")
Back to Journals » Research and Reports in Urology » Volume 15
Comparative Study of Prone Position Variations for Percutaneous Nephrolithotomy
Received 26 April 2023
Accepted for publication 5 June 2023
Published 23 June 2023 Volume 2023:15 Pages 233—241
DOI https://doi.org/10.2147/RRU.S415426
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Guglielmo Mantica
Mehmet Yilmaz, Yusuf Sahin
Department of Urology, University of Health Sciences Bağcılar Training and Research Hospital, Istanbul, Turkey
Correspondence: Mehmet Yilmaz, Email [email protected]
Objective: In this comparative study, we evaluated the results of flat prone and prone hip flexed percutaneous nephrolithotomy in terms of efficacy and safety to contribute to the optimal prone percutaneous nephrolithotomy position.
Materials and Methods: Data of the patients who underwent percutaneous nephrolithotomy operations in a flat-prone or prone hip flexed positions due to renal pelvis and/or ≥ 2 Calix filling stones between January 2016 and January 2022 were collected retrospectively. Demographic data of the patient groups in different prone positions as well as clinical findings, stone characteristics and operative data were analyzed. The groups were also compared in terms of post-operative findings and complications.
Results: The average age and CROES scores of patients included in the study were 47.15± 15.6 years and 221.76± 62.49, respectively. There was no statistically significant difference between the two groups in terms of patient demographic data, stone-free status and complication rates. Operation Room Time (ORT) (min) in flat prone PCNL group was shorter in average (100.57± 32.74 min vs 92.32± 28.75 min, p = 0.041) and duration with nephrostomy (days) and hospitalization (days) parameters were statistically significantly shorter in prone hip flexed PCNL (respectively, p < 0.001; p = 0.005).
Conclusion: Flat-prone PCNL provides significantly shorter ORT. However, the time with nephrostomy and hospitalization with the prone hip flexed PCNL were shorter than flat-prone position. The findings will guide the optimal prone PCNL position.
Keywords: flat prone position, hip flexed prone position, kidney stone, percutaneous nephrolithotomy
Introduction
Percutaneous nephrolithotomy (PCNL) is still a procedure of choice with its ability to provide standard or miniaturized access tracts in different diameters in addition to rigid and flexible endoscopic options for large kidney stones (>20 mm).1
PCNL operation is performed in the well-known prone position as defined originally today, while the supine position and its modifications have gained popularity due to its positional, anesthetic and retrograde access comfort despite its lower stone-free rates.2,3 In studies comparing these two positions, the parameters of higher stone-free status (SFS), wider renal anatomy, easy access, and the risk of lesser adjacent organ injury are in favor of the prone position, while other operative parameters (operation time, hospitalization, anesthesia comfort) are in favor of supine position.4,5 Because of the conflicting results of the studies for these two positions, it seems impossible to mention an optimal position.
Although the concept of indication has been determined with certain limits, developments in instrument diameters, energy and optic diversity enable smaller stones to receive PNL indication, while it seems essential to consider positional modifications as well as these developments in order to obtain maximum benefit from PNL in the management of larger and complicated stones.6
Positional modifications in both prone and supine PCNL, and improvements in endoscopic technology explain the limited and uncertain level of evidence in the comparison between these two positions.7,8 Thus, comparisons to be made between these two positions in terms of their own modifications will guide the determination of the most ideal method. However, studies on the prone position modifications in the literature are limited to comparisons in terms of probable ease of access and adjacent organ injury with related radiological findings and case series, and there is neither enough comparison study on operative parameters nor sufficient evidence.9,10 Similarly, other than case series, case reports, technical descriptions and illustrates on supine PCNL modifications in the literature, we did not find any comparative studies on other supine PCNL modifications.11–13
As a tertiary center with a high stone case volume, in our clinic, PCNL operations are performed with the conventional method in positions with flat prone or variations. In this study, we aimed to compare demographic, operative and complication data of patients who underwent PCNL in flat prone (FP) and prone hip flexed (PHF) positions.
