")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 15
Development and Validation of a Three-Parameter Scoring System for Monitoring HIV/AIDS Patients in Low-Resource Settings Using Hematological Parameters
Authors Al-Mughales JA
Received 17 August 2023
Accepted for publication 26 September 2023
Published 5 October 2023 Volume 2023:15 Pages 599—610
DOI https://doi.org/10.2147/HIV.S431139
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Jamil A Al-Mughales1,2
1Department of Clinical Microbiology and Immunology, King Abdul-Aziz University, Jeddah, Kingdom of Saudi Arabia; 2Department of Clinical Laboratories-Diagnostic Immunology Division, King Abdul-Aziz University Hospital, Jeddah, Kingdom of Saudi Arabia
Correspondence: Jamil A Al-Mughales, Tel +966126408405 ; +966505598324, Email [email protected]
Objective: This study aimed to test the validity of a composite score using complete blood count (CBC) for monitoring HIV patients receiving antiretroviral therapy (ART) in the absence of viral load and CD4 count.
Methods: This retrospective cohort study analyzed the laboratory data of 82 HIV patients who had pre- and post-treatment viral load, CD4 count, and CBC data. Pre- and post-treatment data were pooled to analyze the correlation of CBC parameters with Polymerase Chain Reaction (PCR) ranks and their performance in indicating a CD4 count< 200 cells/mm3 using the Operating Characteristics Curve (ROC), with the determination of cutoffs. A score combining the significant parameters was tested to predict a CD4 count of < 200.
Results: Total lymphocyte count (TLC), percentage (TLP), and hemoglobin concentration (Hb) were the most significant parameters, showing negative correlations with PCR (Spearman’s Rho = − 0.357 to − 0.242). The risk of acquired immunodeficiency syndrome (AIDS) was independently associated with TLC< 1345 cells/mm3 (OR=2.92), TLP< 29.07% (OR=3.53), and Hb< 10.55 mg/dL (OR=3.60). A combined score of 2– 3 indicated a CD4 count< 200 with an odds ratio of 8.3– 86.7.
Conclusion: The proposed 3-parameter score combining the use of TLC, TLP, and Hb, is an affordable and practical approach that may have clinical utility in monitoring HIV patients receiving ART in low-resource settings.
Keywords: lymphocytes, hemoglobin, hematology, HIV, antiretroviral, monitoring
Introduction
Human immunodeficiency virus (HIV) infection is a global public health concern. Since the onset of the disease, 79 million people have been infected and 36 million people have died.1 The introduction of antiretroviral therapy (ART) and, more recently, highly active ART (HAART) has changed the course and health burden of the HIV pandemic.2 Combined regimens of highly effective and well-tolerated ART molecules have been prescribed, leading to a substantial reduction in morbidity, mortality, and HIV transmission.3
To combat HIV/AIDS pandemic, the Joint United Nations Program on HIV/AIDS (UNAIDS) has set specific goals to achieve 95% suppression of the viral load among the treated patients, projecting to end the pandemic in 2030 (Fast-Track - Ending the AIDS epidemic by 2030.4 To achieve these goals, global action against HIV/AIDS aims to promote access to ART, notably in low- and middle-income countries (UNAIDS, 2012; UNAIDS Report on the Global AIDS Epidemic | 2012, 2012).5 This implies that monitoring the viral load (number of viral RNA copies per mL) in treated patients is a fundamental test for determining treatment efficacy (Fast-Track - Ending the AIDS epidemic by 2030.5
However, these goals are challenged by the unequal distribution of treatment and management resources; the highest epidemiological figures concern low-income countries with poorly equipped facilities.6 As of December 2020, the World Health Organization (WHO) estimated that 27% of people living with HIV (PLHIV) had no access to ART.1 Additionally, treatment implementation has increased the demand for viral load testing, which may constitute an economic challenge for low-resource settings that add to the economic burden of the disease in highly impacted and low-income countries.7 For example, many sub-Saharan African countries struggle to implement viral load monitoring because of a lack of appropriate infrastructure and laboratory systems, in addition to financial and political challenges.8
Furthermore, until 2013, the indication of ART initiation was determined by CD4+ lymphocytes (T helper cells) count. The initial WHO guidelines recommend treating HIV patients with CD4+ cell counts less than 350 cells per mL.9 However, in 2013, the threshold was increased to 500 cells/mL, and in 2016, the WHO recommended treating all HIV-infected patients infected with HIV regardless of their CD4 count.10,11 However, the use of the CD4+ count test remains of interest in some clinical situations, notably in cases of late diagnosis,12 as well as in several low-resource countries that have not implemented updated recommendations.8 However, compliance with local CD4+ monitoring recommendations in these countries remains suboptimal owing to economic issues. A study from seven Latin American countries involving 14,476 newly treated HIV patients showed that approximately two-thirds of the patients had inadequate CD4+ count measurement or monitoring. The same study highlighted significant inter-country variability in the costs of the tests, ranging between $7.4 to $64.1 for CD4+ cell count and $20.3 to $186.3 for HIV viral load.11
Consequently, there is an unmet need for more cost-effective strategies to monitor patients with HIV and their treatment efficacy in low-resource settings. Hence, several other biological parameters have been proposed to monitor HIV patients as proxies for the CD4+ count or HIV viral load. For instance, a total lymphocyte count (TLC) <1200 cells/mm3, this is no longer solely dependent on CD4 cell counts.11 Several other studies have discussed the use of TLC as a surrogate for HIV progression over the past years.13–15 Other studies have suggested that TLC combined with blood hemoglobin level provides more sensitive predictions for the progression of HIV.16–18 Other data highlight further hematological dysfunctions in HIV patients, such as normocytic normochromic anemia, thrombocytopenia, and monocytosis, which are associated with immunological and clinical severity and stage of the disease and tend to improve after ART initiation.19,20 However, the use of hematological parameters to monitor HIV patients and predict HIV progression remains controversial.21,22
Using a different approach, the present study tested the performance of a composite score, combining the most significant hematological parameters, in indicating ART efficacy, viral load, and AIDS stage, which is defined here as a CD4 count <200 mm3. Such a composite score offers a more comprehensive proxy for monitoring disease stage and treatment efficacy, making it particularly valuable in low-resource settings where access to viral load and CD4 count measurements may be limited. Therefore, this study aimed to test the validity of a composite score using CBC for monitoring HIV patients on ART in the absence of viral load and CD4 count.
Materials and Methods
Study Design
A retrospective cohort study was conducted on 82 HIV patients with pre- and post-treatment data for viral load, CD4 count, and CBC.
