")
Back to Journals » International Journal of Nephrology and Renovascular Disease » Volume 16
Current Knowledge of Beta-Blockers in Chronic Hemodialysis Patients
Received 29 March 2023
Accepted for publication 29 September 2023
Published 12 October 2023 Volume 2023:16 Pages 223—230
DOI https://doi.org/10.2147/IJNRD.S414774
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pravin Singhal
Intissar Haddiya,1,2 Siria Valoti3
1Department of Nephrology, Faculty of Medicine and Pharmacy, University Mohamed Premier, Oujda, Morocco; 2Laboratory of Epidemiology, Clinical Research and Public Health, Faculty of Medicine and Pharmacy, University Mohamed Premier, Oujda, Morocco; 3Department of Medicine, Faculty of Medicine, Università degli Studi di Milano Statale, Milano, Italia
Correspondence: Intissar Haddiya, Department of Nephrology, Faculty of Medicine and Pharmacy, University Mohamed Premier, BP 724 Hay Al Quods, Oujda, 60000, Morocco, Tel +212 661 28 14 00, Email [email protected]
Abstract: Beta-blockers include a large spectrum of drugs with various specific characteristics, and a well-known cardioprotective efficacy. They are recommended in heart failure, hypertension and arrhythmia. Their use in chronic hemodialysis patients is still controversial, mainly because of the lack of specific randomized clinical trials. Large observational studies and two important clinical trials have reported almost unanimously their efficacy in chronic hemodialysis patients, which seems to be related to their levels of dialyzability and cardioselectivity. A recent meta-analysis suggested that high dialyzable beta-blockers are correlated to a reduced risk of all-cause mortality and cardiovascular complications compared with low dialyzable beta-blockers. Despite their benefits, beta-blockers may have adverse effects, such as intradialytic hypotension with low dialyzability beta-blockers or the risk of sub-therapeutic plasma concentration of high dialyzable ones during dialysis sessions. Both cases are linked to adverse cardiovascular events. A solution for both high and low dialyzable drugs could be their administration after dialysis sessions. Futhermore, the bulk of existing literature seems to favor cardioselective beta-blockers with moderate-to-high dialyzability as the ideal agents in dialysis patients, but further, larger studies are needed. This review aims to analyze beta-blockers’ characteristics, indications and evidence-based role in chronic hemodialysis patients.
Keywords: beta-blockers, hemodialysis, hypertension, mortality, intradialytic hypotension
Introduction
Chronic hemodialysis patients are at high risk of cardiovascular morbidity and mortality.1 In fact, the prevalence of mortality is 10–20 fold higher in these patients than in the general population and three times higher than in other risk groups,2,3 and cardiovascular diseases are responsible for 25% of hospitalizations and 50% of deaths in chronic hemodialysis.4 This is mainly due to the fact that end stage kidney disease (ESKD) patients are characterized by a complex pathophysiology that involves renin-angiotensin-aldosterone system (RAAS) and sympathetic nervous system overactivation, leading to hypertension or its worsening.5,6 Furthermore, hemodialysis sessions may cause sudden and frequent fluctuations in hemodynamics, heart rate and electrolytes balance, which may also exacerbate cardiovascular events.7
Prevention and treatment of cardiovascular complications are the biggest challenges that practitioners are confronted with in order to improve hemodialysis patients’ survival:8 therefore, the choice of the appropriate anti-hypertensive or anti-arrhythmic drug is fundamental. Beta-blockers have cardioprotective effects that are well described in the general population, whereas evidence of their advantages in dialysis patients is still limited.9,10 This review analyses beta-blockers’ characteristics, indications and evidence-based role in chronic hemodialysis patients.
Methods
In order to perform this review it was useful to consult relevant publications on various aspects of the topic, using the following keywords: Beta blockers, Pharmacology of beta blockers, Beta blockers in hypertension, Beta blockers in CKD, Beta blockers in dialysis.
Data research was conducted in databases such as PubMed, ResearchGate, Scopus and Google Scholar.
Beta-Blockers: Definition, Classification, Use and Adverse Effects in the General Population
Beta-blockers are beta-adrenergic blocking agents and their effect is mainly recognized in controlling the activation of the “fight-or-flight” stress response.
