")
Back to Journals » Clinical Ophthalmology » Volume 18
Comparative Analysis of Tolerance to Experimentally Induced Astigmatism with Three Types of Multifocal Intraocular Lenses
Authors Chang JSM , Liu SCT, Ma NTC, Ng JCM
Received 8 July 2023
Accepted for publication 2 November 2023
Published 13 January 2024 Volume 2024:18 Pages 139—149
DOI https://doi.org/10.2147/OPTH.S429630
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
John So Min Chang,1 Sylvia Chui Ting Liu,1 Nadine Tsz Ching Ma,1 Jack Chun Man Ng2
1Department of Ophthalmology, Hong Kong Sanatorium & Hospital, Hong Kong; 2Department of Ophthalmology, Grantham Hospital, Hong Kong
Correspondence: John So Min Chang, Department of Ophthalmology, Hong Kong Sanatorium & Hospital, Hong Kong, Tel +852 2835 8884, Fax +852 2835 8887, Email [email protected]
Purpose: The effect of residual astigmatism and its axis on distance and near visual acuities (VAs) with multifocal intraocular lenses (IOLs) has not been studied extensively. This study compared the tolerance to experimentally induced residual astigmatism among bifocal, trifocal, and extended depth-of-focus (EDOF) IOLs.
Patients and Methods: This retrospective, comparative study included 70 eyes of 70 patients implanted with bifocal, trifocal, or EDOF IOLs. Distance and near VAs were assessed with experimentally induced astigmatism by placing positive cylindrical lenses in increments of 0.50 diopters to 2.00 diopters at 90° and 180° axes over the best distance correction.
Results: Both distance and near VAs worsened with increasing magnitudes of experimentally induced astigmatism except in the EDOF group, in which the near VA remained within a clinically acceptable limit, ie, within one line from the best corrected VA under all ranges of experimentally induced astigmatism. Furthermore, the EDOF group showed the highest astigmatic threshold for losing VA lines following experimental astigmatic induction at both distance and near. The distance VA was generally better at with-the-rule (WTR) than against-the-rule (ATR) astigmatism for all three IOL groups. On the other hand, the near VA was generally better at WTR than ATR astigmatism in the bifocal group, comparable between WTR and ATR astigmatism in the trifocal group, and generally better at ATR than WTR astigmatism in the EDOF group.
Conclusion: The EDOF IOL demonstrated the highest tolerance to experimentally induced astigmatism at both distance and near. VA was generally less affected by WTR astigmatism than ATR astigmatism, especially at distance. We proposed the residual astigmatism thresholds for clinically acceptable VA reduction in all three IOL groups.
Keywords: residual astigmatism, bifocal, extended depth-of-focus, trifocal
Introduction
Due to their good visual outcomes and high possibilities of spectacle independence, leading to high patient satisfaction,1,2 modern multifocal intraocular lenses (MIOLs) and extended depth-of-focus (EDOF) IOLs have gained in popularity in the last two decades.3 However, residual refractive error, a major determinant of postoperative spectacle independence, remains an issue regarding patient satisfaction.4–6 Therefore, careful planning of the postoperative refraction is vital to achieve excellent performance, particularly with MIOL implantation.
For patients with low or moderate corneal astigmatism, the use of toric MIOLs may be too costly, whereas clear corneal incision could be less effective. In addition, it has been suggested that mild postoperative astigmatism may be beneficial to near vision while preserving acceptable distance vision in eyes implanted with monofocal IOLs.7–10 To make an informed decision, surgeons should understand the tolerance to residual astigmatism of different types of MIOLs and EDOF IOLs so as to achieve acceptable vision at various distances.