Study Setting
This study was conducted at the Department of Clinical Laboratories-Diagnostic Immunology Division, King Abdulaziz University Hospital (KAUH), Jeddah, Saudi Arabia.
Participants
We included newly diagnosed and treated HIV patients who had baseline data for HIV viral load, CD4 count, and complete blood count (CBC) and at least one follow-up data point for the same parameters, at 3–12 months after the start of treatment. All eligible patients who were followed at the Infectious Disease Department of KAUH between January 2009 and December 2016 were included.
Sampling Technique
Based on a convenience sampling technique, eligible patients with HIV who attended the Infectious Disease Department of KAUH between January 2009 and December 2016 were included in this study as retrospective study.
Data Collection
Data was collected from electronic laboratory records and captured in an Excel sheet. These included HIV PCR level, CD4 count, white blood cell (WBC) count, TLC, total lymphocyte percentage (TLP), monocyte count and percentage, platelet count, and hemoglobin concentration.
HIV PCR level was ranked into 5 levels: ≤500, 501–3000, 3001–10,000, 10,001–30,000, and >30,000 copies /mL. This ranking corresponds to the five risk categories determined by Mellors et al and was demonstrated to be associated with a differential 6-year risk of progression to AIDS of 5.4%, 16.6%, 31.7%, 55.2%, and 80.0%.23
Laboratory and Immunoassays
The viral load was measured by calculating the HIV-1 RNA signal using Polymerase Chain Reaction (PCR) technology provided by the commercial COBAS® AmpliPrep/COBAS® TaqMan® HIV-1 Test (v2.0, Roche, Switzerland). CD4 counts were measured using flow cytometry to determine the percentages and absolute counts of mature human lymphocytes and lymphocyte subsets (BD Biosciences, San Jose, CA, USA). Complete blood counts were performed according to routine laboratory standards using a Sysmex XN-3100 Automated Hematology Analyzer (Kobe, Japan). All laboratory tests were performed in accordance with the manufacturer’s guidelines.
Statistical Analysis
Two different approaches were used in the present study including paired and pooled analysis.
Paired Analysis
This approach consisted of analyzing 82 paired observations of baseline (pre-treatment) and outcome (3–12 months after treatment initiation) data for viral load, CD4 count, and CBC. The Wilcoxon signed-rank test was used to analyze the paired change in HIV PCR rank and the levels of other non-normally distributed levels of WBC, TLC, TLP, monocyte count and percentage, platelet counts, and hemoglobin concentration. The McNemar test was used to analyze the paired change in AIDS status, defined as a CD4 count of <200 cells/mm3.24
Pooled Analysis
This analysis included all baseline and follow-up data of the 82 patients that provided matched results of PCR and CD4 counts with CBC results, and tested two objectives:
- The association of CBC parameters with PCR ranks was analyzed using the Kruskal–Wallis test and Spearman correlation, and the results are presented as median and interquartile range (IQR) and Spearman’s Rho coefficient.
- The performance of TLC, TLP, platelet count, monocyte percentage, and hemoglobin level in indicating disease stage (AIDS) was analyzed using a receiver operating characteristic (ROC) curve with estimation of the area under the curve (AUC). Since the significant CBC parameters had negative relationships with positive AIDS status, another ROC curve analysis was carried out using the reciprocal values of TLC, TLP, and hemoglobin levels. This analysis was completed by calculating the Youden’s index with the determination of the best cutoffs and estimation of the respective sensitivity and specificity. Multivariate logistic regression was performed to verify the independent associations of TLC, TLP, and hemoglobin concentration with AIDS status. Subsequently, a discrete scoring system (range 0–3) was built to predict AIDS status by combining the levels of TLC, TLP, and hemoglobin with reference to their respective cutoffs (≤cutoff [score =0], > cutoff [score=1]). The chi-square test and logistic regression were used to estimate the levels of risk and analyze the significance of the model.
Both paired and pooled databases were edited, processed, and analyzed using the Statistical Package of Social Science (SPSS) version 21 for Windows (IBM, Chicago, IL, USA). A p-value<0.05, was considered to reject the null hypothesis.
Results
Pre- to Post-Treatment Change in the Studied Parameters
From baseline to follow-up times, there was a statistically significant rise in the median TLC (1.30 K to 1.65 K cell/mm3, p=0.002), TLP (35.20% to 43.40%, p0.001), and hemoglobin concentration (11.50 to 12.55 g/dL, p=0.003). This was linked to a significant decline in viral load rank (p 0.001) and a significant drop in the proportion of patients with a CD4 count below 200 cells/mm3 (from 48.8% to 29.3%; p 0.001), (Table 1).