Their targets are the adrenergic receptors that are physiologically targeted by the catecholamines (such as epinephrine and noradrenaline). These drugs are also called beta-adrenergic antagonists. They prevent catecholamines from binding to the target receptor and therefore oppose their physiological effects. Some receptors are more sensitive to noradrenaline while others are more sensitive to epinephrine. Beta-blockers attach to these same receptor sites and block them, reducing the number of the receptors that are available for activation. Thus, leading to the decrease of the catecholamines’ effects.11
Adrenergic Receptors (α and β)
Adrenergic receptors are classified into two groups, alpha receptors and beta receptors, with 9 subtypes in total.12,13 Many cell types have adrenergic receptors, but they are mainly present in smooth muscle and cardiac muscle. Increased cAMP has an effect that differs between smooth and cardiac muscle. In fact, high levels of cAMP promote smooth muscle relaxation while they increase contractility in cardiac muscle.14
Beta Receptors
Beta receptors can be classified into three main subtypes, β1, β2 and β3 receptors, with different effects depending on their location.
- β1 receptors can be found in myocardial cells and the kidney. The effects of these receptors on the heart are due to a positive chronotropic effect (increased heart rate), positive dromotropic effect (increased conduction speed), positive ionotropic effect (increased contractility); whereas in the kidney, β1 receptors increase renin secretion and cause hypertension.15
- β2 receptors have an inhibitory effect on smooth muscle cells, causing their relaxation.16
- β3 receptors are localized in the fat tissue and their activation increases lipolysis.17
Beta-Blockers Classification
There are several types of beta-blockers, with similar activities but each one of them has its own distinctive characteristics and pharmacokinetic/pharmacodynamic properties that have been extensively studied.18 They are classified as first, second and third generation beta-blockers.
- First generation beta-blockers are nonselective active principles that have effect both on β1 and β2 adrenergic receptors. In this category, there are propranolol (the first developed beta-blocker), nadolol, pindolol and timolol.
- Second generation beta-blockers (cardioselective) act by blocking the β1 receptor only. These receptors are localized mainly in the cardiac tissue. These are atenolol, bisoprolol, acebutolol, metoprolol and esmolol.
- Third generation beta-blockers are β1 selective, but they also have vasodilatory properties, making these medications more effective. Moreover, they can be characterized by the interaction with other adrenergic receptors (such as α1 receptors) so they have a mixed antagonism. This is the case of carvedilol and labetalol. Other third generation drugs, such as nebivolol, also have a vasodilatory effect by stimulating nitric oxide release.19
Some beta-blockers have an intrinsic sympathomimetic action (ISA), e.g. acebutolol, pindolol, labetalol. This means that although they are beta-blockers, these drugs have also a modest stimulation effect on β2 receptors. They have less effect on decreasing heart activity, but they also promote vasodilatation in order to avoid a peripheral resistance increase. This is particularly useful in chronic kidney disease patients.11
Beta-Blockers Use
Beta-blockers are used to prevent or treat several cardiovascular diseases, such as angina, heart failure, atrial fibrillation, arrhythmias, heart attacks and hypertension, thyrotoxicosis and RAAS blocker, but they can also be used for migraine, tremors, anxiety and glaucoma.
These drugs can have various uses, due to the fact that their receptors are spread throughout the whole body. It is important to note that different beta-blockers have different indications. In hypertension, they are not the first-line treatment, but rather an add-on treatment.20
Adverse Effects and Contraindications of Beta-Blockers
The main side effects of beta-blockers are nausea and diarrhea, fatigue, hypotension, bradycardia and heart block especially in the elderly, shortness of breath, bronchospasm and sexual dysfunction.21
Beta-blockers should be carefully used in diabetic patients, because they interact with glucose metabolism and could mask signs of hypoglycemia. If prescribed in a diabetic patient, it is mandatory to check blood glucose continuously. It is important to note that adverse effects such as bronchospasm, peripheral vasoconstriction, impairment of glucose and lipid metabolism are associated with the use of β2-adrenergic receptor antagonist activity. Consequently, these are considered as contraindications to the use of nonselective beta-blockers.21
Beta-Blockers Use in Hemodialysis Patients
The use of beta-blockers in hemodialysis patients is largely based on the extrapolation of their efficacy in the general population.22 This is the consequence of the lack of consistent strong data on the benefits of beta-blockers in dialysis patients, due to their exclusion from clinical trials because of the risk of adverse effects, such as fluid overload, intradialytic muscle cramps, hypotension and hyperkalemia.23,24 Nevertheless, comorbidities (hypertension, atrial fibrillation, coronary artery disease and heart failure) in these patients justify the use of beta-blockers in many cases.25 In fact, although the extension of clinical trials proven benefits of beta-blockers from the general population to dialysis patients may seem reasonable, their use cannot be considered evidence-based.
