")
Back to Journals » Patient Preference and Adherence » Volume 18
Construction of Hospice Care Evaluation System for Terminally Ill Patients in ICU
Authors Wang QL, Liu CR, Yue P, Han BR
Received 11 October 2023
Accepted for publication 18 December 2023
Published 6 January 2024 Volume 2024:18 Pages 29—37
DOI https://doi.org/10.2147/PPA.S444290
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Qing-Ling Wang,1,* Cheng-Rui Liu,2,* Peng Yue,3 Bin-Ru Han1
1Department of Emergency, Xuanwu Hospital, Capital Medical University, Beijing, 100053, People’s Republic of China; 2School of Economics and Management, Beijing University of Technology, Beijing, 100124, People’s Republic of China; 3Capital Medical University, School of Nursing, Beijing, 100069, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bin-Ru Han, Department of Nursing, Xuanwu Hospital, Capital Medical University, No. 45 of Changchun Street, Xicheng District, Beijing, 100053, People’s Republic of China, Tel +8613693377666, Fax +86 10 8316 1294, Email [email protected]
Background: Terminally ill patients can benefit from hospice care, which specifically addresses the needs of patients and families affected by terminal illness. However, there is a lack of standardized evaluation criteria to assess the quality of hospice care for terminally ill patients in the ICU, and it is impossible to evaluate the service quality of hospice care. To use the Delphi method to construct a hospice care system for terminally ill patients in ICU that meets clinical needs, and to provide theoretical support for nursing decision-making of terminally ill patients in clinical ICU.
Methods: Obtain relevant literatures by entering specific key words into the database, the hospice care nursing system for terminally ill patients in ICU was preliminarily drawn up by literature analysis, and 24 experts in this field were consulted for 3 rounds by Delphi method to discuss the development status of hospice care and finally establish the hospice care nursing system.
Results: In the three rounds of letter inquiries, the positive coefficients of experts were all high, the expert authority coefficient (Cr) were 0.864, 0.849, 0.832, and the expert opinion coordination coefficient(W) were 0.186, 0.319, 0.224; The system includes 8 first-level indicators, 27 second-level indicators and 9 third-level indicators.
Conclusion: In this study, three rounds of Delphi consultation methods were used to construct an evaluation index system for the nursing quality of hospice care for ICU patients. The evaluation indicators formulated closely focus on the physiological and psychological characteristics of ICU patients, which can provide a better reference for ICU patients with advanced life in the future.
Keywords: Delphi method, late life, hospice care nursing system, letter inquiry
Introduction
Hospice care is a product of the development of modern medicine to a certain stage. It refers to providing all-round physical and mental care for patients and their families who are progressively deteriorating or whose lives are about to end, so as to relieve the physical pain of patients and relieve the psychological distress faced by patients and their families, and ultimately improve their quality of life.1,2 China is in urgent need of palliative care development in the face of growing population ageing and a growing shortage of medical resources. In January 2017, the former National Health and Family Planning Commission (NHFPC) issued the “Practice Guidelines on hospice care (trial)”, which marked that hospice care in China has gradually received attention.3 Hospice care ICU is an important clinical department, and a considerable proportion of patients admitted are at the end of life. Such patients not only suffer from great physical pain, but also increase the economic burden on the family and society due to the large medical consumption, and the quality of life of the patients is also significantly reduced.4 Therefore, how to help ICU patients spend the last period of life better and relieve their physical and mental pain to the greatest extent has become an important research topic for medical staff. Studies have shown that providing high-quality end-of-life care services for patients at the end of life can significantly reduce their physical pain, properly solve their psychological problems.5 This not only reflects the value of their lives and dignity, and to a certain extent can reduce the burden of the family, saving limited health resources. A 1995 study in the United States found that every dollar spent on palliative care saved $1.52 in health insurance costs.6 According to the survey in China, the average treatment fee, drug fee, nursing fee and hospitalization fee for each person receiving hospice care is 17,000 yuan ($2331.16), while the total cost of the elderly patients with the same length of hospitalization is 31,000 yuan ($4250.94), which is a saving of 14,000 yuan ($1919.78).6 It is necessary to constantly explore and supplement end-of-life care standards and evaluation systems suitable for national conditions and people’s conditions in services, which can benefit both individuals and society.6
At present, there is a lack of standardized evaluation standards for the nursing quality of hospice care for terminally ill patients in the ICU, and it is impossible to evaluate the service quality of hospice care.7,8 This is the main factor resulting in ineffective hospice care.9 The Delphi method is based on systematic procedures and adopts the method of anonymous expression of opinions, so that experts are not allowed to discuss with each other, do not have horizontal contact, and can only have relationships with investigators, after repeated consultation, induction, and modification, the consensus of the experts was finally summarized as the result of the prediction.10,11 The aim of this study is to construct an evaluation system for the quality of end-of-life care services for elderly patients in ICU and improve the quality of end-of-life care services for ICU patients. This study uses the Delphi method to provide service standards for nurses to implement end-of-life care for ICU patients, and as a basis for evaluating the quality of end-of-life care services.
