")
Back to Journals » Cancer Management and Research » Volume 7
Clinical utility of RapidArcTM radiotherapy technology
Authors Infusino E
Received 29 April 2015
Accepted for publication 21 September 2015
Published 12 November 2015 Volume 2015:7 Pages 345—356
DOI https://doi.org/10.2147/CMAR.S72775
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Kenan Onel
Erminia Infusino
Department of Radiotherapy, Campus Bio-Medico University Hospital, Rome, Italy
Abstract: RapidArcTM is a radiation technique that delivers highly conformal dose distributions through the complete rotation (360°) and speed variation of the linear accelerator gantry. This technique, called volumetric modulated arc therapy (VMAT), compared with conventional radiotherapy techniques, can achieve high-target volume coverage and sparing damage to normal tissues. RapidArc delivers precise dose distribution and conformity similar to or greater than intensity-modulated radiation therapy in a short time, generally a few minutes, to which image-guided radiation therapy is added. RapidArc has become a currently used technology in many centers, which use RapidArc technology to treat a large number of patients. Large and small hospitals use it to treat the most challenging cases, but more and more frequently for the most common cancers. The clinical use of RapidArc and VMAT technology is constantly growing. At present, a limited number of clinical data are published, mostly concerning planning and feasibility studies. Clinical outcome data are increasing for a few tumor sites, even if only a little. The purpose of this work is to discuss the current status of VMAT techniques in clinical use through a review of the published data of planning systems and clinical outcomes in several tumor sites. The study consisted of a systematic review based on analysis of manuscripts retrieved from the PubMed, BioMed Central, and Scopus databases by searching for the keywords "RapidArc", "Volumetric modulated arc radiotherapy", and "Intensity-modulated radiotherapy".
Keywords: IMRT, VMAT, SBRT, SRS, treatment planning software
Introduction
Varian Medical Systems, Inc. (Palo alto, CA, USA) has launched into the marketplace a new arc delivery technique named RapidArc™. In this method, the treatment is delivered in one or more arc rotations of the linac gantry; in this rotation, the multileaf collimators (MLCs) are moving dynamically and, at the same time, the dose rate is varied throughout variation of the gantry speed rotation.1
The earliest form of arc therapy, termed intensity-modulated arc therapy (IMAT), was first described by Yu et al in 19952 and required the use of multiple superimposed arcs to achieve a satisfactory dose distribution.3 The general IMAT concept as described by Yu et al2 makes use of several arcs, all delivered in a cone-beam fashion, but as an “arc-in-arc” approach, where each arc patches in the missing dose levels from the previous arcs to obtain the desired dose distribution.
With the RapidArc technique, to obtain an extremely conformal dose distribution by means of the increase of degrees of freedom, the variation of dose rate is gained in a single arc by the mishmash of gantry speed combined with dynamic MLCs, all specified in a large number of control points over the rotation. There is a limit to the modulation factor that is related to the movement allowable of the MLCs per second per degree of gantry rotation.
The RapidArc approach can be considered an extension to dynamic MLC IMRT, and the machine commissioning and quality assurance should validate standard dynamic MLC delivery, and the combination with dose rate variations and gantry rotation with variable speed, which is specific to RapidArc.
Comparisons between RapidArc and IMRT have been evaluated for quite a lot of tumor sites. Relevant works have largely demonstrated that RapidArc, compared to IMRT, is capable of creating analogous or better dose distributions, compared to IMRT, is capable of creating analogous or better dose distributions, while attaining a reduction in treatment time and monitor units are halved.4–8 The quantity of radiation generated by the linear accelerator is expressed in MUs; growth in MUs is connected with a higher scatter radiation from the accelerator, which would hypothetically increase the risk of secondary malignancies. Above all, two studies have assessed treatment with RapidArc for head and neck cancer and observed that the distribution is comparable to or improved with respect to IMRT; there is a decrease in MUs and, consequently, an important decrease in treatment times.8,9 Compared to other techniques, specifically tomotherapy and fixed-field IMRT, RapidArc has the extra benefit of more rapid treatment times. Elongated treatment time has been known as one of the disadvantages of the fixed-field IMRT technique. In the event that the IMRT plan is particularly complicated, the delivery of a fraction of the treatment can last even more than 15–30 minutes;10,11 however, most fractions of three-dimensional conformal radiation therapy (3D-CRT) require only a few minutes, depending on difficulty. This has always been considered as an inevitable consequence to achieve an extremely conformal radiotherapy, a condition that we could accept to enhance dose distribution obtained by IMRT. The extension of treatment time has more than a few undesirable implications. It requires patients to pass a lot of time on the radiotherapy couch, which can lead to patient distress and increases the risk of intra-fraction movement of the tumor or patient. Formally, it considerably reduces the quantity of patients who can be treated per treatment unit every day.12 This is particularly true when considering that the tumors are treated on a slice by-slice basis, as an axial tumor shift could cause a portion of the tumor to be underdosed, notably when single or few large fractions are used.13
Longer treatment times could cause a following increase of the time needed by the physicians for quality assurance in order to verify the dose distribution before delivering it to the patient. As well, other reflections with prolonged treatment time are necessary, such as there may be detrimental radiobiological consequences. According to some authors, with long treatment times, the tumor cells will have the possibility for DNA repair, leading to their proliferation,14,15 as in vitro data from several investigators showed.16–18
Particularly demanding radiotherapy treatments, such as stereotactic lung radiotherapy treatments, which are mainly challenging in that they deliver up to 20 Gy per fraction to a moving target, often require 30–45 minutes to deliver radiotherapy treatment utilizing IMRT, whereas, using RapidArc, it can be delivered in 4–11 minutes.19 The better treatment times with RapidArc are a consequence of a number of factors: more MUs are required for IMRT plans, and this involves having the treatment machine turned on for an extended time, verify and set accurately the parameters field and rotate the gantry require more time to send information to the treatment machine.20 With RapidArc, the arc must be able to be considered as a single field and all parameters are set just once per arc. Table 1 summarizes some articles relating to treatment times for RapidArc and VMAT techniques and tomotherapy. Figure 1 shows the dose distribution across the most representative RapidArc plans.
