")
Back to Journals » Lung Cancer: Targets and Therapy » Volume 13
Deconstructing ADAURA: It is Time to Forgo Adjuvant Platinum-Based Chemotherapy in Resected IB-IIIA EGFR+ NSCLC (Except with RB Alterations?) When Adopting Adjuvant Osimertinib
Received 22 January 2022
Accepted for publication 6 April 2022
Published 26 April 2022 Volume 2022:13 Pages 23—31
DOI https://doi.org/10.2147/LCTT.S358902
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Fengying Wu
Shannon S Zhang,1 Sai-Hong Ignatius Ou1,2
1University of California Irvine School of Medicine, Department of Medicine, Orange, CA, USA; 2Chao Family Comprehensive Cancer Center, Orange, CA, USA
Correspondence: Sai-Hong Ignatius Ou, University of California, Irvine School of Medicine, Department of Medicine, 200 South Manchester Ave, Suite 400, Orange, CA, 92868, USA Email [email protected]
Abstract: Adjuvant cisplatin-based chemotherapy is considered the standard of care for resected stage IB (tumor ≥ 4m)–IIIA non-small cell lung cancer (NSCLC). The ADAURA trial is a randomized placebo-controlled Phase III trial that demonstrated statistically significant improved disease-free survival (DFS) with the use of 3-years of adjuvant osimertinib in resected stage IB–IIIA NSCLC harboring epidermal growth factor receptor (EGFR) del 19 or L858R mutations. Subgroup analysis revealed that the DFS improvement with adjuvant osimertinib is independent of adjuvant chemotherapy in the primary analysis. A recent follow-up report suggested that adjuvant cisplatin-based chemotherapy provided no additional 2-year DFS improvement on top of adjuvant osimertinib regardless of stage (IB, II, or IIIA) and minimal numerical DFS benefit in stage II or IIIA resected EGFR+ NSCLC for those patients who did not receive adjuvant osimertinib. Here, we argue that if clinicians adopt the use of 3 years of adjuvant osimertinib in resected early-stage EGFR+ NSCLC, there is no role for adjuvant platinum-based chemotherapy. The use of adjuvant chemotherapy was balanced between the osimertinib and the placebo arms by stage even though adjuvant chemotherapy was not one of the three stratification factors (del 19 vs L858R; Stage IA vs II vs III; Asians versus non-Asian) in ADAURA. There may be a potential role of adjuvant cisplatin/vinorelbine in a small subgroup of EGFR+ NSCLC patients whose tumor harbors retinoblastoma (RB) gene alterations but requires further investigation.
Keywords: ADAURA, osimertinib, EGFR mutation, resected NSCLC, adjuvant, platinum-based chemotherapy, cisplatin; disease-free survival
Adjuvant Cisplatin-Based Chemotherapy as Standard of Care in Resected (IB–IIIA) NSCLC
Surgical resection of early-stage NSCLC for cure is the standard of choice although less than half of patients survive at five years.1 The addition of adjuvant cisplatin-based chemotherapy is the standard of care in resected stage IB (usually ≥ 4cm)–IIIA NSCLC based on several large scale international randomized trials supported by meta-analyses to augment this survival. Overall, from the early large scale meta-analysis adjuvant chemotherapy was only beneficial with cisplatin-based chemotherapy with a 13% relative reduction of death and absolute overall survival (OS) increase of 5% at 5 years.2 Subsequently, four large-scale randomized trials comparing platinum-based chemotherapy versus observation reported absolute OS benefit;3–6 although one trial on longer follow up the OS benefit was not significant (IALT)7 and another trial was an unplanned post-hoc analysis (CALGB9633) (Figure 1).