Methods
Research Group
The research group consists of 8 people, including 2 senior professional titles and 6 intermediate professional titles; educational background: 2 doctors, 3 masters, and 3 undergraduates. The members of the research group are responsible for selecting experts, designing questionnaires and summarizing and analyzing the results. To prevent bias, exclude people with conflicts of interest from the research team. An independent researcher was responsible for the main coordination of the Delphi study.
Preliminary Formulation of Hospice Care Evaluation System
The research group entered the keywords “Late life”, “Palliative care” and “Nursing system” into databases such as HowNet and Wanfang to obtain relevant literature and materials. Kolcaba’s comfort theory is a middle range theory developed by Kolcaba, which is taken as the basic theoretical framework in this paper.12 And with referring to “Palliative Therapy Guidelines for Nursing Practice”,13 the hospice care evaluation system includes six aspects: environmental management, psychological care, pain care, sleep care, comfort care, and social and cultural support. On this basis, open-ended interviews were conducted with 16 family members of the patients, and 10 clinical nursing staff participated in the formulation of indicators to preliminarily formulate a hospice care system, including 8 first-level indicators (adding nutritional intervention and support to the family on the basis of the above-mentioned 5 aspects), and 28 second-level indicators and 9 third-level indicators.
Expert Consultation
Selection of Experts
According to the purpose sampling method, the inclusion criteria of experts are determined: (1) Education background is not lower than undergraduate, and professional title is at least intermediate; (2) Engaged in hospice care services in related fields for more than 10 years; (3) Have a strong interest in this research and a high level of participation. (4) Can continue to participate in expert consultation during the project research period. The list of experts participating in this letter consultation was determined by the research group through joint discussion, including 8 medical experts from the critical care department, 12 nursing experts and 4 experts in psychology related fields. A total of 24 experts in this field were consulted for 3 rounds by Delphi method to discuss the development status of hospice care and finally establish the hospice care nursing system.
Design of Questionnaire by Letter
A total of 3 rounds of letter inquiries were carried out, all of which were sent by email.
The First Round of Letter Inquiries
Pre-consultation was conducted with experts, and revisions were made based on their opinions to produce the first round of consultation questionnaires. Contents include: (1) research purpose and questionnaire filling requirements; (2) expert basic information questionnaire, including name, age, education background, professional title, years of medical or nursing work. (3) Hospice care system for terminally ill patients in ICU. Experts scored each indicator one by one in terms of importance, and each indicator was scored with a 5-point scoring method (1 point for extremely unimportant, 2 points for unimportant, 3 points for general, 4 points for important, 5 points for extremely important) for scoring. There is an opinion column on the questionnaire, which is convenient for experts to supplement, delete and modify indicators. (4) the experts’ familiarity with indicators (Cs) and judgment basis (Ca). Cs scoring method: 0.2 points for extremely unfamiliar, 0.4 points for unfamiliar, 0.6 points for general, 0.8 points for familiarity, and 1 point for extremely familiar. The method of Ca assignment is shown in Table 1.
