")
Back to Journals » Clinical Optometry » Volume 15
Decision Behavior and Influential Factors of Spectacle Prescription for Schoolchildren in Taiwan
Authors Huang CY , Chen CM, Chang CK
Received 6 June 2023
Accepted for publication 27 July 2023
Published 2 August 2023 Volume 2023:15 Pages 159—166
DOI https://doi.org/10.2147/OPTO.S424678
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Mr Simon Berry
Ching Yao Huang,1 Chih Ming Chen,1 Chao Kai Chang1,2
1Department of Optometry, Da-Yeh University, Changhua, Taiwan; 2Nobel Eye Institute, Taipei, Taiwan
Correspondence: Chao Kai Chang, Nobel Eye Institute, Taipei, 100008, Taiwan, Tel +886-4-7232105 Ext 3222, Email [email protected]
Purpose: The prevalence of children myopia in Taiwan is among the highest in the world. The study aimed to understand the status of the final prescription of the spectacle prescribed by the Taiwan optometrists when they conducted the visual inspection of elementary school, middle school and high school students, and to evaluate the influencing factors of their decision-making behavior.
Methods: Among the attendants of the continuing education course activities held by optometrist associations in Taiwan, an anonymous questionnaire survey was given on the spot to optometrists who have passed the national examination. This study received 442 questionnaire surveys, including 174 optometrists and 268 assistant optometrists. The data were analyzed by using chi-square test in IBM SPSS.
Results: There are statistically significant differences in the decision-making of spectacle prescription for myopia of − 1.00D~− 1.50D and − 2.25D~− 2.50D in the primary school stage between optometrists and assistant optometrists. There are also significant differences for myopia of − 2.25D and above in the middle school students. By the time of high school, there are significant differences for myopia from − 0.75D to − 3.25D and above. The higher the grade, the greater the difference in the final prescription of the spectacles given. As for the judgment factors of the final prescription, only children among elementary school and junior high school show a statistically significant difference in professional judgment between optometrists and assistant optometrists. There is no significant difference in the judgment factors for high school children. Depending on the educational level of optometrists and assistant optometrists and their distribution area, the prescription decisions are also different.
Conclusion: The optometrists prefer to prescribe full correction for schoolchildren, while the assistant optometrists mostly prescribe under-correction in prescriptions for low-degree myopia and lower grades. Further investigation is needed to study its impact on children’s visual health.
Keywords: children myopia, optometrists, assistant optometrists, prescription
Introduction
Taiwan has one of the highest myopia prevalence in the world, especially for children, where the weighted prevalence is 25.41% for 7-year-olds and to 76.67% for 12-year-olds,1 Once myopia starts in children and teenagers, it is difficult to control from getting worse. The continuous increase in myopia not only causes inconvenience in daily life but also leads to complications in the future. Recent evidence-based studies have also confirmed that the time spent outdoors is a crucial protective factor in delaying the onset of myopia.2
The prevalence of myopia among young people is rising globally, particularly among 6 to 10-year-olds who experience an average yearly increase of −1.00D to −1.25D.This increase is likely due to the widespread use of technology such as smartphones and prolonged screen viewing, which causes eye strain and increases the likelihood of vision problems and myopia.3,4
In Taiwan, some ophthalmologists advocate for the use of atropine, with 60% of Taiwanese children using it.5 Treatment by pediatric ophthalmologists can reduce the progression of myopia, with multiple interventions reducing its development. Atropine 0.01% is reportedly the most popular and safe treatment.6 Many methods exist to correct myopia, but their efficacy varies. Studies have shown that the daily use of DIMS lenses can significantly delay the progression and axial growth of myopic children, while only 7.4% of children with SV lenses had no myopia progression in 2 years.7 Preventing the worsening of myopia in school-aged children and finding effective ways to control it are valuable research topics.6,8
A recent survey of 940 global ophthalmologists found that 8.2% prescribe under-correction for myopia as a control strategy.6 The study aimed to understand the status of the final prescription of the spectacle prescribed by the Taiwan optometrists when they conducted the visual inspection of elementary school, middle school and high school students, and to evaluate the influencing factors of their decision-making behavior.