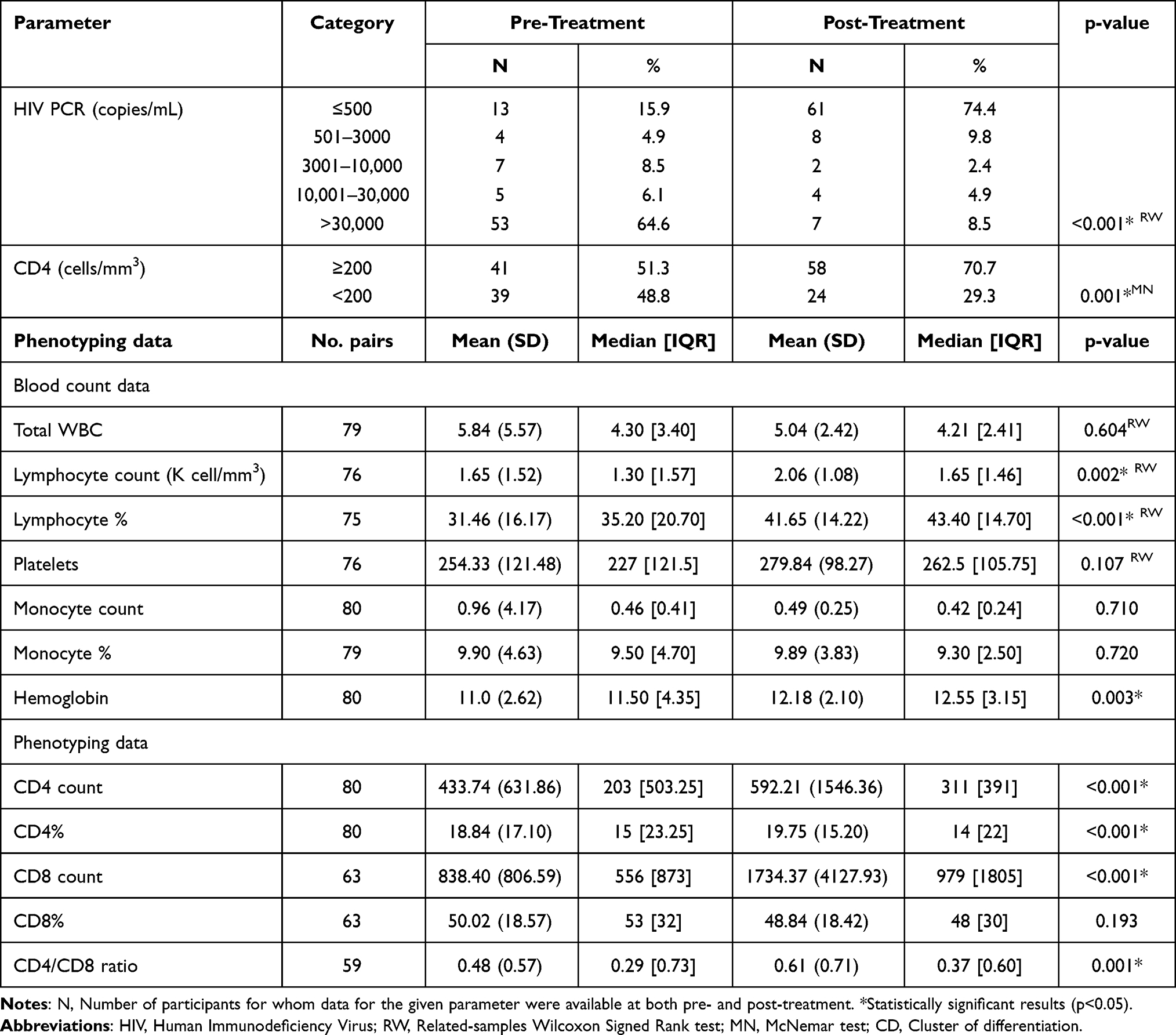 |
Table 1 Pre- to Post-Treatment Changes in Various Biological Parameters (N=82) |
Correlation of CBC Parameters with PCR Levels
The average CBC parameters for each of the five viral load levels are compared in Table 2, along with Spearman correlations between each parameter and the PCR level. According to the results, there was a negative connection between PCR rank and WBC (Rho = −0.140, p=0.008), TLC (Rho = −0.302, p0.001), TLP (Rho = −0.242, p0.001), platelet count (Rho = −0.156, p=0.003), and hemoglobin concentration (Rho = −0.357, p0.001). In contrast, the correlation between PCR rank and monocyte proportion was positive (Rho = 0.137, p=0.009). The median TLC, TLP, platelet count, proportion of monocytes, and hemoglobin level by PCR rank are shown in Figure 1.
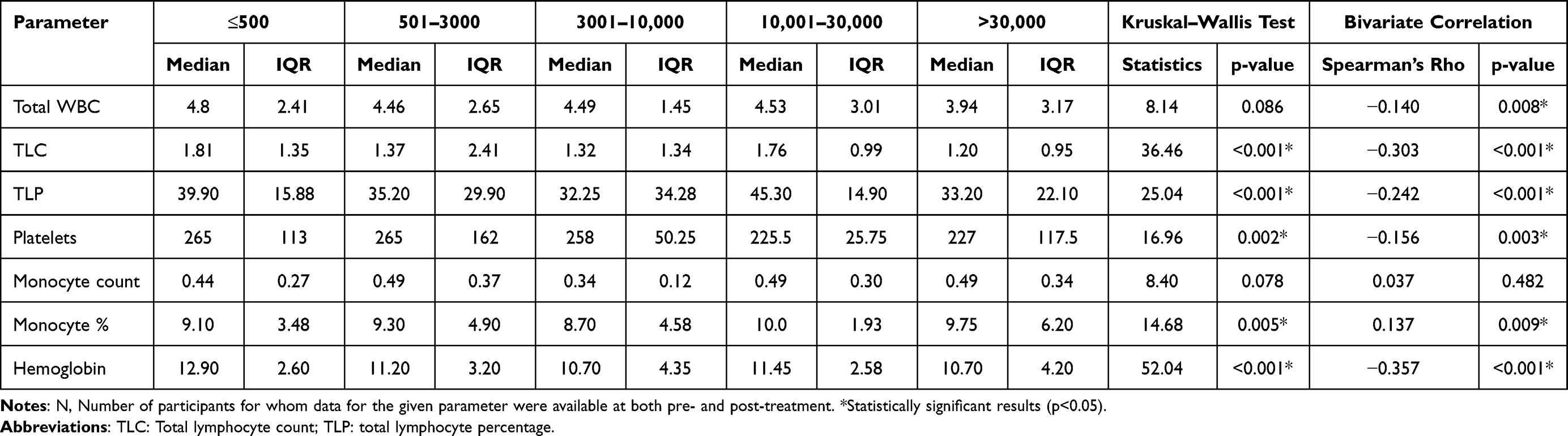 |
Table 2 Correlation of Hematological Parameters with PCR Levels (Pooled Data, N=384) |
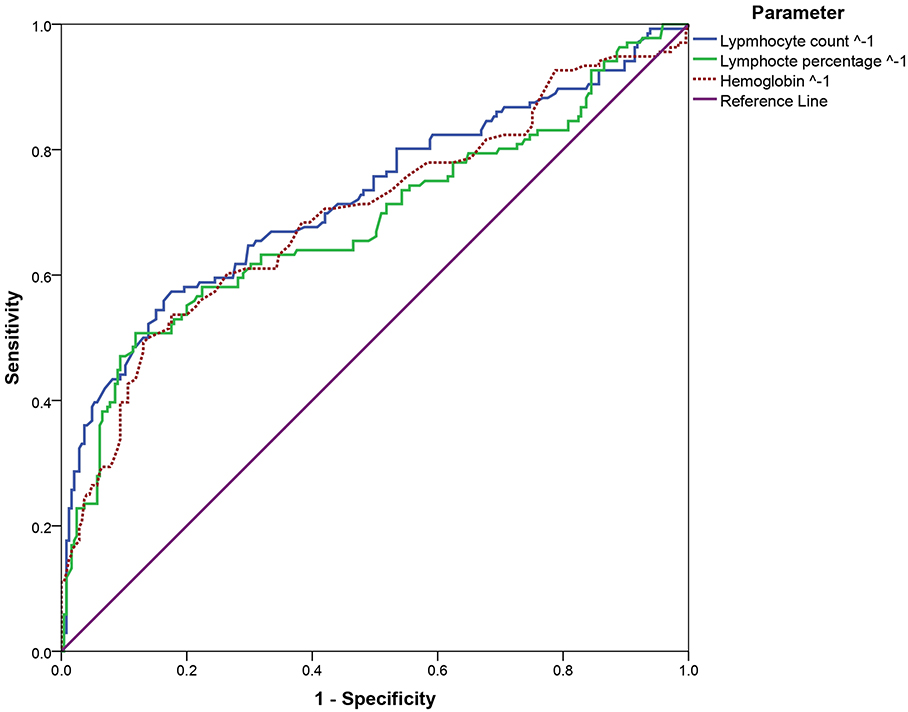 |
Figure 1 Correlation of blood cell count parameters with HIV PCR levels (N=384). |
Accuracy of CBC Parameters in Predicting CD4 Count Level and AIDS Status
The first ROC curve analysis showed an acceptable-to-high AUC for TLC (0.73, p<0.001), TLP (0.69, p<0.001), and hemoglobin level (0.70, p<0.001) for CD4 count≥200 (non-AIDS), while platelet count was not significant (AUC=0.48, p=0.542), and monocyte count and percentage showed a low AUC (0.43, p=0.029 and 0.59, p=0.004, respectively). Hence, only TLC, TLP, and hemoglobin levels were included in the second ROC curve analysis using reciprocal transformation of the variables. The AUC for TLC-1 (0.73), TLP-1 (0.69), and hemoglobin level-1 (0.70) and the corresponding cutoffs with sensitivity and specificity were determined (Figure 2 and Table 3).
