")
Back to Journals » Drug Design, Development and Therapy » Volume 18
Dupilumab Treatment in Pediatric Patients Aged 6–11 Years with Severe Atopic Dermatitis Whose Disease Is Not Adequately Controlled: A Review
Authors Cork MJ, Danby SG, Rossi AB, Bansal A
Received 26 July 2023
Accepted for publication 3 January 2024
Published 3 February 2024 Volume 2024:18 Pages 277—289
DOI https://doi.org/10.2147/DDDT.S426947
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Manfred Ogris
Video abstract presented by Rossi.
Views: 107
Michael J Cork,1,2 Simon G Danby,1,2 Ana B Rossi,3 Ashish Bansal4
1Sheffield Dermatology Research, University of Sheffield, Sheffield, UK; 2Sheffield Children’s Hospital, Sheffield, UK; 3Sanofi, Cambridge, MA, USA; 4Regeneron Pharmaceuticals Inc., Tarrytown, NY, USA
Correspondence: Michael J Cork, Sheffield Dermatology Research, Department of Infection and Immunity, The University of Sheffield, K Floor, The Medical School (RHH tower), Beech Hill, Sheffield, S10 2RX, UK, Email [email protected]
Abstract: Atopic dermatitis (AD) is the most common inflammatory skin disease in children. Children with severe AD have a multidimensional disease burden characterized by skin lesions, itching, frequent infections, sleep deprivation, and a high rate of comorbidities. These impact the mental health and overall quality of life of not only the children but also of their parents and caregivers. There are few effective available treatment options for young children with severe AD that are suitable for long-term use. Due to their adverse effects, practice guidelines consider systemic agents inappropriate for this age group, although they are still used off-label in extreme cases. The biologic dupilumab has recently been approved for children aged 6– 11 years with severe (EU) and moderate-to-severe (USA) AD, offering hope to this population of patients with a high unmet clinical need. The purpose of this review is to describe the unmet needs of AD patients aged 6– 11 years prior to dupilumab approval and to summarize existing clinical data supporting dupilumab’s safety and efficacy in these children.
Keywords: atopic dermatitis, children, dupilumab, pediatric, severe
Introduction
Atopic dermatitis (AD) is a common inflammatory skin disease of childhood affecting as many as 20% of children worldwide, with a prevalence of 13% in children aged 6–11 years.1 The proportion of children aged 6–11 years with mild AD that can be controlled adequately with topical therapies ranges from 33.2% to 76.4%, while a small subset (0.9–12.3%) have severe disease.1
Children with severe AD have multidimensional disease burden characterized by skin lesions, itching, frequent infections, sleep deprivation, and a high rate of comorbidities, all of which impact the mental health and the overall quality of life of the children and also their parents and caregivers.2–4
Once young children with severe AD have become refractory to conventional topical medications, there are few effective available treatment options suitable for long-term use available to them . Due to the adverse effects of systemic agents, practice guidelines generally consider them inappropriate for this age group; however, they are still used off-label in severe cases.5–7 Prior to dupilumab’s approval, the only approved treatments for children with uncontrolled moderate-to-severe AD in the USA and EU were topical agents and systemic corticosteroids. Cyclosporine is approved in several countries for patients aged ≥16 years but used off-label in younger children.5,8–10
The biologic dupilumab was approved for children aged 6–11 years with severe (EU) and moderate-to-severe (USA) AD in 2020, ameliorating the high unmet clinical need in this population of patients.11,12 The purpose of this narrative review is to describe the unmet needs of patients with AD aged 6–11 years prior to dupilumab’s approval and to summarize existing clinical data supporting the safety and efficacy of dupilumab in these children.
Pathophysiology of AD
For decades, dermatologists considered skin barrier dysfunction to be an earlier factor in AD pathophysiology than inflammatory response. Recent data have shown that the skin barrier dysfunction that enables penetration of antigens is caused mainly by the type 2 inflammatory cytokines interleukin (IL)-4 and IL-13. These cytokines – produced by keratinocytes, lymphocytes (eg, T helper type 2 cells), mast cells, basophils, and eosinophils – disrupt the skin barrier through interference in several different components: downregulating filaggrin expression; reducing tight junction barrier function; reducing synthesis of long-chain ceramides; reducing production of antimicrobial peptides and natural moisturizing factors; and inducing microbiome dysbiosis.13 Additional clinical evidence has confirmed this finding by showing reversibility of skin barrier dysfunction with dupilumab treatment.14–17
AD in Children Aged 6–11 Years
Prevalence, Clinical Presentation, and Multidimensional Disease Burden
The Epidemiology of Children with Atopic Dermatitis Reporting on their Experience (EPI-CARE) study is a cross-sectional worldwide survey set up to establish the prevalence and severity of AD across the pediatric age range, with the aim of informing country-specific healthcare allocation and evaluating the real-world burden of AD.1 Among more than 22,000 6–11-year-olds surveyed from 18 countries in North America, Latin America, Europe, the Middle East, and Eurasia/East Asia, the 1-year diagnosed AD prevalence was 13%, ranging from 2.4% in Israel to 19.5% in Italy.1 Across all countries, disease severity as assessed by the Patient-Oriented Eczema Measure (POEM)18 was moderate in 22.4–57.3% and severe in 1.5–12.3% of included patients.1
Identifying patients with more severe disease is important. A systematic review of 110,651 patients with AD aged between 0.04 and 17.5 years showed that children with persistent disease, later-onset disease, and/or more severe disease were more likely to have AD that persists into adulthood.19 Analysis of data from two British cohorts followed from birth through midlife identified subtypes of AD based on patterns of disease, in which similar proportions of participants had a decreasing, increasing, or persistently high probability of AD symptoms with age.20 Individuals in the persistently high subtype were most likely to experience asthma and rhinitis, and those in the increasing subtype were at higher risk of poor self-reported general (OR, 1.29; 95% CI, 1.09–1.53) and mental (OR 1.45; 95% CI, 1.23–1.72) health in midlife.
