")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 15
Comprehensive Knowledge, Attitudes, Behaviors, and Associated Factors of HIV/AIDS in Gondar City Public Health Facilities Among HIV Testing and Counselling Service Users, Northwest Ethiopia, 2022; an Ordinal Logistic Regression Analysis
Authors Terefe B , Techane MA , Assimamaw NT
Received 17 October 2023
Accepted for publication 25 November 2023
Published 7 December 2023 Volume 2023:15 Pages 713—726
DOI https://doi.org/10.2147/HIV.S441447
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Bewuketu Terefe,1 Masresha Asmare Techane,2 Nega Tezera Assimamaw2
1Department of Community Health Nursing, School of Nursing, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Department of Pediatric and Child Health, School of Nursing, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Bewuketu Terefe, Department of Community Health Nursing, School of Nursing, College of Medicine and Health Sciences, University of Gondar, Post Office Box: 196, Gondar, Amhara Region, Ethiopia, Tel +251918099504, Email [email protected]
Background: The primary cause of HIV transmission is a failure to deliver proper HIV/AIDS information, which is a major public health issue in low- and middle-income nations. While global health coverage continues, there is still little understanding of HIV/AIDS in Ethiopia, and there is a data gap. As a result, the aim of this study was to investigate the factors that influence comprehensive HIV/AIDS knowledge among HIV testing and counselling (HTC) service users in Gondar, northwest Ethiopia.
Methods: A facility-based cross-sectional study was conducted from June to July 2022. About 423 clients were included. Data on HIV/AIDS knowledge, attitude, and behavior were collected. Stata 17 was used to analyze. A pre-tested questionnaires were used. Using ordinal logistic regression model, variables having p values of 0.2 and < 0.05 were chosen as a candidate variable in binary and final model.
Results: The total knowledge, favorable attitude, and good behaviors of HIV/AIDS were approximately 258 (61%), 220 (52%), and 210 (49.5%), respectively. Being male (AOR = 1.39, 95% CI = 1.28– 3.01), age from 31 to 35 years (AOR = 2.13, 95% CI = 1.88– 4.18), and above 36 years old (AOR = 2.21, 95% CI = 1.98– 3.44), primary (AOR = 1.21, 95% CI = 1.67– 3.20), and higher education (AOR = 1.19, 95% CI = 1.03– 3.01), employed (AOR = 1.33, 95% CI = 1.09, 3.37), and media exposure (AOR = 2.02, 95% CI = 1.21, 3.61) were factors associated with comprehensive knowledge of HIV/AIDS, respectively.
Conclusion: The study participants’ knowledge, attitudes, and behaviors regarding HIV/AIDS were rather low. Since HIV/AIDS is still a major public health issue, if the concerned body uses and designs media effectively, encouraging females to attend school, it will have a better chance of combating HIV/AIDS by increasing their knowledge.
Keywords: knowledge, attitude, behavior, factors, ordinal logistic regression, HIV/AIDS, Ethiopia
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Fikri has been published for this article.
Introduction
The 2021 World Health Organization (WHO) and USAIDS updated report estimated that about 36 million adult people are living with HIV, 1.3 million new people will acquire HIV infection, and 580,000 people will die from HIV-related causes in 2020(1). The report also indicated that the African region remains the most severely attacked, with a proportion of one every 25 adults, which accounts for two-thirds of the globe.1,2 Hence, HIV/AIDS is the most fatal infectious disease; it accounted for 1.5% of deaths in the world in 2019. However, the rate is much higher in Africa, at approximately 28% across countries.3 The alarming rate of HIV is an important public health issue for women and children in developing countries. For instance, the 2015 report showed that, from a total estimation of 25.6 million people living with HIV, about 59% of them were women of reproductive age,4 and more than 1.2 million infants were exposed to HIV due to the comprehensive knowledge gap in the transmission of HIV, according to UNICEF.5 Globally, less than 30% of women of reproductive age have a thorough understanding of HIV/AIDS.6 As a result, about 90% of sub-Saharan African (SSA) countries were severely hit by HIV/AIDS, with reproductive-age women bearing the brunt of the pandemic.7,8 Furthermore, SSA nations provided 70% of new HIV infections and 74% of AIDS-related fatalities.6
The following factors were identified by several studies as contributing to increasing the transmission rate of HIV: lack of awareness of HIV status, poor knowledge, education level, wealth index, failure to access ART prophylaxis, poor adherence to ART, lack of clinic-based HIV education and counseling, types of residencies, being exposed to mass media, being exposed to HIV/AIDS education, and having taken an HIV test.9–14 In response to the HIV epidemic, the Ethiopian government has been at the forefront of developing and implementing national plans that conform to global directions while combining innovations with best practices within the country.15,16 To raise people’s knowledge of HIV/AIDS, most programs have focused on information education and behavioral change communication. Accurate HIV/AIDS knowledge about transmission and prevention is critical for avoiding HIV infection and eradicating stigma and prejudice against HIV/AIDS patients.17–19
Despite its significance, many Ethiopians lack thorough HIV awareness. According to the 2016 Ethiopian Demographic and Health Survey (EDHS), just 20% and 38% of women and men aged 15–49 years have comprehensive knowledge of HIV/AIDS, respectively.20 The increase in the percentage of women and men with comprehensive HIV/AIDS knowledge between 2011 and 2016 was significantly more moderate, rising from 19% to 20% among women and 32% to 38% among men.21 Despite the achievements and reductions in the HIV epidemic, however, it has remained a challenge for Ethiopia, and a paucity of information is available. One justification could be related to the poor, comprehensive knowledge of the people about HIV and its preventive strategies. So, the current study was intended to assess the adult population’s knowledge and attitude toward HIV/AIDS and its determinant factors in northwest Ethiopia.
