")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 20
Determinants of Metabolic Syndrome Among Patients Receiving Anti-Retro-Viral Treatment in A Tertiary Hospital, Central Ethiopia: Unmatched Case–Control Study
Authors Jarso G , Aman H , Megerso A
Received 29 December 2023
Accepted for publication 11 March 2024
Published 18 March 2024 Volume 2024:20 Pages 195—205
DOI https://doi.org/10.2147/TCRM.S453699
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Godana Jarso,1 Haji Aman,2 Abebe Megerso2
1Department of Internal Medicine, Adama Hospital Medical College, Adama, Oromia, Ethiopia; 2Department of Public Health, Adama Hospital Medical College, Adama, Oromia, Ethiopia
Correspondence: Abebe Megerso Adlo, Tel +251911044525, Email [email protected]; [email protected]
Purpose: Scaling up antiretroviral treatment (ART) reduces morbidity and mortality among people living with HIV/AIDS (PLHA). This success is challenged by the constellation of interrelated metabolic disorders such as metabolic syndrome (MetS). Given the changing ART regimens and schedules, increasing patient age and methodological limitations, existing evidence regarding the determinants of MetS remains inconclusive. Therefore, in the current study, we aimed to identify the determinants of MetS in patients receiving ART at a tertiary hospital in central Ethiopia.
Patient and Methods: We conducted an unmatched case–control study that included 393 patients with a case-to-control ratio of 1 to 2. Data were collected by interviewing patients, reviewing charts, physical examinations, and laboratory testing. The data were entered into Epi-Info version 7.2 and analyzed using SPSS version 26. A binary logistic regression analysis was used to identify the determinants of MetS. The adjusted odds ratio (AOR) with a 95% confidence interval (CI) was used to estimate the strength of the association between MetS and its determinants. Statistical significance was set at p-value < 0.05.
Results: In this study, higher odds of developing MetS were identified among patients aged 40– 60 years (AOR 3.75; 95% CI: 1.66– 8.49) and those older than 60 years (AOR 6.18; 95% CI: 2.12– 17.95) than among those aged < 40 years. Similarly, higher odds were observed among patients who frequently consumed animal source foods than among those who consumed cereals or vegetables (AOR, 1.94; 95% CI, 1.03– 3.63), those who had HIV lipodystrophy (AOR 1.73; 95% CI: 1.05– 2.86), those who were treated with stavudine (AOR 3.08; 95% CI: 1.89– 5.04), and those who were treated with zidovudine (AOR 1.71, 95% CI: 1.02– 2.88) compared to their counterparts.
Conclusion: Older age, diet from animal sources, exposure to zidovudine or stavudine, and the presence of lipodystrophy were independent determinants of MetS.
Keywords: adama, cardiometabolic, diabetes, dyslipidemia, hypertension, obesity
Introduction
Metabolic syndrome (MetS) is a constellation of interrelated metabolic conditions including abdominal obesity, elevated blood pressure, dyslipidemia, and hyperglycemia.1 Several criteria were used to define MetS by different organizations. MetS was defined by the presence of insulin resistance (IR) or its markers, impaired glucose tolerance (IGT), or type-2 diabetes mellitus (T2DM), as essential components of the syndrome, along with at least two of the following parameters: elevated blood pressure, hypertriglyceridemia, and/or low high-density lipoprotein-cholesterol (HDL-c), central obesity, and microalbuminuria, with different weights given to each component.2,3
In 2001, the National Cholesterol Education Program Adult Treatment Panel III (NCEP: ATPIII) published a new set of criteria, which included waist circumference, blood lipids, blood pressure (BP), and fasting glucose. These criteria differed from both the WHO and the European Group for the Study of Insulin Resistance (EGIR) definitions in that IR was not considered a mandatory component.4 Subsequently, the International Diabetes Federation (IDF) published newer criteria with obesity as a prerequisite for the diagnosis of MetS, in an attempt to improve comparability in different settings and better prediction of cardiovascular risk.5
In 2009, the joint interim statement (JIS) of the IDF Task Force on Epidemiology and Prevention, the National Heart, Lung, and Blood Institute, the American Heart Association, the World Heart Federation, the International Atherosclerosis Society, and the International Association for the Study of Obesity suggested using the IDF global consensus definition as the presence of three or more of the five parameters but without central obesity as an obligatory parameter.6
A major importance of MetS is that it is an important predictor of cardiovascular disease (CVD) and T2DM risks.7 Studies have shown that adult individuals with MetS have three times the risk and a five-fold greater risk of acquiring CVDs and T2DM, respectively.8
The introduction and expansion of antiretroviral therapy (ART) in the mid-1990s has led to a decline in morbidity and mortality among PLHA, but was later followed by an increase in cardiometabolic diseases such as obesity, hypertension, dyslipidemia, and T2DM.9
Although the magnitude of MetS in PLHA is still debatable, the reported global prevalence of MetS in PLHA ranges from 11.2% to 45.4%, although there are variations in prevalence based on the diagnostic criteria used to define MetS itself.10,11 Similarly, a systematic review from Africa showed the prevalence of MetS among PLHA to be 21.5% with substantial heterogeneity.12 Furthermore, a study from Ethiopia showed that the cumulative proportion of MetS was 42.5%.13
The exact mechanism of MetS in PLHA is not well known but believed to be due to an interaction between HIV-triggered low-grade inflammatory injury, alterations in lipid and glucose metabolism, and fat redistribution.14 Use of ART is associated with body fat redistribution and cardio-metabolic abnormalities such as hypertension, dyslipidemia, insulin resistance, and dysglycemia.15 Although exposure to other modifiable risk factors such as unhealthy diets and reduced physical activity contribute to MetS, additional influences exceptional to PLHA further escalate their susceptibility to cardio-metabolic abnormalities.16 Moreover, HIV infection itself through chronic inflammation and immune dysfunction mechanisms and metabolic side effects of ART medications is expected to be determinants of MetS.17,18 Studies have shown that factors related to socio-demographic characteristics, behavior and lifestyle, as well as HIV and its treatment are potential predictors of MetS in PLHA.9,19 Among socio-demographic factors, age and gender have been reported as a consistent predictor of MetS by many studies across the globe.20,21 A systematic review of global studies on PLHA reported that males were about three times more likely to have metabolic disorders than females.22 However, a study from Ethiopia showed rather females were twice at risk compared to males.23 Different lifestyle and behavioral factors such as smoking, alcohol use, lack of physical activity and obesity have been reported by many researchers to have significant association with metabolic syndrome.24,25 A study from the United States showed that the prevalence of MetS was higher among those who spend longer time engaged in sedentary activities such as watching television or videos or using a computer.24
Factors related to HIV infection and its treatment have been considered as determinants in the development of MetS in PLHA.26 One of which is advanced disease stage (AIDS), which has been reported in studies in white population to be significant determinants of MetS.27 Another study also showed that disease severity indicators, such as the level of CD4+ counts, the duration of diagnosed HIV infection, exposure to ART, and type of regimen used, were strong predictors of MetS in PLHA.11
However, available evidence regarding the determinants of MetS in PLHA populations is inconsistent and inconclusive. Moreover, most previous studies analyzed data collected for clinical care purposes and did not include many potential determinants with no uniformity in the definitions of MetS. Another limitation of previous studies was the use of a cross-sectional design with odds ratios as a measure of the association between various independent variables and MetS. When the magnitude of MetS is high (>10%), the use of odds ratios leads to erroneous results.28 Additionally, ART regimens and their schedules frequently change over time, which can lead to differences in the results of previous studies.