Materials and Methods
This study protocol was reviewed and approved by Biruni University Non-Invasive Clinical Research Ethics Committee, approval number 2022/70-21. In our study with human participants, ethical standards of the 1964 Helsinki Declaration were complied with, as well as the ethical standards of the national research association at the procedural stages. We obtained informed consent from patients included in the study. Data of the patients between 18 and 80 years of age who underwent PCNL for stones in the renal pelvis and/or ≥2 calix filling stones in our clinic between January 2019 and July 2022 were collected retrospectively and analyzed. Of 497 patients who underwent PCNL operations, 39 patients were excluded due to patient factors (bleeding diathesis, malformed and malrotated kidney, and multiple comorbidities), 67 due to procedural factors (mini PCNL and supine PCNL) and 113 due to data factors (lack of laboratory or radiological data). The remaining 278 patients were divided into two groups as the FP-PCNL (164 patients) and the PHF-PCNL (114 patients). All cases in our clinic were operated by endourologists (YS-MY) without considering any randomization and case-specific position. These two endourologists performed stone surgery in their daily practice and had similar case volumes. First room’s table had a table modification according to the prone hip flexed position, while second ones allowed only flat position. Although the general orientation in our clinic is the flat prone PNL position, the PHF position was used to get comparation regardless of the location of the kidney stone and the physical characteristics of the patient. The number of cases in these rooms by both surgeons was close to each other.
Every patient was evaluated in terms of suitability for operation with laboratory and radiological examinations before procedures. One week at most before any procedure, hematological evaluation with whole blood count and coagulation factors, biochemical-microbiological evaluation with renal and hepatic function tests and urinary analysis – urine culture, and radiological evaluation with low dose non-contrast computerized tomography (NCCT) and/or urography (only in complex cases) were performed. The most suitable percutaneous entry points were predicted with NCCT which helps to determine stone dimensions (by multiplying the two longest dimensions, as mm2), stone density (Hounsfield Unit), skin-to-stone distance (mm), stone location, adjacent organ evaluation in addition to estimated kidney calix anatomy.
Both PCNL procedures were performed under general anesthesia and single dose antibiotic prophylaxis. Procedures initiated with the retrograde placement of 5F Both-End-Open Hydrophilic Ureteral Catheters (Plasti-med) into the kidney and continued in the prone position (Figure 1). For the PHF PCNL, patient was taken into 30° hip and 15° knee flexions different from the FP position (Figure 2). For both positions, posterior calix access (upper, medium or lower according to stone statement and burden) was provided by delivering retrograde contrast under fluoroscopy guidance with an initial puncture needle (18G/20mm/2 parts, plasti-med). Following the application of amplatz dilator until 12 French (F), renal access was performed by entering with nephrostomy balloon dilator (nephroflex) and 24F nephroscope (ALKEN-HOHENFELLNER, Karl Storz, Germany) within 30 F amplatz cover. Stone fragmentation was performed with pneumatic and ultrasonic lithotripters. After reaching SFS endoscopically and fluoroscopically, 14 F malecot nephrostomy set was placed in the kidney. On the postoperative 1st day, both SFS and pleural injury control were performed with kidney-urine-bladder radiography (KUB) and chest radiography. When the content of the nephrostomy tube was completely clear urine colour, the tube was clamped and pulled out when there was no pain or wetting. The patient was discharged according to the presence of tractus dryness after the removal of the nephrostomy catheter. The first control of the urinary system was provided with KUB and urinary USG in postoperative 1st month, while SFS control was actualized with low dose NCCT at third month postoperatively.
 |
Figure 1 Flat prone PCNL position. |
 |
Figure 2 Prone hip flexed PCNL position. |
The groups were compared according to demographic data (age, gender, ASA score, previous procedure status), stone characteristics (stone location, size, density, SSD and stone scores), operative data (ORT, intercostal access between 11 and 12 ribs, transfusion status and complications) and postoperative results (duration of hospitalization, decrease in hemoglobin, transfusion status, duration with nephrostomy, SFS, and complications). ORT is the time elapsed between insertion of the ureteral catheter and returning the patient to the supine position at the end of the operation (excluding the duration of anesthesia), duration of hospitalization is the duration between performance of the procedure and removal of nephrostomy catheter and uncomplicated discharge of the patient. The absence of >3 mm residual fragment is taken as a basis for the SFS.14 The modified Clavien-Dindo system was used for postoperative complications.
Statistical Analyses
Statistics Standard Grad Pack Student v29 (IBM SPSS 29.0.0.0) was used to analyze the data. Since the data were not normally distributed, the analysis was continued with non-parametric tests. Mean±SD was used to present continuous independent variables. Differences between the two groups were compared with the Mann–Whitney U-test. Categorical data were evaluated by Chi-square and Fisher exact tests. A value of p ≤ 0.05 was considered statistically significant.
Results
Of the patients included in the study, 109 were female and 169 were male and the average age was 47.15±15.6 years. While the kidney side that was the object of the operation was right in 153 and left in 125, average stone size, skin-to-stone distance and stone density were 596.53±493 mm2; 87.35±22 mm and 955.14±310.84 HU, respectively. The median ASA and Guy Stone scores were 1 (1–4) and 2 (1–4), respectively, while the average Croes score was 221.76±62.49. There was no statistically significant difference between the FP and the PHF-PCNL groups in terms of demographic parameters. The demographic characteristics of the groups are summarized in Table 1.