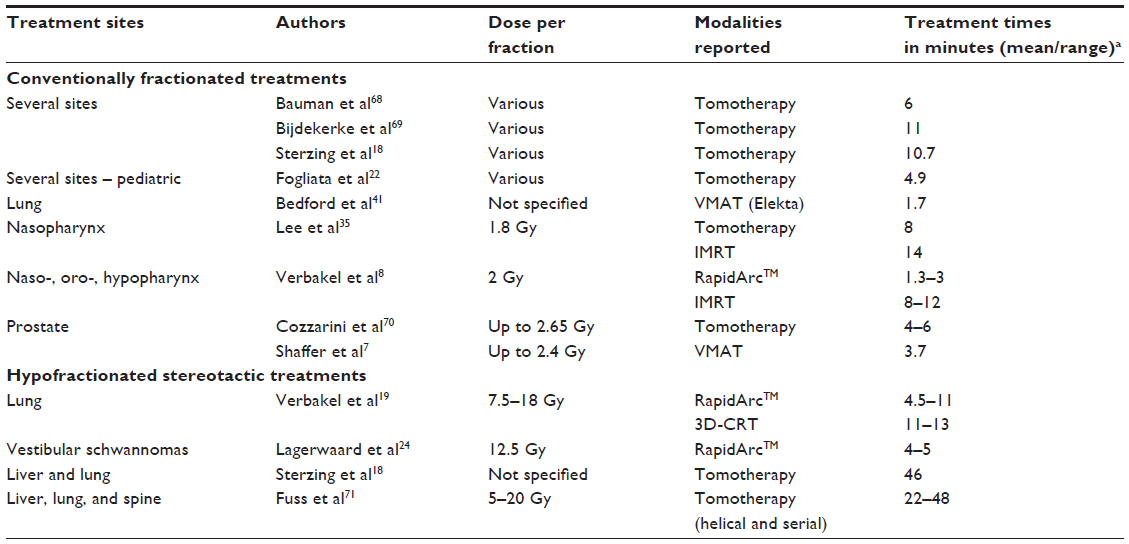 | Table 1 Representative treatment times with VMAT techniques and tomotherapy |
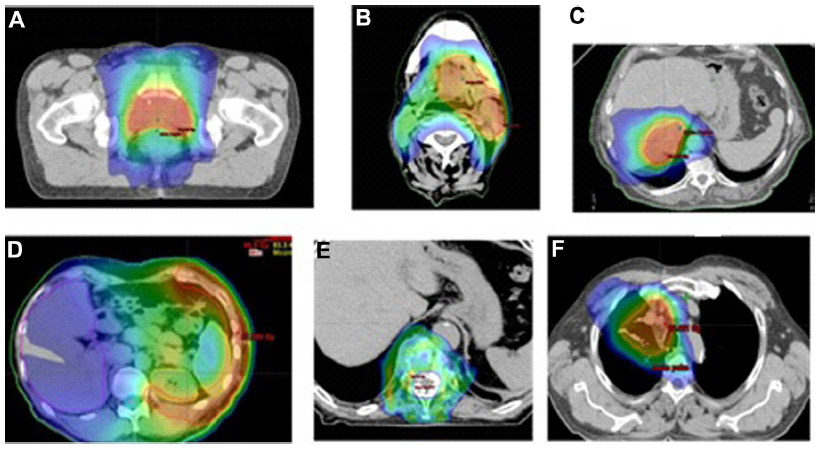 | Figure 1 The dose distribution of representative volumetric modulated arc therapy plans. |
Clinical applications of RapidArc
Brain tumors
RapidArc has been employed to treat brain cancers and metastases. Davidson et al21 determined the advantages of VMAT compared with IMRT for brain glioma and evaluated the effect of complete arc and partial arc with the VMAT technique. The investigators found particular benefit in relation to IMRT with respect to spinal cord sparing, saw a reduction in the integral dose using an additional partial arc, and came to the conclusion that VMAT gives faster delivery than IMRT for brain tumors, maintaining a very similar dosimetric effect to IMRT plans.
