")
Back to Journals » Clinical Optometry » Volume 16
Corneal Characteristics of Myopic Malay School Children and Their Association with Axial Length
Authors Syed Mohd Dardin SF , Mohd-Ali B , Mohamad Shahimin M , Mohd Saman MN, Mohidin N
Received 21 July 2023
Accepted for publication 6 March 2024
Published 4 April 2024 Volume 2024:16 Pages 107—114
DOI https://doi.org/10.2147/OPTO.S431608
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Mr Simon Berry
Syarifah Faiza Syed Mohd Dardin,1,2 Bariah Mohd-Ali,1 Mizhanim Mohamad Shahimin,1 Mohd Norhafizun Mohd Saman,1 Norhani Mohidin1
1Optometry & Vision Science Program and Research Centre for Community Health (ReaCH), Faculty of Health Science, Universiti Kebangsaan Malaysia, Kuala Lumpur, Malaysia; 2Optometry Service, Allied Health Science Division, Medical Programme, Ministry of Health, Putrajaya, Malaysia
Correspondence: Bariah Mohd-Ali, Optometry & Vision Science Programme, Research Centre for Community Health (ReaCH), Faculty of Health Science, Universiti Kebangsaan Malaysia, Kuala Lumpur Campus, Jalan Raja Muda Abdul Aziz, Kuala Lumpur, 50300, Malaysia, Tel +60392897602, Fax +60392897604, Email [email protected]
Introduction: Corneal characteristics are unique to each eye and can vary among different levels of refractive errors. However, minimal data are available in the literature on corneal characteristics in myopic Malay school children including the difference between the low myopic group and the moderate myopic group. Therefore, this study aims to determine the corneal characteristics of myopic Malay school children and their associations with axial length.
Methods: A total of eighty-four data samples were extracted from forty-two myopic Malay school children. Measurements of the central corneal thickness (CCT), corneal curvature, corneal diameter, and axial length were measured using Lenstar LS900, a non-contact optical biometer. Data were later stratified by the spherical equivalent refraction (SER) into a low myopic group and a moderate myopic group, and paired t-test were employed to determine the differences in the corneal characteristics between these two groups. Univariate and multivariate linear regressions were performed to identify factors that are significantly associated with axial length.
Results: There was no significant difference in the CCT, corneal curvature and corneal diameter between the low myopic group and the moderate myopic group (t82=0.015, P=0.99), (t82=− 0.802, P=0.43) and (t82=− 0.575, P=0.57), respectively. Pearson univariate correlation analysis found that axial length significantly correlated with corneal curvature (r=− 0.765, P< 0.001) and corneal diameter (r=0.614, P< 0.001) but no significant correlation found with CCT (r=0.046, P=0.68). Multiple regression analysis showed that axial length was significantly associated with a flatter corneal curvature (P< 0.001), older age (P< 0.001) and larger corneal diameter (P=0.02).
Conclusion: This study reported the corneal characteristics in myopic Malay school children and its associations with axial length. Results of this study can serve as a reference value for the myopic Malay schoolchild population.
Keywords: Lenstar LS900, corneal characteristics, Malay, myopic school children
Introduction
Myopia is the most prevalent refractive problem worldwide and it is estimated that 22.9% (1406 million people) of the world population is affected by myopia1 especially in the Asian countries.2 These rates are projected to increase, and it is estimated that by 2050, half of the world population will have myopia with 9.8% will suffer from high myopia.3
The cornea, together with the sclera, coats the eyeball, forming the outermost layer of the eye and plays an important role in maintaining the shape of the eyeball.4 As myopia progresses, the elongation process of the eyeball may disrupt the eyeball dimensions, including the corneal characteristics. Corneal characteristics are commonly described via a few different markers including the central corneal thickness (CCT), the corneal curvature, and the corneal diameter.