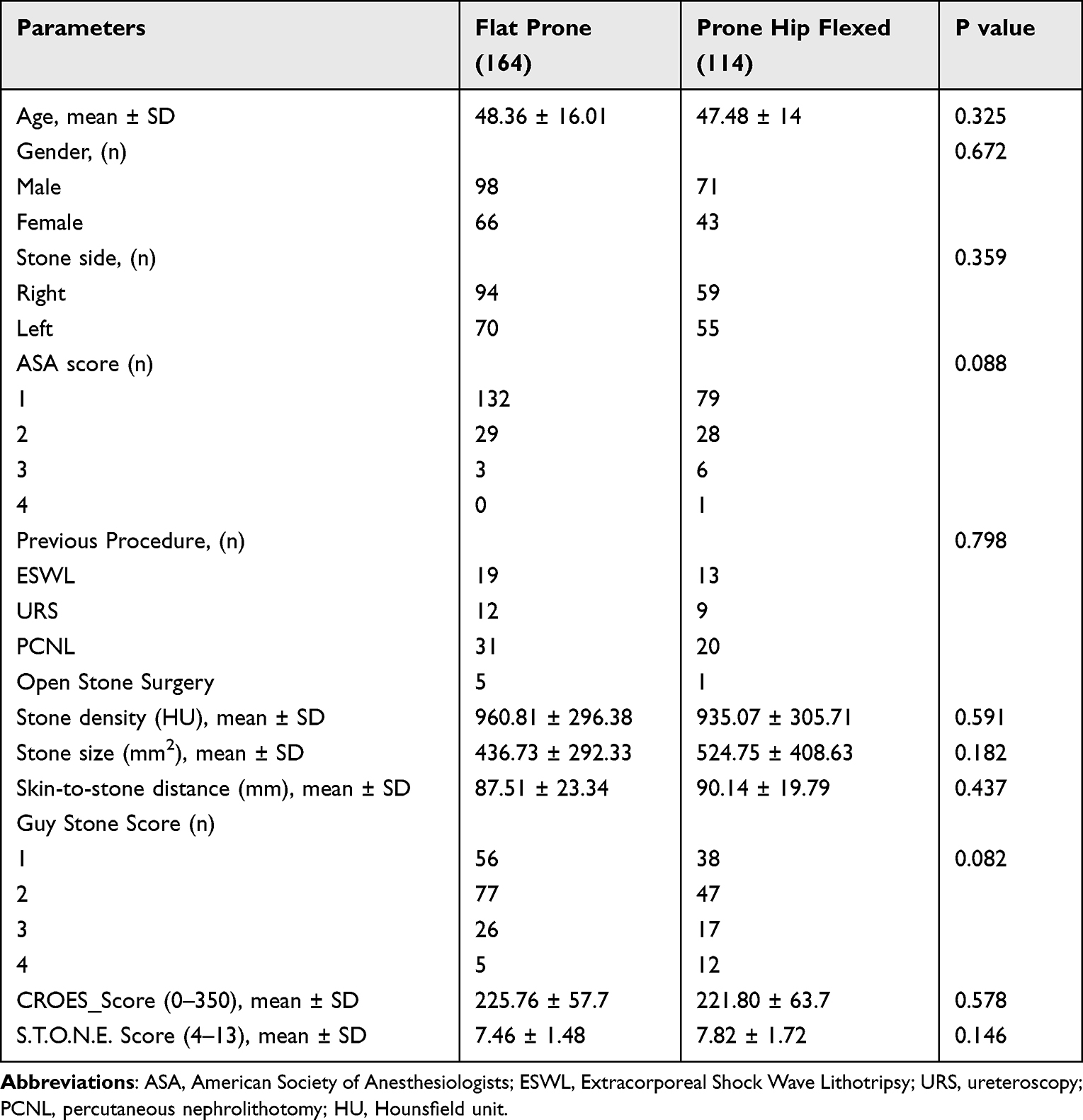 |
Table 1 Patients’ Demographics |
The overall stone free rate in our cohort was 75.4% (n = 208), while the complete stone free rate was 78.9% in the PHF-PCNL group and 72.8% in the FP-PCNL group (p = 0.246). First and 3rd month rates of residual stone were similar (p = 0.522). In both groups, the need for intercostal access was similar (p = 0.983). Although the magnitude of decrease in hemoglobin (2.11 ± 1.14 vs 2.02 ± 1.08) and the rate of need for transfusion (8.53% vs 3.5%) were high in the FP-PCNL group, there was no statistically significant difference between groups (p = 0.489 and 0.074, respectively). Average ORT was statistically longer in the PHF-PCNL group than the other group (100.57±32.74 min vs 92.32±28.75 min, p = 0.041). Both duration with nephrostomy (days) and duration of hospitalization (days) parameters were significantly longer in the FP-PCNL than in the PHF-PCNL group (2.46±1.83 vs 1.79±1.83, p < 0.001; 2.65±1.24 vs 2.62±2.41, p = 0.005, respectively). The comparison of operative parameters between groups is summarized in Table 2.