Therefore, this study was designed to identify independent determinants of MetS with due attention to address at least some of the drawbacks observed in the existing literature by using the most comprehensive criteria of MetS, the JIS,29 a better study design, primary data collected for the purposes of the study, and evaluation of patient data by senior internists and laboratory technologists. Therefore, results of this work will add useful information to existing body of literature, contribute to the identification of factors that may cause MetS in PLHA, and may provide opportunities for treatment and thereby improve quality of life.
Methods and Materials
Study Setting and Period
This study was conducted at Adama Comprehensive and Specialized Hospital, a referral teaching hospital of Adama Hospital Medical College, located in the Oromia region, Adama City, approximately 100 km southeast of Addis Ababa. The hospital is among the first few hospitals in Ethiopia that started ART services and has the second largest HIV/ART clinic with over 20000 PLHA enrolled in comprehensive care in all categories of care, including those on 1st line, 2nd line, and 3rd line regimens for the last two decades.
The HIV clinic uses the national consolidated HIV guideline for HIV care, which is based on “test-and-treat” approach irrespective of their CD4 count and compressive care for opportunistic infection prevention and treatment including for tuberculosis.
Most regimens are based on nucleoside reverse transcriptase inhibitors (NRTI), non-nucleoside reverse transcriptase inhibitors (NNRTI), and boosted protease inhibitors (PIs). The preferred first-line regimen for adults and adolescents is TDF+3TC+DTG or TDF+3TC+EFV at a once-daily dose. Fixed-dose and once-daily regimens are preferred for antiretroviral therapy.
Study Design
Facility-based unmatched case–control study was conducted.
Population
All adult PLHA enrolled in ART at the hospital were considered the source population, while all adult PLHA who received ART during the data collection period were considered the study population for the current study. The study units were individual PLHA on ART, who were randomly selected as either cases or controls.
Cases: Adult PLHA who received ART at the Hospital during the study period was diagnosed with MetS based on the case ascertainment criteria described below.
Controls: Adult patients who received ART at the Hospital during the study period confirmed the absence of MetS based on the criteria.
Inclusion and Exclusion Criteria
Inclusion
Adult PLHA aged 18 years or older who had been on ART for at least six months period and attended the service during the data collection period were included in the study.
Exclusion
Pregnant women and patients with known familial hypercholesterolemia were excluded from the study because these affect waist circumference and cholesterol levels.
Sample Size Determination and Sampling Procedure
Sample Size Determination
Sample sizes were calculated using different variables reported in previous studies using the Epi Info application software30 statistical calculator for an unmatched case–control study with the assumption of a power of 80% and two-sided confidence level of 95%. A case–control ratio of 1:2 was used to calculate the sample size for potential determinants, such as sex, duration of HIV infection, duration of ART, sedentary lifestyle, and lipodystrophy identified in the literature reviewed for this purpose.
Of these determinants, ART duration of ≥5 years was found to be the main exposure variable for MetS, which produced the largest of the calculated sample sizes. Accordingly, 419 patients were evaluated to identify 131 patients. Of the 288 MetS-free patients evaluated, 262 were randomly selected, resulting in a final sample size of 131 cases and 262 controls, with a total of 393.
Sampling Methods
Case Identification Procedure
Cases were identified by screening all adult patients visiting Adama Hospital for HIV care follow-up with consent to participate in the study. Initially patients are interviewed for socio-demographic and behavioral factors such as smoking, alcohol intake, physical activity, and dietary habits using a questionnaire adapted from the WHO STEPS instrument.31 In addition to this screening for lipodystrophy was done. This was followed by physical measurements including BP, body weight, height, and waist circumference (WC). Blood samples were taken from patients for biochemical measurements, including fasting plasma glucose levels and lipid profiles (total cholesterol, triglycerides, and high- and low-density lipoprotein cholesterol).
Finally, all the physical and biochemical measurement data gathered were used to ascertain and classify participants as a case (those with MetS) or a control (those without MetS), using the below designated MetS diagnosis criteria.