Clinical signs of AD change with age. Infants and children under 2 years of age tend to have pruritic, erythematous, weeping lesions on the cheeks, scalp, and extensor surfaces of extremities (Figure 1A). In children (aged 2–12 years), these lesions can progress into thickened dry plaques, papules, and excoriations located on the wrists and flexural surfaces of extremities (Figure 1B).21 The cardinal symptom of childhood AD is a debilitating pruritus (itch), but sleep loss and impaired mental health are also very common and debilitating.
 |
Figure 1 Clinical signs of atopic dermatitis in infants (A) and children (B). Photos courtesy of Dr Tanigushi Abagge. Caregivers and investigators authorized the publication of these photos. |
Children with AD have a multidimensional disease burden, which increases with higher disease severity.22,23 The physical burden of AD made patients experience chronic sleep disturbance, which can lead to high rates of emotional distress, social isolation, depression, anxiety, attention deficit hyperactivity disorder-associated behaviors, and other behavioral problems such as irritability, crying, learning disability, school productivity losses, and limitations to everyday activities.23–29 In a population-based birth cohort study, AD was associated with emotional and conduct problems, as well as symptoms of hyperactivity and inattention in children. Risk of internalizing symptoms was increased even for children with mild AD beginning early in childhood, highlighting the importance of behavioral and mental health awareness in this population.28 In a global, observational survey, the PEDIatric Study in Atopic Dermatitis (PEDISTAD; NCT03687359) of children aged <12 years in approximately 20 countries,30 baseline disease activity analysis revealed that children in the cohort aged 6–11 years (n = 431) had moderate-to-severe symptoms and that their disease had a moderate-to-very large impact on quality of life, based on mean baseline POEM and Children’s Dermatology Life Quality Index (CDLQI) scores, respectively (mean [standard deviation, SD] POEM, 15.3 [7.2]; mean [SD] CDLQI 10.8 [6.7]).2
Parents and caregivers of children with AD also frequently report sleep disturbance, exhaustion, worry, and social isolation related to their child’s disease,31 and the psychological impact on their children, along with emotional and behavioral difficulties, may impact their ability to implement treatment plans effectively.24,32 In the PEDISTAD study, caregivers of children with AD reported low-to-moderate family impact (Dermatitis Family Impact [DFI] questionnaire) and moderate-to-severe disease severity (Caregiver’s Global Assessment of Disease), demonstrating a multidimensional impact of AD on children and their caregivers.33 EPI-CARE surveyed 7465 pairs of pediatric participants and their parents/caregivers, and it found that DFI score increased with disease severity and that, across geographic areas and age groups, even mild AD affected family life.3 AD also poses a serious public health and financial burden due to its high prevalence, significant morbidity, and increased healthcare utilization to treat medical and mental comorbidities and associated costs.22,34,35
Specific Challenges in Treatment Management
Type 2 Inflammatory Comorbidities in Patients with AD
Other diseases resulting from aberrant type 2 inflammation often occur as comorbidities in adult and adolescents with AD and include allergic rhinitis (AR), asthma, chronic rhinosinusitis with or without nasal polyps, food allergies, inhaled allergies, and eosinophilic esophagitis. These comorbidities increase the disease burden and healthcare costs and have an additional detrimental effect on quality of life, adding to the complexity of treatment management.22,36–38
As is the case with adults and adolescents, atopic comorbidities are common among pediatric patients with AD; prevalence increases with disease severity and adds to the complexity of treatment management.22,23 Currently available systemic therapies for AD, such as oral corticosteroids and cyclosporin A, have not been shown to have a positive treatment impact on these comorbidities. In fact, there are data showing that immunoglobulin E production stimulated by allergen exposure is not inhibited by cyclosporin A-mediated T-cell suppression39 and that cyclosporin may exacerbate AD in some patients.40
Data from the EPI-CARE study have shown that children with AD have a high burden of self-reported atopic comorbidities, most notably asthma and AR. This burden is high even among those with clear/mild AD and is worse with increasing AD severity. Of 7465 children surveyed, 92% of those in the cohort aged 6–11 years reported at least one atopic comorbidity.4 In the cohort aged 6–11 years of the PEDISTAD study, 68% of patients had at least one comorbidity at baseline; the most common were AR (46%) and asthma (36%), and these appeared to increase with age vs younger cohorts.2
Therapeutic Options and the Unmet Need of Patients Aged 6–11 Years with AD
There are few effective treatment options suitable for long-term use available to children aged 6–11 years with severe AD; as a result, a significant unmet need exists for these patients.
Most therapeutic guidelines recommend a stepped approach, in which treatment is tailored to disease severity and is stepped up or down accordingly.5,6,21,41 Emollients and moisturizers form the basis of treatment and should always be used, even when lesions are not active.
As a chronic disease, AD requires long-term treatment and disease management. Topical therapies often fail to adequately control AD.42,43 In addition to therapeutic inadequacies, topical treatments are limited by low adherence and potential local and systemic side effects, especially for patients in whom AD occurs in sensitive areas or covers a large body surface area. Oral corticosteroids are unsuitable for chronic or relapsing AD due to their poor benefit–risk profile and likelihood of disease recurrence.5 Systemic non-steroidal immunosuppressants (NSISS), including cyclosporin A, methotrexate, mycophenolate mofetil, and azathioprine, are frequently prescribed to treat severe AD that is refractory to topical therapy.5,44 Despite the extensive use of these in the moderate-to-severe AD population, there is a lack of robust evidence from large, well-designed, randomized clinical trials to support their use, especially in children. Multiple small trials have supported the use of cyclosporin A to treat moderate-to-severe AD refractory to topical therapy, but the toxicity profile requires frequent laboratory monitoring, and long-term treatment is not recommended. Apart from cyclosporin A, which is approved in some countries for severe AD, in patients 16 years and older the remaining NSISS are prescribed off-label. Of note, cyclosporin A use for treatment of severe AD was approved in the 1980s, when robust randomized controlled studies were not required for registration, and medications could be approved by national procedures based on small studies, potentially with methodological flaws.
