")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 15
Determinants of HIV/Aids Knowledge Among Females in Somalia: Findings from 2018 to 2019 SDHS Data
Authors Mohamud LA , Hassan AM , Nasir JA
Received 14 April 2023
Accepted for publication 13 July 2023
Published 24 July 2023 Volume 2023:15 Pages 435—444
DOI https://doi.org/10.2147/HIV.S414290
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Liban Ali Mohamud,1 Abdirashid Moallim Hassan,2 Jamal Abdul Nasir3
1Department of Statistics and Planning, SIMAD University, Mogadishu, Somalia; 2Department of Medicine and Surgery, SIMAD University, Mogadishu, Somalia; 3Department of Statistics, Government College University Lahore, Lahore, Pakistan
Correspondence: Liban Ali Mohamud, Email [email protected]
Background: Immunodeficiency syndrome (AIDS), which is caused by the human immunodeficiency virus (HIV), has become a serious global public health concern, particularly in underdeveloped countries. Even though the fact that just a few case studies have addressed on the HIV/AIDS in the context of Somalia, to the best of our knowledge, no national-scale study on the topic has been attempted. Limited knowledge of HIV/AIDS is highlighted as one of the major factors linked to the high prevalence of HIV among female population. This study aims to fill this knowledge gap in the literature by investigating the effects of several sociodemographic factors on females’ knowledge about HIV/AIDS in Somalia.
Methods: Secondary data from the Somalia Demographic Health Survey 2018– 19 were used in this study. A total of 16,335 women between the ages of 15 and 49 who fit our inclusion criteria have been chosen. The application of multiple logistic regressions was then performed to see if the predictors had a significant association with knowledge of HIV/AIDS.
Findings: Women aged 35– 39 (AOR = 1.608; 95% CI: 1.372– 1.886), women lived in urban (AOR: 2.833, 95% CI: 2.246– 3.572), Women’s education (AOR: 2.246, 95% CI: 1.988– 2.537), frequency of listening to a radio (AOR = 2.312; 95% CI: 1.995– 2.679), and frequency of watching television (AOR = 3.936; 95% CI: 3.445– 4.497) were significantly related with current knowledge about HIV/AIDS among eligible women in Somalia.
Conclusion: This study highlights the importance of mass media (TV and radio) interventions, education, and place of habitation as the main significant predictors of women’s knowledge of HIV/AIDS in Somalia. Based on the study, women are more likely to be aware of HIV/AIDS as their education level, frequency of listening a radio and watching a television watching rises. The research additionally indicates that women who reside in urban centers are nearly three times more likely than women who live in nomadic areas to know more about HIV/AIDS.
Keywords: knowledge of HIV/AIDS, public health, logistic regression, SDHS2018-19
Introduction
Acquired Immunodeficiency Syndrome (AIDS) caused by Human Immunodeficiency Virus (HIV) has emerged as a serious public health problem across the globe, and particularly in developing countries. The latest 2022 UNAIDS global statistics reported that 38.4 million people are living with HIV infection worldwide, comprising 36.7 million adults (15+ years) and 1.7 million children (<15 years).1 Amongst these, 1.5 million people are newly infected. Overall, the number of HIV-infected adult women (15+ years) is higher with 19.7 million, which represents 54% of the total people living with HIV-infection.1 Since the beginning of the epidemic, 84.2 million people have acquired HIV infection and more than 40.1 million HIV/AIDS-related deaths are reported.2 In 2022, the World Health Organization estimated that roughly 28.7 million people had received antiretroviral therapy.2
The African continent is home to more than two-third (25.6 million) of the HIV-infected population.1 Majority of the people with HIV/AIDS are living in low- and middle-income countries. In 2021, there were 20.6 million (53%) people with HIV living in eastern and southern Africa, while 5 million (13%) reside in western and central Africa.2 Additionally, sub-Saharan Africa (SSA) remains the most dramatically affected region with about 67% of the global burden of HIV and more than half of the people living with HIV in this region being women.3
Somalia has some of the world’s lowest-ranked health indicators.4 More than three decades of civil war and instability has weakened Somalia’s health system and caused more than 2.5 million people to be displaced within the country.5,6 The protracted conflicts, droughts, flooding, locust plagues in the country have caused sustained food crises, poverty, and poor infrastructure.7 Furthermore, even though sub-Saharan Africa accounts for more than half of all maternal deaths worldwide, Somalia tops the list for both maternal and infant mortality.8
Data from UNAIDS 2021 reveal that 7700 adults and children in Somalia are HIV-positive, with more than 45% of these people being women over the age of 15.9 The total number of adult and child deaths related to HIV/AIDS was less than 500 people.9 The country-wide survey conducted in 2018 also showed that average antenatal HIV prevalence was 0.1%. The World Bank estimated that 0.1% of Somali population had HIV/AIDS in 2021.10 Just 62% of women with HIV in 2020 were aware that they had the virus.11
Most of the reproductive-age women living in developing countries including Somalia have poor comprehensive knowledge on HIV/AIDS.12 Exposure to mass media (television, radio, and newspapers) is an important source for spreading HIV knowledge throughout the community as well as an effective method for promoting awareness and education about HIV/AIDS.13
Knowledge about HIV AIDS and its transmission has been reported to be significantly insufficient in the Somali population, but no generalized studies have ever been done in the urban and rural populations.14 The understanding of HIV/AIDS was found to be low among semi-nomadic and local agro-pastoralists in northern Somalia in 2013.15
Similarly, there are no generalized studies conducted to determine the magnitude and determinants of knowledge of HIV/AIDS among reproductive-age women in Somalia. Therefore, this study aimed to investigate the knowledge of HIV/AIDS among reproductive-age women in Somalia using Somali Health Demographic Surveys 2018-2019.
