")
Back to Journals » International Journal of General Medicine » Volume 17
Door-to-Balloon Time and Mortality Among Patients Undergoing Primary PCI, Challenges and Experience from Somalia’s Largest PCI Center
Authors Hassan MO , Ahmed SA , Hassan MS , Köprülü D
Received 21 November 2023
Accepted for publication 17 January 2024
Published 22 January 2024 Volume 2024:17 Pages 237—244
DOI https://doi.org/10.2147/IJGM.S448750
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Prof. Dr. Yuriy Sirenko
Mohamed Omar Hassan,1 Said Abdirahman Ahmed,1 Mohamed Sheikh Hassan,2 Diyar Köprülü1
1Department of Cardiology, Mogadishu Somali Turkish Training and Research Hospital, Mogadishu, Somalia; 2Department of Neurology, Mogadishu Somali Turkish Training and Research Hospital, Mogadishu, Somalia
Correspondence: Mohamed Omar Hassan, Email [email protected]
Introduction: The door-to-balloon time, the time between a patient’s arrival at the hospital and percutaneous coronary intervention, is crucial for managing myocardial infarction. Aiming for less than 90 minutes is recommended, as shortened times are associated with improved outcomes. However, limited healthcare resources, infrastructure, transportation and poverty impact management, leading to poorer outcomes and delayed door to balloon time. Addressing these challenges and their causes is essential for optimal care.
Methodology: A retrospective analysis of 103 patients’ medical history records from May 2022 to June 2023 at the Mogadishu Somali Turkish Training and Research Hospital in Somalia was conducted. The data was mainly collected from the hospital’s electronic medical records system, analyzing patient demographics, clinical characteristics, and angiographical records. The study analyzed variables responsible for door-to-balloon (D2B) time delay, patient angiography results, cause of delay, procedure length, etc.
Results: A study of 103 patients who had angiography performed between May 2022 and July 2023 was done. The predominant gender in the study was 73% male, with a mean age of 58 years. The most common risk factors were hypertension (33%), smoking (38%), and diabetes (39%). Of all the vessels, the Left Anterior Descending (LAD) was the most commonly obstructed (63%). Time delays from door-to-balloon were frequent, median door-to-balloon time was 169 minutes, frequently brought on by social problems and financial limitations. The majority (77.4%) of the patients had only percutaneous angiography (PCI), while 22.6% were recommended for bypass following PCI of the infarct-related artery (IRA). Complications in the delayed treatment group were the main cause of the death rate of 24.2%.
Conclusion: Door-to-balloon time is crucial for acute myocardial infarction treatment which is challenging in impoverished countries like Somalia. Investments in healthcare infrastructure, public health education, and emergency services can improve patient outcomes.
Keywords: door-to-balloon time, Somalia, myocardial infarction, ST segment elevation myocardial infarction
Introduction
Door-to-balloon time refers to the time between a patient’s arrival at the hospital and the initiation of PCI to restore blood flow to the blocked artery. This is an essential aspect of managing myocardial infarction (MI). The ideal door-to-balloon time for STEMI (ST-segment elevation myocardial infarction) varies depending on the references given. It is advised to aim for a door-to-balloon time of less than 90 minutes, according to several studies.1,2
“Acute coronary syndrome” (ACS) refers to a group of myocardial ischemia diseases that have a common cause.3 ACS can manifest as either STEMI or NSTEMI (non-ST-segment elevation myocardial infarction), which both include a blockage of blood flow to the heart muscle. Unstable angina, NSTEMI, and STEMI are only a few of the manifestations that fall under the umbrella of the clinical emergency condition known as ACS.4
The objective is to minimize this time as much as possible, as research indicates that shortened door-to-balloon times are associated with improved outcomes and lower mortality rates.5,6 If not intervened within the necessary time, ischemia-induced irreparable damage and limited regenerative potential in adult mammalian hearts often lead to pathological LV remodeling and progressive cardiac dysfunction.7
Coronary artery disease (CAD) is a significant public health concern in Somalia. CAD is frequently the underlying cause of myocardial infarction. However, optimal management of CAD and MI in Somalia is difficult due to limited healthcare resources, a lack of infrastructure, and the impacts of poverty on healthcare access and affordability. Poverty has a variety of implications on the most effective way to handle CAD and MI in Somalia. Access to healthcare services, including prompt diagnosis and treatment, can be restricted by poverty. Additionally, it may have an impact on the cost of treatments and medications, which could result in less effective management and poorer outcomes.1 Furthermore, a larger burden of CAD risk factors, such as a poor diet, inactivity, and restricted access to preventative care, may be associated with impoverishment.8 In addition, a lack of knowledge hinders the optimal management of this condition and the recognition of its dangers. In this article, the challenges, characteristics, and outcomes of delayed door-to-balloon presentations, as well as methods for improving them, are discussed.
