")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 17
Death Caused by Disseminated Herpes Zoster in a Patient with Multiple Myeloma: A Case Report and Literature Review
Authors Bo Y, Zhong X , Xiang Y, Ren Q, Hao P
Received 15 February 2024
Accepted for publication 22 April 2024
Published 27 April 2024 Volume 2024:17 Pages 941—951
DOI https://doi.org/10.2147/CCID.S464039
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Rungsima Wanitphakdeedecha
Yang Bo, Xiaojing Zhong, Yanping Xiang, Qingjun Ren, Pingsheng Hao
Department of Dermatology, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China
Correspondence: Pingsheng Hao, Department of Dermatology, Hospital of Chengdu University of Traditional Chinese Medicine, 39 Shi-Er-Qiao Road, Jinniu District, Chengdu, Sichuan, 610072, People’s Republic of China, Tel +86138 8196 5024, Fax +86-28-87732407, Email [email protected]
Abstract: We report a fatal case of disseminated herpes zoster in a patient with multiple myeloma, illustrating the severe risks immunocompromised individuals face from viral infections. By combining a detailed case report with an extensive literature review, the paper seeks to shed light on the underlying susceptibility factors for varicella-zoster virus infection in multiple myeloma patients. We further evaluate effective prophylactic protocols for herpes zoster, aiming to equip clinicians with improved therapeutic strategies. The case underscores the critical need for vigilant clinical assessments and tailored patient management to mitigate infection risks and enhance patient outcomes.
Keywords: multiple myeloma, disseminated herpes zoster, antiviral prophylaxis, immunodeficiency
Introduction
Herpes zoster (HZ) is an acute infectious skin disease caused by reactivation of varicella zoster virus (VZV) latent in the ganglia. Lesions of HZ are usually confined to a single dermatomal area, and non-adjacent HZ involving two or more dermatomes is rare. Disseminated herpes zoster (DHZ) is termed when more than two contiguous zones are affected or when more than 20 or more varicella-like rashes or visceral involvement are observed outside the initial zone.1 Multiple myeloma (MM) is a malignant disease of the haematological system, in which the clonal proliferation of plasma cells in the bone marrow produces large amounts of aberrant monoclonal immunoglobulins, which inhibit normal immunoglobulin synthesis, leading to reduced immune function, and MM cells act on the bone marrow microenvironment, which further contributes to the patient’s immunocompetence, leading to herpes zoster.2,3 In individuals with MM, the sustained use of antineoplastic agents, including immunosuppressives and proteasome inhibitors, leads to the suppression of both humoral and cellular immune responses. This immunosuppression significantly increases the risk of herpes zoster, with an incidence rate that is 14.8 times higher than that of the general population.4 Here, we report a case of multiple myeloma patient complicated with disseminated herpes zoster resulting in death. We hope to review this case to analyse the susceptibility factors for VZV infection in MM patients, as well as to summarise effective prophylactic protocols for herpes zoster in patients with multiple myeloma through an extensive review of the literature, with a view to providing clinicians with better therapeutic strategies.
Case Presentation
A 58-year-old Chinese male presented to the hospital on 23 May 2023 with a week-long history of erythematous blisters accompanied by pruritus and pain localized to the right inner thigh and buttock. Initially characterized by clustered papules and vesicles, the lesions evolved rapidly, and some of the blisters broke and oozed. Within a day post-admission, a generalized blister-like rash ensued, marked by widespread itching. The patient was in poor physical condition and suffered from hypertension for 10 years. On 25 October 2021, he was hospitalized in other hospital because of oedema of both lower limbs and foamy urine. The biochemical profile was revealing, with albumin at 23.1g/L, globulin at 16.8g/L, creatinine at 190 umol/L, an estimated glomerular filtration rate (eGFR) of 33.21 mL/min/1.73m², triglycerides at 3.03 mmol/L, and a concerning 24-hour urine protein excretion of 4.54g, pointing towards nephrotic syndrome and stage 3 chronic kidney disease. Further investigations, including a renal biopsy conducted on October 28, 2021, revealed amyloid renal degeneration. A subsequent bone marrow biopsy on November 3, 2021, confirmed the presence of multiple myeloma. The patient embarked on a rigorous therapeutic regimen, encompassing bortezomib (2.5mg weekly), dexamethasone (15mg twice weekly), and cyclophosphamide (four tablets twice weekly) for seven cycles, alongside seven sessions of bedside dialysis, culminating in a stem cell transplantation in September 2022. However, the post-chemotherapy trajectory was fraught with myelosuppression, manifesting as anemia, thrombocytopenia, and granulocytopenia, and marred by recurrent hospital admissions due to pulmonary infections. These clinical episodes were meticulously cataloged as severe pneumonia, hypoxemia, stage 5 chronic kidney disease, hemodialysis reliance, compounded by the underlying specters of multiple myeloma, renal amyloidosis, leukopenia, thrombocytopenia, and coagulation dysfunction. Remarkably, the patient did not receive prophylactic treatment for VZV infection. The patient negated any history of infectious diseases or drug allergies. Upon physical examination, vital signs remained stable, and systemic scrutiny revealed no notable anomalies. Dermatological evaluation disclosed a clustered arrangement of corn-grain-sized red macules, papules, and blisters on the right inner thigh and buttocks, circumscribed by a basal red halo, with mild tenderness upon palpation. Additionally, over 20 dispersed blisters, ranging from mung bean to soybean in size, were observed across the bilateral forearms, trunk, and left lower limb, as depicted in Figure 1.