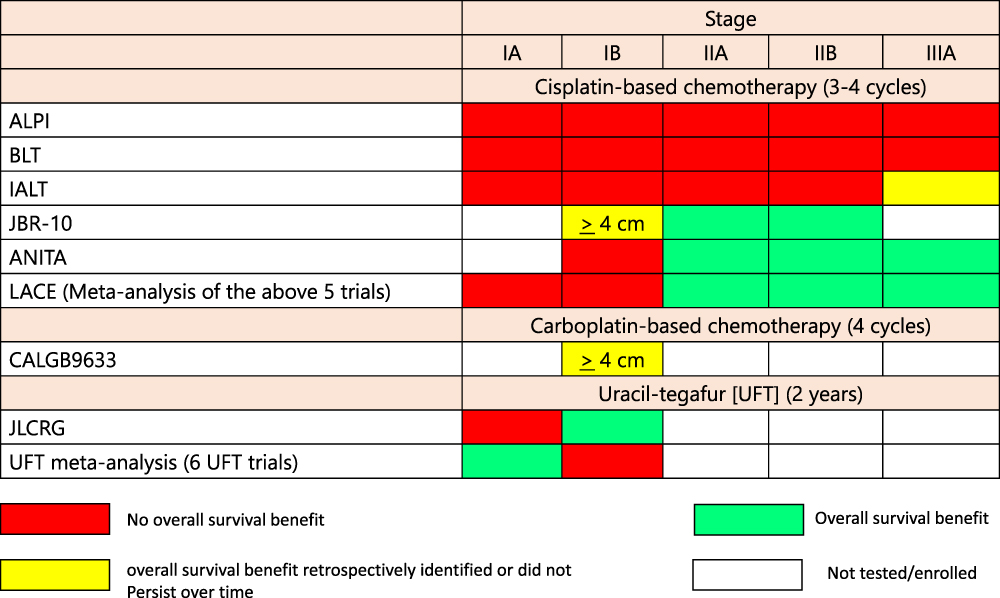 |
Figure 1 Color matrix showing OS benefit or lack of benefit by stage among the large adjuvant platinum-based chemotherapy or other adjuvant chemotherapy versus observation. Red box indicated no OS benefit. Yellow box indicated OS benefit determined retrospectively or OS did not persist overtime. Green box indicated OS benefit. White box indicated that particular stage was not investigated in the trial. Abbreviations: ALPI, Adjuvant Lung Cancer Project Italy; ANITA, Adjuvant Navelbine International Trialist Association; BLT, Big Lung Trial; CALGB, Cancer and Leukemia Group B; IALT, International Adjuvant Lung Trial. |
First, the International Adjuvant Lung Trial (IALT) reported absolute survival improvement of 4.1% years at 5 years, but benefit was only limited to stage III from the subgroup analysis.3 Furthermore, with longer follow up with a median follow up of 7.5 years, the OS benefit significance was lost (HR = 0.91; 95% CI: 0.81–1.02; P = 0.10) with an absolute increased OS of 3.9% at 5 years7 (Figure 1).
Second, The National Cancer Center of Canada trial JBR-10 trials comparing cisplatin/vinorelbine (VP) for 4 cycles versus observation reported an absolute improvement in 5-year survival of 15% with 5.1 years of follow up4 which importantly remained at 11% with 9.3 years follow up8 (Figure 1).
Third, the Adjuvant Navelbine International Trialist Association (ANITA) death was significantly reduced in patients assigned chemotherapy compared with controls (hazard ratio 0.80 [95% CI 0.66–0.96]; p=0.017). The absolute overall survival benefit for patients receiving VP compared with observation was 2.8% at 1 year, 4.7% at 2 years, 8.6% at 5 years, and 8.4% at 7 years5 (Figure 1).
Fourth, the CALGB9633 demonstrated no OS benefit with 4 cycles adjuvant carboplatin-paclitaxel compared to observation in resected stage IB NSCLC. Post-hoc unplanned analysis indicated tumor size that was 4 cm or larger achieved a (HR = 0.69, 95% CI: 0.48–0.99; p = 0.043).6 Hence post-hoc unplanned analysis of CALBG9633 and established that adjuvant chemotherapy is indicated for stage IB NSCLC with tumor size 4 cm or larger (≥ 4 cm) that was retrospectively confirmed by JBR-108 (Figure 1).
However not all randomized trials were positive for OS. The Adjuvant Lung Cancer Project Italy (ALPI) and the under-powered Big Lung Trial (BLT) from United Kingdom did not demonstrate OS with adjuvant cisplatin-based chemotherapy over observation9,10 (Figure 1).
The most updated and comprehensive meta-analysis using individual patient data indicated adjuvant cisplatin-based chemotherapy confers a 14% reduction of death and an absolute improvement of OS of 4% at 5 years.11 Not surprisingly, further meta-analyses revealed cisplatin-vinorelbine was the most efficacious regimen with a relative risk reduction of death of 20% and a 5-year absolute OS survival benefit of 8.9% given the two persistently positive randomized trials ANITA and JBR-10 received VP exclusively.12 Furthermore, adjuvant cisplatin-based chemotherapy regimen based on pharmacogenomic biomarker expression did not confer any OS benefit over standard chemotherapy.13
Adjuvant Uracil-Tegafur (UFT) Maintenance Trials
In Asia, especially in Japan, clinical investigators have pursued a more adjuvant maintenance approach. Uracil-tegafur (UFT) is a combination of the 5FU prodrug tetrahydrofuranyl-5-fluorouracil (tegafur) and uracil in a 1:4 ratio. Uracil inhibits the uracil-reducing enzyme dihydropyrimidine dehydrogenase (DPD), thereby inhibiting first-pass DPD-mediated hepatic metabolism of the uracil analogue 5-FU and permitting administration of 5-FU as the orally bioavailable prodrug tegafur.14 UFT has been used extensively in Japan as an oral form of 5FU and in the adjuvant setting usually continuously for 2 years.
