive to changes in CS.24 Furthermore, CS testing results have been reported to be greatly affected by lighting conditions.25 For this study, a Pelli-Robson chart was used to test CS under mesopic conditions, and an average postoperative CS of 1.45±0.12 was reported (Table 3). The testing method and lack of a comparison group means that it is difficult to meaningfully compare CS results for this study to previously published literature. However, CS was statistically similar between the monocular and micro-monovision groups (P = 0.93), suggesting that neither treatment has a benefit over the other in terms of maintaining CS, with both groups achieving what is considered a clinically normal outcome.
Reduced vision under low light conditions following implantation of multifocal lenses is caused by the diffractive design of the lens limiting the amount of usable light available to the eye. PresbyLASIK-treated corneas follow a similar pattern, with different refractive zones of the cornea responsible for the focusing of light from distant and near objects. While this study reports similar UDVA under photopic and mesopic conditions (P = 0.53), UIVA and UNVA were reduced under mesopic conditions (P = <0.001; Table 3). As monocular presbyLASIK treats the dominant eye with a standard monofocal profile, it was postulated that UIVA and UNVA may not be as severely affected in monocular treated eyes compared to micro-monovision treated eyes. However, monocular and micro-monovision groups performed similarly (P = 0.31, 0.26 and 0.26 for UDVA, UIVA and UNVA respectively). While most patients achieved full spectacle independence, two patients (i.e., 12.5%) required spectacles for fine print suggesting that the effect of the splitting of light is not clinically significant for either treatment mode.
Multifocal lenses are reported to have an increased incidence of haloes and glare compared to monofocal lenses by approximately 1.4 to 1.9-fold and 3.1 to 3.6-fold respectively.19,24 In a study of patients that had undergone monocular presbyLASIK, Epstein5 reported that haloes were recorded in 55% of patients, predominately in the near-corrected eye. However, the symptoms gradually resolved over 3 months. For this study, the predominant subjective complaints in the early postoperative period were blurred distance and near vision which had largely resolved by 6 months (Table 4), likely a result of postoperative dry eye. Starbursts and haloes were reported in a small proportion of patients within the monocular group and improved with time (20% at 3 months and 10% at 6 months). Visual artefacts such as haloes/starbursts in the early postoperative period may be a result of induced HOAs and may improve as the cornea stabilizes. An adequate postoperative routine that incorporates lubricating eye drops may help stabilize vision postoperatively while patient expectations can be managed with counselling.
Limitations of this study include a small sample size, a relatively short follow up period and the lack of a comparison group. The results suggest that early outcomes may be affected by the induction of corneal aberrations and tear film instability; further long-term studies will be required to assess long term safety. The retrospective nature of this study also resulted in incomplete data due to some patients being lost to follow up. Testing methods for CS made it difficult to meaningfully compare the results to the literature; a universally consistent testing and reporting method for CS would be beneficial to adequately assess the impact of presbyLASIK and other presbyopia correcting techniques on CS. Stereopsis was also not routinely performed at the time of preoperative testing; comparing stereopsis for virgin corneas or eyes that have undergone implantation with multifocal lenses would be beneficial in assessing the impact of presbyLASIK on stereopsis. Further long-term large-scale prospective studies comparing directly to outcomes achieved with multifocal lenses would be beneficial.
Conclusions
PresbyLASIK using the Schwind PresbyMAX module allows for an effective minimally-invasive alternative for the correction of presbyopia in patients deemed too young for consideration of lens-based correction or those intolerant of photic symptoms or loss of stereopsis. Stereopsis and CS appear to be well maintained. Early outcomes may be affected by the induction of corneal aberrations. Selection of the treatment mode and planning of procedures needs to consider patient preference and lifestyle. While monocular treatments are likely to be better suited to patients that prefer distance vision and micro-monovision those who prefer near vision, subjective vision and refractive stability is similar between treatments. Appropriate patient counselling, particularly regarding limitations under low light conditions and quality of vision in the early postoperative period is vital in ensuring patient satisfaction.
Abbreviations
SE, spherical equivalent; UDVA, uncorrected distance visual acuity; UIVA, uncorrected intermediate visual acuity; UNVA, uncorrected near visual acuity; CDVA, corrected distance visual acuity; LASIK, laser assisted in situ keratomileusis; DOF, depth of focus; SA, spherical aberration; OSI, objective scattering index; MTF, modulation transfer function; CS, contrast sensitivity; WTR, with the rule; ATR, against the rule; EDOF, extended depth of focus.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Frick KD, Joy SM, Wilson DA, Naidoo KS, Holden BA. The global burden of potential productivity loss from uncorrected presbyopia. Ophthalmology. 2015;122:1706–1710. doi:10.1016/j.ophtha.2015.04.014
2. Pajic B, Pajic-Eggspuehler B, Mueller J, Cvejic Z, Studer H. A novel laser refractive surgical treatment for presbyopia: optics-based customization for improved clinical outcome. Sensors. 2017;17(6):1367. doi:10.3390/s17061367
3. Stival LR, Figueiredo MN, Santhiago MR. Presbyopic excimer laser ablation: a review. J Cataract Refract Surg. 2018;34:698–710. doi:10.3928/1081597X-20180726-02
4. Luger MH, Ewering T, Arba-Mosquera S. Nonwavefront-guided presby reversal treatment targeting a monofocal cornea after bi-aspheric ablation profile in a patient intolerant to multifocality. J Refract Surg. 2014;30:214–216. doi:10.3928/1081597X-20131223-01
5. Epstein R, Gurgos MA. Presbyopia treatment by monocular peripheral presbyLASIK. J Refract Surg. 2009;25:516–523.
6. Gharaibeh AM, Villanueva A, Mas D, Espinosa J, Alio JL. Corneal stability following hyperopic LASIK with advanced laser ablation profiles analysed by a light propagation study. J Ophthalmol. 2018;2018:10.