 |
Table 3 Diagnostic Accuracy of Reciprocal Hematological Parameters in Predicting AIDS Status Among HIV Patients |
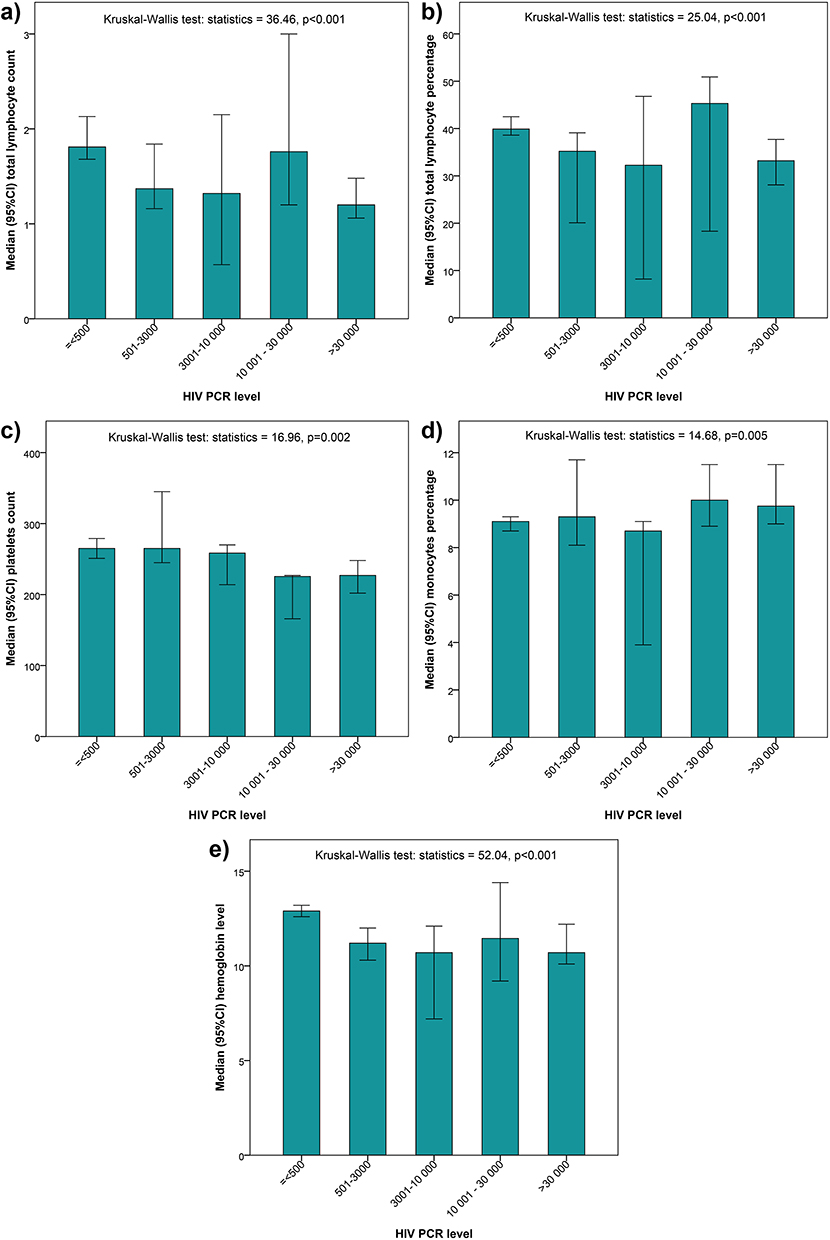 |
Figure 2 Receiver Operating Characteristic (ROC) Curve Analysis for the Significance of Reciprocal Lymphocyte Count, Percentage, and Hemoglobin Level in Predicting AIDS Status among HIV Patients. Notes: The ROC curve analysis revealed a prediction of HIV PCR level using lymphocyte count, lymphocyte percentage, platelets count and hemoglobin level. The sub figure (A) showed the low AUC for lymphocyte count (0.43, p< 0.001), while Sub figure (B), showed AUC for lymphocyte percentage (0.59, p< 0.001). Additionally, sub figure (C) reflected an acceptable-to-high AUC for platelets count (0.73, p=0.002), and sub figure (D) revealed the monocytes percentage (0.69, p=0.005). The sub figure (E) showed the hemoglobin level (0.70, p< 0.001) for CD4 count 200 (non-AIDS). |
TLC1345 cells/mm3, TLP29.07%, and hemoglobin 10.55 mg/dL were independently linked with AIDS risk using back-transformed cutoffs, with adjusted ORs of 2.92, 3.53, and 3.60, respectively (Table 4).
