")
Back to Journals » Patient Preference and Adherence » Volume 17
Development and Validation of the Missed Nursing Care Tool for Pre-Operative Patients with Lung Cancer in China
Authors Shi XP , Dychangco MEA, Yang XM, Olivar JJR
Received 9 April 2023
Accepted for publication 6 June 2023
Published 17 June 2023 Volume 2023:17 Pages 1451—1465
DOI https://doi.org/10.2147/PPA.S413585
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qizhi (Cathy) Yao
Xin-ping Shi,1,* Ma Encarnacion A Dychangco,2,* Xu-ming Yang,3 Jennifer Joy R Olivar4
1The Nursing Department, Henan Provincial People’s Hospital, People’s Hospital of Zhengzhou University, Zhengzhou, People’s Republic of China; 2Paulinian Leadership Academy, University Research Council, St Paul University Manila, Manila, Philippine; 3Operating Room, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, People’s Republic of China; 4Nursing and Allied Health Sciences, St Paul University Manila, Manila, Philippine
*These authors contributed equally to this work
Correspondence: Ma Encarnacion A Dychangco, St Paul University Manila, 680 Pedro Gil st. Malate, Manila, 1004, Philippines, Tel +632 85245687, Fax +632 85260410, Email [email protected]
Introduction: Current research suggests that missed nursing care is widespread in preoperative lung cancer patients in China, and preoperative airway management nursing care for lung cancer patients is not standardized. Missed nursing care for preoperative lung cancer patients, on the other hand, is rarely investigated, particularly from the patient’s perspective. This study aimed to develop and validate the MISSCARE Survey for pre-operative patients with lung cancer in China.
Methods: This study generated the preliminary draft of the MISSCARE Survey - Lung Cancer Patient (MS-LCP) and tested its reliability and stability through three rounds of lung cancer resection (494, 50, and 309 cases, respectively). 20 patients and 6 experts determined the face and content validity. EFA and CFA assessed construct and convergent validity. Internal consistency, including Cronbach’s alpha, Spearman-Brown reliability, and re-test reliability, was also examined.
Results: The scale contained 15 items, including specific care, communicative care, timely care, and basic care. KMO was 0.932 (> 0.6), and Bartlett’s Test of Sphericity showed P = 0.000 (< 0.05). The attribution factor’s item loads ranged from 0.765 to 0.853, accounting for 82.20% of the variation. The scale’s Cronbach’s alpha, Spearman-Brown, and retest reliability were 0.945, 0.879, and 0.824. CFA showed goodness of fit (RMSEA = 0.021, χ2/df = 1.138, GFI = 0.900, AGFI = 0.945, CFI = 0.996, NFI = 0.967, IFI = 0.996). For each dimension, AVE ranged from 0.555 to 0.717 (> 0.50) and CR from 0.861 to 0.904 (> 0.70).
Conclusion: The MS-LCP was reliable and valid in this study, making it appropriate for the Chinese lung cancer patient population. This tool is more objective in its presentation of missed nursing care, assisting nursing staff in optimizing nursing procedures before surgery, increasing the implementation of higher-quality tumor care, and promoting the recovery of lung cancer surgery patients.
Keywords: China, lung cancer, missed nursing care, psychometric properties, scale development
Introduction
Missed nursing care was defined for the first time in a qualitative study by the American scholar Kalisch1 as every care activity necessary for the patient that was not provided or seriously delayed. Unlike traditional outcome-based quality indicators like mortality or length of stay, missed nursing care is a sole process-based indicator of patient care quality that is more likely to forewarn of worsening in nursing quality.2,3 It is widespread and directly related to adverse outcomes.4 Studies have showed that missed nursing care not only leads to negative patient outcomes such as less/poor quality of patient care (eg, bed sores, falls, and hospital-acquired infection) and lower patient satisfaction, but also result in increased ineffective pain management, malnourishment, and high mortality.5–7 For lung cancer patients, missed nursing care results in delayed detection or management of complications.4,8 It is very important to reduce this phenomenon in the oncology ward. The reason is that the majority of patients are immunocompromised due to chemo or other treatments, while missed nursing care in turn hastens mortality for at-risk cancer patients.4,8 A study revealed that for lung cancer patients, nursing care may be able to limit disease progression before treatment, increase patient satisfaction, and possibly improve clinical outcomes by reducing missed nursing care, such as providing timely care at all stages of the lung cancer care continuum.9 At present, most foreign studies mainly focus on emergency department, oncology department, pediatrics and other fields.10–15 Domestic research on missed nursing care began belatedly and focused primarily on pediatric care and general cancer care as research objects. Regarding specialist care in oncology, there is only one study, which is aimed at breast cancer.16,17 For the missed nursing care tool, Kalisch recognized that patient attention is a way for engaging patients and meeting more patient-centered patient criteria, so he developed the MISSCARE Survey-Patient in 2014.18 Si Fei measured the degree to which hospitalized patients’ experience of missed nursing care in China by sinicizing and assessing the validity and reliability of this instrument.19
Lung cancer is a malignant tumor with China’s highest morbidity and mortality.20,21 According to Globocan,22 China accounts for 37% and 39.8% of the world’s lung cancer incidence and mortality, respectively, and the mortality rate will rise by 40% by 2025–2030.23 Currently, the main clinical treatment method for early-stage lung cancer is surgery.24 The incidence of pulmonary complications after lobectomy is as high as 19% to 59%.25 Preoperative airway management may reduce postoperative complications by increasing SP-A expression in lung tissue and assisting patients in adapting to surgical damage.26,27 Chinese experts have established the following consensus on preoperative airway management28 for lung cancer patients as of now: 1) It consists of health education (such as smoking and alcohol cessation), muscle training for the respiratory system, effective cough assistance, and physical therapy (such as airway humidification and chest tremor). 2) It can provide surgical options for lung cancer patients who are unable to have surgery due to poor lung function and improve lung cancer patients’ quality of life after surgery. Therefore, accurately and fully evaluating preoperative airway management for lung cancer patients to reduce related missed nursing care has become a critical issue. The effectiveness of preoperative airway management and the amount of missed nursing care are closely connected to the patient’s quality of life after surgery and the severity of complications. Trained professional nurses are critical because they serve as assessors, implementers, observers, and coordinators throughout the preoperative airway management phase.29 They must provide reasonable and timely care, focus on patient preparation, and assess risks during this period.