In comparative studies that assessed the distance vision in eyes implanted with MIOLs, EDOF IOLs provided greater tolerance to astigmatism than bifocal or trifocal IOLs,11 whereas bifocal IOLs were more tolerant than trifocal IOLs.12 For near vision, trifocal IOLs were generally and slightly more tolerant to astigmatism than bifocal IOLs.12
The astigmatic axis might also play a role. Studies have suggested that with-the-rule (WTR) astigmatism is generally more favorable than against-the-rule (ATR) astigmatism for distance vision in virgin eyes,13,14 eyes with prior corneal refractive surgery,15 and eyes implanted with monofocal IOLs,16,17 whereas the opposite is true for near vision in virgin eyes18 and eyes implanted with monofocal IOLs.7,8,19 However, one study found no significant difference in effect of residual astigmatism axis on distance vision.20
Besides, these results may not be generalized to eyes implanted with MIOLs. One study reported that ATR astigmatism resulted in greater reduction in distance visual acuity (VA) than WTR astigmatism for trifocal IOL.16 Other studies have reported a similar reduction in distance VA between experimentally induced WTR and ATR astigmatism for MIOLs,20 in particular bifocal, trifocal, and EDOF IOLs.11 Notably, these studies did not evaluate the near vision. Overall, the benefit of targeting mild residual astigmatism at a particular axis to meet the visual demands of individual patients appears conflicting.
Given that few comparative studies of MIOLs have simultaneously evaluated the effect of residual astigmatism on distance and near vision and that they have focused only on ATR astigmatism,12,21,22 we compared the effect of residual astigmatism and its axes (ATR vs WTR) on both distance and near vision among bifocal, trifocal, and EDOF IOLs in this study.
Materials and Methods
Patients and Intraocular Lenses
This retrospective, comparative case series included patients who underwent cataract surgery or refractive lens exchange with unilateral or bilateral implantation of one of the following MIOLs at the Hong Kong Sanatorium & Hospital: TECNIS ZMB00 (Johnson & Johnson Vision, Santa Ana, CA, USA) [bifocal group]; FineVision Pod F (Physiol, Liége, Belgium) and FineVision Pod FT (Physiol) [trifocal group]; LENTIS Comfort (LS-313 MF15) (Teleon Surgical BV, Spankeren, the Netherlands), LENTIS Comfort Toric (LS-313 MF15Tx) (Teleon Surgical BV), and LENTIS Mplus toric (LU-313 MF15T) (Teleon Surgical BV) [EDOF group].
The inclusion criteria were age of 40 years or older, postoperative corrected distance VA of 20/25 or better, and postoperative follow-up period of 28 days or longer. The exclusion criteria were the presence of any systemic or ocular disease that might affect vision, use of systemic or ocular medications that might affect vision, history of corneal refractive surgery, and presence of intraoperative complications.
The bifocal IOL used in this study is diffractive and provides +4.00 diopters (D) of near addition (~ +3.20 D at the spectacle plane). Light energy is distributed symmetrically between the distance and near foci and is independent of pupillary size.
The trifocal IOL is diffractive and provides a near addition of +3.50 D (~ +2.80 D at the spectacle plane) and an intermediate addition of +1.75 D (~ +1.40 D at the spectacle plane). The light energy is distributed to the distance, intermediate, and near foci by 42%, 15%, and 29%, respectively. The toric version was also included.
The EDOF IOL is rotationally asymmetric and refractive. It contains an aspheric distance zone and a sector-shaped near zone of +1.50 D near addition (~ +1.20 D at the spectacle plane) with a transition zone for intermediate vision. The two toric versions were also included in this study, with one allowing spherical and cylindrical power being customized to the nearest 0.01 D.
Surgical Technique
One surgeon performed all surgeries. A keratome was used to create a 2.25-mm clear corneal incision either superiorly or temporally. DisCoVisc ophthalmic viscosurgical device (Alcon Laboratories Inc., Fort Worth, TX, USA) was injected into the anterior chamber, and a manual continuous curvilinear capsulorhexis was made. Coaxial phacoemulsification was performed after hydrodissection and nuclear splitting. The residual cortex was irrigated and aspirated. Posterior capsule was polished using a coaxial system. All IOLs were placed into the capsular bag.
Preoperative and Postoperative Examination
Preoperatively, all patients underwent a comprehensive ophthalmic assessment, including history taking, VA, biometry, and ocular health examination.
Follow-up visits were scheduled for postoperative 1 day, 1 week, 1 month, and 3 months. The outcome measures included uncorrected distance and near VAs, non-cycloplegic subjective refraction, and distance-corrected VA with and without experimentally induced astigmatism at distance and near. The near viewing distance was 30 cm for the bifocal and trifocal groups, and 40 cm for the EDOF group.