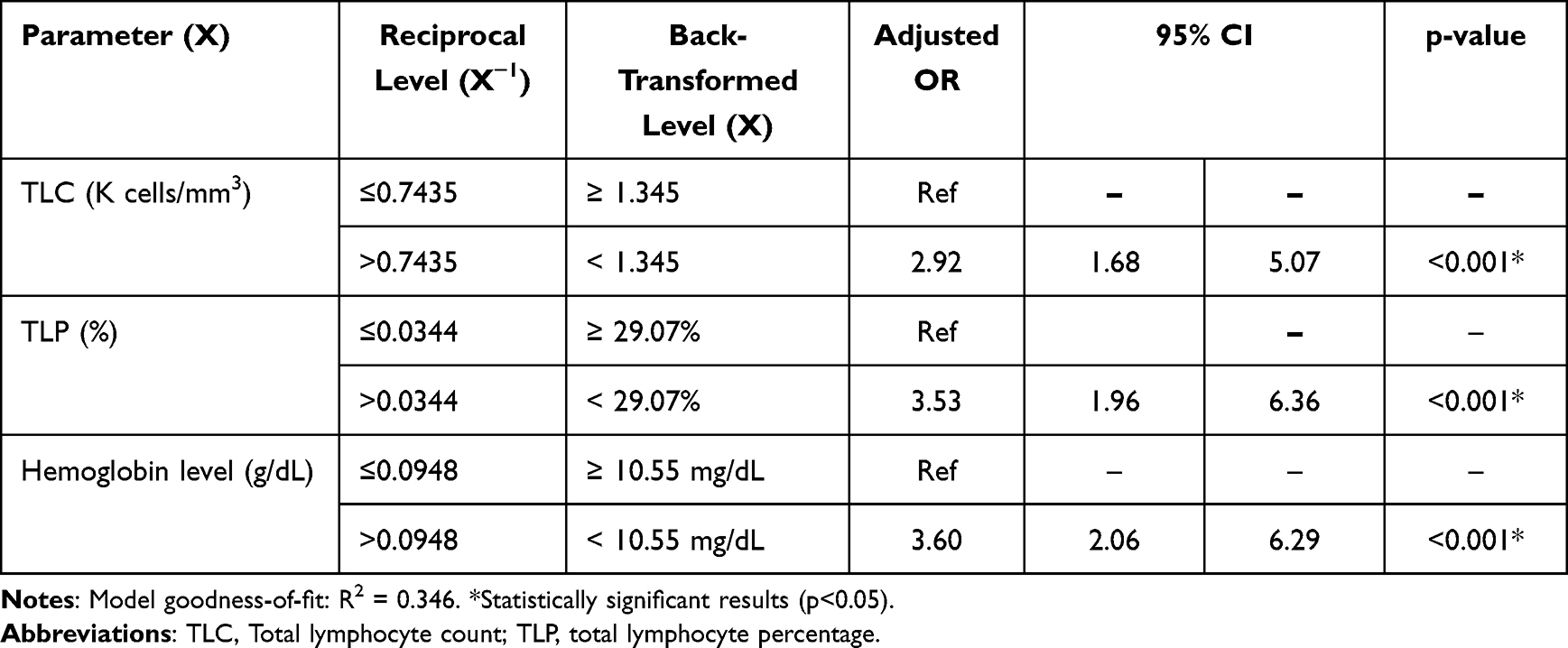 |
Table 4 Multivariate Logistic Regression Analysis of the Association Between Total Lymphocyte Count, Percentage, Hemoglobin Level, and AIDS Status (CD4<200) |
Performance of the 3-Parameter Score
Each parameter value below the specified cutoff was given a unitary score of 1; otherwise, a unitary score of 0 was given. The three unitary scores were added together to create the risk score (Table 5). As a function of risk score, the likelihood of having AIDS increased dramatically, ranging from 18.3 to 95.1%. In comparison to score 0, score 2 (two parameters below the threshold) was linked to an OR of 8.25 (95% confidence interval [CI] = 4.31, 15.81) of CD4 count 200, while score 3 (all three parameters below the cutoff) was linked to an OR of 86.96. (20.09, 376.33). A total score of 1 did not indicate any notable risk. The total model accounted for 34.6% of the variation in the CD4 count, (Table 6).
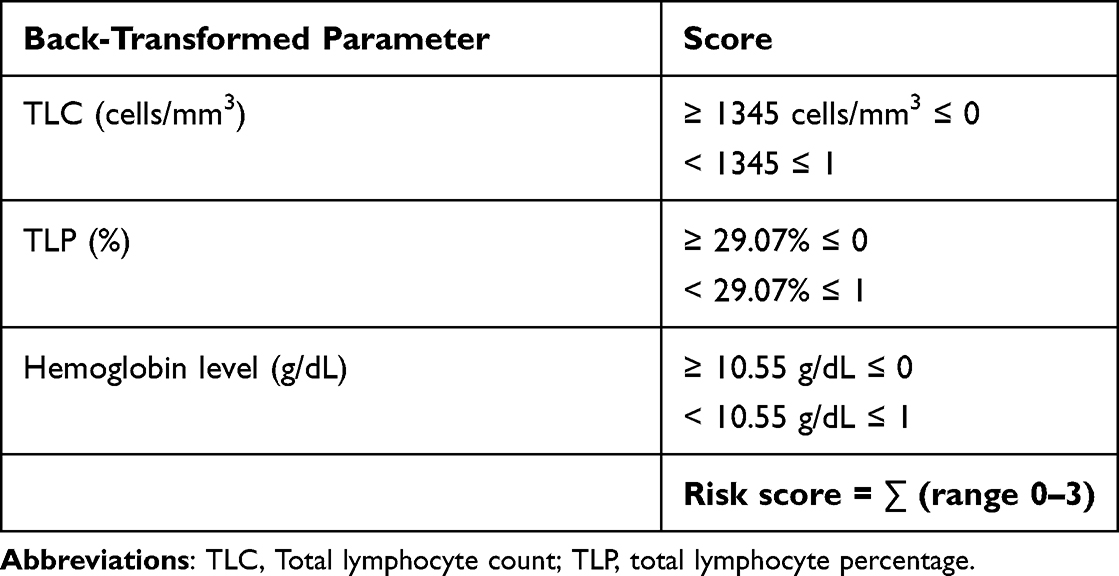 |
Table 5 Risk Score Calculation for Predicting CD4 < 200 Using TLC, TLP, and Hemoglobin |
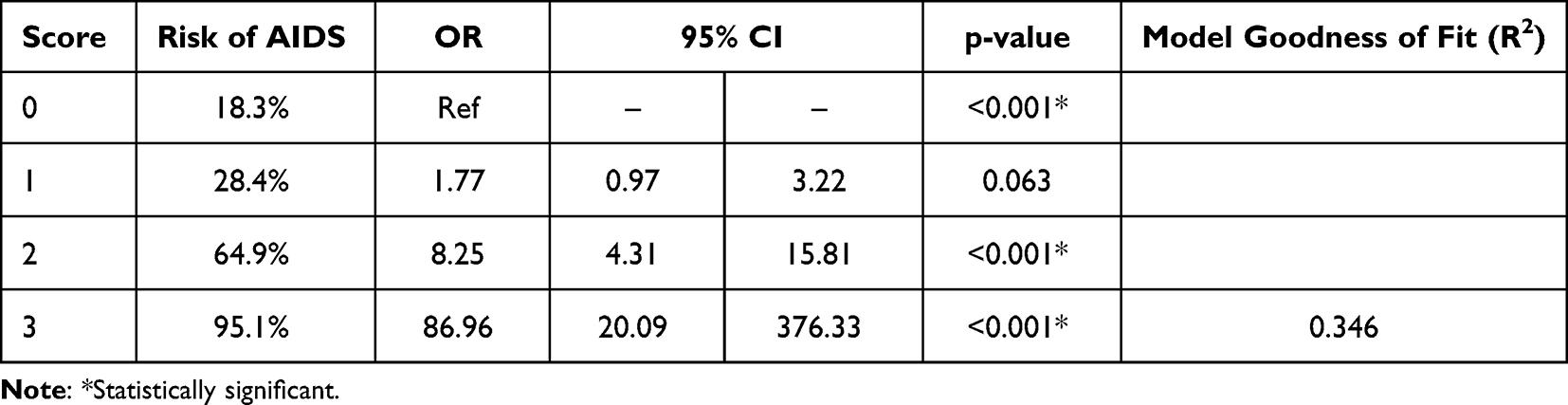 |
Table 6 Association of the Proposed Score with AIDS Status (CD < 200 Cells/Mm³) |
Discussion
Summary of Findings
Despite remarkable progress in health outcomes among PLHIV globally in the last few decades, several factors still limit access to adequate care in low-income countries.25 Our study introduces a novel composite score that combines significant hematological parameters, namely TLC, TLP, and hemoglobin concentration, to monitor HIV patients on ART. This composite score aims to provide an alternative and potentially more cost-effective approach for assessing treatment efficacy and disease progression, particularly in low-resource settings where access to viral load and CD4 count measurements may be limited. In a cohort of newly treated HIV patients, the introduction of ATR was associated with a significant increase in TLC, TLPm, and hemoglobin levels compared to baseline. In the pooled data, the viral load titer was negatively correlated with TLC and TLP, platelet count, and hemoglobin levels, while it was positively correlated with monocyte percentage; nevertheless, all these correlations were weak to moderately weak. More interestingly, reciprocal values of TLC (in thousands cells/mm3), TLP, and hemoglobin levels showed good accuracy in indicating AIDS status defined as a CD4+ count <200 cells/mm3, with a high specificity. This enabled computing cutoffs and elaborating a 3-dimension risk score model that could be easily implemented in clinical practice and predicted AIDS with 34.6% goodness-of-fit.
The Use of Lymphocyte Count and Hemoglobin in HIV Monitoring