However, there is a shortage of literature that focuses on the needs of lung cancer patients, even if the care needs for lung cancer patients are much higher than those of other cancer patients.30–32 Moreover, in these very few pieces of research literature, there are more than eight33 unmet needs of lung cancer patients. It is likely to be related to the apparent gap between the actual support care they received and the support care they really need from their own.34 In addition, there is no clear conclusion on nursing methods for preoperative airway management in lung cancer patients, which are deficient in various ways and not standardized in China.35–37 That is to say, there is no study on missed nursing care specifically for pre-operative lung cancer patients in China. As the population with the largest cancer prevalence, lung cancer patients differ from those in emergency departments and other clinical departments in pain management, nutrition management, radiotherapy and chemotherapy, and hospice care. Due to the particularity of lung cancer itself, the degree of active cooperation of the patient before surgery is the premise for the nurse to carry out airway management smoothly, and it has a significant impact on patients’ recovery. Suppose we use the original general scale without optimization. In that case, the validity of the content will be limited, and it will not be able to detect meaningful research content closely related to the disease. To the best of our knowledge, there is little research on missed nursing care for preoperative lung cancer patients, especially from the patients’ point of view.
Therefore, in order to more comprehensively and objectively confirm the data on the degree and type of missed nursing care reported by patients, deeply analyze and explore the phenomenon of missed nursing care, assess the lung cancer patient’s perception of the missed nursing care they receive, and make up for the data bias that occurs only from the nurse’s unilateral self-assessment, it is urgent to develop a MISSCARE Survey-Lung cancer Patient in line with China’s cultural and medical background, covering the relevant content of preoperative airway management for lung cancer patients. It is of great significance for nursing managers to effectively improve the health status of patients as a whole, optimize the quality of clinical nursing services, improve patient satisfaction, and improve the relationship between nurses and patients.
In this study, missed nursing care was considered an error of omission, defined as any aspect of required patient care for the airway management of lung cancer patients. Moreover, this study focused on developing and validating a MISSCARE survey tool for preoperative patients with lung cancer in China. Data was taken from nursing experts, patients, and literature as the basis for developing the survey tool. The study did not include doctors and medical experts in developing the MISSCARE survey tool for preoperative airway management of lung cancer patients in China. Instead, a literature analysis, including the Multi -disciplinary surgery Period Pathotic China Expert Consensus (2018 Edition), was used.
Material and Methods
Participants and Procedure
This study complied with the Declaration of Helsinki. This study contains two phases that show the process towards developing a tool to measure missed nursing care among preoperative patients with lung cancer: 1) scale development, content validity, and surface validity of the draft scale; and 2) psychometric evaluation of the scale, which included validity and reliability assessments.
Phase I: Scale Development, Content Validity, and Surface Validity of the Draft Scale
Scale Development
To ensure a full range of views were represented, purposeful sampling was used to identify respondents to conduct individual in-depth interviews using a semi-structured interview guide until data saturation was achieved and no more new information was obtained. In order to fully represent the population in this cohort, patients were purposefully selected considering their gender, age, marriage history, clinical features, and diagnosis. 19 patients from the thoracic surgery department of a 3A-rated hospital in Henan were chosen on purpose. We also considered China’s distinct social and cultural background. To guarantee that patients’ preoperative needs were fully addressed, we combined the findings from the existing research (which emphasized missed nursing care was most prevalent in communicative care, basic care, and timely care) and the Chinese expert consensus on Multidisciplinary Perioperative Airway Management-2018 Edition (excerpts from related content before surgery),28 except the results of participant interviews. The relevant material on specialized preoperative care for missed nursing care was then categorized, analyzed, and potentially relevant elements were retrieved again. Using the Likert 5-level scoring standard, a pool of 20 initial scale items was created. The manner of evaluation was self-evaluation, and the exam questions were multiple-choice. Items were scored on a five-point scale (1 = always/not more than 5 min, 2 = frequently/5–10 min, 3 = sometimes/11–20 min, 4 = occasionally/21–30min, and 5 = never/more than30 min), with higher scores suggesting more instances of missed nursing care.
Interview Outline: 1) Have you heard of missed nursing care? Please talk about your understanding of the concept. 2) Throughout the hospitalization, what nursing care did the nurse neglect to provide? What should have been executed but was not? What nursing care is frequently delayed? 3) What do you think of the instances listed above? Please provide the department with pertinent suggestions regarding these issues.
Content Validity
The content validity of the draft scale was then examined by distributing a questionnaire along with an information page to experts. We calculated the S-CVI/UA, S-CVI/AVE, and I-CVI of the questionnaire test draft based on the correlation between each item and the questionnaire test draft. For content validity, I-CVI≥ 0.78, S-CVI/UA≥ 0.8, and S-CVI/Ave≥ 0.9 were the minimum content validity requirements for the questionnaire.38 This step utilized the technique of purposive sampling. The postal survey was finished by six nursing experts, including two (2) experts in lung cancer research, one (1) clinical nursing expert, two (2) experts in tool development, and one (1) expert in lung cancer research. It was individually emailed to each expert, who was required to complete it and explain its irrelevance, missing components, or other modifications.
Surface Validity
By June 2021, we had assessed the readability of the scale and the suitability of each item’s language by evaluating its surface validity. Twenty inpatients were selected for the preliminary exam. Simultaneously, the participants’ opinions on the expression were gathered, and the scale was modified and adjusted based on feedback. Patient consent was obtained following an oral explanation of the study. A participant information sheet and a questionnaire were distributed to collect data. Each item was assigned a rating between 0 (“not at all”) and 4 (“completely”). In addition, participants were asked to complete the questionnaire, confirm the amount of time required to respond to the scale, and offer suggestions for enhancements.
Phase II: Psychometric Properties of the MS-LCP
Sample Size and Setting
The initial phase of the approach was purposeful sampling. Data for exploratory factor analysis were acquired at this stage. The sample count exceeds 300.39 Based on the sample size for the first stage, at least 10% of lung cancer patients who underwent surgery were retested two weeks later at the hospital’s Thoracic Surgery Department. This data was largely utilized to determine the scale’s test-retest reliability. Those who could participate in the third phase were chosen via convenience sampling. The data gathered at this step was used for the confirmatory factor analysis of the development scale, with a sample size of at least 300 cases.
The following criteria were used to select participants: (1) being diagnosed with lung cancer; (2) having a hospital stay of two days; (3) being 18 years old (if the patient was unable to fill in, the caregiver may answer the survey but must be a fixed caregiver and have accompanied the patient for at least 5 hours a day; (4) being informed and agreeing to sign an informed consent form; and (5) being able to speak or read Chinese. Participants who (1) have cognitive or other impairments such as poor eyesight or hearing, (2) are not accompanied by a fixed family member, (3) have had disputes with the hospital, (4) are unwilling to participate in this survey, and (5) have serious diseases of essential organs such as the cardiovascular system, brain, liver, and kidney, the hematopoietic system, acute and chronic infectious diseases, and mental illness were excluded.