Methodology
Study Design and Setting
We performed a retrospective analysis. From May 2022 to June 2023, 103 patients’ medical history records were obtained from electronic medical records (EMRs), Angiography images, and equipment records at the Mogadishu Somali Turkish Training and Research Hospital in Mogadishu, Somalia.
Data Collection and Assessment
The study collected data from the hospital’s electronic medical records system, including patient demographics, clinical characteristics, and medical history. Angiographical records were analyzed to assess diseased vessels, contrast used, balloon time, access site, stents used, radiation dose, and other procedures during primary PCI. Patients with STEMI were included, excluding those receiving thrombolytics, having a STEMI in the hospital, or having an undetermined arrival time.
Statistical Analysis
The percentages of the variables responsible for the door-to-balloon time delay were reported. In addition, we gathered information on patient angiography results, D2B time, length of the procedure, complications, hemodynamic status, interventions performed, stent size used, number of stents, and mortality rate. All variables were analyzed using SPSS Var 23.0 software for statistical analysis. Calculated descriptive statistics were presented as means and standard deviations. The median was calculated for continuous variables such as door-to-balloon time in minutes. While other variables, such as gender, hypertension, diabetes, dyslipidemia, previous myocardial infarction, renal failure, and smoking, are reported in percentages.
Ethical Consideration
Due to the fact that our hospital is a research hospital, a general informed consent is obtained from every patient admitted to obtain their data for retrospective research purposes from the hospital medical records, and this study did not disclose any personal information. The study was approved by the research ethics committee of Mogadishu Somali Turkey Training and Research Hospital (Ethics Protocol No: MSTH/14848). The study was performed in line with the principles of the Declaration of Helsinki.
Results
From May 2022 to July 2023, 103 patients who had angiography at Mogadishu Somali Turkish Training and Research Hospital and fulfilled the inclusion criteria were enrolled in the study. Females accounted for 28 (27%), while men accounted for 75 (73%). The mean age (standard deviation) of the 103 patients was 58±13.6, and most of the patients were in the 50–60 age group. The most prevalent risk factor was diabetes 40 (39%), followed by smoking 39 (38%), and hypertension 34 (33%). Table 1 summarizes demographic characteristics and risk factors. The majority of the patients, 69 (67%), had anterior STEMI, and 31 (30%) had inferior STEMI (see Figure 1). The majority (77.4%) of the patients had only PCI, while 22.6% were recommended for bypass following PCI of the IRA. In terms of Culprit vessel involvement, LAD was the most occluded vessel, 65 (63%), followed by RCA 22 (21.4%). Table 2 shows the culprit vessel among different patients. Regarding door-to-balloon time, the majority of patients were in delay time group 63 (61.2%) vs 40 (38.8%). As shown in Figure 2, the most common reason for delay was social issues, mainly lack of education and awareness about the dangers of myocardial infarction and also lack of trust in the doctor’s diagnosis (see Figure 3). Financial issues accounted for the second-most common cause of delay. Lastly, the medical delay group included patients who were unstable at the time of PCI and whose other interventions or procedures were more emergent at the time. Other issues for delay include medical conditions that prevent early intervention due to the lack of mechanical support devices. The average contrast and radiation exposure doses were 30±15 cc and 430±20 g, respectively. The mean stent diameter was 3.0 ± 0.5 mm, and the mean stent length was 18.0 ± 7.0 mm. Furthermore, the average number of stents used per procedure was 1.37. The total average duration of the procedure was 18 minutes. Sadly, the total mortality rate was 25 (24.2%), which only included one person from the no delay group. The remaining percentage comes from the delayed time group as a result of myocardial complications such as cardiogenic shock, pulmonary oedema, heart failure, and other mechanical complications. The mortality rate for the delayed door-to-balloon time group is approximately 38.10%. While for the on-time group it was 2.5%.