Methods
This study surveyed qualified optometrists and assistant optometrists in the country through a questionnaire. Participants were included if they passed the national exam and excluded if they did not. The original plan was to conduct 1600 surveys, but due to the COVID-19 pandemic, the number was reduced to 442, with 174 from optometrists and 268 from assistant optometrists.
The questionnaire included professional judgment on lens prescription for primary, junior high, and high school students who were diagnosed with myopia by ophthalmologists. It also asked about prescription options, including full correction, under-correction (reducing spherical or cylindrical), prescription differences, and factors affecting decision-making (initial wearing, distance demand, parent request, and professional judgment).
The questionnaire was reviewed and revised by three expert scholars for relevance, accuracy, and suitability. The study was approved by the regional ethics committee of China Medical University. We confirm that all participants had provided informed consent. The collected surveys were analyzed using Student’s t-test and chi-square test to determine the association between optometrists’ decision-making and prescription differences for different levels of students and the factors affecting their decisions. Statistical significance was considered as a P-value < 0.05.
Results
The characteristics of the participants are summarized in Table 1.Optometrists with mean (SD) age of 41.14(10.01) years and assistant optometrists with mean (SD) age of 43.11(10.06) years, the difference was statistically significant (P =0.002).The proportion of males to females among the 174 optometrists is 118 (67.8%) to 56 (32.2%) respectively. Among the 268 assistant optometrists, the proportion of males to females is 154 (57.5%) to 114 (42.5%) respectively. Both groups show a similar trend with a higher proportion of males compared to females. Comparing the rates of gender between optometrists and assistant optometrists revealed a significant difference (P=0.029) (Table 1).
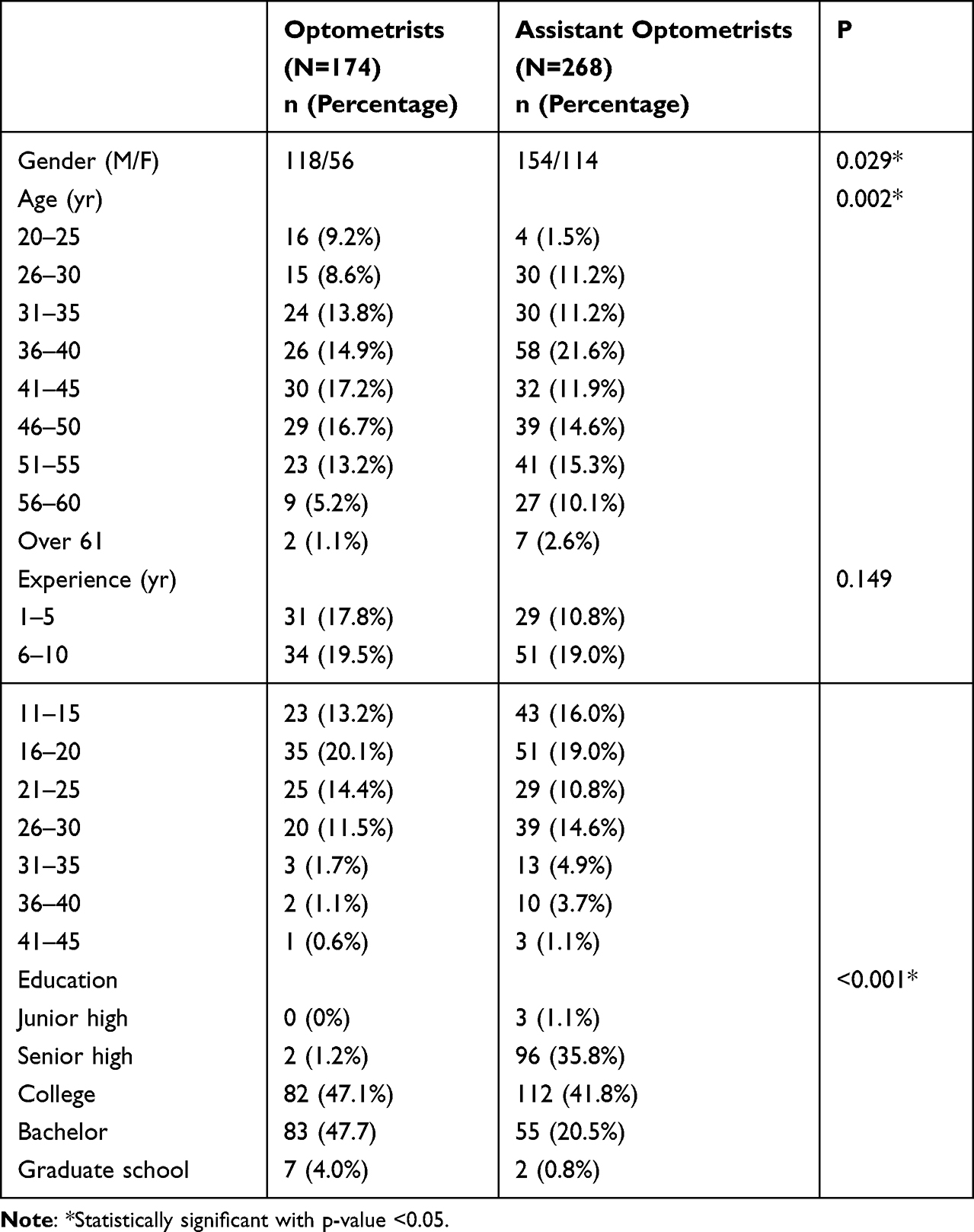 |
Table 1 Demographics of Optometrists and Assistant Optometrists |