Methods and Materials
Study Setting and Period
From June to July 2022, nine public health facilities in Gondar city took part in an institution-based cross-sectional survey. Gondar city, one of the 13 zonal cities of the Amhara regional state in northwest Ethiopia, is composed of 6 sub-cities, 11 semi-urban kebeles, and 27 urban kebeles (the smallest administrative unit in Ethiopia). According to the city administration’s population register, Gondar today has a population of over 700,000, even though the city’s health sector annual plan for Ethiopian Fiscal Year (EFY) 2012 includes a total population of over 344,046 based on the census report from 10 years ago. Gondar is a city in northwest Ethiopia that is separated from Bahir Dar, the regional state capital, and Addis Ababa by 185 and 738 kilometers, respectively. In the city right now, there is just one complete specialist hospital, eight functioning governmental health centers, and fourteen health posts. In all of the health centers, the voluntary HIV counseling and testing program has begun to be implemented. Similar to other various health services, the University of Gondar Specialist Hospital is the first to break ground, but the Gondar Poly Center is the first to break ground among the health centers. Saint Gabriel, Mintiwab, and Bilajig are three recently built healthcare facilities that make use of the service. Gondar Poly health center, Woleka, Maraki, Azezo, Teda, Saint Gabriel, Mintwanb, and Bilajig Health Centers are the names of the eight health centers that are registered, in that order. In addition to these, the city has more than 20 private healthcare facilities. The districts (named woreda in Ethiopian context) of Chilga and Dambia border the city on the west, the woreda of Gondar Zuria borders the city on the east, and Amba Giorgi’s woreda borders the city on the north. The city is home to private clinics, hospitals, pharmacies, drug sellers, and other community-based voluntary health experts or providers.
Source and Study Population
The source population of this study was all clients visiting the HIV testing and counseling service in all public health facilities in Gondar city, whereas the study population was each client who was attending HIV testing and counseling service centers during the data collection period.
Inclusion and Exclusion Criteria
All adult clients (≥18 years old) who were attending an HIV testing and counseling service consultation centers during the data collection from June to July 2022 were included. On the other hand, client who has a mental disorder was excluded.
Sample Size Determination and Sampling Procedure
The sample size was computed for binary values, but not scores because, of which the power for this study sample size would be higher. The power for finding risk factors is lower than the nominal power, but is likely not too bad, because of the use of 50% as the prevalence in the power formula. Then, the sample size was determined using a single population proportion formula by considering the assumptions  = critical value for normal distribution at a 95% confidence level, which equals 1.96 (z value at α = 0.05), estimated proportion (p = 50%), and absolute precision or margin of error 5% (d = 0.05).
= critical value for normal distribution at a 95% confidence level, which equals 1.96 (z value at α = 0.05), estimated proportion (p = 50%), and absolute precision or margin of error 5% (d = 0.05).  ;
;  ; sample size = 384. Considering 10% of the non-respondents, the final sample size for the study was 423. We opted to use it since we could not identify previous research in Ethiopia with similar population characteristics and study settings as our study participants. Therefore, 423 adult VCT service clients who were receiving VCT services at the time of data collection made up the final sample. Following the launch of the VCT service, the university of Gondar hospital, Azezo, Maraki, Saint Gabriel, Mintwab, Bilajig, Woleka, Maraki, and Teda health centers are have been enrolling in the service and have, on average, 92, 35, 32, 5, 7, 4, 13, and 11 clients visiting the VCT service each day, respectively. Based on the number of patients visiting each health institution each day, the sample was proportionately distributed among them by applying the systematic sampling technique.
; sample size = 384. Considering 10% of the non-respondents, the final sample size for the study was 423. We opted to use it since we could not identify previous research in Ethiopia with similar population characteristics and study settings as our study participants. Therefore, 423 adult VCT service clients who were receiving VCT services at the time of data collection made up the final sample. Following the launch of the VCT service, the university of Gondar hospital, Azezo, Maraki, Saint Gabriel, Mintwab, Bilajig, Woleka, Maraki, and Teda health centers are have been enrolling in the service and have, on average, 92, 35, 32, 5, 7, 4, 13, and 11 clients visiting the VCT service each day, respectively. Based on the number of patients visiting each health institution each day, the sample was proportionately distributed among them by applying the systematic sampling technique.
Data Entry Process
After the completion of data collection, cleaning, editing, and coding were performed in a scientifically rigorous way; then, the data were entered using Epi Data Software version 4.6 and analyzed using Stata 17.0. Any errors were repaired as necessary.
Data Analysis Process, and Measurements
Stata version 17 software was used. Descriptive statistics were used to compute the means and standard deviations of the continuous variables and the frequency of categorical variables. The survey consisted of thirty-two questionnaires, and it was broken up into five sections. First, there were eight variables related to sociodemographic; second, there were five variables related to HIV/AIDS information; third, there were seven variables related to knowledge; fourth, there were eight variables related to attitudes; and fifth, there were four types of variables related to behavior. The correct and incorrect answers were coded as 0, 1, and 2, for knowledge, 0 and 1 for both attitude and behaviors towards HIV/AIDS, respectively. A statistical test using binary and multiple ordinal logistic analysis were conducted to search for any associations. Chi-scores and odds ratios were used in data analysis to examine any relationships between independent variables and the dependent variable.
To generate the overall knowledge, attitude, and behavior score, all correct responses were added accordingly. Respondents correctly responding to at least five of the seven of questions were considered to have “comprehensive knowledge”, and those correctly responding to at least four of the seven knowledge-related questionnaires were considered to have “fair knowledge”, while those correctly responding to only two or none of the seven of HIV/AIDS questions were considered to have “poor knowledge”. The independent determinants of level of knowledge were identified using binary and multiple ordinal logistic regressions. The outcome variable (comprehensive knowledge of HIV/AIDS) was classified as ‘comprehensive, moderate, and poor”. Similarly, to generate the attitude, and behavior results on HIV/AIDS, those participants who scored mean, and above them mean were considered as good/favorable attitude, and good behavior towards HIV/AIDS, respectively. The mean was used over other metrics, because the distribution of the data was normally distributed.
