")
Back to Journals » Risk Management and Healthcare Policy » Volume 16
Determinants of and Willingness to Use and Pay for Digital Health Technologies Among the Urban Elderly in Hangzhou, China
Received 22 October 2022
Accepted for publication 14 March 2023
Published 27 March 2023 Volume 2023:16 Pages 463—478
DOI https://doi.org/10.2147/RMHP.S393767
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Keng Yang,1,2 Yang Li,3 Hanying Qi4,5
1Institute of Economics, Tsinghua University, Beijing, People’s Republic of China; 2One Belt-One Road Strategy Institute, Tsinghua University, Beijing, People’s Republic of China; 3Wuyi University, Jiangmen, People’s Republic of China; 4The New Type Key Think Tank of Zhejiang Province “China Research Institute of Regulation and Public Policy”, Zhejiang University of Finance and Economics, Hangzhou, People’s Republic of China; 5China Institute of Regulation Research, Zhejiang University of Finance and Economics, Hangzhou, People’s Republic of China
Correspondence: Hanying Qi, Zhejiang University of Finance and Economics, Hangzhou, 310018, People’s Republic of China, Tel +86 151 5802 5275, Email [email protected]
Purpose: In recent years, little research has been conducted on the willingness to use and pay for digital health technologies for elderly people. Thus, this study investigates the willingness to use and pay for digital health technologies and their influential factors among urban elderly in Hangzhou, China.
Methods: A structured questionnaire was completed by 639 older adults from 12 communities in Hangzhou. This paper presents a descriptive statistics analysis and performs a multivariate regression to identify the determinants of willingness to use and pay for digital health technologies among the elderly.
Results: The result shows the percentage of participants who chose very willing (3.6%) and partly willing (10%) to use was lower than those who were less unwilling (26.4%) and not willing (27.1%) to use. The percentage of participants who are unwilling (less unwilling,30.5%; not willing, 39.7%) to pay for digital health technology is even higher. The regression results show that age, working status, exercise and physical activity, medical insurance, income, life satisfaction and history of illness were significantly associated with willingness to use digital health technology among urban elderly. On the other hand, age, exercise status, income and history of illness were significantly associated with willingness to pay for digital health technologies among older adults.
Conclusion: The overall willingness to use and pay for digital health technologies are low among urban older people living in Hangzhou. Our results have important implications for digital health policy making. Practitioner and regulator should develop strategies to improve the supply of digital health technology services to meet different demands of the elderly with different age, working status, exercise and physical activity, medical insurance, income, life satisfaction and history of illness. And medical insurance would be an important instrument to facilitate digital health development.
Keywords: digital health, elderly healthcare, willingness to use, willingness to pay
Introduction
Along with economic development and social modernisation, an aging population has become a common phenomenon around the world. According to the Seventh National Population Census in China, there are 264.02 million people aged 60 or above, 18.7% of the population, including 190.64 million people aged 65 or over, 13.5% of the population.1 According to a report from World Bank, by 2050, people aged 65 are expected to make up 26% of China’s population, and people aged 80 and over are expected to account for 5% of the population.2 This aging population is also increasing medical and health demands, effecting a steady rise in the overall cost of healthcare for society. Consequently, traditional medical and health services have been unable to meet the increasing demand for elderly healthcare.3 Currently, family-based healthcare capacity in China is limited and weak, so digital health technology has been a valuable solution to this problem.4
Innovations in health information technology offer older people the opportunity to reduce healthcare expenditure, achieve higher quality of care and improve health outcomes.5–9 As a result, digital health has become a prominent area of practice in the adoption of conventional and innovative forms of information communications technology to meet healthcare needs.10 In this paper, digital health technology refers to the use of digital technologies in healthcare, such as electronic medical records; telemedicine or telehealth services; robotics and e-health; and m-health supported by smartphones, wearable devices, mobile apps and various monitoring devices.11–13
The digital health technologies used for the elderly are mainly smart, wearable health technologies,14,15 health monitoring technologies,16 telemedicine,17 smart home technologies18,19 and other developments. These technologies have produced new opportunities for protecting the aging population through preventive care and health monitoring. For example, the combination of smart wear and Internet of Things (IoT) technology in the field of health monitoring are becoming useful in improving older people’s quality of life.20 Wearable health technology has potential benefits for the elderly, such as reducing hospitalization and mortality, improving mental health and supporting a healthier overall lifestyle.21 Additionally, during the COVID-19 global pandemic, there has been a surge in interest and use of digital health technology.22
Accordingly, research on digital health technologies in the older adult market has grown considerably over the last decade. Some such studies have examined issues such as engagement with and acceptance of digital health technologies among older people. For example, the technology acceptance model (TAM)23 model and the theory of planned behavior (TPB)24 adopting mobile Health (mHealth) services among middle-aged and elderly users in China. This work revealed that technology anxiety and the need for self-actualisation were the main reasons for patients’ intentions to use mHealth services.25 One study analyzed 12 months of user information from the digital health platform “Lark Health”. It found that on digital health platforms, the elderly showed greater engagement than the young, indicating a willingness of older people to adopt digital health technology despite potential barriers.26 Similarly, some scholars analyzed the adoption and feasibility of digital health and wellness programs for older adults, discovering that this population’s engagement with digital health apps and programs was high and sustained.27 Such works have investigated the views, needs and perceptions of older people on using digital health technologies to facilitate healthy aging, demonstrating that older people generally have positive attitudes towards digital health technologies.28
Other studies have focused on factors influencing the use of digital health technology by older people. For example, The older people tend to be slower to adopt new technology than younger people.29 One study indicates that current use and future intentions to use wearable devices among older people are limited due to a lack of willingness to pay (WTP).21 Researchers have also developed a theoretical model based on the capability approach (CA) framework to examine the factors that impact adoption of digital healthcare technology by elderly people. This study found that when deciding whether to use digital health technologies, older people considered the extent to which these technologies would enhance their ability to live independently in the long run.30 Similarly, a questionnaire was given to examine the willingness of older people in Shanghai, China, to use mHealth and the factors influencing these decisions. This study showed that 46.4% of older people said they were willing to use mHealth. Important factors influencing their willingness to use (WTU) included understanding mHealth, using mHealth, self-testing health, perceived ease of use, perceived usefulness and self-efficacy.31
According to the existing literature, one challenge that remains is identifying the elderly’s WTU and WTP for digital health technologies and the factors that impact WTU and WTP. Understanding WTP and the influential factors can inform health policy planning processes, such as allocating resources or developing pricing strategies for telemedicine services.32 Knowing the WTU of older people for digital health technologies may help to bridge digital divide and promote digital health development. Previous studies have often examined a particular segment of digital health technology, but there is a lack of further research on the identification and comparison of older people’s WTU and WTP for digital health technologies.
