")
Back to Journals » Journal of Inflammation Research » Volume 17
Construction of a Multi-Indicator Model for Abscess Prediction in Granulomatous Lobular Mastitis Using Inflammatory Indicators
Authors Du NN, Feng JM, Shao SJ, Wan H , Wu XQ
Received 9 October 2023
Accepted for publication 20 January 2024
Published 1 February 2024 Volume 2024:17 Pages 553—564
DOI https://doi.org/10.2147/JIR.S443765
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Adam D Bachstetter
Nan-Nan Du, Jia-Mei Feng, Shi-Jun Shao, Hua Wan, Xue-Qing Wu
Breast Department, Shuguang Hospital Affiliated to Shanghai University of Traditional Chinese Medicine, Shanghai, 200021, People’s Republic of China
Correspondence: Xue-Qing Wu; Hua Wan, Breast Department, Shuguang Hospital Affiliated to Shanghai University of Traditional Chinese Medicine, Shanghai, 200021, People’s Republic of China, Tel +86 13817792022 ; +86 13611666266, Email [email protected]; [email protected]
Background: Granulomatous lobular mastitis (GLM) is a chronic inflammatory breast disease, and abscess formation is a common complication of GLM. The process of abscess formation is accompanied by changes in multiple inflammatory markers. The present study aimed to construct a diagnosis model for the early of GLM abscess formation based on multiple inflammatory parameters.
Methods: Based on the presence or absence of abscess formation on breast magnetic resonance imaging (MRI), 126 patients with GLM were categorised into an abscess group (85 patients) and a non-abscess group (41 patients). Demographic characteristics and the related laboratory results for the 9 inflammatory markers were collected. Logistics univariate analysis and collinearity test were used for selecting independent variables. A regression model to predict abscess formation was constructed using Logistics multivariate analysis.
Results: The univariate and multivariate analysis showed that the N, ESR, IL-4, IL-10 and INF-α were independent diagnostic factors of abscess formation in GLM (P< 0. 05). The nomogram was drawn on the basis of the logistics regression model. The area under the curve (AUC) of the model was 0.890, which was significantly better than that of a single indicator and the sensitivity and specificity of the model were high (81.2% and 85.40%, respectively). These results predicted by the model were highly consistent with the actual diagnostic results. The results of this calibration curve indicated that the model had a good value and stability in predicting abscess formation in GLM. The decision curve analysis (DCA) demonstrated a satisfactory positive net benefit of the model.
Conclusion: A predictive model for abscess formation in GLM based on inflammatory markers was constructed in our study, which may provide a new strategy for early diagnosis and treatment of the abscess stage of GLM.
Keywords: granulomatous lobular mastitis, abscess formation, risk factors, inflammation, ROC curve, diagnostic model
Introduction
Granulomatous lobular mastitis (GLM) is a general term for a group of purulent inflammatory conditions that occur in the breasts of women who are not breastfeeding or pregnant.1 Clinical manifestations of GLM include sudden onset of breast lumps, redness and pain, abscesses, and fistula formation. In severe cases, it may be accompanied by systemic symptoms such as fever and erythema of the lower limbs.2–4 The clinical stages of GLM include the self-limited stage, the congestive swelling stage, the abscess formation stage and the complex refractory stage.5 Almost all patients will progress to the abscess formation stage if left untreated.6 Although the abscess formation stage can be treated surgically, this operation often causes distortion of the breast appearance, affecting the attractiveness of the breasts.5,7 Through long-term clinical observation, we have found that Chinese herbs are more effective at the early stage of abscess formation and can maintain the appearance of the breast well while reducing the size of the breast lump.8 It is clear that early detection and treatment of the abscess formation stage of GLM is an important measure to stop the progression of GLM.
Studies have shown that there is a series of inflammatory reactions during the formation of GLM abscesses, patients may present with fever and elevated inflammatory markers such as serum white blood cell (WBC), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) and neutrophil count (N).9–12 In addition, the process of abscess formation may also present a pathophysiological state called a “cytokine storm”.11,13 For example, inflammatory cytokines such as interleukin-10 (IL-10) can induce abscess formation through the mitogen-activated protein kinase (MAPK) pathway.14 Interleukin-4 (IL-4) can antagonise the effects of IL-10 during infection,15 attenuate the inflammatory response and promote repair of necrotic tissue by promoting alternative activation of macrophages.16 IL-6 promotes abscess formation by regulating neutrophil microabscess formation driven by IL-17.17 Although the role of INF-α in abscess formation cannot be determined at this time, results from animal studies indicate that INF-α increases significantly after the development of inflammatory non-caseating granulomas in mice, suggesting that INF-α may play an important role in the pathogenesis of GLM.18 Therefore, in this study, we analysed the risk factors for GLM abscess formation by screening multiple inflammatory indicators and established a multi-indicator diagnostic model, with a view to provide a reference for clinical diagnosis of GLM abscess formation.