The cutoff criteria for choosing variables for the multiple ordinal logistic regression analysis entry in the binary ordinal logistic regression were a p-value of less than or equal to 0.2. While controlling for confounders, multiple ordinal logistic regression was performed to find independent predictors of knowledge among VCT service users in Gondar city public health facilities. The statistical significance was assessed using the 95% confidence interval (CI) and a P-value of less than 0.05. The variance inflation factor (VIF) was used to construct an ordinal logistic regression to examine multicollinearity among the independent variables. The overall mean of VIF was 1.11. Additionally, the final regression model’s overall fitness was evaluated using the Hosmer and Lemeshow tests.
Data Collection Tools, and Its Sources
After the pre-testing was finished, changes were made to the client’s exit interview questionnaires. The purpose of this was to make the questionnaires more acceptable according to participants understanding level. Some of them were semi-structured; however, most of them were designed as structured questionnaires that were used to collect data. During the implementation of this research, data gathering procedures and instruments related to knowledge of HIV/AIDS, attitudes, and behaviors were adapted from Ethiopian national HIV testing and counseling guidelines and from peer-reviewed literature.22–27 All the questionnaires were administered after the participants had been counselled. Data were collected by face-to-face interviewing.
Data Quality Control
The questionnaire was prepared first in English and then translated to Amharic and translated back to English to observe its consistency. Data were collected through interviews using a structured and pre-tested questionnaire adapted from different literatures. Five senior BSc Nursing professionals were tasked with gathering the information. To ensure consistency and reduce data collection errors, two supervisors have taken on the duty of supervision. Over the course of two days, all data collectors and supervisors attended rigorous, standardized training. Data was reviewed and checked for completeness, accuracy, and consistency by the supervisors and investigators daily, and at the end of the whole data collection process, they supervised the data collection process. To ensure the data quality, a pre-test of 5% among the total sample size of was conducted in Gondar Zuria district. Then, necessary modifications were made to the questionnaire based on the findings.
Statistical Models
There are various ordinal logistic regression models that consider the ordinal form of outcomes. The logits of these various ordinal regression models are formed in various ways. For instance, the proportional odds model (considered as cumulative higher category(s) versus cumulative remaining lower category(s)); the continuation ratio model (considered as cumulative higher category(s) versus just lower category alone); and the adjacent category model (between any two consecutive categories). As a result, each form of the logit has its own set of advantages and disadvantages, and the models can be used to meet individual needs. More specifically, the continuation ratio model and nearby category model do not rely on the entire data set. The proportional odds model (POM) is frequently utilized in epidemiological and biological applications. However, the continuation ratio model is also utilized at times.28,29 Furthermore, the decision between the POM and CRM models is determined by the objectives of the statistical study. As is clear, when nodes are involved, interpretation under POM remains more rational and understandable. If the proportionality assumption is violated, the partial proportional odds model may be a preferable option.30,31 Furthermore, the likelihood ratio tests (LR, AIC, and BIC) were used to evaluate the choice between proportional odds and partial proportional odds models. The POM is utilized if the log odds ratio across the cut points is the same, ie, the proportional odds assumption is satisfied.
Model Goodness Fits and Comparison
Three models, namely, binary logistic, ordinal, and multinomial logistic regressions, were taken as candidates. A strategy that was frequently used was the ordinal logistic regression mode since knowledge levels were listed as poor, moderate, and good. To apply ordinal logistic regression model analysis, the assumption of the POM was assessed using the Stata command or Brant test, and we therefore deployed the ordinal logistic regression model. Actually, the three models and significant factors varied slightly from one another. The POM assumptions, which indicate that the effects of all independent factors are constant across categories of the outcome variable, are necessary in order to select a suitable ordinal model for the data. The proportionate odds assumption was verified by using the omodel Stata command and by the Brant test (p = 0.681) to be true. The AIC, BIC, and LLR were also smaller in ordinal logistic regression models as compared to the others. Therefore, the ordinal model was found to be the best fit over binary and multinomial logistic regressions.
Results
Socio-Demographic Descriptive Characteristics of Participants
In this study, a total of 423 participants participated fully in this implementation study, and there was a 100% response rate. The mean age of responders was 30.17 years, with more than 44% of participants being in the 25–30 age range. Urban residents made up more than two-thirds of the respondents (63.25%). Orthodox Christians made up the bulk of respondents (64.5%), and 42.5% of research participants were married. About 112 (26%) of the clients are employed. In relation to educational attainment, more than 33% of participants had higher education, and 113 (26.71%) of participants’ incomes was above 10,000 Ethiopian birr (178.94 USD) (Table 1).