A study by Fogliata et al22 examined a planning study of 12 patients using RapidArc, fixed-field IMRT with five to seven fields, and helical tomotherapy. The patients suffered from meningiomas, acoustic neuromas, and pituitary adenomas. The results demonstrated similar target coverage for all techniques, with an improvement of the coverage, however faint, to the advantage of IMRT treatment. VMAT and IMRT plans were better than helical tomotherapy with regard to organ-at-risk (OAR) sparing and reducing integral dose. Also, doses to OARs were lower with IMRT plans than RapidArc; this can be considered important for patients with brain cancer to minimize the risk of radiation-induced secondary malignancy. Wagner et al23 conducted a study on malignant gliomas (World Health Organization [WHO] grade 3 or 4). They analyzed 14 treatment plans with 3D-CRT, IMRT (sliding window) utilizing five to nine fields, and single-arc VMAT. Planning target volume (PTV) coverage was better in IMRT with respect to VMAT (94.7% and 90.5%, respectively), whereas conformity was superior for VMAT and IMRT compared with 3D-CRT. For OARs far away from PTVs, 3D-CRT and IMRT were more suitable regarding PTV coverage. The trend was inverted when OARs were situated neighboring PTVs. In these cases, PTV coverage was significantly superior for VMAT. The authors recommended that 3D-CRT or IMRT would be the most appropriate solutions for PTVs situated distant from OARs. PTV coverage in these specific cases was satisfactory, with a superior sparing of healthy brain. Nevertheless, for PTVs near to OARs, VMAT technique would be more advisable, considering that PTV coverage was satisfactory, with more sparing of OARs followed by other advantages such as reduced MUs and treatment time. One cannot help but arrive at the conclusion that the choice of radiation technique for these tumors must be examined case by case, and VMAT may not always be the best solution.
For years, stereotactic radiosurgery was achieved with multiple static or conformal arcs delivered by a linear accelerator, or with multiple highly collimated cobalt sources utilizing gamma knife radiosurgery. These methods have been restricted for patients with a single metastasis or oligometastatic diseases with less than three lesions. To date, quite a lot of studies have evaluated the opportunity to use a VMAT technique for radiosurgical irradiations or stereotactic fractionations to multiple brain metastases.24,25 Lagerwaard et al24 compared whole brain radiotherapy (WBRT) with a simultaneous integrated boost to the metastatic lesions using double-arc VMAT with their conventional strategy of WBRT followed sequentially by a single stereotactic boost (21 Gy to 80% isodose) using multiple non-coplanar conformal arcs. For the integrated VMAT plan, the total dose to the metastatic lesions was 40 Gy in five fractions. The authors found adequate coverage for the boost and WBRT PTV in the integrated plans and much steeper dose gradients outside the boost PTV, which resulted in improved conformity compared with the conventional strategy. Clark et al25 evaluated the advantage of single-isocenter plans with respect to multi-isocenter plans with arc therapy for stereotactic radiosurgery of multiple central nervous system metastases. Their first results showed single-isocenter volumetric plans had a dosimetric distribution comparable to multi-isocenter plans. For tumors at close range, multiple single-isocenter plans with non-coplanar arcs were necessary. Radiosurgery for multiple targets with the RapidArc technique would be very efficient, and the delivery requires less than half the time, taking into consideration the setups needed for multi-isocenter plans. VMAT radiosurgery prefigures most likely a possible alternative for multi-isocenter techniques for radiotherapy treatment of multiple targets.
Hsu et al26 made a feasibility study about using arc therapy to deliver WBRT with a simultaneous integrated boost and hippocampal sparing for one to three brain metastases. They demonstrated that, using the Radiation Therapy Oncology Group dosimetric parameters for radiosurgery quality assurance, RapidArc can deliver highly conformal dose distributions to single metastases and in the same way was able to satisfactorily deliver WBRT with hippocampus avoidance. The mean delivery time was under 4 minutes. Awad et al28 valuated the feasibility and acceptability, as well as acute and late toxicity, of the melanoma brain metastases treated with whole brain with a simultaneous integrated and hippocampal sparing. They found only one clinical case with grade IV late toxicity, while slight toxicity in a few cases was clinically unimportant. They concluded that the dose distributions to single metastases were highly conformal and adequately delivered despite the hippocampus avoidance.
In the present author’s institution (Campus Bio-Medico University Hospital, Rome, Italy), RapidArc is also used to treat whole brain with hippocampus sparing. The representative dose distribution of a RapidArc plan is shown in Figure 2.
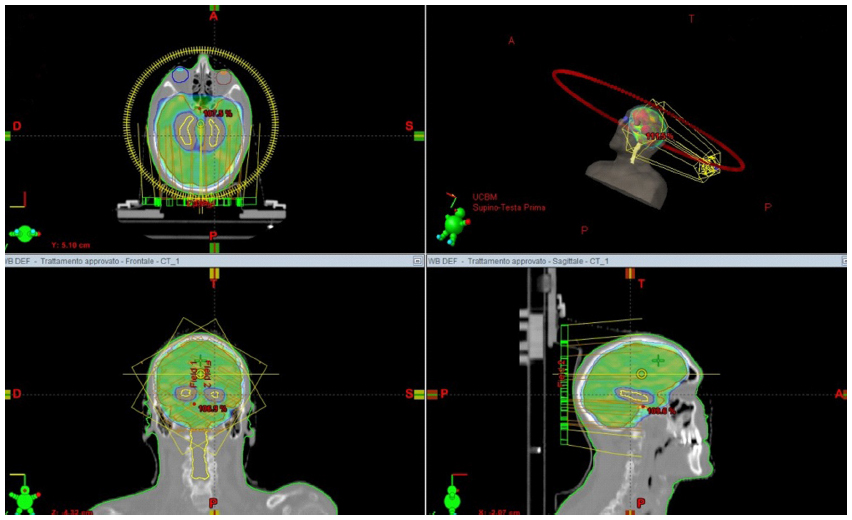 | Figure 2 An example of Arc treatment plan (axial, coronal, and sagittal views) with hippocampal sparing and homogenous dose coverage in the rest of the brain. |
Head and neck cancer