In the early years of research on the corneal curvature, myopic eyes were reported to have a steeper corneal curvature than emmetropic eyes. This finding was supported by Scott and Grosvenor,5 who proposed the idea that when the axial length elongates in myopic eyes, stretching of the eyeball causes the steepening of the cornea. However, recently, based on fourteen years of data collection during the Correction of Myopia Evaluation Trial (COMET) longitudinal study, it was found that the cornea curvature becomes slightly flattened as myopia progresses.6 However, the Anyang Childhood Eye Study reported no significant difference in the corneal curvature between the low and moderate myopic eyes when compared with emmetropic eyes.7
In terms of the corneal diameter, Zha et al8 evaluated 591 eyes of Chinese individuals who underwent a LASIK evaluation and found that when the subjects were divided into four different groups according to their refractive statuses (ranging from −0.60 D to −6.00 D), eyes with a refractive error of more than −3 D had lower corneal diameter values. However, The Shandong Children Eye Study, which investigated 6026 children aged 4–18 years, reported an association between a larger horizontal corneal diameter and a longer axial length, longer corneal curvature radius, and lower intraocular pressure measurements, alongside the systemic parameters of male gender, rural region of habitation, and younger maternal age via their multivariate analysis.9
Few rationalizations were postulated to explain the conflicting findings of corneal characteristics in different level of refractive error as well as conflicting relationships among corneal characteristics and the refractive error/axial length. The differences were attributed to the differences in the patient demographics including the ethnicity, the diverse age groups studied, and the instruments used.10
As mentioned above, the prevalence of myopia across the globe is alarming, and Malaysia is not excluded. The first prevalence study conducted in Malaysia was carried out in 1993, and the study showed an increase in the prevalence of myopia among Malay school children from 4.3% in children aged 7–8 years old to 25.6% in children aged 15–16 years old.11 When a similar study was repeated by Goh et al in an urban area of the Gombak District, the prevalence of myopia in Malay increased from 7.7% in children aged 7 years old to 30.7% in children aged 15 years old.12 Even though individuals of Chinese ethnicity have the highest prevalence of myopia among school children in Malaysia, the quadrupled increment shown in Malay children is concerning, especially when it is considered that Malay individuals represent 57.7% of the total population in Malaysia.
Limited literature discusses the corneal characteristics in young children especially in myopic Malay school children. Study by Mohd-Ali et al13 found that the corneal curvature of the emmetropic young Malays aged between 7 and 12 years old is flatter than observed in young Chinese population and smaller corneal diameter than Caucasians. Indirectly, local forensic and maxillofacial studies have reported significant differences in the intercanthal and interpupillary distances14,15 as well as in the periorbital tissue measurements15 between local Malay and Chinese individuals, the largest two ethnic groups in Malaysia. These findings may suggest further differences in anatomical and ocular dimensions.
There are many corneal imaging devices available in clinical practice for an accurate estimation of the corneal thickness and corneal curvature such as Scheimpflug imaging technique, swept-source optical coherence tomography and Placido-Scheimpflug tomography, and can be used interchangeably to measure corneal thickness and radius measurement in healthy myopic eyes.16 Besides the aforementioned measuring methods, current non-contact optical biometers can also, in combination, produce multiple anterior ocular parameters, such as corneal curvature, lens thickness, CCT, and corneal diameter, in addition to their primary ability, to measure axial length. Current non-contact optical biometers work based on various principle such as partial coherence interferometry, swept-source techniques, and optical coherence low reflectometry such as the Lenstar LS900 (Haag-Streit AG, Switzerland). Lenstar LS900 have limited measurement errors and low variability between other non-contact optical biometers,17–19 and make them ideal for application to research in the myopia field,20 especially among young children. Previously, studies on corneal characteristics were only conducted using corneal imaging techniques, but nowadays, corneal characteristics in myopic children were also reported using non-contact optical biometers.21,22
To the best of our knowledge, this is the first study to report the corneal characteristics and to compare the differences between low and moderate myopic groups in Malay school children using non-contact optical biometer. With the increasing prevalence of myopia in Malay school children, any effort to understand corneal characteristics in myopic Malay school children is essential. Therefore, this study aimed to describe the corneal characteristics of myopic Malay school children, the differences between the low and moderate myopic group and to delineate the relationship between corneal characteristics and the axial length of the eye in healthy myopic Malay school children.
Materials and Methods
This was a cross-sectional study involving healthy Malay school children with low to moderate myopia. The participating children were primary school students aged 7–12 years old. The sample size was calculated from the G-power software (ver.3.1.9.4) using a calculation for linear multiple regression test with an estimated effect size of 0.235, taken from the previous study,23 0.8 as power of test (1-β), and a significance level (α) of 0.05. High contrast (100%) visual acuity for distance was measured using the Logarithmic 2000 series Early Treatment Diabetic Retinopathy Chart (Precision Vision Inc., Woodstock, IL, USA). Cycloplegia was induced with two drops of Cyclopentolate Hydrochloride 1%, (Cyclogyl, Alcon, 15 mL) with five-minute intervals and objective cycloplegic refraction was measured using WAM-5500 autorefractor (Grand Seiko Co., Ltd., Hiroshima, Japan). Corneal curvature, CCT and corneal diameter were measured using Lenstar LS900 (Haag-Streit AG, Switzerland). The Lenstar LS900 was selected to measure the corneal characteristics because it offers excellent repeatability and reliability and can produce multiple anterior ocular parameters at one measurement seating which make it very convenient for young children. Furthermore, non-contact optical biometers are now increasingly utilized in myopia control clinics.