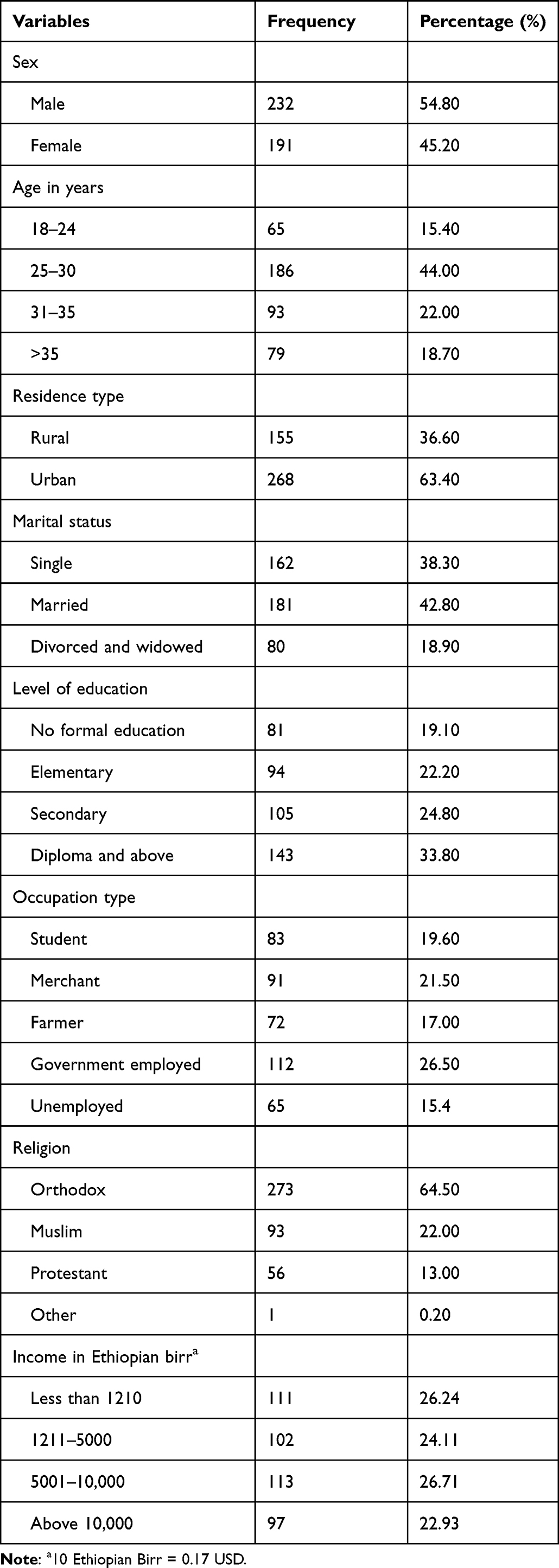 |
Table 1 Socio-Demographic Characteristics of Clients of VCT Service Users in Gondar City Public Health Facilities Northwest Ethiopia, 2022 (n = 423) |
Assessment of Information About HTC/VCT Service
Almost all clients heard about HIV, and about 189 (44.68%) of them have never heard about HIV/AIDS from radio, reading magazines, or newspapers at all. Of the respondents, 53.20% have no cellular phone, and 85.30% are afraid of losing respect from other people if they are positive for HIV (Table 2).
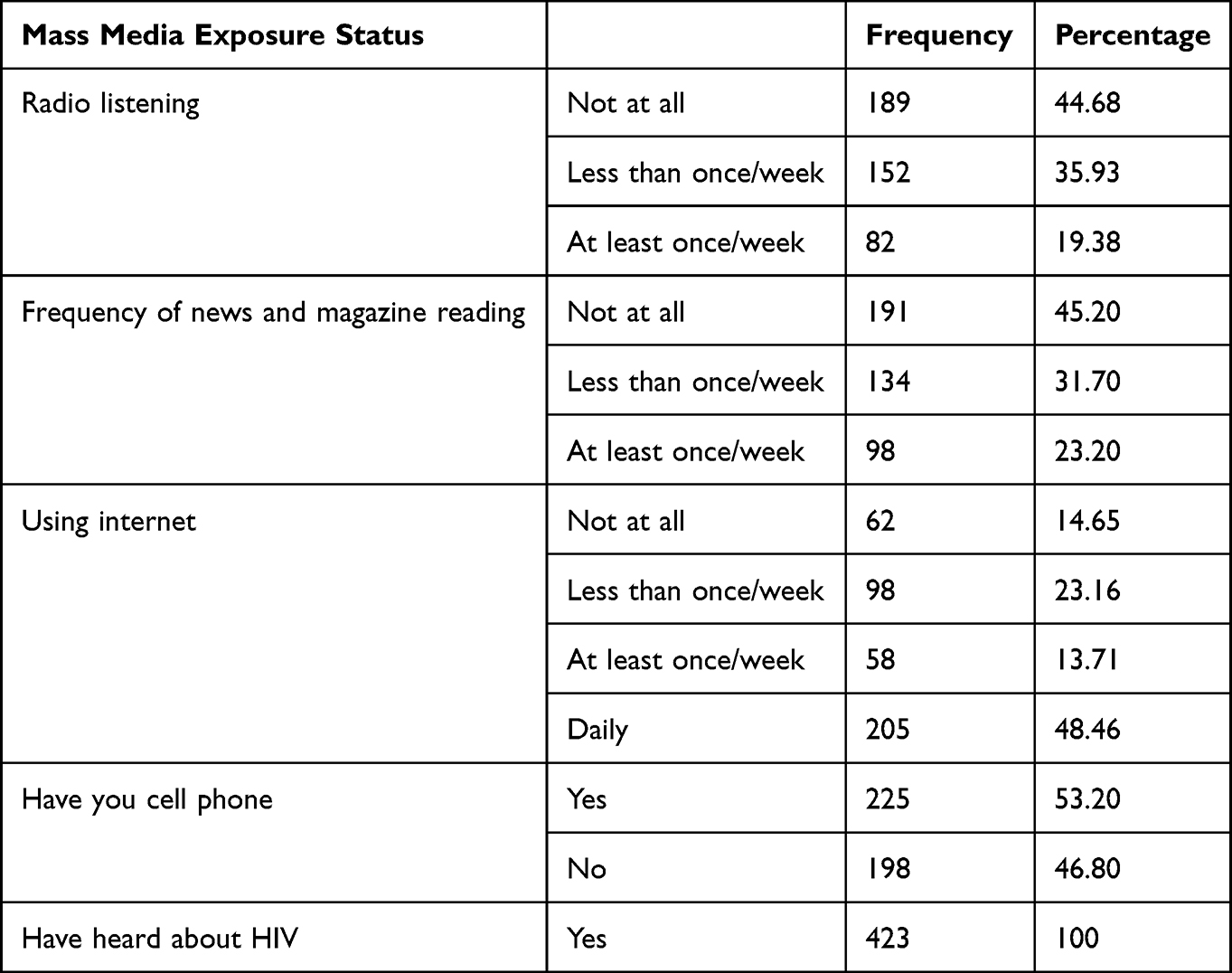 |
Table 2 Assessment of Information About VCT Service in Gondar City Public Health Facilities Northwest Ethiopia, 2022 (n = 423) |
Assessment of Client’s Knowledge and Attitudes About HIV/AIDS
In this study, overall knowledge, favorable attitude, and good behavior of HIV/AIDS were about 258 (61%), 220 (52%), and 210 (49.5%), respectively. Client attitude towards service provider friendly was (41%), knowledge of HIV transmission 46% of respondents were sad about unsafe sex, hesitated to take an HIV test (54%), were realized to not get HIV from contact with saliva from an infected person (58.20%), reduced the risk of getting HIV by having only one sex partner (60.30%), and were ashamed if someone in the family had HIV. Furthermore, about 353 (83.50%) respondents correctly answered no HIV transmission through mosquito bites, 295 (69.70%), and more than 78% of clients had knowledge there was no transmission by sharing food with a person who has AIDS. Almost all clients know that HIV can be transmitted during pregnancy, delivery, and breastfeeding (Table 3).