A meta-analysis of 6 randomized UFT trials indicated there was a 4.1% absolute improvement in OS at 5 years and a 7.0% absolute benefit in OS at 7 years with an HR of 0.74 (95% CI: 0.61–0.88). The OS benefit was significant in stage IA NSCLC (HR = 0.73; 95% CI: 0.56–0.93) but just missed the significance cutoff for stage IB disease (HR = 0.78; 95% CI: 0.60 to 1.01).15 Of the 6 adjuvant UFT randomized trials, the largest one is the Japan Lung Cancer Research Group (JLCRG) which enrolled only stage I resected adenocarcinoma patients. JLCRG reported an absolute improvement of stage IB adenocarcinoma patients 11% at 5 years of 11% (HR = 0.48; 95% CI: 0.29–0.81, p = 0.005). For stage 1A adenocarcinoma, there was a 1% absolute decrease in OS in the UFT group versus no treatment (89% vs 90%, HR = 0.97;95% CI: 0.64–1.46; p = 0.87).16 Thus, a prolonged chemotherapy maintenance approach may be beneficial even in the earliest resected stage I NSCLC, but it is not readily adopted nowadays. Indeed, there is a positive adjuvant trial of bestatin for 2 years in resected stage I squamous cell carcinoma of the lung.17
While adjuvant UFT is rarely used even in Japan nowadays as adjuvant chemotherapy for early-stage NSCLC, the concept of a prolonged suppression can result in OS improvement even in stage IA resected NSCLC indicated a prolonged treatment approach over 2 years may be more beneficial than 4 cycles of adjuvant chemotherapy within a 3-month period.
1st-Generation EGFR TKI versus Chemotherapy in Resected EGFR+ NSCLC
Given the proven efficacy of first-generation epidermal growth factor receptor (gefitinib, erlotinib, icotinib) over platinum-based chemotherapy as first-line treatment of advanced EGFR+ NSCLC,18 this strategy has been investigated against platinum-based chemotherapy in the adjuvant management of resected early-stage EGFR+ NSCLC. All three 1G EGFR TKIs (gefitinib, erlotinib, icotinib) all demonstrated superior DFS over platinum-based chemotherapy in either Phase 2 or 3 trials.
In the EVAN trial, erlotinib was compared to VP in resected stage IIIA EGFR+ NSCLC and there was improvement in median DFS of 42.4 vs 21.2 months (P < 0.0063, HR = 0.327) with the use of erlotinib.19 5-year OS was also significantly improved for erlotinib vs VP (84.8% vs 51.1%; HR = 0.318; P = 0.0015).19
In the ADJUVANT trial, gefitinib was compared to cisplatin/vinorelbine in resected stage II–IIIA EGFR+ NSCLC and there was improvement in DFS of 30.8 with gefitinib vs 19.8 months with VP (P = 0.001, HR = 0.56).20 There was numerically improvement in 5-year OS: 53.2% (gefitinib) vs 51.2% (VP) (P = 0.674, HR = 0.92).21
In the EVIDENCE trial, the median DFS was 47.0 months in the icotinib group versus 22.1 months in the VP group (stratified hazard ratio [HR] 0.36 p<0.0001). Three-year disease-free survival was 63.9% (in the icotinib group versus 32.5% (21.3–44.2) in the chemotherapy group.22
Finally, in the IMPACT trial, the median DFS was 35.9 months in gefitinib group versus and 25.1 months in the VP group (HR = 0.92; 95% CI, 0.67 to 1.28; P = 0.63). There was also no difference in 5-year OS with 78.0% for gefitinib vs 74.6% for VP, (HR = 1.03; P = 0.89).23
Thus, the trials conducted in Asia demonstrated that adjuvant EGFR TKIs are equal if not superior to VP chemotherapy in resected EGFR+ NSCLC, there is still the question ex-Asia where cisplatin-based chemotherapy remained the standard of care. The unanswered question is whether adjuvant chemotherapy is necessary if adjuvant EGFR TKI is given as the incremental benefit of additional cisplatin-based chemotherapy is likely limited.24 The current NCI cooperative group trial (ALCHEMIST, A081105, NCT02193282) is investigating the role of adjuvant erlotinib for 2 years versus placebo in completely resected stage IB (≥ 4 cm)–IIIA EGFR+ NSCLC patients following standard post-operative surgery. The primary endpoint is overall survival. The trial has stopped accrual and results are eagerly awaited.
ADAURA Overall Results
In the meantime, the ADAURA trial is a randomized double-blind placebo-controlled Phase 3 trial that demonstrated three-years of adjuvant osimertinib at 80 mg daily conferred significant disease-free survival (DFS) over placebo for patients with resected stage IB–IIIA EGFR+ NSCLC.25 Patients were stratified by stage, EGFR mutation (exon 19 deletion versus L858R), and race (Asian versus non-Asian), but not by use of adjuvant cisplatin-based chemotherapy. Patients however were allowed to have platinum-based chemotherapy for a maximum of four cycles prior to randomization although this was not mandated.