Item Analysis
We observed the change in Cronbach’s α, and the criteria for this deletion was the increase in the coefficient after eliminating the item.
Construct Validity
Only if both the Bartlett’s sphericity test (p<0.05) and the Kaiser-Meyer-Olkin (KMO> 0.50) were met were the data appropriate for exploratory factor analysis (EFA).40 Principal component analysis and Promax rotation were employed to extract and rotate matrices for factor extraction, respectively. Kaiser-rule The final number of kept variables was determined using Guttman’s and Cattell’s scree tests. The significant component was defined as having an eigenvalue greater than one. The item was eliminated if the factor loadings were less than 0.40.40 The produced factor structure was then validated. Correlation coefficients must be at least 0.40 between each item and its appropriate dimension, as well as between each dimension and the total score.40 Adjusted Goodness of Fit Index (AGFI,>0.90), Goodness-of-fit index (GFI, >0.90), χ2 goodness of-fit test (χ2/df,<3); root mean square error of approximation (RMSEA, <0.10); comparative fit index (CFI, >0.90); Normed Fit Index (NFI,>0.90), Incremental Fit Index (IFI, >0.90).41 After that, the combined reliability, average variance extraction, and dimensions were determined.42 In general, when AVE is greater than 0.5 and CR is greater than 0.7, the polymerization validity is optimal.43
Reliability Analysis
In this study, we determined the Cronbach’s α for each dimension and the whole scale, the Spearman-Brown split-half reliability coefficient, and the retest reliability of the entire table All of those greater than 0.70 are considered reliable.43
Ethical Considerations
This study was conducted with approval from the ethics committee of College of Nursing and Allied Health Sciences in St. Paul University Manila on August 14, 2021 (Approval No. 2021-[115]-[IGS]-[CNA]). The researcher informed the interviewee of some rights, including the right to participate voluntarily, the right to withdraw from the interview, the right to review and withdraw the interview data, and the right to privacy. There was no intervention, but during the interview, care and attention must be observed so the patients will not suffer physical, emotional, or social stress. All collected documents, printed and not printed, will be destroyed or surrendered to the hospital (if requested) after the final paper has been approved. Participants’ withdrawal criteria were established before data collection, and all participants were informed as part of the protocol. The criteria were as follows: participants or their legal representatives withdraw from the research participation agreement; the severe adverse events made it difficult to continue the study (eg, death); the subject failed to visit the clinical trial center and answer the phone within the scheduled time; and the researcher judged the research progress inappropriately.
Data Analysis
Only complete demographic questionnaires were considered valid and were included in the analysis. When an item in the questionnaire was not answered, the average score of the item was used instead to enter the analysis, but if the questionnaires with the same answers ≥ten items continuously checked by the research subjects, they were regarded as invalid questionnaires. The data were entered and checked by two (2) persons using EpiData 3.1, and the data were checked for consistency, completeness, and logic; additionally, missing and discrete values were checked and processed. IBM SPSS Statistics 25.0 and AMOS 23.0 were used for data analysis.