Methods and Data
For this study, secondary data obtained from the Somali Demographic and Health Survey (SDHS) 2018–2019,16 which was conducted by the Ministry of Health (MOH) of the Federal Government of Somali (FGS) and the Somali National Bureau of Statistics (NBS) were used. The SDHS utilized cluster sampling with a multi-stage stratified probability approach. In urban and rural areas, a three-stage stratified cluster sample design was employed, whereas a two-stage design was employed in nomadic areas. A total of 55 sampling strata were created, with each region being divided into urban, rural, and nomadic sectors, with the exception of Banadir, which is entirely urban. Three strata from Lower Shabelle, three strata from Middle Juba regions, and two strata were completely excluded from the survey due to security concerns, resulting in the development of 47 sampling strata.
The study’s target population comprised all women aged 15 to 49, and a total of 17,826 women were selected for the sample, with a response rate of 92.5% among the women who were interviewed. Among those, 16,486 qualified women were successfully interviewed, including 11,876 eligible women who had ever been married and 4610 who had never been married.
All women aged 15 to 49 at the time of the survey met the inclusion criteria, resulting in a sample of 16,486 individuals. Unfortunately, the reporting of data from 151 respondents in the survey had several missing observations. After cleaning the data, the study’s final sample comprised 16,335 individuals, including 7816 women from urban areas, 4204 from rural areas, and 4315 from nomadic areas. For more information on the sample design, refer to the SDHS report (2020).16
Outcome Variable: In this study, the outcome variable is HIV/AIDS Knowledge. In SDHS ever married women questionnaire, the primary question posed to the female respondents was “Have you ever heard of HIV or AIDS?”, with the response options categorized as “Yes” for those who have heard of HIV/AIDS and “No” for those who have not.17,18