Materials and Methods
Clinical Data
A retrospective analysis was performed on the data of GLM patients who visited the Breast Department of the Shuguang Hospital Affiliated to Shanghai University of Traditional Chinese Medicine between August 2020 and December 2022. Inclusion criteria: ① 18 to 60 years old; ② women; ③ meets GLM diagnostic criteria; ④ clinical data integrity; exclusion criteria: ① nursing and pregnant women; ② those who have been treated with antibiotics or glucocorticoids since onset of disease; ③ those with primary cardiovascular, cerebrovascular, endocrine, hepatic, renal or haematopoietic disease who are unstable and require medical treatment; ④ incomplete clinical data related to the study; ⑤ combined malignant tumours.
The current study conformed to the principles drafted in the Helsinki declaration and was approved by the medical ethical committee of Shuguang Hospital Affiliated to Shanghai University of Traditional Chinese Medicine (approval number: 2021–956-31-01). Informed consent was obtained from all patients.
Methods
Diagnostic Criteria of GLM
GLM diagnostic criteria refer to the《Management of Granulomatous Lobular Mastitis: an International Multidisciplinary Consensus》 (2021 edition):5 Clinical manifestations include breast lumps and inverted nipples, nipple discharge, breast pain, and breast lumps forming abscesses secondary to acute infection based on chronic lesions.
Grouping
The patients were divided into an abscess group (85 cases) and a non-abscess group (41 cases) according to whether or not the breast magnetic resonance imaging (MRI) was accompanied by abscess formation.
The Indication for the Use of MRI
According to the consensus, magnetic resonance imaging (MRI) is a useful imaging modality to indicate active lesions, locate the extent of the lesions or monitor the disease in patients who underwent conservative treatment. All patients in this study wished to undergo further surgery after conservative treatment. Therefore, the patients underwent MRI to assess the effectiveness of conservative treatment and the need for further surgical intervention.
Observation Indicators
We collected and recorded the clinical data of all patients with GLM, including age, body mass index (BMI), reproductive history, staging of the course of the disease, WBC, N, CRP, ESR, IL-4, IL-6, IL-10, IL-17, INF-α, and breast MRI.
Statistical Analysis
Univariate and multivariate analyses were performed using logistics regression. The dependent variables were binary ones, in which non-abscess group was assigned a value of 0 and abscess group a value of 1. Among the independent variables, reproductive history and staging of the course of the disease are categorical variables. The units of continuous variables age, BMI, WBC, CRP, ESR, N, IL-4, IL-6, IL-10, IL-17, INF-α were years, kg/m2, ×109/L, mg/L, mm/h, ×109/L, pg/mL, respectively. Variance inflation factors were calculated in multivariate analyses for covariance testing. Based on the results of multivariate regression analysis, the nomogram was depicted to visualize the model. The discrimination, accuracy, and practicability of the model were evaluated using the receiver operating characteristic (ROC) curve, calibration curve, and decision curve analysis (DCA), respectively. Statistical analyses were performed with R software (version 3.5.3) and SPSS (version 24.0). All tests were two sided. A value of P less than 0.05 was considered significant.
Results
MRI Manifestations of GLM Abscess Formation
GLM lesions in the abscess stage become more involved and MRI shows large sheets of long T1 and long T2 signals. Typically, single or multiple rounded or irregular pus cavities of varying sizes are seen in the lesion, some of which are honeycombed and show low signal on T1W1 and high signal on T2W1 (Figures 1 and 2). Enhancement shows circumferential enhancement of the abscess wall and no enhancement of the central pus. The majority of patients in this study presented with honeycomb abscess formation (n=59, 69.41%), with abscess cavities that were not connected to each other; in addition, 26 patients (30.59%) presented with abscesses that were a single large abscess cavity.
 |
Figure 1 GLM abscess formation with honeycomb changes (left T2WI, right T1W1). The red arrows represent abscess formation with a honeycomb shape. High signal in T2W1, low signal in T1W1. |
 |
Figure 2 GLM with multiple irregular abscess formation (left T2WI, right T1W1). The red arrow indicates the location of the abscess cavity. High signal in T2W1, low signal in T1W1. |
Univariate Analysis of GLM with Abscess Formation
A total of 126 patients with GLM were enrolled, including 41 cases in the non-abscess group and 85 cases in the abscess group. All patients had no missing statistical values, which is shown in Figure 3. The univariate analyses of continuous variables revealed that there was no statistically significant difference between the two groups in terms of age, BMI, reproductive history, stage of disease (P>0. 05). WBC, N, CRP, ESR, IL-10, and IL-6 were higher in the abscess group than in the non-abscess group, and IL-4, IL-17, and INF-α were lower than in the non-abscess group (P < 0. 05) (Table 1).