Besides, there are a number of observational studies that aim to determine beta-blockers’ therapeutic efficacy in dialysis patients and claim their cardiovascular protective effect. These studies focus on the main cardiovascular complications of hemodialysis, such as hypertension, heart failure and atrial fibrillation. In Taiwan, a large cohort study of 4435 long-term hemodialysis patients compared beta-blocker (carvedilol, bisoprolol and metoprolol) users with nonusers and reported improved survival among patients with heart failure receiving beta-blockers.26 Another important study that had enrolled 11,142 hemodialysis patients within the US Renal Data System (USRDS), showed that the use of beta-blockers to treat hypertension in hemodialysis patients was associated with a remarkable reduction in mortality.2 What is more, a large-scale retrospective study that had included more than 100,000 hemodialysis patients in Taiwan, showed the efficacy of beta-blockers in the primary prevention of atrial fibrillation.27
Some observational studies discussed the possible efficacy of beta-blockers on myocardial infarction in the setting of hemodialysis. A cohort study of 1025 chronic hemodialysis patients with acute myocardial infarction proved that beta-blocker administration at hospital admission was associated with a lower 30-day mortality.28 Two other observational studies have shown an association between beta-blockers use and the reduction of sudden cardiac death among hemodialysis patients.29,30
However, a Canadian cohort study compared mortality and cardiovascular morbidity rates among dialysis patients taking either a beta-blocker, a calcium channel blocker or a statin and found no evidence of a favorable outcome related to beta-blockers use.31
The contradictory results of different observational studies underline the necessity of clinical trials to analyze the real impact of these drugs in dialysis patients.
Table 1 summarizes the results of three randomized controlled trials (RCTs) that have studied beta-blockers in hemodialysis patients.32
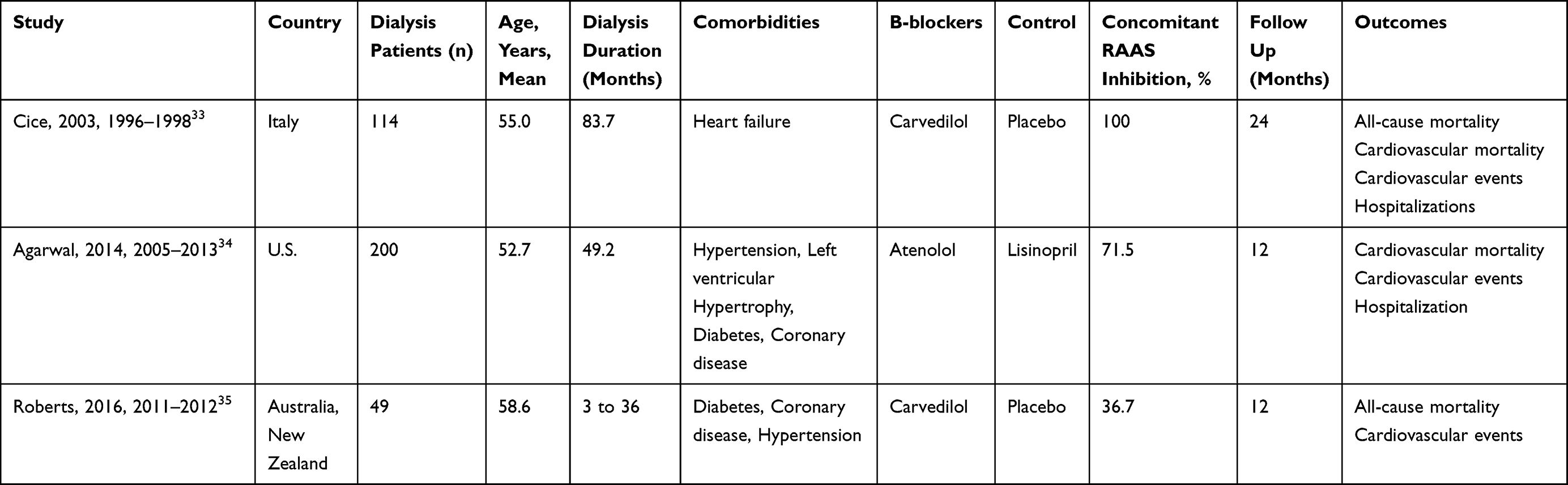 |
Table 1 Summary of Three Randomized Controlled Trials (RCTs) That Have Studied Beta-Blockers in Hemodialysis Patients |
Cice et al33 performed a double-blind, randomized trial focusing on dialysis patients with heart failure. They compared carvedilol versus placebo in 114 dialysis patients and found that it had reduced left ventricular volume and improved patients’ functional status. They also observed that after a two-year follow-up, the included patients who received carvedilol had lower mortality and hospital admissions than the patients under placebo.