 |
Table 1 Summarizes Demographic Characteristics and Risk Factors |
 |
Table 2 Shows Pattern of Vascular Involvement Among Different Patients |
 |
Figure 1 Shows electrocardiographic and echocardiographic location of STEMI. Abbreviation: STEMI, ST segment elevation myocardial infarction. |
 |
Figure 2 Demonstrates the percentage of delayed vs non delayed door-to-balloon time. |
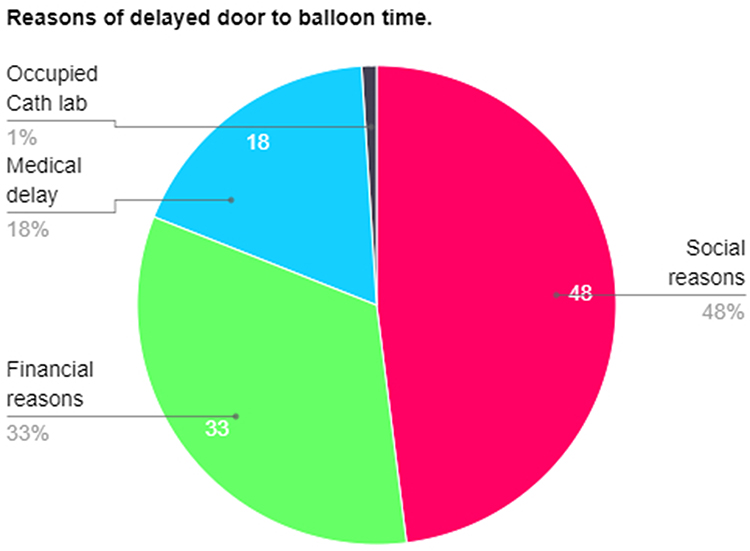 |
Figure 3 Shows reasons of delayed door-to-balloon time among patients. |
Discussion
Door-to-balloon time is significant since it directly affects patient outcomes. A shorter door-to-balloon time has been linked in multiple studies to better clinical results, such as decreased mortality and recurrent MI rates.9 Efforts to reduce the time it takes to transport a patient from the door to the balloon should be implemented for all patients, as research has demonstrated that this is more strongly linked to mortality than the time between the onset of symptoms and the balloon procedure.10
The American College of Cardiology and the American Heart Association recommend a door-to-balloon time of 90 minutes or less for patients with STEMI.5 It is imperative that this target time be met because delays in beginning reperfusion therapy might result in irreparable damage to the myocardium and a worse prognosis.9 The significance of door-to-balloon time as a metric for evaluating performance is emphasized by its submission to the Centers for Medicare & Medicaid Services (CMS) and its connection to the evaluation of hospital quality and reimbursement.11
Reaching the suggested door-to-balloon time, however, can prove difficult, particularly in nations like Somalia where poverty and safety issues are widespread. For instance, a comparable study was conducted with a sample of 45 patients in Kenya, which is thought to be far more stable and developed than Somalia.
It was discovered that door-to-needle time of less than 30 minutes was reached in 43% of the instances. 29% of the instances had door-to-balloon times less than 90 minutes. Every patient lived to be discharged from the hospital.12
Timely management of MI cases is severely hampered by poor access to specialized cardiac care facilities, a lack of resources, and a limited healthcare infrastructure. A primary challenge to meeting the door-to-balloon time in Somalia is the absence of adequately equipped cardiac care facilities and skilled emergency medical personnel. Emergency medical personnel significantly reduce door-to-balloon Time for STEMI patients through early identification, triage, and management, exemplified by prehospital ECGs.13
The scarcity of cardiac catheterization laboratories and qualified interventional cardiologists makes it challenging to administer PCI to MI patients in a timely manner. For contrast, the percentage of South Africans who reside 60 or 120 minutes away from a PCI facility is roughly 53.8 and 71.53%, respectively.14
This is not the case in Somalia where all the available centers are only in the capital city of Mogadishu. Furthermore, the problems are made worse in Somalia, where poverty and safety concerns are common. This can be seen in the results of our study, which shows more than 61% of the patients had a delay in the door-to-balloon time of more than 90 minutes, and the high mortality rate of 24% almost all of whom were in the delayed group. A study conducted in the United States found that the median time from door-to-balloon was 83 minutes.15 Another European study reported a median door-to-balloon time of 60 minutes.16 However, in our study it was 169 minutes. In the United States and Europe, the time from door-to-balloon (D2B) for percutaneous coronary intervention (PCI) is shorter for a number of reasons. An important factor in the effective management of STEMI patients is the presence of well-established healthcare infrastructure and resources in these areas. Furthermore, the standardized approach to emergencies in hospitals and the presence of regional integrated care and emergency medical services in these countries make it easier for STEMI patients to be quickly transported to hospitals that can perform PCI within the recommended time frame, thereby lowering D2B times.17
In addition, studies have repeatedly found a link between longer door-to-balloon times and higher death rates. For example, in one study, in a continuous, nonlinear fashion, longer door-to-balloon times were associated with higher one-year mortality (30 minutes: 10.9%, 60 minutes: 13.6%, 90 minutes: 16.5%, 120 minutes: 19.5%, 150 minutes: 22.5%, 180 minutes: 25.3%, 210 minutes: 27.3%).18 Our study showed a comparable percentage of mortality for our median door-to-balloon time.
