")
Back to Journals » Clinical Ophthalmology » Volume 9
Corneal decompensation following filtering surgery with the Ex-PRESS® mini glaucoma shunt device
Authors Tojo N, Hayashi A , Miyakoshi A
Received 16 January 2015
Accepted for publication 11 February 2015
Published 17 March 2015 Volume 2015:9 Pages 499—502
DOI https://doi.org/10.2147/OPTH.S81050
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Naoki Tojo, Atsushi Hayashi, Akio Miyakoshi
Department of Ophthalmology, Graduate School of Medicine and Pharmaceutical Sciences, University of Toyama, Toyama, Japan
Purpose: To report a case of corneal decompensation due to the Ex-PRESS® mini glaucoma shunt device (Ex-PRESS).
Patient and methods: A 75-year-old man had pseudoexfoliation glaucoma in his right eye. He underwent filtration surgery with Ex-PRESS. His intraocular pressure was 7 mmHg after 9 months.
Results: We observed partial decompensation of the corneal endothelium adjacent to the filtering bleb. Specular microscopy revealed a marked decrease in the endothelial cell density at the center of the cornea.
Conclusion: Anterior segment optical coherence tomography is very useful for evaluating corneal edema and the position of Ex-PRESS. It is important to follow up with an examination of the corneal endothelial cells.
Keywords: Ex-PRESS, bullous keratopathy, trabeculectomy, complication, cornea
Introduction
The Ex-PRESS® mini glaucoma shunt device (Ex-PRESS) was designed to shunt the aqueous humor from the anterior chamber to the subconjunctival space using a filtration bleb.1 Ex-PRESS is a stainless steel, nonvalved, flow-restricting implant that was developed as an alternative to trabeculectomy and other types of glaucoma filtration surgery for patients with open-angle glaucoma.1 Glaucoma filtration surgery with Ex-PRESS has some merits that might be better for high-risk patients – eg, it is associated with fewer complications of early postoperative hypotony and it does not require iridectomy.2,3 In recent years, the use of glaucoma filtration surgery with Ex-PRESS has been increasing.
One of the postoperative complications of glaucoma filtration surgery is corneal endothelium dysfunction. If endothelial cell loss occurs more rapidly than normal, the endothelium will not be able to maintain its function, resulting in bullous keratopathy and a loss of vision. The rates of corneal endothelial cells decreasing after glaucoma filtering surgery have tended to vary widely among different studies.4,5
To our knowledge, this is the first report to describe corneal decompensation resulting from a filtration surgery with Ex-PRESS.
Patient and methods
A 75-year-old man presented with pseudoexfoliation glaucoma in the right eye. He had hypertension with systemic disease. He had undergone cataract surgery 3 years earlier. His intraocular pressure (IOP) was elevated above 31 mmHg despite topical antiglaucoma therapy, and his best-corrected visual acuity was 0.9. His mean deviation from the Humphrey visual field test (Humphrey Field Analyzer; Carl Zeiss Meditec AG, Jena, Germany) was −20.72 dB.
Retrobulbar anesthesia was administered. A standard fornix-based conjunctival incision was made to gain exposure to the scleral bed adjacent to the limbus. A single scleral flap with a size of 3.5 mm × 3.5 mm was created. A mitomycin C (MMC) solution of 0.04 mg/mL was applied for 4 minutes. At this point, the eye was in a complete enclosed space, and thus MMC could not flow into the anterior chamber. Then, the treated area was irrigated with about 100 mL of balanced salt solution. The scleral flap was lifted, and a 25 gauge needle was horizontally inserted into the anterior chamber at the surgical limbus to create a path for Ex-PRESS. The 25 gauge needle was inserted into the anterior chamber from the sclera–cornea transition zone parallel to the iris. Then, Ex-PRESS was inserted into the anterior chamber. The scleral flap was sutured using a 10-0 nylon suture in three places. The conjunctiva was meticulously closed with a 10-0 nylon suture.