Agarwal et al34 studied a population of dialysis patients with hypertension and left-ventricular hypertrophy, in an open-label randomized controlled trial, in which they compared atenolol and lisinopril in 200 hemodialysis patients. This study showed greater blood pressure reduction with atenolol compared with lisinopril, but was interrupted earlier because of serious complications in the lisinopril group. In addition, this study included a majority of black patients. Consequently, it was not possible to generalize its results to hemodialysis patients.
Roberts et al35 performed a multicenter pilot randomized controlled trial, but failed to compare carvedilol with placebo as they could not recruit the planned sample size. The goal was to randomize 150 patients, but they only managed to get a population of 49 patients, due to a high dropout rate and several complications. This trial proves the extreme difficulty of recruiting a large number of dialysis patients to obtain evidence-proved answers regarding beta-blockers use in dialysis, despite the need for larger clinical trials.
Another clinical trial has been published recently.36 It is an open-label, single center randomized control trial that enrolled 46 hemodialysis patients with hypertension. The participants were randomized to receive either amlodipine or bisoprolol. Then two parameters were checked: the left ventricular hypertrophy index (LVMI), and the asymmetric dimethylarginine (ADMA), a marker of cardiovascular disease whose elevation results in NO synthesis inhibition, endothelial function impairment and atherosclerosis promotion. The outcome in patients with amlodipine-based therapy was marked by a significant reduction in ADMA and LVMI and therefore an important reduction in cardiovascular disease in the included patients. Thus, this study suggests the use of amlodipine as the first line antihypertensive agent, instead of beta-blockers. However, larger multicenter clinical trials are required for stronger results.
Beta-Blockers Specificities in Hemodialysis: Dialyzability and Cardioselectivity
There are several studies on the effectiveness of beta-blockers that have similar activities but each type of beta-blocker has its distinctive characteristics, intradialytic kinetics and side effects. This is why, compared with other drugs, selecting the appropriate beta-blocker might seem difficult.
Two major properties that differ among agents are dialyzability and cardioselectivity. Observational studies that have tried to investigate the association between dialyzability or cardioselectivity of beta-blockers and hemodialysis outcome, obtained conflicting results.
Dialyzability is a parameter that reflects drug removal efficiency from the circulation during the dialysis session, with the subsequent possible loss of effectiveness. The dialyzability of a drug depends on several factors, including its water solubility: hydrophilic beta-blockers are removed to a greater extent during dialysis than the lipophilic ones. The explanation is that the latter are present in plasma in a small amount, because they easily pass the lipid bilayer and are distributed in different tissues. Consequentially, in turn, the lipid-soluble ones have a greater tendency to cross the blood–brain barrier, with more potential adverse effects.37
Atenolol and metoprolol are considered highly dialyzable, while propranolol and carvedilol clearances remain lower.38 The classification of bisoprolol is still debated. A study of Weir et al on 3294 hemodialysis patients treated with a highly dialyzable beta-blocker (metoprolol/atenolol/acebutolol) and 3294 with a low dialyzable beta-blocker (mainly bisoprolol) showed a higher mortality and arrhythmia risk in the highly dialyzable beta-blockers group at six months of therapy initiation.39 This study did not take into consideration the effects of carvedilol, but Wu et al compared 15,699 hemodialysis patients treated with a moderate or highly dialyzable beta-blocker (atenolol, acebutolol, metoprolol or bisoprolol) and 20,094 hemodialysis patients treated with a poorly dialyzable beta-blocker (betaxolol, carvedilol or propranolol) and found that the first group had lower mortality and cardiovascular complication risks.38 A large retrospective study by Shireman et al compared hemodialysis patients under cardioselective beta-blockers (atenolol and metoprolol) with those using non-cardioselective beta-blockers (carvedilol and labetalol) and found a lower mortality rate in cardioselective beta-blocker users.40 This seems in contradiction with the overall results of carvedilol in patients with heart failure reported by previous studies.33 Finally, Assimon et al compared 17,506 hemodialysis patients treated with metoprolol (highly dialyzable/cardioselective) with 9558 hemodialysis patients initiated on carvedilol (poorly dialyzable/non-cardioselective) and found that the carvedilol group had a higher cardiovascular and all-cause mortality risk. The authors also found that the carvedilol group had higher rates of intradialytic hypotension and hypothesized that this may provide an explanation for the increased mortality risk observed with carvedilol.41