 |
Table 3 Assessment of Knowledge and Attitude Related Factors at VCT/HTC Service in Gondar City Public Health Facilities Northwest Ethiopia, 2022 (n = 423) |
Factors Associated with Knowledge of HIV/AIDS
Keeping other variables constant, male participants were 39% more likely to be fully knowledgeable than the combined poorly and moderately knowledgeable participants about HIV/AIDS. When all other variables were held constant, as the age of the participants increased from 31 to 35 years (AOR = 2.13, 95% CI, 1.88, 4.18, p-value = 0.001) and above 36 years old (AOR = 2.21, 95% CI, 1.98, 3.44, p-value = 0.001), the odds of being compressively knowledgeable about HIV/AIDS versus poorly and moderately knowledgeable about HIV/AIDS increased by 2.13 and 2.21 times as compared to those participants whose age lies between 18 and 24 years, respectively. Holding the other variable constant, participants who have attained their primary (AOR = 1.21, 95% CI, 1.67, 3.20) and higher education (AOR = 1.19, 95% CI, 1.03, 3.01) educational attainments are 1.21 and 1.19 times higher as compared to non-educated participants, respectively. Holding all other variables constant, participants who have worked as employees are 1.33 (AOR = 1.33, 95% CI: 1.09, 3.37, p-value = 0.0001) more likely to be fully and moderately knowledgeable about HIV/AIDS when compared to participants who are unemployed. For one unit increase in media exposure status (ie, going from 0 to 1), the odds of being fully knowledgeable versus the combined moderately and poorly knowledgeable about HIV/AIDS are 2.02 higher, holding all other variables constant (Table 4).
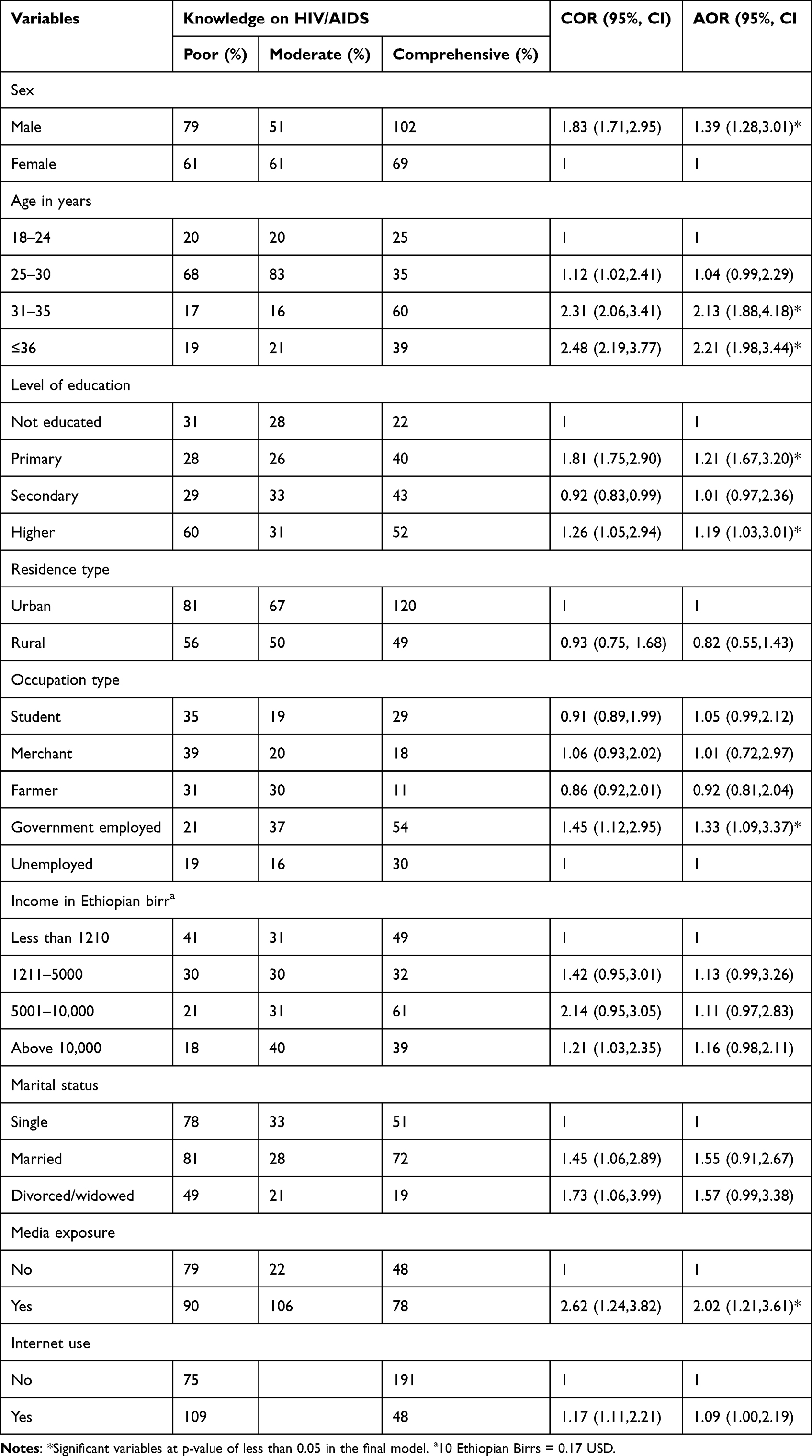 |
Table 4 Factors Associated with Knowledge of HIV/AIDS in Gondar City Public Health Facilities Northwest Ethiopia, 2022 (n = 423) |
Discussion
The aim of this study was to determine the knowledge, attitude, behaviors, and its associated factors using an ordinal logistic regression among VCT service users in Gondar city public health facilities in northwest Ethiopia. In the final model analysis, several factors at health facilities were found to have a significant association with compressive HIV/AIDS knowledge in this study. Males were more likely to be fully knowledgeable than the combined poorly and moderately knowledgeable participants, compared to females, to have a thorough understanding of HIV/AIDS. This finding agrees with several other studies done in several factors at health facilities that were found to have a significant association with compressive HIV/AIDS knowledge in this study. This finding agrees with several other studies done in Ethiopia,26 Sudan,32 Uganda,33 and Nigeria.34 This could be due to cultural mistakes such as accepting male macho while disregarding females, which limits their ability to seek information. Furthermore, it could be explained by social unacceptance of discussions with their friends and family members about sex and sexual concerns, which would further limit their ability to gain conditions.22 Because of deeply ingrained cultural and religious beliefs, women are socialized to have no or poor self-esteem and accept their subservient positions as “God”-given, not subject to change, but arising from their gender. Cultural and religious myths, as well as patriarchal beliefs, cause women to regard themselves as powerless in the absence of men.35–37 Women’s social and economic rights were denied as a result of these socio-cultural conditions. As a result, this provides an opportunity for guys to learn about HIV/AIDS prevention strategies and eliminate previously held misunderstandings.