The start of treatment is further delayed by the general lack of knowledge about MI symptoms, their significance, and the necessity of obtaining prompt medical help. In one study carried on Mogadishu 53.35% of participants lacked sufficient knowledge about myocardial infarction.19
For time-sensitive situations like STEMI, educational programs are very important for making people more aware of and knowledgeable about how important it is to get medical help right away. A lack of knowledge about STEMI reduces the urgency to get help and be seen, which stresses the importance of educational programs to deal with these issues.20
Furthermore, another huge issue is the lack of funds. Patients and health providers both face the challenge of financial difficulties. As the equipment for a PCI procedure are scarce and expensive, health providers find themselves in a difficult situation. For instance, a study pointed out that people in Sub-Saharan Africa do not have easy access to expensive treatments like PCI devices. This means that people in this area have trouble getting advanced and expensive treatments for coronary artery disease.21
Currently, no governmental or organizational support exists for these procedures and there is no easily accessible public health insurance system. Several strategies can be implemented to reduce the time from door-to-balloon in Somalia. First, investments in healthcare infrastructure, including the establishment of well-equipped coronary care centers and the training of healthcare professionals in interventional cardiology, are required. This would increase the accessibility and availability of PCI services, thereby decreasing the time required to initiate treatment. Second, public health campaigns and community education programs should be implemented to increase awareness of the symptoms of MI and the significance of seeking immediate medical care. This would reduce delays in seeking medical care and enhance the likelihood that patients would arrive at the hospital within the optimal time window for PCI. Thirdly, emergency medical services should be made more accessible and efficient. This can be accomplished by establishing a well-coordinated emergency medical service system outfitted with ambulances and trained paramedics to provide prompt pre-hospital care and transport of MI patients to cardiac care centers.
Limitations of Our Study
The small number of patients included in the study is a major limitation of this research on door-to-balloon time in the therapy of STEMI in Somalia. Because of this, the sample size might not accurately reflect the larger STEMI community in Somalia, which could restrict how broadly the study’s conclusions can be applied. Additionally, a limitation related to the broader context of the study is the trivial number of comparable results for door-to-balloon time in other African countries.
Conclusion
Door-to-balloon time is integral to acute myocardial infarction treatment, with heightened challenges in impoverished nations like Somalia. This study illuminates the complexities faced in achieving timely interventions, emphasizing the need for targeted investments in healthcare infrastructure, public health education, and emergency services. Despite acknowledged limitations, our findings contribute to the ongoing discourse on MI management in resource-limited settings, underscoring the urgent need for comprehensive interventions to enhance patient outcomes.
Abbreviations
MI, Myocardial Infarction; 2. D2B, Door-to-Balloon Time; 3. PCI, Percutaneous Coronary Intervention; 4. STEMI, ST-Segment Elevation Myocardial Infarction; 5. ACS, Acute Coronary Syndrome; 6. IRA, Infarct-Related Artery; 7. LAD, Left Anterior Descending (Artery); 8. RCA, Right Coronary Artery; 9. CKD, Chronic Kidney Disease; 10. DM, Diabetes Mellitus; 11. IMA, Intermediate Artery; 12. LCX, Left Circumflex Artery; 13. LMCA, Left Main Coronary.
Ethical Consideration
Due to the fact that our hospital is a research hospital, a general informed consent is obtained from every patient admitted to obtain their data for retrospective research purposes from the hospital medical records, and this study did not disclose any personal information. The study was approved by the research ethics committee of Mogadishu Somali Turkey Training and Research Hospital (Ethics Protocol No: MSTH/14848). The study was performed in line with the principles of the Declaration of Helsinki.
Funding
No funding to be disclosed.
Disclosure
The authors declare there is no conflict of interest.
References
1. Prior P, Gray WA. The remnant of our success. Catheterization Cardiovasc Interventions. 2021;97(6):1118–1119. doi:10.1002/ccd.29725
2. Nissen S, Brush J, Krumholz H. President’s page: gap-d2b: an alliance for quality. J Am Coll Cardiol. 2006;48(9):1911–1912. doi:10.1016/j.jacc.2006.10.011
3. Tucker B, Patel S. Acute Coronary Syndrome: unravelling the Biology to Identify New Therapies. Cells. 2022;11(24):4136. doi:10.3390/cells11244136
4. Fu R, Song C, Dou K, et al. Differences in symptoms and pre-hospital delay among acute myocardial infarction patients according to st-segment elevation on electrocardiogram. Chine Med J. 2019;132(5):519–524.