A recent meta-analysis, based on the prospective cohort studies mentioned earlier, compared all-cause mortality and cardiovascular outcomes between highly dialyzable and low dialyzable beta-blockers. In fact, Tella et al underwent a systematic review of the literature suggesting that the two classes have similar mortality events but the highly dialyzable ones have fewer cardiovascular outcomes.42 It is interesting to note how the only study in favor of low dialyzability beta-blockers classified bisoprolol as poorly dialyzable, on the basis of earlier pharmacokinetics studies.43 In sharp contrast, recently Tieu et al showed that bisoprolol is characterized by a substantial dialytic clearance.44 Therefore, considering the fact that in Weir et al’s analysis the majority of patients of the low-dialyzability group were treated with bisoprolol, Tella et al performed a sensitivity analysis, considering the misclassification of bisoprolol as a poorly dialyzable beta-blocker. Accordingly, the new conclusion of their meta-analysis claimed that highly dialyzable beta-blockers were linked with 13% reduced risk of all-cause mortality and adverse cardiovascular events.39,42
Besides dialyzability other factors, such as cardioselectivity should be considered while interpreting the results of the above-mentioned studies. In fact, the high dialyzability beta blockers mainly used in these studies are cardioselective (metoprolol and atenolol), while the chosen low-dialyzability beta-blockers are mainly non-cardioselective (labetalol, carvedilol or propranolol). Consequently, other pharmacologic characteristics of beta-blockers could influence the results and be partially responsible for the observed benefits of highly dialyzable beta-blockers.
Beta-Blockers Concerns and Adverse Effects in Dialysis
Beta-blockers used in hemodialysis may present various complications, the most common being Intradialytic hypotension (IDH). This adverse effect has a higher occurrence in elderly patients with multiple comorbidities.45 It occurs in up to 20% or more of dialysis sessions and can result in significant morbidity secondary to end-organ hypoperfusion, which is caused by a drop in absolute blood volume (ABV) due to an excessive ultrafiltration (UF) rate, not compensated by a vascular refilling volume from interstitial to intravascular compartment. It is possible that the use of beta-blockers may affect compensatory responses to ABV drop and contribute to IDH development.46,47 Recently a retrospective study48 has investigated this hypothesis, thanks to a new measurement technology to calculate ABV and vascular refilling volume.49 The study aimed to analyze how beta-blockers modify vascular refilling volume during hemodialysis sessions, focusing on carvedilol, characterized by being non-cardioselective, poorly dialyzable and consequently more involved in intradialytic hemodynamics than other beta-blockers. The results showed that the use of carvedilol in dialysis patients led to a higher risk of IDH if administered before the hemodialysis session, so it could be suggested to prescribe this drug after the hemodialysis session. These findings could explained by the action of beta-blockers, as these drugs reduce cardiac output and vasoconstriction, leading to an increase in hydrostatic pressure in the capillary bed that may inhibit refilling.50 Also, Assimon et al reported the higher incidence of IDH in patients using carvedilol compared with patients under metoprolol. Therefore, poorly dialyzable beta-blockers, that are not efficiently removed during dialysis, have a long action in patients who experience rapid changes in hemodynamics and therefore are linked to hypotension and cardiovascular events.41
On the contrary, highly dialyzable beta-blockers such as atenolol are easily removed during dialysis, diminishing blood pressure effects over the course of dialysis. This leads to their rapid decline and sub-therapeutic plasma concentrations in the interdialytic interval. In the general population, a sudden discontinuation of beta-blockers has been linked to hypertension, tachycardia and adverse cardiovascular events.51 Accordingly, it can be hypothesized that highly dialyzable beta-blockers may be linked to similar adverse effects, with a higher risk of cardiovascular events and all-cause mortality. For this reason, the authors of one study claimed that it could be beneficial to take these drugs after the dialysis session in order to achieve a longer effect and improve patient outcomes.52 In fact, although sudden changes in highly dialyzable beta-blockers concentrations may be a predisposing factor for cardiovascular events, it is noteworthy to mention that it rarely occurs when these drugs are taken after dialysis, as shown in the HDPAL trial.34
Furthermore, in addition to hypotension and bradycardia, non-cardioselective beta-blockers such as carvedilol and propranolol have been suggested to induce hyperkalemia in patients with ESKD and in those who use mineralocorticoid receptor antagonists.23,35
Conclusion
Despite the limited evidence, cardioprotective and overall survival benefits with beta-blockers use in dialysis patients is suggested by several authors, but there are still controversial opinions about the specific beta-blockers to choose in order to guarantee the best outcome.