Results
General Demographic Characteristics of Participants
Skewness and kurtosis verified normalcy. The first survey round issued 506 questionnaires and recovered 99.01%. The recovered had 494 valid questions, 97.62% effective. The second stage distributed 52 instances at a 96.15% effective rate-50 people. The third phase disseminated 316 surveys and retrieved 310, for a 98.10% recovery rate. 309 valid surveys yielded 99.70% successful recovery. The characteristics of all the participants in this study are displayed in Table 1.
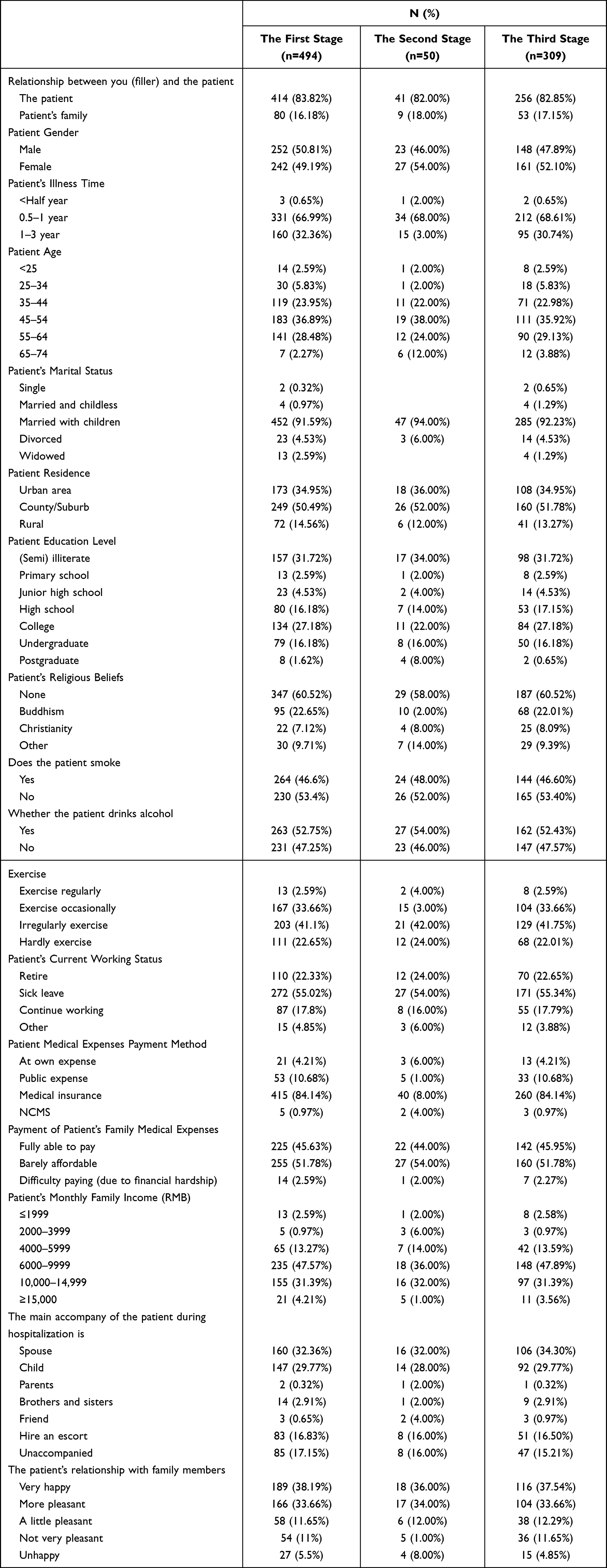 |
Table 1 Characteristics of Samples |
Content Validity
According to the correlation score between each item and the questionnaire by six experts, the S-CVI/UA of the questionnaire was 0.882, S-CVI/Ave was 0.98, and I-CVI was 0.83–1.00. At this stage, we merged and removed three items based on free-response comments regarding the experts’ modifications. As a result, after two rounds of expert review, the first draft of the MISSCARE Survey for Preoperative Airway Management of Lung Cancer Patients in China was reduced from 20 to 17 items. Table 2 shows the scores of the six experts on the first edition of the item scale:
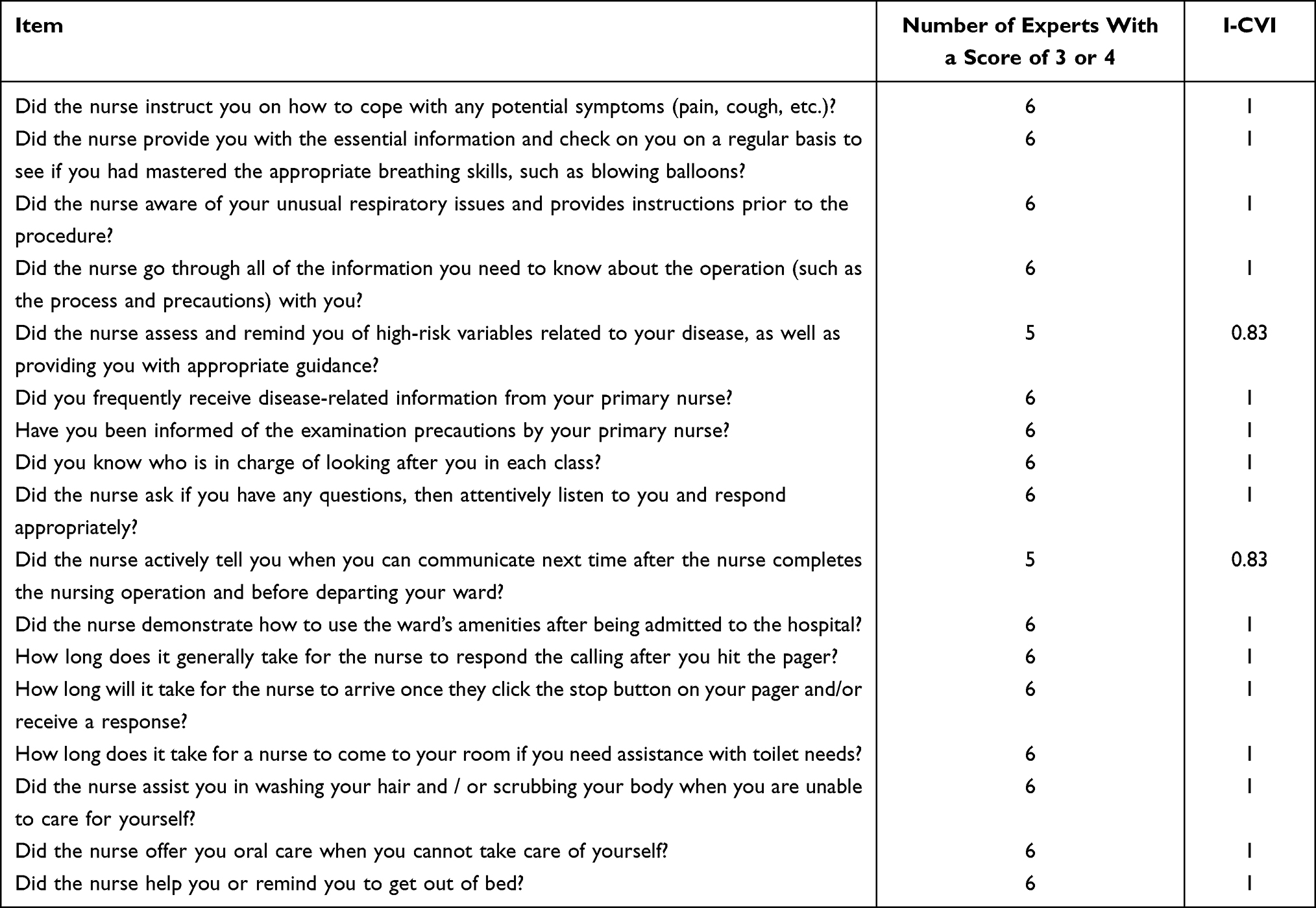 |
Table 2 Expert Scoring Situation (n=6) |
Surface Validity
The questionnaire took an average of four minutes to complete for 20 patients after lung cancer surgery. All patients thought the dimensions and item descriptions were precise and appropriate.
Item Analysis
Two items were deleted totally. Table 3 shows that the coefficient increased after deleting the item. “Did you frequently receive disease-related information from your primary nurse?” and “Have you been informed of the examination precautions by your primary nurse?”
 |
Table 3 Item Analysis |
Construct Validity
Exploratory Factor Analysis
As shown in Table 4, a 15-item exploratory factor analysis produced a Kaiser-Meyer-Olkin measure of 0.932 (>0.6) and a P = 0.000 (<0.05) result on Bartlett’s test of sphericity. The exploratory factor analysis finally determined the questionnaire with 15 items in four dimensions, explaining 82.20% of the total variation. The four factors were “specific care, communicative care, timely care, and basic care.”
 |
Table 4 Exploratory Factor Loadings |
Correlation Analysis
Table 5 shows the correlation coefficient between each item and its dimension’s total score: 15 items and their dimension correlations after calibration were 0.684–0.788. (P<0.05). The correlation coefficients between each item on Dimension 1 and its dimension total score varied between 0.684 and 0.788, for Dimension 2 between 0.751 and 0.784, for Dimension 3 between 0.698 and 0.731, and Dimension 4 between 0.754 and 0.784. These correlation coefficients were moderate (more than 0.40); the correlation coefficient between the four dimensions in the questionnaire and the overall level of the questionnaire was 0.834–0.902, and the correlation coefficient between the four dimensions was 0.585–0.900, all of which were statistically significant (P < 0.01). See Table 5 for details.