HIV infection is associated with multiple hematological abnormalities, especially anemia and neutropenia, the prevalence and degree of which are significantly correlated with the CD4 count and disease progression.26 According to previous WHO guidelines, TLC below 1200 cells/mm3 in asymptomatic HIV patients could be used for ART initiation in low-resource settings, as it is indicative of a low CD4 count (<200 cells/mm3). However, the same WHO guidelines stated that lymphocyte count had a high positive predictive value, but a low negative predictive value.27 This is consistent with our findings that TLC <1345 cells/mm3 was indicative of a CDs count<200 with high specificity (82.4%) but relatively low sensitivity (58.1%). This limits its utility as a screening test for AIDS because of the high percentage of false negative results.
Several studies have explored the validity of TLC or hemoglobin for monitoring HIV patients in the past two decades, revealing interesting observations with mixed conclusions. A longitudinal multicenter study by Lau et al using survival analysis showed that a rapid decrease in TLC was associated with a 4.7-fold hazard ratio of progression to AIDS, while a rapid decrease in hemoglobin level was associated with a 5.5-fold hazard ratio.16 Another study assessed the accuracy of TLC in monitoring treatment efficacy by analyzing its covariance with CD4 count 24 months after the initiation of HAART. The findings showed that an increase in TLC was indicative of an increase in CD4 count with very high sensitivity (86–94%) and specificity (80–85%), and that an increase in CD4 count by 100 cells/mm3 or higher was associated with an average increase in TLC by 766 cells/mm3.28 Conversely, a study in 2007 showed a weak correlation between TLC and CD4 count (r=0.41), and predictive models using cutoffs <2000 and <1000 cells/mm3 were not significant in indicating a CD4 count<200.29 Another recent study by Wande et al analyzed the correlation of CD4 count with TLC, hemoglobin, and lymphocyte/leukocyte and lymphocyte/neutrophil ratios. TLC showed the strongest correlation with CD4 count (r=0.57), followed by lymphocyte/leukocyte ratio (r=0.51), and lymphocyte/neutrophil ratio (r=0.46), while the correlation with hemoglobin was the weakest (r=0.32).30 This is consistent with our findings showing a significant association of both viral load and CD4 count<200 with TLC and hemoglobin, in addition to TLP, which is mathematically identical to the lymphocyte/leukocyte ratio used by Muhamad et al.30
Thrombocytopenia or Thrombocytosis?
We observed that the platelet count was inversely correlated with the HIV PCR titer; however, this correlation was weak. In contrast, the platelet count showed a two-phase correlation with AIDS status, as demonstrated by the ROC curve crossing the reference line. This indicates the existence of a “turning point”, beyond which the levels of platelets count (thrombocytosis) may be paradoxically indicative for more advanced disease. This may further be indicative of drug toxicity, consistent with a study showing that 9% of patients on highly active ART had chronic thrombocytosis, which was associated with decreased natural killer cell counts and an increased risk of cardiovascular events.31 This suggests that the interpretation of platelet count changes differs by reference to the turning point and depends on potential iatrogenic factors, which challenges its use in monitoring HIV patients.