Near VA was measured using the SLOAN Two-Side Early Treatment Diabetic Retinopathy Study Format Near Vision Chart (Precision Vision, La Salle, IL, USA). Because this chart is designed for a viewing distance at 40 cm, the actual near VAs for the bifocal and trifocal groups were calculated by the visual angle subtended. All vision tests were performed under photopic condition at 85 candelas/m2.
Simulation of Residual Astigmatism
Older patients usually have ATR astigmatism.23 In contrast, patients undergoing refractive lens exchange for presbyopia correction are usually younger and tend to have WTR astigmatism. As such, we considered only the effect of residual WTR and ATR astigmatism. We simulated residual astigmatism by experimentally inducing cylindrical lenses over the eyes.11,12,16,21,22 All patients were best corrected at distance before simulation of the residual astigmatism, which was accomplished by placing positive cylindrical lenses from 0.50 diopter of cylinder (DC) to 2.00 DC in 0.50 DC steps at 180° and 90° axes to mimic simple myopic WTR and ATR astigmatism, respectively. We defined clinically acceptable reduction in vision as loss of no more than one line of VA from the best-corrected VA.
Statistical Analysis
In general, one eye was randomly chosen for analysis for patients with bilateral implantation. However, due to the lower implantation rate of trifocal IOLs compared to other IOL types, the eye implanted with trifocal IOL was chosen for analysis when the other eye was implanted with a bifocal or EDOF IOL.
All VAs were converted to the logarithm of minimum angle of resolution (logMAR) for statistical analysis.
Normality of data was checked using Shapiro–Wilk test. Patient demographics between IOL groups were compared using one-way analysis of variance with Bonferroni-corrected independent t-test, except for IOL cylindrical power with independent t-test, which involved only two IOL groups. The differences in VA between experimentally induced ATR and WTR astigmatism for each DC for each IOL group and the difference in VA reduction for each condition of experimentally induced astigmatism between distance and near were assessed using paired t-test. The differences in VA reduction from plano for each condition of experimentally induced astigmatism among the three IOL groups were assessed using one-way analysis of variance and post-hoc pairwise analysis using the Bonferroni-corrected independent t-test.
A corresponding alternative statistical test was used when there was a violation in statistical assumption.
A p-value <0.05 was considered statistically significant. All statistical analyses were performed using SPSS (version 25.0, SPSS Inc.).
Ethics Approval
The research ethics committee of Hong Kong Sanatorium & Hospital approved the study, which adhered to the tenets of the Declaration of Helsinki. Patient consent was waived due to the retrospective nature of the study. Patient’s personal information was maintained with confidentiality.
Results
This study included 70 eyes of 70 patients (31 men [44%]; mean age, 59.6±7.0 years; range, 47 to 78 years). The bifocal, trifocal, and EDOF groups comprised 25, 23, and 22 eyes, respectively.
Table 1 shows the patient demographics overall and by IOL group. Patients in the EDOF group were significantly older at surgery than those in the bifocal and trifocal groups. The EDOF group had a greater proportion of men than the bifocal group. The follow-up period was significantly longer in the bifocal group than the trifocal and EDOF groups.
 |
Table 1 Patient Demographics (70 Eyes of 70 Patients) |
Table 2 shows the postoperative refraction and distance-corrected VAs overall and by IOL group. The postoperative refractions (sphere, cylinder, and spherical equivalent) and corrected distance VAs did not differ significantly among the groups. The distance-corrected near VAs were significantly better in the bifocal and trifocal groups than the EDOF group.
 |
Table 2 Postoperative Refraction and Distance-Corrected Visual Acuity at Distance and Near |
Effect of Astigmatism Magnitude
Figure 1 shows the comparison of the reduction in VA from plano under different conditions of experimentally induced astigmatism among the IOL groups. The distance VA worsened with increasing magnitude of experimentally induced astigmatism in all three IOL groups, with more remarkable VA reduction in the bifocal group than the EDOF group (Figure 1A). The near VA worsened with increasing magnitude of experimentally induced astigmatism in the bifocal and trifocal groups only (Figure 1B). The near vision in the EDOF group remained within the clinically acceptable reduction in VA for all ranges of experimentally induced astigmatism magnitudes and axes. In all three IOL groups, the VA reduction for all experimentally induced astigmatism magnitudes was more pronounced at distance than near (p<0.05) except with WTR astigmatism of 0.50 DC in the bifocal group, and WTR astigmatism of 0.50 DC and 1.00 DC in the trifocal group.