Holding the other variable constant, participants who have completed their primary (AOR = 1.21,95% CI, 1.67, 3.20) and higher education (AOR = 1.19,95% CI, 1.03, 3.01) educational attainments have 1.21- and 1.19-times higher odds of being fully or comprehensively knowledgeable versus the combined poorly and moderately knowledgeable regarding HIV/AIDS compared to non-educated participants. This finding has been found to be similar to other studies done in Ethiopia,38 Uganda,33 Nigeria,19,34 and Ghana.39 This could be attributed to people becoming more proactive about their own health and seeking knowledge to protect themselves against HIV/AIDS as a result of education. School-based HIV/AIDS interventions can also provide people with HIV/AIDS information. Employment had a good relationship with complete HIV/AIDS knowledge. This finding is reinforced by research from Ethiopia,40 Malawi,41 and Ghana.39 This could be because employed individuals have greater education, living standards, and access to information, education, and communication than illiterate ones.
When all other variables are held constant, the odds of being compressively knowledgeable about HIV/AIDS versus poorly and moderately knowledgeable about HIV/AIDS increase by 2.13 (AOR = 2.13, 95% CI, 1.88, 4.18, p-value = 0.001) and 2.21 (AOR = 2.21, 95% CI, 1.98, 3.44, p-value = 0.001) times as compared to those participants whose age is between 18 and 24 years, respectively. Because of a variety of circumstances, people’s understanding of HIV/AIDS tends to rise as they age. For starters, older people may have had more opportunities to learn about HIV/AIDS through personal and social experiences.42 Second, during the last few decades, HIV/AIDS education has been more widespread, and older individuals have been exposed to a variety of campaigns. Third, due to their experience and learned skills, older people may have a stronger capacity to process and retain new knowledge than their younger counterparts.43,44 Finally, because HIV/AIDS is commonly identified later in life in older persons, the disease may have had more time to do greater harm to the immune system, and the repercussions of this damage may promote increasing interest in and awareness of HIV/AIDS.
Media exposure enhances the likelihood of having full HIV/AIDS information. The odds of having a complete understanding of HIV/AIDS were 2.02 greater among participants who had media exposure compared to their counterparts as we progressed from thoroughly knowing to poorly and moderately knowledgeable persons. This finding is consistent with the findings of a study conducted in Ethiopia,23 Bangladesh,45 and Pakistan.46 This could be because media is an efficient medium for communicating crucial messages regarding this incurable condition in the form of music, news stories, plays, movies, ads, and so on. This could be owing to the media’s significant effect in teaching and imparting accurate knowledge, which dispels pre-existing misconceptions about HIV/AIDS. Therefore, this can have a significant impact on public knowledge of health and health-related concerns, including HIV/AIDS.47
Despite its strengths, there are certain limitations to this study that must be acknowledged. Cross-sectional study designs may fail to demonstrate the cause-and-effect relationship of variables, making the results less credible. The questionnaire was not subjected to exploratory factor analysis. Furthermore, the study is facility-based and quantitative only, with private health facilities excluded.
Conclusion
The study participants’ knowledge, attitudes, and behaviors regarding HIV/AIDS were rather low in this study. Age, educational status, employment status, sex, and media exposure were all associated with low HIV/AIDS knowledge. Our findings highlight the importance of improving the role of policymakers and implementers in gender and young people’s HIV/AIDS awareness programs. This is significant since teaching school-age children about HIV/AIDS and safe sex is one of the most effective means of delaying the initiation of sexual behavior among them. Intervention programs providing sex education have been shown to result in a significant improvement in students’ understanding of HIV/AIDS and a favorable shift in their attitude toward the disease. If the concerned body uses and designs media effectively, encouraging females to attend school, it will have a better chance of combating HIV/AIDS by increasing their knowledge.
Data Sharing Statement
All data concerning this study are accommodated and presented in this document. The detailed data set can be accessible on the correspondence author with reasonable request.