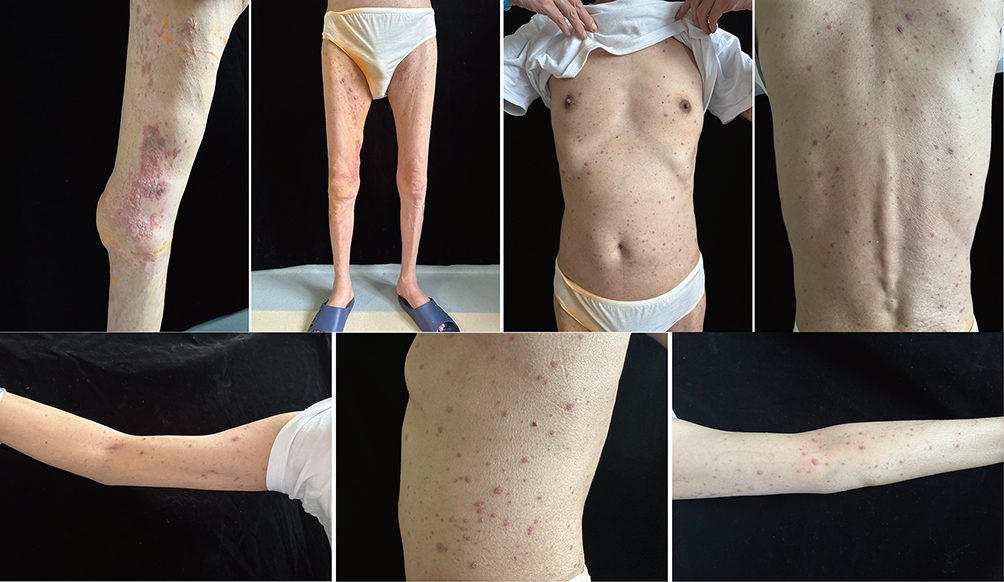 |
Figure 1 The patient develops a blister-like rash all over the body with widespread itching. |
Laboratory investigations revealed the following hematological and immunological profiles: The white blood cell count was elevated at 9.82 × 10^9/L, with a predominance of neutrophils (8.64 × 10^9/L) and a diminished lymphocyte count (0.7 × 10^9/L). Red blood cell metrics indicated a count of 3.63 × 10^12/L with a hemoglobin concentration of 120g/L. Inflammatory indices revealed a pronounced elevation in whole blood C-reactive protein, registering at 38.73 mg/L—remarkably above the normal range of 0–5 mg/L, signifying a marked inflammatory response. Renal function tests highlighted compromised kidney function, with urea at 46.48mmol/L and creatinine significantly elevated at 324.4 μmol/L. Assessment of cellular immunity displayed an altered profile: the helper/inducible T lymphocyte percentage stood at 18.35%, whereas the inhibitory/cytotoxic T lymphocyte percentage was 43.52%. The CD4+/CD8+ ratio was notably reduced at 0.42%. Natural killer cell activity was represented by a percentage of 36.7%, and B lymphocyte percentage was critically low at 0.47%. Quantitative T lymphocyte evaluations revealed a total count of 421/uL, with helper/inducible T lymphocytes at 124/uL and B lymphocytes at 3/uL. Screening for syphilis and the AIDS virus returned negative results. As shown in Figure 2, a biopsy conducted on the abdominal lesions revealed intraepidermal vesicle formation. Within these vesicles, degenerated and loosely arranged spindled cells were observed, a histopathological hallmark consistent with herpes zoster. Consequently, the diagnosis was established as disseminated herpes zoster.
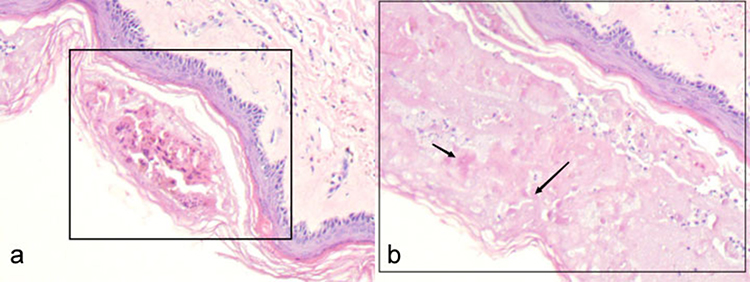 |
Figure 2 Histopathologic images of the patient’s skin lesions (HE × 100). (a) Microscopic evaluation revealed the presence of blister-like formations beneath the stratum corneum, characterized by the presence of loosened spinous cells. There was a mild disintegration observed at the base of these structures, coupled with a discernible lymphocytic infiltration encircling the periphery. (b) Disintegration of blisters and balloon-like degeneration of cells with a little inflammatory cell infiltration are seen under the stratum corneum. The arrows in the figure indicate cellular balloon-like degeneration. |
The patient was administered valacyclovir hydrochloride tablets for antiviral therapy, pregabalin for analgesia, and methylcobalamin tablets for nerve nutrition, alongside other symptomatic supportive measures. On 28 May, the patient experienced intermittent fever, with temperatures ranging from 36.3°C to 39°C. Laboratory investigations indicated elevated white blood cell count (WBC: 12.47 × 10^9/L), granulocytes (GRAN: 11.6 × 10^9/L), reduced lymphocytes (LYMPH: 0.5 × 10^9/L), increased C-reactive protein (CRP: 80.43mg/L), and procalcitonin (PCT: 0.45ng/mL). Injectable vancomycin hydrochloride was administered for anti-infective therapy. Subsequently, the patient experienced recurrent high fevers, with PCT levels exceeding 50ng/mL. Auxiliary examinations on 5 June revealed: fungal D-glucan at 932.62pg/mL, thrombocytopenia (platelet count: 42 × 10^9/L), elevated interleukin-6 (5448.44pg/mL), PCT (>50ng/mL), CRP (293.87mg/L), high-sensitivity troponin (0.182ng/mL), and brain natriuretic peptide (BNP: 18056.7pg/mL). Chest CT imaging indicated multiple infectious foci within both lungs, predominantly in the left lung. The patient subsequently suffered an acute myocardial infarction and acute heart failure, necessitating emergency coronary angiography. On 11 June, gastrointestinal bleeding and purpura emerged, managed with blood transfusions and symptomatic care. Other detailed findings of this patient are shown in Tables 1 and 2. Throughout this period, a comprehensive anti-infective regimen was employed, including piperacillin-tazobactam, ganciclovir, meropenem, minocycline, azithromycin, sulfamethoxazole, polymyxin B, amphotericin B, fluconazole, voriconazole, tigecycline, omadacycline, and ceftazidime-avibactam, alongside imipenem-cilastatin. The patient’s condition deteriorated, leading to respiratory and cardiac arrest on 7 July. Electrocardiography displayed an isoelectric line, culminating in clinical death. The primary cause of death was identified as septic shock due to carbapenem-resistant Klebsiella pneumoniae septicaemia, compounded by multi-organ infections, including carbapenem-resistant Klebsiella pneumoniae, Acinetobacter baumannii pneumonia, fungal infections (Aspergillus fumigatus, Candida albicans), viral pneumonia, and severe acute respiratory distress syndrome, leading to respiratory and cardiac failure on 7 July.