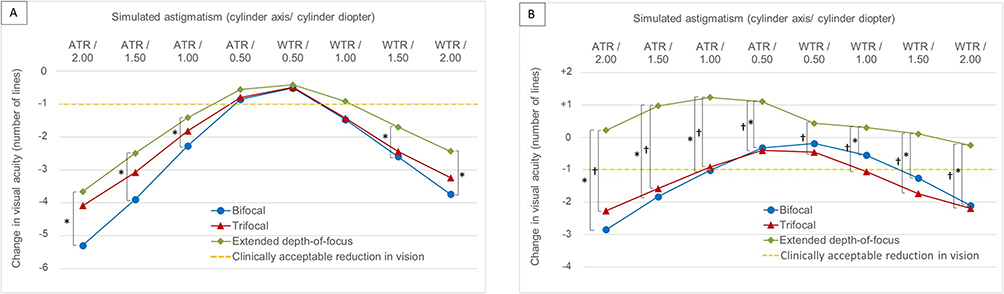 |
Figure 1 The reductions in visual acuities (VAs) from plano under different conditions of experimentally induced astigmatism at distance (A) and near (B). The dotted line indicates the astigmatic threshold for clinically acceptable reduction in vision. The asterisks (*) and daggers (†) denote a significant difference in VA reduction between bifocal/extended depth-of-focus and trifocal/extended depth-of-focus intraocular lens groups, respectively. Data on distance VAs was unavailable for 11 eyes (44%) in the bifocal group under experimentally induced against-the-rule (ATR) astigmatism of 2.00 diopter of cylinder (DC); 1 (4%) and 4 eyes (17%) in the trifocal group under experimentally induced with-the-rule (WTR) and ATR astigmatism of 2.00 DC respectively. Data on near VAs was unavailable for 9 eyes (36%) and 1 eye (4%) in the bifocal group under experimentally induced ATR astigmatism of 2.00 DC and all other magnitudes respectively; 2 (9%) and 5 (22%) eyes in the trifocal group under experimentally induced WTR and ATR astigmatism of 2.00 DC, respectively; 1 eye (4%) in the trifocal group under experimentally induced WTR and ATR astigmatism of 0.50, 1.00, and 1.50 DC. |
Effect of Astigmatism Axis
The distance VA was generally better with WTR than ATR astigmatism for all three IOL groups (Figure 2A-C). The near VA was generally better with WTR than ATR astigmatism in the bifocal group (Figure 2D), comparable between WTR and ATR astigmatism in the trifocal group (Figures 2E), and generally better with ATR than WTR astigmatism in the EDOF group (Figure 2F).
 |
Figure 2 Comparisons of visual acuities (VAs) under different magnitudes of experimentally induced astigmatism between with-the-rule (WTR) and against-the-rule (ATR) axes for each intraocular lens group at distance (A-C) and near (D-F). The asterisks (*) denote a significant difference between the WTR and ATR astigmatism. Data on distance VAs was unavailable for 11 eyes (44%) in the bifocal group under experimentally induced ATR astigmatism of 2.00 diopter of cylinder (DC); 1 (4%) and 4 eyes (17%) in the trifocal group under experimentally induced WTR and ATR astigmatism of 2.00 DC respectively. Data on near VAs was unavailable for 9 eyes (36%) and 1 eye (4%) in the bifocal group under experimentally induced ATR astigmatism of 2.00 DC and all other magnitudes respectively; 2 (9%) and 5 (22%) eyes in the trifocal group under experimentally induced WTR and ATR astigmatism of 2.00 DC, respectively; 1 eye (4%) in the trifocal group under experimentally induced WTR and ATR astigmatism of 0.50, 1.00, and 1.50 DC. |
Astigmatic Threshold for Acceptable Vision
Table 3 and Table 4 show the astigmatic thresholds for clinically acceptable reduction in VA by IOL group and the axis of experimentally induced astigmatism. The EDOF group showed the highest astigmatic thresholds at distance (Table 3) and near (Table 4), with a higher threshold at near than distance.