Therefore, this study assesses the WTU and WTP for digital health technologies among the elderly in urban communities of Hangzhou, in China. The remaining parts of this paper are organized as follows: (1) To analyse through a questionnaire how willing older people are in urban communities in China to use and pay for digital health technologies, (2) To explore the main factors influencing older people’s WTU and WTP for digital health technologies and (3) To compare and analyse the differences in the factors affecting the WTU and WTP. Additionally, this paper provides suggestions for enhancing the adoption and quality of digital health technologies for the elderly.
Methods and Data
Study Design
Questionnaire has been a useful method to study the willingness of older people in relation to a particular technology or service. For example, some scholars used questionnaire to study the home healthcare needs of empty nesters and their WTP in China;33 WTP and the elderly’s willingness to accept (WTA) informal care;34 the elderly’s WTA related to the COVID-19 vaccine;35 internet use; and demand for digital health technology among older people.4
However, there did not exist a standard framework of questionnaire to analyse the WTU and WTP for digital health technology among the elderly in China. The Andersen Behavioural Model classifies factors related to people’s health into predisposing factors (ie demographic characteristics such as age and gender; social factors such as education, occupation and race; social relationships; and psychological factors); enabling factors (ie financial and organisational factors); and demand factors (perceived need for health services).36 Thus, this study developed a quantitative questionnaire based on existing research and incorporating Grossman’s theory of health needs37 and Andersen’s theory of behaviour.36,38 Grossman’s theory developed a model that connects people’s daily health decisions in a coherent way, examining individual health decisions over the entire life span. In the Grossman model, health can be viewed as consumer goods, production inputs (factors of production), and capital. Andersen’s Behavioral Model of Health Services Use is a conceptual model designed to demonstrate the drivers of health service utilization. The model indicates that Health service use is determined by three dynamic factors: predisposing, enabling, and demand factors, and has been widely used in studies investigating health service use.
The questionnaire contains four sections: older adults’ WTU and WTP for digital health, predisposing factors for older adults, enabling factors and demand factors. As for the ethical consideration, the study was only a willingness survey of older adults and did not involve some medical clinical trials or human trials. This study also complies with the Declaration of Helsinki. The surveyed elderly people are anonymous, people’s information is confidential, and the author’s organization supervises the process of collecting information about the survey activities.
Variables
Dependent and Independent Variables
The dependent variables refer to the psychological disposition of WTU and WTP. Therefore, a 5-point Likert scale was used to express the intensity of WTU and WTP for digital health technologies among older adults (the scale included 1= “very willing”, 2= “partly willing”, 3= “neutral”, 4 = “less unwilling”, and 5= “unwilling”).
The independent variables consist of three parts: predisposing factors, enabling factors and demand factors. (1) The predisposing factors include age, gender, education, marriage, children, working status and exercise. All of these are categorical variables (Table 1 and Table 2). (2) The enabling factors include medical insurance, income (monthly income). These are also categorical variables (Table 1 and Table 2). (3) The demand factors include psychological demand factors and physiological demand factors. The variable of life satisfaction belongs to psychological demand factor, which is a person’s evaluation of their life and can measure one’s subjective well-being.39 Physiological demand factors include the variables of hospitalization (hospitalization or illness history in the past year), disability (disabled or not) and ADL (activities of daily living). The explanation and scale of the variables is reported in Appendix. Since most of the questions were non-scale questions, we conducted a pilot-tested to ascertain its validity. In addition, the Cronbach’s alpha coefficient of variables measured by scale is 0.729. This questionnaire has good validity and reliability.