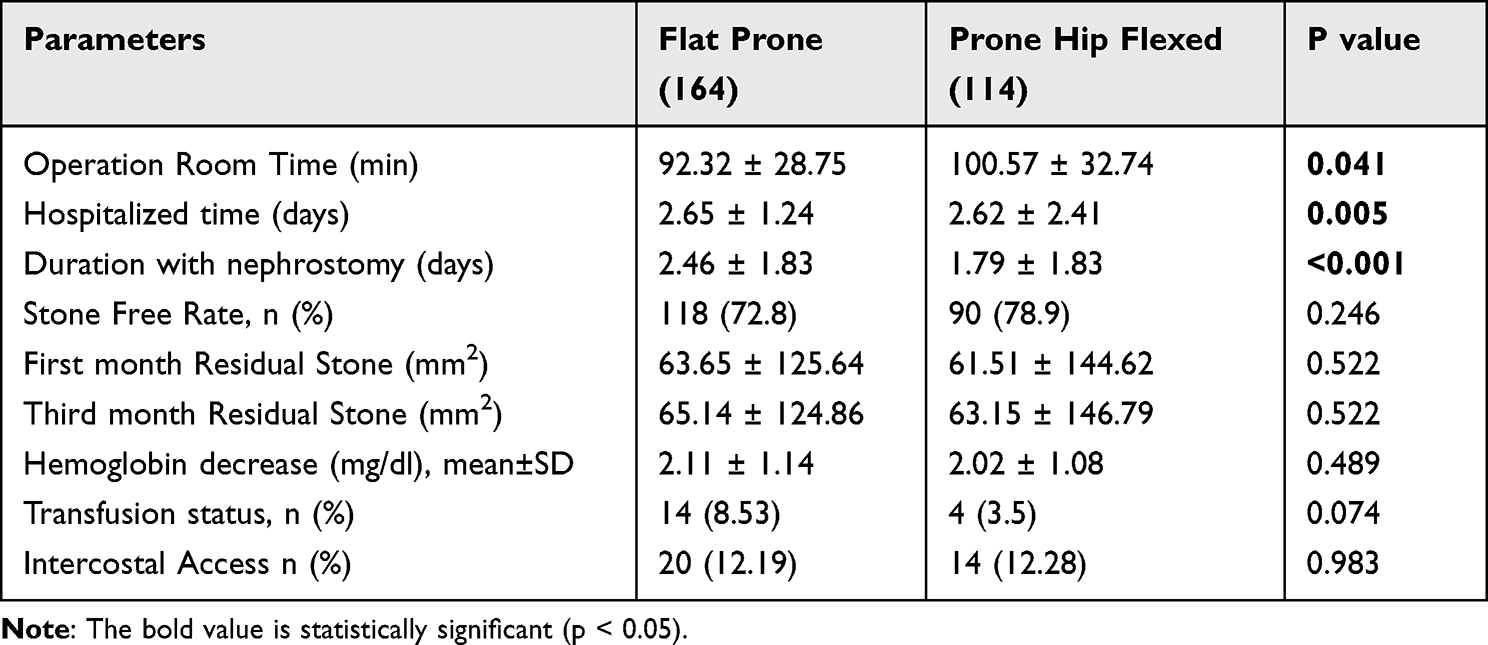 |
Table 2 Groups Characteristics and Operative Data |
Postoperative complications were classified by Clavien-Dindo, but there was no statistically significant difference between groups in terms of complications (p = 0.749). The rate of uncomplicated cases in the FP-PCNL group was 73.2% and 71.9% in the PHF-PCNL group. The predominant part of the complications seen in both groups were reported as Clavien grade 1 complications [n = 12 (7.3%) in the FP-PCNL and n = 10 in the PHF-PCNL (8.8%)], 1 Clavien Grade 5 complication (mortality) in the FP-PCNL group and 1 Clavien Grade 4 complication (Nephrectomy) in the PHF-PCNL group. In total, urine leakage requiring Double-J stent placement was detected in 7, pneumothorax in 2, urinoma in 1 and bleeding requiring angioembolization in 3 patients. Postoperative complications and outcomes are summarized in Table 3.