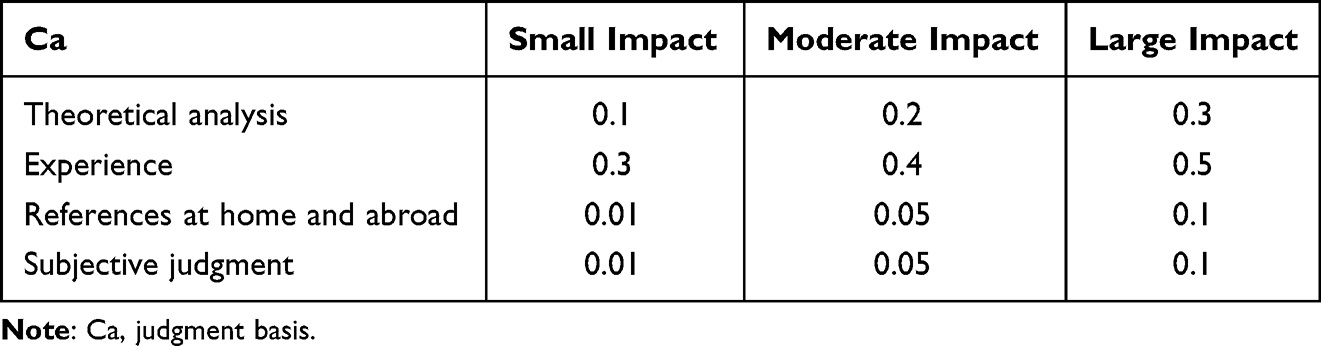 |
Table 1 Ca Scoring Method |
The Second Round of Inquiries
The last round of questionnaires was revised based on expert advice and the results of the letter inquiry, and the second round of letter questionnaire was prepared, including: (1) Explanation of the results of the last round of letter inquiry; (2) Explain how to fill out the questionnaire; (3) End-of-life patients in the ICU care system. The quantitative scoring method for the importance of each indicator is the same as the previous round, and the results of the round-robin inquiry are attached. Ask the experts to score again and fill in relevant suggestions. (4) Expert authority coefficient (Cr) and Ca of experts on indicators.
The Third Round of Inquiry
Combined with the results of the second round of letter inquiries, the third round of letter questionnaires were made. Compared to the second round of questionnaire, the third round questionnaire added a secondary indicator (to help patients’ families form a correct view of death) and deleted a secondary indicator (physical environment management of wards). The third round of questionnaires brings expert opinions more concentrated.
Index Screening Criteria
All material provided to the expert panel at the outset of the project and throughout the Delphi process should be carefully reviewed and piloted in advance in order to examine the effect on experts’ judgements and to prevent bias. The average value of each round of importance assignment exceeds 3.5 and the coefficient of variation is below 0.2 as the screening criteria, and the indicators are screened based on expert opinions. Among them, the coefficient of variation = the importance assignment of the indicator / arithmetic mean score.
Statistical methods
SPSS22.0 software was used to analyze, the basic information of experts, positive coefficient and other percentages (%) were expressed, and the descriptive analysis of each index of the nursing system was expressed by (±s) and coefficient of variation. The Kendall coordination coefficient was used to test the consistency of the evaluation results of the experts on each index. See Figure 1 for the procedural diagram.
 |
Figure 1 Procedural diagram. |
Result
Basic Information of Experts
The percentage of experts with a master’s degree or above is 50%, the percentage of associate senior titles and above is 54.17%, and the percentage of experts with more than 10 years of working experience is 100%. See Table 2 for details.
 |
Table 2 Basic Information of Experts (n=24) |
Expert Positive Coefficient
The recovery rate of the three rounds of questionnaires reached 100%. In the first round, 75.00% (18/24) of the experts gave their opinions. In the second round, 62.50% (15/24) of the experts gave their opinions. After the 3rd round of inquiry, no experts proposed amendments.