 |
Table 3 Astigmatic Threshold for Clinically Acceptable Reduction in Distance Visual Acuity |
 |
Table 4 Astigmatic Threshold for Clinically Acceptable Reduction in Near Visual Acuity |
Discussion
Our study showed that experimentally induced residual astigmatism had a clinically significant impact on the distance VA in all three IOL groups. In contrast, residual astigmatism adversely affected the near VA mainly in the bifocal and trifocal IOL groups but improved the near VA in the EDOF IOL group. ATR astigmatism had a greater adverse effect than WTR astigmatism on distance VA with all IOL types and on near VA with bifocal IOL only. An opposite trend was observed for near vision with the EDOF IOL.
Discussion of Findings and Comparison to the Literature
The overall better distance visual performance with WTR than ATR astigmatism in all three IOL groups in our study agrees with previous studies of virgin eyes,14 post-LASIK eyes,15 pseudophakic monofocal and multifocal-implanted eyes.16,17 This may be explained in part by the Conoid of Sturm principle, whereby in eyes with simple myopic WTR astigmatism, the image is focused on the vertical focal line on the retina when viewing a distant object. Since the alphabet optotype used in our study had more prominent vertical than horizontal strokes, the image was sharper in eyes with WTR astigmatism than those with ATR astigmatism. However, previous studies have reported no significant difference in the impact of astigmatic axis on virgin eyes9,24–26 or eyes implanted with monofocal IOLs7,19,20 or MIOLs.11,20
For near vision, our results showed that VA with WTR astigmatism was significantly better than ATR astigmatism with bifocal IOL. However, no previous study has assessed the impact of astigmatism axis on near vision in eyes implanted with bifocal IOLs. On the other hand, near VA was similar between WTR and ATR astigmatism with trifocal IOLs, which is in line with studies on virgin eyes27,28 and a study on eyes implanted with EDOF IOL.29 However, for EDOF IOLs, near VA was significantly better with ATR than WTR astigmatism, which agrees with one study on virgin eyes18 and few studies on monofocal IOLs.7,8,10,19,30 The difference in astigmatism’s impact on near vision between IOLs might be due to the different lens design.
The greater VA reduction with experimentally induced astigmatism at distance than at near in all three IOL groups was consistent with the findings reported in virgin eyes,28 eyes implanted with monofocal, bifocal, and trifocal IOLs.12,22
The tolerance to astigmatism was the highest with the EDOF IOL at both distance and near. This is consistent with the findings reported by Carones.11 We also found that the impact of experimentally induced astigmatism was generally similar between the bifocal and trifocal groups. In contrast, Hayashi et al12 and Carones11 reported that bifocal IOL (ReSTOR +2.0 D and +3.0 D, Alcon Laboratories Inc.) was less affected by experimentally induced astigmatism than trifocal IOL (PanOptix, Alcon Laboratories Inc.). Their opposite findings might be due to the different IOL models studied in our study.
The astigmatic thresholds for different types of MIOLs have been reported previously.11,12,16,21,22 Due to the varied definitions of astigmatic thresholds among studies, we present the results of studies with similar definitions to our study in Table 5.11,12,16 With trifocal IOLs, our astigmatic threshold was generally similar to those reported in other studies.11,12,16 With bifocal IOL, our threshold (≤0.50 DC) was similar to5 or lower than12 other studies. This might be due to the more stringent threshold in our study (reduction of ≤1 line from the best-corrected VA) compared to the threshold (VA of 20/32 or better) used by Hayashi et al.12 With the EDOF IOL, we found a notably high threshold exceeding 2.00 DC for near vision. However, we could not identify any study that assessed the near threshold of EDOF IOLs. Our threshold for distance vision with the EDOF IOL (≤0.70 DC) was slightly lower than that of Carones (≤1.00 DC), possibly due to the use of different IOL models.11
 |
Table 5 Astigmatic Threshold of Multifocal Intraocular Lens in Other Studies and in the Current Study |
Clinical Implications
Our results may aid preoperative planning if surgeons wish to leave mild residual WTR or ATR astigmatism according to patients’ visual demands and the type of MIOL being implanted.