For this study, all subjects were divided into two groups according to their refractive status, the low myopic group (−0.50 ≤ SER ≤ −3.00 D) and the moderate myopic group (−3.00 < SER < −6.00 D).24 All subjects had monocular best-corrected visual acuity of 20/20 (0.00 LogMAR notation) or better. Subjects with astigmatism and anisometropia of more than 1.50 D were excluded from this study. Subjects were also screened to ensure that they were free from any ocular or systemic diseases.
The study and data collection were performed with the approval of the local ethics committee (UKM PPI/111/8/JEP-2020-667). Informed consent was obtained from the parents of every subject who took part in the study, and the study protocol was consistent with the tenets of the Declaration of Helsinki.
Statistical analyses were conducted using commercial software (SPSS version 23.0; SPSS, Inc., Chicago, IL). The distribution of the measured variables was estimated by the Shapiro–Wilk test, and all data were normally distributed. Parametric tests were then used for further analysis. Corneal characteristics were described using mean ± standard deviation. An independent sample t-test was employed to compare the measured CCT, corneal curvature, and corneal diameter values between the low myopic group and the moderate myopic group. Pearson’s correlation coefficient (r) was calculated to assess the relationship between the axial length with the CCT, corneal curvature and corneal diameter. Multiple regression analyses were used to assess the contribution of CCT, corneal curvature, corneal diameter, age and gender to the axial length. Results were considered statistically significant when the P-value was less than 0.05.
Results
Forty-two myopic Malay school children (17 boys and 25 girls) were recruited for participation in this study. The mean age of all subjects was 9.55 ± 1.51 years old (range 7–12 years old). Since each eye contributes to an independent observation, data from both eyes were used in the subsequent analysis (N=84). The mean cycloplegic spherical equivalent refraction (SER) was −2.93 ± 1.24 D (range −0.63 D to −5.50 D), and the mean axial length was 24.34 ± 0.92 mm (range 22.53 mm to 26.26 mm). The mean SER of the low myopic group was −1.93 ± 0.71 D, and the mean SER of the moderate myopic group was −3.97 ± 0.69 D. The demographic profile of the subjects recruited in this study is shown in Table 1. Earlier on, the distributions of the axial length and all corneal characteristics of interest (CCT, corneal curvature, and corneal diameter) were assessed. The distributions of the axial length, CCT, corneal curvature, and corneal diameter were mesokurtic with skewness values of 0.63, 0.14, −0.23 and 0.20. All data were normally distributed.
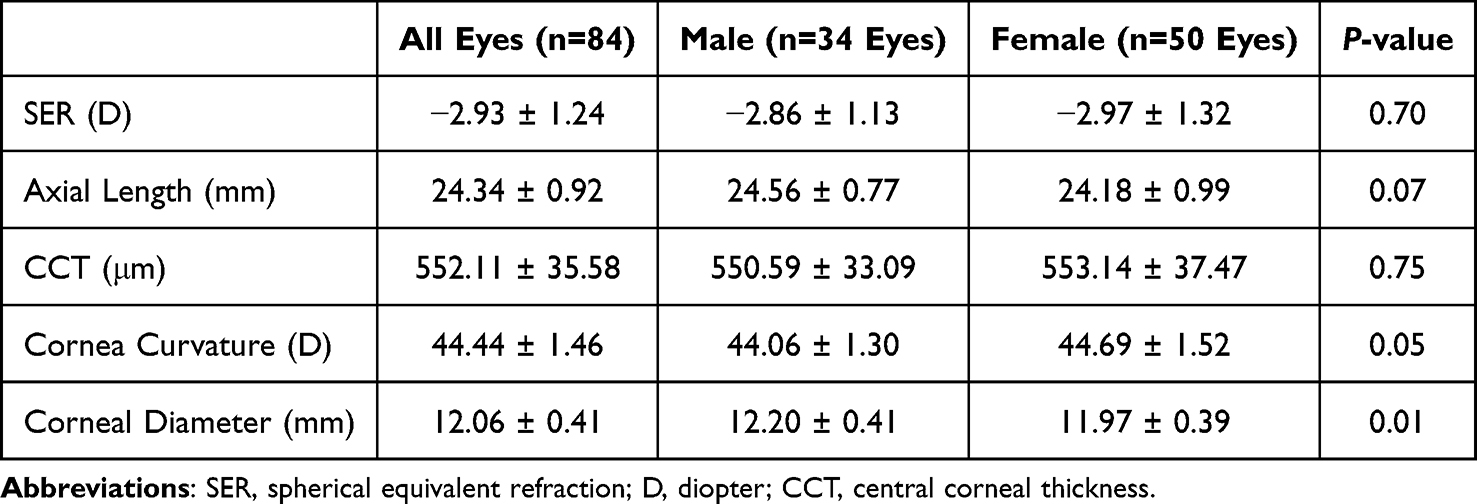 |
Table 1 Patients’ Demographic Profile |
The mean CCT, corneal curvature, and corneal diameter values were 552.11 ± 35.58 μm, 44.44 ± 1.46 D, and 12.06 ± 0.41 mm, respectively. A steeper corneal curvature and larger corneal diameter were found in the moderate myopic group than in the low myopic group, but the differences were not statistically different, as shown by the independent sample t-test. The CCT value was similar between groups: the CCT in the low myopic group was 552.16 ± 27.17 μm, while the CCT in the moderate myopic group was 552.05 ± 43.02 μm. A summary of the findings and P-values for each comparison is presented in Table 2.