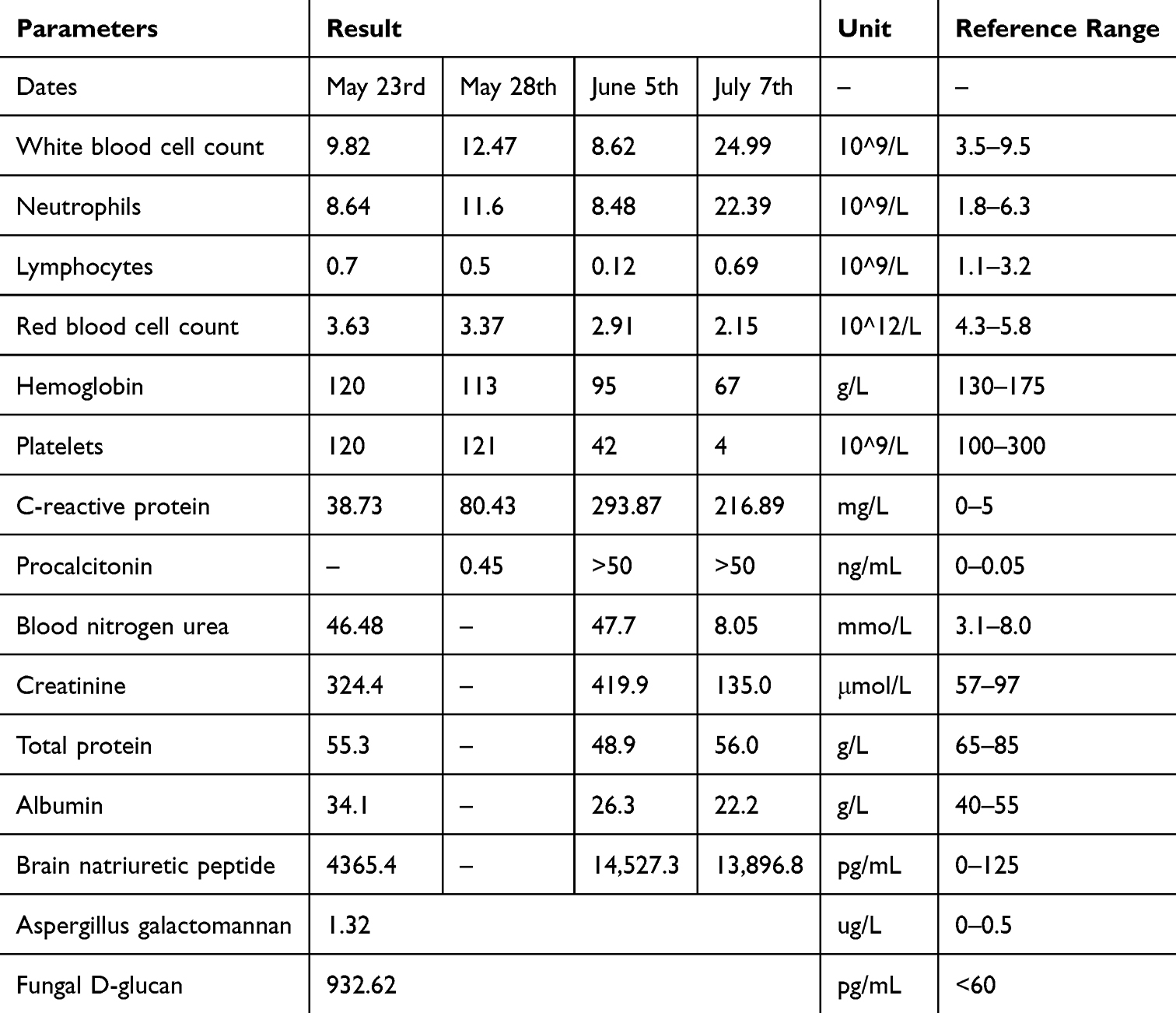 |
Table 1 Results of the Patient’s Blood Tests |
 |
Table 2 Laboratory Test Results in the Patient |
Discussion
Disseminated herpes zoster, a clinical rarity, predominantly afflicts the elderly, the frail, individuals with malignancies, those suffering from acquired immunodeficiency syndromes, and patients subjected to prolonged regimes of immunosuppressants or glucocorticoids. Particularly vulnerable are patients with malignant hematological disorders, whose compromised immunological status—stemming from the disorder itself or from factors like extensive chemotherapy and transplantation—renders them prone to opportunistic infections.5,6 Such infections include HZ, triggered by the reactivation of the VZV. In the context of MM, the incidence of herpes zoster escalates, a consequence of dysfunctional plasma cell activity, weakened host defenses, and the chronic administration of immunosuppressants and proteasome inhibitors. These agents collectively dampen both humoral and cellular immune responses. The susceptibility of MM patients to infections is multifaceted, involving deteriorating host defenses due to disease progression—characterized by agranulocytosis, T-cell immunodeficiency, hypogammaglobulinemia, advanced age, renal failure—and the immunosuppressive impact of prolonged steroid use and previous treatments leading to reductions in CD4+, CD45+, CD19+ cells, and natural killer (NK) cells.7–9 Empirical evidence from numerous studies underscores the significance of pretreatment lymphopenia, the administration of bortezomib or cyclophosphamide, and the absence of prophylactic antiviral therapy as pivotal risk factors for the emergence of herpes zoster in MM patients.10,11 These findings illuminate the intricate interplay between disease-induced immunodeficiency, therapeutic interventions, and the heightened risk of opportunistic infections within this patient demographic.