When the IOL cylindrical power is unavailable in precise increments or if different IOL formulas or biometers give different results, targeting mild postoperative residual WTR astigmatism (≤0.50 DC) would be more desirable for bifocal and trifocal IOLs because it could offer better distance vision and similar or better near vision compared to mild ATR astigmatism. For EDOF IOLs, surgeons may consider targeting mild ATR astigmatism (≤0.50 DC) especially when the patient has a greater visual demand at near than distance, because it provided better near VA while offering similar distance vision when compared to mild WTR astigmatism.
If monovision is planned for bilateral implantation with an EDOF IOL, surgeons may allow more postoperative astigmatism (especially ATR astigmatism) in eyes targeting myopia. Although this can lead to worsened distance VA in the eye targeting myopia, the binocular distance VA should only be minimally affected.31–33
Surgeons should also take into account the type of MIOL when deciding whether to leave the corneal astigmatism untreated (ie, using a non-toric IOL). Due to the higher tolerance to residual astigmatism with EDOF IOL, surgeons may offer a non-toric IOL to candidates for implantation of EDOF IOL even if they have moderate corneal astigmatism. However, the possible advantages and disadvantages of the non-toric option should be thoroughly explained to patients preoperatively.
Study Limitations
Our study has several limitations. First, the increment of the astigmatic simulation was 0.50 DC, which might have yielded a less precise astigmatic threshold. However, a finer step with 0.25 DC would significantly lengthen the examination time, causing patient fatigue. Second, not all the bifocal, trifocal, or EDOF IOLs have the same design. Our results may not be generalized to other IOLs of the same type. Third, oblique astigmatism was not evaluated because it was less commonly seen in cataract surgery planning23,34,35 and also significantly increased examination time. Future studies may include oblique astigmatism for comprehensiveness.
Conclusions
In conclusion, at both distance and near, the EDOF IOL provided the highest tolerance to experimentally induced astigmatism, whereas the bifocal and trifocal IOLs performed similarly. The EDOF IOL provided a slight improvement in near vision, especially with ATR astigmatism. For all three IOL types, the distance vision was generally less affected by WTR astigmatism than ATR astigmatism. The near vision was less adversely affected by WTR astigmatism for the bifocal IOL, but less adversely affected by ATR astigmatism for the EDOF IOL, and affected in a similar extent by WTR and ATR astigmatisms for the trifocal IOL. The distance vision was generally more affected by astigmatism than the near vision with all three IOL types. Our study reported the astigmatic threshold for clinically acceptable vision for all three IOLs. Surgeons may target mild-to-moderate residual WTR or ATR astigmatism based on the patients’ visual demand and the type of MIOL being implanted.
Disclosure
John S M Chang has received lecture honoraria and research grant from Alcon Laboratories Inc. and Carl Zeiss Inc.; and lecture honoraria from Global Vision HK Ltd and Johnson & Johnson Vision. The other authors have no conflicts of interest in this work.