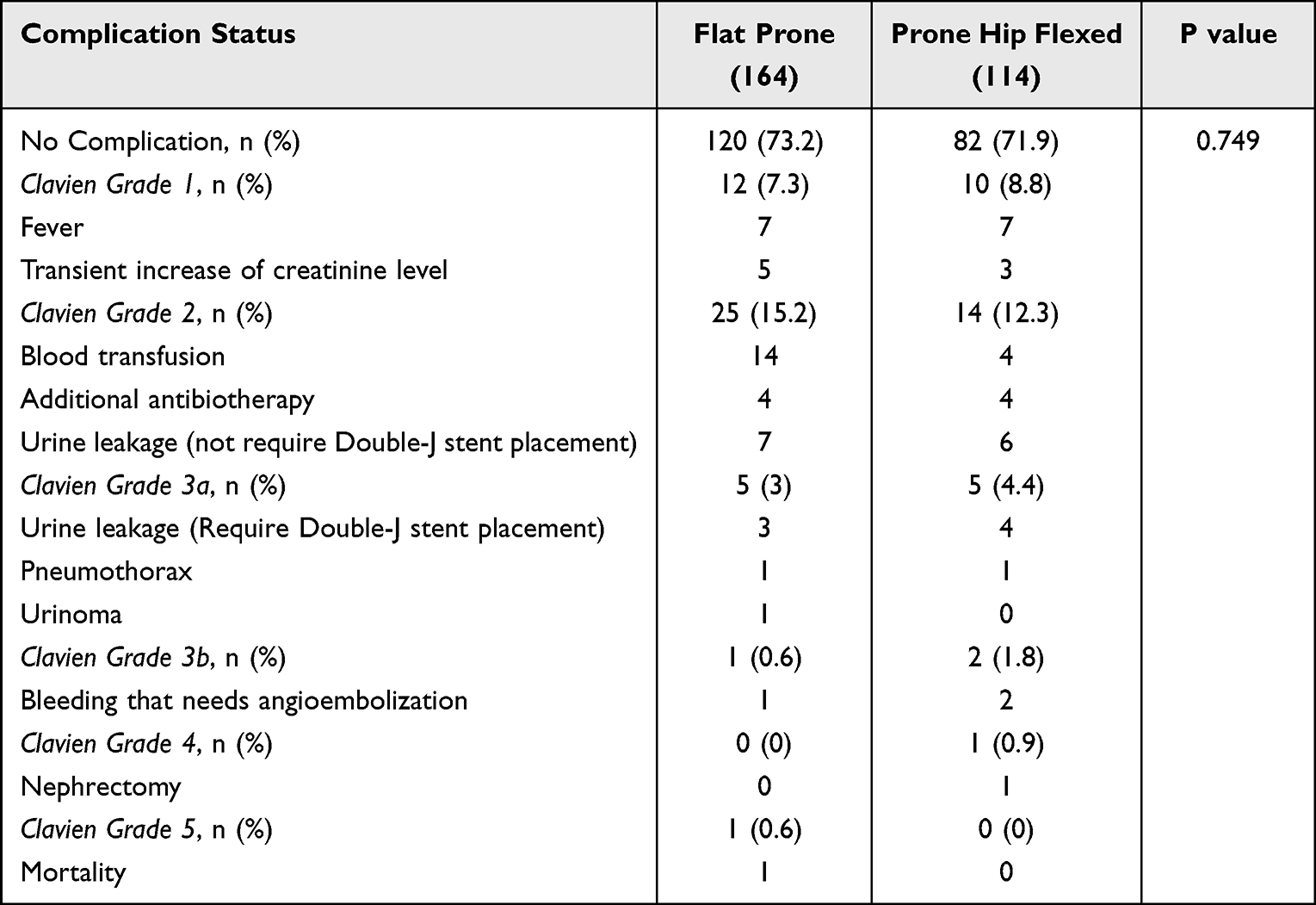 |
Table 3 Complication of Groups |
Discussion
Today, percutaneous stone surgery is performed preferably in a prone position due to its advantages like ease of renal access, wider work area, minimal complication and high stone-free rates despite its anesthetic and positional unfavorable aspects.5,15 In addition to improvement in endoscopic instruments, positional modifications also play an important role in the procedure to provide lower complication and higher stone-free rates.8 In the literature, positional comparative studies are mainly on supine-prone, and despite conflicting SFS rates reported in meta-analyses, emphasis has been placed on short operation times provided by supine position.5,15–17 In the studies reviewed in the above-mentioned meta-analyses, the FP position was mainly used in prone PCNL while using different modified positions characteristically in supine PCNL explains different SFS rates. A similar situation could also explain shorter operation time in favor of supine PCNL. To our knowledge, this is the first comparative study on PCNL in flat and modified prone positions. With this study, there was no statistical difference between the PHF and the FP positions in terms of SFS and complications, while the PHF was advantageous in terms of nephrostomy and hospitalization times and disadvantageous in terms of operation time. Although there was no statistical difference in this study, the advantage in terms of SFS and postoperative residual stone parameters was observed in the PHF group. It was determined that our PHF SFR was close to prone SFR according to the SFR of supine versus prone meta-analyses.5,15
Well-defined positional modifications in supine PCNL are the result of the efforts to improve inferior operative parameters obtained with prone PCNL defined 10 years ago and to perform simultaneous retrograde intrarenal surgery.18 With the prone PCNL standard method, there is less need for modified positions thanks to a wider work area, easy access and prevailing pelvicalyceal anatomy, while prone modifications defined in the literature are the products of simultaneous endoscopic study efforts.9,19–21 However, the advantages such as easier access to the kidney upper pole and higher mobility of the lower pole with prone flexion modification at the expense of anesthetic difficulties are a matter of debate.22,23
Ray et al found that prone-flexed position increases the distance between the posterior iliac crest and 12th costa and that subcostal access would be sufficient instead of the intercostal access in 45.5% of the patients. They suggested that the supine position increases the risk of solid organ injury in upper pole access while the prone or prone-flexed position increases the risk of colon injury in lower pole access in the section of anatomical effects of patient positioning according to CT in their study. They also suggested that lower pole access difficulty due to hip spur could be overcome with prone flexion.10 Sign et al in their study in which they obtained a similar modification by using a horizontal bolster to prone flexed position also emphasized that the kidney upper pole is displaced toward the caudal and ease of upper pole access could be increased with lesser supracostal access. They also emphasized that, by displacement of kidney lower pole toward posterior with vertical bolster, skin-calix distance is decreased, and favorable position for access to middle and lower calyces could