Specificity of This Study – Use of a 3-Parameter Risk Score
The specificity of the present study is the elaboration of a predictive model for CD4<200 that combines three hematological parameters, including TLC <1345 cells/mm3), TLP (<29.07%) and hemoglobin concentration (<10.55 g/dL), using their respective cutoffs in the ROC curve analysis. All three binary variables were significant in the adjusted analysis, indicating that each parameter was independently associated with the AIDS status and could be included in the cumulative risk score. A cumulative risk score of 2 (two out of three parameters below the cutoff) was associated with an 8.25-fold risk of AIDS, and this risk was multiplied by 10 for a cumulative score of 3 (OR=87). However, the goodness-of-fit of the model was moderate, as it explained 34.6% of the CD4 count variance. The main advantage of this model is its practicality and ease of implementation in routine practice, particularly in low-resource settings. However, the interpretation of the risk score for a specific patient should consider the baseline values and normal variability between repeated measurements. Further studies are warranted to assess the validity of this model and to determine its further application conditions and improvement perspectives.
Limitations of the Hematological Parameters in Monitoring HIV
The present approach of using hematological parameters to monitor HIV patients is limited by the hematological toxicity of ART drugs. This is the case for patients on zidovudine-containing regimens, which entail a relatively high risk of anemia, especially during prolonged periods of use.32 Zidovudine has been demonstrated to have a dose-dependent cytotoxic effect on erythroid precursor cells in the bone marrow.33 Other iatrogenic factors may interfere with anemia in patients with HIV, such as cotrimoxazole prophylaxis,34 the confounding effect of which should be addressed in further studies and considered for each specific case. This represents a strong confounder for the model developed in the present study, notably when drug toxicity is associated with low adherence to treatment, which may falsely potentiate the correlation between anemia and HIV PCR and CD4 count. However, one should consider that the risk of anemia is drug- and time-dependent, and may be potentiated by other factors inherent to disease progression. A study from Cambodia involving 1180 patients who were on a zidovudine-containing regimen showed that 12% developed anemia after one year of treatment, leading to the discontinuation of zidovudine. Analysis of the cumulative incidence curve showed that the risk was 5% at three months and 10% at 6 months.35 Another Ethiopian study observed a prevalence of anemia as high as 26% among treated HIV patients, which was associated with advanced stages of the disease and a history of opportunistic infections, whereas drug-induced anemia accounted for only 5.5%.36 This finding suggests that the use of the model developed in the present study can be considered after ruling out all iatrogenic and other confounding factors that affect hematological parameters, which may be time- and resource-intensive in routine practice.
Methodological Limitations
The present model was developed on the basis of a retrospective series of patients with readily available parameters of interest. This is exposed to selection and information bias, which may affect the generalizability of the model. Therefore, it is necessary to test the validity of the present model in a prospective series of patients by using a more rigorous data collection procedure, which could further improve the model.
Conclusion
The study reveals the clinical utility of the three haematological parameters (total lymphocyte count, lymphocyte percentage, and haemoglobin concentration) as cost-effective tests for monitoring HIV patients in low resource settings, particularly where viral load and CD4 count assessments are absent. Independently, each parameter shows high specificity in predicting AIDS status, with defined cutoff values. Moreover, the combination of these parameters in a cumulative risk score significantly enhances their predictive value, indicating an approximately 8-fold to 87-fold increase in the risk of AIDS progression for scores of 2 and 3, respectively. These findings underscore the promise of our composite risk score as a practical tool for HIV patient management.
Data Sharing Statement
Data are available upon request from the corresponding author.
Ethics Approval and Consent to Participate
This study was approved by the Research Ethics Committee of King Abdulaziz University (Ref # 197-22). The consent forms were not taken from the patients since the data used was from the records previously collected and there was no presence of patients at the time of data collection. The review board confirmed this issue and provided the ethical approval. The patient data was kept with confidentiality and compliance with the Declaration of Helsinki.
Acknowledgment
The author is grateful to Scientia Vallis (Paris, France), represented by Dr Mohamed Amine Haireche, for valuable inputs in the statistical analysis and editing of the present manuscript.
Funding
The author thanks the Deanship of Scientific Research of King Abdul-Aziz University, Jeddah, Saudi Arabia (RG-12-140-42) for funding this research.
Disclosure
The author reports no conflicts of interest in this work.
References
1. UNAIDS. AIDS statistics—fact sheet. Unaids org; 2021.
2. Barbaro G, Scozzafava A, Mastrolorenzo A, Supuran CT. Highly active antiretroviral therapy: current state of the art, new agents and their pharmacological interactions useful for improving therapeutic outcome. Curr Pharm Des. 2005;11(14):1805–1843. doi:10.2174/1381612053764869
3. Nosyk B, Min JE, Lima VD, Hogg RS, Montaner JS. Cost-effectiveness of population-level expansion of highly active antiretroviral treatment for HIV in British Columbia, Canada: a modelling study. Lancet HIV. 2015;2(9):e393–e400. doi:10.1016/S2352-3018(15)00127-7
4. HIV/AIDS JUNPo. Fast-track: ending the AIDS epidemic by 2030. Geneva: UNAIDS; 2014.
5. UNAIDS. Report on the global AIDS epidemics 2012; 2012.
6. Parker R. The global HIV/AIDS pandemic, structural inequalities, and the politics of international health. Am J Public Health. 2002;92(3):343–347. doi:10.2105/AJPH.92.3.343
7. Mwau M, Syeunda CA, Adhiambo M, et al. Scale-up of Kenya’s national HIV viral load program: findings and lessons learned. PLoS One. 2018;13(1):e0190659. doi:10.1371/journal.pone.0190659
8. Lecher S, Williams J, Fonjungo PN, et al. Progress with scale-up of HIV viral load monitoring—seven sub-Saharan African countries, January 2015–June 2016. Morb Mortal Wkly Rep. 2016;65(47):1332–1335. doi:10.15585/mmwr.mm6547a2
9. Gilks C, Vitoria M. Antiretroviral therapy for HIV infection in adults and adolescents: recommendations for a public health approach. Antiretroviral therapy for HIV infection in adults and adolescents: recommendations for a public health approach; 2006.
10. World Health Organization. Antiretroviral Therapy for HIV Infection in Adults and Adolescents: Recommendations for a Public Health Approach-2010 Revision. World Health Organization; 2010.