Results
Early postoperative complications were not noted during the first 2 months after the surgery. The postoperative IOP remained under 10 mmHg until 9 months after the surgery without any glaucoma drops. The best-corrected visual acuity was 0.6 at 6 months after the surgery. However, at 9 months after the surgery, we observed partial decompensation of the corneal endothelium resulting in a well-demarcated clear zone of the cornea and a second zone with thickening of the cornea with a Descemet membrane fold and a partial bullous keratopathy in the area adjacent to the filtering bleb (Figure 1A). The best-corrected visual acuity decreased to 0.3 at that time. The conjunctival bleb was maintained and confirmed with anterior segment optical coherence tomography (AS-OCT) (SS-1000 CASIA; Tomey Corporation, Nagoya, Japan).
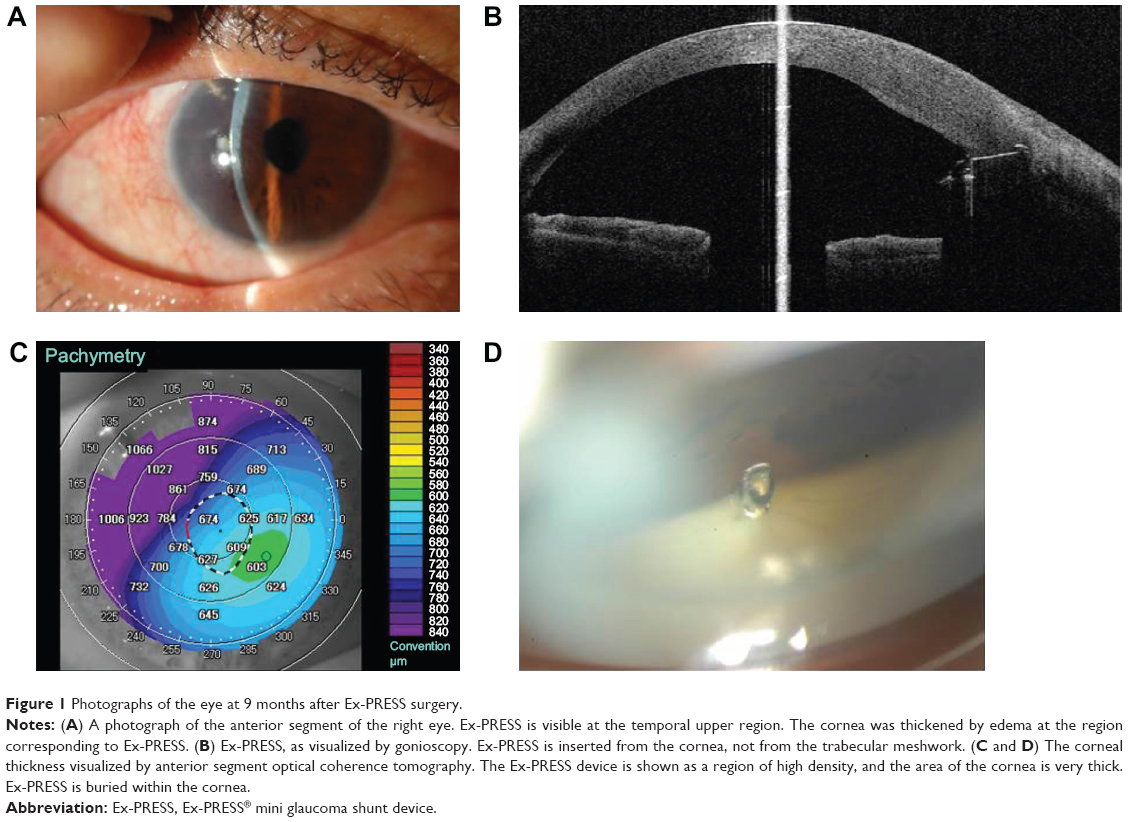 | Figure 1 Photographs of the eye at 9 months after Ex-PRESS surgery. |
When we checked the position of Ex-PRESS with AS-OCT and gonioscopy, we found that Ex-PRESS was inserted from the cornea, not the trabecular meshwork (Figures 1B–D). The cornea adjacent to the bleb appeared to be very thick. The endothelial cell density rapidly decreased during the 9 months after the surgery (Figure 2). The central corneal endothelial cells appeared to be enlarged, while the peripheral corneal endothelium at the side opposite the bleb had regularly-shaped margins (Figure 3).