References
1. Galvis V, Escaf LC, Escaf LJ, et al. Visual and satisfaction results with implantation of the trifocal Panoptix® intraocular lens in cataract surgery. J Optom. 2022;15(3):219–227. doi:10.1016/j.optom.2021.05.002
2. Moshirfar M, Stapley SR, Corbin WM, et al. Comparative visual outcome analysis of a diffractive multifocal intraocular lens and a new diffractive multifocal lens with extended depth of focus. J Clin Med. 2022;11(24):7374. doi:10.3390/jcm11247374
3. Rampat R, Gatinel D. Multifocal and extended depth-of-focus intraocular lenses in 2020. Ophthalmology. 2021;128(11):e164–e185. doi:10.1016/j.ophtha.2020.09.026
4. de Silva SR, Evans JR, Kirthi V, Ziaei M, Leyland M. Multifocal versus monofocal intraocular lenses after cataract extraction. Cochrane Database Syst Rev. 2016;12(12):CD003169. doi:10.1002/14651858.CD003169.pub4
5. de Vries NE, Webers CAB, Touwslager WRH, et al. Dissatisfaction after implantation of multifocal intraocular lenses. J Cataract Refract Surg. 2011;37(5):859–865. doi:10.1016/j.jcrs.2010.11.032
6. Hawker MJ, Madge SN, Baddeley PA, Perry SR. Refractive expectations of patients having cataract surgery. J Cataract Refract Surg. 2005;31(10):1970–1975. doi:10.1016/j.jcrs.2005.03.065
7. Nagpal KM, Desai C, Trivedi RH, Vasavada AR. Is pseudophakic astigmatism a desirable goal? Indian J Ophthalmol. 2000;48(3):213–216.
8. Serra P, Chisholm C, Sanchez Trancon A, Cox M. Distance and near visual performance in pseudophakic eyes with simulated spherical and astigmatic blur. Clin Exp Optom. 2016;99(2):127–134. doi:10.1111/cxo.12350
9. Singh A, Pesala V, Garg P, Bharadwaj SR. Relation between uncorrected astigmatism and visual acuity in pseudophakia. Optom Vis Sci. 2013;90(4):378–384. doi:10.1097/OPX.0b013e318288afb5
10. Sharma R, Khurana AK, Chawla U, Bura N, Khurana A. Study on the role of simple myopic against-the-rule astigmatism in visual rehabilitation in monofocal pseudophakic patients. Int J Med Ophthalmol. 2020;1(2):17–22. doi:10.33545/26638266.2020.v2.i1a.25
11. Carones F. Residual astigmatism threshold and patient satisfaction with bifocal, trifocal and extended range of vision intraocular lenses. Open J Ophthalmol. 2017;7(1):1–7. doi:10.4236/ojoph.2017.71001
12. Hayashi K, Yoshida M, Igarashi C, Hirata A. Effect of refractive astigmatism on all-distance visual acuity in eyes with a trifocal intraocular lens. Am J Ophthalmol. 2021;221:279–286. doi:10.1016/j.ajo.2020.07.051
13. Atchison DA, Mathur A. Visual acuity with astigmatic blur. Optom Vis Sci. 2011;88(7):E798–E805. doi:10.1097/OPX.0b013e3182186bc4
14. Little JA, Molloy J, Saunders KJ. The differing impact of induced astigmatic blur on crowded and uncrowded paediatric visual acuity chart results. Ophthalmic Physiol Opt. 2012;32(6):492–500. doi:10.1111/j.1475-1313.2012.00939.x
15. Mimouni M, Nemet A, Pokroy R, Sela T, Munzer G, Kaiserman I. The effect of astigmatism axis on visual acuity. Eur J Ophthalmol. 2017;27(3):308–311. doi:10.5301/ejo.5000890
16. Ang RE. Comparison of tolerance to induced astigmatism in pseudophakic eyes implanted with small aperture, trifocal, or monofocal intraocular lenses. Clin Ophthalmol. 2019;13:905–911. doi:10.2147/OPTH.S208651
17. Yamamoto T, Hiraoka T, Beheregaray S, Oshika T. Influence of simple myopic against-the-rule and with-the-rule astigmatism on visual acuity in eyes with monofocal intraocular lenses. Jpn J Ophthalmol. 2014;58(5):409–414. doi:10.1007/s10384-014-0337-1
18. Casagrande M, Baumeister M, Bühren J, Klaproth OK, Titke C, Kohnen T. Influence of additional astigmatism on distance-corrected near visual acuity and reading performance. Br J Ophthalmol. 2014;98(1):24–29. doi:10.1136/bjophthalmol-2013-303066