 |
Table 1 Univariate Analysis of General Information and Clinical Characteristics of the Two Groups |
 |
Figure 3 Statistical chart of missing values for GLM. Abbreviations: BMI, body mass index; reproductive, reproductive history; stage, staging of the course of the disease; WBC, white blood cell; N, neutrophil count; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; IL-4, interleukin-4; IL-6, interleukin-6; IL-10, interleukin-10; IL-17, interleukin-17; INF-α, interferon-alpha. |
Multivariate Analysis of Factors Related to Abscess Formation in GLM
Variables with a P-value <0.05 in the univariate analysis were enrolled in the multivariate analysis. The results revealed that WBC(P=0.003), N(P=0.002), ESR(P<0.001), IL-4(P=0.005), IL-10(P=0.008) and INF-α(P=0.004) were independent risk factors for GLM formation (Table 2). At the same time, the collinearity test demonstrated that the variance inflation factor of WBC, N, ESR, IL-4, IL-10 and INF-α was 29.86, 30.86, 1.68, 1.31, 1.88 and 1.54, respectively. The variance inflation factors for WBC and N were greater than 10, indicating collinearity between these two indicators, N with a smaller P-value was selected in the multivariate analysis. Based on the multivariate logistic regression model, a visible nomogram was developed, which is shown in Figure 4.
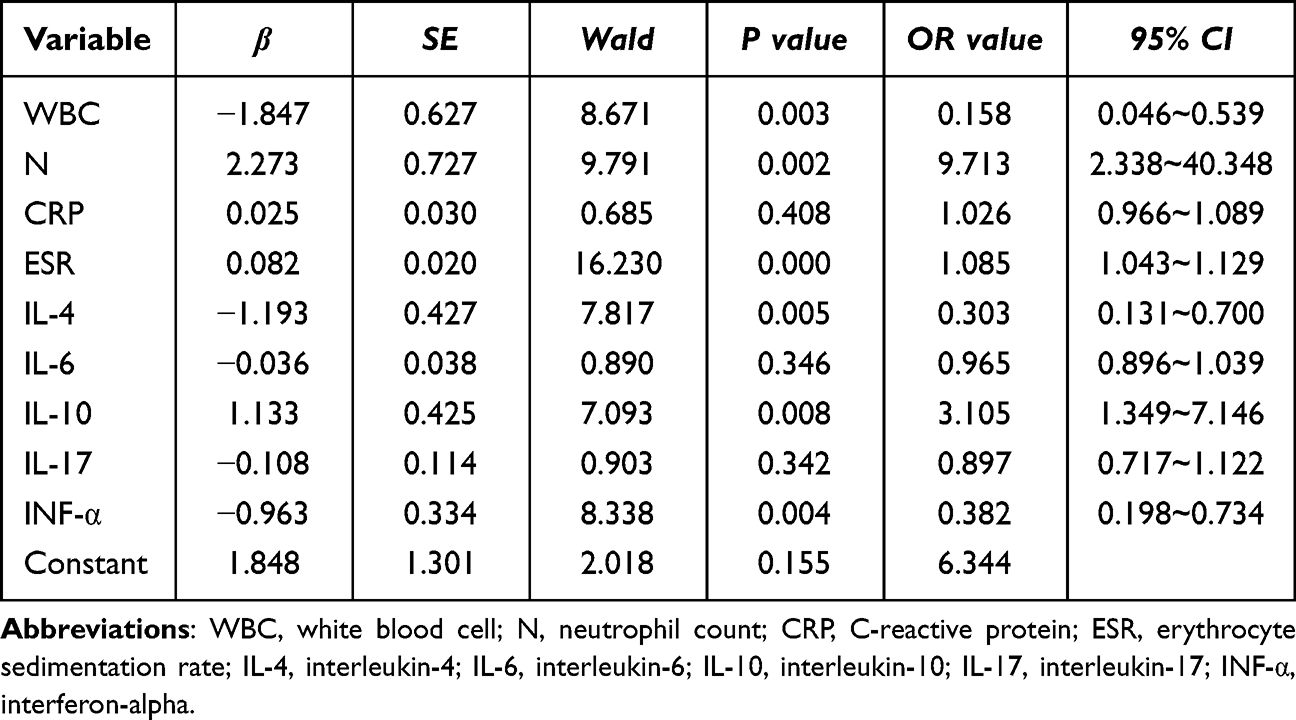 |
Table 2 Logistics Multivariate Analysis of GLM Abscess Formation |
 |
Figure 4 Nomogram of differential diagnosis of abscess formation in GLM. Abbreviations: N, neutrophil count; ESR, erythrocyte sedimentation rate; IL-4, interleukin-4; IL-10, interleukin-10; INF-α, interferon-alpha. |
Predictive Value of Individual and Combined Multi-Indicator Early Warning Models for Abscess Formation in GLM
The ROC curves of N, ESR, IL-4, IL-10, INF-α, and the regression model are shown in Figure 5. The area under the curve (AUC) of the model was 0.890 (95% CI: 0.834–0.946), which was significantly better than that of each single factor (N: 0.789, 95% CI: 0.702–0.876; ESR: 0.825, 95% CI: 0.747–0.902; IL-4: 0.654, 95% CI: 0.552–0.757; IL-10: 0.625, 95% CI: 0.522–0.757; INF-α: 0.633, 95% CI: 0.524–0.742). In addition, the model showed higher sensitivity and specificity (81.2 and 85.4%, respectively) (Table 3). The calibration curve showed that the diagnostic results using the present model were highly consistent with the actual diagnostic results (Figure 6). DCA showed a satisfactory positive net benefit of the model, which indicated the value of the model in the clinical differential diagnosis (Figure 7). The Hosmer-Lemeshow test showed χ2=6.173, P=0.628 >0.05, suggesting that there is no statistically significant difference between the model predictions and the actual observations, and that the predictive model has a good calibration ability (Table 4).