5. Bradley E, Herrin J, Wang Y, et al. Strategies for reducing the door-to-balloon time in acute myocardial infarction. N Engl J Med. 2006;355(22):2308–2320. doi:10.1056/nejmsa063117
6. Kong P, Connolly D, Varma C, et al. High-risk myocardial infarction patients appear to derive more mortality benefit from short door-to-balloon time than low-risk patients. Int J Clin. 2009;63(12):1693–1701.
7. Kumar V, Prabhu SD, Bansal SS. CD4+ T-lymphocytes exhibit biphasic kinetics post-myocardial infarction. Front Cardiovascular Med. 2022;9:992653. doi:10.3389/fcvm.2022.992653
8. Zhou Y, Yuan J, Fan Y, et al. Proteomic landscape of human coronary artery atherosclerosis. IntJ Mol Med. 2020;46(1):371–383. doi:10.3892/ijmm.2020.4600
9. Chen F, Lin Y, Kung C, Cheng C, Li C. The association between door-to-balloon time of less than 60 minutes and prognosis of patients developing st segment elevation myocardial infarction and undergoing primary percutaneous coronary intervention. Bi. BioMed Res Int. 2017;2017:1–6. doi:10.1155/2017/1910934
10. Denktas AE, Anderson HV, McCarthy J, Smalling RW. Total ischemic time: the correct focus of attention for optimal ST-segment elevation myocardial infarction care. JACC Cardiovasc Interv. 2011;4(6):599–604. doi:10.1016/j.jcin.2011.02.012
11. McCabe JM, Kennedy KF, Eisenhauer AC, et al. Reporting trends and outcomes in ST-segment–elevation myocardial infarction national hospital quality assessment programs. Circulation. 2014;129(2):194–202. doi:10.1161/CIRCULATIONAHA.113.006165
12. Wachira BW, Owuor AO, Otieno HA. Acute management of ST-elevation myocardial infarction in a tertiary hospital in Kenya: are we complying with practice guidelines?: phase active de prise en charge des infarctus du myocarde avec élévation du segment ST dan. Af J Em Med. 2014;4(3):104.
13. Vavalle JP, Granger CB. The need for regional integrated care for ST-segment elevation myocardial infarction. Circulation. 2011;124(7):851–856. doi:10.1161/CIRCULATIONAHA.110.012617
14. Stassen W, Wallis L, Vincent-Lambert C, Castren M, Kurland L. The proportion of South Africans living within 60 and 120 minutes of a percutaneous coronary intervention facility. Cardiovascular J Africa. 2018;29(1):6–11. doi:10.5830/CVJA-2018-004
15. Cannon CP. Relationship of symptom-onset-to-balloon time and door-to-balloon time with mortality in patients undergoing angioplasty for acute myocardial infarction. JAMA. 2000;283(22):2941. doi:10.1001/jama.283.22.2941
16. Nozari Y, Geraiely B, Alipasandi K, et al. Time to treatment and in-hospital major adverse cardiac events among patients with st-segment elevation myocardial infarction who underwent primary percutaneous coronary int. JMIR Res Protocols. 2019;8(3):e13161.
17. Gadre A, Kotaru V, Mehta A, Kumar D, Rayasam V. Delayed presentation during covid-19 pandemic leading to post-myocardial infarction ventricular septal defect. Cureus. 2021. doi:10.7759/cureus.15945
18. Rathore SS, Curtis JP, Nallamothu BK, et al. Association of door-to-balloon time and mortality in patients≥ 65 years with ST-elevation myocardial infarction undergoing primary percutaneous coro. Am J Cardiol. 2009;104(9):1198–1203.
19. Hassan MO, Ahmed SA, Hassan MS, Mohamud MA, Abdi AE. Exploring Myocardial Infarction Knowledge, Attitudes, and Practice Among Mogadishu’s Somali Residents. Vasc Health Risk Manag. 2024;20:13–20. doi:10.2147/VHRM.S448220
20. Ahmed T, Lodhi S, Kapadia S, Shah G. Community and healthcare system-related factors feeding the phenomenon of evading medical attention for time-dependent emergencies during covid-19 crisis. BMJ Case Rep. 2020;13(8):e237817. doi:10.1136/bcr-2020-237817
21. Nascimento BR, Brant LC, Marino BC, Passaglia LG, Ribeiro AL. Implementing myocardial infarction systems of care in low/middle-income countries. Heart. 2018.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.