 |
Table 2 Comparisons of SER, Axial Length and Corneal Characteristics Between the LMG and the MMG |
A further bivariable analysis showed that the corneal diameter (Figure 1A) and corneal curvature (Figure 1B) were significantly correlated with the axial length, but no significant correlation was found between the axial length and the CCT (r=0.046, P=0.68) (Figure 1C). In this study, there was a strong positive correlation between the axial length and the corneal diameter (r=0.614, P<0.001) and strong negative correlation between the axial length and the corneal curvature (r=−0.765, P<0.001). The linear regression of this relationship shows that for every 1 mm increase in the axial length, the corneal diameter increases by 0.27 mm and corneal curvature flattens by 1.21 D with coefficients of determination of 38% and 59%.
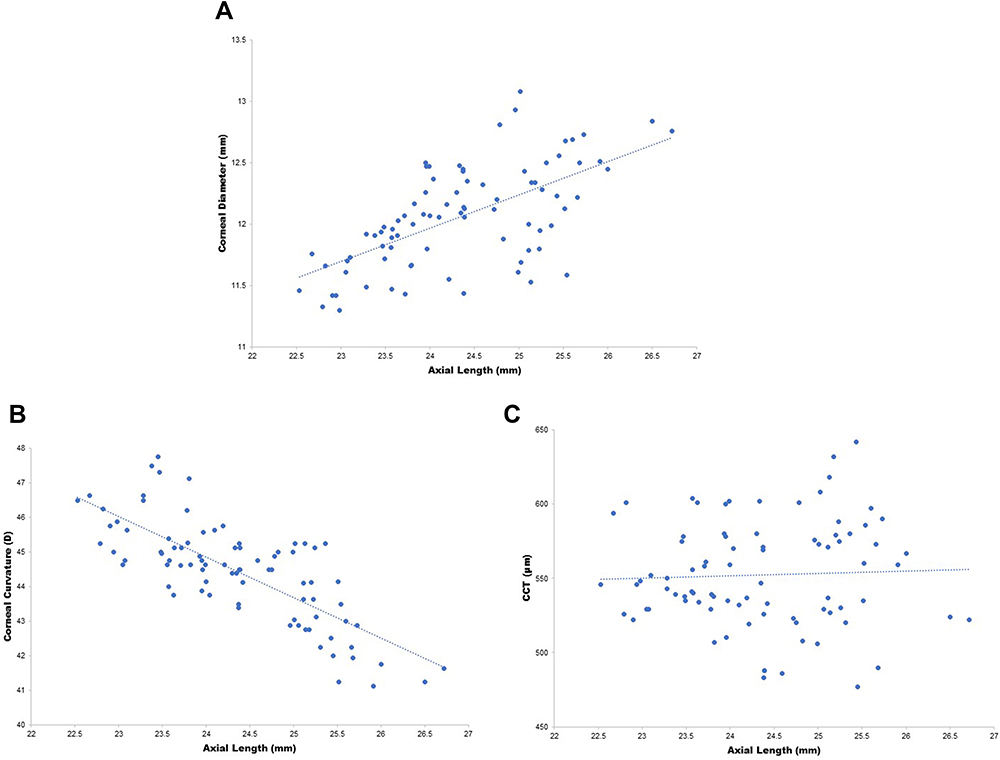 |
Figure 1 (A) Relationship between the axial length and corneal diameter. (B) Relationship between the axial length and corneal curvature. (C) Relationship between the axial length and central corneal thickness (CCT). |
Multivariate linear regression analyses were further performed with the axial length as the dependent variable and age, gender, corneal curvature, corneal diameter and CCT as the independent variables. The analyses showed that the age, corneal curvature and corneal diameter explained 71.7% of the axial length variations in this study. The most important contributor to axial length was the corneal curvature followed by age and the corneal diameter (Table 3).