 |
Table 3 Predictive Value of N, ESR, IL-4, IL-10, INF-α and Regression Models for GLM Abscess Formation |
 |
Table 4 Hosmer and Lemeshow Test |
 |
Figure 5 ROC curves for prediction of GLM abscess formation by N, ESR, IL-4, IL-10, INF-α and the regression model. Abbreviations: AUC, area under the curve; ROC, receiver operator characteristic; N, neutrophil count; ESR, erythrocyte sedimentation rate; IL-4, interleukin-4; IL-10, interleukin-10; INF-α, interferon-alpha. |
 |
Figure 6 Calibration curves for predictive models of abscess formation in GLM. |
 |
Figure 7 Decision curve of nomogram graph. |
Discussion
The univariate analysis showed that WBC, CRP, ESR, N, IL-4, IL-6, IL-10, IL-17, and INF-α were associated with abscesses formation. After excluding collinearity indicators, the results of multiple indicators revealed that N, ESR, IL-4, IL-10, and INF-α were independent diagnostic factors. Subsequently, the nomogram was obtained using the regression model based on the multivariate analysis. The ROC curve showed that the AUC of the model was 0.890 (95% CI: 0.834–0.946), which was significantly better than that of every single factor. The model had high sensitivity and specificity (81.2 and 85.4%, respectively). The calibration curve and DCA curve revealed that the model had high diagnostic accuracy and positive net benefit, which indicated the value of the model in the differential diagnosis of abscess formation in GLM.
An intense inflammatory response may be important in promoting the formation of GLM abscesses, as reflected by changes in various inflammatory markers. Cystic neutrophilic granulomatous mastitis (CNGM) is a newly identified form of GLM with unique pathological features, which is closely related to Corynebacterium infection.19,20 In addition to the fact that such patients are more likely to form extensive abscesses at the site of the lesion,11,21 there is a higher incidence of extra-mammary symptoms such as fever, erythema of the lower extremities, and joint pain. All of these clinical manifestations are associated with a more intense inflammatory storm response in the patient’s body as evidenced by a significant increase in ESR, N, IL-10 and a decrease in IL-4, INF-α.
As non-specific inflammatory marker, the diagnostic performance of N, ESR is often underestimated in laboratory diagnosis, and all of these can be used to predict abscess formation in a variety of diseases.22 Studies have shown that N and ESR are risk factors for the development of pyogenic spondylodiscitis (PS), soft tissue abscesses of the forearm and hand, and intra-abdominal abscesses (IA), which promotes abscess formation and improves the positive predictive values (PPV) in patients.23–25 Yildirim et al reported significantly elevated levels of neutrophil to lymphocyte ratio(NLR) in tubo-ovarian abscesses, with an NLR value >4.15 having a sensitivity of 95.2% and a specificity of 99.4% for diagnosing tubo-ovarian abscesses.26 GLM with erythema nodosum often suggests a more aggressive disease, characterised by the appearance of slightly red, tender nodules on the lower legs. These patients have significantly higher serum ESR, N and are more likely to have abscesses in the breast that can break down and form fistulas.27 It has been found that GLM abscess formation is associated with N and ESR, and that high levels of N and ESR can promote GLM abscess formation.9,10,28 ESR refers to the rate at which erythrocytes settle under certain conditions, which is related to inflammatory factors in the plasma, the number of erythrocytes, fibrin, etc. During abscess formation, an elevated ESR may indirectly reflect the intensity of inflammation in the body.
GLM is an autoimmune disease and cytokines can be used to assess the degree of immune dysregulation in patients, which may play an important role in the pathogenesis of GLM.29–33 Koksal et al investigated the expression levels of IL-4, IL-8, IL-10 and IL-17 in patients with GLM and showed that the levels of IL-8, IL-10 and IL-17 were significantly increased and the levels of IL-4 were decreased in patients with GLM.33 IL-4 and IL-10 can be used to assess T helper cell type 2 (Th2) cell function, IL-8 levels can be used to assess neutrophil chemotaxis and IL-17 can be used to assess inflammation and T helper cell type 17 (Th17) cell function. Coskun et al further analysed the changes in cytokine profiles in patients with active and remission GLM, and their results showed that patients with active GLM may have elevated IL-8 and IL-17 and reduced IL-10, but none of these results were significant.34 Therefore, the authors concluded that cytokines may play a role in autoimmune and granulomatous reactions and have a less significant role in the pathogenesis of GLM. Thus, instead of focusing on the role of cytokines in the pathogenesis of GLM, our study focused on the analysis of cytokine changes during abscess formation.