At 24 months follow up, 89% (95% CI: 85–92) of stage IB to IIIA patients who received osimertinib were alive and disease free compared to 52% (95% CI: 46–58) in placebo group (HR = 0.20; 99.1% CI: 0.14–0.30; P < 0.001). Importantly, the DFS benefit was significant regardless of stage; stage IB: HR = 0.39 (95% CI: 0.18–0.76); stage II: HR = 0.17 (95% CI: 0.08–0.31); stage IIIA: HR = 0.12 (95% CI: 0.07–0.20). Furthermore, the DFS benefit is independent of adjuvant chemotherapy use (no adjuvant chemotherapy, HR = 0.23 (95% CI: 0.13–0.40); prior adjuvant chemotherapy, HR = 0.16 (95% CI: 0.10–0.26)). However, the absolute benefit of additional chemotherapy if any was not initially reported and no comparison of the two HRs about chemotherapy was performed in the initial report.26,27
Adjuvant Platinum-Based Chemotherapy
Professor Wu et al follow up with a detailed analysis of the role of adjuvant chemotherapy in ADAURA. Given adjuvant chemotherapy was not a stratification factor in ADAURA, patients were treated according in “real world” situation. Indeed, in both treatment arms, the higher stage of the resected EGFR+ NSCLC, the higher the percentage of patients who received adjuvant chemotherapy. Despite not being a stratification factor, the used of cisplatin-based chemotherapy was well balanced by stage between the treatment arms (Figure 2).25 Overall, the 2-year DFS benefit seen with osimertinib was 89% regardless whether patients had received adjuvant chemotherapy or not (Figure 3).28 Furthermore, patients who received osimertinib had the same 2-year DFS regardless of whether they received chemotherapy or not when analyzed by stage (IB, II, IIIA) (Figure 3). These data provided clear evidence that addition of 4 cycles of adjuvant cisplatin-based chemotherapy did not confer any additional DFS benefit when 3-year of adjuvant osimertinib was given.
 |
Figure 2 Bar-charts showing the percentage of patients who received adjuvant chemotherapy by stage (IB, II, III) and by treatment arms (Osimertinib, placebo). |
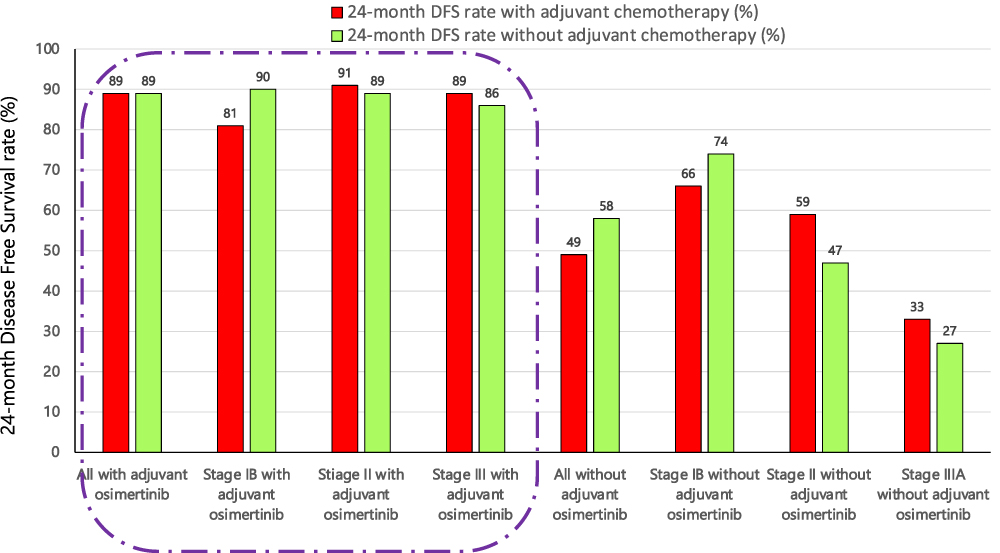 |
Figure 3 Side by side comparison of 2-year Disease-free survival (DFS) by treatment arms according to stage. |
Others have commented given cisplatin-based chemotherapy had OS benefit albeit a small absolute in 5-year OS rate whether it is better to wait to give EGFR TKI after disease relapse in view of OS in ADAURA is still immature. However, as shown in Figure 3, the 2-DFS rate was significantly lower without adjuvant osimertinib even with the use of adjuvant chemotherapy. The 2-years DFS was worst with stage IIIA and adjuvant chemotherapy increased the percentage from 27% to 33%. (Figure 3).28 Thus, even with the use of adjuvant chemotherapy, it is not advisable to withhold adjuvant osimertinib in resected stage II–IIIA disease.
Supporting Retrospective Evidence
A pooled analysis of the 3 positive adjuvant trials (IALT, JRB-10, and CALGB9633) on the effect of adjuvant cisplatin-based chemotherapy in the EGFR+ NSCLC patients indicated adjuvant cisplatin chemotherapy did not result in OS benefit (HR, 0.67 [95% CI, 0.20 to 2.21]; P = 0.51) or even when EGFR mutation is in the presence of TP53 mutations (HR, 1.06 [95% CI, 0.23 to 4.94]; P = 0.94).29
Disadvantages of Adjuvant Cisplatin-Based Chemotherapy
The main challenge of delivering cisplatin-based chemotherapy is toxicities such as nausea/vomiting, peripheral neuropathy, nephrotoxicity, and ototoxicity. The percentages of patients who completed the assigned cisplatin-based chemotherapy in unselected NSCLC or EGFR+ NSCLC are listed in Table 1. Furthermore, it requires 12 weeks to complete 4 cycles of chemotherapy plus additional recovery time from side effects thus potentially delaying the start of adjuvant osimertinib for at least 12 weeks.