Cr
Cr is judged based on Cs and Ca. Cr=(Ca+Cs) ×0.5. The Cr values in the two rounds of this study were 0.864, 0.849, and 0.832, all of which exceeded 0.7 (the lower limit of acceptable reliability), indicating that the experts have high authority for this study. See Table 3 for details.
 |
Table 3 Results of 2 Rounds of Cr |
W After the Third Round of Expert Consultation
After the second round of expert letter inquiry, the W significance test P<0.001, it can be seen that the experts’ opinions on the indicators tend to be consistent, see Table 4 for details.
 |
Table 4 W After the Third Round of Expert Consultation |
Results of 2 Rounds of Expert Inquiry
After the first round of inquiry, 2 second-level indicators (including protecting patients’ privacy and satisfying patients’ dying wishes) were added in combination with expert suggestions, and 3 second-level indicators with an average value of importance assignment below 3.5 and a coefficient of variation of 0.2 or above were deleted (Including providing religious support for patients, helping relatives with funeral affairs, and informing patients of their illness in detail). After the second round of letter inquiries, combined with expert suggestions, one secondary indicator was added (to help patients’ families form a correct view of death), and one secondary indicator (physical environment management of wards) was deleted. After the third round of inquiry, the opinions of experts were basically the same.
Hospice Nursing System
Finally, 8 first-level indicators (including environmental management, psychological care, pain care, sleep care, comfort care, nutritional support, social and cultural support, and family support) and 27 second-level indicators were formed. See Table 5 for details.
 |
Table 5 Hospice Care System |
Discussion
Statement of Principal Findings
In the three rounds of letter inquiries, the positive coefficients of experts were all high, the expert authority coefficient (Cr) were 0.864, 0.849, 0.832, and the expert opinion coordination coefficient(W) were 0.186, 0.319, 0.224; The system includes 8 first-level indicators, 27 second-level indicators and 9 third-level indicators. In this study, three rounds of Delphi consultation methods were used to construct an evaluation index system for the nursing quality of hospice care for ICU patients.
Strengths and Limitations
The general principles of the guidance provided in the European Association for Palliative Care white paper apply to Western cultures, and although we did not find that perceptions of the applicability of palliative care for terminally ill patients in ICU differed elsewhere, it may be examined for applicability locally, especially in cultures more distant to Western Europe and in specific healthcare systems that provide palliative or comfort care based on prognosis. The strength of this study is that it provides systematically obtained opinions on the optimal management of hospice care evaluation system for terminally ill patients in ICU.
Due to the limitations of the Delphi method, the evaluation of indicators by experts is a subjective judgment, which will affect the selection and determination of evaluation indicators to a certain extent. The number of experts in this study is 24, and this study has not received financial support from funds or projects, and there is a large consumption of human, material and financial resources. In addition, the experts selected in this study may have the defect of regional concentration of experts. The next step is to expand the geographical scope of experts, improve the indicator system, and conduct clinical application research on the constructed indicators to further verify the scientificity, objectivity and operability of the indicators. Furthermore, there is a lack of uniform standards in the evaluation system of the quality-of-care services between medical institutions, which makes it difficult to compare evaluation results. As a result, the current system may not be suitable for international evaluation of care systems. In view of the limitations of Delphi method research, it is suggested that blockchain technology can be used in the future to build a database of hospice care indicators for ICU patients with advanced life, so that researchers can directly authorize access to experts in related fields, and at the same time avoid the manpower generated by multiple letters to experts. The consumption of material and financial resources maximizes the utilization of resources in the region.
Interpretation Within the Context of the Wider Literature
The hospice care in China develops rapidly in the eastern and southern regions, followed by the northern region, and the western region develops relatively slowly. This is related to the economic development among various regions, and it is also related to the policies of hospice care programs in various regions. According to data, the average daily medical expenses of patients with advanced malignant tumors in family beds is only 31.56 yuan ($4.33), while that of secondary hospitals is 810.63 yuan ($111.16), which is 25.7 times that of the former. The use of palliative care in family beds saves unnecessary treatment fees, examination fees and other cost.14 Similarly, Deana et al15 reported that health-related quality of life of patients remains low and patient care costs are high 1 year after patients are discharged from the ICU. From the perspective of economic input and output, hospice care is not only a humanitarian cause, but also a low-cost and high-efficiency charity.16–18 As a new type of service in mainland China, hospice care has vague concepts and classification methods that make it difficult to clarify its identity, so whether it can enter the medical insurance system has also become confusing. It would be exciting to see end-of-life care integrated into the health care system. This policy will largely address the financial burden of the hospice population.