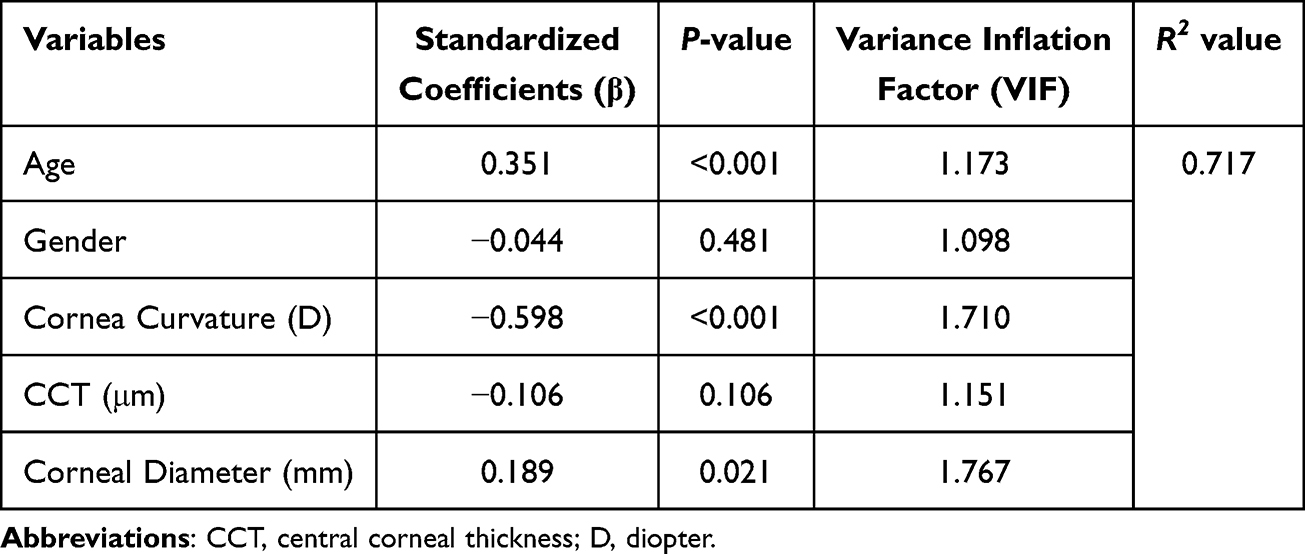 |
Table 3 Multivariate Analysis of the Associations Between Axial Length and Age, Gender, Corneal Curvature, CCT and Corneal Diameter |
Discussion
Central Corneal Thickness
The mean CCT value in our study population was 552.11 ± 35.58 μm and was 94 μm thinner than the mean CCT value obtained from previous study on 188 young Malays aged 7–12 years old in Malaysia.13 The CCT value obtained in our population was also 22 μm thicker than reported by Heidary et al,25 who investigated the CCT in 54 healthy Malays aged 8–16 years old. However, subjects from both studies were not myopic and the CCT measurements were conducted using optical pachymetry and specular microscopy. In comparison with myopic group, the mean CCT in this study population was 25 μm thicker than the CCT value reported in one local study involving healthy myopic Malaysian children of Chinese ethnicity using a noncontact specular microscope.23 They studied 111 myopic eyes with a mean SER of −2.01 ± 1.73 D from school children aged 8–9 years old, and the average CCT was 527.01 ± 26.17 μm.