The bulk of existing literature suggests that cardioselective beta-blockers with moderate-to-high dialyzability (such as atenolol, bisoprolol and metoprolol) could be the ideal agents in hemodialysis patients.
Nevertheless, further and larger randomized clinical trials are needed to produce stronger evidence about these drugs.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jha V, Garcia-Garcia G, Iseki K, et al. Chronic kidney disease: global dimension and perspectives. Lancet. 2013;382(9888):260–272. doi:10.1016/S0140-6736(13)60687-X
2. Foley RN, Parfrey PS, Sarnak MJ. Epidemiology of cardiovascular disease in chronic renal disease. J Am Soc Nephrol. 1998;9(12 Suppl):S16–S23.
3. Wanner C, Amann K, Shoji T. The heart and vascular system in dialysis. Lancet. 2016;388(10041):276–284. doi:10.1016/S0140-6736(16)30508-6
4. United States Renal Data System. 2019 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2019.
5. Blankestijn PJ. Sympathetic hyperactivity in chronic kidney disease. Nephrol Dial Transplant. 2004;19(6):1354–1357. doi:10.1093/ndt/gfh242
6. Georgianos PI, Agarwal R. Epidemiology, diagnosis and management of hypertension among patients on chronic dialysis. Nat Rev Nephrol. 2016;12(10):636–647. doi:10.1038/nrneph.2016.129
7. Tan Z, Ke G, Huang J, et al. Effects of Carvedilol on Cardiovascular Events and Mortality in Hemodialysis Patients. Iran J Kidney Dis. 2020;14(4):256–266.
8. Weir MA, Herzog CA. Beta blockers in patients with end stage renal disease-Evidence-based recommendations. Semin Dial. 2018;31:219–225. doi:10.1111/sdi.12691
9. Unger T, Borghi C, Charchar F, et al. 2020 International Society of Hypertension global hypertension practice guidelines. J Hypertens. 2020;38(6):982–1004. doi:10.1097/HJH.0000000000002453
10. Konstantinidis I, Nadkarni GN, Yacoub R, et al. Representation of patients with kidney disease in trials of cardiovascular interventions: an updated systematic review. JAMA Intern Med. 2016;176(1):121–124. doi:10.1001/jamainternmed.2015.6102
11. British and Irish Hypertension Society. Drug classes Beta-adrenoceptor antagonists (beta-blockers); 2017. Available from: https://bihsoc.org/wp-content/uploads/2017/11/Beta-adrenoceptor-Antagonists-Final-2017.pdf.
12. Seiler R, Rickenbacher A, Shaw S, Balsiger BM. alpha- and beta-adrenergic receptor mechanisms in spontaneous contractile activity of rat ileal longitudinal smooth muscle. J Gastrointest Surg. 2005;9(2):227–235. doi:10.1016/j.gassur.2004.05.012
13. Piascik MT, Perez DM. Alpha1-adrenergic receptors: new insights and directions. J Pharmacol Exp Ther. 2001;298(2):403–410.