In this case study, we examine an elderly male patient with renal failure and hypoproteinemia, who is in a post-stem cell transplantation state. The patient’s chemotherapy regimen, complicated by chemotherapeutic drug toxicity, resulted in myelosuppression. Laboratory results revealed impaired cellular immunity, characterized by low percentages of helper/inducer T lymphocytes (18.35%), suppressor/cytotoxic T lymphocytes (43.52%), a reduced CD4+/CD8+ ratio (0.42), alongside diminished natural killer cells (36.7%) and B lymphocytes (0.47%). The significantly lowered lymphocyte count and CD4+/CD8+ ratio indicate severely compromised immune function. The relationship between herpes zoster occurrence and CD4+ T lymphocyte subsets is well-documented, with opportunistic infection rates escalating markedly below a CD4+ T lymphocyte threshold of 200/μL.12 Several studies have been conducted on lymphocyte subsets in MM patients. Dosani T et al found that the percentage of peripheral blood B-lymphocytes decreased in MM patients as the disease progressed.13 Suen H et al’s research in the context of MM patients reveals a progression-dependent decrease in peripheral blood B-lymphocytes and an altered immune profile characterized by reduced cytotoxic T-cell proliferation, diminished Th17 cell levels, and an increase in regulatory T-cells.14 The findings of Trotta R. et al and Blimark et al further underscore the immune dysregulation in MM, highlighting decreased numbers of NK cells and impaired expression of surface-activated receptors.4,15 This dysregulation, coupled with an imbalance in CD4+/CD8+ ratios and deficiencies in natural killer and dendritic cells, disrupts the immune microenvironment, complicating infection control. The interplay between immunodeficiency, recurrent infections, drug resistance, and disease progression underscores the critical need for further exploration into the roles of immune deficiencies in MM’s diagnosis, prognosis, prophylactic treatment, and immunotherapeutic mechanisms. Understanding the intricate relationship between peripheral immunity, the tumor microenvironment, and disease progression is essential. This knowledge could enhance the survival and quality of life for MM patients, paving the way for long-term disease-free survival through targeted immunotherapeutic strategies.
Innovative therapies like immunomodulatory drugs (IMiDs), proteasome inhibitors (PIs), and monoclonal antibodies (moAbs) have substantially enhanced the depth of response and clinical outcomes for MM.16 This advancement is illustrated by drugs like pomalidomide, an oral immunomodulator improving the immune response against MM cells, and carfilzomib, a proteasome inhibitor inducing tumor cell death through the accumulation of misfolded proteins. Daratumumab, a monoclonal anti-CD38 antibody, has demonstrated significant efficacy but also poses a higher infection risk, necessitating vigilant antiviral and antibacterial precautions.17 Yarlagadda et al found that the use of high-dose chemotherapy followed by autologous stem cell transplantation (ASCT) in patients with severe daratumumab-refractory MM resulted in long-term control of MM.18 Recent advancements, such as bispecific T cell engagers and BCMA-specific CAR T cell therapies, offer new hope for treatment-resistant MM,19 while Cliff et al emphasise the importance of careful monitoring of infections and adverse events.20 Relapsed/refractory patients often receive multiple lines of therapy and may exhibit significant immunosuppression compared to newly diagnosed MM patients, making the risk of infection even more severe,21 with a prevalence of invasive fungal infections of up to 15.0%,22 suggesting vigilant surveillance and proactive infection prevention strategies for such patients.23 The treatment plan for MM in this patient was bortezomib (2.5mg weekly), dexamethasone (15mg twice weekly), and cyclophosphamide (four tablets twice weekly). Bortezomib, as a proteasome inhibitor officially approved for the treatment of multiple myeloma, functions by stalling tumor cell proliferation, inducing apoptosis, and curbing neovascularization, thereby extending patient survival. However, the heightened susceptibility of MM patients to severe infections under bortezomib treatment has been documented, attributed to its inhibition of the NF-κB signaling pathway. This inhibition results in a diminished presence of Th1 and CD4+ T cells, curtailed T cell proliferation, and compromised cellular immunity. The mechanism extends to impeding the activation, proliferation, and survival of T cells, alongside abnormalities in dendritic and natural killer (NK) cells.10,24–26 The collective impact of antitumor agents and immunosuppressants further undermines the body’s defense mechanisms, facilitating pathogenic invasions. It was found that the incidence of herpes zoster in patients who had previously applied bortezomib-containing drugs was significantly higher than in other patients. The reason for this may be related to the fact that the site of action of bortezomib treatment for MM patients is related to T cell immunity, and impaired T cell immunity can lead to herpes zoster virus infection.24 Research, including studies by Heider et al and Seok et al, underlines the temporal correlation between bortezomib administration and reduced CD4+ T cell counts, with the nadir observed six weeks post-initiation.27,28 This period aligns with heightened vulnerability to herpes zoster, suggesting that bortezomib’s impact on T cell immunity directly influences this risk. Further, the occurrence of herpes zoster predominantly within the initial treatment cycles indicates a minimal relationship with bortezomib’s cumulative dosage. A Phase III pivotal trial emphasized varicella-zoster virus as the most frequent viral infection amidst bortezomib therapy, with a noticeable increase in herpes zoster incidence from 5% to 13% among participants.29 These clinical studies suggest that bortezomib-containing chemotherapy regimens elevate the risk of herpes virus infections in MM patients, significantly impinging upon their quality of life and disrupting standard chemotherapy protocols. This situation necessitates a strategic exploration for viable prophylactic measures against herpes zoster in the context of bortezomib-based chemotherapy for MM. Such preventive strategies must not only retain the therapeutic efficacy of chemotherapy but also prioritize patient safety, ensuring a balanced approach that mitigates infection risk while facilitating uninterrupted treatment trajectories.
The National Comprehensive Cancer Network (NCCN) and the European Myeloma Collaborative Group both advocate for the prophylactic use of acyclovir or valacyclovir against herpes zoster virus in patients undergoing proteasome inhibitor-based therapy. This prophylaxis is advised to extend until six weeks post the discontinuation of the proteasome inhibitor.30 Furthermore, the European Society for Clinical Microbiology and Infectious Diseases (ESCMID) has offered a prophylactic regimen for managing herpes zoster associated with bortezomib treatment, albeit acknowledging the current absence of a consensus on precise prophylactic dosages owing to limited studies.31 Prophylactic administration of antiviral agents like acyclovir, valacyclovir, and famciclovir is recognized for its potential to diminish the incidence of secondary herpes zoster in MM cases.32,33 However, challenges persist regarding the uniformity in the selection, application, and dosing of these antivirals, coupled with concerns over long-term use potentially inducing toxic side effects, including hematological, hepatic, renal, and gastrointestinal toxicities. Notably, suggestions have been made advocating for intermittent or reduced dosages of valaciclovir to prevent herpes zoster effectively in MM patients, thereby enhancing patient compliance and minimizing drug-related toxicities.34,35 The enduring nature of MM maintenance therapy poses a challenge of prolonged treatment durations, necessitating extended prophylactic antiviral therapy. This is particularly critical for MM patients who may already have compromised liver and kidney functions due to their underlying condition, where long-term antiviral use could exacerbate organ damage and increase patient burden. In light of these considerations, we have synthesized experiences from various centers in recent years concerning the prevention of herpes zoster in MM patients, aiming to furnish clinicians with pertinent insights, as detailed in Table 3.