Differences in the mean CCT found in different studies might be due to the influences of the age groups and refractive status of the population studied, the instruments used, and the ethnicity of the study population.26,27
A further investigation found no correlations between the CCT and the axial length in myopic Malay school children. The contribution of the CCT to the axial length was also not significant in the multiple regression analysis. These findings support a poor correlation between axial length and CCT. The same finding has been reported by other researchers.23,28–30 Thiagarajan et al28 compared the CCT between the low, moderate and high myopic group in children aged 7–15 years old and found a no statistically significant difference in the mean value between groups. In their study, measurement of the CCT was done using TonopachyTM and Ultrasound Pachymetry. This finding suggests that the elongation of the eyeball and the increment in the refractive error have a minimal or no effect on the CCT. The stretching of the eyeball was probably limited only to the peripheral eyeball and did not influence the CCT to a measurable degree.23 In addition, the Pediatric Eye Disease Investigator Group (PEDIG) investigated 2079 children and observed a subtle change in the CCT and the refractive error where, on average, the CCT was only 1 μm thinner for a 1.00D increase in the myopic refractive error.31
Corneal Curvature
The cornea contributes significantly towards the refractive system. In this study population, the mean central cornea curvature was 44.44 ± 1.46 D. Further investigation found that the mean cornea curvature did not differ significantly between the low myopic group and the moderate myopic group (t82 = −0.802, P = 0.43) with values of 44.31 ± 1.40 D and 44.57 ± 1.52 D, respectively. The cornea curvature value found in this study was slightly steeper than found in previously reported corneal studies on Malay school children.13,32 Both studies measured the cornea curvature in healthy Malay children with lower refractive error than refractive error that found in our study, which specifically focused on the myopic population. This current study, however, only recruited subjects with astigmatism of less than 1.50 D. This study also found a negative and strong correlation between the corneal curvature and the axial length (r = −0.765, P = 0.001), where longer eyes associated with flatter corneal curvature and is similar to the results of several other studies.6,21,23,33 This negative correlation could be explained via the compensatory mechanism that operates in emmetropization, where the cornea flattens during the early emmetropization process as the axial length increases. This mechanism masks the excessive growth of the axial length.34 However, fourteen years of longitudinal changes in corneal curvature from Correction of Myopia Evaluation Trial (COMET) study reported a gradual decrease in this correlation as the eyes grew longer and suggested that environmental factors may play a role in changing the coordinated growth of these components, affecting axial length to a greater extent than corneal curvature, regardless of gender or ethnicity.6
Corneal Diameter
About 20% of corneal diameter growth occurs during early infancy and early childhood. An adult corneal diameter value of 11.7 mm is normally reached by 7 years of age. In this study, the mean corneal diameter was 12.06 ± 0.41 mm. The corneal diameter in the low myopic group was 12.04 ± 0.41 mm, which did not differ significantly from the corneal diameter in the moderate myopic group of 12.09 ± 0.42 mm (t82 = −0.575, P = 0.57). This value is within the normal corneal diameter range of 11.24–12.76 mm. The corneal diameter measured in this study population also did not differ significantly from the value of 11.89 ± 0.36 mm reported by Mohd-Ali et al,13 who investigated ocular dimensions in healthy young Malays. The corneal diameter was mostly found to be independent of age. Previous studies have reported a mean corneal diameter within the normal range, despite vast differences in the study populations in terms of age. Rüfer et al35 found a mean horizontal corneal diameter of 11.71 ± 0.42 mm in 390 healthy, Caucasian subjects aged 10–80 years old, and Popov et al21 reported a corneal diameter of 11.96 ± 0.49 mm in 2340 patients aged 19–96 years old who had undergone cataract surgery at their center. Data from this study also found a moderate but significant correlation between the corneal diameter and the axial length (r=0.624, P < 0.001), which is in agreement with the results from the study by Jiang et al,9 who found that the axial length has a lesser association with the corneal diameter than the associations between the corneal diameter and the corneal curvature. Individuals with an axial length of less than 26.5 mm with longer horizontal and vertical globe diameters have a larger retinal surface area, more retinal photoreceptors, retinal pigment epithelium cells, and retinal ganglion cell axons, a larger optic disc, and a larger cornea.36
Conclusions
The measurement of the CCT, corneal curvature, and corneal diameter in myopic Malay school children using optical biometry with the Lenstar LS900 and the differences of these measurements between the low and moderate myopic group were reported for the first time in this study. Despite the small number of children, this study has its own strengths in terms of its homogenous and specific study population, as only myopic Malay school children aged 7–12 years old were recruited for the data collection. Results from this study can serve as a future reference for eye care practitioners to understand the corneal characteristics in our local myopic Malay schoolchild population. In addition, availability of this data will allow more reliable and comprehensive use of the non-contact optical biometers, especially in young children. However, there are limitations in this study. Besides the small number of subjects, this was a cross-sectional study, where we only looked at one time point. A prospective longitudinal study would be beneficial for in-depth understanding particularly in the changes of the corneal characteristics with the progression of the axial length. Since this study intends to focus on corneal changes in myopic young children, it is also recommended to explore corneal characteristics in high myopic group in the future and to include more parameters such as lens thickness and anterior chamber depth.