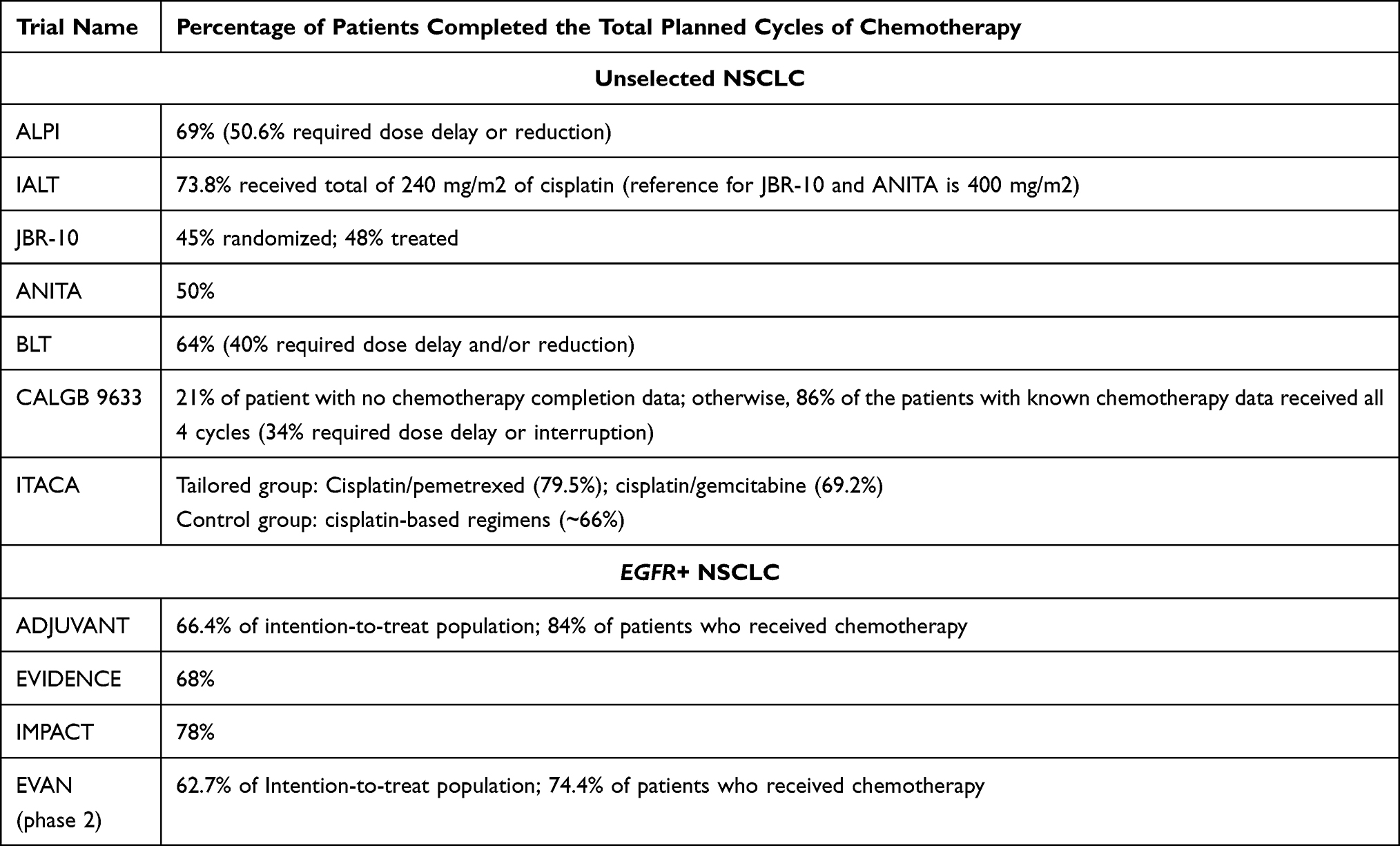 |
Table 1 Percentages of Patients Completed the Full Planned Adjuvant Platinum-Based Chemotherapy |
Correlative Sciences to Identify Which EGFR+ NSCLC Patients May Benefit from VP
The ADJUVANT clinical investigators performed an elegant multi-gene analysis of the intra-tumor genomic alterations among the EGFR+ NSCLC patients who would benefit from 2 years of adjuvant 1G EGFR gefitinib versus VP chemotherapy. The authors identified three molecular subgroups of EGFR+ NSCLC using a 5-gene MINERVA score: highly TKI-response, TKI-responsive, and VP-responsive. VP-responsive account for 14% of the patients and had mutations in the retinoblastoma (RB) gene. With this non-TKI responsive group VP had a significantly longer median DFS than gefitinib (34.2 months vs 19.3 months) and a significantly higher 2-year DFS rate [69.2% (95 CI: 48.2–99.5) vs 41.6% (95% CI: 19.9–86.8) (P = 0.041). Importantly, the DFS Kaplan-Meier curves diverged at 18 months with a decline for the gefitinib. However, the number of patients analyzed was very limited thus at most hypothesis generating (N = 13 on the VP arm vs N = 11 for the gefitinib arm).30 It remained to be determined whether using a more potent and longer EGFR TKI will overcome this DFS disadvantage.