Radiation therapy for head and neck cancer can be problematic owing to the anatomy of this region, forasmuch as these tumors are generally adjacent to the critical organs where limiting dose irradiation is necessary. Besides, these cancers often show an aggressive phenotype and grow rapidly due to the rich lymphatic supply in the head and neck region, and can therefore present at a locally advanced stage. Radiotherapy is an important treatment modality in these tumors as it offers an alternative treatment option to surgical resection, which can cause unacceptable cosmetic deformity and functional impairment. Head and neck cancers are clinical cases typically treated with IMRT standard technique. Up until a short time ago, this was the best-suited solution to spare OARs in close proximity to the tumor volume. Twenty-five patients with hypopharyngeal or oropharyngeal tumors treated with IMRT were replanned by Bertelsen et al28 with one-arc VMAT. In the shift from the IMRT to VMAT, a substantial improvement occurred in all dosimetric values of the treatment plan. Low dose volumes in the healthy tissue were increased in the VMAT plan, while high dose volumes were reduced. The reduction of treatment time improved from 8.5% to 35%, showing the advantage of the VMAT plans, and a moderate reduction in the MUs was observed in the VMAT treatment plans. In an article by Johnston et al,29 head and neck cancer was planned with a simultaneous integrated boost to compare VMAT plans with IMRT plans. Making a comparison between the two techniques, both plans were dosimetrically and clinically acceptable, but IMRT plans had three times MUs of VMAT plans. Comparisons between VMAT and serial tomotherapy for nasopharyngeal carcinoma on clinical quality, OAR sparing, and efficiency of the delivery process were reported by several authors.30,31 Generally, tomotherapy provides comparable dose distribution and, in some cases, it might be argued, the best homogeneity and conformity of treatment plans, but a longer period of time was required for delivery. Neubauer et al32 studied the interfractional movement of the shoulders in respect to isocenter during treatment and evaluated the possibility of dosimetric effects of this shift in head and neck cancer treated with VMAT and IMRT plans. The mean shoulder displacement was 2–5 mm in all directions; in an extreme case, it reached 20 mm. A displacement upwards would be responsible for the loss of coverage, while, with movement downwards, there would be a risk of overdose of the brachial plexus. The research results were similar in both cases, VMAT and IMRT plans. With regard to observed shifts, the clinical target volume coverage to 99% came down to 101 cGy and the dose to the brachial plexus increased to over 72 cGy. For rear displacements, IMRT plans were more sensitive compared with VMAT plans. Oliver et al33 evaluated the practical tradeoffs between IMRT and dual-arc VMAT (DA-VMAT) for locally advanced head and neck cancer. For advanced head and neck cancer, both DA-VMAT and IMRT plans with nine fields (step-and-shoot) reached the dosimetric objectives. Although the DA-VMAT delivery time was shorter, the planning time was longer compared to IMRT. Stieler et al30 examined dose distribution of IMRT (step-and-shoot), VMAT radiotherapy, and serial tomotherapy for head and neck with conservation of one parotid; this is a situation often encountered in head and neck radiotherapy. They considered VMAT delivery in terms of dosimetric accuracy and concluded that VMAT, IMRT (with static and dynamic MLCs), and tomotherapy treatment plans were similar regarding dosimetric distribution, but VMAT indicated better efficiency with regard to treatment time and MUs required. Also, Verbakel et al8 made a comparison of head and neck treatment plans obtained by RapidArc plans and conventional IMRT with seven-field sliding window. The two different types of plans were similar regarding dose distribution; also, in this case, a mean reduction in number of MUs (approximately 60%) was noted in RapidArc plans. Single-arc RapidArc plans showed a reduced dose homogeneity in PTV compared with IMRT plans. PTV homogeneity of RapidArc plans was improved using two arcs compared with IMRT plans, and the OAR sparing in the two treatment techniques was nearly the same. Lee at al35 made a comparison of IMRT with seven fixed beams and VMAT plans with single and double arcs on nasopharyngeal carcinomas, evaluating the possible dosimetric advantages of both techniques. The results were contradictory. VMAT plans achieved better, worse, or similar results to IMRT plans depending on the complexity and size of the target volume and on the number of VMAT arcs. Even so, double-arc VMAT was still more suitable regarding OAR sparing and PTV coverage in respect to single-arc; at the same time, Lee et al35 showed similar performance compared with IMRT without forgoing the delivery efficiency. The delivery efficiency was improved thanks to the reduction in treatment time both with single and double arcs: delivery time was reduced by 51% and 41% depending on whether the user had chosen one or two arcs.
The target volumes in head and neck radiotherapy are particularly complex. On the strength of the abovementioned remarks, it seems clear that more than one arc is necessary to achieve a satisfactory dose distribution. Johnston et al29 analyzed various treatment plans with a nine-field fixed-field IMRT plan and single-arc, double-arc, and triple-arc VMAT plans in patients receiving primary or postoperative radiotherapy for pharyngeal tumors and paranasal sinus tumors. Comparing the IMRT and VMAT plans in terms of dosimetric efficiency, single-arc VMAT showed an inferior PTV coverage to the IMRT plan; in all the other cases (double- and triple-arc), PTV coverage and homogeneity were similar or superior. In primary pharyngeal patients, both single-arc and double-arc VMAT plans were inferior to the IMRT plan, while the triple-arc plan was equivalent. In the paranasal sinus group, all VMAT plans were inferior to the IMRT plan for dose coverage, particularly in the region between the orbits.
It must be emphasized that, in most studies, IMRT plans were achieved with five to seven fields. When more beams were used (seven or nine), the quality of the IMRT plan improved, but a greater number of MUs and longer treatment times corresponded to a higher number of beams.
An example of standard dose distributions for head and neck cancer is displayed in Figure 3.