 | Figure 2 Changes of endothelial cell density at the center of the eye. |
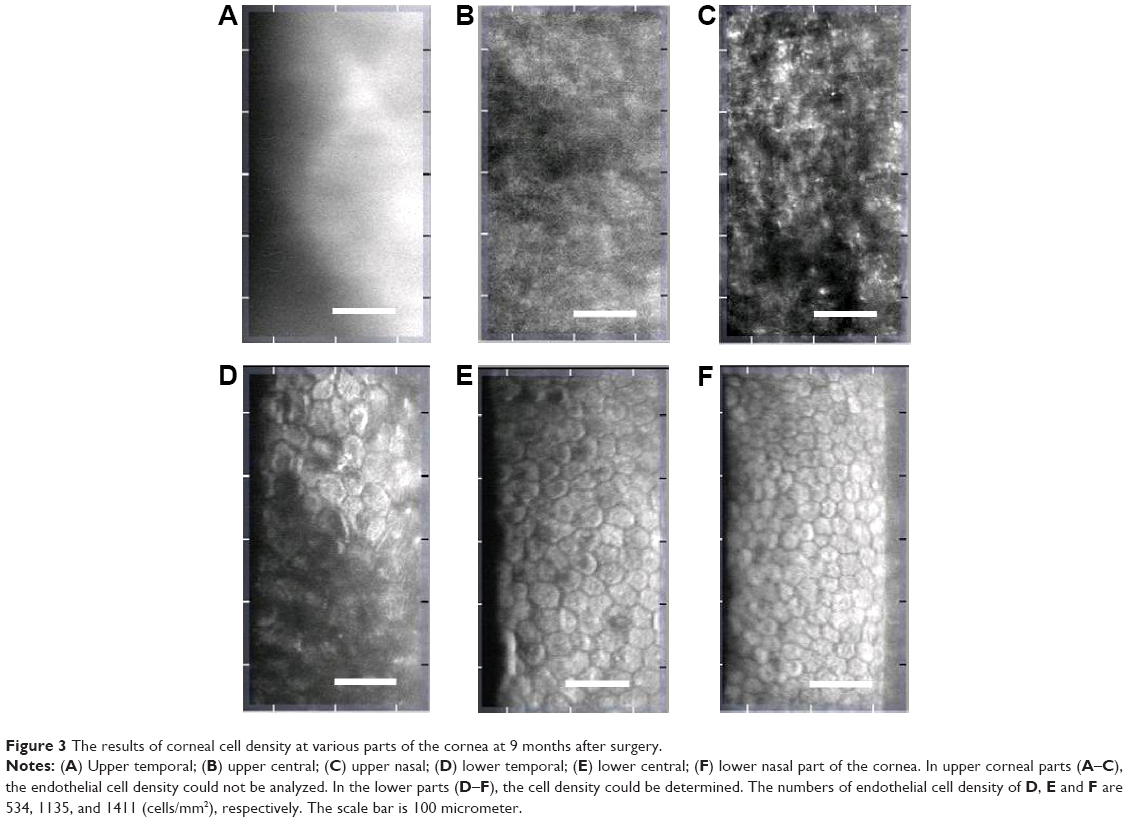 | Figure 3 The results of corneal cell density at various parts of the cornea at 9 months after surgery. |
Discussion
Bullous keratopathy is one of the most severe postoperative complications of glaucoma filtration surgery. As to the cause of corneal endothelium decompensation, there are several hypotheses. Sagoo et al6 reported that anterior chamber inflammation may play a major role in the pathogenesis of bullous keratopathy. The authors demonstrated that inflammatory cytokines such as interleukin-1, interferon-γ, and tumor necrosis factor induce corneal endothelium apoptosis through the production of nitric oxide. Yamamoto et al7 reported that serious corneal endothelial dysfunction was caused by an unusual streaming of the aqueous flow that should be present after filtration surgery. The application of MMC may have an additional toxic effect on the endothelium and may result in a partial bullous keratopathy.8,9 In a laboratory experiment using human corneas that had been obtained from transplantation, a toxic effect of MMC to the endothelium was noted by McDermott et al.10 In addition, contact with a foreign body, such as the Ex-PRESS device, may cause corneal endothelium decompensation.11
In this case, the cause of the corneal decompensation was not clear and, indeed, multiple causes might have participated. However, we speculated that the main cause was the physical contact between the corneal endothelium and Ex-PRESS. It is difficult to determine whether the Ex-PRESS device has actually come into contact with the corneal endothelium by gonioscopy. Using AS-OCT, however, the position and angle of the Ex-PRESS can be seen more clearly. In our case, the tip of the Ex-PRESS was in the anterior chamber, with almost all portions of the needle buried among the cornea. Ex-PRESS might have touched the corneal endothelium during eye blinking, causing the corneal edema and Ex-PRESS to come into contact. AS-OCT is very useful for evaluating the region of corneal edema. The present case suggests that it is important to avoid touching the corneal endothelium or the iris with the EX-PRESS device but, in some cases, it can be difficult to determine whether or not the Ex-PRESS device attached intraoperatively. Surgeons thus need to exercise caution in regard to the insertion angle of the Ex-PRESS device.