Summary Arguments for No Adjuvant Cisplatin-Based Chemotherapy in Resected IB-IIIA EGFR+ NSCLC Who Will Receive 3 Years of Adjuvant Osimertinib
- The debate in this editorial is not about whether to give 3-years of adjuvant osimertinib in resected early stage EGFR+ NSCLC based on the ADAURA results. The US FDA in their approval of the use of 3 years of adjuvant osimertinib considered “DFS in ADAURA is statistically significant, is clinically meaningful, and provides evidence of effectiveness. Although data for OS are immature at the time of this interim analysis, there is no evidence of a detriment on OS, and a positive trend toward improvement in OS [(HR = 0.40; 95% CI: 0.18–0.89) abstracted from the manuscript text] was observed in patients treated with osimertinib.”31
- The US FDA also was neutral in the use of adjuvant chemotherapy based on the data from ADAURA. “Early-stage NSCLC is a life-threatening condition with high rates of disease recurrence after surgical resection with or without adjuvant chemotherapy.” “Exploratory analyses by receipt of adjuvant chemotherapy did not reveal a substantial difference in efficacy or safety results.”31
- The use of adjuvant platinum-based chemotherapy for resected early-stage NSCLC is based primarily on 4 positive randomized trials (IALT, ANITA, JBR-10, and CALGB9633) and supported by meta-analysis. One of these trials lost OS benefit significance over time (IALT) and was only positive for resected stage III NSCLC in the original publication.
- Another trial (CALGB9633) was not positive for the primary endpoint and only by an unplanned post-hoc that found tumor 4 cm or larger had improved OS with 4 cycles of carboplatin/paclitaxel and had been questioned by others.32
- The most efficacious adjuvant chemotherapy is cisplatin/vinorelbine, a chemotherapy regimen not commonly used in the US. The OS benefit of cisplatin/pemetrexed has not been fully explored.
- Pharmacogenomic-based biomarker selection of adjuvant chemotherapy was not superior to standard adjuvant chemotherapy.
- Pooled biomarker analysis indicated adjuvant cisplatin-based chemotherapy did not show OS improvement over observation in EGFR+ NSCLC patients though the analysis was done with limited number of EGFR+ NSCLC patients.
- Only half of patients in the randomized clinical trials completed the full treatment cycles of cisplatin-based chemotherapy thus demonstrating significant toxicities of cisplatin-based chemotherapy.
- Not completing the planned doses/cycles of cisplatin-based chemotherapy will likely compromise the benefit of adjuvant chemotherapy while simultaneously delaying the start of adjuvant Osimertinib.
- The use of adjuvant cisplatin-based chemotherapy can potentially delay initiation of adjuvant osimertinib by at least 12 weeks even if patients can complete the 4 cycles of planned cisplatin-based chemotherapy.
- 2 years of adjuvant first-generation EGFR TKIs provided statistically significant superior PFS over 4 cycles of adjuvant cisplatin-vinorelbine chemotherapy in resected early stage EGFR+ NSCLC three different randomized clinical trials (EVAN, ADJUVANT, EVIDENCE) indicating adjuvant VP unlikely to provide incremental DFS benefit.
- The addition of adjuvant cisplatin-based chemotherapy to 3 years of adjuvant osimertinib did not provide any additional numerical benefit in DFS overall and by stage (Figure 2).
- The DFS benefit of adjuvant chemotherapy (improved from 47% to 59% 2-year DFS) was numerically best among resected stage II EGFR+ NSCLC patients who did NOT receive adjuvant osimertinib.
- Resected stage IIIA EGFR+ NSCLC patients who did not receive adjuvant osimertinib had poor 2-year DFS and adjuvant chemotherapy only minimally improved 2-year DFS by 5% (from 27% to 33%). The bulk of the DFS benefit came from adjuvant osimertinib.
- The ALCHEMIST trial conducted in the US comparing 2 years of maintenance gefitinib to observation may provide additional data on the role of adjuvant chemotherapy as patients were allowed to receive post-op adjuvant treatment prior to randomization to gefitinib or placebo. However, given the lack of OS from ADJUANT and IMPACT trials, if ALCHEMIST is negative for OS benefit which is highly likely, it may be hard to discern any DFS benefit from adjuvant chemotherapy.