Biologic Therapy
Several biologic drugs targeting key pathogenic mechanisms of the atopic immune response are under clinical investigation, including those targeting cytokines, Janus kinases, and phosphodiesterases;41,45 however, only dupilumab is approved for the treatment of children aged 6–11 years.11,12
Dupilumab is a fully human monoclonal antibody that blocks the shared receptor component for IL-4 and IL-13, inhibiting signaling of both IL-4 and IL-13, key and central drivers of type 2-mediated inflammation in multiple diseases.46 The efficacy and safety of dupilumab have also been established in adult and adolescent patients with moderate-to-severe AD.47–52 In addition, a Phase III study in children aged 6 months to less than 6 years showed that dupilumab provided clinically meaningful benefits in this age group and is well tolerated.53
Clinical Experience with Dupilumab in Patients Aged 6–11 Years with AD
The pediatric clinical development program for dupilumab in AD includes several clinical trials (Figure 2). Efficacy and safety have been investigated in pediatric patients aged as young as 6 months and up to 18 years. In addition to the Phase II and Phase III trials, there are several ongoing Phase IV and observational studies in pediatric populations. Dupilumab dosing in the various clinical trials is shown in Figure 2. This review focuses on the clinical data in children aged 6–11 years with severe AD inadequately controlled by topical medication, enrolled in clinical trials R668-AD-1412 (NCT02407756), LIBERTY AD PEDS (AD-1652; NCT03345914), and LIBERTY AD PED-OLE (R668-AD-1434; NCT02612454).
 |
Figure 2 Dupilumab pediatric development program: clinical trials. Abbreviations: AD, atopic dermatitis; SC, subcutaneously; TCS, topical corticosteroids; q2w, every 2 weeks; q4w, every 4 weeks. |
Open-Label and Extension Studies
R668-AD-1412 (NCT02407756) was a global, multicenter, open-label, ascending-dose, sequential cohort Phase IIa study; it was followed by LIBERTY AD PED-OLE (R668-AD-1434; NCT02612454), an ongoing, open-label extension (OLE) Phase III study. Of 38 children enrolled, 37 completed AD-1412 and 33 continued to the PED-OLE; full study design details and data have been reported previously.54
Briefly, children aged 6–11 years with severe AD inadequately controlled by topical medications were enrolled. Patients received single-dose dupilumab 2 or 4 mg/kg (Part A) followed by an 8-week pharmacokinetic sampling period. Thereafter, patients received the same dose weekly for 4 weeks (Part B), followed by an 8‐week safety follow‐up period. To assess long-term safety and efficacy of dupilumab, the patients could then enroll in the PED-OLE, continuing the same dose regimen for up to Week 52 of the PED-OLE study.
Signs of AD were assessed using the Investigator’s Global Assessment (IGA), Eczema Area and Severity Index (EASI), SCORing Atopic Dermatitis (SCORAD), and body surface area (BSA) affected by AD. Improvements in all measures were observed after a single dose of dupilumab at Week 2 and increased in Part B of the study, and then were maintained throughout the PED-OLE to Week 52 (Table 1), at which time over 90% of patients achieved 50% improvement from baseline in EASI score (EASI-50), over 80% achieved EASI-75, and over 50% achieved an IGA score of 0 or 1 and/or EASI-90. Improvement in SCORAD was defined as a reduction by more than 70%, and improvement in BSA as a reduction by more than 50%.
 |
Table 1 Efficacy of Dupilumab in Clinical Trials in Children Aged 6 to 11 Years with Severe Atopic Dermatitis |
AD symptoms in AD-1412 and the PED-OLE were assessed using the Peak Pruritus Numerical Rating Scale (NRS) (Table 1). Proportions of patients with a ≥3-point and a ≥4-point reduction in Peak Pruritus NRS increased from Part A to Part B in AD-1412, and then in the PED-OLE, in which over 75% of patients achieved a ≥3-point reduction, and over 65% achieved a ≥4-point reduction, in the pruritus measure.
Additionally, symptoms in the PED-OLE were assessed by POEM, and health-related quality of life were assessed by the CDLQI. Mean improvements (SD) by 11.6 points (6.6) were reported in POEM [range 0–28] and by 8.8 points (6.4) in CDLQI [range 0–30] at Week 52.
Dupilumab treatment for up to 52 weeks was generally well tolerated in this population, with an acceptable safety profile consistent with the known safety profile in adolescents and adults with moderate-to-severe AD.47–50,52 Two patients (5.4%) reported serious treatment-emergent adverse events (TEAEs) in AD-1412 and 5 (15.2%) in the PED-OLE; none were deemed to be related to the study drug (Table 2). The majority of TEAEs were mild or moderate and transient and none led to treatment discontinuation54 (Table 2). The most frequent TEAEs in both AD-1412 and the PED-OLE were nasopharyngitis and exacerbation of atopic dermatitis (Table 2).