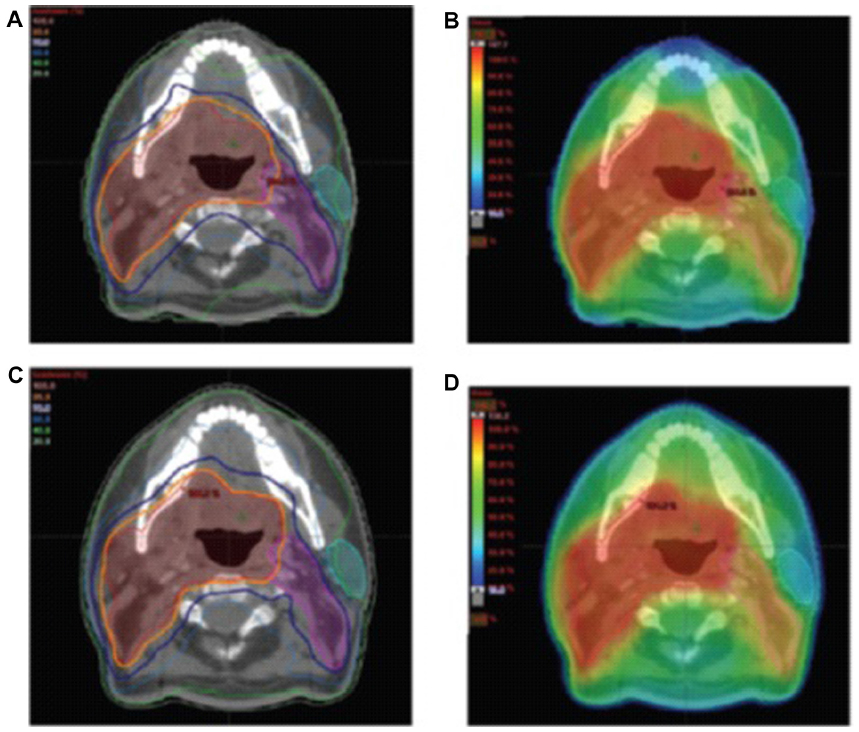 | Figure 3 An example of dose distribution in IMRT and VMAT plans for oropharyngeal cancer. |
Lung cancer
The transition from 3D-CRT to IMRT in the treatment of lung cancer has shown room for improvement regarding dosimetric parameters and normal tissue sparing.35,36
Intrafraction motion results in significant geometric and dosimetric uncertainties in radiation treatment planning and dose delivery. Many methods may be used to achieve visualization of the tumor positions during the respiratory cycle, among which are deep inspiration breath-hold techniques, respiratory gating, four-dimensional CT scanning, Active Breathing Coordinator, and marker tracking.37–39
The combination of dynamic MLC tracking and RapidArc has rendered achievable the optimization of the dose distribution to a moving target. A recent feasibility study showed promising results of tracking target motion for arc therapy associated to a dynamic multi-leaf collimator algorithm.40
Not much of the scientific literature describes VMAT use in advanced lung tumors, apart from a review which included a case report of lung cancer treated with arc therapy and which affirmed the capability of arc therapy to deliver an optimal radiotherapy treatment in the shortest time.41 A lung tumor often takes the shape of a convex hull; for this reason, the rapid delivery of VMAT is an advantage which makes this technique competitive in respect to conventional IMRT.41 Scorsetti et al42 treated 24 patients affected by unresectable locally advanced lung cancer of large volume with RapidArc; initial results of the clinical cases reported acute toxicity.
Dosimetric parameters attained with RapidArc concerning target coverage and dose homogeneity were satisfactory also in non-strongly heterogeneous regions.42 A considerable contralateral lung sparing was observed, while the maximum dose to the spinal cord was under the tolerance level. The authors considered the heart irradiation worrying, seeing as the target position was extremely cranial. RapidArc proved to be a safe and advantageous treatment modality for non-small cell lung cancer with large volumes because it diminishes acute toxicity. Long term observation of patients is needed to assess the outcome and late toxicity. VMAT technique for lung tumors might be employed both for conventional fractionated radiotherapy and for stereotactic radiotherapy. VMAT technique and non-coplanar plans with five fields showed that the higher dose comes down in normal lung tissue and, furthermore, improves target coverage compared with coplanar beams;43 this is advantageous for stereotactic radiotherapy of non-small-cell lung cancer. Very high conformal dose distributions were obtained with single-arc VMAT plans; moreover, these plans kept a high standard of control of dose distribution in OARs and a reduction in lung dosimetric parameters. VMAT is ideal for stereotactic lung radiotherapy, both for delivery efficiency and to reduce specific problems associated with intrafraction movement given that treatment time diminishes by 37%–63%.43,44 Brock et al compared dosimetric parameters of VMAT plans to 3DCT plans with three, five, seven, and nine non-coplanar fields.43 Stereotactic lung radiotherapy with non-coplanar plans with a number of beams, inclusive within five to seven, showed really good tumor coverage while minimizing the higher dose to normal lung tissue compared with coplanar beam arrangements, and VMAT was equivalent to non-coplanar plans with regard to target coverage and V20 (percentage of lung volume that receives a dose of 20 Gy), but with a shorter treatment time, although McGrath et al44 observed a better V5, V10, V12.5, and V20 in 3D conformal plans compared to VMAT plans. In McGrath et al’s study, partial arcs were used in order to avoid the contralateral lung; this could explain the considerable discrepancy with regard to the article by Brock et al.43 According to recent papers45–47 on inoperable non-small-cell lung cancer, stereotactic radiotherapy appears to be an excellent method to control disease and toxicity.