Methods of Case Ascertainment
The cases were ascertained based on the JIS29 of the International Diabetes Federation Task Force on Epidemiology and Prevention criteria, which require the presence of any three of the five risk factors constituting a diagnosis of MetS and the international IDF criteria, as having at least three of the following traits:
- Waist circumference ≥ 94 cm or 40 inches (male), ≥ 88 cm or 35 inches (female)
- Dyslipidemia-1: (triglyceride level ≥ 150 mg/dl (1.7 mmol/L)) or treatment
- Dyslipidemia-2 (HDL-C < 40 mg/dL (male), < 50 mg/dL (female)) or on treatment
- BP ≥ 130/85 mmHg or antihypertensive medication
- Fasting plasma glucose levels ≥ 100 mg/dl (6.1 mmol/L) or previous diagnosis of type 2 diabetes mellitus or antidiabetic treatment.
Control Selection Method
The number of controls was determined based on the number of cases identified as the required sample at a ratio of 1:2. We consecutively included 419 eligible patients until 131 patients (those with MetS) were identified. Of the remaining 288 patients (those without MetS), 262 patients were randomly included as controls.
Data Collection
The data collection was done using a standardized questionnaire adapted from WHO – STEPS instrument for assessment of non-communicable diseases (NCDs).31 The data on socio-demographic, behavioral/lifestyle, HIV, and ART related clinical factors were obtained from multiple sources through face-to-face interview, review of patient’s record, and focused physical examination by trained health personnel. Physical measurement data, including blood pressure, body weight, height, and waist circumference (WC), were collected using a BP apparatus (aeromed digital apparatus), weight scale, height scales, and tape meter.
Likewise, biochemical measurements, including fasting plasma glucose levels and lipid profiles, were collected through laboratory tests, arranged the day after completion of the physical measurements of the data collection process and after overnight fasting, by drawing–3–5 mL of Venus blood.
Data Quality Assurance
Trained nurses collected data using a questionnaire adapted from the WHO STEPS tool for non-communicable disease risk surveys and pre-tested it in other health facilities. Physical measurements such as blood pressure, weight, height, and abdominal circumference were collected using standardized and validated equipment. Training regarding the data collection tools and procedures was provided to the data collectors before embarking on the main study. Data were collected after one day of training by a laboratory technician on sample collection, standard operating procedure, and reporting using a standardized chemistry machine at designated centers. At the end of each day of data collection, the collected data were double-checked and the status of the patient was determined by a consultant internist.
Data Processing and Analysis
The collected data were coded and entered into a computer using EpiInfo 7.2 application software and exported to SPSS version 26 for processing and analysis. Descriptive statistical analysis techniques such as frequency distribution and numerical summary measures were used to summarize the characteristics of the study participants, and the results are presented in the tables.
