")
Back to Journals » Veterinary Medicine: Research and Reports » Volume 14
Coxiellosis in Livestock: Epidemiology, Public Health Significance, and Prevalence of Coxiella burnetii Infection in Ethiopia
Authors Robi DT , Demissie W, Temteme S
Received 11 May 2023
Accepted for publication 14 August 2023
Published 18 August 2023 Volume 2023:14 Pages 145—158
DOI https://doi.org/10.2147/VMRR.S418346
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Young Lyoo
Dereje Tulu Robi,1 Wondimagegn Demissie,2 Shiferaw Temteme1
1Ethiopian Institute of Agricultural Research, Tepi Agricultural Research Center, Tepi, Ethiopia; 2Jimma University College of Agriculture and Veterinary Medicine School of Veterinary Medicine, Jimma, Ethiopia
Correspondence: Dereje Tulu Robi, Email [email protected]
Abstract: Coxiellosis is a zoonotic disease that is prevalent globally and can pose significant challenges, especially in less developed countries like Ethiopia. Coxiella burnetii is responsible for causing an infection called Q fever in humans and coxiellosis in ruminants. Pneumonia and endocarditis are the only signs that characterize the acute and chronic forms of Q fever, respectively. Ruminants exhibit symptoms such as abortion during the later stages of pregnancy, impaired fertility, perinatal death, premature delivery, and reduced birth weight. C. burnetii infection typically spreads among healthy cattle via tick bites and exposure to infected cattle or their bodily secretions. The primary source of human infection is through the ingestion of contaminated milk and milk products, but transmission through aerosols and dust generated during livestock operations is also common. Cattle, sheep, camels and goats are the primary sources of human infection, and the bacterium can be found in various bodily fluids of infected animals. Several factors, including host characteristics, environmental conditions, and management practices, can potentially affect the occurrence of C. burnetii infection in livestock, such as cattle, camels, sheep, and goats. Coxiellosis is prevalent in Ethiopia’s pastoral and mixed cattle management systems, as individuals frequently interact with cattle and are therefore more prone to exposure to the C. burnetii bacterium. Vaccination and biosecurity measures are effective techniques for managing C. burnetii infection. Therefore, it is crucial to implement appropriate mitigation strategies, raise awareness about the spread of C. burnetii infection, and conduct further studies on C. burnetii infection in high-risk groups.
Keywords: C. burnetii, zoonosis, epidemiology, cattle, sheep, goats, Ethiopia
Introduction
Livestock provides a multitude of benefits, such as animal protein, crop cultivation support, export commodities, fertilization of farmland, household energy, and the potential for wealth accumulation. Despite these and other factors, livestock diseases continue to be a serious problem in some African countries, particularly Ethiopia. Anthrax, rabies, brucellosis, bovine tuberculosis, hydatidosis, cysticercosis, leptospirosis, and Q-fever are among the zoonotic diseases that are currently recognized.1,2 One of the challenges is Query (Q) fever, a bacterial infection affecting both human and animal health. Q-fever is classified as one of the thirteen most significant zoonotic disease worldwide.3,4
Coxiella burnetii (C. burnetii) is a gram-negative bacterium that is capable of causing an infection called Q-fever in humans and coxiellosis in animals. It can remain in a spore state for extended periods of time and is found extensively throughout the environment.5 Many mammals, birds, and arthropods are affected.6 Cattle, goats, and sheep are the primary transmitters of C. burnetii infection to humans.7 Although the disease is asymptomatic, it has been associated to fragile fetuses, late abortions, stillbirths, and infertility.8 Ticks, among the most prevalent arachnids, are one of the most significant arthropods known to serve as reservoirs for C. burnetii. Ticks can spread C. burnetii to their young both transovarially and transstadially by ingesting the blood meals of infected animals.9
Q-fever is a major occupational zoonosis with significant socioeconomic consequences since it is related to exposure to animals. However, it is now understood to impact everyone,10 as the main mode of transmission to humans is inhaling pathogen-contaminated dust or aerosols. Moreover, C. burnetii is extremely resistant and can become airborne, traveling for over a mile on wind currents. Therefore, exposure to C. burnetii can happen even in the absence of direct contact with diseased animals,10,11 and it has caused outbreaks in several countries around the world. Despite its widespread prevalence, the disease is considered neglected, and rarely reported due to its varied signs, self-restricting nature, and lack of diagnostic tools.12 Veterinarians, slaughterhouse workers, animal owners, and scientists involved in animal studies were more affected by Q fever.10 There have not been many detailed epidemiological studies on this bacterium since 1947 when the first case of Q-fever in Africa was reported.13
Recent reports of serological studies on C. burnetii in cattle revealed that humans living in rural areas had significantly higher seroprevalence (27%) in the Somali region.14 Ethiopia faces a significant public health concern due to the proximity between humans and animals and the customary consumption of animal products in their raw form, which increases the risk of zoonotic diseases.15 The occurrence of abortion and infertility in domestic ruminants has become a growing concern in the country.16–20 The high rate of pregnancy loss and resulting infertility among livestock represents a significant economic loss in the country and livestock producers have been severely affected by a major setback to their means of earning a living. Coxiellosis has been recognized as a potential reason for these pregnancy loss episodes since it can affect all three ruminant species (cattle, sheep, and goats). The available data on the epidemiology and zoonotic ramifications of C. burnetii infection among cattle, sheep, and goats in Ethiopia is scarce. Hence, the objective of this paper is to review the current status of C. burnetii infection in Ethiopia, including its epidemiology and zoonotic implications.
C. burnetii Infection: Challenges, Control, and Its Status in Ethiopia
Q-Fever History
In Brisbane, Australia, back in 1935, a group of workers at a slaughterhouse experienced an episode of febrile illness. This disease was then termed “Q” fever by Derrick Edward Holbrook, who could not diagnose it based on patient history, physical examination, and limited investigations.21 Several employees mentioned that the origin of the “Q” was related to Queensland, the state in Australia where the illness was initially discovered. Q fever has been referred to by various names, such as Australian Q-fever, Abattoir fever, Nine Mile fever, and Balkan influenza, reflecting its global presence.22 Q fever has been documented in over 50 countries worldwide. Despite the fact that its symptoms are diverse, it has a self-limited course, and there is no reporting requirement, it is still regarded as a significant public health issue, and its actual occurrence may be underreported.23,24
After the epidemiology of Q fever was understood and it was recognized as a zoonosis, research into the disease fell out of favor. However, Burnet and Freeman25 managed to isolate a fastidious intracellular bacterium from guinea pigs that had been injected with blood or urine from Derrick’s patients. This bacterium was later classified by Philip CB as a new genus, named Coxiella, in 1948. This genus consists of only one species, C. burnetii, which is similar in both morphology and biochemistry to other gram-negative bacteria. C. burnetii has been found in various mammals and ticks and can survive in the environment.26 Despite being first discovered in Africa in 1947, there has been limited epidemiological study on this bacterium, both in terms of quantity and quality.27 As a “category B” bioterrorism agent, C. burnetii is categorized.28
Etiology and Taxonomy
C. burnetii, the bacterial agent responsible for Q fever, is a small gram-negative bacterium with polymorphic properties. It is classified under the family Coxiellaceae, order Legionellales, class Gamma proteobacteria, and phylum Proteobacteria, and belongs to the Coxiella genus.29 The bacterium is an obligate intracellular pathogen that reproduces within an acidic vacuolar compartment, displaying several phagolysosome traits. During its process of development, C. burnetii undergoes morphological changes and exists in two forms: a large, less electron-dense cell variant, and a smaller, more metabolically active intracellular form. The projected period for C. burnetii to double ranges from 20 to 45 hours. Moreover, generation times were computed to be around 11 hours during the phase of exponential growth.30