The professional judgement data analysis of optometrists and assistant optometrists on the disposal of final lens prescription obtained after examining elementary school children is shown in Table 2. There is a statistically significant difference in the choice of full correction lens or under-correction lens between the two groups, with optometrists tending to choose full correction lenses and assistant optometrists tending to choose under-correction lenses, particularly in the cases of myopia of −1.00~−1.50D (P=0.004) and myopia of −2.25D~−2.50D (P=0.05) (Table 2).
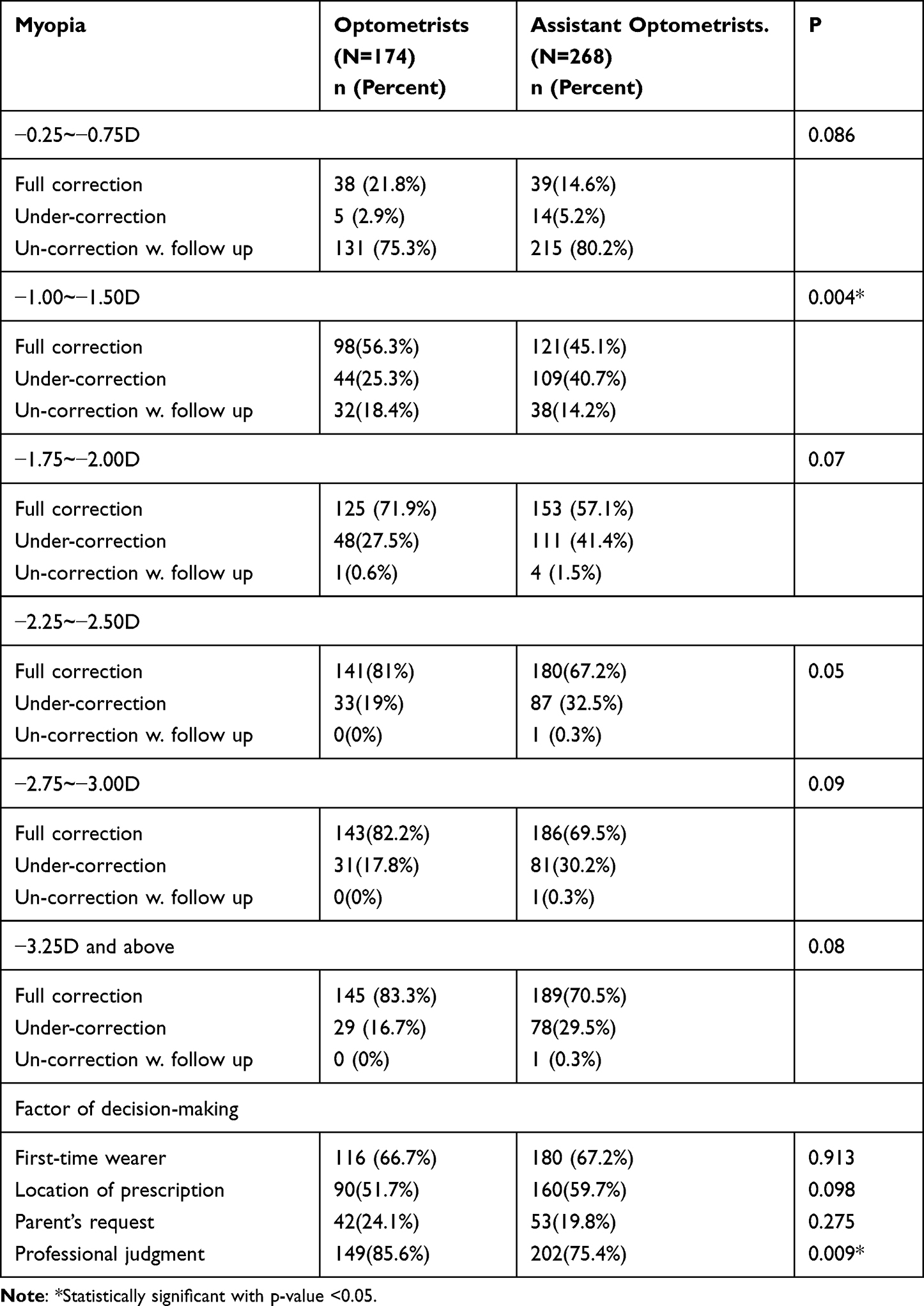 |
Table 2 Comparison of Decision Making on Elementary School Students |
The statistical analysis of the professional judgement data on how to dispose the final prescription for glasses after examining Junior high school students, as shown in Table 3, reveals significant differences in prescription levels −2.25 to −2.50D (P=0.017), −2.75 to −3.00D (P=0.005), and −3.25D or higher (P=0.01). Optometrists tend to choose full correction glasses more frequently than assistant optometrists, who choose under-correction glasses more frequently.
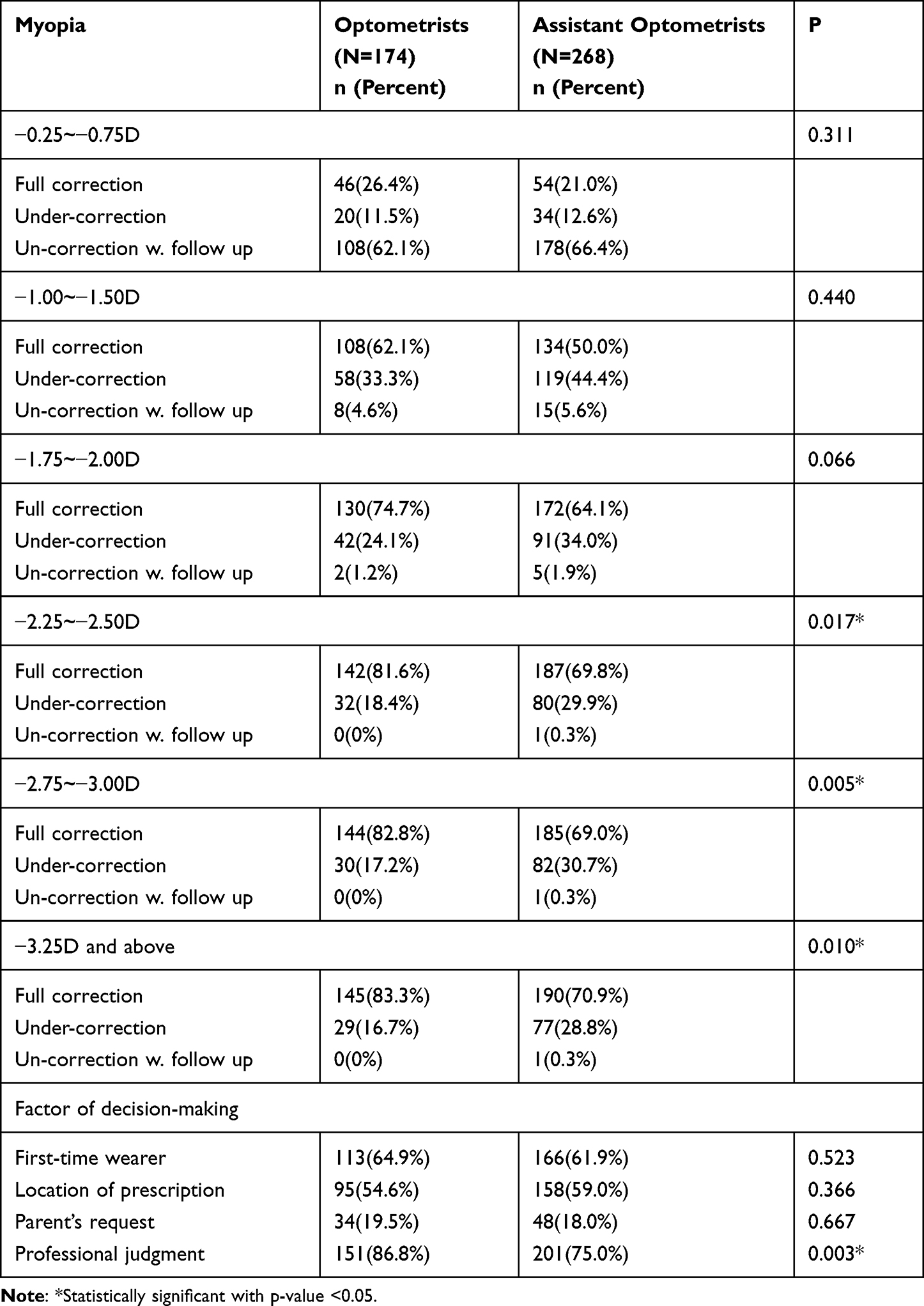 |