The outcome variable was dichotomized as having metabolic syndrome (MetS) and not having MetS and coded as 1 and 0, respectively. A binary logistic regression analysis was used to identify the determinants of MetS. First, a simple regression analysis was performed in which all covariates were regressed with MetS one by one, in order to assess the presence of crude association. At this level, the independent variables with P-value < 0.25 were selected as candidates for adjusted regression analysis. The final logistic regression model was fitted using the enter or standard model-building approach. The goodness of fit of the fitted regression model was tested using the Hosmer–Lemeshow goodness-of-fit test, which was 0.426 for the final model. Multicollinearity was also checked for a variance inflation factor, which was less than five. The strength of association was estimated in an adjusted odds ratio with 95% confidence interval, and p-value <0.05, was used to determine the significance of associations between dependent and independent variables.
Results
Characteristics of the Study Participants
Among the study participants, 67 (51.1%) cases and 91 (34.7%) controls were female, while 104 (79.4%) cases and 177 (67.6%) controls were aged 40–60 years. Furthermore, 123 (93.9%) cases and 237 (90.5%) controls were urban residents, whereas 73 (55.7%) cases and 109 (41.6%) controls attended secondary or higher education (Table 1).
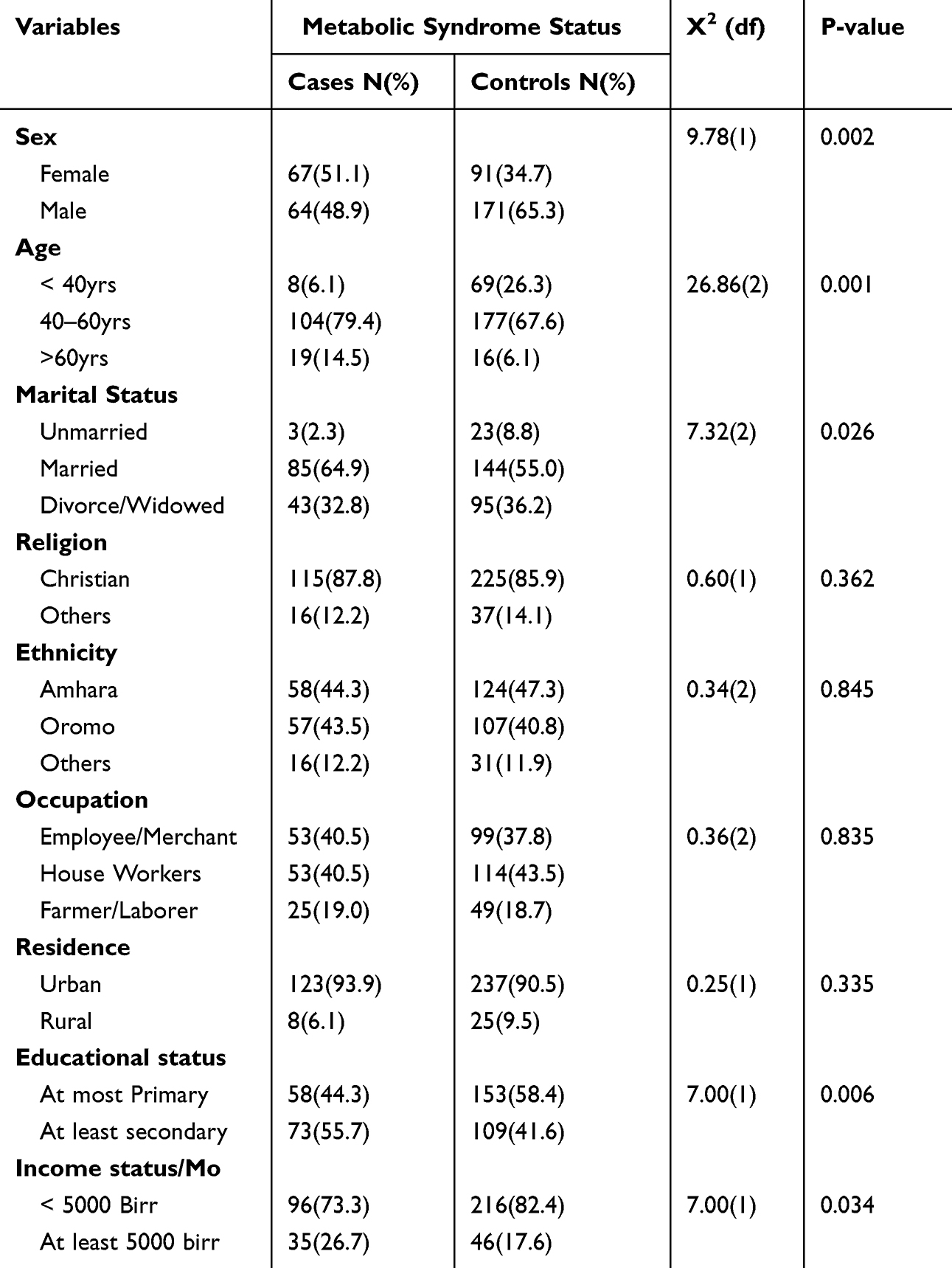 |
Table 1 Socio-Demographic Characteristics of the Study Participants, Who Were on ART at ACSH, Oromia Region, Ethiopia, 2023 |
Regarding the behavioral characteristics of the study participants, 21 (16%) and 63 (24%) controls reported alcohol use described by standard drink (12gm Alcohol) as one unit. Frequent consumption of diets from animal sources (meat or milk products consumption more than three times per week) was reported in 33 (25.2%) and 29 (11.1%) cases and controls, respectively. Physical activity for at least 30 min/day was reported in 49 (37.0%) and 89 (34.0%) patients, respectively.
The median ART duration was 15 years (IQR=11–19) years in both the cases and controls. The mean baseline weight was 58 (±SD,11.0) Kgs in the patient group and 50 (±SD,8.8) Kgs in the control group. Ever use of Zidovudine (ZDV) was administered to 53 (40.5%) patients and 66 (25.2%) controls. Similarly, the use of stavudine (d4T) was 75 (57.3%) and 80 (30.5%) for cases and controls, respectively (Table 2).
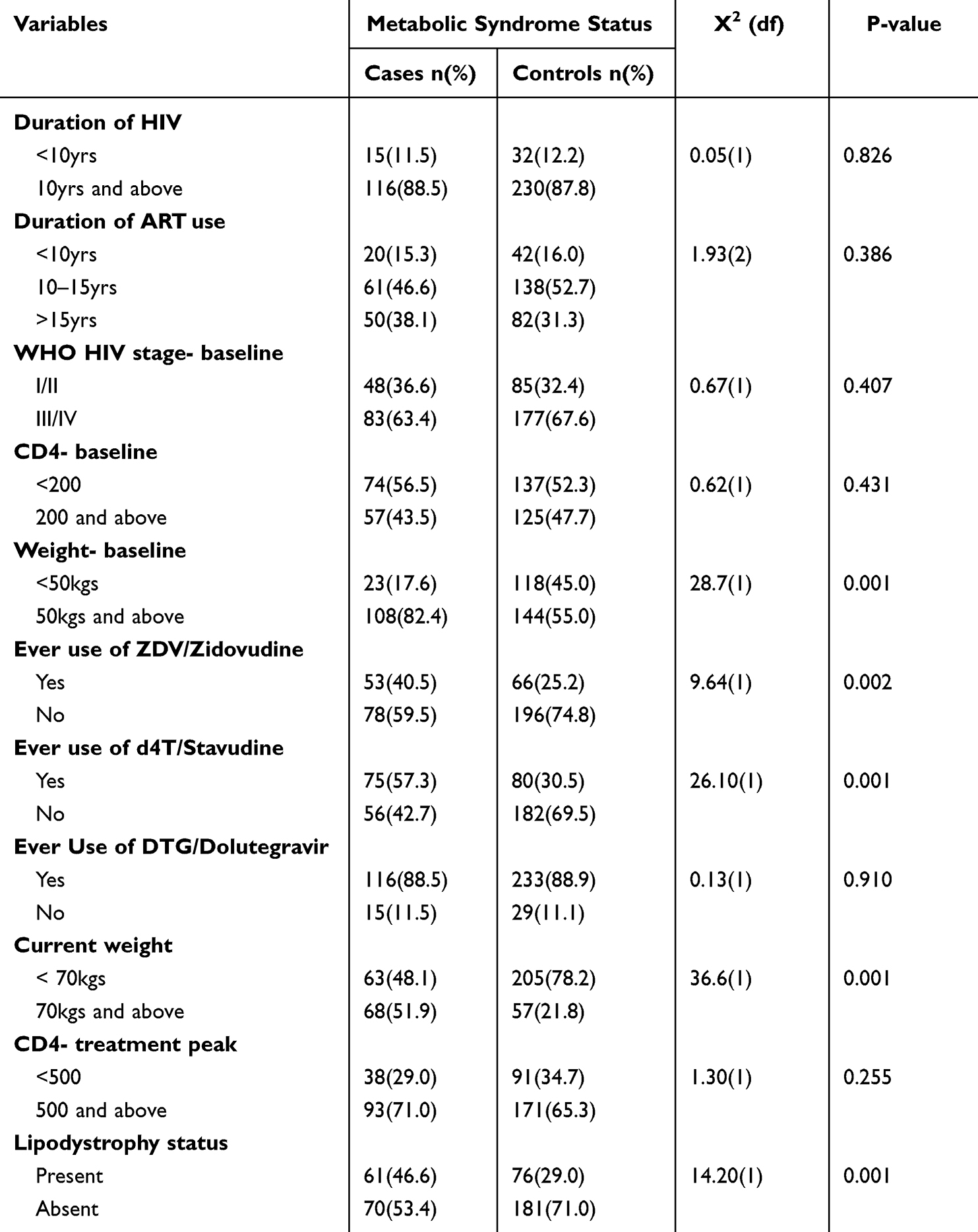 |
Table 2 HIV- and ART-Related Characteristics of Cases and Controls, Who Were on ART at ACSH, Oromia Region, Ethiopia, 2023 |
Determinants of the Metabolic Syndrome
In the final model of the analysis, after adjusting for potential confounding effects, age, dietary source, baseline weight, ever use of d4T, and ever use of ZDV and HIV lipodystrophy were significantly associated with MetS.