C. burnetii displays two different antigenic phases, namely Phase I and Phase II, which are determined by the changes in the organism induced through in vitro culture. The antigenicity of the bacteria is due to the lipopolysaccharide (LPS) of the membrane. The smooth phase of Gram-negative bacteria corresponds to phase I antigens, which are more infectious and virulent, while the granular (rough) phase corresponds to Phase II antigens, which are less virulent.31 Coxiella-like bacteria are commonly found in ticks, and a related organism was recently discovered in horses. These discoveries may have an impact on the epidemiology of C. burnetii. Although C. burnetii is reported to occur in over 40 tick species, the accuracy of current PCR tests is questionable as they may also amplify Coxiella-like bacteria, which raises doubts about whether all of these ticks are genuinely infected with C. burnetii.32
Epidemiology of C. burnetii Infection
Location-Based Distribution
C. burnetii infection is a zoonotic disease that has a worldwide distribution and can manifest itself as sporadic cases or as outbreaks. According to recent studies, there is a possibility that it could be considered as an emerging disease, which may be related to climate change.9 Australia has experienced significant Q fever outbreaks in the past. The country has a large livestock industry, and infection rates among people who work closely with animals, such as farmers and abattoir workers, have been notable. The Australian government has implemented successful vaccination campaigns and public health initiatives to manage the disease.33,34 The Netherlands faced a major Q fever outbreak between 2007 and 2010, with thousands of human cases reported. The outbreak was linked to infected goat farms. Since then, the Dutch government has implemented strict control measures, such as culling infected animals, to prevent further outbreaks.35,36 Q fever is present in the United States, with sporadic outbreaks occurring. The risk of infection is higher in agricultural areas where livestock farming is common.37
C. burnetii was first discovered in Africa in 1947. The prevalence of Q fever varies across different regions of Africa due to various factors, including livestock farming practices, awareness and surveillance measures, and healthcare infrastructure.38 Some African countries may have higher incidence rates of Q fever due to the close interaction between humans and animals in agricultural settings, limited awareness of the disease, and challenges in diagnosing and reporting cases. In areas where livestock farming is more intensive, Q fever may be more common.3,39 It is crucial to recognize that the epidemiological situation may vary significantly between countries. Accurate data and research are vital for understanding the true burden of Q fever and implementing effective control measures.40
In Ethiopia, like in many other countries, C. burnetii infection is a significant public health concern. Due to the country’s agrarian nature, where a large proportion of the population depends on livestock farming, the risk of transmission from animals to humans is relatively high.14,41 Furthermore, Ethiopia faces challenges in terms of healthcare infrastructure and access to proper diagnostic and treatment facilities in rural areas, which may impede early detection and effective management of the C. burnetii infection. Moreover, factors like climate change, changing agricultural practices, and population movement could also influence the prevalence and distribution of the disease in Ethiopia.14,16 One research study carried out in Ethiopia have shown that 6.5% of abattoir workers in Addis Ababa were seropositive for C. burnetii, and that goats and sheep slaughtered in the same area and its peri-urban zones also had C. burnetii antibodies.42
Reservoirs and Host Range of C. burnetii Infection
C. burnetii can be found in various wild and domestic animals, including mammals, birds, and arthropods like ticks, which act as reservoirs for the bacteria.43 Ticks are particularly important, as they allow the bacteria to multiply within their midgut and stomach cells. The bacteria are then excreted in the saliva and feces of ticks.44 Human infections with C. burnetii are primarily linked to farm animals, such as cattle, goats, and sheep, while urban outbreaks of the disease may be attributed to pets, including cats, rabbits, and dogs.45
Livestock, which comprises animals such as cattle, sheep, camels, and goats, is recognized as the primary host and origin of infection for humans.46,47 C. burnetii has also been detected in various wild creatures, including roe deer, wild boars, rodents, European hare, Pacific harbour seals, Steller sea lions, Northern fur seals, and harbour porpoises, in both land-based and marine environments.48,49 In the wildlife of the Netherlands, roe deer and rats have been found to have C. burnetii infection.50 However, human cases of Q fever are typically observed clinically, and cattle, sheep, and goats are considered the primary sources of human infection.51
Source of Infection and Transmission Methods
Animal Source of Infection and Transmission Methods
C. burnetii likely persists through animal infection via tick bites, which may also spread the infection among wild vertebrates, including rodents, lagomorphs, and wild birds.52–54 In female animals, C. burnetii is present in the uterus and mammary glands, and is expelled into the environment through birth products, feces, urine, and milk.53,55 Dogs and wild carnivores may become infected through consuming contaminated ruminant placenta or birth products, or via aerosol transmission.56 Ticks are not essential for C. burnetii’s life cycle, but they could play a role in transmitting the infection among animals, including both wild and domestic animals.57 Nursing calves may also contract the infection through their mother’s milk, with over 90% of dairy herds in the northeastern United States infected with C. burnetii based on surveillance of bulk milk samples.58
Source of Infection and Transmission Methods in Humans
The potential source of human infection for Q fever is through the ingestion of contaminated milk and milk products. However, this mode of transmission has not been conclusively proven in experimental studies. However, several recent studies have proven Q fever transmission through pasteurized and unpasteurized milk.59,60 Human-to-human transmission has occurred in rare, sporadic cases, such as during autopsies and contact with pregnant women.61 The microorganism, C. burnetii, can be found in various bodily fluids of infected animals, including milk, urine, feces, placenta, and birth fluids. Humans typically contract the infection by inhaling contaminated dust or aerosols that are generated during livestock operations involving cattle, camels, sheep, and goats.17–19,62 In laboratory settings, even the inhalation of a single C. burnetii bacterium can cause human infection and clinical disease. The bacteria can also be transmitted indirectly through the handling of contaminated farm materials like utensils, straw, manure, or dust from farm vehicles. Domestic ruminants like cattle, sheep, and goats are the primary sources of human infection.12 During parturition, these animals can release large amounts of bacteria through amniotic fluid and fetal membranes, which can lead to contamination by aerosols.63 The bacterium can also be transmitted through the air, which means that even people who have no direct contact with animals can become infected.47
Risk Factors
Agent Factors
The severity of Q fever in humans caused by C. burnetii varies among different strains of the bacterium.64 Strains I, II, and III are more likely to result in acute infections, while strains IV and V are associated with chronic infections. Currently, there is no available information on the virulence of strain VI.65,66
Host Factors
The occurrence of Q fever in humans is influenced by various host factors, such as age and gender. The most vulnerable age group is between 30–60 years old, and the disease is more commonly found in men.67 Certain individuals are at a higher risk of infection or seropositivity, including those with a previous history of valvulopathy, immunosuppressive diseases like AIDS, pregnant women, veterinarians, animal farm workers, abattoir workers, laboratory personnel, and immunosuppressed individuals.32,68 In animals, the prevalence of C. burnetii infection increases with age or the number of pregnancies in cattle and sheep. Prevalence is higher in dairy cows compared to beef cattle, and sheep flock size can also affect seroprevalence.69
Season, Environment and Management Factors