Ethics Statement
This research adhered to the tenets of the Declaration of Helsinki. This research also received an ethical clearance from the Universiti Kebangsaan Malaysia Ethics Committee (UKM PPI/111/8/JEP-2020-667).
Consent to Participate
The parents of the subjects were provided with a comprehensive explanation of the research, and consents were obtained from them prior to the commencement of the study.
Acknowledgments
The authors express gratitude towards all the subjects and parents for their collaborations and cooperation.
Funding
This research received a University Research Grant (GUP-2020-054) from the Universiti Kebangsaan Malaysia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Alvarez-Peregrina C, Martinez-Perez C, Sánchez-Tena MÁ. Myopia and other visual disorders in children. Int J Environ Res Public Health. 2022;19(15):1–5. doi:10.3390/ijerph19158912
2. Grzybowski A, Kanclerz P, Tsubota K, Lanca C, Saw S-M. A review on the epidemiology of myopia in school children worldwide. BMC Ophthalmol. 2020;20(1):27. doi:10.1186/s12886-019-1220-0
3. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036–1042. doi:10.1016/j.ophtha.2016.01.006
4. Zhang Y, Wang Y, Li L, et al. Corneal stiffness and its relationship with other corneal biomechanical and nonbiomechanical parameters in myopic eyes of Chinese patients. Cornea. 2018;37(7):881–885. doi:10.1097/ICO.0000000000001605
5. Scott R, Grosvenor T. Structural model for emmetropic and myopic eyes. Ophthalmic Physiol Opt. 1993;13(1):41–47. doi:10.1111/j.1475-1313.1993.tb00424.x
6. Scheiman M, Gwiazda J, Zhang Q, et al. Longitudinal changes in corneal curvature and its relationship to axial length in the Correction of Myopia Evaluation Trial (COMET) cohort. J Optom. 2016;9(1):13–21. doi:10.1016/j.optom.2015.10.003
7. S-M L, Iribarren R, Kang M-T, et al. Corneal power, anterior segment length and lens power in 14-year-old Chinese children: the Anyang Childhood Eye Study. Sci Rep. 2016;6(1):20243. doi:10.1038/srep20243
8. Zha Y, Feng W, Han X, Cai J. Evaluation of myopic corneal diameter with the Orbscan II Topography System. Graefe’s Arch Clin Exp Ophthalmol. 2013;251(2):537–541. doi:10.1007/s00417-012-2069-6
9. Jiang WJ, Wu H, Wu JF, et al. Corneal diameter and associated parameters in Chinese children: the Shandong Children Eye Study. Clin Exp Ophthalmol. 2017;45(2):112–119. doi:10.1111/ceo.12821
10. Saw SM. A synopsis of the prevalence rates and environmental risk factors for myopia. Clin Exp Optom. 2003;86(5):289–294.
11. Norhani M, Chung KM, Garner LF. Myopia and sex in Malay schoolchildren. Sains Malays. 1993;22(3):97–101.
12. Goh PP, Abqariyah Y, Pokharel GP, Ellwein LB. Refractive error and visual impairment in school-age children in Gombak District, Malaysia. Ophthalmology. 2005;112(4):678–685. doi:10.1016/j.ophtha.2004.10.048
13. Mohd-Ali B, Abdul-Rahim MAS, Mohamed Z, Mohidin N. Ocular dimensions of young Malays in Malaysia. J Sains Kesihat Malaysia. 2011;9(1):35–39.
14. Gabriel GF, Pawita S, Amir A, Sia BP. Development of eye shape photofit database of the Chinese and Malay population in Malaysia. SM J Forensic Res Criminol. 2018;1(3):1011.