 |
Table 1 The Descriptive Statistics for WTU of the Elderly |
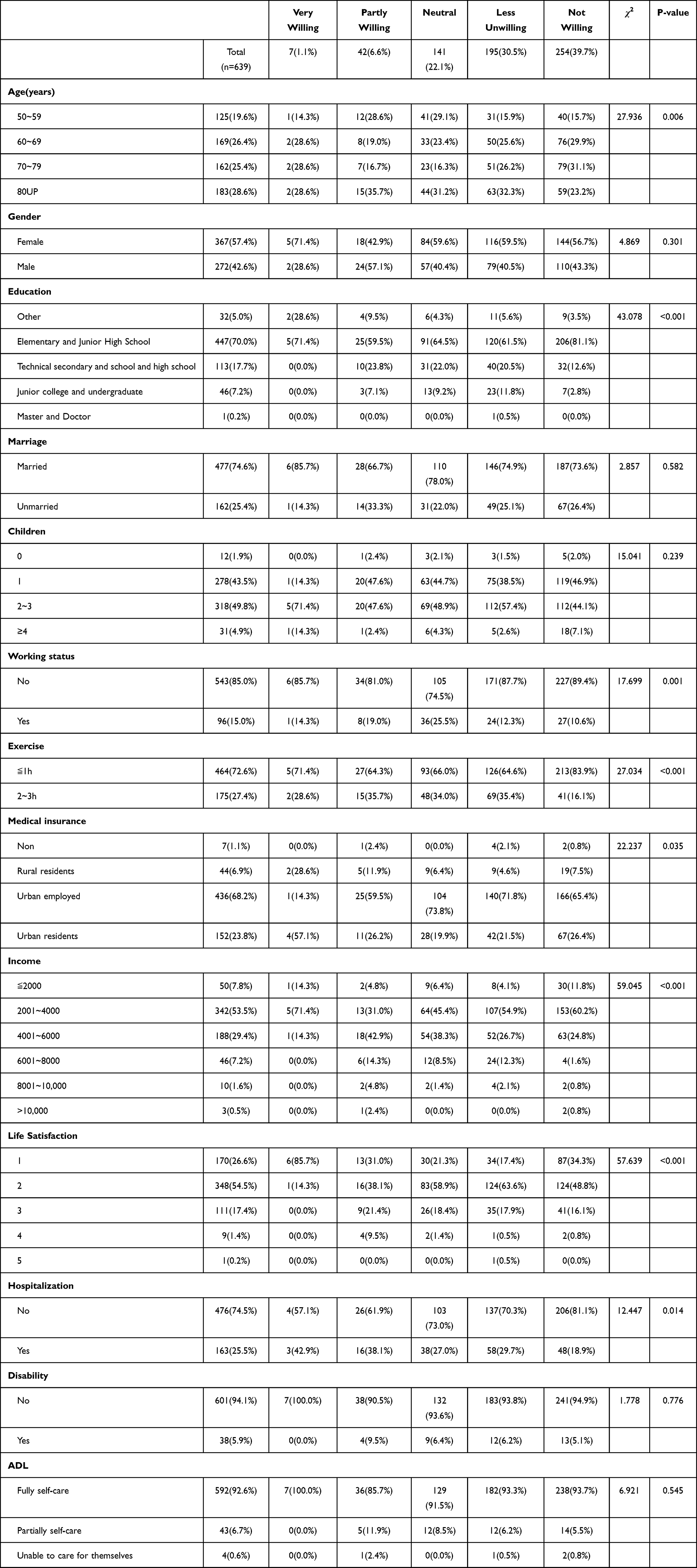 |
Table 2 WTP of the Elderly for Digital Health Technologies and Differences in Their Characteristics |
Data and Statistic Analysis
Data
This study’s participants were from Hangzhou, Zhejiang Province, China. By the end of 2021, the resident population of Hangzhou was 12,204,000. According to the seventh national population census of China, Hangzhou is classified as a megacity with a high and maturing level of Internet development. The participants were 50 years of age or older, conscious, thinking clearly, and willing volunteers in the survey. In China, the Law on the Protection of the Rights and Interests of the Elderly stipulates that one becomes elderly at 60 years old. However, this paper includes participants from 50 to 60 years old because including the people from 50 to 60 years old can well represent the differences in the WTU and WTP of the elderly in the aging process through comparison of different ages. The questionnaire distributors received standard training. They explained the purpose and significance of the study to the participants. Questionnaires were distributed after obtaining informed consent from the participants. The questionnaires were preferred to be completed by the elderly themselves. For those who had difficulty completing the questionnaires, the questionnaire distributors read the questionnaires aloud item by item and recorded the elder’s responses. The survey was conducted during April–June 2021 in 12 different communities in Hangzhou. A total of 700 questionnaires were distributed randomly, and 639 valid questionnaires were returned, a return rate of 91.29%.
Statistical Analysis
A descriptive analysis was used to describe the distribution and characteristics of older adults’ WTU and WTP for digital health technologies. The chi-square test was used to explore the correlation of independent variables with WTU and WTP. This study used the SPSS Statistics 26 to perform descriptive statistics and chi-square tests. The results would be statistically significant if P-value < 0.05.
Results
Descriptive Statistics of WTU and WTP
The WTU and WTP for digital health among the elderly are shown in Table 1 and Table 2, respectively. Of the 639 participants, in terms of WTU (see Table 1.), 3.6% (n = 23) chose “very willing”, 10% (n = 64) chose “partly willing”, 32.9% (n = 210) chose “neutral”, 26.4% (n = 169) chose “less unwilling”, and 27.1% (n = 173) chose “not willing”. Overall, the willingness of older adults to use digital health technologies was low. For WTP, 1.1% (n = 7) chose “very willing”, 6.6% (n = 64) chose “partly willing”, 22.1% (n = 141) chose “neutral”, 30.5% (n = 195) chose “less unwilling”, and 39.7% (n = 254) chose “not willing”. Comparing WTU and WTP demonstrated that the older adults in the sample were less willing to pay for digital health technology than to use it.
Descriptive Statistics of Predisposing Factors for WTU and WTP
According to Table 1 and Table 2, the participants were over 50 years old and relatively evenly distributed in age. Of the 639 respondents, 19.6% were aged 50~59 years, 26.4% were 60~69, 25.4% were 70~79 and 28.6% were 80 or older. Female participants accounted for 57.4% (n = 367) of the respondents, and male participants comprised 42.6% (n = 272) of the group. The education levels of elementary and junior high school accounted for a majority of 70% (n = 447). Additionally, 74.6% (n = 477) of the respondents were married, and 25.4% (n = 162) were non-married (including unmarried, divorced, and widowed). Of these respondents, 1.9% (n = 12) had no children, 43.5% (n = 278) had one child, 49.8% (n = 318) had 2~3 children and 4.9% (n = 31) had ≥4 children. Beyond this, 85% (n = 543) of the participants were unemployed, 15% (n = 96) had either paid or unpaid work and 72.6% (n = 464) of the participants exercised less than one hour per day.