It has been observed that there is a seasonal fluctuation in human Q fever cases, but the precise pattern differs based on the location. Q fever cases are frequently documented during the spring or early summer months, though the incidence appears to be more closely linked to rainfall than a particular season.70 Individuals residing near animals carrying the infection or in regions with a high concentration of livestock are at a greater risk of developing Q fever.71 Animal management strategies, such as housing methods and segregation of newly introduced animals, can also impact the prevalence of C. burnetii infection among animals.68,69
Clinical Manifestations
Clinical Manifestations of Coxiellosis in Animal
The clinical manifestations of coxiellosis are generally non-specific in most animals, but they can cause various reproductive issues in ruminants, particularly in cases where C. burnetii is present. These issues include reduced fertility, late-term abortion, perinatal mortality, premature delivery, and low birth weight. Aborted fetuses may appear normal, and the percentage of abortions can range from 3% to 80%. Infected animal placentas display exudates and intracotyledonary fibrous thickening. Goats may experience a severe inflammatory response in the myometrium, while cattle frequently experience metritis as a result of the disease.9,70
Sign of C. burnetii Infection in Human
The infection caused by C. burnetii in humans can lead to three different types of illnesses, namely asymptomatic, acute, or chronic. The symptoms of Q fever can differ greatly, with some individuals not experiencing any symptoms at all, while others may develop flu-like symptoms, severe pneumonia, or chronic endocarditis. The clinical presentation of the disease may be influenced by host factors such as age, gender, and pre-existing medical conditions. Individuals who are older than 15 years are more likely to exhibit clinical symptoms.72,73
Acute C. burnetii Infection
The incubation period of Q fever is typically 20 days, but can range from 3 to 30 days. Although approximately 50–60% of those infected with Q fever may not experience any symptoms, symptomatic patients can present with over 30 different clinical syndromes.72,73 Symptoms of acute Q fever may include a sudden onset of fever (up to 40°C-40.5°C), chills, profuse sweating, severe headache with retro-orbital pain, weakness, nausea, vomiting, diarrhea, non-productive cough, and abdominal or chest pain. Without treatment, the fever may last for up to 9 to 14 days.74 Pneumonia is observed in approximately 30–50% of cases, while acute hepatitis, meningoencephalitis, and myocarditis are also possible. Abnormal liver function tests and thrombocytopenia are common. Although pregnant women are believed to have an increased risk of pre-term delivery or miscarriage, a study from the Netherlands did not find any association between seropositive status and elevated risk.10,75 A study has described other acute disease manifestations, which can affect nearly every organ system.72
Chronic C. burnetii Infection
Chronic Q fever typically manifests as endocarditis, which occurs after several weeks to years following an acute infection.76 Certain individuals are at a higher risk of developing chronic Q fever, such as those with immunosuppression, heart valve lesions, vascular abnormalities, and pregnancy.72 Endocarditis is the most common form of chronic Q fever, accounting for 60–70% of cases and representing 3–5% of all endocarditis cases.72,76 Recent studies have provided new insights into endocarditis in Q fever. While immunosuppression was previously considered a risk factor, recent evidence indicates that underlying valvulopathies pose a greater risk.76 Moreover, minor valvular abnormalities like mitral valve prolapse, bicuspid aortic valve, and minor valvular leak may also contribute to endocarditis.77 The risk of developing endocarditis is reported to be 75% in patients with untreated underlying valvulopathies.76 In one study, patients who received only doxycycline had a 50% chance of developing endocarditis, whereas those who were treated with both doxycycline and hydroxychloroquine did not develop endocarditis.76 Vascular infections are the second most common form of chronic Q fever, with aortic aneurysms or vascular grafts being frequently involved, as reported in a study of 30 cases in France.78
Pathogenesis
The precise mechanism by which C. burnetii infects animals and humans is not well understood. Research indicates that the bacterial LPS is significant in the development of Q fever in animals and humans.56 The bacterium is believed to enter the lungs and intestine via the oropharyngeal route. Q fever is highly contagious, and even a small number of bacteria can cause infection. After initial entry, the pathogen multiplies in the regional lymph nodes, resulting in transient bacteremia that lasts for 5–7 days.29
C. burnetii undergoes a biphasic life cycle, alternating between a replicating large cell variant (LCV) and a non-replicating, infectious small cell variant (SCV). The SCV is highly resistant to environmental conditions due to its spore-like structure, which includes highly condensed chromatin.30 One variant is a large cell variant (LCV) that is active metabolically and found inside cells. The LCV has the ability to replicate and is larger and less electron-dense. The other variant is a small cell variant (SCV) that is spore-like and has a unique morphology and function. The SCV is rod-shaped and compact with a dense central region. It is considered metabolically inactive and less likely to replicate.79,80
Animals that are infected with C. burnetii release small cell variants (SCVs) that attach to the cell membrane of phagocytic cells. Once the phagosome containing the SCV merges with the lysosome, the SCVs can grow and develop into large cell variants (LCVs). Both LCVs and activated SCVs can divide by binary fission, while LCVs can also undergo sporogenic differentiation.12 These spores can mature into metabolically inactive SCVs, which can be released from the infected host cell via cell lysis or exocytosis. C. burnetii’s entire development cycle occurs in acidic phagolysosomes, which safeguard the pathogen from the host’s microbicidal actions and the impact of antibiotics.81 The SCV and spore forms are more resistant to denaturation than LCVs. Moreover, the acidic environment reduces the effectiveness of antibiotics against C. burnetii.82
C. burnetii undergoes changes in antigenicity during in vitro culture resulting in two distinct antigenic phases, Phase I and Phase II. Antibodies against Phase II are produced early in the infection, while antibodies against Phase I become predominant if the infection persists. This switch is useful in differentiating acute and chronic infections in humans, although it is not applicable in animals. Phase I bacteria are isolated from infected humans, animals, and arthropods and have a smooth full-length LPS. In contrast, the wild virulent type Phase I bacterium changes to virulent Phase II with rough LPS after multiple passages in embryonated egg or cell cultures.12,83 C. burnetii’s virulence and pathogenicity are associated with its genetic characteristics, plasmid groups, strain types, and host factors such as pregnancy.66,84
Diagnosis
The symptoms of Q fever are not unique and can be observed in both animals and humans, making it crucial to confirm the diagnosis through laboratory tests. There are four types of diagnostic tests accessible, including isolation of the organism with the use of biosafety-level 3 laboratory procedures, serologic tests like IFA, ELISA, complement fixation, antigen detection assays like IHC, and nucleic acid detection assays such as PCR.85
To identify the pathogen, it is necessary to obtain appropriate samples such as placenta, vaginal mucus, milk, colostrum, feces, and various tissues from the aborted fetus (such as liver, lung, and stomach contents). Various techniques, including staining methods (stamp, Gimenez, Machiavello, or Giemsa) are available for identifying C. burnetii. Although some techniques can be used to detect certain pathogens, such as Brucella spp or Chlamydia spp, they may not be reliable due to their low sensitivity and specificity, which may lead to false-positive results.85 For this reason, experts suggest using serological analysis with complement fixation or ELISA to improve accuracy.
Routine veterinary diagnosis usually does not involve isolating the bacteria due to various reasons, including the agent’s zoonotic nature, the need for specialized BSL3 laboratories, expertise, and the time-consuming testing process. Nonetheless, isolation methods, such as shell-vial cell culture or culture in embryonated eggs’ yolk sacs, can be utilized to achieve isolation.86 To detect C. burnetii inclusions in the cytoplasm of endodermal cells, smears of yolk sacs can be prepared and stained using the Gimenez method.