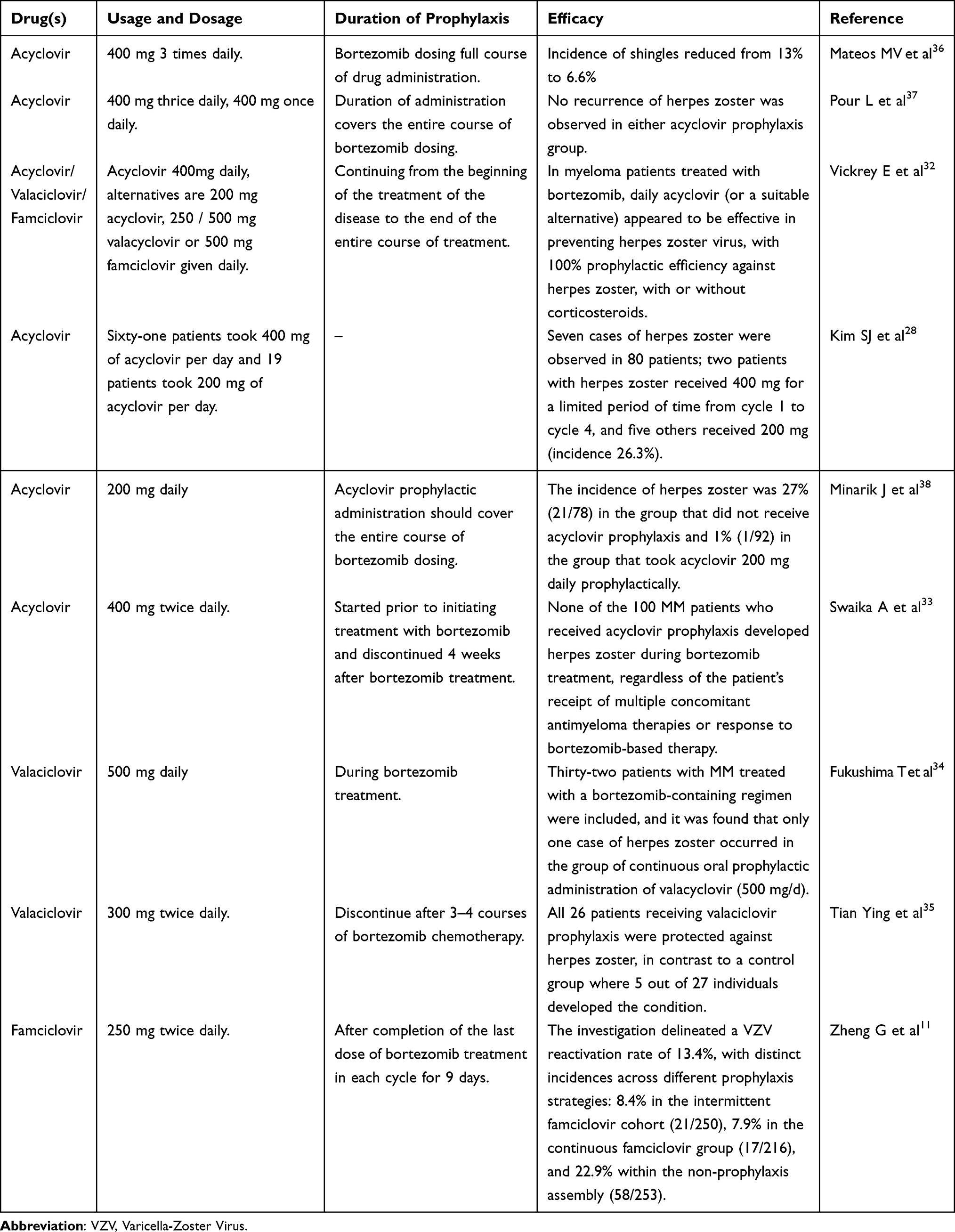 |
Table 3 Prophylactic Medication in Special Situations |
A multicenter retrospective analysis conducted in Spain demonstrated that prophylactic administration of acyclovir significantly mitigates the risk of herpes zoster following bortezomib therapy in MM patients. The study observed a reduction in herpes zoster incidence from 13% to 6.6% with the administration of acyclovir at a dosage of 400 mg three times daily throughout the bortezomib treatment course.36 Concurrently, various other centers have endorsed a daily prophylactic dosage of 400 mg acyclovir as effective.32,37,39 Kim SJ et al posited that 400 mg/day of acyclovir effectively forestalls herpes zoster, whereas a daily dose of 200 mg might prove insufficient for preventing the condition.39 Contrarily, Minarik J et al and Vickrey E et al have presented evidence suggesting that a 200 mg daily dosage of acyclovir can successfully prevent bortezomib-associated herpes zoster, showcasing efficacy comparable to the 400 mg/day regimen.32,38 Additionally, research indicates that valacyclovir, administered at a daily dose of 500 mg, is efficacious in averting viral reactivation.34 Zheng G et al have proposed that intermittent prophylaxis with famciclovir presents a safe and effective strategy for managing herpes zoster, potentially reducing the duration of oral therapy relative to continuous acyclovir prophylaxis, underscoring the importance of tailored prophylactic approaches in enhancing patient care in MM.11 The efficacy of prophylaxis against herpes zoster in MM patients is significantly influenced not only by the dosage but also by the duration of administration. An investigation revealed that subsequent to the discontinuation of acyclovir prophylaxis, instances of herpes zoster reactivation in patients treated with bortezomib were recorded on days 15 and 65 post-acyclovir cessation. This observation underscores the potential for VZV reactivation following the termination of acyclovir therapy, thereby highlighting the critical need for uninterrupted acyclovir prophylaxis. Further supporting this notion, Asano et al observed within the context of haematopoietic stem cell transplantation that patients discontinuing acyclovir prophylaxis exhibited a predisposition towards VZV reactivation.40 Abbasov E et al observed that administering low-dose acyclovir as a prophylactic measure against HZ was both effective and well-tolerated when extended beyond 12 months following autologous stem cell transplantation.41 The ESCMID highlighted the potential for herpes zoster virus reactivation at any phase during bortezomib chemotherapy, advocating for the continuous use of acyclovir throughout the entire bortezomib treatment cycle. This approach was substantiated by the absence of herpes zoster reactivation post-completion of all bortezomib courses, indicating that extending acyclovir administration beyond the chemotherapy period may not be necessary.31 This collective evidence accentuates the importance of maintaining continuous antiviral prophylaxis during bortezomib treatment to mitigate the risk of herpes zoster reactivation, thereby emphasizing the integral role of both dosage and administration duration in the prophylactic strategy against VZV in MM patients.