11. Belaunzarán-Zamudio PF, Caro-Vega YN, Shepherd BE, et al. Monitoring of HIV treatment in seven countries in the WHO region of the Americas. Bull World Health Organ. 2015;93:529–539. doi:10.2471/BLT.14.147447
12. Ford N, Meintjes G, Pozniak A, et al. The future role of CD4 cell count for monitoring antiretroviral therapy. Lancet Infect Dis. 2015;15(2):241–247. doi:10.1016/S1473-3099(14)70896-5
13. Kwantwi LB, Tunu BK, Boateng D, Quansah DY. Body mass index, haemoglobin, and total lymphocyte count as a surrogate for CD4 count in resource limited settings. J Biomark. 2017;2017:1–6. doi:10.1155/2017/7907352
14. Acheampong I, Quaye L, Obirikorang C. Total lymphocyte count as a surrogate marker for CD4 count in resource-limited settings; 2012.
15. Rostina R, Aprianti S, Arif M. Prediksi jumlah sel limfosit T Cd4+ menggunakan nilai TLC (total lymphocyte count) pada penderita HIV/Aids. Indones J Clinical Pathol Med Lab. 2008;14(2):64–65. doi:10.24293/ijcpml.v14i2.902
16. Lau B, Gange SJ, Phair JP, Riddler SA, Detels R, Margolick JB. Use of total lymphocyte count and hemoglobin concentration for monitoring progression of HIV infection. JAIDS. 2005;39(5):620–625.
17. Zhang Q, Rojhani A, Gulló-Rivera A, Kwak S. Prevalence and knowledge of anemia among pregnant women enrolled in women, infants and children supplemental food program. Nutr Food Sci. 2018;48(6):990–1002. doi:10.1108/NFS-03-2018-0097
18. Spacek LA, Griswold M, Quinn TC, Moore RD. Total lymphocyte count and hemoglobin combined in an algorithm to initiate the use of highly active antiretroviral therapy in resource-limited settings. AIDS. 2003;17(9):1311–1317. doi:10.1097/00002030-200306130-00005
19. Ancuta P, Kamat A, Kunstman KJ, et al. Microbial translocation is associated with increased monocyte activation and dementia in AIDS patients. PLoS One. 2008;3(6):e2516. doi:10.1371/journal.pone.0002516
20. Mathews SE, Srivastava D, Yadav RB, Sharma A. Association of hematological profile of human immunodeficiency virus-positive patients with clinicoimmunologic stages of the disease. J Lab Physicians. 2013;5(01):34–37. doi:10.4103/0974-2727.115929
21. Daka D, Loha E. Relationship between Total Lymphocyte Count (TLC) and CD4 count among peoples living with HIV, Southern Ethiopia: a retrospective evaluation. AIDS Res Ther. 2008;5:1–5. doi:10.1186/1742-6405-5-26
22. Akanmu A, Akinsete I, Eshofonie A, Davies A, Okany C. Absolute lymphocyte count as surrogate for CD4+ cell count in monitoring response to antiretroviral. Niger Postgrad Med J. 2001;8(3):105. doi:10.4103/1117-1936.170869
23. Mellors JW, Munoz A, Giorgi JV, et al. Plasma viral load and CD4+ lymphocytes as prognostic markers of HIV-1 infection. Ann Intern Med. 1997;126(12):946–954. doi:10.7326/0003-4819-126-12-199706150-00003
24. Yoshimura K. Current status of HIV/AIDS in the ART era. J Infect Chemother. 2017;23(1):12–16. doi:10.1016/j.jiac.2016.10.002
25. Abgrall S, Del Amo J. Effect of sociodemographic factors on survival of people living with HIV. Curr Opin HIV AIDS. 2016;11(5):501–506. doi:10.1097/COH.0000000000000301
26. Munyazesa E, Emile I, Mutimura E, et al. Assessment of haematological parameters in HIV-infected and uninfected Rwandan women: a cross-sectional study. BMJ open. 2012;2(6):e001600. doi:10.1136/bmjopen-2012-001600
27. World Health Organization. Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV Infection: Recommendations for a Public Health Approach. World Health Organization; 2016.
28. Mahajan AP, Hogan JW, Snyder B, et al. Changes in total lymphocyte count as a surrogate for changes in CD4 count following initiation of HAART: implications for monitoring in resource-limited settings. JAIDS. 2004;36(1):567–575. doi:10.1097/00126334-200405010-00004
29. Mbanya D, Assah F, Ndembi N, Kaptue L. Monitoring antiretroviral therapy in HIV/AIDS patients in resource-limited settings: CD4 counts or total lymphocyte counts? Int J Infect Dis. 2007;11(2):157–160. doi:10.1016/j.ijid.2006.02.008
30. Muhamad RF, Solichul H, Hadi S. The correlation between total lymphocyte count, hemoglobin levels, lymphocyte/leukocyte ratio (LLR), and lymphocyte/neutrophil ratio (LNR) to CD4 levels in patients with human immunodeficiency virus infection at sanglah hospital. Bali Med J. 2019;8(2):429–433. doi:10.15562/bmj.v8i2.1408
31. Miguez-Burbano M, Burbano X, Rodriguez A, Lecusay R, Rodriguez N, Shor-Posner G. Development of thrombocytosis in HIV+ drug users: impact of antiretroviral therapy. Platelets. 2002;13(3):183–185. doi:10.1080/0953371027984
32. Zhou J, Jaquet A, Bissagnene E, et al. Short-term risk of anaemia following initiation of combination antiretroviral treatment in HIV-infected patients in countries in sub-Saharan Africa, Asia-Pacific, and central and South America. J Int AIDS Soc. 2012;15(1):1–12. doi:10.1186/1758-2652-15-5
33. Nordic Medical Research Councils’ HIV Therapy Group. Double blind dose-response study of zidovudine in AIDS and advanced HIV infection. BMJ. 1992;304:13–17. doi:10.1136/bmj.304.6818.13
34. Berhane Y, Haile D, Tolessa T. Anemia in HIV/AIDS Patients on antiretroviral treatment at ayder specialized Hospital, Mekele, Ethiopia: a case-control study. J Blood Med. 2020;Volume 11:379–387. doi:10.2147/JBM.S275467
35. Phe T, Thai S, Veng C, Sok S, Lynen L, van Griensven J. Risk factors of treatment-limiting anemia after substitution of zidovudine for stavudine in HIV-infected adult patients on antiretroviral treatment. PLoS One. 2013;8(3):e60206. doi:10.1371/journal.pone.0060206
36. Aynalem YA, Shibabaw Shiferaw W, Woldiye Z. Prevalence of anemia and its associated factors in antiretroviral-treated HIV/AIDS-positive adults from 2013 to 2018 at Debre Berhan Referral Hospital, Ethiopia. Adv Hematol. 2020;2020:1–7. doi:10.1155/2020/2513578
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.