Predictor variables: To accomplish the study’s objectives, we selected seven variables that we considered might have an effect on HIV/AIDS knowledge. These variables were divided into three groups, including four individual-level factors: a woman’s age, education level, exposure to news (radio and television), a household-level factor (wealth), and two community-level factors (place of residence and region). The individual-level factors were included as they are typically associated with health knowledge and behavior, while the community-level factors were selected to explore the potential impact of the social and cultural context on HIV/AIDS knowledge. The wealth index was also considered, as it can provide insight into the potential influence of economic status on HIV/AIDS knowledge.17–19
The study utilized the frequentist Pearson Chi-square test, to evaluate the significance of bivariate variables. Furthermore, logistic regression model was utilized to assess the association between various independent variables and women’s knowledge of HIV/AIDS.20
Results
Table 1 illustrates the univariate analysis results, depicting the demographic and socio-economic characteristics of the study respondents. Notably, the data reveals that a substantial proportion of women (67.6%) possessed knowledge about HIV/AIDS. Further analysis indicates that the highest percentage of women (26.97%) belonged to the age group of 15–19, while the largest proportion of respondents (13.67%) was from the Banadir region. In terms of residency, more than one-third of participants (47.85%) lived in urban areas, and the majority (74.44%) had not received any formal education. Additionally, the study found that a significant proportion of women did not engage with electronic media, with 88.6% of respondents reporting that they did not listen to the radio, and 83.9% not watching television.
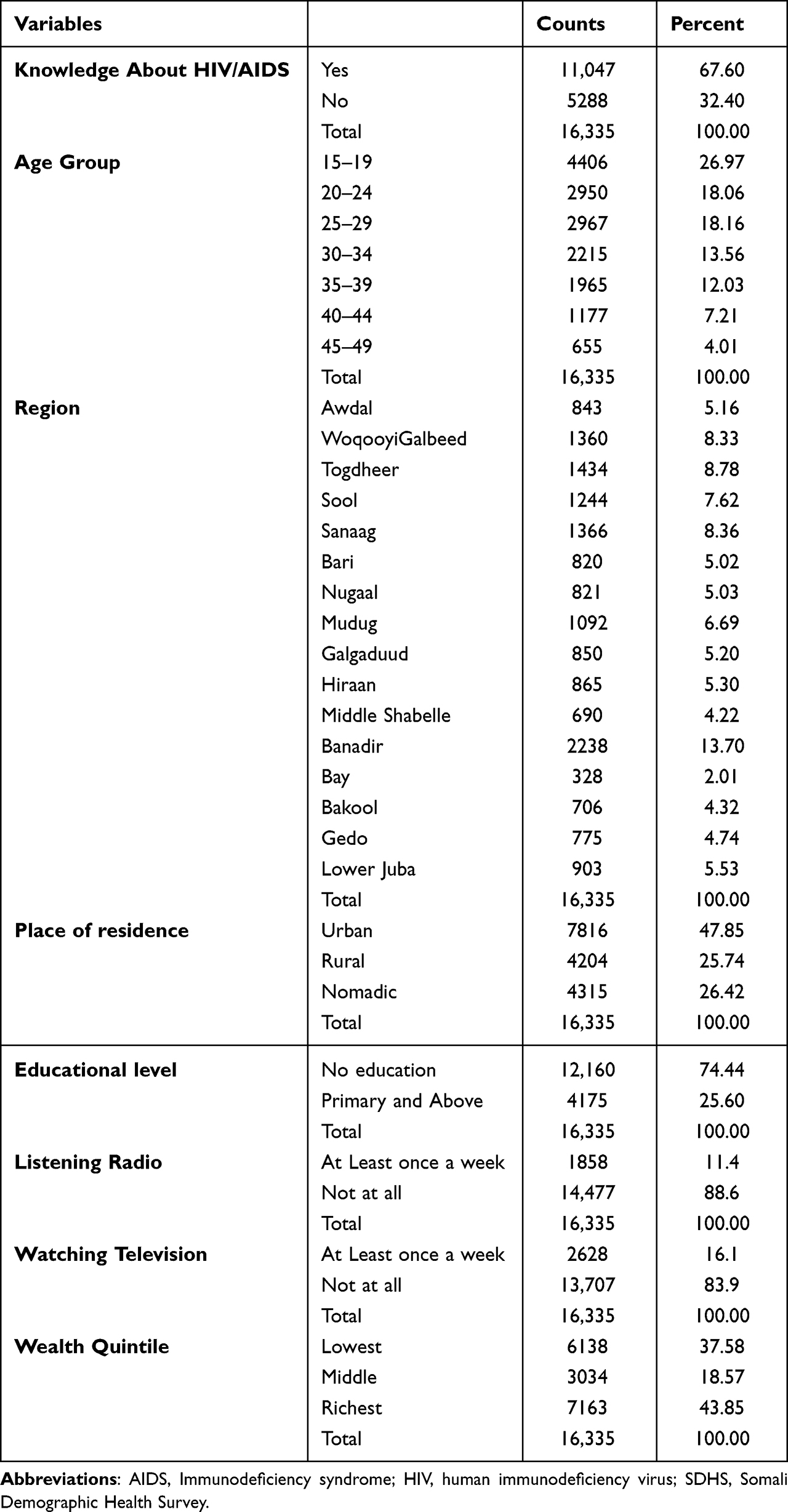 |
Table 1 Univariate Analysis of Sociodemographic Profile of the Females Responses in Somalia, SDHS 2018–19 (n = 16,335) |
In Bivariate analysis, we adopted the chi-square test of association between the outcome variable (knowledge about HIV/AIDS) and the potential factors affecting knowledge about HIV/AIDS. The results are presented in Table 2, showed significant associations for all variables: age group (χ2= 45.084, df = 6, n = 16,335, p-value = 0.000), region (χ2= 1405.457, df = 15, n = 16,335, p-value = 0.000), residence (χ2= 1714.900, df = 2, n = 16,335, p-value = 0.000), education level (χ2= 977.511, df = 1, n = 16,335, p-value = 0.000), listening to the radio (χ2= 368.497, df = 1, n = 16,335, p-value = 0.000), and watching television (χ2= 681.846, df = 1, n = 16,335, p-value = 0.000). Hence, the results suggest that all of these variables are significant predictors of HIV/AIDS knowledge among Somali women of childbearing age.