Holt et al48 delivered 54 Gy in three fractions for early-stage lung cancer and illustrated the potentiality of VMAT for stereotactic body radiotherapy treatment with comparison to IMRT technique. Utilizing coplanar arcs for early-stage lung cancer, the authors obtained high-quality dose distribution and skin dose levels similar to those of non-coplanar IMRT and a little improvement compared with coplanar IMRT. It cannot be ignored that delivery time was reduced up to 70% using VMAT. Tumor motion in lung cancer treatment is a concern with VMAT and IMRT techniques due to the interplay between tumor motion during the respiratory cycle and the movement of the MLC leaves.49
IMRT techniques have also been evaluated for malignant pleural mesothelioma. de Perrot et al evaluated adjuvant high-dose radiation therapy (up to 60 Gy) for malignant pleural mesothelioma. They used trimodality therapy (radiotherapy after surgery followed by chemotherapy), which consisted of chemotherapy with cisplatin followed by extrapleural pneumonectomy. Trimodality therapy can be considered practicable for patients with absent nodal metastasis because the results were promising; on the contrary, when there was N2 disease, the outcome of the therapy was unsuccessful.50 Arc therapy with RapidArc was studied on malignant pleural mesothelioma to examine the performance of this irradiation technique. Treatment plans with two arcs on six patients with mesothelioma were analyzed and compared with IMRT plans with nine fixed fields.51 As far as this last technique, sliding window IMRT has been considered the standard of care.
RapidArc and standard IMRT obtained comparable coverage of the target; also, the conformity index was similar for both techniques, but dose sparing was better in RapidArc. The value of MUs was reduced by one-third with RapidArc; in a similar vein, the delivery time was reduced from 13.4 minutes for IMRT to 3.7 minutes for RapidArc.51 Taking into consideration the decrease of the MUs and the time necessary to deliver treatment radiotherapy, arc therapy can be regarded as a possible alternative for patients affected with malignant pleural mesothelioma.
Prostate cancer
IMRT has been the standard technique utilized in several institutions for primary prostate radiotherapy for a long time. With the introduction of arc therapy, the transition from IMRT to VMAT techniques was short. VMAT can be ideal for prostate cancer due to the geometry of this kind of anatomical district. Localized prostate cancer was studied by Palma et al,4 who examined 3D-CRT, IMRT, and VMAT. Taking into account all dosimetric parameters, the sparing of critical organs was better with IMRT and VMAT methods compared to 3D conformal plans. The highest sparing to OAR obtained with RapidArc was borne out by a comparison with the IMRT plans. In particular, femoral head, rectum, and bladder were the organs which benefited most from the VMAT technique. Contrary to the study by Palma et al,4 Yoo et al52 found that for prostate cancer that included seminal vesicles and lymph nodes, dose sparing was better in IMRT plans for rectum, bladder, and small bowel compared to VMAT with a single arc. However, for a prostate target that included seminal vesicles and lymph nodes, RapidArc with a double arc seemed to reach the dosimetric values of the IMRT. The treatment delivery is more efficient with RapidArc. The improved OAR sparing with VMAT has been reported in other planning studies. A planning study of eleven prostate cancer patients at the Memorial Sloan Kettering Cancer Center compared five-field fixed-field IMRT (step-and-shoot) with VMAT.53 The authors saw the normal tissue improved; in particular, they reported improvements to rectal wall sparing and complication probability (normal tissue complication probability) (by 1.5%) and lower doses to the bladder wall (not statistically significant) and femoral heads. Treatment of prostate cancer was also examined by Wolff et al,54 who compared 3D-CRT, step-and-shoot IMRT, VMAT, and serial tomotherapy. All modulated techniques (tomotherapy, IMRT, and VMAT) were obviously more efficient compared to 3D-CRT. The best healthy-organ sparing was obtained with tomotherapy, but the treatment delivery was more practical with RapidArc. 3D conformal plans offered excellent tumor coverage, but caused side effects of the high dose to the rectum and bladder. Pardo-Montero and Fenwick55 compared VMAT and tomotherapy techniques for prostate cancer from the point of view of the delivery efficiency, optimization of cost function, and dependence on machines. They established that the value of tomotherapy plans is strictly conditioned by the width and pitch of the fan beam utilized in treatment delivery. The better tomotherapy plans were obtained with a 1 cm fan beam width; only in these cases were tomotherapy plans superior to VMAT plans. When the fan beam width was 2.5 cm, the results were opposite, and VMAT was superior to tomotherapy. A different study, by Wolff et al,54 compared VMAT radiotherapy with 3D-CRT, fixed-field IMRT, and serial tomotherapy. These authors reported inferior mean doses to the rectum in IMRT and serial tomotherapy compared with VMAT plans. Myrehaug et al56 compared conventional IMRT and VMAT for high-risk prostate cancer. All dosimetric data were very similar in both cases, both IMRT and VMAT had respected Radiation Therapy Oncology Group parameters for the PTV coverage, and the same applied to OAR sparing and integral doses. To get a benefit from VMAT plans, it was necessary to use two