be found.23 In our study, we did not find any difference between groups in terms of the need for intercostal access and common secondary pleural complications. Additionally, we did not detect solid organ or colon injury in any of our cases. However, we concluded that statistically insignificant hemoglobin decrease and transfusion need and statistically significant shorter nephrostomy time in the PHF-PCNL group might be the result of wider work area and lesser rigid instrument rotation injury. In addition, whether positional and anesthetic advantages with the use of vertical and horizontal bolster could be obtained with vertical bolster and the PHF-PCNL combination could be a new research topic.
The increased risk of thoracic complications is generally associated with the need for upper pole access and characteristically upper-level intercostal access dependent on the closeness of the diaphragm to the upper pole rather than positional choice.24,25 Chow et al emphasized that the rate of thoracic complication increases as the distance of the diaphragm to the kidney’s upper pole decreases in posterior supracostal access.25 We did not find any study in the literature comparing standard prone position and flexion modifications in terms of thoracic complications. In our study, we did not find any significant difference between groups. However, it was a limitation of our study that the distance between the diaphragm and kidney upper pole and which intercostal interval was used were not mentioned. As Ray et al mentioned, the risk of thoracic complication decreases with the decreased need for supracostal access in the PHF position.10
In the literature, although the main topics in supine-prone PCNL comparison studies are SFS, operation time and complication rates, similar or higher SFS in prone PCNL and similar or lower complication rates and shorter operation times in supine PCNL came to the fore in those meta-analyses.2,5,15,17 In these meta-analyses, there was no significant difference between the two groups in terms of hospitalization time. Considering the heterogenous character of the studies, our FP-PCNL hospitalization value (mean: 2.65 days) was consistent with the studies in the literature that reported shorter hospitalization.26–28 The other original aspect of our study is that it is the first study in which two groups were compared in terms of hospitalization, duration with nephrostomy, and ORT and that the first two parameters were significant in favor of the PHF-PCNL. The only parameter that was significantly observed in favor of the FP-PCNL was operation time. We concluded that prolonged operation time with the PHF-PCNL is due to positional arrangement. Shorter nephrostomy time is correlated with shorter hospitalization, and this might provide lesser renal injury and bleeding due to lesser rigid nephroscope manipulation thanks to shorter access distance and wide calyceal work area in the PHF position.29
Although data of our study were collected retrospectively, our study is an original study since it is the first study that compares values of demographic and operative parameters obtained with stone scoring and Clavien complication classification between PCNL case groups performed in the FP and the PHF positions by two urologists who are interested only in endourology in the tertiary hospital urology clinic. In addition, the imaging method performed in the 3rd month provides an important standardization for the evaluation of SFS and late complications.