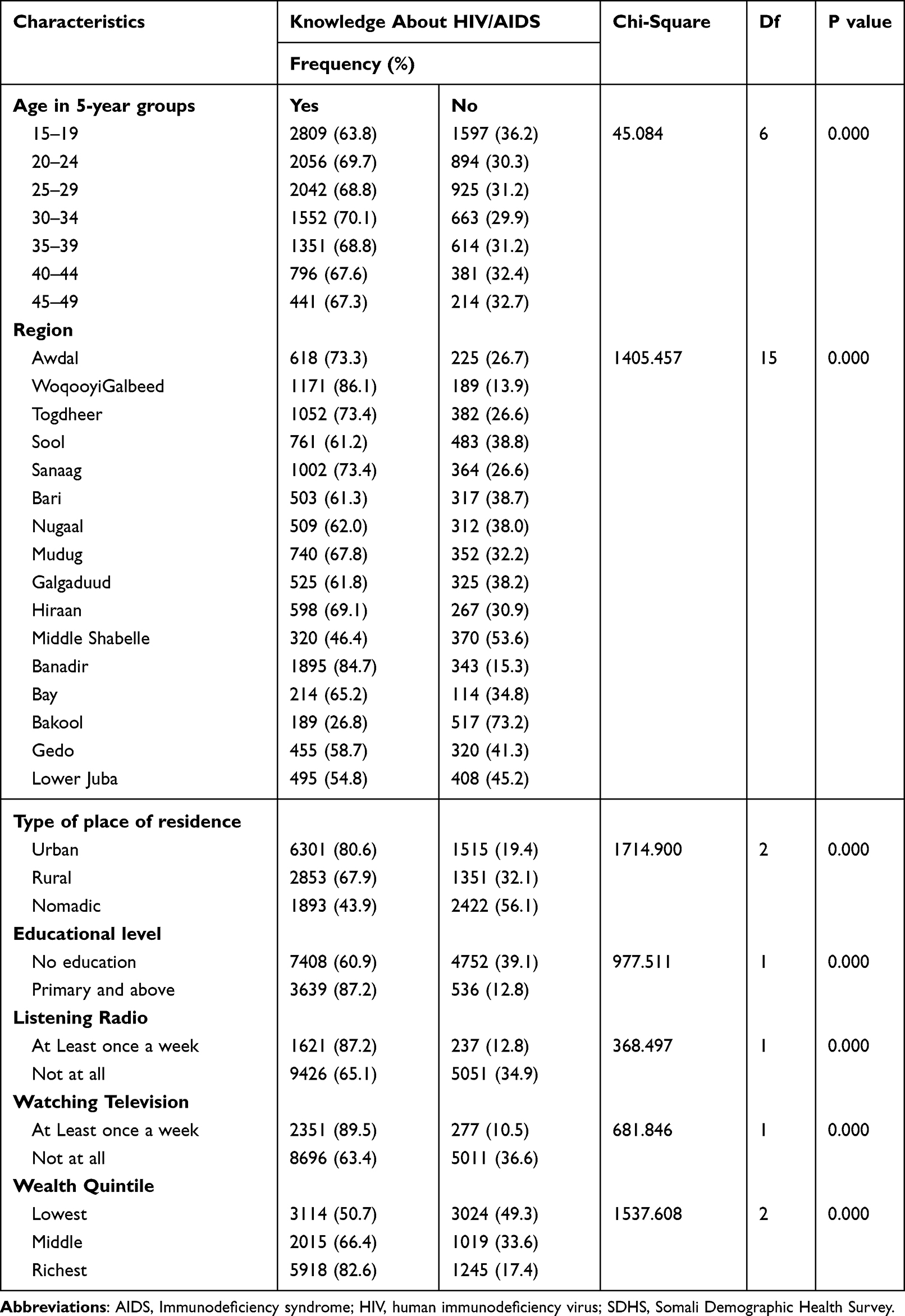 |
Table 2 Bivariate Analysis of Females Responses on HIV/AIDS Knowledge in Somalia, SDHS 2018–19 (n = 16,335) |
The multivariate binary logistic regression was used to assess the relationship between the outcome variable (knowledge about HIV/AIDS) and predictor variables (age, region, type of residence, education, wealth index, and media factors (radio/Television)). Table 3 presents the results, which show that all predictor variables are significantly associated with the outcome variable. Holding other factors constant, women aged 20–24 years (AOR = 1.302; 95% CI = 1.137–1.491), 25–29 years (AOR = 1.407; 95% CI = 1.218–1.625), and 45–49 years (AOR = 1.315; 95% CI = 1.057–1.636) were more likely to have knowledge about HIV/AIDS than those aged 15–19 years. Similarly, women aged 30–34 years (AOR = 1.494; 95% CI = 1.280–1.744), 35–39 years (AOR = 1.608; 95% CI = 1.372–1.886), and 40–44 years (AOR = 1.556; 95% CI = 1.299–1.863) were almost two times more likely to have knowledge about HIV/AIDS than those aged 15–19 years.
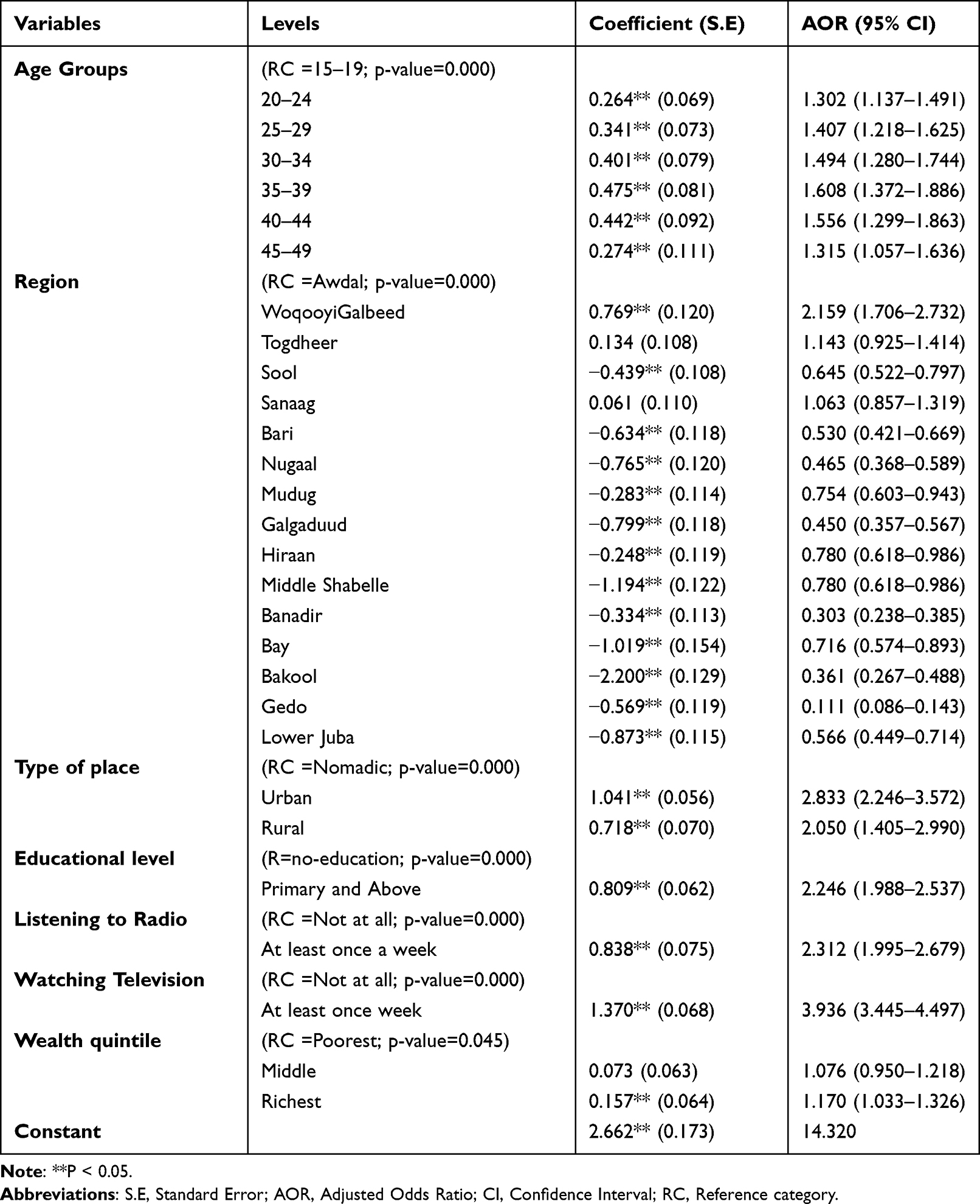 |
Table 3 Multivariate Logistic Regression Estimates of the Factors Associated with HIV/AIDS Knowledge by Females of Somalia, SDHS 2018–19 (n = 16,335) |
Respondents from Woqooyi Galbeed Region had almost two times higher odds of having knowledge about HIV/AIDS than those from Awdal region (AOR = 2.159; 95% CI = 1.706–2.732), holding other factors constant. Similarly, respondents from Togdheer Region (AOR = 1.143; 95% CI = 0.925–1.414) and Sanaag Region (AOR = 1.063; 95% CI = 0.857–1.319) had higher odds of having knowledge about HIV/AIDS than those from Awdal Region, but the difference was not statistically significant. Conversely, respondents from Sool Region (AOR = 0.645, 95% CI = 0.522–0.797), Bari Region (AOR = 0.530, 95% CI = 0.421–0.669), Nugaal Region (AOR = 0.465, 95% CI = 0.368–0.589), Mudug Region (AOR = 0.754, 95% CI = 0.603–0.943), Galgaduud Region (AOR = 0.450, 95% CI = 0.357–0.567), Hiraan and Middle Shabelle Regions (AOR = 0.780, 95% CI = 0.618–0.986), Banadir Region (AOR = 0.303, 95% CI = 0.238–0.385), Bay Region (AOR = 0.716, 95% CI = 0.574–0.893), Bakool Region (AOR = 0.361, 95% CI = 0.267–0.488), Gedo Region (AOR = 0.111, 95% CI = 0.086–0.143), and Lower Juba Gedo Region (AOR = 0.566, 95% CI = 0.449–0.714) had lower odds of having knowledge about HIV/AIDS than those from Awdal Region, holding other factors constant.
Respondents living in urban (AOR = 2.833, 95% CI = 2.246–3.572) and rural areas (AOR = 2.050, 95% CI = 1.405–2.990) had a higher likelihood of having knowledge about HIV/AIDS compared to those residing in nomadic areas. Women with primary and higher levels of education (AOR = 2.246, 95% CI = 1.988–2.537) were twice as likely to have more knowledge about HIV/AIDS than those with no education. Those who watched television at least once a week (AOR = 3.936; 95% CI = 3.445–4.497) had four times higher odds of having more knowledge about HIV/AIDS than those who never watched television. Similarly, those who listened to the radio at least once a week (AOR = 2.312; 95% CI = 1.995–2.679) had almost two times higher odds of having more knowledge about HIV/AIDS than those who never listened to the radio. Lastly, women categorized as the richest by the wealth index had 1.2 times higher odds of having knowledge about HIV/AIDS than those categorized as poorest in wealth quintiles (AOR = 1.170; 95% CI = 1.033–1.326).
Discussions
In this study, the knowledge of Somalia women towards HIV/AIDS and its associated risk factors were assessed. A nationally representative data from the Somali Demographic and Health Survey (SDHS) conducted in 2018–2019 were analyzed to understand the level of knowledge and awareness about HIV/AIDS in Somalia and assess its association with sociodemographic risk factors.
The results highlighted that 67.6% of Somali women have knowledge about HIV/AIDS. Furthermore, the data revealed that age group, region, residence, educational level, listening radio, and watching television were significantly associated with knowledge about HIV/AIDS among Somali women in childbearing age. It was also found that been in the 15–19 years age group, being nomadic and residing in the rural areas, illiteracy, and lack of access to media (radio and television) were significantly associated with greater likelihood of having lower level of knowledge about HIV/AIDS.