Descriptive Statistics of the Enabling Factors for WTU and WTP
Regarding medical insurance participation, most of the respondents had urban employee medical insurance (68.2% [n = 436]). In terms of income profile, the largest proportion of respondents earned RMB 2001~4000 per month (53.5% [n = 342]), followed by 4001~6000 RMB accounting for 29.4% (n = 188) of the group.
Descriptive Statistics of Demand Factors for WTU and WTP
In this study, 26.6% (n = 170) of participants expressed that they were “very satisfied” with life, and 54.5% (n = 348) were “partly satisfied”. Additionally, the overall life satisfaction level of the sample was high. For instance, 74.5% (n = 476) of the participants had had no inpatient recuperation in the past year, and 5.9% (n = 38) of the participants were more or less disabled. The descriptive statistics of ADLs showed that 92.6% (n = 592) of the participants were able to take care of themselves completely, 6.7% (n = 43) partially and 0.6% (n = 4) were unable to care for themselves.
The chi-square test in Table 1 showed that factors associated with WTU included age (P = 0.004), education (P = 0.004), working status (P < 0.001), exercise (P < 0.001), medical insurance (P = 0.008), income (P = 0.02), life satisfaction (P < 0.001) and hospitalization (P = 0.008). There was no statistically significant relationship between WTU and gender, marriage, children, disability and ADL (Table 1).
The chi-square test in Table 2 demonstrates that factors associated with WTP included age (P = 0.006), education (P < 0.001), working status (P = 0.001), exercise (P < 0.001), medical insurance (P = 0.035), income (P < 0.001), life satisfaction (P < 0.001) and hospitalization (P = 0.014). Additionally, WTP was not statistically significantly related to gender, marriage, children, disability or ADL.
Ordered Logistic Regression Analysis of WTU and WTP
Due to the large number of classifications of dependent and independent variables in this paper, the result of Brant test was not convergent indicating that the regression deviates from the proportional odds assumption. So, some of the variables were adjusted to increase the validity of the ordered logistic regression. The research by Murad suggested that when data clearly deviates from the proportional odds assumption, it is common to consider combining categories of a variable to increase the fit of the model.40 Additionally, the dependent variable WTU or WTP each has a total of five categories to measure the degree of willingness, some of which can be combined into one category. For example, to different degrees, “very willing” and “partly willing” belong to “willing”, whereas “less unwilling” and “unwilling” belong to “unwilling”. In this regard, this paper drew from the work of Preisser et al, combining adjacent categories into one category.41 The categories “1, 2” of WTU and WTP were combined into “willing” (WTU = 1, WTP = 1); “3” as “neutral” (WTU = 2, WTP = 2); “4, 5” are combined into “unwilling” (WTU = 3, WTP = 3). Thus, the dependent variables “WTU” and “WTP” both became ordered three-level variables.
Additionally, there were more categories of income and education than other independent variables, and some of these categories had smaller sample sizes. For instance, researchers referred to the approach of Brooks et al, where adjacent, small sample categories were combined into one category.42 Regarding the variable income income, the categories “8001~10,000” and “>10,000” represent only 2.1% of the total sample. Therefore, this paper combined these two categories and the category “6001~8000” to form the larger category “income > 6000”, regarded as a higher salary level. Concerning the education variable, the category of people with a master’s degree or doctoral degree had only one sample, which is classified as undergraduate degree or above.
Following these treatments, the results of the Brant test are displayed in Table 3. The p-values of the Brant test for both models were greater than 0.05, indicating that the models did not violate the proportional odds assumption. Thus, an impact analysis could be performed with ordered logistic regression.
 |
Table 3 The Brant Test for Two Models |
Table 4 demonstrates the results of ordered logistic regressions to analyse the factors related to WTU and WTP for digital health technologies among older adults Age, working status, exercise, medical insurance, income, life satisfaction and hospitalization were significantly correlated with the WTU of digital health technologies among the elderly. Additionally, age, exercise, income and hospitalization were significantly correlated with WTP for digital health technologies among older adults. Additionally, working status, medical insurance and life satisfaction were not significantly correlated with WTP for digital health technologies among the elderly.
 |
Table 4 The Result of Ordered Logistic Regression for WTU and WTP |
Effects of Age on WTU and WTP
The results of this study showed that the coefficient of the variable age (s) were all significantly positive and the OR gradually increased (60~69:OR = 1.603, P = 0.083; 70~79: OR = 1.728, P = 0.075; 80UP: OR = 2.254, P = 0.016). Thus, the older elderly groups were less likely to use digital health technologies than those aged 50~59. Specifically, older adults in the 60~69 age group were 1.6 times, the 70~79 age group were 1.7 times, and 80 or over were 2.3 times more likely to be reluctant to use services and products with digital health technology than those aged 50~59. In terms of WTP, the elderly’s WTP for digital health technology services (eg smart healthcare services and products) was similar to their WTU. The older the person was, the lower the WTP was (60~69:OR = 1.863, P = 0.037; 70~79: OR = 2.729, P = 0.075; 80UP: OR = 1.42, P = 0.335).
Effects of Working Status on WTU and WTP
Compared with older adults who worked (paid or unpaid work), those without work were less likely to use digital health technologies (OR = 1.762, p = 0.039). According to the odds ratio, older adults who were not employed were 1.762 times more reluctant to use digital health technology than older adults who were employed. Additionally, working status was not significantly associated with WTP.