Serological Diagnosis
The Complement Fixation Test (CFT) is a method to detect complement-fixing antibodies in serum. Although it is specific, it is less sensitive than ELISA or IFA tests.51,87 While Immunofluorescence Assay (IFA) is species-specific, it is not commonly used for diagnosing C. burnetii infection in animals. However, it is widely used for diagnosing human infections. IFA can distinguish between acute and chronic infections by analyzing the ratio of phase I and phase II IgG antibodies. Notably, there is no commercially available kit for veterinary investigations using IFA.88
The Enzyme-linked Immunosorbent Assay (ELISA) is a recommended diagnostic tool for sero-epidemiological studies in animals due to its high sensitivity and good specificity, which allows it to detect antibodies against both phase I and phase II. ELISA has been shown to be more sensitive than the Complement Fixation Test (CFT) in animal studies. While CFT is a quick diagnostic technique that can test a large number of samples at the same time and is commonly used for sero-epidemiological studies in animals, ELISA has been found to have higher sensitivity than both CFT and IFA in human studies.51,69,87
Molecular Diagnosis
Polymerase chain reaction (PCR) is an effective method for detecting C. burnetii DNA in cell cultures and clinical samples. This is achieved through the use of PCR techniques, which offer high sensitivity and specificity.89 PCR has been rapidly and effectively employed to diagnose Q fever in veterinary science, improving the accuracy of detection.90
Differential Diagnosis
Numerous diseases share similar symptoms with Q fever, including brucellosis, salmonellosis, leptospirosis, listeriosis, campylobacteriosis, influenza, and rickettsia infection. During the early stages, influenza may be considered due to its similar presentation. Listeriosis, also known as “circling disease”, can cause fever, blindness, head pressing, and placental necrosis leading to abortion. Brucella can cause female animal abortion during the seventh month of pregnancy, as well as placental retention and metritis. In males, Brucella can cause epididymitis, orchitis, synovitis, and sterility. Salmonellosis can result in foul-smelling diarrhea, fever, dehydration, and abortion in the last two months of gestation. Leptospirosis can lead to excessive salivation, conjunctivitis, hemoglobinuria, muscular rigidity, jaundice, and mucosal pallor. Leptospiral abortion can occur with or without placental degeneration and encephalitis. Typically, abortion happens 3–4 weeks later, and affected animals are often discovered dead due to septicemia.68
Public Health Significance
Q-fever is a global public health issue that has been identified in over 59 countries.91 The infection occurs in humans when they inhale contaminated dust generated from infected manure and placenta, leading to the formation of aerosols. C. burnetii can be carried by the wind, spreading to urban areas where people may not have direct contact with infected animals.92 While groups such as veterinarians, laboratory workers, farmers, and abattoir workers are at higher risk, birds can also transmit the disease to humans in urban areas through their feces or ectoparasites.93
While Q fever does not always cause illness, individuals who contract the disease may experience symptoms such as headache, muscle pain, sore throat, nausea, vomiting, chest and stomach pains, as well as a high fever that can persist for up to two weeks. Pneumonia or liver complications may also arise. Those with weakened immune systems or pre-existing heart valve issues are at higher risk of severe complications, which can lead to fatality. Furthermore, some individuals may develop chronic fatigue as a post-Q fever syndrome. There have been multiple outbreaks involving 15 or more people, making Q fever the second most commonly reported laboratory infection.94
The first encounter with C. burnetii in humans can cause either no noticeable symptoms or only mild infection.32 However, it can also result in acute or chronic illness. Diagnosing Q fever clinically can be difficult due to its wide range of manifestations, and the factors contributing to this variability are largely unknown. Nevertheless, certain risk factors for severe forms of the disease have been identified, such as pregnancy, immunosuppression, pre-existing heart valve abnormalities, and the presence of vascular grafts or aneurysms.56
Treatment of C. burnetii Infection
Treatment in Animal
The available information on the effectiveness of antibiotic treatments in animals for decreasing the occurrence of C. burnetii-related abortions and bacterial shedding during parturition is limited. Administration of Oxytetracycline injections at a dose of 20 mg/kg body weight twice during the final trimester of pregnancy is a common practice, but it may not offer complete protection against abortions or bacterial shedding during parturition.95 The primary aim of using antimicrobial treatment is to minimize the shedding of the bacterium in the birth fluids and placenta, rather than eradicating it altogether. However, despite treatment, there is still a chance of C. burnetii shedding during parturition and occurrence of abortions.9,47
Treatment in Human
Acute Q-fever usually resolves on its own and antimicrobial therapy is not necessary for many patients who recover without treatment. Treatment for acute Q-fever is not typically recommended for individuals without symptoms or those whose symptoms have disappeared. However, it may be considered for individuals who have a high risk of developing chronic Q fever, such as those with valvular heart disease, vascular graft, aneurysm, or immunosuppression. The standard treatment for acute Q-fever involves taking Doxycycline at a daily dosage of 200 mg for two weeks. For patients who are allergic to Doxycycline, pregnant, or younger than 8 years old, cotrimoxazole and rifampin are alternative options that are also effective in treating Q-fever. Pregnant women are recommended to take cotrimoxazole with folic acid for more than 5 weeks.12,46,96
The mentioned treatment for chronic Q fever in adults involves taking a combination of 100 mg doxycycline every 12 hours and 200 mg hydroxychloroquine every 8 hours for duration of 18 months. Although doxycycline and rifampin have been suggested as an alternative treatment, its effectiveness may be limited due to drug interactions. Patients who are receiving extended hydroxychloroquine treatment must undergo ophthalmologic examination once every 12 months. Prior to beginning hydroxychloroquine therapy, at-risk individuals should be tested for glucose-6-phosphate dehydrogenase deficiency. Furthermore, patients who are taking doxycycline should be informed about the possibility of photosensitivity. Approximately 9% of cases of chronic Q fever result in endovascular complications, and surgery, such as aortic aneurysm repair or graft replacement, may be necessary in these cases.46
Control and Prevention
To minimize the spread of C. burnetii infection in animals during an outbreak, certain sanitation measures should be taken. These may include modifying farming practices, such as covering or ploughing manure and treating it with lime or calcium cyanide, as well as disposing of animal birth and abortion products. Disinfecting infected premises, paths, and holding areas, as well as implementing a farm animal breeding program are also recommended.97 However, it is uncertain how effective these measures are, as the prevalence of the infection in an affected herd typically decreases over time, even without specific control measures. It is possible that this is due to natural immunization of suspected animals.95
Vaccinations
Research findings indicate that animal vaccinations have proven effective in reducing abortion rates, C. burnetii shedding, and the occurrence of infections. Vaccinating already infected herds can also help to control outbreaks.97 The inactivated phase I vaccine has demonstrated the ability to safeguard against abortion and lower the levels of bacterial shedding in bodily fluids such as vaginal mucus, feces, and milk. Killed vaccines are capable of eliciting a strong and long-lasting antibody response, thereby limiting bacterial excretion. Notably, the phase I vaccine has been shown to be 100 times more effective in preventing colonization of the mouse spleen than phase II vaccines. In 1989, the Australian government approved the use of a formaldehyde-inactivated vaccine, which was derived from the phase I C. burnetii strain.97 Similarly, the European Union has provisionally licensed an inactivated Nine Mile strain phase I vaccine for use in cattle and goats as a long-term control measure. With regards to human vaccination, the aim is to minimize the risk of clinical Q fever in previously unexposed individuals. The formalin-inactivated Henzerling strain phase I whole-cell vaccine has been licensed for use in humans and is recommended for high-risk, occupationally-exposed individuals who are seronegative.98,99
Bio-Securities
C. burnetii has been categorized as a group B bioterrorism agent by the CDC in the USA, owing to its high morbidity rate and remarkably low infectious dose.100 Single bacterium infections have been documented in both humans and guinea pigs.101,102 Therefore, the EU has classified C. burnetii as a containment level 3 organism, which necessitates the use of bio-safety level 3 laboratories and animal facilities, as well as well-trained and experienced personnel to work with them. To ensure the safety of the personnel handling C. burnetii, it is essential to establish emergency procedures and implement medical monitoring.103
Challenges and Strategies for Control and Prevention of C. burnetii Infection
C. burnetii is a type of bacteria that causes Q fever, a disease that can be passed from animals to humans and can have significant implications for public health and the economy. Despite its potential impact, the extent of C. burnetii infection in Ethiopia has not been thoroughly investigated, and there is a need for improved strategies to prevent and control it.
The absence of dependable diagnostic tools presents a significant obstacle to managing C. burnetii infection. The symptoms of Q fever in humans are vague and do not allow for easy diagnosis without serological testing. Furthermore, the variability of antibody titers and the lack of clinical symptoms frequently result in underreporting of C. burnetii seroprevalence in ruminants. Consequently, it is necessary to devise more sensitive and precise diagnostic methods, such as PCR and antigen detection tests, to correctly identify C. burnetii infection in both animals and humans.104
The absence of adequate knowledge and consciousness about the ailment among farmers, veterinarians, and public health officers is yet another hurdle. Insufficient tracking and documentation of Q fever cases in Ethiopia also obstruct the application of efficient control measures. Consequently, it is imperative to raise awareness and educate all concerned parties about the disease, how it spreads, and preventive measures. Moreover, enhancing communication and cooperation between the veterinary and public health domains can aid in the timely recognition and management of outbreaks.97
There are various methods available for managing and preventing the spread of C. burnetii infection. One approach that has demonstrated efficacy in reducing the frequency and amount of C. burnetii shed in ruminants is vaccination. The use of antibiotics such as doxycycline and oxytetracycline has also been suggested to control the disease in animals, although this approach is not sustainable in the long term due to the development of antibiotic resistance.105 Furthermore, implementing good hygiene practices, such as regular cleaning and disinfection of animal premises, can reduce the risk of environmental contamination and transmission.