Ethical Considerations and Consent to Participate
The School of Nursing’s ethical review committee and Institutional Review Committee (IRB) provided ethical review on behalf of the University of Gondar College of Medicine and Health Sciences with Ref.SoNCHNU/67/10/22. The healthcare facilities were addressed in a formal permission letter of collaboration. A waiver letter of cooperation was received from hospital administrators (medical directors). The nature of this study did not involve any invasive or biological samples from any participants, however, to meet the ethical consideration, and the consent to participate, each participant received signed informed permission following a brief description of the study’s goals and methods for gathering data. Additionally, participants were made fully aware of their right to deny participation in the study and to withdraw from it. Those participants who could read and write signed in the space provided after confirming their voluntarism. For individuals who could not read or write, however, a fingermark (finger thumb) was taken. Finally, all personal information was removed from the participants’ confidentially. Participants were informed that any information they provided would remain confidential and that their names would not be mentioned. Participants’ identity and privacy were protected, and confidentiality was ensured by removing their names from the informed consent form. The interview was conducted from each participant after they had received services from the VCT service centers to find out how they felt about the services. Participants were informed that any information they provided would remain confidential and that their names would not be mentioned. All the methods and materials in this study have been regulated based on the Declaration of Helsinki.
Acknowledgments
We would like to acknowledge the School of Nursing for providing permission for this study following research ethics.
Author Contributions
All authors have involved in conception, study design, execution, acquisition of data, analysis and interpretation, drafted, revised, and critically reviewed the article, have agreed on the journal to which the article will be submitted. All authors are also realized all versions of the article. Furthermore, authors agreed to take responsibility and be accountable for the contents of the article. The authors approved the final version of the manuscript and agreed on the journal to which the article submitted.
Funding
This study was not supported financially by anyone.
Disclosure
The authors declared that there are no competing interests.
References
1. World Health Organization. The Global Health Observatory Explore a World of Health Data. World Health Organization; 2021.
2. Pandey A, Galvani AP. The global burden of HIV and prospects for control. Lancet HIV. 2019;6(12):e809–e11. doi:10.1016/S2352-3018(19)30230-9
3. Roser M, Ritchie H HIV/AIDS. Our World in Data; 2018.
4. World Health Organization. HIV/AIDS Fact Sheet. Vol. 2021. World Health Organization; 2020.
5. World Health Organization. GLOBAL MONITORING FRAMEWORK and STRATEGY for the Global Plan Towards the Elimination of New HIV Infections Among Children by 2015 and Keeping Their Mothers Alive (EMTCT). Vol. 2012. World Health Organization; 2015.
6. UNAIDS. Global report on the global AIDS epidemic; 2013. Available from: https://www.unaids.org/sites/default/files/media_asset/UNAIDS_Global_Report_2013_en_1.pdf.
7. UNAIDS. Global Report on the global AIDS epidemic Joint United Nation Programme on HIV/AIDS; 2012. Available from: https://www.unaids.org/sites/default/files/media_asset/20121120_UNAIDS_Global_Report_2012_with_annexes_en_1.pdf.
8. Organization WH. HIV and AIDS; 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/hiv-aids.
9. Mude W, Oguoma VM, Gesesew HA, et al. HIV/AIDS knowledge and attitudes assessment among women of child-bearing age in South Sudan: findings from a Household Survey. PLoS One. 2020;15(12):e0243969. doi:10.1371/journal.pone.0243969
10. Teshale AB, Tessema ZT, Alem AZ, et al. Knowledge about mother to child transmission of HIV/AIDS, its prevention and associated factors among reproductive-age women in sub-Saharan Africa: evidence from 33 countries recent demographic and health surveys. PLoS One. 2021;16:6.
11. Darteh EKM, Abraham SA, Seidu -A-A, Chattu VK, Yaya S. Knowledge and determinants of women’s knowledge on vertical transmission of HIV and AIDS in South Africa. AIDS Res Treat. 2021;18(1):1–9. doi:10.1186/s12981-021-00367-7
12. Haile ZT, Teweldeberhan AK, Chertok IR. Correlates of women’s knowledge of mother-to-child transmission of HIV and its prevention in Tanzania: a population-based study. AIDS Care. 2016;28(1):70–78. doi:10.1080/09540121.2015.1062465
13. Luba TR, Feng Z, Gebremedhin SA, et al. Knowledge about mother–to–child transmission of HIV, its prevention and associated factors among Ethiopian women. J Glob Health. 2017;7(2). doi:10.7189/jogh.07.020414
14. Okoko NA, Owuor KO, Kulzer JL, et al. Factors associated with mother to child transmission of HIV despite overall low transmission rates in HIV-exposed infants in rural Kenya. Int J STD AIDS. 2017;28(12):1215–1223. doi:10.1177/0956462417693735
15. Office FHAPa C. HIV Prevention in Ethiopia National Road Map 2018 –2020; 2018. Available from: https://ethiopia.unfpa.org/sites/default/files/pub-pdf/HIV%20Prevention%20in%20Ethiopia%20National%20Road%20Map%202018%20-%202020%20FINAL_FINAL.pdf.
16. Federal HIV/AIDS Prevention and Control Office Addis Ababa E. HIV/AIDS Strategic Plan 2015–2020 In An Investment Case Approach; 2014. Available from: https://www.childrenandaids.org/sites/default/files/2018-05/Ethiopia_Nat%20Strat%20Plan%20HIV_2015-2020.pdf.
17. Fagbamigbe A, Lawal A, Idemudia E. Modelling self-assessed vulnerability to HIV and its associated factors in a HIV-burdened country. SAHARA-J. 2017;14(1):140–152. doi:10.1080/17290376.2017.1387598
18. Bamise O, Bamise C, Adedigba M. Knowledge of HIV/AIDS among secondary school adolescents in Osun state, Nigeria. Niger J Clin Pract. 2011;14(3):338–344. doi:10.4103/1119-3077.86780
19. Obidoa CA, M’Lan CE, Schensul SL. Factors associated with HIV/AIDS sexual risk among young women aged 15–24 years in Nigeria. J Public Health Afr. 2012;3(1):15. doi:10.4081/jphia.2012.e15
20. Csa I. Central Statistical Agency (CSA)[Ethiopia] and ICF. Ethiopia and Calverton, Maryland, USA: Ethiopia demographic and health survey, Addis Ababa; 2016:1.