7. Luger MHA, McAlinden C, Buckhurst PJ, Wolffsohn JS, Verma S, Arba-Mosquera S. Long-term outcomes after LASIK using a hybrid bi-aspheric micro-monovision ablation profile for presbyopia correction. J Refract Surg. 2020;36:89–96. doi:10.3928/1081597X-20200102-01
8. Fu D, Zhao J, Zhou XT. Objective optical quality and visual outcomes after the PresbyMAX monocular ablation profile. Int J Ophthalmol. 2020;13:1060–1065. doi:10.18240/ijo.2020.07.07
9. Uthoff D, Pozlz M, Hepper D, Holland D. A new method of cornea modulation with excimer laser for simultaneous correction of prebyopia and ametropia. Graefes Arch Clin Exp Ophthalmol. 2012;250:1649–1661. doi:10.1007/s00417-012-1948-1
10. Baudu P, Penin F, Arba Mosquera S. Uncorrected binocular performance after biphasic ablation profile for presbyopic corneal treatment using AMARIS with the PresbyMAX module. Am J Ophthalmol. 2013;155:636–647. doi:10.1016/j.ajo.2012.10.023
11. Luger MH, McAlinden C, Buckhurst PJ, Wolffsohn JS, Verma S, Arba Mosquera S. Presbyopic LASIK using hybrid bi-aspheric micro-monovision ablation profile for presbyopic corneal treatments. Am J Ophthalmol. 2015;160:493–505. doi:10.1016/j.ajo.2015.05.021
12. Chan TCY, Kwok PSK, Jhanji V, Woo VCP, Ng ALK. Presbyopic correction using monocular bi-aspheric ablation profile (PresbyMAX) in hyperopic eyes: 1-year outcomes. J Refract Surg. 2017;33:37–43. doi:10.3928/1081597X-20161006-03
13. Moawad EM, Abd Elghany AA, Gab-Alla SA, Elbassiouny OM, Badawy MS. LASIK-induced corneal changes after correction of hyperopia with and without application of mitomycin-C. BMC Ophthalmol. 2019;19:19. doi:10.1186/s12886-019-1100-7
14. Yu EYW, Leung A, Rao S, Lam DSC. Effect of laser in situ keratomileusis on tear stability. Ophthalmology. 2000;107:2131–2135. doi:10.1016/S0161-6420(00)00388-2
15. Chalita MR, Xu M, Krueger RR. Correlation of aberrations with visual symptoms using wavefront analyis in eyes after laser in situ keratomileusis. J Refract Surg. 2003;19:S682–S686. doi:10.3928/1081-597X-20031101-13
16. Mimouni M, Nemet A, Pokroy R, Sela T, Munzer G, Kaiserman I. The effect of astigmatism axis on visual acuity. Eur J Ophthalmol. 2017;27:308–311. doi:10.5301/ejo.5000890
17. Sigireddi RR, Weikert MP. How much astigmatism to treat in cataract surgery. Curr Opin Ophthalmol. 2020;31:10–14. doi:10.1097/ICU.0000000000000627
18. Javitt JC, Steinert RF. Cataract extraction with multifocal intraocular lens implantation: a multinational clinical trial evaluating clinical, functional, and quality-of-life outcomes. Ophthalmology. 2000;107:2040–2048. doi:10.1016/S0161-6420(00)00368-7
19. Cao K, Friedman DS, Jin S, et al. Multifocal versus monofocal intraocular lenses for age-related cataract patients: a system review and meta-analysis based on randomised controlled trials. Surv Ophthalmol. 2019;64:647–658. doi:10.1016/j.survophthal.2019.02.012
20. Khandelwal SS, Jun JJ, Mak S, Booth MS, Shekelle PG. Effectiveness of multifocal and monofocal intraocular lenses for cataract surgery and lens replacement: a systematic review and meta-analysis. Graefes Arch Clin Exp Ophthalmol. 2019;257:863–875. doi:10.1007/s00417-018-04218-6
21. Altemir-Gomez I, Millan MS, Vega F, et al. Comparison of visual and optical quality of monofocal versus multifocal intraocular lenses. Eur J Ophthalmol. 2020;30:299–306. doi:10.1177/1120672119827858
22. Pinelli R, Ortiz D, Simonetto A, Bacchi C, Sala E, Alio JL. Correction of presbyopia in hyperopia with a center-distance, paracentral-near technique using the technolas 217z platform. J Refract Surg. 2008;24:494–500.
23. Schlote T, Heuberger A. Multifocal corneal ablation (Supracor) in hyperopic presbyopia: 1-year results in a cross-sectional study. Eur J Ophthalmol. 2017;27:438–442. doi:10.5301/ejo.5000871
24. de Silva SR, Evans JR, Kirthi V, Ziaei M, Leyland M. Multifocal versus monofocal intraocular lenses after cataract extraction. CDSR. 2016;12:CD003169. doi:10.1002/14651858.CD003169.pub4
25. Buhren J, Terzi E, Bach M, Wesemann W, Kohnen T. Measuring contrast sensitivity under different lighting conditions: comparison of three tests. Optom Vis Sci. 2006;83:290–298. doi:10.1097/01.opx.0000216100.93302.2d
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.