In humans, prevention measures include avoiding contact with infected animals and their products, wearing personal protective equipment, and practicing good hygiene, particularly in high-risk occupations such as farming and veterinary medicine. Health education and public awareness campaigns can also be effective in preventing the spread of the disease among the general population.106
Status of Coxiella burnetii Infection in Ethiopia
Antibodies against Coxiella burnetii have been identified in goats and sheep that were slaughtered in and around the Addis Ababa abattoir in Ethiopia. According to a study, the use of CFT revealed a seroprevalence of 6.5% among abattoir workers in Addis Ababa.107 A recent report demonstrated that humans residing in rural areas had a substantially higher seroprevalence (27%) for C. burnetii in the Somali region using indirect ELISA.14 To detect C. burnetii in ticks in Ethiopia, Quantitative RT-PCR that targeted two different genes and multispacer sequence typing were employed. As a result, the overall prevalence was determined to be 6.4%. Amblyomma gemma (28.6%) and Rhipicephalus pulchellus (25%) had the highest rates of C. burnetii detection among other tick species. Bersissa et al29 noted that these two tick species had significantly higher frequencies of C. burnetii DNA. Q fever is one of the infectious diseases leading to abortions in Ethiopia, which is a significant reproductive health concern for dairy cows due to its economic consequences involving both infectious and non-infectious factors.17 Tsouloufi et al108 noted that Q-fever, a zoonotic disease with considerable socio-economic consequences, is emerging in Ethiopia. However, only a limited number of studies have been carried out, indicating the need for additional research in the future.
The prevalence of Coxiella burnetii infection varied among the different livestock species and study locations. The highest prevalence was reported in camels from Southeast Ethiopia (90.0%), followed by goats from the same region (54.2%). In contrast, the lowest prevalence was reported in cattle from Jimma town (8.8%) and Somali region (9.6%). Sheep and goats in Menza and Horro areas had a high prevalence of infection at 68.3% and 73.3% respectively, while the prevalence in Borana areas was relatively lower at 18.3% and 35.5% for sheep and goats respectively. Overall, the results suggest that Coxiella burnetii infection is widespread in livestock populations in Ethiopia, with varying levels of prevalence depending on the species and location (Table 1).
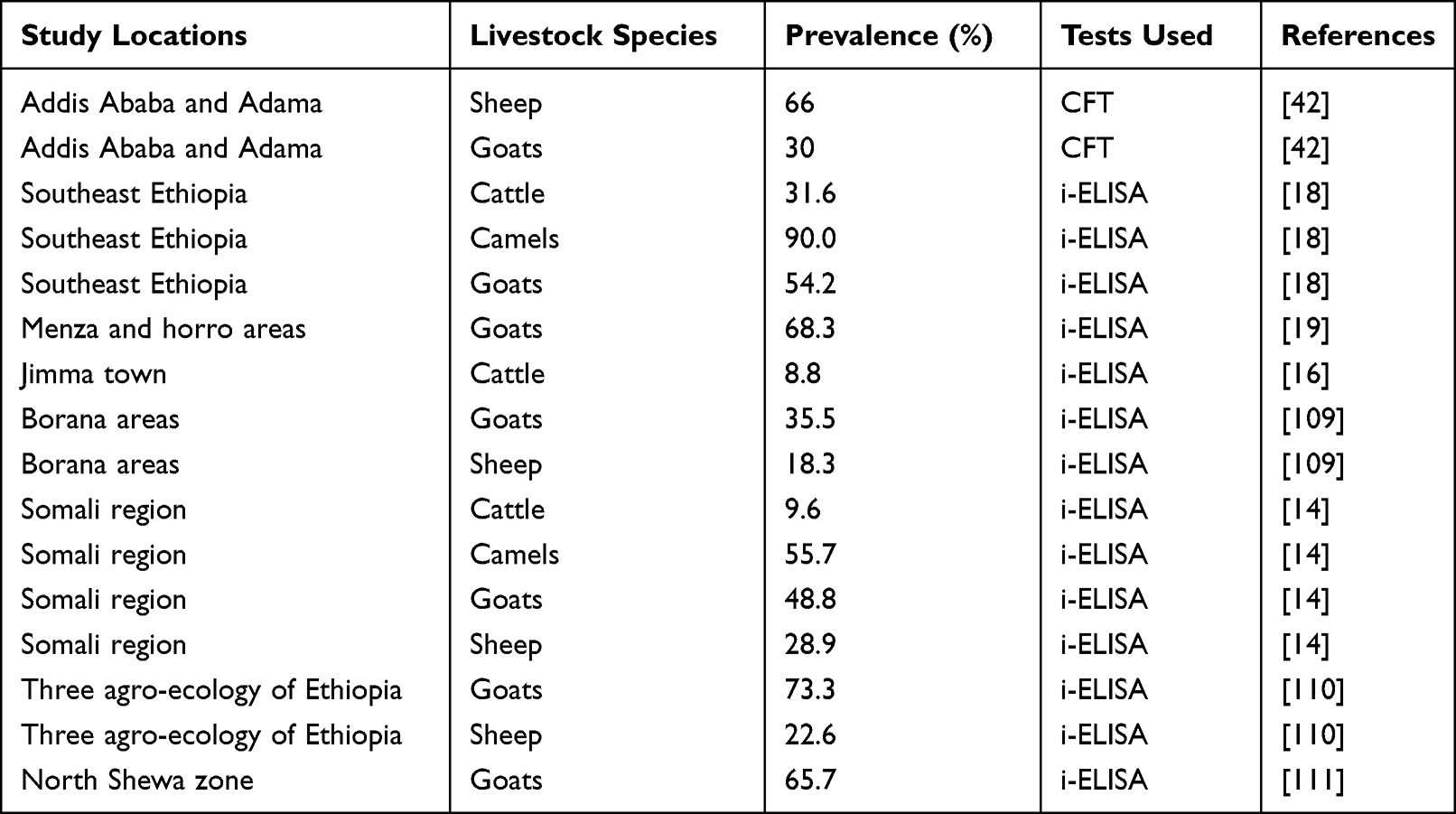 |
Table 1 Prevalence of Coxiellosis in Different Species of Livestock in Ethiopia(from 1966–2021) |
Conclusion
The infection caused by C. burnetii is a notable concern in Ethiopia. Its impact on cattle production and potential harm to human health cannot be overlooked. The spread of the infection is impacted by a range of factors, including age, herd size, production methods, and agro-ecological conditions. Human transmission of the infection primarily occurs through direct exposure to infected cattle or consumption of unpasteurized milk. Vaccination and biosecurity are the most effective techniques for managing C. burnetii infection. Raising awareness within the community about the zoonotic transmission of C. burnetii infection is crucial in preventing its spread. Effective control measures such as biosecurity practices, proper disposal of aborted fetuses, and pasteurization or boiling of milk before consumption should be used to minimize the risk of transmission. C. burnetii infection is widespread in livestock populations in Ethiopia, with varying levels of prevalence depending on the species and location. In addition, efficient management approaches such as acaricidal should be established to mitigate tick infestation and cattle contact with wild animals. To control C. burnetii infection, one health approaches should be encouraged. In order to gain a better understanding of the prevalence of C. burnetii infection in both animals and humans, further research is necessary. It is vital to implement the suggested measures to effectively manage the infection and mitigate its negative effects on cattle production and public health in Ethiopia.
Acknowledgments
We would like to express our sincere gratitude to the Ethiopian Institute of Agricultural Research (EIAR) for their valuable assistance during this review. Their expertise and support have been instrumental in ensuring the accuracy and quality of our work. We would also like to extend our heartfelt thanks to all the individuals and organizations who contributed to this review.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tesfaye D, Fekede D, Tigre W, Regassa A, Fekadu A. Perception of the public on the common zoonotic diseases in Jimma, South western Ethiopia. Intl J Med Med Sci. 2013;5(6):279–285.
2. Pieracci EG, Aron JH, Radhika G, et al. Prioritizing zoonotic diseases in Ethiopia using a one health approach. One Health. 2016;2:131–135. doi:10.1016/j.onehlt.2016.09.001
3. Njeru J, Henning K, Pletz MW, Heller R, Neubauer H. Q fever is an old and neglected zoonotic disease in Kenya: a systematic review. BMC Public Health. 2016;16(1):297. doi:10.1186/s12889-016-2929-9
4. Johnson SAM, Kaneene JB, Asare‐Dompreh K, et al. Seroprevalence of Q fever in cattle, sheep and goats in the Volta region of Ghana. Vet Med Sci. 2019;5(3):402–411. doi:10.1002/vms3.160
5. OIE. Manual of diagnostic tests and vaccines for terrestrial animals. In: Q Fever. World Organization for Animal Health; 2010:1–13.