15. Lu TY, Kadir K, Ngeow WC, Othman SA. The prevalence of double eyelid and the 3D measurement of orbital soft tissue in Malays and Chinese. Sci Rep. 2017;7(1):1–9. doi:10.1038/s41598-017-14829-4
16. Biswas S, Biswas P. Agreement and repeatability of corneal thickness and radius among three different corneal measurement devices. Optom Vis Sci. 2021;98(10):1196–1202. doi:10.1097/OPX.0000000000001785
17. Rauscher FG, Hiemisch A, Kiess W, Michael R. Feasibility and repeatability of ocular biometry measured with Lenstar LS 900 in a large group of children and adolescents. Ophthalmic Physiol Opt. 2021;41(3):512–522. doi:10.1111/opo.12807
18. Buckhurst PJ, Wolffsohn JS, Shah S, Naroo SA, Davies LN, Berrow EJ. A new optical low coherence reflectometry device for ocular biometry in cataract patients. Br J Ophthalmol. 2009;93(7):949–953. doi:10.1136/bjo.2008.156554
19. Cruysberg LPJ, Doors M, Verbakel F, Berendschot TTJM, De Brabander J, Nuijts RMMA. Evaluation of the Lenstar LS 900 non-contact biometer. Br J Ophthalmol. 2010;94(1):106–110. doi:10.1136/bjo.2009.161729
20. Wolffsohn JS, Kollbaum PS, Berntsen DA, et al. IMI - Clinical myopia control trials and instrumentation report. Invest Ophthalmol Vis Sci. 2019;60(3):M132–M160. doi:10.1167/iovs.18-25955
21. Popov I, Waczulikova I, Stefanickova J, et al. Analysis of biometric parameters of 2340 eyes measured with optical biometer Lenstar LS900 in a Caucasian population. Eur J Ophthalmol. 2022;32(1):213–220. doi:10.1177/1120672121998920
22. Meng Q, Cui Y, Zhang M, et al. Design and baseline characteristics of a population-based study of eye disease in southern Chinese people: the Dongguan Eye Study. Clin Exp Ophthalmol. 2016;44(3):170–180. doi:10.1111/ceo.12670
23. Norhani M, Low YC, Bariah M-A, Mizhanim MS, Norlaili A. Corneal endothelial morphology of healthy myopic Malaysian children of Chinese ethnicity aged 8–9 years and its association with axial length. F1000Research. 2022;11:339. doi:10.12688/f1000research.110560.2
24. Flitcroft DI, He M, Jonas JB, et al. IMI – defining and classifying myopia: a proposed set of standards for clinical and epidemiologic studies. Investig Ophthalmol Vis Sci. 2019;60(3):M20–M30. doi:10.1167/iovs.18-25957
25. Heidary F, Gharebaghi R, Wan Hitam WH, Naing NN, Wan-Arfah N, Shatriah I. Central corneal thickness and intraocular pressure in Malay children. PLoS One. 2011;6(10). doi:10.1371/journal.pone.0025208
26. Dai E, Gunderson CA. Pediatric central corneal thickness variation among major ethnic populations. J AAPOS. 2006;10(1):22–25. doi:10.1016/j.jaapos.2005.12.007
27. Aghaian E, Choe JE, Lin S, Stamper RL. Central corneal thickness of Caucasians, Chinese, Hispanics, Filipinos, African Americans, and Japanese in a glaucoma clinic. Ophthalmology. 2004;111(12):2211–2219. doi:10.1016/j.ophtha.2004.06.013
28. Thiagarajan K, Srinivasan K, Gayam K, Rengaraj V. Comparison of central corneal thickness using non-contact tono-pachymeter (Tonopachy) with ultrasound pachymetry in normal children and in children with refractive error. Indian J Ophthalmol. 2021;69(8):2053. doi:10.4103/ijo.IJO_364_21
29. Ortiz S, Mena L, Rio-San Cristobal A, Martin R. Relationships between central and peripheral corneal thickness in different degrees of myopia. J Optom. 2014;7(1):44–50. doi:10.1016/j.optom.2013.03.005
30. Shimmyo M, Orloff PN. Corneal thickness and axial length. Am J Ophthalmol. 2005;139(3):553–554. doi:10.1016/j.ajo.2004.08.061
31. Pediatric Eye Disease Investigator Group*. Central Corneal Thickness in Children. Arch Ophthalmol. 2011;129(9):1132. doi:10.1001/archophthalmol.2011.225
32. Ramlee A, Pin GP. Ocular biometric measurements in emmetropic and myopic Malaysian children - A population-based study. Med J Malaysia. 2012;67(5):497–502.
33. Olsen T, Arnarsson A, Sasaki H, Sasaki K, Jonasson F. On the ocular refractive components: the Reykjavik Eye Study. Acta Ophthalmol Scand. 2007;85(4):361–366. doi:10.1111/j.1600-0420.2006.00847.x
34. Ishii K, Iwata H, Oshika T. Quantitative evaluation of changes in eyeball shape in emmetropization and myopic changes based on elliptic Fourier descriptors. Investig Ophthalmol Vis Sci. 2011;52(12):8585–8591. doi:10.1167/iovs.11-7221
35. Rufer F, Schroder A, Erb C. White-to-White Corneal Diameter. Cornea. 2005;24(3):259–261. doi:10.1097/01.ico.0000148312.01805.53
36. Papastathopoulos KI, Jonas JB, Panda-Jonas S. Large optic discs in large eyes, small optic discs in small eyes. Exp Eye Res. 1995;60(4):459–461. doi:10.1016/S0014-4835(05)80102-2
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.