Generally, the study found that almost two-third of the respondents have knowledge regarding HIV/AIDS. This finding is in similar with the other studies done in sub-Saharan Africa that observed trends of HIV-related knowledge within SSA region.21,22 However, the findings from this study are lower than those from a similar study conducted in 13 SSA countries, in which national DHS data of each country was analyzed. The overall HIV knowledge in that study was more than 90% among female respondents.23 Nonetheless, the findings of this study are in line with those of earlier investigations carried out in Southern India,24 Karachi25 (Pakistan), and throughout Pakistan26 where the majority of female respondents had a higher understanding of HIV/AIDS. Despite the protracted conflict leading to destruction of the major healthcare delivery systems and livelihood, the prevalence of HIV and AIDS has been on a steady decline (from higher than 1% in 2013 to 0.10% in 2022) courtesy of a collaborative effort between the WHO and federal states of Somalia.27
In this study, it was also observed that older women were more likely to have knowledge than younger women. This is in line with research from, among other places, Uganda,12 Nigeria,28 and India.29 This might be that older women are matured, understand their susceptibility to disorders, and may search information regarding their wellbeing.30 In contrast, other study conducted in Bangladesh reported that younger women were found to have more knowledge of HIV than older ones belonging to age group 45 or above.31,32
Education level and women’s awareness of HIV were highly associated. Women with primary and higher level in education were two times more likely to have more knowledge about HIV/AIDS than those women with no education. This result agrees with another study from Indonesia33 and other countries, including Tanzania,34 Bangladesh35 and Ethiopia,36 which discovered that women with primary or higher levels of education are more likely to be aware of HIV/AIDS. Educated women may get HIV-related information in their school curricula and might have decision-making power which helps them to decide on their health-related aspects of life.37
The study findings also revealed that majority of women living in urban areas are having more knowledge on HIV/AIDS when compared to their counterparts living in rural and nomadic areas. These results are in agreement with research conducted in different African countries.38,39 Another nationwide study conducted in Rwanda reported that women living in rural areas were less likely to have sufficient knowledge on HIV compared to those in urban areas.40 These observed disparities may be due to differences in access to HIV-related information. Urban women are better exposed to HIV/AIDS information than rural and nomadic people who invariably have limited access to media and other resources. Additionally, wealth was significantly associated with HIV knowledge. Women categorized as the richest by the wealth index were more likely to have knowledge about HIV/AIDS than those categorized as poorest in wealth quintiles. This corroborated the results reported in previous studies in sub-Saharan Africa,41 Ethiopia,42 and Vietnam.43 The plausible reason could be women from higher-wealth quintiles have access to education, media and health information. Limited economic opportunity and poverty have also been shown to contribute to HIV/AIDS as it leads to food insufficiency and homelessness that can drive risky sexual practices including transactional sex.44
Finally, there was significant association between knowledge of HIV/AIDS and exposure to all types of the investigated mass media (Radio and Television). Women who were watching television at least once a week were four times more likely to have more knowledge about HIV/AIDS than those who never watched television. Similarly, the women who listening radio broadcast at least once a week were almost two times more likely to have more Knowledge about HIV/AIDS than those who never listened to the radio. Earlier publications reported similar findings about the influence of mass media on HIV/AIDS knowledge of women in Ethiopia,45 Malawi,46 and Bangladesh35. The possible reason may be the health education campaigns on HIV knowledge and awareness are carried out through media channels especially radio which has become a very functional medium in delivering accurate health-related information.47
Study Limitation
The study has several limitations. At first, the knowledge of HIV/AIDS was measured with one question only. Given that no study has examined knowledge of HIV among females using national SDHS. Second, the study findings cannot be generalized to the whole Somali population as the study was conducted in sixteen states of the country. However, the two states were not included in this study (Lower Shabelle and Middle Juba). Since HIV is a sensitive topic, the possibility of respondents modifying their responses could not be ruled out. Hawthorne effect, modification of behavior by study participants in response to their knowledge of being observed, has a role to play in HIV-related studies.
Despite these several limitations, this is the first study investigating knowledge of HIV among females in Somalia using national SDHS data with a large sample size.
Conclusion
The purpose of this study is to investigate the effect of predictor variables such as age group, region, and type of residence, education, wealth index, and media factors (radio/television) on women’s knowledge of HIV/AID. Strong impact of place of living, education, mass-media accessibility, age group on respondent’s HIV knowledge was identified. The study highlights the importance of exposure to mass media (TV and radio), education, and location of residence as the main potential determinants of knowledge of HIV/AIDS in Somalia. The research further demonstrates that, compared to teenage (15–19 years old), uneducated women living in nomadic areas who are not watching television or listening to the radio at least once a week, the women in the age groups of 35–39 and 40–44 who are educated (primary and above), living in urban areas, and who watch television and listen to the radio at least once a week were more likely to know about HIV/AIDS. Health managers, policymakers, and intended stakeholders working in this area should consider these aspects into account when implementing health intervention programs to increase HIV knowledge among Somali women. Based on its findings, the study advises the Federal Government of Somalia and other stakeholders to launch a knowledge campaign for HIV/AIDS that focuses on young women (15–19 years old), illiterate women living in nomadic regions, and non-socially active women who are uninformed of the disease. Furthermore, incorporating HIV/AIDS-related knowledge into national school curricula, raising knowledge campaigns in public places such as schools and mosques, and utilizing the popularity of mass media (radio, television, and newspaper) to raise knowledge through specially designed programs suitable for both urban and rural people are all strongly recommended to tackle this tremendous pandemic.
Ethics Considerations
The study obtained ethical clearance from both the Somali National Bureau of Statistics (SNBS) (Ref: HIQS/332/2023) and the SIMAD Institutional Review Board (SU-IRB) of human research ethics review committee (Ref: 2023/SU-IRB/FMHS/P004) at SIMAD UNIVERSITY. The study adhered to the standards and regulations of the Declaration of Helsinki.
Acknowledgments
The authors express their gratitude to the Somali National Bureau of Statistics for providing them with access to the SDHS 2018–19 dataset, which was used in this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. UNAIDS. Factsheet. 2022.
2. World Health Organization. Global HIV programme. Key facts HIV. In: HIV Data and Statistics. World Health Organization; 2022.
3. Olopha PO, Fasoranbaku AO, Gayawan E. Spatial pattern and determinants of sufficient knowledge of mother to child transmission of HIV and its prevention among Nigerian women. PLoS One. 2021;16:1–15. doi:10.1371/journal.pone.0253705
4. Organização Mundial de Saúde. World Health Statistics 2022 (Monitoring Health of the SDGs). Organização Mundial de Saúde; 2022.