In addition, the strategic vaccination of MM patients against HZ warrants focused attention. Research has substantiated the efficacy of VZV vaccination in preventing HZ among MM patients. Notably, a comprehensive randomized study involving patients undergoing autologous stem cell transplantation—45% of whom were myeloma patients—demonstrated a marked decrease in VZV reactivation rates, from 21% to 8%, following the administration of four doses of an inactivated VZV vaccine.42 This suggests that inactivated virus vaccination not only offers significant protection in the immediate post-transplant phase but also alleviates the incidence of late-onset herpes zoster and associated complications. Further, an investigation into patients with hematological malignancies, including 132 MM patients undergoing or following immunosuppressive therapy, revealed that 80.2% of vaccinated individuals developed a humoral immune response, in stark contrast to the negligible conversion rate (0.8%) observed in placebo recipients.43 In a large randomized, observer-blinded comparison involving 1846 recipients of autologous stem cell transplants, conducted by Stadtmauer EA et al,44 vaccine efficacy was found to be 72.4% in myeloma patients after two doses of VZV vaccine administered within four months of transplantation. Despite these promising outcomes, consensus on an HZ vaccination strategy specifically tailored for MM patients remains elusive. The immunization protocols applicable to the general populace may not directly translate to the unique needs of this patient cohort. Consequently, there is a pressing need for further research to devise a comprehensive and effective HZ vaccination strategy for individuals with MM, aiming to optimize their protection against VZV reactivation and enhance overall patient care in this vulnerable population.
In recent investigations focusing on newly diagnosed multiple myeloma (NDMM) patients, an array of methodologies including mass spectrometry (MS) technology, immunological analysis, risk scoring, and predictive model development have illuminated novel pathways for therapeutic monitoring and prognostic assessment. Initially, Tew et al underscored the utility of immunological analysis in predicting infection risks among newly diagnosed MM patients, revealing the potential value of immune cell populations and cytokine profiles in assessing infection risk at various treatment stages.45 Furthermore, Dumontet et al,46 through analysis of the FIRST trial, devised a predictive model aimed at identifying early ≥ grade 3 infection risks among MM patients ineligible for transplantation. This model, by integrating MS outcomes with baseline cytogenetics, enhanced the accuracy of prognostic predictions. Subsequently, Mai and co-researchers explored the application and prognostic implications of MS in newly diagnosed MM patients, demonstrating its superiority in monitoring monoclonal proteins, especially when combined with minimal residual disease (MRD) assessment and baseline disease characteristics, thereby providing independent prognostic information.47 Most recently, Mai et al,48 leveraging data from five randomized controlled phase III trials encompassing 3700 patients, developed and validated a risk scoring system to predict early morbidity and mortality. This system effectively identified high-risk groups among transplant-eligible NDMM patients undergoing novel agent-based triplet or quadruplet induction therapies. Collectively, these studies showcase the pivotal role of emerging technologies in enhancing the management efficiency of MM patients, refining treatment precision, and improving prognostic predictions. They hold the potential to become new standards in the management of MM patients, offering a scientific basis for the realization of personalized treatment strategies.
Conclusion
Immunodeficiency stands as a hallmark of MM, with infection constituting a significant comorbidity that directly impacts patient mortality. These infections, predominantly bacterial but also extending to fungal and viral, notably during treatment phases, underscore the critical need for comprehensive clinical assessments. Understanding the clinical precursors to mortality in MM can enhance decision-making regarding treatment benefits and risks. It also informs the necessity for meticulous patient monitoring across various disease and treatment stages, aiming for tailored patient management strategies to potentially extend survival. In addressing the heightened vulnerability of MM patients to VZV infections, a multifaceted approach is essential for effective herpes zoster prevention. Despite the absence of a universally accepted protocol regarding the choice of antivirals, dosage, and prophylaxis duration, existing studies offer valuable insights into potential preventive regimens. The efficacy of low-dose acyclovir (200–400 mg/day) throughout bortezomib treatment cycles in mitigating herpes zoster incidence among MM patients exemplifies such strategies. Given the unique health challenges faced by MM patients, there is an imperative for ongoing research. Future investigations should focus on the optimal selection of antiviral agents, dosage specifics, administration duration, and the comprehensive evaluation of herpes zoster prevention protocols, including vaccination. This encompasses assessing the interplay between therapeutic agents and vaccine efficacy, as well as the influence of prophylactic measures on chemotherapy effectiveness. Through such evidence-based inquiries, the goal is to scientifically forge advanced prevention strategies against herpes zoster, thereby enhancing the care and outcomes for individuals with MM.
Ethics Approval
In crafting this article, adherence to the Declaration of Helsinki’s ethical guidelines was ensured. The process complied with prevailing local legislation and institutional protocols, negating the need for ethical oversight in publishing case details. The consent for the publication of this case report, including all data and images, was duly obtained from the family member of the patient.