To our knowledge, this study is the first to investigate the correlation between serum cytokine changes and GLM abscess formation. Histopathological examination of GLM lesion tissue in previous studies has shown that the number of abscess formations was significantly correlated with the inflammatory infiltration, which was manifested by a large number of neutrophil aggregates at the site of the abscess.34 This is consistent with our serological findings that serum neutrophil levels are positively correlated with GLM abscess formation. Neutrophils are important innate immune cells that can participate in the early host defence response during infection/injury through a variety of pathways, including phagocytosis, degranulation, generation of reactive oxygen species and release of the neutrophil extracellular traps (NETs).35,36 In contrast, dysregulation of neutrophil recruitment, activation or clearance is a major cause of the development and persistence of many chronic inflammatory diseases.37 The process of abscess formation is regulated by a combination of neutrophil infiltration, phagocytosis and neutrophil extracellular trap (NET) formation, a process involving multiple cytokines.38–41
IL-4 is central to T helper cell type 2 (TH2) responses, commonly associated with parasite infections and allergies.42 Recent studies have shown that IL-4 not only reduces local inflammation by inhibiting neutrophil migration through the IL-4/IL-4Rα pathway, but also prevents damage to healthy tissue by inhibiting the formation of neutrophil extracellular traps (NETs) through antagonism of granulocyte colony-stimulating factor (GCSF).43,44 Results from animal studies also showed that IL-4 levels were reduced in septic rats with elevated serum neutrophil counts, and as the sepsis improved, serum IL-4 increased and neutrophil counts decreased.45 These results indirectly confirm that IL-4 was negatively associated with GLM abscess formation in the present study and that the mechanism may be related to the inhibition of neutrophil chemotaxis by IL-4 and the formation of neutrophil extracellular traps (NETs).
IL-10 is a classical immunosuppressive factor synthesised mainly by T cells, macrophages, monocytes and B cells and may play an important role in maintaining tissue homeostasis during infection and inflammation by limiting excessive inflammatory responses, upregulating innate immunity and promoting tissue repair mechanisms.46 Neutrophils are the main target cells for the anti-inflammatory effects of IL-10, which not only significantly inhibits neutrophil chemotaxis and aggregation, but also accelerates the induction of neutrophil apoptosis.38,47 Phagocytosis of apoptotic neutrophils is upregulated with the release of IL-10, and as they disintegrate due to their own apoptosis, they release a variety of lysosomal enzymes that lyse the surrounding tissue and form an abscess.48,49 In addition to its anti-inflammatory effects, IL-10 has pro-inflammatory properties that can characterise aggressive inflammation by switching the function of regulatory B cells from inducing CD8+ T cell tolerance to inducing inflammatory CD4+ T cell responses.50 In our study, IL-10 is a risk factor for GLM abscess formation, and the mechanism may be related to the induction of neutrophil apoptosis and increased inflammatory aggressiveness.
The IFN-α protein family consists of multiple subtypes that contain a 23-amino-acid hydrophobic signal peptide and a 166-amino-acid mature peptide sequence. A variety of immune cells in the body, such as macrophages and dendritic cells (DCs), could produce IFN-α in response to pathogen stimulation of pattern recognition receptors (PRRs).51 Dysregulated IFN-α signaling could cause inflammatory diseases, including autoimmune diseases and chronic infections.52,53 In autoimmune diseases, IFN-α may exert anti-inflammatory effects by inhibiting neutrophil recruitment and reducing the release of reactive oxygen species (ROS) and proteases.54 When serum IFN-α levels are reduced in patients with GLM, neutrophil recruitment and activation are significantly enhanced and may further form NETs to promote abscess formation.
Although the relationship between GLM abscess formation and serum inflammatory markers was explored in this study, the following shortcomings remain: Firstly the present study has not explored the specific molecular mechanisms by which inflammatory indicators promote GLM abscess formation, which may be an important direction for future research. Secondly, the sample size of the study is still small, although univariate analysis found differences in inflammatory indicators such as IL-6, IL-8, and IL-17, multivariate analysis did not yield the desired results, and future expansion of the sample size is needed to strengthen the statistical power and validate the significance of the findings. Thirdly, it was limited by the sample size, and therefore the established model was only verified internally rather than externally. External verification needs to be performed in future prospective studies. In conclusion, this study found that elevated N, ESR, and IL-10 as well as decreased IL-4, and INF-α were risk factors for GLM abscess formation. The best cut-off values were 5.56×109/L, 35.50 mm/h, 0.93 pg/mL, 0.97 pg/mL, and 1.85 pg/mL, respectively, with the largest area under the curve and the strongest predictive efficacy for joint prediction. Early detection of abscess formation is important in the treatment of GLM, and as our previous clinical studies have suggested, herbs can be very effective in treating the early stages of abscess formation, not only in reducing the size of the breast lump and preserving the appearance of the breast, but also in minimising the physiological and psychological pain associated with surgery. Therefore, when N>5.56×109/L, ESR>35.5mm/h, IL-10>0.93pg/mL and IL-4<0.97pg/mL, INF-α<1.85pg/mL, the abscess formation should be fully considered so as not to delay the timing of the most effective herbal treatment.