Table 3 Comparison of Decision Making on Junior High School Students |
After checking the high school students’ vision, the results showed that optometrists prescribe full correction lenses more often than assistant optometrists regardless of the degree of myopia, while assistant optometrists prescribe under-correction lenses more often than optometrists with a statistically significant difference (all P<0.05) (Table 4).
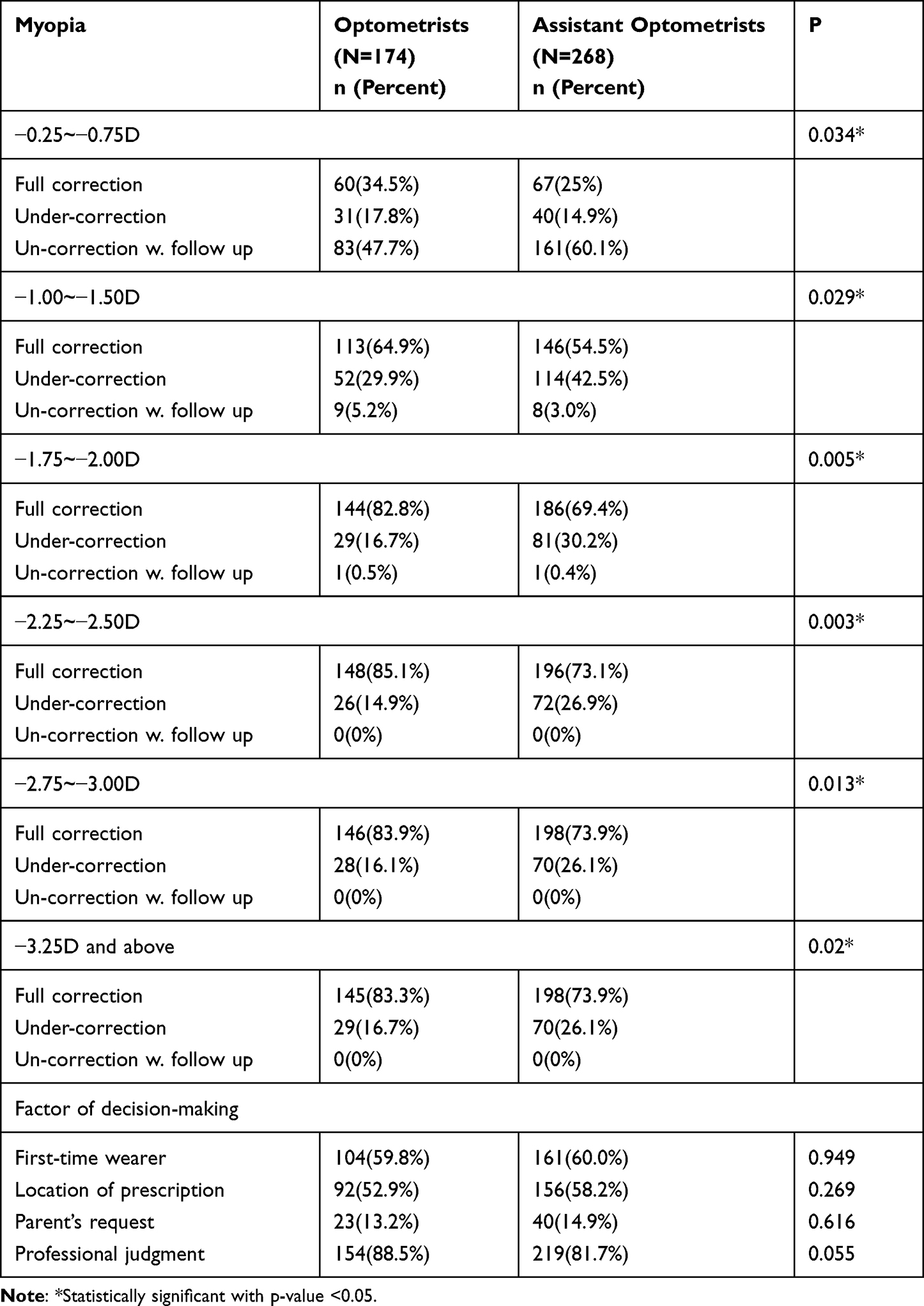 |
Table 4 Comparison of Decision Making on Senior High School Students |
The optometrists and assistant optometrists both show similar opinions statistically in their assessment of under-correction with correction primarily based on reduction in spherical diopter (−0.25D, −0.50D, −0.75D) and under-correction with correction primarily based on reduction in cylindrical diopter (−0.25D, −0.50D, −0.75D) (Table 5).
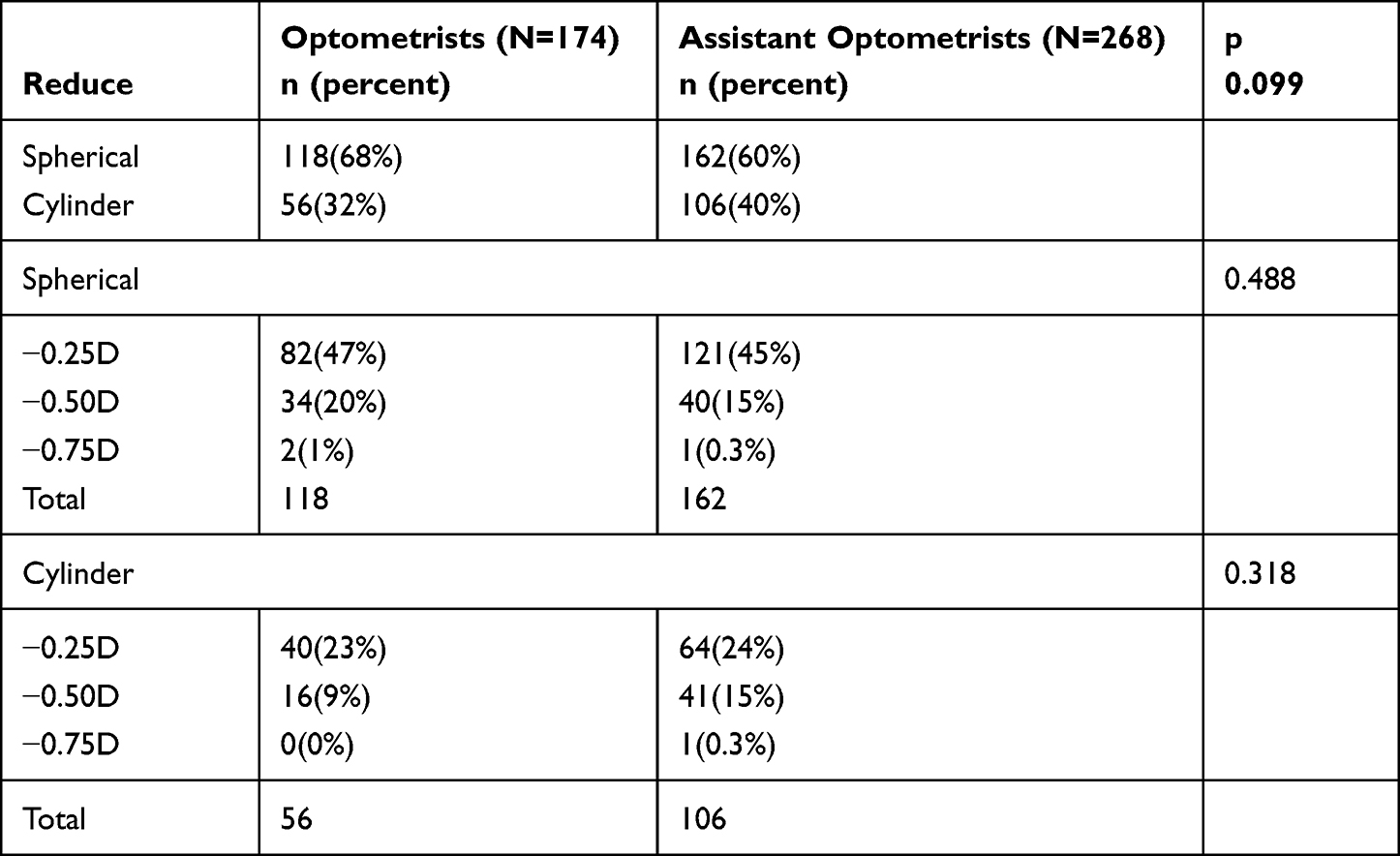 |
Table 5 Clinical Characteristics of Under-Correction |
Discussion
Research has demonstrated that children’s exposure to outdoor environments can reduce the incidence of myopia, without the need for physical activity. Simply being outside the classroom