Accordingly, the odds of developing MetS were approximately four-fold higher among PLHA aged 40–60 yrs (adjusted odds ratio (AOR: 3.75; 95% CI: 1.66–8.49)) and 6.18-fold higher among patients aged 60 years and above (AOR: 6.18; 95% CI: 2.13–17.95) as compared to those younger than 40 years.
Similarly, the odds of developing MetS were nearly two-fold higher among patients who frequently consumed or whose typical weekly dietary source was from animal source foods compared to those whose dietary sources were from cereals or vegetables (AOR, 1.94; 95% CI: 1.03–3.63). Patients with a baseline weight > 50 Kgms had 3.61 times higher odds of having MetS than those with a baseline weight of less than 50 kg (AOR 3.61; 95% CI: 2.02–6.46).
Likewise, the odds of developing MetS were higher among patients who had lipodystrophy than among those who did not have lipodystrophy (AOR 1.73; 95% CI: 1.05–2.86). Patients who were treated with d4T had approximately 3-fold higher odds of developing MetS than those who were not treated with it (AOR, 3.08; 95% CI: 1.89–5.04). Moreover, patients who had a history of treatment with ZDV had 1.71 times higher odds of developing MetS than those without treatment with ZDV (AOR, 1.71; 95% CI, 1.02–2.88) (Table 3).
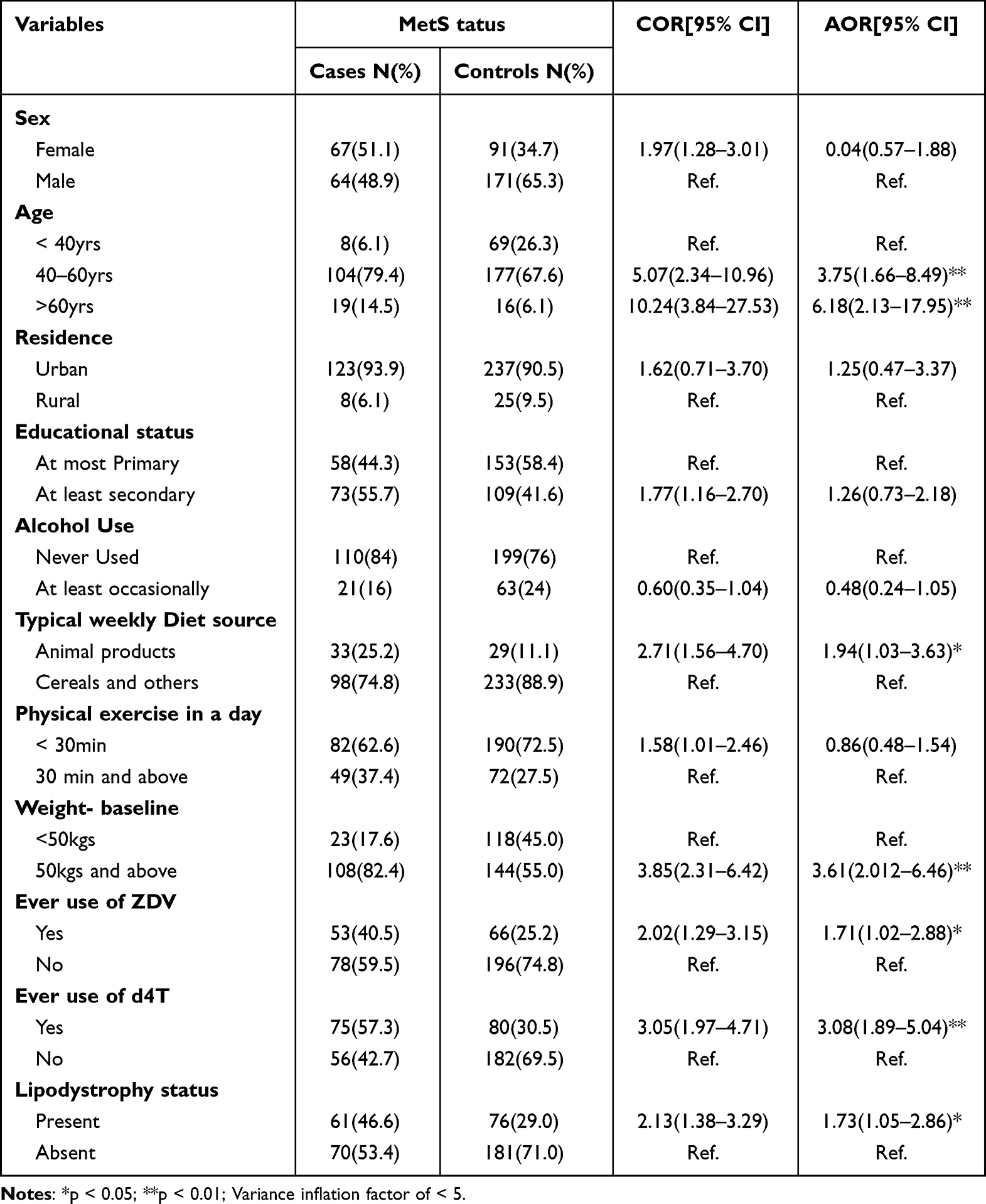 |
Table 3 Determinants of MetS Among the Study Participants, Adama Comprehensive Specialized Hospital, Oromia Region. Ethiopia, 2023 |
Discussion
In this study, we identified age, baseline weight, dietary source, lipodystrophy, and treatment, with an ART regimen containing stavidine and/or zidovudine as the independent determinants of MetS.