- From the ADJUVANT 5-gene MINVERNA expression profiling, EGFR+ NSCLC with RB alterations (mutations or deletion) had better DFS with VP than gefitinib. However, the DFS curves only started to separate at 18 months. It is unknown with longer (3 years instead of 2 years) treatment of a more potent EGFR TKI, whether the benefit of VP still hold.
- Genomic RB alterations represent a TKI-refractory subgroup of EGFR+ NSCLC patients may warrant 4 cycles of adjuvant VP followed by at least 3 years of adjuvant osimertinib.
- The principle of long term maintenance chemotherapy approach such as with 5FU based oral chemotherapy should be revisited.
Abbreviations
ALPI, Adjuvant Lung Cancer Project Italy; ANITA, Adjuvant Navelbine International Trialist Association; BLT, Big Lung Trial; CALGB, Cancer and Leukemia Group B; DFS, Disease free survival; IALT, International Adjuvant Lung Trial; VP, Vinorelbine platinum.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Professor Sai-Hong Ignatius Ou reports personal fees from Caris Life Science, Pfizer, JNJ/Janssen, BeiGene, Lilly, DAVA Oncology LP, and Daiichi Sankyo, stock ownership of Turning Point Therapeutics and Elevation Oncology, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. PORT Meta-analysis Trialists Group. Postoperative radiotherapy in non-small-cell lung cancer: a systematic review and meta-analysis of individual patient data from nine randomized controlled trials. Lancet. 1998;352(9124):257–263. doi:10.1016/S0140-6736(98)06341-7
2. Non-Small-Cell Lung Cancer Collaborative Group. Chemotherapy in nonsmall- cell lung cancer: a meta-analysis using updated data on individual patients from 52 randomized clinical trials. BMJ. 1995;311:899–910. doi:10.1136/bmj.311.7010.899
3. Arriagada R, Bergman B, Dunant A, et al. Cisplatin-based adjuvant chemotherapy in patients with completely resected non-small-cell lung cancer. N Engl J Med. 2004;350(4):351–360.
4. Winton T, Livingston R, Johnson D, et al. Vinorelbine plus cisplatin vs. observation in resected non-small-cell lung cancer. N Engl J Med. 2005;352:2589–2597.
5. Douillard JY, Rosell R, De Lena M, et al. Adjuvant vinorelbine plus cisplatin versus observation in patients with completely resected stage IB-IIIA non-small-cell lung cancer (Adjuvant Navelbine International Trialist Association [ANITA]): a randomized controlled trial. Lancet Oncol. 2006;7(9):719–727.
6. Strauss GM, Herndon JE, Maddaus MA, et al. Adjuvant paclitaxel plus carboplatin compared with observation in stage IB non-small cell lung cancer:CALGB 9633 with the Cancer and Leukemia Group B, Radiation Therapy Oncology Group, and North Central Cancer Treatment Group Study Groups. J Clin Oncol. 2008;26:5043–5051.
7. Arriagada R, Dunant A, Pignon JP, et al. Long-term results of the international adjuvant lung cancer trial evaluating adjuvant Cisplatin-based chemotherapy in resected lung cancer. J Clin Oncol. 2010;28(1):35–42.
8. Butts CA, Ding K, Seymour L, et al. Randomized phase III trial of vinorelbine plus cisplatin compared with observation in completely resected stage IB and II non–small-cell lung cancer: updated survival analysis of JBR-10. J Clin Oncol. 2009;28:29–34.
9. Scagliotti GV, Fossati R, Torri V, et al. Randomized study of adjuvant chemotherapy for completely resected stage I, II, or IIIA non-small-cell Lung cancer. J Natl Cancer Inst. 2003;95(19):1453–1461.
10. Waller D, Peaker MD, Stephens RJ, et al. Chemotherapy for patients with non-small cell lung cancer: the surgical setting of the Big Lung Trial. Eur J Cardiothorac Surg. 2004;26(1):173–182. doi:10.1016/j.ejcts.2004.03.041
11. Burdett S, Pignon JP, Tierney J, et al. Adjuvant chemotherapy for resected early-stage non-small cell lung cancer. Cochrane Database Syst Rev. 2015;2(3):CD011430.
12. Douillard JY, Tribodet H, Aubert D, et al. Adjuvant cisplatin and vinorelbine for completely resected non-small cell lung cancer: subgroup analysis of the lung adjuvant cisplatin evaluation. J Thorac Oncol. 2010;5(2):220–228. doi:10.1097/JTO.0b013e3181c814e7
13. Novello S, Torri V, Grohe C, et al. International Tailored Chemotherapy Adjuvant (ITACA) trial, a phase III multicenter randomized trial comparing adjuvant pharmacogenomic-driven chemotherapy versus standard adjuvant chemotherapy in completely resected stage II-IIIA non-small-cell lung cancer. Ann Oncol. 2022;33(1):57–66. doi:10.1016/j.annonc.2021.09.017