14. Kuo IY, Ehrlich BE. Signaling in muscle contraction. Cold Spring Harb Perspect Biol. 2015;7:a006023. doi:10.1101/cshperspect.a006023
15. Frielle T, Collins S, Daniel KW, Caron MG, Lefkowitz RJ, Kobilka BK. Cloning of the cDNA for the human beta 1-adrenergic receptor. Proc Natl Acad Sci USA. 1987;84(22):7920–7924. doi:10.1073/pnas.84.22.7920
16. Kobilka BK, Dixon RA, Frielle T, et al. cDNA for the human beta 2-adrenergic receptor: a protein with multiple membrane-spanning domains and encoded by a gene whose chromosomal location is shared with that of the receptor for platelet-derived growth factor. Proc Natl Acad Sci USA. 1987;84(1):46–50. doi:10.1073/pnas.84.1.46
17. Gauthier C, Tavernier G, Charpentier F, Langin D. Le Marec H: functional beta3-adrenoceptor in the human heart. J Clin Invest. 1996;98:556–562. doi:10.1172/JCI118823
18. Wachter SB, Gilbert EM. Beta-adrenergic receptors, from their discovery and characterization through their manipulation to beneficial clinical application. Cardiology. 2012;122(2):104–112. doi:10.1159/000339271
19. DiNicolantonio JJ, Lavie CJ, Fares H, Menezes AR, O’Keefe JH. Meta‐analysis of carvedilol versus beta 1 selective beta‐blockers (atenolol, bisoprolol, metoprolol, and nebivolol). Am J Cardiol. 2013;111(5):
20. Fumagalli C, Maurizi N, Marchionni N, et al. β-blockers: their new life from hypertension to cancer and migraine. Pharmacol Res. 2020;151:104587. doi:10.1016/j.phrs.2019.104587
21. Paolillo S, Dell’Aversana S, Esposito I, Poccia A, Perrone Filardi P. The use of β-blockers in patients with heart failure and comorbidities: doubts, certainties and unsolved issues. Eur J Intern Med. 2021;88:9–14. doi:10.1016/j.ejim.2021.03.035
22. Tomaszuk-Kazberuk A, Kozuch M, Malyszko J, Bachorzewska-Gajewska H, Dobrzycki S, Musial WJ. Pharmacologic treatment in dialysis patients hospitalized for cardiovascular reasons: do we follow the guidelines? Ren Fail. 2012;35:235–242. doi:10.3109/0886022X.2012.745119
23. Nowicki M, Szewczyk-Seifert G, Klimek D, Kokot F. Carvedilol does not modulate moderate exercise- induced hyperkalemia in hemodialysis patients. Clin Nephrol. 2002;57(5):352–358. doi:10.5414/CNP57352
24. Bi SH, Linke L, Wu J, Cheng LT, Wang T, Ahmad S. Effects of beta-blocker use on volume status in hemodialysis patients. Blood Purif. 2012;33(4):311–316. doi:10.1159/000337375
25. Frankenfield DL, Weinhandl ED, Powers CA, et al. Utilization and costs of cardiovascular disease medications in dialysis patients in Medicare Part D. Am J Kidney Dis. 2012;59(5):670–681. doi:10.1053/j.ajkd.2011.10.047
26. Tang CH, Wang CC, Chen TH, et al. Prognostic benefits of carvedilol, bisoprolol, and metoprolol controlled release/extended release in hemodialysis patients with heart failure: a 10-year cohort. J Am Heart Assoc. 2016;5:e002584. doi:10.1161/JAHA.115.002584
27. Lin TT, Chiang JY, Liao MT, et al. Primary prevention of atrial fibrillation with beta-blockers in patients with end-stage renal disease undergoing dialysis. Sci Rep. 2015;5(1):17731. doi:10.1038/srep17731
28. Berger AK, Duval S, Krumholz HM. Aspirin, beta-blocker, and angiotensin-converting enzyme inhibitor therapy in patients with end-stage renal disease and an acute myocardial infarction. J Am Coll Cardiol. 2003;42(2):201–202. doi:10.1016/S0735-1097(03)00572-2
29. Matsue Y, Suzuki M, Nagahori W, et al. b-blocker prevents sudden cardiac death in patients with hemodialysis. Int J Cardiol. 2013;165(3):519–522. doi:10.1016/j.ijcard.2011.09.037
30. Pun PH, Lehrich RW, Smith SR, et al. Predictors of survival after cardiac arrest in outpatient hemodialysis clinics. Clin J Am Soc Nephrol. 2007;2(3):491–500. doi:10.2215/CJN.02360706
31. Kitchlu A, Clemens K, Gomes T, et al. Beta-blockers and cardiovascular outcomes in dialysis patients: a cohort study in Ontario, Canada. Nephrol Dial Transplant. 2012;27(4):1591–1598. doi:10.1093/ndt/gfr460
32. Jin J, Guo X, Yu Q. Effects of beta‐blockers on cardiovascular events and mortality in dialysis patients: a systematic review and meta‐analysis. Blood Purif. 2019;48(1):