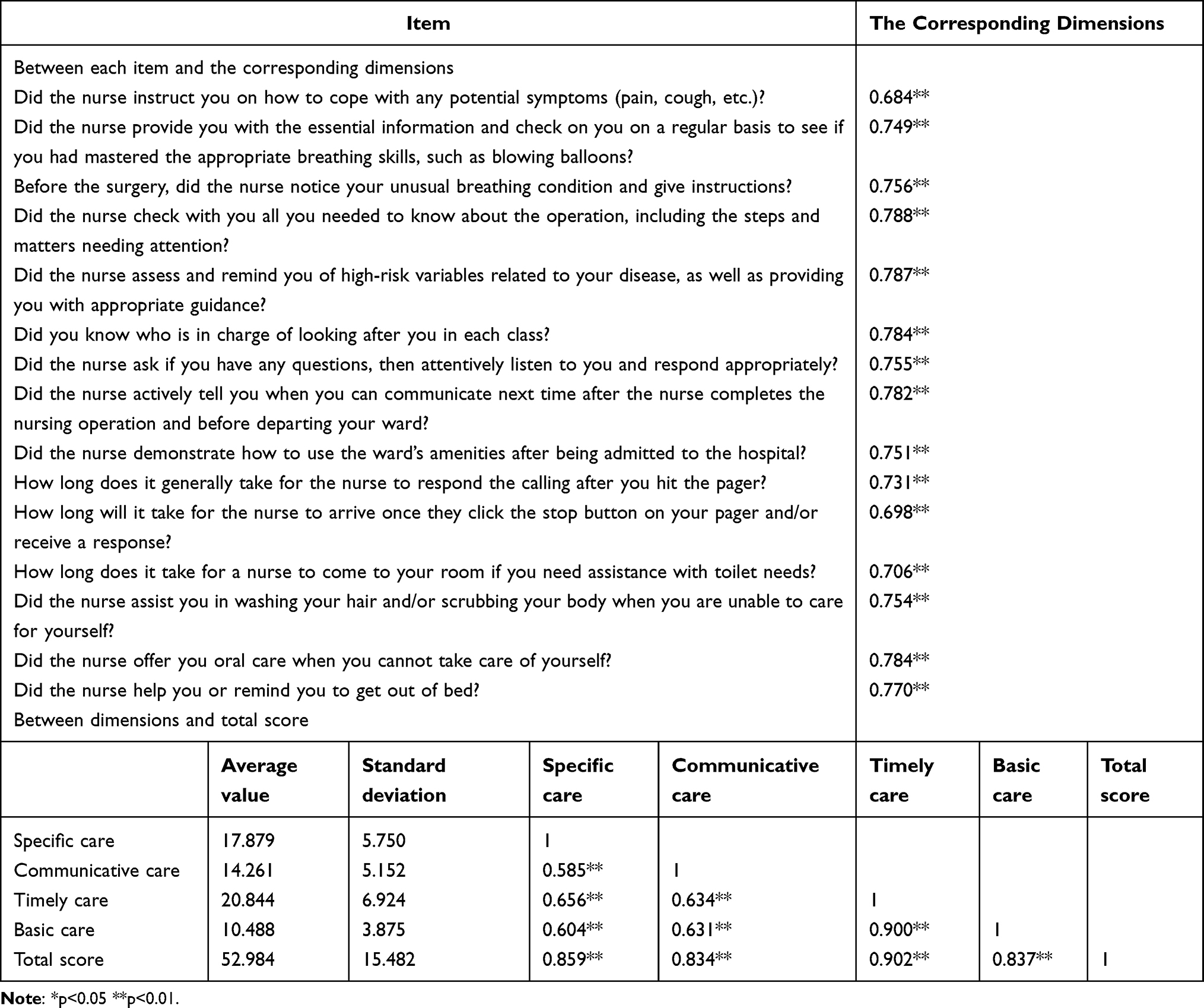 |
Table 5 Correlation Analysis |
Confirmatory Factor Analysis
In this study, confirmatory factor analysis (CFA) was conducted for four factors and 15 analysis items. Sample 2 (309 patients) was used for confirmatory factor analysis, and maximum likelihood estimation (MLE) is used to fit the three-factor model. As shown in Table 6 and Table 7, each fitting index of the 4-factor model has reached the reference value, indicating that the model is well fitted, which indicated ideal.
 |
Table 6 The Indices of the Convergent and Discriminant Validity |
 |
Table 7 Model Fit |
Reliability Analysis
Table 8 shows the reliability of the scale. Cronbach’s α, Spearman-Brown, and retest reliability were 0.945, 0.879, and 0.824 for the complete scale, respectively. For each dimension, Cronbach’s α coefficients ranged from 0.894 to 0.940, and the Spearman-Brown coefficient was between 0.896 and 0.942 (>0.700), indicating that the internal consistency of this questionnaire was ideal.
 |
Table 8 Reliability Test |
Discussion
In this study, we developed the MISSCARE Survey-Lung Cancer Patient (MS-LCP) and examined its psychometric qualities in an effort to enhance the quality of preoperative airway management services in Chinese hospitals from the patients’ perspective.
Psychometric Properties of the Developed Scale
The MISSCARE Survey-Lung Cancer Patient (MS-LCP) questionnaire was established based on a review of the literature and previous studies. We conducted a surface validity experiment after two rounds of expert consultation. Using exploratory factors in the first round, clear stability results were produced in the second round. In the third round, confirmatory factor analysis was utilised to validate the structure’s rationality. Of course, we performed the reliability test, and in addition, the 20 cases of patients with small sample testing showed that the average time to complete the questionnaire was about four (4) minutes. For patients who have just undergone major surgery, the questionnaire has certain advantages.
The scale consists of “specific care” (5 items), “communicative care” (4 items), “timely care” (3 items), and “basic care” (3 items). The first factor, “Specific Care”, includes the patient’s lack of appropriate guidance on how to handle potential symptoms, being noticed with unusual respiratory issues, and being provided instructions by nurses.44,45 This is likely due to the nurse’s lack of awareness about teaching patients breathing exercises, inadequate nurse teamwork resulting from a lack of relevant professional training, and the nurse’s lack of comprehensive abilities, such as sufficient nursing skills and an ability to handle various clinical emergencies flexibly, especially for new nurses.46 Coupled with nurses who, due to time constraints, fail to determine their health literacy.44,47 As a result, nurses have numerous questions about the procedure and require information urgently.48 Patients are especially interested in comprehending the effects and complications of surgery, as well as how they may affect later life and symptom management.44 Training the patient’s respiratory muscles and function can improve lung function, reduce lung damage, and accelerate recovery. Cough and sputum training before surgery enhances respiratory function and facilitates postoperative rehabilitation. Novice nurses lack business skills, including a grasp of theory and clinical operations. They need stronger synchronisation between theory and practice, even though in China, patients prefer to place a higher value on a caregiver’s attitude than on their professional expertise. Structured scientific training with a more defined purpose and objectives can improve the situation.