Effects of Exercise on WTU and WTP
The regression results revealed a significant negative relationship between hours of exercise and WTU (OR = 0.625, p = 0.01). In terms of the odds ratio, the respondents who exercised for 2~3 hours were 0.625 times less likely to be reluctant to use digital health technology products than those who exercised for 1 hour, holding all other variables constant. Consequently, the older population who were more exercise-oriented were more likely to use digital health technology products and services than those who were not. Similarly, in terms of WTP, those who exercised longer had a stronger WTP for digital health technology products and services than those who exercised less (OR = 0.672, p = 0.05).
Effects of Medical Insurance on WTU and WTP
Compared with uninsured older adults, those with urban resident medical insurance and urban employee medical insurance (urban residents: OR = 5.662, P = 0.036; urban employed: OR = 8.922, P = 0.008) were more reluctant to use digital health technology products and services. As shown by the odds ratio, older adults with insurance were more reluctant to use digital health technology (8.922 and 5.662 times than those who did not have medical insurance, respectively). However, the relationship between medical insurance and WTP was not significant.
Effects of Income on WTU and WTP
Older adults with higher incomes were more likely to use digital health technology products and services than those with monthly incomes <= RMB 2000 (RMB 4001~6000: OR = 0.465, p = 0.038; >RMB6000: OR=0.387, p=0.028). Regarding the odds ratio, older adults with a monthly income of RMB 4001~6000 were 0.465 times less likely to be unwilling to use digital health technology products and services than those in the income group <= RMB 2000. Additionally, the respondents with incomes > RMB 6000 were 0.387 times less likely to be more reluctant to use aspects of digital health technology products and services than those with incomes <= RMB 2000. Similarly, the higher the income was, the higher the WTP of the elderly was (RMB 4001~6000: OR = 0.337, p = 0.01; >RMB 6000: OR = 0.327, p = 0.024).
Effects of Life Satisfaction on WTU and WTP
The regression results demonstrated that the relationship between life satisfaction and WTU was significantly negative (coefficient = 0.32, OR = 0.726, p = 0.008). In this study, life satisfaction is measured on a 5-point Likert scale (1 = “very satisfied”, 2 = “partly satisfied”, 3 = “neutral”, 4 = “less satisfied”, 5 = “unsatisfied”). Thus, the negative coefficient indicates that a one-level increase in life satisfaction (becoming more dissatisfied), given other variables constant, was associated with a 0.319 decrease in respondents’ reluctance to use digital health technology products and services. In terms of the odds ratio, for a one-unit increase in life satisfaction (becoming more dissatisfied), the odds of someone’s being “unwilling” to use digital health technology versus the combined “neutral” and “willing” were 0.726 times lower when all other variables were held constant. Thus, the more dissatisfied the respondents were with their lives, the stronger their WTU was for digital health technologies. Lastly, the relationship between life satisfaction and WTP was not significant.
Effects of Hospitalization on WTU and WTP
Compared with older adults with no history of illness or hospitalization in the past year, the elderly with a history of illness hospitalization and recuperation were more likely to use digital health products and services (OR = 0.533, p = 0.001). For older adults with a history of hospitalization and illness in the past year, the odds of their being “unwilling” versus the combined “neutral” and “willing” were 0.533 times lower than for those with no history of hospitalization or illness when all other variables were held constant. Therefore, the elderly with a history of illness and hospitalization in the past year were more likely to use digital health products and services than those without such a history. In the same vein, older adults with a history of hospitalization or illness in the past year had a higher WTP than those with no history of hospitalization or illness in the past year (OR = 0.608, p = 0.02).
Discussion
The analysis of the survey sample of Chinese urban community-dwelling older adults revealed that the WTU and WTP for digital health technologies are more inclined to be unwilling to use or pay among older adults. For instance, 3.6% of the responders were very willing to use digital health technologies, 10% “partly willing”, and 32.9% displayed “neutral” willingness. Overall, the willingness of the elderly to use digital health was low. Only 1.1% of older adults were very willing to pay for digital health technologies, 6.6% were “partly willing”, and 22.1% displayed “neutral” willingness. In comparison, the WTP for digital health technologies was lower than the WTU among older adults in the sample, This is consistent with previous research findings that older adults are less likely to use mHealth.31 It is partly because digital health products and services are still in their formative years. Thus, the supply of products and services is not yet perfect, and product coverage is not extensive, resulting in a lack of access to and availability of digital health products and services that meet the needs of older adults. In addition, there is a digital divide in digital health use, with the older you are the less likely you are to engage in digital health activities.43 Older adults are often reticent to adopt technology, and most of the elderly have limited knowledge and experience in using digital technology.44 For instance, some scholars have found that the overall digital health literacy of older adults in Chinese communities is relatively low, indicating that these adults lack the ability to translate Internet health knowledge into action and apply it to health self-management.45 This issue can also affect the WTU and WTP for digital health among older adults. Additionally, in China, digital health services and products fall under the category of private (out-of-pocket) healthcare expenditure (PHCE) and are not yet covered by medical insurance. This is an important reason for the low WTU and WTP for digital health among the elderly population.
The results from the ordered logistic regressions showed that age, exercise, income and hopitalisation affected both WTU and WTP for digital health among older adults. Both WTU and WTP for digital health decreased with age, an effect like the results of previous studies, possibly because financial insecurity become more prevalent and severe with age.33
In the same vein, older adults who are more physically active are more likely to use digital health products and services and are more willing to pay for them. To some extent, the daily exercise duration of older adults reflects this population’s health and health literacy. This is because previous research has concluded that physical activity can positively impact both physical and mental health in older adults.46,47 Combining our results, it can be inferred that those who are more physically active have better health and higher health literacy and are more willing to use and pay for digital health products and services with health-promoting effects.