Conclusion
Abscess formation is an important marker of the progression of inflammation in GLM and also an important point in determining whether a patient requires surgical intervention. Early detection of abscess formation and treatment with herbal remedies is important to avoid surgery and reduce damage to the patient’s breast shape. Our research underscores the practicality and effectiveness of several inflammatory biomarkers-N, ESR, IL-4, IL-10, INF-α in facilitating the early diagnosis of GLM abscess formation. These insights are important in guiding clinicians in recognising and treating the early stages of abscesses in patients with GLM and may improve clinical outcomes. However, larger sample sizes and specific experimental designs are needed to validate the results of this study in the future.
Acknowledgments
This paper was supported by grants from the Shanghai Municipal Health Commission (No.202040254).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Shi L, Wu J, Hu Y., et al. Biomedical indicators of patients with granulomatous lobular mastitis: a retrospective study. Nutrients. 2022;14(22):4816. doi:10.3390/nu14224816
2. Azizi A, Prasath V, Canner J, et al. Idiopathic granulomatous mastitis: management and predictors of recurrence in 474 patients. Breast J. 2020;26(7):1358–1362. doi:10.1111/tbj.13822
3. Bhattarai P, Srinivasan A, Valenzuela CD, et al. Idiopathic granulomatous mastitis: experience at a New York hospital. Ann R Coll Surg Engl. 2022;104(7):543–547. doi:10.1308/rcsann.2021.0239
4. Chen W, Zhang D, Zeng Y, et al. Clinical characteristics and microbiota analysis of 44 patients with granulomatous mastitis. Front Microbiol. 2023;14:1175206. doi:10.3389/fmicb.2023.1175206
5. Yuan QQ, Xiao SY, Farouk O, et al. Management of granulomatous lobular mastitis: an international multidisciplinary consensus. Mil Med Res. 2022;9(1):20. doi:10.1186/s40779-022-00380-5
6. Liu PZ, Shi XG, Zuo XM, et al. A clinical study on the treatment of granulomatous lobular mastitis by the external application of the internal pus-expelling decoction and operation. Ann Palliat Med. 2020;9(5):2631–2641. doi:10.21037/apm-19-684
7. Chen L, Zhang XY, Wang YW, et al. Zhonghua Bing Li Xue Za Zhi. Zhonghua Bing Li Xue Za Zhi = Chin J Pathol. 2019;48(3):231–236. doi:10.3760/cma.j.issn.0529-5807.2019.03.012
8. Du NN, Wan H, Feng JM, et al. Comparison of clinical efficacy of tuoli xiaodu powder and chaihu qinggan decoction in treatment of granulomatous lobular mastitis with intense heat induced flesh decay syndrome at early stage of abscess: a randomized controlled study [J/OL]. Chin J Integ Tradit West Med. 2023; 20: 1–7.
9. Zeng W, Lao S, Jia W, et al. Clinical features and recurrence of Corynebacterium kroppenstedtii infection in patients with mastitis. BMC Womens Health. 2022;22(1):276. doi:10.1186/s12905-022-01859-y
10. Johnstone KJ, Robson J, Cherian SG, et al. Cystic neutrophilic granulomatous mastitis associated with Corynebacterium including Corynebacterium kroppenstedtii. Pathology. Pathology. 2017;49(4):405–412. doi:10.1016/j.pathol.2017.01.006
11. Shao SJ, Wu LL, Wu XQ, et al. Clinical and prognostic characteristics of cystic neutrophilic granulomatous mastitis[J]. J Cap Med Univer. 2023;44(04):676–683.
12. Lai XL, Wang XQ, Mai JL, et al. Ausiologic characteristics of abscess-type granulomatous mastitis and changes in NLRP3 and IL-1β expression[J]. Chin J Nosocomiol. 2023;33(10):1540–1544.