The most important limitation of our study is that due to the retrospective nature of the available data, some essential clinical data such as “diaphragm-kidney upper pole distance, interval of intercostal access, number of tracts, fluoroscopy time and anesthesiological outcomes” were not included in the comparison. Additionally, the fact that patients were not randomized into different positions might affect the surgeon’s bias to prefer a position according to its relation to stone scores.
Conclusion
The findings of our retrospective study comparing the two prone positions demonstrate that the PHF position appears superior to the FP position with reduced nephrostomy time and short hospitalization at the cost of prolonged operation time. However, there was no significant difference between both prone positions in terms of SFS and complication rates. Although not statistically significant, a lower transfusion rate was observed in favor of the PHF-PCNL. However, multicenter double-blind randomized controlled studies are needed for positional preference standardization.
Data Sharing Statement
Although the data of the study are not available to the public due to privacy or ethical restrictions, it can be obtained from the corresponding author if requested.
Statement of Ethics
In our study with human participants, ethical standards of the 1964 Helsinki Declaration were complied with, as well as the ethical standards of the national research association at the procedural stages. We obtained informed consent from patients included in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. EAU Guidelines. Presented at the EAU Annual Congress Amsterdam; 2022. ISBN 978-94-92671-16-5.
2. Birowo P, Tendi W, Widyahening IS, Rasyid N, Atmoko W. Supine versus prone position in percutaneous nephrolithotomy: a systematic review and meta-analysis. F1000Res. 2020;9:231. PMID: 33014345; PMCID: PMC7509599. doi:10.12688/f1000research.22940.3
3. Gökce Mİ, Ibiş A, Sancı A, et al. Comparison of supine and prone positions for percutaneous nephrolithotomy in treatment of staghorn stones. Urolithiasis. 2017;45(6):603–608. doi:10.1007/s00240-017-0977-y
4. Astroza G, Lipkin M, Neisius A, et al. Effect of supine vs prone position on outcomes of percutaneous nephrolithotomy in staghorn calculi: results from the clinical research office of the endourology society study. Urology. 2013;82(6):1240–1244. PubMed PMID: 24063939. doi:10.1016/j.urology.2013.06.068
5. Yuan D, Liu Y, Rao H, et al. Supine versus prone position in percutaneous nephrolithotomy for kidney calculi: a meta-analysis. J Endourol. 2016;30(7):754–763. PubMed PMID: 27072075. doi:10.1089/end.2015.0402
6. Ganpule AP, Vijayakumar M, Malpani A, Desai MR. Percutaneous nephrolithotomy (PCNL) a critical review. Int J Surg. 2016;36(Pt D):660–664. doi:10.1016/j.ijsu.2016.11.028
7. Karaolides T, Moraitis K, Bach C, et al. Positions for percutaneous nephrolithotomy: thirty-five years of evolution. Arab J Urol. 2012;10(3):307–316. doi:10.1016/j.aju.2012.06.005
8. Zhao Z, Fan J, Liu Y, de la Rosette J, Zeng G. Percutaneous nephrolithotomy: position, position, position! Urolithiasis. 2018;46(1):79–86. doi:10.1007/s00240-017-1019-5
9. Lehman T, Bagley DH. Reverse lithotomy: modified prone position for simultaneous nephroscopic and ureteroscopic procedures in women. Urology. 1988;32(6):529–531. doi:10.1016/S0090-4295(98)90035-8
10. Ray AA, Chung D-G, Honey RJD. Percutaneous nephrolithotomy in the prone and prone-flexed positions: anatomic considerations. J Endourol. 2009;23(10):1607–1614. doi:10.1089/end.2009.0294
11. Papatsoris AG, Zaman F, Panah A, et al. Simultaneous anterograde and retrograde endourologic access: “the Barts technique”. J Endourol. 2008;22(12):2665–2666. doi:10.1089/end.2008.0283
12. Bach C, Goyal A, Kumar P, et al. The Barts “flank-free” modified supine position for percutaneous nephrolithotomy. Urol Int. 2012;89:365–368. doi:10.1159/000341430