6. Bond KA, Vincent G, Wilks CR, et al. One Health approach to controlling a Q-fever outbreak on an Australian goat farm. Epidemiol Infect. 2016;144(6):1129–1141. doi:10.1017/S0950268815002368
7. Brandwagt DA, Herremans T, Schneeberger PM, et al. Waning population immunity prior to a large Q fever epidemic in the south of The Netherlands. Epidemiol Infect. 2016;144(13):2866–2872.
8. Wardrop NA, Thomas F, Cook EA, et al. The sero-epidemiology of Coxiella burnetii in humans and cattle, Western Kenya: evidence from a cross-sectional study. PLoS Negl Trop Dis. 2016;10(10):e0005032. doi:10.1371/journal.pntd.0005032
9. Arricau-Bouvery N, Rodolakis A. Is Q-fever an emerging or re-emerging zoonosis? Vet Res. 2005;36:327–349. doi:10.1051/vetres:2005010
10. Van der Hoek W, Hunink J, Vellema P, Droogers P. Q fever in The Netherlands: the role of local environmental conditions. Int J Environ Health Res. 2011;21(6):441–451. doi:10.1080/09603123.2011.574270
11. Anderson A, Bijlmer H, Fournier J, et al. Diagnosis and management of Q- fever United States. Recommendations from the CDC and the Q Fever Working Group. MMWR. 2013;62(3):
12. Angelakis E, Raoult D. Q-fever. Vet Microbiol. 2010;140(3–4):297–309. doi:10.1016/j.vetmic.2009.07.016
13. Garcia II, Lopez HI, Tutusaus J, Serrano B, Monleon E. Coxiella burnetii shedding during the peripartum period and subsequent fertility in dairy cattle. Reprod Domestic Anim. 2013;48:441–446. doi:10.1111/rda.12095
14. Ibrahim M, Schelling E, Zinsstag J, Hattendorf J, Andargie E, Tschopp R. Sero-prevalence of brucellosis, Q-fever and Rift Valley fever in humans and livestock in Somali Region, Ethiopia. PLoS Negl Trop Dis. 2021;15(1):e0008100. doi:10.1371/journal.pntd.0008100
15. Ghaoui H, Achour A, Temim S, Smai A, Temim S, Bitam I. Between Livestock’s and humans, Q Fever disease is emerging at low noise. New Microbes New Infect. 2019;27. doi:10.1016/j.nmni.2018.11.007
16. Deressa FB, Kal DO, Gelalcha BD, Magalhães RJS. Seroprevalence of and risk factors for Q fever in dairy and slaughterhouse cattle of Jimma town, South Western Ethiopia. BMC Vet Res. 2020;16(1):1–10. doi:10.1186/s12917-020-02598-8
17. Tulu D, Deresa B, Begna F, Gojam A. Review of common causes of abortion in dairy cattle in Ethiopia. J Vet Med Anim Health. 2018;10(1):1–13. doi:10.5897/JVMAH2017.0639
18. Gumi B, Firdessa R, Yamuah L, Sori T, Tolosa T, Aseffa A. Seroprevalence of brucellosis and Q fever in southeast Ethiopian pastoral livestock. J Vet Sci Med Diagnosis. 2013;2(1). doi:10.4172/2325-9590.1000109
19. Gebretensay A, Alemayehu G, Rekik M, et al. Risk factors for reproductive disorders and major infectious causes of abortion in sheep in the highlands of Ethiopia. Small Ruminant Res. 2019;177:1–9. doi:10.1016/j.smallrumres.2019.05.019
20. Robi DT, Bogale A, Urge B, Aleme M, Temteme S. Neglected zoonotic bacteria causes and associated risk factors of cattle abortion in different agro-ecological zones of southwest Ethiopia. Vet Immunol Immunopathol. 2023;259:110592. doi:10.1016/j.vetimm.2023.110592
21. Derrick EH. ”Q” fever, a new fever entity: clinical features, diagnosis and laboratory investigation. Rev Infect Dis. 1983;5(4):790–800. doi:10.1093/clinids/5.4.790
22. McDade J. Historical aspects of Q fever. In: Marrie T, editor. Q Fevers. Volume I. The Disease. Boston: CRC Press; 1990:5–21.
23. Richardus JH, Dumas AM, Huisman J, Schaap GJP. Q fever in infancy: a review of 18 cases. Pediat Infect Dis. 1985;4(4):369–373. doi:10.1097/00006454-198507000-00007
24. Marrie T. Epidemiology of Q fever. Rickettial Dis. 2007;2007:281–289.
25. Fournier PE, Marrie TJ, Raoult D. Diagnosis of Q fever. J Clin Microbiol. 1998;36(7):1823–1834. doi:10.1128/JCM.36.7.1823-1834.1998
26. Abou Abdallah R, Million M, Delerce J, et al. Pangenomic analysis of Coxiella burnetii unveils new traits in genome architecture. Front Microbiol. 2022;13:1022356. doi:10.3389/fmicb.2022.1022356
27. Dupont HT, Brouqui P, Faugere B, Raoult D. Prevalence of antibodies to Coxiella burnetii, Rickettsia conorii, and Rickettsia typhi in seven African countries. Clin Infect Dis. 1995;21(5):1126–1133. doi:10.1093/clinids/21.5.1126
28. Artenstein AW. Bioterrorism and Biodefense. Infect Dis. 2017;670–679.e1. doi:10.1016/B978-0-7020-6285-8.00075-7
29. Bersissa K, Cristina S, Lionel A, Didier R, Philippe P. Occurrence and Genotyping of Coxiella burnetii Ixodid Ticks in Oromia, Ethiopia. Am J Trop Med Hyg. 2015;93(5):1074–1081. doi:10.4269/ajtmh.14-0758
30. Coleman SA, Fischer ER, Howe D, Mead DJ, Heinzen RA. Temporal analysis of Coxiella burnetii morphological differentiation. J Bacteriol. 2004;186(21):7344–7352. doi:10.1128/JB.186.21.7344-7352.2004
31. Tolera T. Q-fever in small ruminants and its public health importance. Dairy and Vet Sci J. 2019;9(1):001–010.
32. Centre for Food Security and Public Health (CFSPH). Centre for Food Security and Public Health, Q Fever: Query Fever, Coxiellosis, Abattoir Fever, Iowa State University, College of Veterinary Medicine. Centre for Food Security and Public Health; 2017.
33. Gidding HF, Wallace C, Lawrence GL, McIntyre PB. Australia’s national Q fever vaccination program. Vaccine. 2009;27(14):2037–2041. doi:10.1016/j.vaccine.2009.02.007
34. Mathews KO, Savage C, Norris JM, et al. Risk factors associated with self-reported Q fever in Australian wildlife rehabilitators: findings from an online survey. Zoonoses Public Health. 2023;70(1):69–80. doi:10.1111/zph.13002
35. Whelan J, Schimmer B, Schneeberger P, et al. Q fever among culling workers, the Netherlands, 2009-2010. Emerg Infect Dis. 2011;17(9):1719–1723. doi:10.3201/eid1709.110051
36. Koeijer AAD, Hagenaars TJ, Leuken J, Swart AN, Boender GJ, Gregori L. Spatial transmission risk during the 2007–2010 Q fever epidemic in The Netherlands: analysis of the farm-to-farm and farm-to-resident transmission. PLoS One. 2020;15(2):e0227491. doi:10.1371/journal.pone.0227491
37. Karakousis PC, Trucksis M, Dumler JS. Chronic Q fever in the United States. J Clin Microbiol. 2006;44(6):2283–2287. doi:10.1128/JCM.02365-05
38. Sadiki V, Gcebe N, Mangena ML, Ngoshe YB, Adesiyun AA. Prevalence and risk factors of Q fever (Coxiella burnetii) in cattle on farms of Limpopo province, South Africa. Front Vet Sci. 2023;10:1101988. doi:10.3389/fvets.2023.1101988
39. Mori M, Roest HJ. Farming, Q fever and public health: agricultural practices and beyond. Arch Public Health. 2018;76(2). doi:10.1186/s13690-017-0248-y
40. Vanderburg S, Rubach MP, Halliday JEB, Cleaveland S, Reddy EA, Crump JA. Epidemiology of Coxiella burnetii infection in Africa: a ONE HEALTH SYSTEMATIC REVIEW. PLoS Negl Trop Dis. 2014;8(4):e2787. doi:10.1371/journal.pntd.0002787
41. Proboste T, Deressa FB, Li Y, Kal DO, Gelalcha BD, Soares Magalhães RJ. Geographical variation in Coxiella burnetii seroprevalence in dairy farms located in South-Western Ethiopia: understanding the broader community risk. Pathogens. 2021;10(6):646. doi:10.3390/pathogens10060646
42. Philip C, Hoogstraal H, Reiss-Gutfreund R, Clifford C. Evidence of rickettsial disease agents in ticks from Ethiopian cattle. Bull World Health Organ. 1966;35(2):127–131.