Funding
This work was supported by the Hundred Talents Programme for Enhancing Research Capacity of the Affiliated Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, China (Grant No. 20-B04).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Shin BS, Na CH, Song IG, Choi KC. A case of human immunodeficiency virus infection initially presented with disseminated herpes zoster. Ann Dermatol. 2010;22(2):199–202. doi:10.5021/ad.2010.22.2.199
2. Valković T, Gačić V, Ivandić J, et al. Infections in hospitalised patients with multiple myeloma: main characteristics and risk factors. Turk J Haematol. 2015;32(3):234–242. doi:10.4274/tjh.2013.0173
3. Shindo T, Kimura S. Immune defects in multiple myeloma. Nihon Rinsho. Japan J Clin Med. 2015;73(1):52–56.
4. Blimark C, Holmberg E, Mellqvist UH, et al. Multiple myeloma and infections: a population-based study on 9253 multiple myeloma patients. Haematologica. 2015;100(1):107–113. doi:10.3324/haematol.2014.107714
5. Tsai CK, Liu YC, Kuan AS, et al. Risk and impact of invasive fungal infections in patients with multiple myeloma. Ann Hematol. 2020;99(8):1813–1822. doi:10.1007/s00277-020-04125-z
6. Nucci M, Anaissie E. Infections in patients with multiple myeloma in the era of high-dose therapy and novel agents. Clin Infect Dis. 2009;49(8):1211–1225. doi:10.1086/605664
7. Pratt G, Goodyear O, Moss P. Immunodeficiency and immunotherapy in multiple myeloma. Br J Haematol. 2007;138(5):563–579. doi:10.1111/j.1365-2141.2007.06705.x
8. Schütt P, Brandhorst D, Stellberg W, et al. Immune parameters in multiple myeloma patients: influence of treatment and correlation with opportunistic infections. Leuk Lymphoma. 2006;47(8):1570–1582. doi:10.1080/10428190500472503
9. Ludwig H, Kumar S. Prevention of infections including vaccination strategies in multiple myeloma. Am J Hematol. 2023;98(Suppl 2):S46–S62. doi:10.1002/ajh.26766
10. Park H, Youk J, Kim HR, et al. Infectious complications in multiple myeloma receiving autologous stem cell transplantation in the past 10 years. Int J Hematol. 2017;106(6):801–810. doi:10.1007/s12185-017-2313-2
11. Zheng G, Guan F, Han X, et al. Efficacy of intermittent, oral famciclovir prophylaxis for bortezomib-induced herpes zoster in multiple myeloma patients. Front Oncol. 2022;12:843032. doi:10.3389/fonc.2022.843032
12. Ghate M, Deshpande S, Tripathy S, et al. Incidence of common opportunistic infections in HIV-infected individuals in Pune, India: analysis by stages of immunosuppression represented by CD4 counts. Int J Infect Dis. 2009;13(1):e1–e8. doi:10.1016/j.ijid.2008.03.029
13. Dosani T, Mailankody S, Korde N, et al. Host-related immunodeficiency in the development of multiple myeloma. Leuk Lymphoma. 2018;59(5):1127–1132. doi:10.1080/10428194.2017.1361026
14. Suen H, Brown R, Yang S, et al. Multiple myeloma causes clonal T-cell immunosenescence: identification of potential novel targets for promoting tumour immunity and implications for checkpoint blockade. Leukemia. 2016;30(8):1716–1724. doi:10.1038/leu.2016.84
15. Trotta R, Dal Col J, Yu J, et al. TGF-beta utilizes SMAD3 to inhibit CD16-mediated IFN-gamma production and antibody-dependent cellular cytotoxicity in human NK cells. J Immunol. 2008;181(6):3784–3792. doi:10.4049/jimmunol.181.6.3784
16. Cowan AJ, Green DJ, Kwok M, et al. Diagnosis and management of multiple myeloma: a review. JAMA. 2022;327(5):464–477. doi:10.1001/jama.2022.0003
17. Nahi H, Chrobok M, Gran C, et al. Infectious complications and NK cell depletion following daratumumab treatment of multiple myeloma. PLoS One. 2019;14(2):e0211927. doi:10.1371/journal.pone.0211927
18. Yarlagadda L, Gundarlapalli S, Parikh R, et al. Salvage autologous stem cell transplantation in daratumumab-refractory multiple myeloma. Cancers. 2021;13(16):4019. doi:10.3390/cancers13164019
19. John L, Sauer S, Hegenbart U, et al. Idecabtagene vicleucel is well tolerated and effective in relapsed/refractory myeloma patients with prior allogeneic stem cell transplantation. Transplant Cell Ther. 2023;29(10):
20. Cliff ERS, Reynolds G, Popat R, Teh BW, Kesselheim AS, Mohyuddin GR. Acknowledging infection risk in bispecific antibody trials in the treatment of multiple myeloma. J Clin Oncol. 2023;41(10):1949–1951. doi:10.1200/JCO.22.02197
21. Teh BW, Teng JC, Urbancic K, et al. Invasive fungal infections in patients with multiple myeloma: a multi-center study in the era of novel myeloma therapies. Haematologica. 2015;100(1):e28–e31. doi:10.3324/haematol.2014.114025
22. Teh BW, Harrison SJ, Worth LJ, Thursky KA, Slavin MA. Infection risk with immunomodulatory and proteasome inhibitor-based therapies across treatment phases for multiple myeloma: a systematic review and meta-analysis. Eur J Cancer. 2016;67:21–37. doi:10.1016/j.ejca.2016.07.025
23. Brioli A, Klaus M, Sayer H, et al. The risk of infections in multiple myeloma before and after the advent of novel agents: a 12-year survey. Ann Hematol. 2019;98(3):713–722. doi:10.1007/s00277-019-03621-1
24. Blanco B, Pérez-Simón JA, Sánchez-Abarca LI, et al. Bortezomib induces selective depletion of alloreactive T lymphocytes and decreases the production of Th1 cytokines. Blood. 2006;107(9):3575–3583. doi:10.1182/blood-2005-05-2118
25. Jones JO, Arvin AM. Inhibition of the NF-kappaB pathway by varicella-zoster virus in vitro and in human epidermal cells in vivo. J Virol. 2006;80(11):5113–5124. doi:10.1128/JVI.01956-05
26. Berges C, Haberstock H, Fuchs D, et al. Proteasome inhibition suppresses essential immune functions of human CD4+ T cells. Immunology. 2008;124(2):234–246. doi:10.1111/j.1365-2567.2007.02761.x