Implications for Policy, Practice and Research
In recent years, many ICUs of hospitals have established a hospice care system, but most of them are not feasible, and there are major deficiencies in terms of scientificity and pertinence.19 Therefore, it is of great clinical significance to use the Delphi method in this study to construct a hospice care system for terminally ill patients in ICU. On the basis of previous relevant studies, this research group is carrying out a preliminary construction of the hospice care system in conjunction with the “Guidelines for Palliative Care Practice” and other relevant guidelines.20–24 The first-level indicators of the system include environmental management, psychological care, pain care, sleep care, comfort care, and social and cultural support, which are basically in line with the mainstream thinking of hospice care for terminally ill ICU patients. In addition, most ICU patients are in a high catabolic state, resulting in insufficient nutrient substrates and abnormal cell metabolism, which can cause or aggravate organ dysfunction.25 Therefore, the follow-up introduction of nutritional intervention in this study aims to adjust the nutritional status of patients through effective nutritional intervention, thereby avoiding damage to the physiological functions of the body. In addition, through interviews with 16 family members, it was found that family members are often unable to face the patient’s death, and tend to stay in grief for a long time, which will significantly affect their future life. Therefore, this study included family support in the first-level indicators, aiming to help family members establish a correct view of death and embrace a new life after the patient’s death.26 The unqualified indicators are continuously eliminated through several rounds of correspondence inquiries, and finally the second and third-level indicators that are unanimously recognized by experts can be screened out. The greater the importance assignment, the smaller the coefficient of variation, and the more concentrated the expert opinions.27
Conclusion
In summary, this study constructed an evaluation index system for the quality of hospice care for ICU patients through three rounds of Delphi consultation. The system of indicators for evaluating the quality of end-of-life care for patients in the hospice care unit includes eight aspects, namely environmental management, psychological care, pain care, sleep care, comfort care, nutritional support, social and cultural support and support for family members, respectively. A scientific approach to establishing a system of care should have a comprehensive evaluation methodology, scientific evaluation criteria and a standardized weighting scheme. If necessary, patients’ opinions and suggestions can be introduced, as far as possible to weigh the interests of all parties, to avoid contradictory evaluation indicators, and real-time monitoring and analysis of patient satisfaction and other situations, timely optimization and improvement of the quality of nursing services. The evaluation indicators established in this study closely focus on the physical and psychological characteristics of ICU patients, and at the same time do a good job in the care and care of family members, which can provide a better reference for ICU patients at the end of life in the future. The next step of this study is to apply the hospice care system to patients with late life in ICU, so that patients can obtain a higher quality of life.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Xuanwu Hospital, Capital Medical University.
Funding
The project was supported by the Construction and feasibility study of a family care plan based on the interactive experience and needs of end-of-life patients and their families (19YJC840059).
Disclosure
All of the authors had no any personal, financial, commercial, or academic conflicts of interest separately.
References
1. Ling M, Wang X, Ma Y, et al. A review of the current state of hospice care in China. Curr Oncol Rep. 2020;22:1–7. doi:10.1007/s11912-020-00959-y
2. Chen L, Li XH, Pan X, et al. Nurses’ knowledge, attitudes, and willingness to practice hospice care: an analysis of influencing factors. PLoS One. 2022;17(2):e0259647. doi:10.1371/journal.pone.0259647
3. National Health and Family Planning Commission Gazette. Circular of the general office of the national health and family planning commission on the publication of practical guidelines on hospice care (for trial implementation). National Health and Family Planning Commission Gazette; 2017:53–73.
4. Weiting GE, Yue L, Yu Q. Research progress of ICU nurses’ palliative care knowledge and behavior. Nurs Res. 2021;35(13):2352–2355.
5. Bai S, Hui Y. Research status of palliative care care for patients with advanced cancer. J Jilin Univer Med. 2020;41(6):457–459.
6. Wang X. Discussion of hospice care from view of economics. Chn Med Ethics. 2010;23(05):26–27+35.
7. Barnes C, Mueller K, Fawcett L, et al. Living and dying in a disparate health care system: rationale and strategies for cultural humility in palliative and hospice care physical therapy. Rehabil Oncol. 2020;38(1):30–38. doi:10.1097/01.REO.0000000000000199
8. Lindley LC, Richar CS, Hoit T, et al. Cost of pediatric concurrent hospice care: an economic analysis of relevant cost components, review of the literature, and case illustration. J Pall Med. 2021;24(9):1291–1298. doi:10.1089/jpm.2020.0495
9. Lin J, Ji Z, Zhao X. Current status of palliative care programs and their implications for our country. Nurs Res. 2019;33(19):3416–3419.