13. Dos Santos AAC, Rodrigues LE, Alecrim-Zeza AL, et al. Molecular and cellular mechanisms involved in tissue-specific metabolic modulation by SARS-CoV-2. Front Microbiol. 2022;13:1037467. doi:10.3389/fmicb.2022.1037467
14. de Souza AP, Vale VL, Silva Mda C, et al. MAPK involvement in cytokine production in response to Corynebacterium pseudotuberculosis infection. BMC Microbiol. 2014;14(1):230. doi:10.1186/s12866-014-0230-6
15. Specht S, Volkmann L, Wynn T, et al. Interleukin-10 (IL-10) counterregulates IL-4-dependent effector mechanisms in murine filariasis. Infect Immun. 2004;72(11):6287–6293. doi:10.1128/IAI.72.11.6287-6293.2004
16. Luzina IG, Keegan AD, Heller NM, et al. Regulation of inflammation by interleukin-4: a review of ”alternatives”. J Leukoc Biol. 2012;92(4):753–764. doi:10.1189/jlb.0412214
17. Croxford AL, Karbach S, Kurschus FC, et al. IL-6 regulates neutrophil microabscess formation in IL-17A-driven psoriasiform lesions. J Invest Dermatol. 2014;134(3):728–735. doi:10.1038/jid.2013.404
18. Zhang C, Asif H, Holt GE, et al. Mycobacterium abscessus-bronchial epithelial cells cross-talk through type I interferon signaling. Front Immunol. 2019;10:2888. doi:10.3389/fimmu.2019.02888
19. Aljawder AAA, Jjx L, Jkm N, et al. Idiopathic granulomatous mastitis and cystic neutrophilic granulomatous mastitis: two sides of the same coin or distinct entities? Pathology. 2023;55(3):335–341. doi:10.1016/j.pathol.2022.09.005
20. Troxell ML, Gordon NT, Doggett JS, et al. Cystic neutrophilic granulomatous mastitis: association with gram-positive bacilli and Corynebacterium. Am J Clin Pathol. 2016;145(5):635–645. doi:10.1093/ajcp/aqw046
21. Li S, Huang Q, Song P, et al. Clinical characteristics and therapeutic strategy of granulomatous mastitis accompanied by Corynebacterium kroppenstedtii: a retrospective cohort study. BMC Womens Health. 2023;23(1):388. doi:10.1186/s12905-023-02509-7
22. Zheng Y, Wang L, Han X, et al. Combining contrast-enhanced ultrasound and blood cell analysis to improve diagnostic accuracy of plasma cell mastitis. Exp Biol Med. 2022;247(2):97–105. doi:10.1177/15353702211049361
23. Yoon YK, Jo YM, Kwon HH, et al. Differential diagnosis between tuberculous spondylodiscitis and pyogenic spontaneous spondylodiscitis: a multicenter descriptive and comparative study. Spine J. 2015;15(8):1764–1771. doi:10.1016/j.spinee.2015.04.006
24. Blumenthal SR, Cheema AN, Zhang SE, et al. Evaluating the utility of inflammatory markers in the diagnosis of soft tissue abscesses of the forearm and hand. J Bone Jt Infect. 2023;8(2):119–123. doi:10.5194/jbji-8-119-2023
25. Levartovsky A, Barash Y, Ben-Horin S, et al. Machine learning for prediction of intra-abdominal abscesses in patients with crohn’s disease visiting the emergency department. Therap Adv Gastroenterol. 2021;14:
26. Yildirim M, Turkyilmaz E, Avsar AF. Preoperative neutrophil-to-lymphocyte ratio has a better predictive capacity in diagnosing tubo-ovarian abscess. Gynecol Obstet Invest. 2015;80(4):234–239. doi:10.1159/000371762
27. Velidedeoğlu M, Papila Kundaktepe B, Mete B, et al. Idiopathic granulomatous mastitis associated with erythema nodosum may indicate a worse prognosis. Int J Rheum Dis. 2021;24(11):1370–1377. doi:10.1111/1756-185X.14218
28. Akalın C, Altas H, Akcay Celik M. White blood count can be a practical guide for the differential diagnosis of breast abscess and idiopathic granulomatous mastitis. Cureus. 2020;12(9):e10468. doi:10.7759/cureus.10468
29. Saydam M, Yilmaz KB, Sahin M, et al. New findings on autoimmune etiology of idiopathic granulomatous mastitis: serum IL-17, IL-22 and IL-23 levels of patients. J Invest Surg. 2021;34(9):993–997. doi:10.1080/08941939.2020.1725190
30. Alungal J, Abdulla MC, Narayan R. Idiopathic granulomatous mastitis with erythema nodosum and polyarthritis. Reumatismo. 2016;68(2):97–99. doi:10.4081/reumatismo.2016.844
31. Fruchter R, Castilla C, Ng E, et al. Erythema nodosum in association with idiopathic granulomatous mastitis: a case series and review of the literature. J Eur Acad Dermatol Venereol. 2017;31(9):e391–e393. doi:10.1111/jdv.14194
32. Koksal H, Vatansev H, Artac H, et al. The clinical value of interleukins-8, −10, and −17 in idiopathic granulomatous mastitis. Clin Rheumatol. 2020;39(5):1671–1677. doi:10.1007/s10067-020-04925-8