has a preventive effect.9 Outdoor activities can slow axial elongation and lower the risk of myopia.10 Outdoor activities are one of the most important environmental factors in controlling myopia.
Torii et al reported that violet light (VL, with a wavelength of 360–400nm) can suppress the progression of myopia.11 Hua et al aimed to determine if higher light levels in rural classroom can protect school-aged children from myopia or its progression by examining 1713 students aged 6–14 from four schools in Northeast region, with 317 participants in the study. The study found that improving the median illuminance of blackboards and desks, as well as desk lighting uniformity, reduced the incidence of new myopia onset by 4% compared to 10% in the control group (p=0.029). The results showed that elevated light levels in classrooms have a significant impact on myopia onset, refraction, and axial growth.12
Many factors contribute to the cause of myopia and its progression, including close-up work,13 Lack of outdoor activities,14 Asian,15 high education, Parents with myopia, low Serum 25-Hydroxyvitamin D,16 even allergic conjunctivitis.17
Taiwan has been proven to be one of the countries with the highest rates of myopia in the world. Most elementary students spend more than 12 hours a day on homework and learning skills to cope with the intense academic pressure. Compared to other regions, this prolonged near-distance visual work may be a significant factor contributing to the high incidence of myopia among Taiwanese students.18 Preventing the development of high myopia during childhood to reduce the impact and inconvenience on quality of life and decrease the incidence of myopia complications is the primary goal in controlling its progression.
Conclusions
Optometrists primarily prescribe full correction for school-aged children. Assistant optometrists tend to prescribe under correction for low degree myopia and for lower grades. Additionally, collecting more parameters, such as presence of anisometropia, for the final decision-making on eyeglass prescription, could provide more conclusive results. Further studies are needed to evaluate the impact on visual health caused by the difference in the choice between optometrists and assistant optometrists.