10. Freeman S, Banner D, Ward V. Hospice care providers experiences of grappling with medical assistance in dying in a hospice setting: a qualitative descriptive study. BMC Palliative Care. 2021;20:1–12. doi:10.1186/s12904-021-00740-3
11. Kincaid RB. Improving consumer assessment of health care providers and systems communication scores in hospice care: a pilot project. J Hospice Palliative Nurs. 2020;22(5):359–362. doi:10.1097/NJH.0000000000000676
12. Lu S, Hu X, Liu R. Kolcaba K’s theory of comfort and its practical application. Hebei Med. 2012;34(21):3312–3314.
13. Jiang S, Zhou N, Jiang B. Misunderstandings, ethical dilemmas and countermeasures in the practice of palliative care for patients with advanced cancer. J Nanj Med Univ. 2019;19(2):110–114.
14. Zhu YY, Shi YX. Cost analysis of community family beds for malignant tumor patients in Shanghai. Res Health Econ. 2001;2021:1.
15. Deana C, Vetrugno L, Cortegiani A, et al. Quality of life in covid-related ards patients one year after intensive care discharge (Odissea Study): a multicenter observational study. J Clin Med. 2023;12:3. doi:10.3390/jcm12031058
16. Xu WY, Shi W, Chen P. analysis of economic burden of Xinjiang malignant tumor patients in hospital. Dis Surveill. 2006;21:1–12.
17. Barbash IJ, Gershengorn HB. Hospital capacity strain as a window into the value of ICU admission: some answers. More Questions Am J Respir Crit Care Med. 2022;205(5):485–487. doi:10.1164/rccm.202111-2570ED
18. Schroeder SA, Showstack JA. Hospital costs. Ann Intern Med. 1977;86(3):360–361. doi:10.7326/0003-4819-86-3-360
19. Kader S. Designing the Post-Pandemic Hospice Environment:“The Last Place”[M]//(Re) Designing the Continuum of Care for Older Adults: The Future of Long-Term Care Settings. Cham: Springer International Publishing; 2023:237–259.
20. Deng L, Ouyang B, Shi H, et al. Icariside II attenuates bleomycin-induced pulmonary fibrosis by modulating macrophage polarization. J Ethnopharmacol. 2023;317:116810. doi:10.1016/j.jep.2023.116810
21. National Comprehensive Cancer Network. NCCN clinical practice guideline inoncology-palliative care (version2. 2017) [EB/OL]; 2017.
22. Zhang QQ, Wang WC, Gu Y. Content analysis of clinical practice guidelines related to adult hospice care. J Nurs Sci. 2022;37(9):99–102.
23. National Health and Family Planning Commission, People’s Republic of China. Notice of the general office of the national health and family planning commission on the issuance of hospice practice guidelines (trial) [EB/OL]; 2017. Available from: http://www.fihc.gov.en/yzygj/s3593/201702/3ec857f8c4a244e69b233ce2f5f270b3.shtml.
24. National Health and Family Planning Commission, People’s Republic of China. Hospice care services into the medical insurance long care insurance reimbursement of the central financial investment of 3 billion preferential policies issued [EB/OL]; 2018. Available from: http://www.cnaflc.org/lzgh/14234.jhtml.
25. Ye XH, Gong XM, Wang HJ, et al. Application of grading intervention of early enteral nutrition tolerance in severe patients. Parenteral Enteral Nutr. 2020;27(2):89–93.
26. Guo XF, Zhao P, Gao F. Soothing the dignity at the end of a life-long JOURNEY-A study of medical social work in the palliative care of patients with advanced cancer. Chin Can Clin Rehab. 2021;28(8):897–900.
27. Lin Q, Zeng L, Ren JH, et al. Research progress on communication management of family members of ICU patients. Chin J Nurs. 2020;55(2):294–298.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.