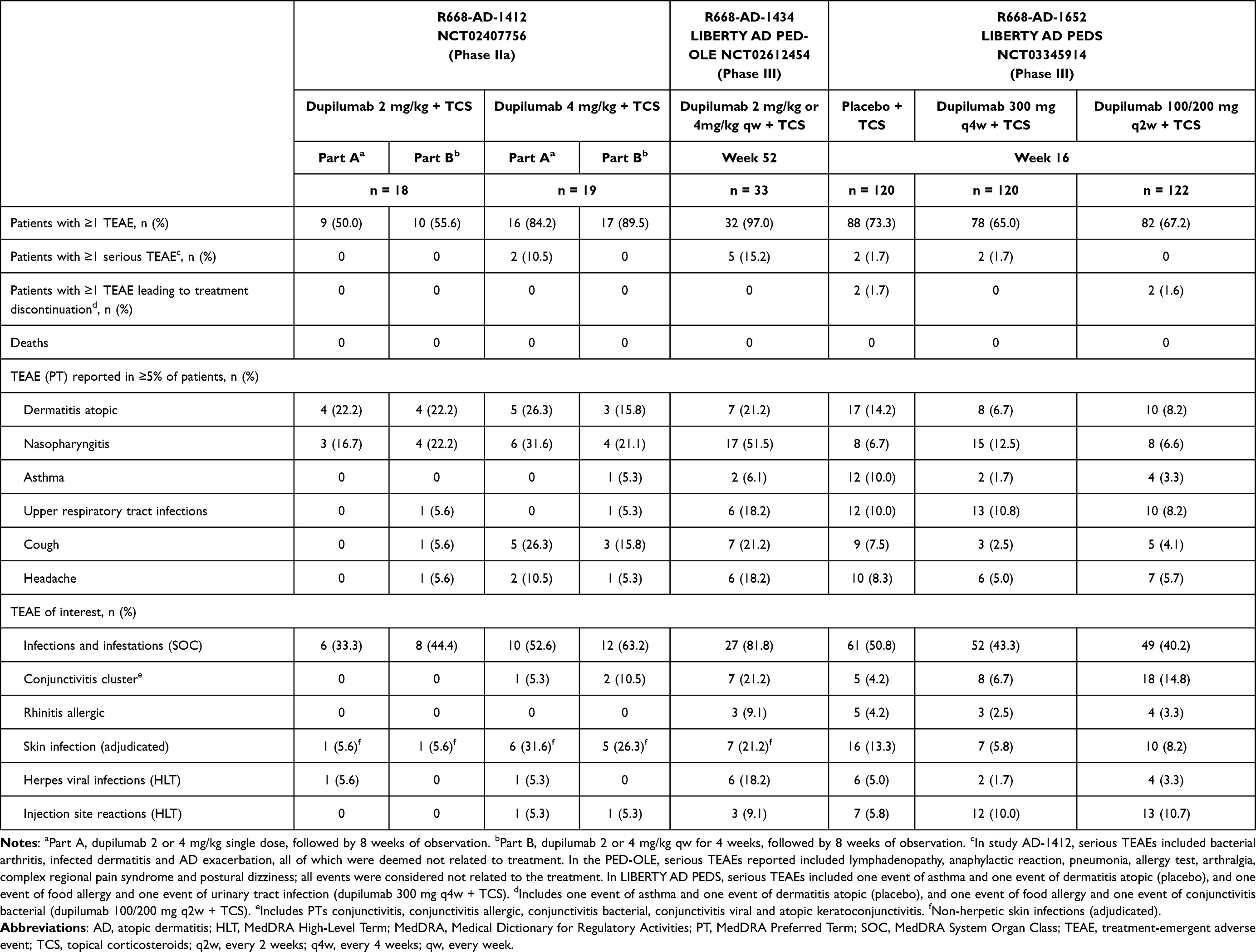 |
Table 2 Safety of Dupilumab in Clinical Trials in Children Aged 6–11 Years with Severe Atopic Dermatitis |
LIBERTY AD PEDS
LIBERTY AD PEDS (AD-1652; NCT03345914) was a randomized, double-blind, parallel-group Phase III trial. Eligible patients were children aged 6–11 years with severe AD inadequately controlled by topical medications. Patients (N = 367) were randomized 1:1:1 to placebo, dupilumab 300 mg every 4 weeks (q4w) (loading dose 600 mg), or weight-based dupilumab every 2 weeks (q2w) (100 mg with loading dose 200 mg if weight <30 kg, or 200 mg with loading dose 400 mg if weight ≥30 kg) for 16 weeks. All patients received medium-potency topical corticosteroids (TCS) starting 2 weeks before baseline, with a possibility to escalate to high-potency TCS as rescue therapy; very-high-potency TCS were prohibited. Results and design details have previously been reported in full.55
The primary endpoint was the proportion of patients with an IGA score of 0 or 1 (“clear” or “almost clear”) at Week 16. A co-primary outcome in EU and EU-reference countries was the proportion of patients with EASI-75 at Week 16. Key secondary endpoints included the percent change in EASI from baseline at Week 16 and changes in the weekly Peak Pruritus NRS score.
The trial met all the primary and key secondary endpoints. Improvements in all measures were consistent with those observed in the PED-OLE, and they were significant compared with placebo for both dupilumab dose regimens (Table 1). At Week 16, ~30% of patients who received dupilumab achieved an IGA score of 0 or 1 vs 11.4% in the placebo group (P < 0.0001 for q4w vs placebo and P < 0.001 for q2w vs placebo). The proportions of patients achieving EASI-75 were 69.7%, 67.2%, and 26.8% for patients who received, respectively, dupilumab q4w, dupilumab q2w, and placebo (P < 0.0001 for each dose regimen vs placebo). These improvements were ongoing at Week 16, suggesting that longer treatment may add further benefit. Significant improvements were also reported in other measures of disease activity such as EASI percent change from baseline, SCORAD, and BSA.
AD symptoms were assessed using Peak Pruritus NRS and POEM scores. Of patients treated with dupilumab q4w, approximately three times more dupilumab-treated patients than placebo-treated patients achieved a ≥3-point reduction in the pruritus measure, and 50.8% vs 12.3% achieved a ≥4-point reduction at Week 16 (P < 0.0001 for both comparisons). Similarly, dupilumab-treated patients reported POEM mean score reductions (SE) of 13.6 points (0.7), compared with 5.3 points (0.7) in placebo-treated patients (P < 0.0001).
Improvements in quality of life, as measured by reduction in CDLQI scores, were also significant compared with placebo and mirrored the improvements in POEM. The efficacy of dupilumab in this study is illustrated by images and outcomes of a participating patient (Figure 3).
 |
Figure 3 Images of dupilumab efficacy before and after treatment. (A) Photo of a patient with AD signs and symptoms depicted in rainbow graphics (B) and spider plots (C) before and after dupilumab treatment in AD-1652. The rainbow graphics show changes in scores from baseline to Week 16. The spider plots show percent improvement from baseline to Week 16. Caregivers and investigators authorized the publication of these photos. Abbreviations: AD, atopic dermatitis; BSA, body surface area; CDLQI, Children’s Dermatology Life Quality Index; EASI, Eczema Area and Severity Index; IGA, Investigator’s Global Assessment; POEM, Patient-Oriented Eczema Measure; PP-NRS, Peak Pruritus Numerical Rating Scale; SCORAD, SCORing Atopic Dermatitis; VAS, Visual Analog Scale. |
More patients receiving placebo than either dupilumab regimen required rescue medication (19.2% vs 4.9% [q2w] and 2.5% [q4w]).