Ethical Declarations
Ethical approval: IRB: CRREC-108-137
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tsai TH, Liu YL, Ma IH, et al. Evolution of the prevalence of myopia among Taiwanese schoolchildren: a review of survey data from 1983 through 2017. Ophthalmology. 2021;128(2):290–301. PMID: 32679159. doi:10.1016/j.ophtha.2020.07.017
2. French AN, Ashby RS, Morgan IG, Rose KA. Time outdoors and the prevention of myopia. Exp Eye Res. 2013;114:58–68. doi:10.1016/j.exer.2013.04.018
3. Wang J, Li M, Zhu D, Cao Y. Smartphone overuse and visual impairment in children and young adults: systematic review and meta-analysis. J Med Internet Res. 2020;22(12):e21923. doi:10.2196/21923
4. Alvarez-Peregrina C, Sánchez-Tena MÁ, Martinez-Perez C, Villa-Collar C. The relationship between screen and outdoor time with rates of Myopia in Spanish children. Front Public Health. 2020;8:560378. doi:10.3389/fpubh.2020.560378
5. Fang YT, Chou YJ, Pu C, et al. Prescription of atropine eye drops among children diagnosed with myopia in Taiwan from 2000 to 2007: a nationwide study. Eye. 2013;27(3):418–424. doi:10.1038/eye.2012.279
6. Zloto O, Wygnanski-Jaffe T, Farzavandi SK, Gomez-de-Liaño R, Sprunger DT, Mezer E. Current trends among pediatric ophthalmologists to decrease myopia progression-an international perspective. Albrecht Von Graefes Arch Klin Exp Ophthalmol. 2018;256(12):2457–2466. doi:10.1007/s00417-018-4078-6
7. Lam CSY, Tang WC, Tse DY, et al. Defocus Incorporated Multiple Segments (DIMS) spectacle lenses slow myopia progression: a 2-year randomised clinical trial. Br J Ophthalmol. 2020;104(3):363–368. doi:10.1136/bjophthalmol-2018-313739
8. Mak CY, Yam JC, Chen LJ, Lee SM, Young AL. Epidemiology of myopia and prevention of myopia progression in children in East Asia: a review. Hong Kong Med J. 2018;24(6):602–609. doi:10.12809/hkmj187513
9. He M, Xiang F, Zeng Y, et al. Effect of time spent outdoors at school on the development of Myopia among children in china: a randomized clinical trial. JAMA. 2015;314(11):1142–1148. doi:10.1001/jama.2015.10803
10. Cao K, Wan Y, Yusufu M, Wang N. Significance of outdoor time for myopia prevention: a systematic review and meta-analysis based on randomized controlled trials. Ophthalmic Res. 2020;63(2):97–105. doi:10.1159/000501937
11. Torii H, Kurihara T, Seko Y, et al. Violet light exposure can be a preventive strategy against myopia progression. EBioMedicine. 2017;15:210–219. doi:10.1016/j.ebiom.2016.12.007
12. Hua WJ, Jin JX, Wu XY, et al. Elevated light levels in schools have a protective effect on myopia. Ophthalmic Physiol Opt. 2015;35(3):252–262. doi:10.1111/opo.12207
13. Lin Z, Gao TY, Vasudevan B, et al. Near work, outdoor activity, and myopia in children in rural China: the Handan offspring myopia study. BMC Ophthalmol. 2017;17(1):203. doi:10.1186/s12886-017-0598-9
14. Yang M, Luensmann D, Fonn D, et al. Myopia prevalence in Canadian school children: a pilot study. Eye. 2018;32(6):1042–1047. doi:10.1038/s41433-018-0015-5
15. Theophanous C, Modjtahedi BS, Batech M, Marlin DS, Luong TQ, Fong DS. Myopia prevalence and risk factors in children. Clin Ophthalmol. 2018;12:1581–1587. doi:10.2147/OPTH.S164641
16. Choi JA, Han K, Park YM, La TY. Low serum 25-hydroxyvitamin D is associated with myopia in Korean adolescents. Invest Ophthalmol Vis Sci. 2014;55(4):2041–2047. doi:10.1167/IOVS.13-12853
17. Wei CC, Kung YJ, Chen CS, et al. Allergic conjunctivitis-induced retinal inflammation promotes Myopia progression. EBioMedicine. 2018;28:274–286. doi:10.1016/j.ebiom.2018.01.024
18. Lin LL, Shih YF, Hsiao CK, Chen CJ. Prevalence of myopia in Taiwanese schoolchildren: 1983 to 2000. Ann Acad Med Singapore. 2004;33(1):27–33.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.