Furthermore, the higher these individuals’ income is, the higher the WTU and WTP for digital health products and services are among older adults. Previous research has also suggested that income level is the most common determinant of WTU and WTP for healthcare.34 Older adults with a history of hospitalization and illness have higher WTU and WTP than those without a history of hospitalization or illness in the past year. A history of illness reflects the recent health status of older adults and fits under the category of demand factors. The poorer the health status is of older adults with a recent history of hospitalization, the stronger these adults’ perceived need is for health services.36 In the same way, their WTU and WTP for digital health are also stronger.
The results from the medical insurance situation showed that older adults with urban resident medical insurance and urban employee medical insurance were more reluctant to use digital health products and services than those who were not insured. The main reason for this was that digital health products and services are not currently reimbursed by medical insurance in China. Older adults with medical insurance, especially those with “urban resident medical insurance” and “urban employee medical insurance”, are more willing than those without medical insurance to use health products or services that are covered by medical insurance and less willing than those without medical insurance to use digital health products and services that are not covered by medical insurance reimbursement. These results indicate that medical insurance payment is a limiting factor for digital health use among older adults. On the insurance product and policy level, appropriate digital health products or services should be actively screened and evaluated for inclusion in medical insurance payment, which would improve the popularity and application of digital health products or services. In terms of life satisfaction, the lower the life satisfaction of older adults is, the stronger their WTU digital health is. People with higher life satisfaction tend to have better health outcomes and behaviours.48 Older adults with lower life satisfaction have lower subjective ratings of well-being and tend to have lower health outcomes than those with higher life satisfaction. These older adults with lower life satisfaction are more willing than others to improve their health through digital health and thus have a stronger WTU digital health. However, the dissatisfaction of life does not affect WTP of the elderly.
According to existing research, only few studies have focused on older adults’ willingness to pay for and use digital health. Previous findings have concluded that older adults have more positive attitudes toward digital health, but have not delved into willingness to use and willingness to pay for digital health.26,28 And the impact of factors such as predisposing, enabling and demand on WTU and WTP is less explored.
Comparing previous studies, this study is one of the early literatures in China to explore the WTU and WTP for digital health technology among older adults, with the following main contributions and implications: (1) A questionnaire survey was used to study the willingness to use and pay for digital health technology among older adults in China. The study explored the differences in the influencing factors of both, which will help to understand the current situation of digital health needs of Chinese older adults. The results of the study will be helpful and informative for the policy development of digital health industry for the elderly in China, and will help explore the development of services or products of digital health to be included in the payment scope of medical insurance. (2) This study is the first to consider the impact of medical insurance on WTU and WTP in China, 3) This study examines the factors influencing WTU and WTP from the perspective of older adults’ own characteristics. The results of this study will be helpful for practitioner to design and provide digital health services based on the personalized needs of the elderly, and to increase the matching between digital health supply and demand.
However, this study had certain limitations: (1) This study did not include factors that could help explain older adults’ participation in digital health, such as digital skills, digital health literacy, and social engagement. Thus, future studies should investigate the impact of these factors on older adults’ behaviours. (2) The evaluation of digital health technologies was affected by selective non-engagement, and this selective non-engagement could prevent the expression of needs and interests of certain target populations and bias the study results.49 This study collected information through questionnaire survey, which could have selective bias due to the non-participation or non-responsiveness of certain individuals. (3) This study was based on a small sample of an older adult population, limiting the generalisability of the findings. The sample sources came from several different communities in one city, so there may have been regional differences among the needs of the elderly population. Therefore, this study could be expanded to different cities, and those results could be compared with this study’s results.
Furthermore, future research could be conducted to examine how improving digital health literacy of the elderly could enhance the WTU and WTP for digital health among older adults. Some scholars have found a profound digital health divide among the elderly population in the community, a difference related to age, formal education, income, and ethnicity.50 Similarly, some scholars have discovered that the use of digital health technology in healthcare delivery has created health inequities.12 Older adults are often limited by their education levels, financial circumstances, or lack of Internet access, but they are also more likely to need medical support more than other people. Thus, the digital divide is a serious barrier to achieving health equity.51 The digital health divide can impact the use and perception of health-related technologies among older adults. In advancing digital health technologies, future research could examine how bridging the digital divide among older adults could reduce health inequities and investigate how digital health technologies affect the unequal distribution of healthcare services for older adults.
Conclusion
This study shows that the willingness to use and pay for digital health technologies among older adults in urban communities in China is relatively low. Actually, the elderly population is a vulnerable group in the digital age, so bridging the digital health divide would help promote the development of digital health among older adults.
The results of the study revealed that age, work status, exercise status, medical insurance, income status, life satisfaction and sickness history were significantly associated with the WTU for digital health technologies among older adults. Additionally, age, exercise status, income status and sickness history were significantly associated with WTP for digital health technologies among older adults. These factors should be considered when promoting digital health technology products and services for the elderly population to meet the individual needs of older adults. Beyond this, medical insurance is a limiting factor in the use of digital health technologies among older adults. In this study, the elderly group with medical insurance were less willing than those without medical insurance to use digital health products and services. Thus, policymakers should actively explore the inclusion of appropriate digital health into the coverage of medical insurance payments, which would improve the popularity and adoption of digital health products or services.
Moreover, this paper’s findings could help product and service suppliers of digital health technologies and healthcare professionals to better understand the real WTU and WTP of the elderly population. Additionally, this work could provide recommendations for suppliers to design and provide patient-centred digital health services to meet the elderly’s needs. Finally, this work could help the digital health market and regulator develop appropriate strategies to improve the matching of digital health supply and demand, enhancing the adoption of digital health in the older population.