The overall incidence of TEAEs was lower in dupilumab-treated patients than in placebo-treated patients for both dupilumab dose groups (65.0% [q4w] and 67.2% [q2w] vs 73.3%) (Table 2). Two placebo-treated patients and two dupilumab-treated patients in the q4w group reported serious TEAEs; none were related to the study drug. Treatment discontinuations due to TEAEs were uncommon (placebo, n = 2; dupilumab q2w, n = 2). No deaths, treatment-related hypersensitivity, or anaphylaxis events were observed.
Injection-site reactions were more common with dupilumab than placebo treatment (approximately 10% of dupilumab-treated patients vs 5.8% of placebo-treated patients); none were severe or led to discontinuation. Conjunctivitis was also more common in dupilumab-treated patients (14.8% [q2w] and 6.7% [q4w] vs 4.2%). Apart from one event, all were of mild-to-moderate severity; one patient in the dupilumab q2w group discontinued treatment due to moderate bacterial conjunctivitis. In contrast, exacerbation of atopic dermatitis occurred in approximately twice as many placebo-treated patients (14.2%) than in either dupilumab treatment group (8.2% [q2w] and 6.7% [q4w]).
Dupilumab-treated patients vs placebo-treated patients also had lower incidences of systemic infections, skin infections, and herpes virus infections, as well as reduced incidence of exacerbation of other type 2 inflammatory diseases (Table 2 and Figure 4).
 |
Figure 4 Rate of infections and skin infections in LIBERTY AD PEDS (NCT03345914). Abbreviations: MedDRA, Medical Dictionary for Regulatory Activities; SOC, MedDRA system organ class; TCS, topical corticosteroids, q2w, every 2 weeks; q4w, every 4 weeks. |
Laboratory outcomes from LIBERTY AD PEDS indicate no need for routine laboratory monitoring of children aged 6–11 years treated with dupilumab plus TCS for severe AD.56
AD and Other Type 2 Inflammatory Conditions
As stated previously, most children with AD have at least one type 2 comorbidity, irrespective of disease severity.2,4,22,23 The shared pathophysiology between type 2 conditions provides a compelling rationale for treatments targeting their underlying type 2 inflammatory processes.57 Indeed, in adults with moderate-to-severe AD and comorbid asthma and/or chronic sino-nasal conditions, dupilumab significantly improved the signs and symptoms of all three diseases in a clinically meaningful manner.58 Post hoc analyses of LIBERTY AD PEDS have also shown that dupilumab with concomitant TCS significantly improved the signs and symptoms of severe AD in children aged 6–11 years with and without comorbid asthma59 or comorbid AR,60 although no data were collected during these studies with respect to the efficacy of dupilumab on comorbid asthma or AR directly. This demonstrates that the efficacy of dupilumab on AD disease parameters is maintained irrespective of the presence of comorbid atopic conditions and, as with adults, is likely to benefit comorbid conditions that share a common underlying mechanism.
Discussion and Future Perspectives
Severe AD has a multidimensional patient burden and can have significantly negative impacts on the physical and psychosocial development of children aged 6–11 years. Prior to dupilumab’s approval, few effective treatment options that were suitable for long-term use existed for these patients, resulting in a significant unmet need in this population.
Currently, the clinical experience of these patients with dupilumab administered either open-label up to 52 weeks or for 16 weeks in a placebo-controlled Phase III trial is consistent with those of adults and adolescents.47–52 Rapid, sustained, and long-term improvements were observed in signs and symptoms of AD and patient quality of life. Given the high prevalence of comorbidities in children aged 6–11 years with AD, dupilumab treatment offers the potential added benefit of treating these comorbidities as well.
The lower incidence of infections with dupilumab treatment compared with placebo is likely due to its targeted action on IL-4 and IL-13, key type 2 inflammation cytokines that drive skin barrier dysfunction. It has been demonstrated that dupilumab treatment normalizes the skin barrier, including Staphylococcus aureus colonization, in both lesional and non-lesional skin.13–16 Another benefit of specifically targeting type 2 inflammation is that the human body’s defenses against bacteria, viruses, and fungi are not affected, as is observed with the use of broad immunosuppressors (including JAK inhibitors).
Needle phobia, which can interfere with treatment in some of the patients in this age group, can be substantially reduced or cured by cognitive behavioral therapy. In addition, needle-hiding devices have become available to address this problem. Moreover, the lack of required lab monitoring during treatment with dupilumab is valuable for these patients.
A technical limitation of the paper is that clinical data of placebo-controlled dupilumab treatment beyond 16 weeks in the pediatric population is not available. However, the results consistently show a positive impact of dupilumab in the treatment of AD in this population.
The data suggest that dupilumab offers an effective treatment option for children aged 6–11 years with severe AD and support its use as a continuous long-term treatment in this age group.
Abbreviations
AD, atopic dermatitis; AR, allergic rhinitis; BSA, body surface area; CDLQI, Children’s Dermatology Life Quality Index; CI, confidence interval; DFI, dermatitis family impact; EASI, Eczema Area and Severity Index; EASI-50/75/90, ≥50%/75%/90% improvement from baseline in EASI; HLT, MedDRA High-Level Term; IGA, Investigator’s Global Assessment; JAK, Janus kinase; MedDRA, Medical Dictionary for Regulatory Activities; N/A, not available; NRS, Numerical Rating Scale; NSISS, systemic non-steroidal immunosuppressants; OLE, open-label extension; OR, odds rate; POEM, Patient-Oriented Eczema Measure; PP-NRS, Peak Pruritus Numerical Rating Scale; PT, MedDRA Preferred Term; q2w, every 2 weeks; q4w, every 4 weeks; qw, weekly; SCORAD, SCORing Atopic Dermatitis; SD, standard deviation; SE, standard error; SOC, MedDRA System Organ Class; TCS, topical corticosteroids; TEAE, treatment-emergent adverse event; VAS, Visual Analog Scale.
Data Sharing Statement
No original data are reported in this article.