or three arcs, but even when more than one arc was used, delivery times were greater with IMRT. Tsai et al57 compared VMAT plans with helical tomotherapy and fixed-field IMRT plans and saw better conformity and superior OAR sparing with helical tomotherapy. An analogous study by Rao et al58 likened VMAT to fixed-field IMRT and helical tomotherapy. In this study, the authors found similar dosimetric values across the three techniques and comparable sparing of OARs. On the whole, most of the mentioned studies have shown satisfactory PTV coverage for VMAT, fixed-field IMRT, and tomotherapy. In the matters of homogeneity and conformity of the target volume, the results are in disagreement: some studies showed an advantage of VMAT, reporting improved conformity or homogeneity, while other studies observed better results with fixed-field IMRT. These different results could be due to many changing factors, among which are the arcs utilized in the VMAT plans (insofar as it has been possible to observe that double-arc plans can attain superior conformity and homogeneity compared with single-arc plans), the number of fields utilized in the IMRT plans, and the type of VMAT or IMRT optimization approach. Usually, each increase in the number of fields corresponds to an improvement in the plan’s quality; this could explain the higher results with fixed-field IMRT observed in the works by Yoo et al52 and Wolff et al.54
All the studies in this review have one thing in common, namely the better efficiency of VMAT delivery that reduces the treatment times. The impact of this change in treatment schedules is increased MUs and treatment time per fraction, therefore faster VMAT delivery techniques may be an attractive solution. On the other hand, the times required for optimization and dose calculation for fixed-field IMRT are briefer compared with VMAT planning. Few studies have reported clinical outcome data because of the novelty of VMAT technology. Pesce et al59 described their clinical outcomes on 45 patients treated with VMAT. There was no acute rectal toxicity (grade 2 or 3), while 12% of patients presented dysuria (grade 2) and 44% had preserved erectile function. After 6 weeks, patients reported a good biochemical response, with median PSA levels reduced to 0.4 ng/mL. Subsequent follow-up will be needed to evaluate other clinical results including late toxicity and local control and survival. More problems such as secondary malignancy induction should be examined, given that there is not sufficient information to quantify this type of risk for IMRT and VMAT techniques.
An example of dose distributions for prostate tumors with VMAT and conventional IMRT is displayed in Figure 4.
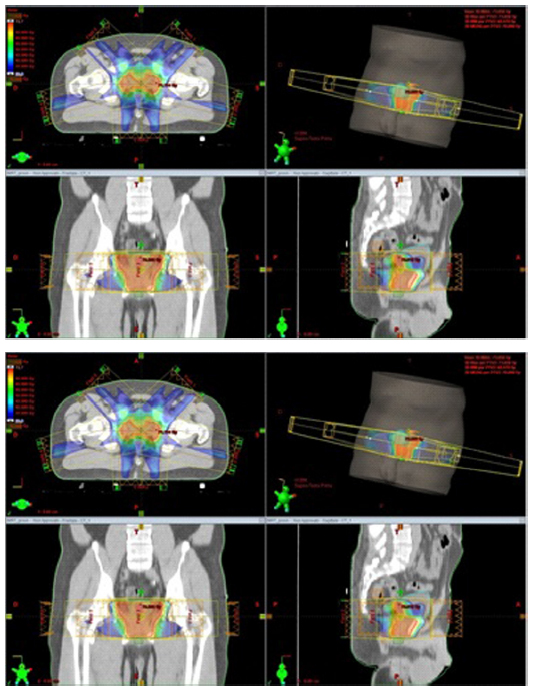 | Figure 4 An example of dose distributions achieved with VMAT and fixed-field IMRT for prostate cancer (color wash). |
Gynecological cancer
In view of the fact that RapidArc treatment in prostate cancer has achieved a positive dosimetric response, the use of Arc techniques has garnered attention and interest in the radiation treatment of other pelvic malignancies and gynecological cancers.
IMAT was the first arc therapy examined in gynecological cancers. It was used for the first time for whole abdominopelvic radiotherapy, in particular for relapsed ovarian cancer.60 Another study, by Wong et al,61 utilized the same IMAT technique for women affected with high-risk endometrial cancers. In the matter of multimodality therapy, the irradiation of the nodules and tumor bed did not go over the dose limits for OARs. IMAT produced adequate dose distributions and better dose homogeneity compared with conventional IMRT and spared OARs to the same amount, but was simpler to deliver in respect to several fixed-field IMRT techniques. A consequent development of the IMAT was the volumetric intensity-modulated arc VMAT, which led to the possibility to deliver dose distribution in the target in only one arc. The performance of the volumetric modulated arc radiotherapy on cervix uterine tumors has been evaluated by Cozzi et al.6 As a benchmark of this study, a fixed-field IMRT technique was utilized. Even though target coverage was almost the same for RapidArc and IMRT, dose distribution homogeneity was better with the VMAT treatment. RapidArc showed a further improvement in healthy-tissue sparing and in OAR avoidance as compared with conventional IMRT without jeopardizing target coverage. With the addition of the shorter treatment times, RapidArc can be considered a good technique to fully exploit for these tumor sites. Further prospective studies will be necessary to evaluate clinical results in favor of arc therapy. Wong et al61 reported that two anterior arcs were sufficient in treating the target volume satisfactorily with adequate sparing of OARs. VMAT has been considered as a next logical step given the possibility of treating the entire target volume in a single arc, which would reduce treatment delivery time. A study by Mahantshetty et al62 compared dosimetric parameters of VMAT and IMRT for whole abdomen radiotherapy after ovarian cancer. Fixed-field IMRT and RapidArc were comparable for target coverage. The homogeneity index was slightly improved with RapidArc, while the OARs were spared to a similar degree. Another study, by Matuszak et al,63 analyzed dosimetric advantages and delivery efficiency of volumetric modulated arc radiotherapy with IMRT and 3D-CRT. Both studies showed acceptable PTV coverage, with a decrease in MUs and treatment times, much to the advantage of RapidArc.