14. Available from: https://www.cancer.gov/publications/dictionaries/cancer-drug/def/tegafur-uracil.
15. Hamada C, Tanaka F, Ohta M, et al. Meta-analysis of postoperative adjuvant chemotherapy with tegafur-uracil in non-small-cell lung cancer. J Clin Oncol. 2005;23(22):4999–5006. doi:10.1200/JCO.2005.09.017
16. Kato H, Ichinose Y, Ohta M, et al. A randomized trial of adjuvant chemotherapy with uracil-tegafur for adenocarcinoma of the lung. N Engl J Med. 2004;350(17):1713–1721. doi:10.1056/NEJMoa032792
17. Ichinose Y, Genka K, Koike T, et al. Randomized double-blind placebo-controlled trial of bestatin in patients with resected stage I squamous-cell lung carcinoma. J Natl Cancer Inst. 2003;95(8):605–610. doi:10.1093/jnci/95.8.605
18. Hasegawa Y, Ando M, Maemondo M, et al. The role of smoking status on the progression-free survival of non-small cell lung cancer patients harboring activating epidermal growth factor receptor (EGFR) mutations receiving first-line EGFR tyrosine kinase inhibitor versus platinum doublet chemotherapy: a meta-analysis of prospective randomized trials. Oncologist. 2015;20(3):307–315. doi:10.1634/theoncologist.2014-0285
19. Yue D, Xu S, Wang Q, et al. Erlotinib versus vinorelbine plus cisplatin as adjuvant therapy in Chinese patients with stage IIIA EGFR mutation-positive non-small-cell lung cancer (EVAN): a randomised, open-label, phase 2 trial. Lancet Respir Med. 2018;6:863–873. doi:10.1016/S2213-2600(18)30277-7
20. Zhong WZ, Wang Q, Mao WM, et al. Gefitinib versus vinorelbine plus cisplatin as adjuvant treatment for stage II-IIIA (N1-N2) EGFR-mutant NSCLC (ADJUVANT/CTONG1104): a randomised, open-label, phase 3 study. Lancet Oncol. 2018;19(1):139–148. doi:10.1016/S1470-2045(17)30729-5
21. Zhong W-Z, Wang Q, Mao W-M, et al. Gefitinib versus vinorelbine plus cisplatin as adjuvant treatment for stage II-IIIa (N1-N2) EGFR-mutant NSCLC: final overall survival analysis of CTONG1104 phase III trial. J Clin Oncol. 2021;39(7):713–722. doi:10.1200/JCO.20.01820
22. He J, Su C, Liang W, et al. Icotinib versus chemotherapy as adjuvant treatment for stage II-IIIA EGFR-mutant non-small-cell lung cancer (EVIDENCE): a randomised, open-label, phase 3 trial. Lancet Respir Med. 2021;Sep(9):1021–1029.
23. Tada H, Mitsudomi T, Misumi T, et al. Randomized Phase III study of gefitinib versus cisplatin plus vinorelbine for patients with resected stage II-IIIA non-small-cell lung cancer with EGFR mutation (IMPACT). J Clin Oncol. 2021;40:JCO2101729.
24. Ng TL, Camidge DR. Lung cancer’s real adjuvant EGFR targeted therapy questions. Lancet Oncol. 2018;19(1):15–17.
25. Wu Y, Tsuboi M, He J, et al. Osimertinib in resected EGFR-mutated non-small-cell lung cancer. NEJM. 2020;383(18):1711–1723.
26. Gyawali B, West H. Lessons from ADAURA on adjuvant cancer drug trials: evidence, ethics, and economics. J Clin Oncol. 2021;39(3):175–177.
27. Uprety D. Osimertinib should not yet be considered the standard of care for EGFR-mutant NSCLC in the adjuvant setting. J Thorac Oncol. 2021;16(3):371–374.
28. Wu YL, John T, Grohe C, et al. Postoperative chemotherapy use and outcomes from ADAURA: osimertinib as adjuvant therapy for resected EGFR-Mutated NSCLC. J Thorac Oncol. 2021;17(3):423–433.
29. Shepherd FA, Lacas B, Le Teuff G, et al. Pooled analysis of the prognostic and predictive effects of TP53 comutation status combined with KRAS or EGFR mutation in early-stage resected non-small-cell lung cancer in four trials of adjuvant chemotherapy. J Clin Oncol. 2017;35(18):2018–2027.
30. Liu SY, Bao H, Wang Q, et al. Genomic signatures define three subtypes of EGFR-mutant stage II-III non-small-cell lung cancer with distinct adjuvant therapy outcomes. Nat Commun. 2021;12(1):6450.
31. Koch AL, Vellanki PJ, Drezner N, et al. FDA approval summary: osimertinib for adjuvant treatment of surgically resected non-small cell lung cancer, a collaborative project orbis review. Clin Cancer Res. 2021;27(24):6638–6643.
32. Katz A, Saad ED. CALGB 9633: an underpowered trial with a methodologically questionable conclusion. J Clin Oncol. 2009;27(13):2300–2301.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.