Data Sharing Statement
Data available on request, any of the authors should be contacted to request the data.
Research Ethics and Consent
One Belt-One Road Strategy Institute, Tsinghua University approved this study. This study complies with the Declaration of Helsinki. And both written and verbal consent was obtained from the participants prior to the interviews for this project. People’s information is confidential.
Acknowledgments
We would like to thank all the older adults that took part in the survey.
Disclosure
The authors declare that there is no conflict of interest regarding the publication of this article.
References
1. NBS. Main data of the seventh national population census; 2021.
2. Glinskaya E, Feng Z. Options for aged care in China: building an efficient and sustainable aged care system; 2018.
3. Majumder S, Aghayi E, Noferesti M, et al. Smart homes for elderly healthcare—recent advances and research challenges. Sensors. 2017;17(11):2496. doi:10.3390/s17112496
4. Sun X, Yan W, Zhou H, et al. Internet use and need for digital health technology among the elderly: a cross-sectional survey in China. BMC Public Health. 2020;20(1):1–8 doi:10.1186/s12889-020-09448-0.
5. Hall AK, Bernhardt JM, Dodd V, Vollrath MW. The digital health divide: evaluating online health information access and use among older adults. Health Educ Behav. 2015;42(2):202–209 doi:10.1177/1090198114547815.
6. Levine DM, Lipsitz SR, Linder JA. Trends in seniors’ use of digital health technology in the United States, 2011–2014. JAMA. 2016;316(5):538–540 doi:10.1001/jama.2016.9124.
7. Urban M. “This really takes it out of you!” senses and emotions in digital health practices of elderly. Digital Health. 2017;3:2055207617701778.
8. Singh H, Armas A, Law S, et al. How digital health solutions align with the roles and functions that support hospital to home transitions for older adults: a rapid review study protocol. BMJ Open. 2021;11(2):e045596 doi:10.1136/bmjopen-2020-045596.
9. Evangelista L, Steinhubl SR, Topol EJ. Digital health care for older adults. Lancet. 2019;393(10180):1493 doi:10.1016/S0140-6736(19)30800-1.
10. World Health Organization. WHO Guideline: Recommendations on Digital Interventions for Health System Strengthening. World Health Organization; 2019.
11. Scott BK, Miller GT, Fonda SJ, et al. Advanced digital health technologies for COVID-19 and future emergencies. Telemed E-Health. 2020;26(10):1226–1233. doi:10.1089/tmj.2020.0140
12. Yao R, Zhang W, Evans R, et al. Inequities in health care services caused by the adoption of digital health technologies: scoping review. J Med Internet Res. 2022;24(3):e34144. doi:10.2196/34144
13. Thuemmler C, Bai C. Health 4.0: how virtualization and big data are revolutionizing healthcare; 2017.
14. Stavropoulos TG, Papastergiou A, Mpaltadoros L, Nikolopoulos S, Kompatsiaris I. IoT wearable sensors and devices in elderly care: a literature review. Sensors Basel. 2020;20(10):2826. doi:10.3390/s20102826
15. Majumder S, Mondal T, Deen MJ. Wearable sensors for remote health monitoring. Sensors Basel. 2017;17(1):130. doi:10.3390/s17010130
16. Al-Khafajiy M, Baker T, Chalmers C, et al. Remote health monitoring of elderly through wearable sensors. Multimed Tools Appl. 2019;78(17):24681–24706. doi:10.1007/s11042-018-7134-7
17. Bhaskar S, Bradley S, Chattu VK, et al. Telemedicine as the new outpatient clinic gone digital: position paper from the pandemic health system REsilience PROGRAM (REPROGRAM) international consortium (Part 2). Front Public Health. 2020;8:410 doi:10.3389/fpubh.2020.00410.
18. Pal D, Funilkul S, Charoenkitkarn N, Kanthamanon P. Internet-of-things and smart homes for elderly healthcare: an end user perspective. IEEE Access. 2018;6:10483–10496. doi:10.1109/ACCESS.2018.2808472
19. Ghorayeb A, Comber R, Gooberman-Hill R. Older adults’ perspectives of smart home technology: are we developing the technology that older people want? Int J Hum-Comput St. 2021;147:102571. doi:10.1016/j.ijhcs.2020.102571
20. Chen M, Ma Y, Song J, Lai C, Hu B. Smart clothing: connecting human with clouds and big data for sustainable health monitoring. Mob Netw Appl. 2016;21(5):825–845. doi:10.1007/s11036-016-0745-1
21. Kekade S, Hseieh C, Islam MM, et al. The usefulness and actual use of wearable devices among the elderly population. Comput Meth Prog Bio. 2018;153:137–159. doi:10.1016/j.cmpb.2017.10.008
22. Jnr BA. Use of telemedicine and virtual care for remote treatment in response to COVID-19 pandemic. J Med Syst. 2020;44(7):1–9 doi:10.1007/s10916-020-01596-5.
23. Agarwal R, Prasad J. Are individual differences germane to the acceptance of new information technologies? Decision Sci. 1999;30(2):361–391. doi:10.1111/j.1540-5915.1999.tb01614.x
24. Armitage CJ, Conner M. Efficacy of the theory of planned behaviour: a meta‐analytic review. Brit J Soc Psychol. 2001;40(4):471–499. doi:10.1348/014466601164939
25. Deng Z, Mo X, Liu S. Comparison of the middle-aged and older users’ adoption of mobile health services in China. Int J Med Inform. 2014;83(3):210–224. doi:10.1016/j.ijmedinf.2013.12.002
26. Graham SA, Stein N, Shemaj F, et al. Older adults engage with personalized digital coaching programs at rates that exceed those of younger adults. Front Digit Health. 2021;2021:93 doi:10.3389/fdgth.2021.642818.