Acknowledgments
ClinicalTrials.gov Identifiers: NCT02407756, NCT03346434, NCT02612454, NCT03054428, NCT03345914. The study sponsors participated in the writing of the report and the decision to submit the article for publication. Medical writing/editorial assistance was provided by Lola MacRae, PhD, and Carolyn Ellenberger, PhD, of Excerpta Medica, and was funded by Sanofi and Regeneron Pharmaceuticals Inc., according to the Good Publication Practice guidelines. Spider gram and rainbow graphics were developed by Ana B. Rossi and Marthe Vuillet of Sanofi.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Research sponsored by Sanofi and Regeneron Pharmaceuticals Inc.
Disclosure
Professor Michael J Cork has served as a consultant and/or advisory board member and/or received research grants from Almirall, Amgen, Astellas Pharma, Bayer, GSK, Hyphens Pharma, Johnson & Johnson, LEO Pharma, L’Oréal, Novartis, Perrigo, Pfizer, Procter & Gamble, Sanofi, Stiefel, Regeneron Pharmaceuticals Inc., and Unilever. Professor Michael J Cork is a voluntary medical advisor to the National Eczema Society UK.
Dr Simon G Danby reports grants from Sanofi, Almirall, Johnson & Johnson, and Leo Pharma; grants, personal fees from Perrigo, Pfizer, and Hyphens Pharma, outside the submitted work.
Dr Ana B. Rossi is an employee of and may hold stock and/or stock options in Sanofi.
Dr Ashish Bansal is an employee and shareholder of Regeneron Pharmaceuticals Inc.
References
1. Silverberg JI, Barbarot S, Gadkari A, et al. Atopic dermatitis in the pediatric population: a cross-sectional, international epidemiologic study. Ann Allergy Asthma Immunol. 2021;126(4):417–428.e2. doi:10.1016/j.anai.2020.12.020
2. Paller AS, Guttman-Yassky E, Schuttelaar ML, et al. Disease characteristics, comorbidities, treatment patterns and quality of life impact in children <12 years old with atopic dermatitis: interim results from the PEDISTAD real-world registry. J Am Acad Dermatol. 2022;87(5):1104–1108. doi:10.1016/j.jaad.2022.01.018
3. Barbarot S, Silverberg JI, Gadkari A, et al. The family impact of atopic dermatitis in the pediatric population: results from an international cross-sectional study. J Pediatr. 2022;246:220–226.e5. doi:10.1016/j.jpeds.2022.04.027
4. Silverberg JI, Simpson EL, Weidinger S, et al. Children with atopic dermatitis (AD) have a high burden of atopic comorbidities: results from a large worldwide survey. J Allergy Clin Immunol. 2021;147(2):AB31. doi:10.1016/j.jaci.2020.12.149
5. Sidbury R, Davis DM, Cohen DE, et al. Guidelines of care for the management of atopic dermatitis: section 3. Management and treatment with phototherapy and systemic agents. J Am Acad Dermatol. 2014;71(2):327–349. doi:10.1016/j.jaad.2014.03.030
6. Wollenberg A, Kinberger M, Arents B, et al. European guideline (EuroGuiDerm) on atopic eczema: part I - systemic therapy. J Eur Acad Dermatol Venereol. 2022;36(9):1409–1431. doi:10.1111/jdv.18345
7. Wollenberg A, Kinberger M, Arents B, et al. European guideline (EuroGuiDerm) on atopic eczema - part II: non-systemic treatments and treatment recommendations for special AE patient populations. J Eur Acad Dermatol Venereol. 2022;36(11):1904–1926. doi:10.1111/jdv.18429
8. Drucker AM, Eyerich K, de Bruin-Weller MS, et al. Use of systemic corticosteroids for atopic dermatitis: international Eczema Council consensus statement. Br J Dermatol. 2018;178(3):768–775. doi:10.1111/bjd.15928
9. Senner S, Seegräber M, Frey S, Kendziora B, Eicher L, Wollenberg A. Dupilumab for the treatment of adolescents with atopic dermatitis. Expert Rev Clin Immunol. 2020;16(7):641–650. doi:10.1080/1744666X.2020.1801420
10. Simpson EL, Bruin-Weller M, Flohr C, et al. When does atopic dermatitis warrant systemic therapy? Recommendations from an expert panel of the International Eczema Council. J Am Acad Dermatol. 2017;77(4):623–633. doi:10.1016/j.jaad.2017.06.042
11. U.S. Food and Drug Administration. Dupilumab, Highlights of Prescribing Information; 2022. Available from: https://www.regeneron.com/downloads/dupixent_fpi.pdf.
12. European Medicines Agency. Dupilumab Summary of Product Characteristics. Available from: https://www.ema.europa.eu/en/documents/product-information/dupixent-epar-product-information_en.pdf.