27. Heider U, Rademacher J, Kaiser M, Kleeberg L, von Metzler I, Sezer O. Decrease in CD4+ T-cell counts in patients with multiple myeloma treated with bortezomib. Clin Lymphoma Myeloma Leuk. 2010;10(2):134–137. doi:10.3816/CLML.2010.n.019
28. Kim SJ, Kim K, Kim BS, et al. Bortezomib and the increased incidence of herpes zoster in patients with multiple myeloma. Clin Lymphoma Myeloma. 2008;8(4):237–240. doi:10.3816/CLM.2008.n.031
29. Chanan-Khan A, Sonneveld P, Schuster MW, et al. Analysis of herpes zoster events among bortezomib-treated patients in the phase III APEX study. J Clin Oncol. 2008;26(29):4784–4790. doi:10.1200/JCO.2007.14.9641
30. Terpos E, Kleber M, Engelhardt M, et al. European Myeloma Network guidelines for the management of multiple myeloma-related complications. Haematologica. 2015;100(10):1254–1266. doi:10.3324/haematol.2014.117176
31. Redelman-Sidi G, Michielin O, Cervera C, et al. ESCMID Study Group for Infections in Compromised Hosts (ESGICH) Consensus Document on the safety of targeted and biological therapies: an infectious diseases perspective (Immune checkpoint inhibitors, cell adhesion inhibitors, sphingosine-1-phosphate receptor modulators and proteasome inhibitors). Clin Microbiol Infect. 2018;2(Suppl 2):S95–S107. doi:10.1016/j.cmi.2018.01.030
32. Vickrey E, Allen S, Mehta J, Singhal S. Acyclovir to prevent reactivation of varicella zoster virus (herpes zoster) in multiple myeloma patients receiving bortezomib therapy. Cancer. 2009;115(1):229–232. doi:10.1002/cncr.24006
33. Swaika A, Paulus A, Miller KC, et al. Acyclovir prophylaxis against varicella zoster virus reactivation in multiple myeloma patients treated with bortezomib-based therapies: a retrospective analysis of 100 patients. J Support Oncol. 2012;10(4):155–159. doi:10.1016/j.suponc.2011.10.006
34. Fukushima T, Sato T, Nakamura T, et al. Daily 500 mg valacyclovir is effective for prevention of Varicella zoster virus reactivation in patients with multiple myeloma treated with bortezomib. Anticancer Res. 2012;32(12):5437–5440.
35. Ying T, Aijun L. Chen Wenming Clinical observation of the use of bortezomib in the prevention of herpes zoster in patients with multiple myeloma using valacilovir. Chin J Clin Physic. 2013;7(12):5634–5636.
36. Mateos MV, Hernández JM, Hernández MT, et al. Bortezomib plus melphalan and prednisone in elderly untreated patients with multiple myeloma: results of a multicenter Phase 1/2 study. Blood. 2006;108(7):2165–2172. doi:10.1182/blood-2006-04-019778
37. Pour L, Adam Z, Buresova L, et al. Varicella-zoster virus prophylaxis with low-dose Acyclovir in patients with multiple myeloma treated with bortezomib. Clin Lymphoma Myeloma. 2009;9(2):151–153. doi:10.3816/CLM.2009.n.036
38. Minarik J, Pika T, Bacovsky J, Langova K, Scudla V. Low-dose Acyclovir prophylaxis for bortezomib-induced herpes zoster in multiple myeloma patients. Br J Haematol. 2012;159(1):111–113. doi:10.1111/j.1365-2141.2012.09233.x
39. Kim SJ, Kim K, Do YR, Bae SH, Yang DH, Lee JJ. Low-dose Acyclovir is effective for prevention of herpes zoster in myeloma patients treated with bortezomib: a report from the Korean Multiple Myeloma Working Party (KMMWP) Retrospective Study. Jpn J Clin Oncol. 2011;41(3):353–357. doi:10.1093/jjco/hyq194
40. Asano-Mori Y, Kanda Y, Oshima K, et al. Long-term ultra-low-dose Acyclovir against varicella-zoster virus reactivation after allogeneic hematopoietic stem cell transplantation. Am J Hematol. 2008;83(6):472–476. doi:10.1002/ajh.21152
41. Abbasov E, Metzner B, Müller TH, et al. Herpes zoster prophylaxis with low-dose Acyclovir in patients with malignant lymphoma and multiple myeloma treated with autologous stem cell transplantation. Eur J Haematol. 2022;109(3):298–304. doi:10.1111/ejh.13810
42. Winston DJ, Mullane KM, Cornely OA, et al. Inactivated varicella zoster vaccine in autologous haemopoietic stem-cell transplant recipients: an international, multicentre, randomised, double-blind, placebo-controlled trial. Lancet. 2018;391(10135):2116–2127. doi:10.1016/S0140-6736(18)30631-7
43. Dagnew AF, Ilhan O, Lee WS, et al. Immunogenicity and safety of the adjuvanted recombinant zoster vaccine in adults with haematological malignancies: a Phase 3, randomised, clinical trial and post-hoc efficacy analysis [published correction appears in Lancet Infect Dis. 2020 Jan; 20(1):e1]. Lancet Infect Dis. 2019;19(9):988–1000. doi:10.1016/S1473-3099(19)30163-X
44. Stadtmauer EA, Sullivan KM, El Idrissi M, et al. Adjuvanted recombinant zoster vaccine in adult autologous stem cell transplant recipients: polyfunctional immune responses and lessons for clinical practice. Hum Vaccin Immunother. 2021;17(11):4144–4154. doi:10.1080/21645515.2021.1953346
45. Teh BW, Harrison SJ, Allison CC, et al. Predicting risk of infection in patients with newly diagnosed multiple myeloma: utility of immune profiling. Front Immunol. 2017;8:1247. doi:10.3389/fimmu.2017.01247
46. Dumontet C, Hulin C, Dimopoulos MA, et al. A predictive model for risk of early grade ≥ 3 infection in patients with multiple myeloma not eligible for transplant: analysis of the FIRST trial. Leukemia. 2018;32(6):1404–1413. doi:10.1038/s41375-018-0133-x
47. Mai EK, Huhn S, Miah K, et al. Implications and prognostic impact of mass spectrometry in patients with newly-diagnosed multiple myeloma. Blood Cancer J. 2023;13(1):1. doi:10.1038/s41408-022-00772-9
48. Mai EK, Hielscher T, Bertsch U, et al. Predictors of early morbidity and mortality in newly diagnosed multiple myeloma: data from five randomized, controlled, phase III trials in 3700 patients. Leukemia. 2024;38(3):640–647. doi:10.1038/s41375-023-02105-6
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.