13. Vicentini FC, Torricelli FCM, Mazzucchi E, et al. Modified complete supine percutaneous nephrolithotomy: solving some problems. J Endourol. 2013;27:845–849. doi:10.1089/end.2012.0725
14. Biswas K, Gupta SK, Tak GR, Ganpule AP, Sabnis RB, Desai MR. Comparison of STONE score, Guy’s stone score and Clinical Research Office of the Endourological Society (CROES) score as predictive tools for percutaneous nephrolithotomy outcome: a prospective study. BJU Int. 2020;126(4):494–501. doi:10.1111/bju.15130
15. Zhang X, Xia L, Xu T, et al. Is the supine position superior to the prone position for percutaneous nephrolithotomy (PCNL)? Urolithiasis. 2014;42(1):87 93. doi:10.1007/s00240-013-0614-3
16. Liu L, Zheng S, Xu Y. Systematic review and meta analysis of percutaneous nephrolithotomy for patients in the supine versus prone position. J Endourol. 2010;24(12):1941. doi:10.1089/end.2010.0292
17. Wu P, Wang L, Wang K. Supine versus prone position in percutaneous nephrolithotomy for kidney calculi: a meta-analysis. Int Urol Nephrol. 2011;43(1):67–77. PMID: 20628815. doi:10.1007/s11255-010-9801-0
18. Miçooğulları U, Kamacı D, Yıldızhan M, et al. Prone versus Barts “flank-free” modified supine percutaneous nephrolithotomy: a match-pair analysis. Turk J Med Sci. 2021;51(3):1373–1379. doi:10.3906/sag-2011-21.end.2006.0401
19. Grasso M, Nord R, Bagley DH. Prone split leg and flank roll positioning: simultaneous antegrade and retrograde access to the upper urinary tract. J Endourol. 1993;7:307–310. doi:10.1089/end.1993.7.307
20. Hamamoto S, Yasui T, Okada A, et al. Developments in the technique of endoscopic combined intrarenal surgery in the prone split-leg position. Urology. 2014;84:565–570. doi:10.1016/j.urology.2014.04.020
21. Hamamoto S, Yasui T, Okada A, et al. Endoscopic combined intrarenal surgery for large calculi: simultaneous use of flexible ureteroscopy and mini-percutaneous nephrolithotomy overcomes the disadvantageous of percutaneous nephrolithotomy monotherapy. J Endourol. 2014;28(1):28–33. PMID: 23987470. doi:10.1089/end.2013.0361
22. Honey RJ, Wiesenthal JD, Ghiculete D, Pace S, Ray AA, Pace KT. Comparison of supracostal versus infracostal percutaneous nephrolithotomy using the novel prone-flexed patient position. J Endourol. 2011;25(6):947–954. doi:10.1089/end.2010.0705
23. Singh P, Nayyar R, Bagga B, et al. Effects of horizontal versus vertical bolster alignment on anatomical orientation of kidney as applied to prone percutaneous nephrolithotomy. World J Urol. 2021;39(12):4471–4476. doi:10.1007/s00345-021-03728-z
24. He Z, Tang F, Lu Z, et al. Comparison of supracostal and infracostal access for percutaneous nephrolithotomy: a systematic review and meta-analysis. Urol J. 2019;16(2):107–114. doi:10.22037/uj.v0i0.4727
25. Chow AK, Ogawa S, Seigel C, et al. Evaluation of perirenal anatomic landmarks on computed tomography to reduce the risk of thoracic complications during supracostal percutaneous nephrolithotomy. J Endourol. 2021;35(5):589–595. doi:10.1089/end.2020.0551
26. Shoma AM, Eraky I, El-Kenawy MR, et al. Percutaneous nephrolithotomy in the supine position: technical aspects and functional outcome compared with the prone technique. Urology. 2002;60:388–392. doi:10.1016/S0090-4295(02)01738-7
27. McCahy P, Rzetelski-West K, Gleeson J. Complete stone clearance using a modified supine position: initial experience and comparison with prone percutaneous nephrolithotomy. J Endourol. 2013;27(6):705–709. doi:10.1089/end.2012.0650
28. Karami H, Mohammadi R, Lotfi B. A study on comparative outcomes of percutaneous nephrolithotomy in prone, supine, and flank positions. World J Urol. 2013;31(5):1225–1230. doi:10.1007/s00345-012-0889-y
29. Tepeler A, Binbay M, Akman T, et al. Parenchymal thickness: does it have an impact on outcomes of percutaneous nephrolithotomy? Urol Int. 2013;90(4):405–410. doi:10.1159/000346336
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.