33. Cakir C, Nayci AE, Ferlengez E, et al. Cytokines the etiology of idiopathic granulomatous mastitis. J Coll Physicians Surg Pak. 2022;32(7):869–873. doi:10.29271/jcpsp.2022.07.869
34. Azzam MI, Alnaimat F, Al-Nazer MW, et al. Idiopathic granulomatous mastitis: clinical, histopathological, and radiological characteristics and management approaches. Rheumatol Int. 2023;43(10):1859–1869. doi:10.1007/s00296-023-05375-6
35. Ogawa Y, Muto Y, Kinoshita M, et al. Neutrophil extracellular traps in skin diseases. Biomedicines. 2021;9(12):1888. doi:10.3390/biomedicines9121888
36. Fousert E, Toes R, Desai J. Neutrophil extracellular traps (NETs) take the central stage in driving autoimmune responses. Cells. 2020;9(4):915. doi:10.3390/cells9040915
37. Ward C, Murray J, Clugston A, et al. Interleukin-10 inhibits lipopolysaccharide-induced survival and extracellular signal-regulated kinase activation in human neutrophils. Eur J Immunol. 2005;35(9):2728–2737. doi:10.1002/eji.200425561
38. Morita Y, Saito M, Rangel-Moreno J, et al. Systemic IL-27 administration prevents abscess formation and osteolysis via local neutrophil recruitment and activation. Bone Res. 2022;10(1):56. doi:10.1038/s41413-022-00228-7
39. von Stebut E, Boehncke WH, Ghoreschi K, et al. IL-17A in psoriasis and beyond: cardiovascular and metabolic implications. Front Immunol. 2020;10:3096. doi:10.3389/fimmu.2019.03096
40. Navrazhina K, Frew JW, Gilleaudeau P, et al. Epithelialized tunnels are a source of inflammation in hidradenitis suppurativa. J Allergy Clin Immunol. 2021;147(6):2213–2224. doi:10.1016/j.jaci.2020.12.651
41. Putz EJ, Palmer MV, Ma H, et al. Case report: characterization of a persistent, treatment-resistant, novel Staphylococcus aureus infection causing chronic mastitis in a holstein dairy cow. BMC Vet Res. 2020;16(1):336. doi:10.1186/s12917-020-02528-8
42. Walker JA, McKenzie ANJ. TH2 cell development and function. Nat Rev Immunol. 2018;18(2):121–133. doi:10.1038/nri.2017.118
43. Impellizzieri D, Ridder F, Raeber ME, et al. IL-4 receptor engagement in human neutrophils impairs their migration and extracellular trap formation. J Allergy Clin Immunol. 2019;144(1):267–279.e4. doi:10.1016/j.jaci.2019.01.042
44. Egholm C, Heeb LEM, Impellizzieri D, et al. The regulatory effects of interleukin-4 receptor signaling on neutrophils in type 2 immune responses. Front Immunol. 2019;10:2507. doi:10.3389/fimmu.2019.02507
45. Yue L, Liu X, Wu C, et al. Toll-like receptor 4 promotes the inflammatory response in septic acute kidney injury by promoting p38 mitogen-activated protein kinase phosphorylation. J Bioenerg Biomembr. 2023;55(5):353–363. doi:10.1007/s10863-023-09972-9
46. Ouyang W, O’Garra A. IL-10 family cytokines IL-10 and IL-22: from basic science to clinical translation. Immunity. 2019;50(4):871–891. doi:10.1016/j.immuni.2019.03.020
47. Wang X, Wong K, Ouyang W, et al. Targeting IL-10 family cytokines for the treatment of human diseases. Cold Spring Harb Perspect Biol. 2019;11(2):a028548. doi:10.1101/cshperspect.a028548
48. Schroeder-Castagno M, Del Rio-Serrato A, Wilhelm A, et al. Impaired response of blood neutrophils to cell-death stimulus differentiates AQP4-IgG-seropositive NMOSD from MOGAD. J Neuroinflam. 2022;19(1):239. doi:10.1186/s12974-022-02600-0
49. Zizzo G, Cohen PL. IL-17 stimulates differentiation of human anti-inflammatory macrophages and phagocytosis of apoptotic neutrophils in response to IL-10 and glucocorticoids. J Immunol. 2013;190(10):5237–5246. doi:10.4049/jimmunol.1203017
50. Wang XY, Wei Y, Hu B, et al. c-Myc-driven glycolysis polarizes functional regulatory B cells that trigger pathogenic inflammatory responses. Signal Transduct Target Ther. 2022;7(1):105. doi:10.1038/s41392-022-00948-6
51. Ji L, Li T, Chen H, et al. The crucial regulatory role of type I interferon in inflammatory diseases. Cell Biosci. 2023;13(1):230. doi:10.1186/s13578-023-01188-z
52. Fernandez-Ruiz R, Niewold TB. Type I Interferons in Autoimmunity. J Invest Dermatol. 2022;142(3 Pt B):793–803. doi:10.1016/j.jid.2021.11.031
53. McNab F, Mayer-Barber K, Sher A, et al. Type I interferons in infectious disease. Nat Rev Immunol. 2015;15(2):87–103. doi:10.1038/nri3787
54. Harigai M. Growing evidence of the safety of JAK inhibitors in patients with rheumatoid arthritis. Rheumatology. 2019;58(Suppl 1):i34–i42. doi:10.1093/rheumatology/key287
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.