27. Tam E, Boas PKV, Ruaro F, et al. Feasibility and adoption of a focused digital wellness program in older adults. Geriatrics. 2021;6(2):54. doi:10.3390/geriatrics6020054
28. Ienca M, Schneble C, Kressig RW, Wangmo T. Digital health interventions for healthy ageing: a qualitative user evaluation and ethical assessment. Bmc Geriatr. 2021;21(1):1–10. doi:10.1186/s12877-021-02338-z
29. Vaportzis E, Giatsi Clausen M, Gow AJ. Older adults perceptions of technology and barriers to interacting with tablet computers: a focus group study. Front Psychol. 2017;8:1687. doi:10.3389/fpsyg.2017.01687
30. Nikou S, Agahari W, Keijzer-Broers W, de Reuver M. Digital healthcare technology adoption by elderly people: a capability approach model. Telemat Inform. 2020;53:101315 doi:10.1016/j.tele.2019.101315.
31. Chen Y, Xu Q. The willingness to use mobile health and its influencing factors among elderly patients with chronic heart failure in Shanghai, China. Int J Med Inform. 2022;158:104656 doi:10.1016/j.ijmedinf.2021.104656.
32. Chua V, Koh JH, Koh CHG, Tyagi S. The willingness to pay for telemedicine among patients with chronic diseases: systematic review. J Med Internet Res. 2022;24(4):e33372 doi:10.2196/33372.
33. Liu L, Fu Y, Qu L, Wang Y. Home health care needs and willingness to pay for home health care among the empty-nest elderly in Shanghai, China. Int J Gerontol. 2014;8(1):31–36 doi:10.1016/j.ijge.2013.01.013.
34. Liu W, Lyu T, Zhang X, Yuan S, Zhang H. Willingness-to-pay and willingness-to-accept of informal caregivers of dependent elderly people in Shanghai, China. BMC Health Serv Res. 2020;20(1):1–11 doi:10.1186/s12913-020-05481-2.
35. Wang J, Yuan B, Lu X, et al. Willingness to accept COVID-19 vaccine among the elderly and the chronic disease population in China. Hum Vacc Immunother. 2021;17(12):4873–4888 doi:10.1080/21645515.2021.2009290.
36. Babitsch B, Gohl D, Von Lengerke T. Re-revisiting andersen’s behavioral model of health services use: a systematic review of studies from 1998–2011. GMS Psycho Soc Med. 2012;9. doi:10.3205/psm000089
37. Grossman M. The human capital model of the demand for health; 1999.
38. Andersen RM, Davidson PL, Baumeister SE. Improving access to care in America. In: Changing the US Health Care System: Key Issues in Health Services Policy and Management.
39. Pavot W, Diener E. The satisfaction with life scale and the emerging construct of life satisfaction. J Posit Psychol. 2008;3(2):137–152 doi:10.1080/17439760701756946.
40. Murad H, Fleischman A, Sadetzki S, Geyer O, Freedman LS. Small samples and ordered logistic regression: does it help to collapse categories of outcome? Am Stat. 2003;57(3):155–160 doi:10.1198/0003130031892.
41. Preisser JS, Phillips C, Perin J, Schwartz TA. Regression models for patient‐reported measures having ordered categories recorded on multiple occasions. Community Dent Oral. 2011;39(2):154–163 doi:10.1111/j.1600-0528.2010.00583.x.
42. Brooks J, Oxley D, Vedlitz A, Zahran S, Lindsey C. Abnormal daily temperature and concern about climate change across the U nited States. Rev Policy Res. 2014;31(3):199–217 doi:10.1111/ropr.12067.
43. Kontos E, Blake KD, Chou WS, Prestin A. Predictors of eHealth usage: insights on the digital divide from the Health Information National Trends Survey 2012. J Med Internet Res. 2014;16(7):e172 doi:10.2196/jmir.3117.
44. Niehaves B, Plattfaut R. Internet adoption by the elderly: employing IS technology acceptance theories for understanding the age-related digital divide. Eur J Inform Syst. 2014;23(6):708–726 doi:10.1057/ejis.2013.19.
45. Liu S, Zhao H, Fu J, et al. Current status and influencing factors of digital health literacy among community-dwelling older adults in Southwest China: a cross-sectional study. BMC Public Health. 2022;22(1):1–12 doi:10.1186/s12889-022-13378-4.
46. Lok N, Lok S, Canbaz M. The effect of physical activity on depressive symptoms and quality of life among elderly nursing home residents: randomized controlled trial. Arch Gerontol Geriat. 2017;70:92–98 doi:10.1016/j.archger.2017.01.008.
47. Koivula N. Sport participation: differences in motivation and actual. J Sport Behav. 1999;22(3):15.
48. Kim ES, Delaney SW, Tay L, et al. Life satisfaction and subsequent physical, behavioral, and psychosocial health in older adults. Milbank Q. 2021;99(1):209–239 doi:10.1111/1468-0009.12497.
49. Poli A, Kelfve S, Klompstra L, et al. Prediction of (Non) participation of older people in digital health research: exergame intervention study. J Med Internet Res. 2020;22(6):e17884 doi:10.2196/17884.
50. Tappen RM, Cooley ME, Luckmann R, Panday S. Digital health information disparities in older adults: a mixed methods study. J Racial Ethn Health Disparities. 2022;9(1):82–92 doi:10.1007/s40615-020-00931-3.
51. Zhou X, Chen L. Digital health care in China and access for older people. Lancet Public Health. 2021;6(12):e873–e874 doi:10.1016/S2468-2667(21)00051-7.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.