13. Beck LA, Cork MJ, Amagai M, et al. Type 2 inflammation contributes to skin barrier dysfunction in atopic dermatitis. JID Innov. 2022;2(5):100131. doi:10.1016/j.xjidi.2022.100131
14. Bissonette R, Leung DYM, Bologna G, Levit NA, Rossi AB, Zhang A. Dupilumab treatment restores skin barrier function and improves clinical and patient reported outcomes in adults and adolescents with moderate to severe atopic dermatitis. J Am Acad Dermatol. 2022;87(Suppl 3):AB160. doi:10.1016/j.jaad.2022.06.670
15. Berdyshev E, Goleva E, Bissonnette R, et al. Dupilumab significantly improves skin barrier function in patients with moderate-to-severe atopic dermatitis. Allergy. 2022;77(11):3388–3397. doi:10.1111/all.15432
16. Callewaert C, Nakatsuji T, Knight R, et al. IL-4Rα blockade by dupilumab decreases Staphylococcus aureus colonization and increases microbial diversity in atopic dermatitis. J Invest Dermatol. 2020;140(1):191–202.e7. doi:10.1016/j.jid.2019.05.024
17. Lee S-J, Kim S-E, Shin K-O, Park K, Lee SE. Dupilumab therapy improves stratum corneum hydration and skin dysbiosis in patients with atopic dermatitis. Allergy Asthma Immunol Res. 2021;13(5):762–775. doi:10.4168/aair.2021.13.5.762
18. Charman CR, Venn AJ, Williams HC. The patient-oriented eczema measure: development and initial validation of a new tool for measuring atopic eczema severity from the patients’ perspective. Arch Dermatol. 2004;140(12):1513–1519. doi:10.1001/archderm.140.12.1513
19. Kim JP, Chao LX, Simpson EL, Silverberg JI. Persistence of atopic dermatitis (AD): a systematic review and meta-analysis. J Am Acad Dermatol. 2016;75(4):681–687.e11. doi:10.1016/j.jaad.2016.05.028
20. Abuabara K, Ye M, Margolis DJ, et al. Patterns of atopic eczema disease activity from birth through midlife in 2 British birth cohorts. JAMA Dermatol. 2021;157(10):1191–1199. doi:10.1001/jamadermatol.2021.2489
21. Huang A, Cho C, Leung DYM, Brar K. Atopic dermatitis: early treatment in children. Curr Treat Options Allergy. 2017;4(3):355–369. doi:10.1007/s40521-017-0140-6
22. Silverberg JI, Simpson EL. Association between severe eczema in children and multiple comorbid conditions and increased healthcare utilization. Pediatr Allergy Immunol. 2013;24(5):476–486. doi:10.1111/pai.12095
23. Weidinger S, Simpson EL, Eckert L, et al. 15115 The patient-reported disease burden in pediatric patients with atopic dermatitis: a cross-sectional study in the United States, Canada, Europe, and Japan. J Am Acad Dermatol. 2020;83(Suppl 6):AB29. doi:10.1016/j.jaad.2020.06.203
24. Drucker AM, Wang AR, Li W-Q, Sevetson E, Block JK, Qureshi AA. The burden of atopic dermatitis: summary of a report for the national eczema association. J Invest Dermatol. 2017;137(1):26–30. doi:10.1016/j.jid.2016.07.012
25. Kruse LL, Cices A, Fishbein AB, Paller AS. Neurocognitive function in moderate-severe pediatric atopic dermatitis: a case-control study. Pediatr Dermatol. 2019;36(1):110–114. doi:10.1111/pde.13710
26. Wan J, Mitra N, Hooper SR, Hoffstad OJ, Margolis DJ. Association of atopic dermatitis severity with learning disability in children. JAMA Dermatol. 2021;157(6):1–7. doi:10.1001/jamadermatol.2021.0008
27. Hou A, Silverberg JI. Predictors and age-dependent pattern of psychologic problems in childhood atopic dermatitis. Pediatr Dermatol. 2021;38(3):606–612. doi:10.1111/pde.14588
28. Keller W, Vogel M, Prenzel F, et al. Atopic diseases in children and adolescents are associated with behavioural difficulties. BMC Pediatr. 2021;21(1):197. doi:10.1186/s12887-021-02663-7
29. Vittrup I, Andersen YMF, Droitcourt C, et al. Association between hospital-diagnosed atopic dermatitis and psychiatric disorders and medication use in childhood. Br J Dermatol. 2021;185(1):91–100. doi:10.1111/bjd.19817
30. Paller AS, Guttman-Yassky E, Irvine AD, et al. Protocol for a prospective, observational, longitudinal study in paediatric patients with moderate-to-severe atopic dermatitis (PEDISTAD): study objectives, design and methodology. BMJ Open. 2020;10(3):e033507. doi:10.1136/bmjopen-2019-033507
31. Capozza K, Gadd H, Kelley K, Russell S, Shi V, Schwartz A. Insights from caregivers on the impact of pediatric atopic dermatitis on families: ‘I’m tired, overwhelmed, and feel like I’m failing as a mother’. Dermatitis. 2020;31(3):223–227. doi:10.1097/DER.0000000000000582
32. Mitchell AE. Bidirectional relationships between psychological health and dermatological conditions in children. Psychol Res Behav Manag. 2018;11:289–298. doi:10.2147/PRBM.S117583
33. de Bruin-Weller M, Schuttelaar M, Lynde CW, et al. Family impact of moderate-to-severe atopic dermatitis in children aged <12 years: results from 732 patients in the PEDIatric STudy in Atopic Dermatitis (PEDISTAD) observational study. J Am Acad Dermatol. 2022;87(Suppl 3):AB168. doi:10.1016/j.jaad.2022.06.703
34. Silverberg JI. Public health burden and epidemiology of atopic dermatitis. Dermatol Clin. 2017;35(3):283–289. doi:10.1016/j.det.2017.02.002
35. Cork MJ, Danby SG, Ogg GS. Atopic dermatitis epidemiology and unmet need in the United Kingdom. J Dermatolog Treat. 2020;31(8):801–809. doi:10.1080/09546634.2019.1655137
36. Simpson EL, Bieber T, Eckert L, et al. Patient burden of moderate to severe atopic dermatitis (AD): insights from a phase 2b clinical trial of dupilumab in adults. J Am Acad Dermatol. 2016;74(3):491–498. doi:10.1016/j.jaad.2015.10.043
37. Shrestha S, Miao R, Wang L, Chao J, Yuce H, Wei W. Burden of atopic dermatitis in the United States: analysis of healthcare claims data in the commercial, Medicare, and Medi-Cal databases. Adv Ther. 2017;34(8):1989–2006. doi:10.1007/s12325-017-0582-z