Conclusion
In conclusion, this is the first report of the clinical complications of Ex-PRESS as a possible cause of corneal decompensation. Surgeons should be aware of the possibility of this side effect in order to identify patients at risk for this complication before surgery.
Disclosure
The authors report no conflicts of interest in this work.
References
Traverso CE, De Feo F, Messas-Kaplan A, et al. Long term effect on IOP of a stainless steel glaucoma drainage implant (Ex-PRESS) in combined surgery with phacoemulsification. Br J Ophthalmol. 2005;89(4):425–429. | ||
Maris PJ Jr, Ishida K, Netland PA. Comparison of trabeculectomy with Ex-PRESS miniature glaucoma device implanted under scleral flap. J Glaucoma. 2007;16(1):14–19. | ||
Dahan E, Carmichael TR. Implantation of a miniature glaucoma device under a scleral flap. J Glaucoma. 2005;14(2):98–102. | ||
Soro-Martínez MI, Villegas-Pérez MP, Sobrado-Calvo P, Ruiz-Gómez JM, Miralles de Imperial Mora-Figueroa J. Corneal endothelial cell loss after trabeculectomy or after phacoemulsification, IOL implantation and trabeculectomy in 1 or 2 steps. Graefes Arch Clin Exp Ophthalmol. 2010;248(2):249–256. | ||
Storr-Paulsen T, Norregaard JC, Ahmed S, Storr-Paulsen A. Corneal endothelial cell loss after mitomycin C-augmented trabeculectomy. J Glaucoma. 2008;17(8):654–657. | ||
Sagoo P, Chan G, Larkin DF, George AJ. Inflammatory cytokines induce apoptosis of corneal endothelium through nitric oxide. Invest Ophthalmol Vis Sci. 2004;45(11):3964–3973. | ||
Yamamoto Y, Uno T, Shisida K, et al. Demonstration of aqueous streaming through a laser iridotomy window against the corneal endothelium. Arch Ophthalmol. 2006;124(3):387–393. | ||
Mietz H, Roters S, Krieglstein GK. Bullous keratopathy as a complication of trabeculectomy with mitomycin C. Graefes Arch Clin Exp Ophthalmol. 2005;243(12):1284–1287. | ||
Mohammadpour M, Jabbarvand M, Javadi MA. Focal corneal decompensation after filtering surgery with mitomycin C. Cornea. 2007;26(10):1285–1287. | ||
McDermott ML, Wang J, Shin DH. Mitomycin and the human corneal endothelium. Arch Ophthalmol. 1994;112(4):533–537. | ||
Bersudsky V, Treviño A, Rumelt S. Management of endothelial decompensation because of glaucoma shunt tube touch by Descemet membrane endothelial keratoplasty and tube revision. Cornea. 2011;30(6):709–711. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.