The second factor is communicative care, which means that patients want to be asked if they have any questions and told when they can talk again after their concerns have been listened to carefully and dealt with in the right way. Chinese nurses inadvertently classified communicative care as a non-priority issue because they believed that communication nursing activities would not have an immediate impact on the patient’s health and their workload was excessively heavy.49 Marsh thought this might be due to the requirement to keep treatments on schedule throughout the day.47 Without standardised communication skills and content training, patients will quickly feel a need for a more human touch in nursing care.50 Nurses frequently employ a one-way communication technique in which they speak just about what they believe they should say, without knowing if the patient has further questions or needs, and with minimal patient touch. This conclusion was also supported by Koduah,46 who found that nurses should enquire more about their patients’ health literacy by asking about their level of education. It is recommended that the primary nurses participate in the preoperative education of patients and employ a variety of communication tactics based on the patients’ social backgrounds, personality traits, psychological traits, educational level, and economic status. Also advised is notifying the patient and scheduling the next communication time following each nurse-patient conversation, as this can considerably reduce the patient’s feelings of uncertainty and dread resulting from the illness. Despite the fact that patients in China have a fundamental expectation of maintaining harmonious relationships with others, a lack of trust with nurses may prevent them from discussing their wants and concerns. However, some studies have shown that patients who cannot express their needs or who are unable to self-care have an effect on the decision-making and nursing time of nurses, thereby increasing the likelihood of missed nursing care and creating a vicious circle.4 So, we must prioritise communicative care, engaging the family in the treatment plan and offering help for their care is consistent with both Chinese cultural expectations and the hospital’s job content, which should foster the formation of an atmosphere that provides a human touch to cancer patients.
The third factor is timely care. According to the researchers, patients and their families utilise the call bell for five major reasons: very urgent medical difficulties, restroom assistance, intravenous infusion problems, and management of pain. The nurse handles the alarm sound of the instrument in time to ensure that the ward is quiet, which is convenient for patients to rest and is conducive to the adjustment of the preoperative state. In this study, excessive and time-consuming paperwork not only takes up too much of a nurse’s working time but also hampers or disrupts patient care work,51 reducing the overall time spent on patient care.52 Furthermore, other research indicates that material resources, hospital affairs, and medical communication all have a significant impact on nurses’ ability to provide timely care: 1) A lack of resources, or difficulty obtaining them, lowers the efficiency of nurses’ jobs and costs nursing time. For example, when medicine is not delivered on time,52 the nurse must then choose among the available nursing tasks, which may not provide patients with timely and high-quality care but rather only rush care.53 2) When nurses are involved in too many multi-hospital activities, such as internal management, multi-party coordination, policy choices, scientific research activities, and committee work, time spent actually caring for patients amounts to only 37% of total working time.54 This makes timely care even more challenging;53,55 3) Because clinical nursing work involves a wide range of activities and interruptions, individual efforts frequently fall short of meeting all of a patient’s nursing needs, necessitating good communication among medical personnel. Each point of efficient communication between medical staff increases the odds of care being supplied by one point and reduces the likelihood of treatment not being provided by 21.9%.54,55 We found that, faced with such a situation, patients had to do things independently or seek help from other patients. The phenomenon of “patient peer support” was also found in another study and has been utilised to improve cancer care (providing help and support from treated patients to others).51 But it is not the reason we ignore the negative results. In addition, in response to the low nurse-patient ratio in China, management must consider the nursing level when distributing nursing workers. When the position level of the department nursing staff is unreasonable, it is essential to ensure that different departments from the same sub-specialty within the hospital are dynamically changed and corrected in a timely manner.
The fourth factor is “basic care.” At present, basic care or ADLs are compromised, and they are even degraded due to a busy schedule. Prior research has established that by focusing on basic care, Cypriot nurses are more likely to lack hand washing and monitoring vital signs, while Italian and Australian nurses are more likely to lack basic treatment care.56 While in this study, it may have resulted from a lack of supplies, poor infrastructure, and a shortage of staff, especially when the patient’s family members are unavailable, the nursing staff should assist the patient with daily tasks such as toileting and body cleaning. This is especially critical for the elderly, who find it difficult to move and are at risk of falling. This is consistent with the outcomes of Si Fei,19 she found that in China, body cleansing (72.3%), considering the patient’s suggestion (48.9%), assisting in bed activities to get out of bed activities (38.6%), patient listening and answering (22.3%), and so on were nursing aspects that were frequently absent in the patient’s perception. The author speculates that this is related to regional and cultural differences, as well as an emphasis on fundamental nursing in hospital and department categories, nurse duties, and assessment.
Limitations
Limitations exist in the current research. Firstly, all of the study’s samples came from the thoracic surgery department of a tertiary hospital in Henan Province. It is vital to increase the sample size and sampling scope in future studies. Secondly, the researcher did not receive training and answered questions on the spot before the test, while in this study, investigators’ qualitative research training experience partially compensates for the deficiency. Finally, due to the single research facility, immunotherapy was not administered to a large number of patients. Although this item arose in qualitative research, we eventually chose not to include it on the scale because it is not widely used. Because neoadjuvant immunotherapy will become more widespread prior to surgery in the future, it is suggested that relevant specific care be adequately incorporated into future studies.
Conclusions
The MISSCARE Survey scientifically and effectively reflected the lack of preoperative care items and has good credibility and validity in this study, which was suitable for the Chinese lung cancer patient population. There were 15 items in the MISSCARE Survey-Lung Cancer Patient (MS-LCP), including specific care, communicative care, timely care, and basic care. From the standpoint of patients, this study analyzes practical strategies to improve the quality of preoperative airway management services in Chinese hospitals. The MNC tool for preoperative lung cancer patients can improve nursing services for this specific population by focusing on missed nursing care, which is useful not only for strengthening the public service role recognition of nurses in Chinese tertiary hospitals, but also for enhancing the hospital’s overall humanistic care environment and atmosphere.