43. Schimmer B, Ter Schegget R, Wigwam M, Buchner L, de Bruin A. The use of a geographic information system to identify a dairy goat farm as the most likely source of an urban Q-fever outbreak. BMC Infect Dis. 2010;10(1):69. doi:10.1186/1471-2334-10-69
44. Darryn L, Knobel Alice N, Maina Sally J, et al. Coxiella burnetii in humans, domestic ruminants, and ticks in rural Western Kenya. Am J Trop Med Hyg. 2013;88(3):513–518. doi:10.4269/ajtmh.12-0169
45. Porter S, Caplicki G, Mainil J, Guatteo R, Saegerman C. Q-fever; current state of knowledge and perspectives of research of a neglected zoonosis. Int J Microbial. 2011;2011:248–418.
46. Tissot-DuPont H, Antoinette Amadei M, Nezri M, Raoult D. Wind in November, Q -fever in December. Emerg Infect Dis. 2004;10(7):1264–1269. doi:10.3201/eid1007.030724
47. Berii M, Rekiki A, Boumedine S, Rodolakis A. Simultaneous differential detection of Chlamydophila abortus, Chlamydophiapecorum and Coxiella burnetii from aborted ruminants clinical samples using multiplex PCR. BMC Microbiol. 2009;9:1471–2180.
48. Lapointe JM, Gulland FM, Haines DM, Barr BC, Duignan PJ. Placentitis due to Coxiella Burnetii in a Pacific Harbor Seal (Phoca Vitulina Richardsi). J Vet Diagn Invest. 1999;11(6):541–543. doi:10.1177/104063879901100612
49. Duncan C, Kersh GJ, Spraker T, Patyk KA, Fitzpatrick KA. Coxiella burnetii in Northern Fur Seal (Callorhinus ursinus) Placentas from St. Paul Island, Alaska. Vector Borne Zoonotic Dis. 2012;12(3):192–195. doi:10.1089/vbz.2011.0715
50. Reusken C, van der Plaats R, Opsteegh M, de Bruin A, Swart A. Coxiella burnetii (Q fever) in Rattus norvegicus and Rattus rattus at livestock farms and urban locations in the Netherlands; could Rattus spp. represent reservoirs for (re)introduction. Prev Vet Med. 2011;101(1–2):124–130. doi:10.1016/j.prevetmed.2011.05.003
51. Rousset E, Berri M, Durand B, Dufour P, Prigent M. Coxiella burnetii shedding routes and antibody response after outbreaks of Q fever-induced abortion in dairy goat herds. Appl Environ Microbiol. 2009;75(2):428–433. doi:10.1128/AEM.00690-08
52. Stoker MG, Fiset P. Phase variation of the Nine Mile and other strains of Rickettsia burnetii. Can J Microbiol. 1956;2(3):310–321. doi:10.1139/m56-036
53. Dumas A, Bouchard C, Dibernardo A, et al. Transmission patterns of tick-borne pathogens among birds and rodents in a forested park in southeastern Canada. PLoS One. 2022;17(4):e0266527. doi:10.1371/journal.pone.0266527
54. Lang G. Coxiellosis (Q Fever) in Animals. CRC Press; 1990:23–48.
55. Marrie TJ, Raoult D. Update on Q fever, including Q fever endocarditis. Curr Clin Top Infect Dis. 2002;22:97–124.
56. Agerholm JS. Coxiella burnetii associated reproductive disorders in domestic animals-a critical review. Acta Vet Scand. 2013;55(1):13. doi:10.1186/1751-0147-55-13
57. Cantas H, Muwonge A, Sareyyupoglu B, Yardimci H, Skjerve E. Q-fever abortions in ruminants and associated on-farm risk factors in Northern Cyprus. BMC Vet Res. 2011;7(1):13. doi:10.1186/1746-6148-7-13
58. Kim SG, Kim EH, Lafferty CJ, Dubovi E. Coxiella burnetii in Bulk Tank Milk Samples, United States. Emerg Infect Dis. 2005;11(4):619–621. doi:10.3201/eid1104.041036
59. Valkovska L, Mališevs A, Kovaļenko K, Bērziņš A, GrantiņaIeviņa L. Coxiella Burnetii DNA in milk, milk products, and fermented dairy products. J Vet Res. 2021;65(4):441–447. doi:10.2478/jvetres-2021-0055
60. Abdali F, Hosseinzadeh S, Berizi E, Shams S. Prevalence of Coxiella burnetii in unpasteurized dairy products using nested PCR assay. Iran J Microbiol. 2018;10(4):220–226.
61. Roest A, Dubas JS, Gerris JR. Value transmissions between fathers, mothers, and adolescent and emerging adult children: the role of the family climate. J Fam Psychol. 2009;23(2):146. doi:10.1037/a0015075
62. EFSA Panel on Animal Health and Welfare (AHAW). Scientific Opinion on Q- Fever. EFSA Panel on Animal Health and Welfare; 2010.
63. Van den Brom R, Van Engelen E, Roest HIJ, Van der Hoek W, Vellema P. Coxiella burnetii infections in sheep or goats: an opinionated review. Vet Microbiol. 2015;181(1–2):119–129.
64. Gürtler L, Bauerfeind U, Blümel J, et al. Coxiella burnetii - pathogenic agent of Q (Query) fever. Transfus Med Hemother. 2014;41(1):60–72. doi:10.1159/000357107
65. Long CM, Beare PA, Cockrell DC, Larson CL, Heinzen RA. Comparative virulence of diverse Coxiella burnetii strains. Virulence. 2019;10(1):133–150. doi:10.1080/21505594.2019.1575715
66. Carcopino X, Raoult D, Bretelle F, Boubli L, Stein A. Managing Q-fever during pregnancy. The benefits of long-term cotrimoxazole therapy. Clin Infect Dis. 2007;45(5):548–555. doi:10.1086/520661
67. Epelboin L, Eldin C, Thill P, et al. Human Q Fever on the Guiana Shield and Brazil. Recent Findings and Remaining Questions. Curr Trop Med Rep. 2021;8(3):173–182. doi:10.1007/s40475-021-00243-4
68. Gebremedhin Y, Shallom M. Review on Q fever in Small Ruminants and its Public Health Importance. J Ethol Animal Sci. 2018;1(1):1–12. doi:10.23880/jeasc-16000102
69. Eldin C, Mahamat A, Demar M, Abboud M, Djossou F, Abboud P. Q-fever in French Guiana. Amazon J Trop Med Hygiene. 2014;91(4):771–776. doi:10.4269/ajtmh.14-0282
70. Bildfell RJ, Thomson GW, Haines DM, McEwen BJ, Smart N. Coxiella burnetii infection is associated with placentitis in cases of bovine abortion. J Vet Diagnos Invest. 2000;12(5):419–425. doi:10.1177/104063870001200505
71. Emery M, Ostlund E, Schmitt B. Comparison of Q fever serology methods in cattle, goats, and sheep. J Vet Diagnos Invest. 2012;24(2):379–382. doi:10.1177/1040638711434943
72. Parker NR, Barralet JH, Bell AM. Q fever. Lancet. 2006;367(9511):679–688.
73. Raoult D, Marrie T, Mege J. Natural history and pathophysiology of Q-fever. Lancet Infect Dis. 2005;5(4):219–226. doi:10.1016/S1473-3099(05)70052-9
74. Heydel C, Willems H. Pathogens in Milk – Coxiella burnetii. In: Fuquay JW, Fox PF, McSweeney PLH, editors. Encyclopedia of Dairy Sciences. Vol. 4,
75. Angelakis E, Million M, D’Amato F, et al. Q-fever and pregnancy: disease, prevention, and strain specificity. Eur J Clan Microbiol Infect Dis. 2012;28:361–368.