5. Morrison J, Malik S. M. M. R. Population health trends and disease profle in Somalia 1990–2019, and projection to 2030: will the country achieve sustainable development goals 2 and 3?. 2023; 23(1):1–9. doi:10.1186/s12889-022-14960-6
6. UNFPA. So Many Mouths to Feed: Addressing High Fertility in Famine-Stricken Somalia, April 2012. Available from: https://www.unfpa.org/news/so-many-mouths-feed-addressing-high-fertility-famine-stricken-somalia.
7. Bile K, Warsame M, Ahmed AD. Fragile states need essential national health research: the case of Somalia. Lancet Glob Heal. 2022;10(5):e617–e618. doi:10.1016/S2214-109X(22)00122-X
8. Aden JA, Ahmed HJ, Östergren PO. Causes and contributing factors of maternal mortality in Bosaso District of Somalia. A retrospective study of 30 cases using a Verbal Autopsy approach. Glob Health Action. 2019;12(1):1672314. doi:10.1080/16549716.2019.1672314
9. UNAIDS and AIDSinfo. Estimates Adults and Children Living with Country Factsheets DRC | 2020 HIV Testing and Treatment Cascade People Living with HIV Coverage of Adults and Children. UNAIDS. 2021:1–6.
10. Somalia - Prevalence Of HIV, Total (% Of Population Ages 15–49) - 2023 Data 2024 Forecast 1990–2021 Historical. 2023.
11. UNAIDS. Program HIV/AIDS. UNAIDS; 2020:1–436.
12. Ankunda D, Asiimwe JB. Determinants of comprehensive knowledge of HIV/AIDS among women of the reproductive age (15–49) in Uganda. Int J Community Med Public Heal. 2017;4(10):3530. doi:10.18203/2394-6040.ijcmph20174215
13. Brown JD, Einsiedel EF. Public health campaigns: mass media strategies. 1990.
14. IngvilKrarupSorbye. Ê- /1 / “Ê 9- -Ê” Ê, *”, 1 / 6 / Ê. A Situat Anal Reprod Heal Somalia. 2009;2009:237–256.
15. Abdi IA, Ereg D, Ali M, Rahlenbeck SI. Knowledge and attitudes about AIDS/HIV in a semi-nomadic population in Somaliland. J Community Health. 2013;38(2):246–249. doi:10.1007/s10900-012-9606-4
16. Somalia | ReliefWeb. The Somali health and demographic survey. 2020.
17. Nasir JA, Khan MD, Ahmed Zaidi SA. Factor associated with HIV/AIDS knowledge among males: findings from 2017–18 Pakistan Demographic and Health Survey. J Biosoc Sci. 2023;1999:1–9. doi:10.1017/s0021932022000542
18. Srivastava S, Chauhan S, Patel R, Kumar P. A study of awareness on HIV/AIDS among adolescents: a longitudinal study on UDAYA data. Sci Rep. 2021;11(1):1–8. doi:10.1038/s41598-021-02090-9
19. Nasir JA, Imran M, Zaidi SAA. HIV/AIDS awareness in Pakistan. Prof Med J. 2015;22(05):603–609. doi:10.29309/tpmj/2015.22.05.1274
20. Buckalew LW, Pearson WH. Critical factors in the chi-square test of Independence: a technique for exploratory data analysis. Bull Psychon Soc. 1982;19(4):225–226. doi:10.3758/BF03330240
21. Dai X, Wang H. Change in knowledge and attitude about HIV/AIDS in sub-Saharan Africa, 1990–2017: an analysis of national survey data. Lancet Global Health. 2019;7:S4. doi:10.1016/S2214-109X(19)30089-0
22. De Coninck Z, Feyissa IA, Ekström AM, Marrone G. Improved HIV awareness and perceived empowerment to negotiate safe sex among married women in Ethiopia between 2005 and 2011. PLoS One. 2014;9(12):e115453. doi:10.1371/JOURNAL.PONE.0115453
23. Jung M, Arya M, Viswanath K. Effect of media use on HIV/AIDS-related knowledge and condom use in Sub-Saharan Africa: a cross-sectional study. PLoS One. 2013;8(7):e68359. doi:10.1371/JOURNAL.PONE.0068359
24. Bhagavathula AS, Bandari DK, Elnour AA, et al. Across sectional study: the knowledge, attitude, perception, misconception and views (KAPMV) of adult family members of people living with human immune virus-HIV acquired immune deficiency syndrome-AIDS (PLWHA). Springerplus. 2015;4(1):1–12. doi:10.1186/S40064-015-1541-2
25. Farid-ul-Hasnain S, Johansson E, Krantz G. What do young adults know about the HIV/AIDS epidemic? Findings from a population based study in Karachi, Pakistan. BMC Infect Dis. 2009;9(1):1–11. doi:10.1186/1471-2334-9-38/TABLES/5
26. Article O, Khan R, Bilal A, Siddiqui SH. Knowledge about HIV and discriminatory attitudes toward people living with HIV in Pakistan. Pakistan J Public Heal. 2019;9(1):37–41. doi:10.32413/PJPH.V9I1.237
27. WHO EMRO. WHO Somalia Calls for Breaking the Barriers to Ensure Equal Access to HIV Services | News | Somalia Site. WHO; 2023.