Odds for MetS increased as the age of patients increased from 40 years. This finding is consistent with those of studies done in Brazil,32 Burkina Faso,14 and Ethiopia.13 The consistent increase in MetS with increasing age may be due to the increased risk of developing each component of MetS, particularly hypertension, diabetes, and dyslipidemia, which are related to an increase in blood vessel (arterial) stiffness due to hypertension and physiological alterations in the metabolism of glucose and lipids.
Additionally, patients who had a baseline weight of 50kg or above had higher odds of developing MetS than those who had a baseline weight of <50 kg. This finding is concurrent with those of studies conducted in the southern United States33 and South Korea.34 This could be explained by the baseline risk of MetS that the patient might have due to higher baseline weight and the associated risk of obesity, which can later be exacerbated by weight gain after treatment with ART.
This study also showed that PLHA with a typical weekly diet from animal sources had higher odds of developing MetS than those with a diet from cereal or vegetable sources. This finding is in line with a study done in Italy35 and another study done in Uganda,36 and Zambia.37 This is also true in our setting, where consumption of a diet of animal sources such as meat, milk, and butter is considered a good practice to restore weight and health that was otherwise affected by HIV wasting syndrome in the majority of our patients. It is also common to see health-care givers encourage those diets that they believe help in weight gain as a presumed sign of success in HIV treatment and care.
Similarly, this study found that patients with lipodystrophy had higher odds of developing MetS than those without lipodystrophy. This finding is consistent with a report from studies done in Brazil38,39 and another study done in Spain,40 and Ethiopia23 which showed an increased risk of MetS or its component in PLHA with lipodystrophy. This consistent association between lipodysplasia and metabolic syndrome is likely due to physiological changes that are characterized by high insulin resistance, dyslipidemia, and central obesity, all of which are components of metabolic syndrome. However, our finding is contrary to that of another study by Brazil41 which showed no association between MetS and overall lipodystrophy, except for visceral fat accumulation. This difference could be due to differences in measurement in central obesity diagnosis, which was just waist circumference in our study as compared to imaging evidence of visceral fat accumulation in another study.
Furthermore, this study revealed that treatment with either a d4T or ZDV-containing ART regimen was independently associated with higher odds of MetS among patients who received the drugs than among those who had never taken those drugs. These findings are in line with those of a study done in Ghana,42 which showed a strong association between MetS and the ZDV-based regimen. Similarly, a study conducted in Denmark43 showed a significant association between the use of NRTIs such as ZDV and d4T. However, our findings are contrary to those of a study conducted in Nigeria44 that showed protease PIs, rather than NRTIs, as predictors of MetS. These findings are explained by the long-term use of older ART regimens known for their metabolic side effects, such as d4T and ZDV, owing to the lack of alternative replacements in our setup. However, the absence of association with PIs could be due to their preferential use in children and second-line regimens in our study setting, both of which were not included in the study population.
However, sociodemographic factors such as sex did not show any association with MetS in the current study, and this finding is consistent with that of another study in Ethiopia.45 However, these results are contrary to many studies42,46,47 which reported a strong association between female sex and MetS. This could be due to differences in the gender composition of the participants in these studies and differences in the study design, as these studies were cross-sectional.
Strength and Limitations
Some of the notable strengths of this study include use of primary data directly collected from the study participants, use of comprehensive criteria for diagnosis of MetS, and use of standard laboratory tests, among others. However, the fact that we included study participants (cases) consecutively and in one comprehensive specialized hospital can be considered as limitations of the study. Nonetheless, results of this study remain valuable as we were conscious of the potential risk of bias due to our sampling approach such as information contamination and necessary precautions were taken during data collection.
Conclusion
In conclusion, we found that increased age above 40 years, high baseline weight over 50kg, diets from animal sources, exposure to ZDV or d4T, and presence of lipodystrophy are independent determinants of MetS among patients receiving ART in the current study setting. Therefore, we recommend that caretakers should pay due attention to older patients, those with high baseline body weight, exposure to ZDV or d4T and to those with lipodystrophy to minimize the risk of CVDs. Furthermore, patient counseling and health education on dietary practice are essential.
Ethics Statement
This work was performed in accordance with the Declaration of Helsinki and has no conflicts of interest. Ethical approval was obtained from the ethics committee of Adama Hospital Medical College. The patients were informed about the purpose of the study, and verbal informed consent was obtained from each of them. The verbal informed consent process was acceptable and approved by the Ethics Committee of Adama Hospital Medical College.
Acknowledgment
We are thankful to our data collectors, laboratory technicians, and supervisors for their contribution to this work. Our sincere appreciation goes to our study participants for consenting and providing us with valuable information, without which this work would not have been realized. Finally, we would like to thank the Adama Comprehensive specialized hospital leaders, ART clinic staff for their unreserved cooperation, and the Adama Hospital Medical College ethical review board for the ethical clearance and approval of our protocol.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Alberti KG, Eckel RH, Grundy SM, et al. Harmonizing the metabolic syndrome: a joint interim statement of the international diabetes federation task force on epidemiology and prevention; national heart, lung, and blood institute; American Heart Association; world heart federation; international atherosclerosis society; and international association for the study of obesity. Obes Metabol. 2010;7:63–65.