21. Ababa A, Calverton E. Central statistical agency (Ethiopia) and ICF international. Ethiopia and Calverton. 2011;2011:14.
22. Ethiopia F. National guidelines for comprehensive HIV prevention, care and treatment. AAMo Health. 2017;2:1.
23. Kefale B, Damtie Y, Yalew M, Adane B, Arefaynie M. Predictors of comprehensive knowledge of HIV/AIDS among people aged 15–49 years in Ethiopia: a multilevel analysis. HIV/AIDS-Res Palliative Care. 2020;12:449–456. doi:10.2147/HIV.S266539
24. Demographic E. Health Survey: Addis Ababa. Vol. 2011. Ethiopia and Calverton, Maryland, USA: Central statistics agency and ORC macro; 2011.
25. Baart J, Taaka F. Barriers to healthcare services for people with disabilities in developing countries: a literature review. Disabil CBR Inclus Devel. 2017;28(4):26–40. doi:10.5463/dcid.v28i4.656
26. Oljira L, Berhane Y, Worku A. Assessment of comprehensive HIV/AIDS knowledge level among in‐school adolescents in eastern Ethiopia. J Int AIDS Soc. 2013;16(1):17349. doi:10.7448/IAS.16.1.17349
27. Gemeda TT, Gandile AU, Bikamo DS. HIV/AIDS knowledge, attitude and practice among Dilla University Students, Ethiopia. Afr J Reprod Health. 2017;21(3):49–61. doi:10.29063/ajrh2017/v21i3.4
28. McCullagh P. Regression models for ordinal data. J R Stat Soc. 1980;42(2):109–127.
29. Cox C, Chuang C. A comparison of chi‐square partitioning and two logit analyses of ordinal pain data from a pharmaceutical study. Stat Med. 1984;3(3):273–285. doi:10.1002/sim.4780030309
30. Long JS, Freese J. Regression Models for Categorical Dependent Variables Using. Stata: Stata press; 2006.
31. Ananth CV, Kleinbaum DG. Regression models for ordinal responses: a review of methods and applications. Int J Epidemiol. 1997;26(6):1323–1333. doi:10.1093/ije/26.6.1323
32. Elbadawi A, Mirghani H. Assessment of HIV/AIDS comprehensive correct knowledge among Sudanese university: a cross-sectional analytic study 2014. Pan Afr Med J. 2016;24(1). doi:10.11604/pamj.2016.24.48.8684
33. Ciccio L, Sera D. Assessing the knowledge and behavior towards HIV/AIDS among youth in Northern Uganda: a cross-sectional survey. Giornale Italiano di Medicina Tropicale. 2010;15(1/4):29–34.
34. Oginni AB, Adebajo SB, Ahonsi BA. Trends and determinants of comprehensive knowledge of HIV among adolescents and young adults in Nigeria: 2003–2013. Afr J Reprod Health. 2017;21(1):26–34. doi:10.29063/ajrh2017/v21i2.4
35. U. BSaS. Gender Equality And HIV/AIDS Comprehensive Web Portal for Gender Equality Dimensions of the HIV/AIDS Epidemic. International Council of AIDS Service Organizations (ICASO); 2007. Available from: https://www.hivlawandpolicy.org/sites/www.hivlawandpolicy.org/files/genderreport_web_080331.pdf.
36. Prah M. Insights into Gender Equity, Equality and Power Relations in Sub-Saharan. Africa: African Books Collective; 2013.
37. Luhamaa K The Domestic limitations to the Implementation of CEDAW to Combat Violence Against Women in Nigeria. 2020.
38. Megabiaw B, Awoke T. Comprehensive knowledge, attitude and practice of street adults towards human immunodeficiency virus/acquired immune deficiency syndrome (HIV/AIDS) in Northwest Ethiopia. J AIDS HIV Res. 2013;5(6):181–187.
39. Fenny AP, Crentsil AO, Asuman D. Determinants and distribution of comprehensive HIV/AIDS knowledge in Ghana. Glob J Health Sci. 2017;9(12):32. doi:10.5539/gjhs.v9n12p32
40. Kassie GM, Mariam DH, Tsui AO. Patterns of knowledge and condom use among population groups: results from the 2005 Ethiopian behavioral surveillance surveys on HIV. BMC Public Health. 2008;8(1):1–14. doi:10.1186/1471-2458-8-429
41. Barden-O’Fallon JL, deGraft-Johnson J, Bisika T, Sulzbach S, Benson A, Tsui AO. Factors associated with HIV/AIDS knowledge and risk perception in rural Malawi. AIDS & Behav. 2004;8(2):131–140. doi:10.1023/B:AIBE.0000030244.92791.63
42. Davis TE, Elder MA. HIV knowledge and preferences for HIV prevention among older adults living in the community. Gerontol Geriatr Med. 2020;6:2333721420927948. doi:10.1177/2333721420927948
43. HIVinfo.NIH.gov. HIV and Specific Populations, HIV and Older People; 2021. Available from: https://hivinfo.nih.gov/understanding-hiv/fact-sheets/hiv-and-older-people.
44. Fana T. Knowledge, attitude and practices regarding HIV and AIDS among high school learners in South Africa. Open AIDS J. 2021;15(1):84–92. doi:10.2174/1874613602115010084
45. Dey R, Hassan M, Hossain M. Prevalence of comprehensive knowledge about HIV/AIDS among ever married men and women in Bangladesh. J Sci Technol. 2013;11:91–99.
46. Iqbal S, Maqsood S, Zafar A, Zakar R, Zakar MZ, Fischer F. Determinants of overall knowledge of and attitudes towards HIV/AIDS transmission among ever-married women in Pakistan: evidence from the demographic and health survey 2012–13. BMC Public Health. 2019;19(1):1–14. doi:10.1186/s12889-019-7124-3
47. Sood S, Shefner-Rogers CL, Sengupta M. The impact of a mass media campaign on HIV/AIDS knowledge and behavior change in North India: results from a longitudinal study. Asian J Commun. 2006;16(3):231–250. doi:10.1080/01292980600857740
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.