19. Trindade F, Oliveira A, Frasson M. Benefit of against-the-rule astigmatism to uncorrected near acuity. J Cataract Refract Surg. 1997;23(1):82–85. doi:10.1016/S0886-3350(97)80155-1
20. Schallhorn SC, Hettinger KA, Pelouskova M. Effect of residual astigmatism on uncorrected visual acuity and patient satisfaction in pseudophakic patients. J Cataract Refract Surg. 2021;47(8):991–998. doi:10.1097/j.jcrs.0000000000000560
21. Hayashi K, Hayashi H, Nakao F, Hayashi F. Influence of astigmatism on multifocal and monofocal intraocular lenses. Am J Ophthalmol. 2000;130(4):477–482. doi:10.1016/S0002-9394(00)00526-2
22. Hayashi K, Manabe S, Yoshida M, Hayashi H. Effect of astigmatism on visual acuity in eyes with a diffractive multifocal intraocular lens. J Cataract Refract Surg. 2010;36(8):1323–1329. doi:10.1016/j.jcrs.2010.02.016
23. Chen W, Zuo C, Chen C. Prevalence of corneal astigmatism before cataract surgery in Chinese patients. J Cataract Refract Surg. 2013;39(2):188–192. doi:10.1016/j.jcrs.2012.08.060
24. Ohlendorf A, Tabernero J, Schaeffel F. Visual acuity with simulated and real astigmatic defocus. Optom Vis Sci. 2011;88(5):562–569. doi:10.1097/OPX.0b013e31821281bc
25. Remón L, Tornel M, Furlan WD. Visual acuity in simple myopic astigmatism: influence of cylinder axis. Optom Vis Sci. 2006;83(5):311–315. doi:10.1097/01.opx.0000216099.29968.36
26. Serra PM, Cox MJ, Chisholm CM. The effect of astigmatic axis on visual acuity measured with different alphabets in Roman alphabet readers. Clin Optom. 2018;10:93–102. doi:10.2147/OPTO.S166786
27. Kobashi H, Kamiya K, Shimizu K, Kawamorita T, Uozato H. Effect of axis orientation on visual performance in astigmatic eyes. J Cataract Refract Surg. 2012;38(8):1352–1359. doi:10.1016/j.jcrs.2012.03.032
28. Tavazzi S, Vlasak N, Zeri F. Effects of lens-induced astigmatism at near and far distances. Clin Optom. 2023;15:105–117. doi:10.2147/OPTO.S405472
29. Cochener B. Tecnis Symfony intraocular lens with a “sweet spot” for tolerance to postoperative residual refractive errors. Open J Ophthalmol. 2017;7(1):14–20. doi:10.4236/ojoph.2017.71003
30. Nanavaty MA, Vasavada AR, Patel AS, Raj SM, Desai TH. Analysis of patients with good uncorrected distance and near vision after monofocal intraocular lens implantation. J Cataract Refract Surg. 2006;32(7):1091–1097. doi:10.1016/j.jcrs.2006.03.021
31. Chang JSM, Liu SCT, Jcm N, Ma PL. Monovision with a bifocal diffractive multifocal intraocular lens in presbyopic patients: a prospective, observational case series. Am J Ophthalmol. 2020;212:105–115. doi:10.1016/j.ajo.2019.11.010
32. Cochener B; Concerto Study Group. Clinical outcomes of a new extended range of vision intraocular lens: international Multicenter Concerto Study. J Cataract Refract Surg. 2016;42(9):1268–1275. doi:10.1016/j.jcrs.2016.06.033
33. Cochener B. Influence of the level of monovision on visual outcome with an extended range of vision intraocular lens. Clin Ophthalmol. 2018;12:2305–2312. doi:10.2147/OPTH.S184712
34. de Bernardo M, Zeppa L, Cennamo M, Iaccarino S, Zeppa L, Rosa N. Prevalence of corneal astigmatism before cataract surgery in Caucasian patients. Eur J Ophthalmol. 2014;24(4):494–500. doi:10.5301/ejo.5000415
35. Duman R, Duman R, Cetinkaya E, et al. Analysis of corneal astigmatism with NIDEK axial length scan in Caucasian cataract surgery candidates. Niger J Clin Pract. 2018;21(4):456–461. doi:10.4103/njcp.njcp_117_17
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.