2. Kassi E, Pervanidou P, Kaltsas G, et al. Metabolic syndrome: definitions and controversies. BMC Med. 2011;9(1):48. doi:10.1186/1741-7015-9-48
3. Onesi S, Ignatius U. Metabolic syndrome: performance of five different diagnostic criterias. Indian J Endocr Metab. 2014;18(4):496. doi:10.4103/2230-8210.137494
4. Grundy SM, Brewer HB, Cleeman JI, et al. Definition of metabolic syndrome: report of the national heart, lung, and blood institute/American Heart Association conference on scientific issues related to definition. Circulation. 2004;109(3):433–438. doi:10.1161/01.CIR.0000111245.75752.C6
5. Parikh R, Mohan V. Changing definitions of metabolic syndrome. Indian J Endocr Metab. 2012;16(7):7. doi:10.4103/2230-8210.91175
6. Alberti KGMM, Eckel RH, Grundy SM, et al. Harmonizing the metabolic syndrome: a joint interim statement of the international diabetes federation task force on epidemiology and prevention; national heart, lung, and blood institute; American heart association; world heart federation; international atherosclerosis society; and international association for the study of obesity. Circulation. 2009;120(16):1640–1645. doi:10.1161/CIRCULATIONAHA.109.192644
7. Gami AS, Witt BJ, Howard DE, et al. Metabolic syndrome and risk of incident cardiovascular events and death. J Am Coll Cardiol. 2007;49(4):403–414. doi:10.1016/j.jacc.2006.09.032
8. Dimitrov BD, Bahchevanov KM, Atanassova PA, et al. Metabolic syndrome severity score: range and associations with cardiovascular risk factors. Arch Med Sci Atheroscler Dis. 2016;1(1):90–97. doi:10.5114/amsad.2016.62137
9. Husain NE, Noor S, Elmadhoun W, et al. Diabetes, metabolic syndrome and dyslipidemia in people living with HIV in Africa: re-emerging challenges not to be forgotten. HIV. 2017;9:193–202. doi:10.2147/HIV.S137974
10. Samaras K, Wand H, Law M, et al. Prevalence of metabolic syndrome in HIV-infected patients receiving highly active antiretroviral therapy using international diabetes foundation and adult treatment panel III criteria. Diabetes Care. 2007;30(1):113–119. doi:10.2337/dc06-1075
11. Nguyen KA, Peer N, Mills EJ, et al. A meta-analysis of the metabolic syndrome prevalence in the global HIV-infected population. PLoS One. 2016;11(3):e0150970. doi:10.1371/journal.pone.0150970
12. Todowede OO, Mianda SZ, Sartorius B. Prevalence of metabolic syndrome among HIV-positive and HIV-negative populations in sub-saharan Africa—a systematic review and meta-analysis. Syst Rev. 2019;8(4). doi:10.1186/s13643-018-0927-y
13. Bune GT, Yalew AW, Kumie A. The extents of metabolic syndrome among antiretroviral therapy exposed and ART naïve adult HIV patients in the gedeo-zone, Southern-Ethiopia: a comparative cross-sectional study. Arch Public Health. 2020;78(1):40. doi:10.1186/s13690-020-00420-3
14. Guira O, Tiéno H, Diendéré AE, et al. Features of metabolic syndrome and its associated factors during highly active antiretroviral therapy in Ouagadougou (Burkina Faso). J Int Assoc Provid AIDS Care. 2016;15(2):159–163. doi:10.1177/2325957415601503
15. De Wit S, Sabin CA, Weber R, et al. Incidence and risk factors for new-onset diabetes in HIV-infected patients. Diabetes Care. 2008;31(6):1224–1229. doi:10.2337/dc07-2013
16. Mallya SD, Reddy T, Kamath A, et al. Determinants of metabolic syndrome and 5-year cardiovascular risk estimates among HIV-positive individuals from an Indian tertiary care hospital. AIDS Res Treat. 2020;2020:1–8. doi:10.1155/2020/5019025
17. Jaggers JR, Prasad VK, Dudgeon WD, et al. Associations between physical activity and sedentary time on components of metabolic syndrome among adults with HIV. AIDS Care. 2014;26(11):1387–1392. doi:10.1080/09540121.2014.920075
18. Paula AA, Falcão MC, Pacheco AG. Metabolic syndrome in HIV-infected individuals: underlying mechanisms and epidemiological aspects. AIDS Res Ther. 2013;10(1):32. doi:10.1186/1742-6405-10-32
19. De Luca A, de Gaetano Donati K, Colafigli M, et al. The association of high-sensitivity c-reactive protein and other biomarkers with cardiovascular disease in patients treated for HIV: a nested case–control study. BMC Infect Dis. 2013;13(1):414. doi:10.1186/1471-2334-13-414
20. Ataro Z, Ashenafi W. Metabolic syndrome and associated factors among adult HIV positive people on antiretro- viral therapy in jugal hospital, Harar, Eastern Ethiopia. East Afr J Health and Biomed Sci. 2020;4(1):13–24.
21. Tadesse WT, Adankie BT, Shibeshi W, et al. Prevalence and predictors of glucose metabolism disorders among people living with HIV on combination antiretroviral therapy. PLoS One. 2022;17(1):e0262604. doi:10.1371/journal.pone.0262604
22. Mashinya F, Alberts M, Van Geertruyden JP, et al. Assessment of cardiovascular risk factors in people with HIV infection treated with ART in rural South Africa: a cross sectional study. AIDS Res Ther. 2015;12(1):42. doi:10.1186/s12981-015-0083-6
23. Berhane T, Yami A, Alemseged F, et al. Prevalence of lipodystrophy and metabolic syndrome among HIV positive individuals on highly active anti-retroviral treatment in Jimma, South West Ethiopia. Pan Afr Med J. 2012;13(1).