76. Pratschke J, Dragun D, Hauser IA, et al. Immunological risk assessment: the key to individualized immunosuppression after kidney transplantation. Transplant Rev. 2016;30(2):77–84. doi:10.1016/j.trre.2016.02.002
77. Song JK. Infective endocarditis involving an apparently structurally normal valve: new epidemiological trend? Korean J Intern Med. 2015;30(4):434–442. doi:10.3904/kjim.2015.30.4.434
78. Botelho-Nevers E, Fournier PE, Richet H. Coxiella burnetii infection of aortic aneurysms or vascular grafts: report of 30 new cases and evaluation of outcome. Eur J Clin Microbiol Infect Dis. 2007;26(9):635–640. doi:10.1007/s10096-007-0357-6
79. Gardon J, Heraud J, Laventure S, Ladam A, Capot P. Suburban transmission of Q fever in French Guiana: evidence of a wild reservoir. J Infect Dis. 2007;184(3):278–284. doi:10.1086/322034
80. Grace D, Mutua F, Ochungo P, et al. Mapping of poverty and likely zoonoses hotspots. Zoonoses Project 4, report to Department for International Development, UK. Nairobi: International research Institute; 2012.
81. Selim AF, Elhaig M. Q fever in domestic small ruminant. Asian J Anim Vet Adv. 2016;11:1–8.
82. Hillenbrand W, Breuer T, Petersen L. Changing epidemiology of Q fever in Germany, 1947–1999. Emerg Infect Dis. 2001;7(5):789–796. doi:10.3201/eid0705.010504
83. Herremans T, Hogema B, Nabuurs M, Peeters M, Wegadam Blans M. Comparison of the performance of IFA, CFA and elisa as says for the serodiagnosis of acute Q fever by quality assessment. Diagnost Microbial Infect Dis. 2013;75(1):16–21.
84. Hollenbeck B, Gannon S, Qinan Q, Grad Y. Genome sequence and analysis of resistance and virulence determinants in a strain of Neisseria mucosa causing native-valve endocarditis. JMM Case Rep. 2015;2(3). doi:10.1099/jmmcr.0.000049
85. Angesom H, Venkataramana K, Mahendra P. Epidemiology and public health implications of Q-fever. Perspect Med Res. 2016;4(3):42.
86. Pal M. Coxiellosis: a rickettial zoonosis. Vet World. 2006;4:127–128.
87. Kittelberger R, Mars J, Wibberley G, et al. Comparison of the Q-fever complement fixation test and two commercial enzyme-linked immunosorbent assays for the detection of serum antibodies against Coxiella burnetii (Q-fever) in ruminants: recommendations for use of serological tests on imported animals in New Zealand. N Z Vet J. 2009;57(5):262–268.
88. Soleimani Z, Jaydari A. Seroprevalence of Q fever in Lorestan province veterinary staff using IFA method. Int J Infect. 2021;8(1):e110731. doi:10.5812/iji.110731
89. Rousset E, Durand B, Berri M, et al. Comparative diagnostic potential of three serological tests for abortive Q-fever in goat herds. Vet Microbiol. 2007;124(3–4):286–297. doi:10.1016/j.vetmic.2007.04.033
90. Scott G, Williams J. Susceptibility of Coxiella burnetii to chemical disinfectants. Ann N Y Acad Sci. 2010;590:291–296. doi:10.1111/j.1749-6632.1990.tb42235.x
91. Norlander L. Q fever epidemiology and pathogenesis. Microbes Infect. 2000;2(4):417–424. doi:10.1016/S1286-4579(00)00325-7
92. Sampere M, Font B, Font J, Sanfeliu I, Segura F. Q fever in adults: review of 66 clinical cases. Eu J Clin Microbial Infect Dis. 2003;22(2):108–110. doi:10.1007/s10096-002-0873-3
93. Kagawa FT, Wehner JH, Mahindra V. Q fever as a biological weapon. SEM Resp Infect. 2003;18(3):183–195.
94. OIE (2019) World organization of animal health OIE. Manual of diagnostic tests and vaccines for terrestrial animals. In: Q-Fever. World Organization for Animal Health; 2010:1–13.
95. Toman R, Heinzen R, Samet J, Mege J. Coxiella burnetii, Recent Advances and New Perspectives in Research of the Q Fever Bacterium. New York: Springer; 2012:406.
96. Ford N, Shubber Z, Jao J, Abrams EJ, Frigati L, Mofenson L. Safety of cotrimoxazole in pregnancy: a systematic review and meta-analysis. J Acquir Immune Defic Syndr. 2014;66(5):512–521. doi:10.1097/QAI.0000000000000211
97. Woldehiwet Z. Q fever (Coxiellosis) epidemiology and pathogenesis. Res Vet Sci. 2004;77(2):93–100. doi:10.1016/j.rvsc.2003.09.001
98. Maurin M, Raoult D. Q fever. Clin Microbiol Rev. 1999;12(4):
99. Chiu CK, Durrheim DN. A review of the efficacy of human Q fever vaccine registered in Australia. N S W Public Health Bull. 2007;18(8):133–136. doi:10.1071/NB07057
100. Oyston P, Davies C. Q fever: the neglected bio threat agent. J Med Microbiol. 2011;60(1):9–21. doi:10.1099/jmm.0.024778-0
101. Tigertt WD, Benenson AS, Gochenour WS. Airborne Q fever. Bacteriol Rev. 1961;25(3):285–293. doi:10.1128/br.25.3.285-293.1961
102. Jones RM, Nicas M, Hubbard A, Reingold A. The infectious dose of Coxiella burnetii (Q- fever). Appl Biosafety. 2006;11(1):
103. Hendrik-Jan R. Coxiella burnetii in Pregnant Goats [PhD Thesis]. Wageningen, Netherlands: Central Veterinary Institute, Canisius Wilhelmina Hospital; 2013: 200.
104. Lemtudo AP, Mutai BK, Mwamburi L, Waitumbi JN. Seroprevalence of Coxiella burnetii in patients presenting with acute febrile illness at Marigat District Hospital, Baringo County, Kenya. Vet Med Sci. 2021;7(5):2093–2099. doi:10.1002/vms3.493
105. Tukur HB, Ajogi I, Kabir J, Umoh JU. Seroprevalence of Coxiella Burnetii in cattle and its risk factors in Kaduna Metropolis, Kaduna State, Nigeria. IOSR J Agric Vet Sci. 2014;7(2):1–5. doi:10.9790/2380-07210105
106. Fesseha H, Kefelegn T, Mathewos M. Animal care professionals’ practice towards zoonotic disease management and infection control practice in selected districts of Wolaita zone, Southern Ethiopia. Heliyon. 2022;8(5):e09485. doi:10.1016/j.heliyon.2022.e09485
107. Abebe A. Prevalence of Q fever infection in the Addis Ababa abattoir. Ethiop Med J. 1990;28(3):119–122.
108. Tsouloufi TK, MacVicar IS, Donnison LM, Smyth KL, Peters AR. Systematic map of the most recent evidence (2010–2019) on ruminant production-limiting disease prevalence and associated mortality in Ethiopia. Front Vet Sci. 2023;10:995213. doi:10.3389/fvets.2023.995213
109. Tesfaye A, Sahele M, Sori T, Guyassa C, Garoma A. Seroprevalence and associated risk factors for chlamydiosis, coxiellosis and brucellosis in sheep and goats in Borana pastoral area, southern Ethiopia. BMC Vet Res. 2020;16:145. doi:10.1186/s12917-020-02360-0
110. Alemayehu G, Mamo G, Alemu B, et al. Causes and Flock Level Risk Factors of Sheep and Goat Abortion in Three Agroecology Zones in Ethiopia. Front Vet Sci. 2012;8:615310. doi:10.3389/fvets.2021.615310
111. Alemnew E, Yitagesu E, Aydefruhim D, Areaya A. Clinical abortion and serological investigation of Brucella melitensis, Coxiella burnetii and toxoplasma gondii in goat’s in Ataye boer nucleus site north Shewa zone. Ethiopia Res Agric Vet Sci. 2021;20215(2):55–65.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.