Acknowledgments
The authors appreciate everyone who participated in this study. We thank all those who took part in the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kalisch BJ. Missed nursing care. J Nurs Care Qual. 2006;21(4):306–313. doi:10.1097/00001786-200610000-00006
2. Imam A, Obiesie S, Aluvaala J, Maina JM, Gathara D, English M. Identifying gaps in global evidence for nurse staffing and patient care outcomes research in low/middle-income countries: an umbrella review. BMJ Open. 2022;12(10):e064050. doi:10.1136/bmjopen-2022-064050
3. Imam A, Obiesie S, Aluvaala J, Maina M, Gathara D, English M. Missed nursing care in acute care hospital settings in low-middle income countries: a systematic review protocol. Wellcome Open Res. 2021;6:359. doi:10.12688/wellcomeopenres.17431.1
4. Dehghan-Nayeri N, Shali M, Navabi N, Ghaffari F. Perspectives of oncology unit nurse managers on missed nursing care: a qualitative study. Asia Pac J Oncol Nurs. 2018;5(3):327–336. doi:10.4103/apjon.apjon_6_18
5. Schubert M, Ausserhofer D, Bragadóttir H, et al. Interventions to prevent or reduce rationing or missed nursing care: a scoping review. J Adv Nurs. 2020;77(2):550–564. doi:10.1111/jan.14596
6. Imam A, Obiesie S, Gathara D, Aluvaala J, Maina M, English M. Missed nursing care in acute care hospital settings in low-income and middle-income countries: a systematic review. Hum Resour Health. 2023;21(1). doi:10.1186/s12960-023-00807-7
7. Chaboyer W, Harbeck E, Lee B, Grealish L. Missed nursing care: an overview of reviews. Kaohsiung J Med Sci. 2020;37(2):82–91. doi:10.1002/kjm2.12308
8. Friese CR, Kalisch BJ, Lee KH. Patterns and correlates of missed nursing care in inpatient oncology units. Cancer Nurs. 2013;36(6):E51–E57. doi:10.1097/ncc.0b013e318275f552
9. Nwagbara UI, Ginindza TG, Hlongwana KW. Health systems influence on the pathways of care for lung cancer in low- and middle-income countries: a scoping review. Global Health. 2020;16(1). doi:10.1186/s12992-020-00553-8
10. Simpson KR, Lyndon A, Spetz J, Gay CL, Landstrom GL. Missed nursing care during labor and birth and exclusive breast milk feeding during hospitalization for childbirth. MCN. 2020;45(5):280–288. doi:10.1097/nmc.0000000000000644
11. Tubbs-Cooley HL, Mara CA, Carle AC, Mark BA, Pickler RH. Association of nurse workload with missed nursing care in the neonatal intensive care unit. JAMA Pediatr. 2019;173(1):44. doi:10.1001/jamapediatrics.2018.3619
12. Ogboenyiya AA, Tubbs-Cooley HL, Miller E, Johnson K, Bakas T. Missed nursing care in pediatric and neonatal care settings. MCN. 2020;45(5):254–264. doi:10.1097/nmc.0000000000000642
13. Bagnasco A, Zanini M, Aleo G, Catania G, Kalisch BJ, Sasso L. Development and validation of the MISSCARE survey – pediatric version. J Adv Nurs. 2018;74(12):2922–2934. doi:10.1111/jan.13837
14. Vryonides S, Papastavrou E, Charalambous A, Andreou P, Eleftheriou C, Merkouris A. Ethical climate and missed nursing care in cancer care units. Nurs Ethics. 2016;25(6):707–723. doi:10.1177/0969733016664979
15. Compton EK, Gildemeyer K, Reich RR, Mason TM. Perceptions of caring behaviours: a comparison of surgical oncology nurses and patients. J Clin Nurs. 2019;28(9–10):1680–1684. doi:10.1111/jocn.14773
16. Xu H, Ye R, Yaling Q. Department of pediatrics, Xiamen Children’s Hospital; cause analysis and countermeasures of neonatal nosocomial infection caused by lack of T1 nursing care. Chin Foreign Med. 2020;150–152. doi:10.16662/j.cnki.1674-0742.2020.36.150
17. Li Y, Yinghuha H, Yuan H, Liu J. Cervical cancer synchronization chemotherapy therapy for patient care list (patient version) preliminary application and preliminary application. Nurs Res. 2021;35(3):522–525.
18. Kalisch BJ, Xie B, Dabney BW. Patient-reported missed nursing care correlated with adverse events. Am J Med Qual. 2013;29(5):415–422. doi:10.1177/1062860613501715
19. Si F, Qian Z, Zhang J, Zhu N, Chen S. Localization, reliability and validity evaluation of the miss care survey-patient. China Nurs Manag. 2019;19(05):667–671. doi:10.3969/j.issn.1672-1756.2019.05.006
20. Cao W, Chen HD, Yu YW, Li N, Chen WQ. Changing profiles of cancer burden worldwide and in China: a secondary analysis of the global cancer statistics 2020. Chin Med J. 2021;134(7):783–791. doi:10.1097/cm9.0000000000001474
21. Tersigni C, Venturini E, Montagnani C, Chiappini E, de Martino M, Galli L. Antimicrobial stewardship in children: more shadows than lights? Expert Rev Anti Infect Ther. 2019;17(11):871–876. doi:10.1080/14787210.2019.1686355
22. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA. 2021;71(3):209–249. doi:10.3322/caac.21660
23. Martín-Sánchez JC, Lunet N, González-Marrón A, et al. Projections in breast and lung cancer mortality among women: a bayesian analysis of 52 countries worldwide. Cancer Res. 2018;78(15):4436–4442. doi:10.1158/0008-5472.can-18-0187
24. Fuzhi Y, Dongfang T, Wentao F, et al. Rapid recovery of postoperative pulmonary function in patients with lung cancer and influencing factors. Front Oncol. 2022;12. doi:10.3389/fonc.2022.927108
25. Yasuura Y, Maniwa T, Mori K, et al. Quantitative computed tomography for predicting cardiopulmonary complications after lobectomy for lung cancer in patients with chronic obstructive pulmonary disease. Gen Thorac Cardiovasc Surg. 2019;67(8):697–703. doi:10.1007/s11748-019-01080-z
26. Chi M, Wang X, Li X, Daqiang S. The effect of preoperative pulmonary protection on surfactant protein A content in lung tissue. Tianjin Med J. 2017;45(3):310–313. doi:10.11958/20161397
27. Guo H. Research on respiratory tract management during surgery during lung cancer patients. Cardiovasc Dis Electron J Integrat Trad Chin West Med. 2020;8(4):99–100. doi:10.16282/j.cnki.cn11-9336/r.2020.04.082
28. Multi -disciplinary surgery Period Pathotic China Expert Consensus (2018 Edition) Expert G. Multi -disciplinary surgery period The consensus of Chinese experts (2018 edition). Chin J Thorac Cardiovasc Surg. 2018;25(7):545–549. doi:10.7507/1007-4848.201804082
29. Li Y, Yan C, Li J, et al. A nurse‐driven enhanced recovery after surgery (ERAS) nursing program for geriatric patients following lung surgery. Thorac Cancer. 2020;11(4):1105–1113. doi:10.1111/1759-7714.13372
30. Nightingale CL, Steffen LE, Tooze JA, et al. Lung cancer patient and caregiver health vulnerabilities and interest in health promotion interventions: an exploratory study. Glob Adv Health Med. 2019;8:216495611986516. doi:10.1177/2164956119865160
31. Jim HSL, Eisel SL, Hoogland AI, Shaw S, King JC, Dicker AP. Use of a cancer registry to evaluate patient-reported outcomes of immune checkpoint inhibitors. Cancers. 2020;13(1):103. doi:10.3390/cancers13010103
32. Huang ZP, Cheng HL, Loh SY, Cheng KK. Functional status, supportive care needs, and health-related quality of life in advanced lung cancer patients aged 50 and older. Asia Pac J Oncol Nurs. 2020;7(2):151–160. doi:10.4103/apjon.apjon_50_19
33. Konstantinidis TI, Samonis G, Sarafis P, Philalithis A. Assessment of needs of hospitalized cancer patients with advanced cancer. Glob J Health Sci. 2016;9(6):184. doi:10.5539/gjhs.v9n6p184
34. Zhang T, He H, Liu Q, Song Y, Hong J. Supportive care needs of patients with lung cancer in Mainland China: a cross-sectional study. J Nurs Res. 2019;27(6):e52. doi:10.1097/jnr.0000000000000338
35. Huang Y, Chen X, Huang C, Ba Z. NNN-link nursing mode observation of patients in patients with patients with lung cancer. Qilu Nurs Mag. 2022;28(6):1–4.