38. Eckert L, Gupta S, Amand C, Gadkari A, Mahajan P, Gelfand JM. The burden of atopic dermatitis in US adults: health care resource utilization data from the 2013 National Health and Wellness Survey. J Am Acad Dermatol. 2018;78(1):54–61.e1. doi:10.1016/j.jaad.2017.08.002
39. Lucae S, Schmidt-Grendelmeier P, Wütrich B, Kraft D, Valenta R, Linhart B. IgE responses to exogenous and endogenous allergens in atopic dermatitis patients under long-term systemic cyclosporine A treatment. Allergy. 2016;71(1):115–118. doi:10.1111/all.12711
40. Hijnen DJ, Knol E, Bruijnzeel-Koomen C, de Bruin-Weller M. Cyclosporin A treatment is associated with increased serum immunoglobulin E levels in a subgroup of atopic dermatitis patients. Dermatitis. 2007;18(3):163–165. doi:10.2310/6620.2007.06025
41. Vakharia PP, Silverberg JI. New and emerging therapies for paediatric atopic dermatitis. Lancet Child Adolesc Health. 2019;3(5):343–353. doi:10.1016/S2352-4642(19)30030-6
42. Furue M, Terao H, Rikihisa W, et al. Clinical dose and adverse effects of topical steroids in daily management of atopic dermatitis. Br J Dermatol. 2003;148(1):128–133. doi:10.1046/j.1365-2133.2003.04934.x
43. Furue M, Terao H, Moroi Y, et al. Dosage and adverse effects of topical tacrolimus and steroids in daily management of atopic dermatitis. J Dermatol. 2004;31(4):277–283. doi:10.1111/j.1346-8138.2004.tb00673.x
44. Roekevisch E, Spuls PI, Kuester D, Limpens J, Schmitt J. Efficacy and safety of systemic treatments for moderate-to-severe atopic dermatitis: a systematic review. J Allergy Clin Immunol. 2014;133(2):429–438. doi:10.1016/j.jaci.2013.07.049
45. Nguyen HL, Anderson KR, Tollefson MM. New and emerging therapies for pediatric atopic dermatitis. Paediatr Drugs. 2019;21(4):239–260. doi:10.1007/s40272-019-00342-w
46. Haddad E-B, Cyr SL, Arima K, McDonald RA, Levit NA, Nestle FO. Current and emerging strategies to inhibit type 2 inflammation in atopic dermatitis. Dermatol Ther. 2022;12(7):1501–1533. doi:10.1007/s13555-022-00737-7
47. Simpson EL, Bieber T, Guttman-Yassky E, et al. Two phase 3 trials of dupilumab versus placebo in atopic dermatitis. N Engl J Med. 2016;375(24):2335–2348. doi:10.1056/NEJMoa1610020
48. Blauvelt A, de Bruin-Weller M, Gooderham M, et al. Long-term management of moderate-to-severe atopic dermatitis with dupilumab and concomitant topical corticosteroids (LIBERTY AD CHRONOS): a 1-year, randomised, double-blinded, placebo-controlled, phase 3 trial. Lancet. 2017;389(10086):2287–2303. doi:10.1016/S0140-6736(17)31191-1
49. de Bruin-Weller M, Thaçi D, Smith CH, et al. Dupilumab with concomitant topical corticosteroid treatment in adults with atopic dermatitis with an inadequate response or intolerance to ciclosporin A or when this treatment is medically inadvisable: a placebo-controlled, randomized phase III clinical trial (LIBERTY AD CAFÉ). Br J Dermatol. 2018;178(5):1083–1101. doi:10.1111/bjd.16156
50. Cork MJ, Thaçi D, Eichenfield LF, et al. Dupilumab in adolescents with uncontrolled moderate-to-severe atopic dermatitis: results from a phase IIa open-label trial and subsequent phase III open-label extension. Br J Dermatol. 2020;182(1):85–96. doi:10.1111/bjd.18476
51. Paller AS, Bansal A, Simpson EL, et al. Clinically meaningful responses to dupilumab in adolescents with uncontrolled moderate-to-severe atopic dermatitis: post-hoc analyses from a randomized clinical trial. Am J Clin Dermatol. 2020;21(1):119–131. doi:10.1007/s40257-019-00478-y
52. Simpson EL, Paller AS, Siegfried EC, et al. Efficacy and safety of dupilumab in adolescents with uncontrolled moderate to severe atopic dermatitis: a phase 3 randomized clinical trial. JAMA Dermatol. 2020;156(1):44–56. doi:10.1001/jamadermatol
53. Paller AS, Simpson EL, Siegfried EC, et al. Dupilumab in children aged 6 months to younger than 6 years with uncontrolled atopic dermatitis: a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2022;400(10356):908–919. doi:10.1016/S0140-6736(22)01539-2
54. Cork MJ, Thaçi D, Eichenfield LF, et al. Dupilumab provides favourable long-term safety and efficacy in children aged ≥ 6 to < 12 years with uncontrolled severe atopic dermatitis: results from an open-label phase IIa study and subsequent phase III open-label extension study. Br J Dermatol. 2021;184(5):857–870. doi:10.1111/bjd.19460
55. Paller AS, Siegfried EC, Thaçi D, et al. Efficacy and safety of dupilumab with concomitant topical corticosteroids in children 6 to 11 years old with severe atopic dermatitis: a randomized, double-blinded, placebo-controlled phase 3 trial. J Am Acad Dermatol. 2020;83(5):1282–1293. doi:10.1016/j.jaad.2020.06.054
56. Paller AS, Wollenberg A, Siegfried E, et al. Laboratory safety of dupilumab in patients aged 6 to 11 years with severe atopic dermatitis: results from a phase III clinical trial. Paediatr Drugs. 2021;23(5):515–527. doi:10.1007/s40272-021-00459-x
57. Laidlaw TM, Mullol J, Woessner KM, Amin N, Mannent LP. Chronic rhinosinusitis with nasal polyps and ASTHMA. J Allergy Clin Immunol Pract. 2021;9(3):1133–1141. doi:10.1016/j.jaip.2020.09.063
58. Boguniewicz M, Beck LA, Sher L, et al. Dupilumab improves asthma and sinonasal outcomes in adults with moderate to severe atopic dermatitis. J Allergy Clin Immunol Pract. 2021;9(3):1212–1223.e6. doi:10.1016/j.jaip.2020.12.059
59. Boguniewicz M, Sher L, Paller A, et al. Dupilumab improves signs and symptoms of severe atopic dermatitis in children aged 6–11 years with and without comorbid asthma. J Allergy Clin Immunol. 2021;147(Suppl 2):AB32. doi:10.1016/j.jaci.2020.12.151
60. Beck LA, Wollenberg A, Paller A, et al. Dupilumab improves signs and symptoms of severe atopic dermatitis in children aged 6–11 years with and without comorbid allergic rhinitis. J Allergy Clin Immunol. 2021;147(Suppl 2):AB144. doi:10.1016/j.jaci.2020.12.523
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.