24. Ford ES, Kohl HW, Mokdad AH, et al. Sedentary behavior, physical activity, and the metabolic syndrome among U.S. adults. Obesity Res. 2005;13(3):608–614. doi:10.1038/oby.2005.65
25. Haffner S, Taegtmeyer H. Epidemic Obesity and the Metabolic Syndrome. Circulation. 2003;108(13):1541–5. doi:10.1161/01.CIR.0000088845.17586.EC
26. Woldu M, Minzi O, Shibeshi W, et al. Biomarkers and prevalence of cardiometabolic syndrome among people living with HIV/AIDS, Addis Ababa, Ethiopia: a hospital-based study. Clin Med Insights Endocrinol Diabetes. 2022;15:117955142210780. doi:10.1177/11795514221078029
27. Mazzitelli M, Fusco P, Brogna M, et al. Weight of clinical and social determinants of metabolic syndrome in people living with HIV. Viruses. 2022;14(6):1339. doi:10.3390/v14061339
28. Tamhane AR, Westfall AO, Burkholder GA, et al. Prevalence odds ratio versus prevalence ratio: choice comes with consequences: prevalence odds ratio versus prevalence ratio. Statist Med. 2016;35(30):5730–5735. doi:10.1002/sim.7059
29. Ramli AS, Daher AM, Noor Khan Nor-Ashikin M, et al. JIS definition identified more Malaysian adults with metabolic syndrome compared to the NCEP-ATP III and IDF criteria. Biomed Res Int. 2013;2013:1–10. doi:10.1155/2013/760963
30. How to calculate sample size with epi info 7: cross-sectional studies | communitymedicine4all. Available from: https://communitymedicine4all.com/2018/06/23/how-to-calculate-sample-size-with-epi-info-7/.
31. Standard STEPS instrument. Available from: https://www.who.int/publications/m/item/standard-steps-instrument.
32. Gouveia ÉR, Gouveia BR, Marques A, et al. Predictors of metabolic syndrome in adults and older adults from Amazonas, Brazil. IJERPH. 2021;18(3):1303. doi:10.3390/ijerph18031303
33. Sears S, Buendia JR, Odem S, et al. Metabolic syndrome among people living with HIV receiving medical care in southern United States: prevalence and risk factors. AIDS Behav. 2019;23(11):2916–2925. doi:10.1007/s10461-019-02487-8
34. Chang -H-H. Weight gain and metabolic syndrome in human immunodeficiency virus patients. Infect Chemother. 2022;54(2):220. doi:10.3947/ic.2022.0061
35. Agodi A, Maugeri A, Kunzova S, et al. Association of dietary patterns with metabolic syndrome: results from the kardiovize brno 2030 study. Nutrients. 2018;10(7):898. doi:10.3390/nu10070898
36. Kiyimba T, Kigozi F, Yiga P, et al. The cardiometabolic profile and related dietary intake of Ugandans living with HIV and AIDS. Front Nutr. 2022;9:976744. doi:10.3389/fnut.2022.976744
37. Kalaluka PK Dietary patterns and the risk of metabolic syndrome among HIV positive individuals from selected health facilities in Lusaka District, Zambia; 2021.
38. Dos Santos TM, da Silva DB, Franco TM, et al. Lipodistrofia e a relação com fatores de risco cardiovascular e síndrome metabólica em pacientes infectados pelo vírus HIV. Nutricion Clinica y Dietetica Hospitalaria. 2017;37(2):12–20. doi:10.12873/372palmeira
39. Sacilotto LB, Pereira PCM, Manechini JPV, et al. Body composition and metabolic syndrome components on lipodystrophy different subtypes associated with HIV. J Nutr Metab. 2017;2017:1–8. doi:10.1155/2017/8260867
40. González-Domenech CM, Plaza-Andrades IJ, Garrido-Sanchez L, et al. Synergic effect of metabolic syndrome and lipodystrophy on oxidative stress and inflammation process in treated HIV-patients. Enfermedades Infecciosas y Microbiología Clínica. 2022;40(6):310–316. doi:10.1016/j.eimc.2020.11.019
41. Sacilotto LB, Papini SJ, Mendes AL, et al. Relationship between lipodystrophy, body composition, metabolic profile, and serum levels of adipocytokines. Front Nutr. 2021;8:750721. doi:10.3389/fnut.2021.750721
42. Dzudzor B, Essel S, Musah L, et al. Metabolic syndrome and combination antiretroviral therapy in HIV patients in periurban hospital in Ghana: a case-control study. AIDS Res Treat. 2023;2023:1–8. doi:10.1155/2023/1566001
43. Hansen B, Petersen J, Haugaard S, et al. The prevalence of metabolic syndrome in Danish patients with HIV infection: the effect of antiretroviral therapy. HIV Med. 2009;10(6):378–387. doi:10.1111/j.1468-1293.2009.00697.x
44. Iloeje U, Yuan Y, L’Italien G, et al. Protease inhibitor exposure and increased risk of cardiovascular disease in HIV-infected patients. HIV Med. 2005;6(1):37–44. doi:10.1111/j.1468-1293.2005.00265.x
45. Bune GT, Yalew AW, Kumie A. Predictors of metabolic syndrome among people living with HIV in Gedeo-Zone, Southern-Ethiopia: a case–control study. HIV. 2020;12:535–549. doi:10.2147/HIV.S275283
46. Kiama CN, Wamicwe JN, Oyugi EO, et al. Prevalence and factors associated with metabolic syndrome in an urban population of adults living with HIV in Nairobi, Kenya. Pan Afr Med J. 2018;29. doi:10.11604/pamj.2018.29.90.13328
47. Woldu M, Minzi O, Engidawork E. Prevalence of cardiometabolic syndrome in HIV-infected persons: a systematic review. J Diabetes Metab Disord. 2020;19(2):1671–1683. doi:10.1007/s40200-020-00552-x
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.