33. Cice G, Ferrara L, D’Andrea A, et al. Carvedilol increases two- year survival in dialysis patients with dilated cardiomyopathy: a prospective, placebo-controlled trial. J Am Coll Cardiol. 2003;41(9):1438–1444. doi:10.1016/S0735-1097(03)00241-9
34. Agarwal R, Sinha AD, Pappas MK, Abraham TN, Tegegne GG. Hypertension in hemodialysis patients treated with atenolol or lisinopril: a randomized controlled trial. Nephrol Dial Transplant. 2014;29(3):672–681. doi:10.1093/ndt/gft515
35. Roberts MA, Pilmore HL, Ierino FL, et al. The b-Blocker to lower cardiovascular dialysis events (BLOCADE) feasibility study: a randomized controlled trial. Am J Kidney Dis. 2016;67(6):902–911. doi:10.1053/j.ajkd.2015.10.029
36. Youssef AM, Elghoneimy HA, Helmy MW, Abdelazeem AM, El-Khodary NM. Effect of amlodipine versus bisoprolol in hypertensive patients on maintenance hemodialysis: a randomized controlled trial. Medicine. 2021;100(51):28322. doi:10.1097/MD.0000000000028322
37. Furgeson SB, Chonchol M. Beta-blockade in chronic dialysis patients. Semin Dial. 2008;21(1):43–48. doi:10.1111/j.1525-139X.2007.00367.x
38. Wu PH, Lin YT, Kuo MC, et al. b-blocker dialyzability and the risk of mortality and cardiovascular events in patients doing hemodialysis. Nephrol Dial Transplant. 2020;35(11):1959–1965. doi:10.1093/ndt/gfaa058
39. Weir MA, Dixon SN, Fleet JL, et al. bBlocker dialyzability and mortality in older patients receiving hemodialysis. J Am Soc Nephrol. 2015;26(4):987–996. doi:10.1681/ASN.2014040324
40. Shireman TI, Mahnken JD, Phadnis MA, Ellerbeck EF. Effectiveness comparison of cardio-selective to non-selective b-blockers and their association with mortality and morbidity in end-stage renal disease: a retrospective cohort study. BMC Cardiovasc Disord. 2016;16(1):60. doi:10.1186/s12872-016-0233-3
41. Assimon MM, Brookhart MA, Fine JP, et al. A comparative study of carvedilol versus metoprolol initiation and 1-year mortality among individuals receiving maintenance hemodialysis. Am J Kidney Dis. 2018;72(3):337–348. doi:10.1053/j.ajkd.2018.02.350
42. Tella A, Vang W, Ikeri E, et al. β-blocker use and cardiovascular outcomes in hemodialysis: a systematic review. Kidney Med. 2022;4(5):100460. doi:10.1016/j.xkme.2022.100460
43. Levin NW, Kotanko P, Eckardt KU, et al. Blood pressure in chronic kidney disease stage 5D-report from a Kidney Disease: improving Global Outcomes controversies conference. Kidney Int. 2010;77(4):273–284. doi:10.1038/ki.2009.469
44. Tieu A, Velenosi TJ, Kucey AS, Weir MA, Urquhart BL. Beta-blocker dialyzability in maintenance hemodialysis patients: a randomized clinical trial. Clin J Am Soc Nephrol. 2018;13(4):604–611. doi:10.2215/CJN.07470717
45. Rubinger D, Backenroth R, Sapoznikov D. Sympathetic nervous system function and dysfunction in chronic hemodialysis patients. Semin Dial. 2013;26(3):333–343. doi:10.1111/sdi.12093
46. Daugirdas JT. Pathophysiology of dialysis hypotension: an update. Am J Kidney Dis. 2001;38(4):S11–7. doi:10.1053/ajkd.2001.28090
47. Daugirdas JT. Dialysis hypotension: a hemodynamic analysis. Kidney Int. 1991;39(2):233–246. doi:10.1038/ki.1991.28
48. Nadala MA, Viera Ramíreza ER, García Vallejoa M, Martín Capóna I, Fernández Lucas M. Effect of Beta-Blocker Cardioselectivity on Vascular Refilling in Hemodialysis Patients. Cardiorenal Med. 2021;11(5–6):237–242. doi:10.1159/000519661
49. Kron J, Schneditz D, Leimbach T, Aign S, Kron S. A simple and feasible method to determine absolute blood volume in hemodialysis patients in clinical practice. Blood Purif. 2014;38(3–4):180–187. doi:10.1159/000368157
50. Heintzen MP, Strauer BE. Peripheral vascular effects of beta-blockers. Eur Heart J. 1994;15(Suppl C):2–7. doi:10.1093/eurheartj/15.suppl_C.2
51. Houston MC, Hodge R. Beta-adrenergic blocker withdrawal syndromes in hypertension and other cardiovascular diseases. Am Heart J. 1988;116(2 Pt 1):515–523. doi:10.1016/0002-8703(88)90627-8
52. Sinha AD, Agarwal R. Clinical pharmacology of antihypertensive therapy for the treatment of hypertension in CKD. Clin J Am Soc Nephrol. 2019;14(5):757–764. doi:10.2215/CJN.04330418
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.