28. Oginni AB, Adebajo SB, Ahonsi BA. Trends and determinants of comprehensive knowledge of HIV among adolescents and young adults in Nigeria: 2003–2013. Afr J Reprod Health. 2017;21(2):26–34. doi:10.29063/AJRH2017/V21I2.4
29. Yadav J, Gautam S, Singh KJ. (PDF) Differential in awareness and comprehensive knowledge of HIV/AIDS and its determinants among youth in India: a population based cross-sectional study. Am Int J Res Humanit Arts Soc Sci. 2015;13(3):222–230.
30. Nketiah-Amponsah E, Codjoe EA, Ampaw S. HIV/AIDS awareness and knowledge among Ghanaian women of reproductive age: what are the correlates? J Asian Afr Stud. 2019;54(2):267–281. doi:10.1177/0021909618810037
31. Mondal MNI, Rahman MM, Rahman MO, Akter MN. Level of awareness about HIV/AIDS among ever married women in Bangladesh. Food Public Heal. 2012;2(3):73–78. doi:10.5923/J.FPH.20120203.03
32. Yaya S, Bishwajit G, Danhoundo G, et al. Trends and determinants of HIV/AIDS knowledge among women in Bangladesh. BMC Public Health. 2016;16(1):1–9. doi:10.1186/S12889-016-3512-0/TABLES/4
33. Najmah SIP, Kumalasari TN, Davies SG, Andajani S. Factors influencing HIV knowledge among women of childbearing age in South Sumatra, Indonesia. Malaysian J Public Heal Med. 2020;20(1):150–159. doi:10.37268/MJPHM/VOL.20/NO.1/ART.552
34. Haile ZT, Teweldeberhan AK, Chertok IRA. Correlates of women’s knowledge of mother-to-child transmission of HIV and its prevention in Tanzania: a population-based study. AIDS Care. 2016;28(1):70–78. doi:10.1080/09540121.2015.1062465
35. Rahman MS, Rahman ML. Media and education play a tremendous role in mounting AIDS awareness among married couples in Bangladesh. AIDS Res Ther. 2007;4(1):1–7. doi:10.1186/1742-6405-4-10/FIGURES/1
36. Luba TR, Feng Z, Gebremedhin SA, et al. Knowledge about mother–to–child transmission of HIV, its prevention and associated factors among Ethiopian women. J Glob Health. 2017;7(2). doi:10.7189/JOGH.07.020414
37. Tsegaw M, Mulat B, Shitu K. Determinants of Comprehensive HIV knowledge among reproductive-age women in Gambia: further analysis of recent Gambia demographic and health survey. 2022. doi:10.21203/rs.3.rs-1560307/v1.
38. Corno L, De Walque D. Socioeconomic determinants of stigmatization and HIV testing in Lesotho. AIDS Care. 2013;25(Suppl 1):S108–S113. doi:10.1080/09540121.2012.736937
39. Stephenson R. A community perspective on young people’s knowledge of HIV/AIDS in three African countries. AIDS Care. 2009;21(3):378–383. doi:10.1080/09540120802241889
40. Deynu M, Nutor JJ. Determinants of comprehensive knowledge on mother-to-child transmission of HIV and its prevention among childbearing women in Rwanda: insights from the 2020 Rwanda Demographic and Health Survey. BMC Public Health. 2023;23(1):1–14. doi:10.1186/S12889-022-14925-9/TABLES/3
41. Teshale AB, Yeshaw Y, Alem AZ, et al. Comprehensive knowledge about HIV/AIDS and associated factors among women of reproductive age in sub-Saharan Africa: a multilevel analysis using the most recent demographic and health survey of each country. BMC Infect Dis. 2022;22(1):1–10. doi:10.1186/S12879-022-07124-9/TABLES/5
42. Agegnehu CD, Geremew BM, Sisay MM, et al. Determinants of comprehensive knowledge of HIV/AIDS among reproductive age (15–49 years) women in Ethiopia: further analysis of 2016 Ethiopian demographic and health survey. AIDS Res Ther. 2020;17(1). doi:10.1186/S12981-020-00305-Z
43. Hoang CD, Tran BX, Pham MD, et al. HIV- and AIDS-related knowledge and attitude of residents in border regions of Vietnam. Harm Reduct J. 2019;16(1). doi:10.1186/S12954-019-0282-X
44. Riley ED, Gandhi M, Hare CB, Cohen J, Hwang SW. Poverty, unstable housing, and HIV infection among women living in the United States. Curr HIV/AIDS Rep. 2007;4(4):181–186. doi:10.1007/S11904-007-0026-5
45. Kefale B, Damtie Y, Yalew M, Adane B, Arefaynie M. Predictors of comprehensive knowledge of HIV/AIDS among people aged 15–49 years in Ethiopia: a multilevel analysis. HIV/AIDS - Res Palliat Care. 2020;12:449–456. doi:10.2147/HIV.S266539
46. Mandiwa C, Namondwe B, Munthali M. Prevalence and correlates of comprehensive HIV/AIDS knowledge among adolescent girls and young women aged 15–24 years in Malawi: evidence from the 2015–16 Malawi demographic and health survey. BMC Public Health. 2021;21(1):1–9. doi:10.1186/S12889-021-11564-4/TABLES/3
47. Agegnehu CD, Tesema GA. Effect of mass media on comprehensive knowledge of HIV/AIDS and its spatial distribution among reproductive-age women in Ethiopia: a spatial and multilevel analysis. BMC Public Health. 2020;20(1):1–12. doi:10.1186/S12889-020-09536-1/TABLES/4
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.