36. Zhang T, Lv X, He H, Liu Q, Wu D, Hong J. Supportive care needs in patients with lung cancer in tertiary hospitals of Anhui Province. Chin J Dis Control Prev. 2018;22(6):645–647. doi:10.16462/j.cnki.zhjbkz.2018.06.024
37. Sha Y, Kong Q, Liu L, et al. Application of preoperative centralized airway management in the prevention of postoperative pneumonia in patients with lung cancer. J Nurs Train. 2019;34(17):1587–1590. doi:10.16821/j.cnki.hsjx.2019.17.015
38. Grant JS, Davis LL. Selection and use of content experts for instrument development. Res Nurs Health. 1997;20(3):269–274. doi:10.1002/(SICI)1098-240X(199706)20:3<269::AID-NUR9>3.0.CO;2-G
39. Wang Y, Wen Z, Fu Y. Equivalence test —— a new perspective of structural equation model evaluation and measurement invariance analysis. Adv Psychol Sci. 2020;28(11):1961–1969. doi:10.3724/sp.j.1042.2020.01961
40. Abounoori M, Maddah MM, Sharif Nia H, et al. Development and validation of the knowledge and attitude scale toward COVID-19 pandemic breaking transmission chain (KA-C) among Iranian population. Front Public Health. 2021;9(61). doi:10.3389/fpubh.2021.627013
41. Rong TS. AMOS and Its Research Methods. Chongqing: Chongqing University Press; 2009. Chinese.
42. Rodrigues IB, Adachi JD, Beattie KA, Lau A, MacDermid JC. Determining known-group validity and test-retest reliability in the PEQ (personalized exercise questionnaire). BMC Musculoskelet Disord. 2019;20(1):373. doi:10.1186/s12891-019-2761-3
43. Fornell C, Larcker D. Evaluating structural equation models with unobservable variables and measurement error. J Mark Res. 1981;18:39–50. doi:10.1177/002224378101800104
44. Khamboon T, Pakanta I. Intervention for symptom cluster management of fatigue, loss of appetite, and anxiety among patients with lung cancer undergoing Chemotherapy. Asia Pac J Oncol Nurs. 2021;8(3):267–275. doi:10.4103/2347-5625.311003
45. Jacobs C, Patch C, Michie S. Communication about genetic testing with breast and ovarian cancer patients: a scoping review. Eur J Hum Genet. 2018;27(4):511–524. doi:10.1038/s41431-018-0310-4
46. Koduah AO, Leung AYM, Leung DYL, Liu JYW. “I sometimes ask patients to consider spiritual care”: health literacy and culture in mental health nursing practice. Int J Environ Res Public Health. 2019;16(19):3589. doi:10.3390/ijerph16193589
47. Marsh V, Kalisch B, McLaughlin M, Nguyen L. Nurses’ perceptions of the extent and type of missed perioperative nursing care. AORN J. 2020;112(3):237–247. doi:10.1002/aorn.13146
48. Ekstedt M, Schildmeijer K, Wennerberg C, Nilsson L, Wannheden C, Hellström A. Enhanced patient activation in cancer care transitions: protocol for a randomized controlled trial of a tailored electronic health intervention for men with prostate cancer. JMIR Res Protoc. 2019;8(3):e11625. doi:10.2196/11625
49. Du H, Yang Y, Wang X, Zang Y. A cross‐sectional observational study of missed nursing care in hospitals in China. J Nurs Manag. 2020;28(7):1578–1588. doi:10.1111/jonm.13112
50. Nist MD, Harrison TM, Tate J, Robinson A, Balas M, Pickler RH. Losing touch. Nurs Inq. 2020;27(3). doi:10.1111/nin.12368
51. Yoshioka K, Manne-Goehler J, Maguire JH, Reich MR. Access to Chagas disease treatment in the United States after the regulatory approval of benznidazole. PLoS Negl Trop Dis. 2020;14(6):e0008398. doi:10.1371/journal.pntd.0008398
52. Li G, Tian LY, Su YN, et al. Research progress on status quo and strategy of nursing deficiency. Nurs J Chin PLA. 2020;37(10):65–67.
53. Chegini Z, Jafari-Koshki T, Kheiri M, et al. Missed nursing care and related factors in Iranian hospitals: a cross sectional survey. J Nurs Manag. 2020;28(8):2205–2215. doi:10.1111/jonm.13055
54. Chapman R, Rahman A, Courtney M, Chalmers C. Impact of teamwork on missed care in four Australian hospitals. J Clin Nurs. 2016;26(1–2):170–181. doi:10.1111/jocn.13433
55. Park SH, Hanchett M, Ma CJ. Practice environment characteristics associated with missed nursing care. J Nurs Scholarsh. 2018;50(6):722–730. doi:10.1111/jnu.12434
56. Labrague LJ, De Los Santos JAA, Tsaras K, et al. The association of nurse caring behaviours on missed nursing care, adverse patient events and perceived quality of care: a cross-sectional study. J Nurs Manag. 2020;28(8):2257–2265. doi:10.1111/jonm.12894
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.