The shortened treatment time may reduce the impact of intrafraction motion, which may be significant in intraabdominal radiotherapy.
Other tumors
RapidArc has been employed for tumors in several other parts of the body, eg, in total-marrow irradiation,64–66 pancreatic malignancies,67 and breast cancer.65–67 In these studies, it was a common finding that RapidArc was more efficient for dose delivery, while with regard to treatment planning and dose conformity, RapidArc provided considerable added value. These studies emphasize that RapidArc and, in wider terms, VMAT techniques can be considered a possible alternative to traditional irradiation methods for the cure of several cancers.
Discussion
What sets apart VMAT with RapidArc from earlier irradiation techniques such as helical tomotherapy, IMAT, or IMRT is the opportunity to deliver dose distribution for the entire volume and not only slice by slice. In addition to this, the treatment planning algorithm guarantees highly accurate dose delivery and therefore great healthy-tissue sparing.
Examining treatment plans from various points of view, a VMAT plan gives similar or better quality target volume coverage by comparison with other treatment techniques. Nevertheless, it still remains a controversial issue with respect to OAR and healthy-tissue sparing or integral dose. The most significant observation of this study is the difference in terms of MUs and treatment time required to deliver the prescription dose daily between VMAT and IMRT. VMAT delivers significantly less MUs per treatment session compared with IMRT. Treatment time (including mode-up time) was significantly less with VMAT as compared to IMRT. Only a small number of scientific studies have examined clinical results and toxicity after VMAT. All the studies reviewed have shown that VMAT improves efficiency of delivery with reduced MUs and delivery time compared to conventional IMRT. The lower MUs in VMAT delivery may potentially reduce the risk of radiation-induced cancers, which needs to be validated by long-term studies. Few studies have reported on the toxicity and clinical outcomes of VMAT compared to IMRT. In general, VMAT is a safe and efficient treatment modality for various cancer types. The significant difference between VMAT and fixed-field IMRT is the reduction in MUs and treatment delivery time, which was an almost universal finding in all the planning studies. There are inherent limitations with these planning studies. Even if the same strict planning objectives and calculation algorithms were used, it is extremely difficult to completely eliminate planner bias, especially if multiple planners are involved in the process. Direct comparisons between different studies are not possible because of significant differences in target volume definitions, dose prescriptions, and treatment schedules. VMAT gives an optimal treatment delivery for lots of tumors; nevertheless, treatment plan optimization and dose calculation are more complex and need a longer planning time. Compared to tomotherapy, VMAT using a standard linear accelerator, permits the elasticity to employ the other features of the linear accelerators (the use of electrons and different energies of photons) for other patients who do not necessitate VMAT. However, tomotherapy has the benefit of integrating CT imaging for setup verification, consenting the IGRT, without the supplement of other technologies. Linear accelerators do not have an inherent CT scanning capability, but can be done using a cone-beam CT, which is mounted to the linear accelerator19 or other on-board X-ray imaging devices. One uncertainty regards the low dose in the normal tissue, which tends to increase with IMRT and VMAT; this supposedly increases the risk of secondary malignancy. In any case, further follow-up of patients of these techniques will be necessary to quantify this risk.
Conclusion
Few studies are related to clinical outcome data; most of the published literature involves dosimetric planning data. But VMAT is a new technology, and the numbers of patients treated is growing and clinical data will increase. Most dosimetric studies of various tumor sites compared VMAT with 3D-CRT techniques and fixed-field IMRT.
The resemblances between VMAT and IMRT are not unexpected, considering that VMAT is a development of IMRT. The principal difference is the significant reduction in delivery time and MUs in favor of VMAT, as the reviewed studies have shown. Comparisons across various studies are difficult to do due to important divergences in target volume definitions, different dose prescriptions, and doses delivered. Furthermore, in IMRT and VMAT, the numbers of fields or arcs and the gantry angles can be different; for these reasons, the data on target coverage and healthy-organ sparing can deeply differ across studies.
RapidArc has a strong and growing role in the treatment of several tumors, but it cannot be considered the solution to all clinical cases. Each clinical case must be evaluated on an individual basis, choosing the most favorable radiation technique that will give the most suitable outcomes.
Disclosure
The author reports no conflicts of interest in this work.
References
LoSasso T, Chui CS, Ling CC. Comprehensive quality assurance for the delivery of intensity modulated radiotherapy with a multileaf collimator used in the dynamic mode. Med Phys. 2001;28:2209–2219. | |
Yu CX, Li XA, Ma L, et al. Clinical implementation of intensity-modulated arc therapy. Int J Radiat Oncol Biol Phys. 2002;53:453–463. | |
Yu CX. Intensity-modulated arc therapy with dynamic multileaf collimation: an alternative to tomotherapy. Phys Med Biol. 1995;40:1435–1449. | |
Palma D, Vollans E, James K, et al. Volumetric modulated arc therapy for delivery of prostate radiotherapy: comparison with intensity-modulated radiotherapy and three-dimensional conformal radiotherapy. Int J Radiat Oncol Biol Phys. 2008;72:996–1001. | |
Clivio A, Fogliata A, Franzetti-Pellanda A, et al. Volumetric-modulated arc radiotherapy for carcinomas of the anal canal: a treatment planning comparison with fixed field IMRT. Radiother Oncol. 2009;92:118–124. | |
Cozzi L, Dinshaw KA, Shrivastava SK, et al. A treatment planning study comparing volumetric arc modulation with RapidArc and fixed field IMRT for cervix uteri radiotherapy. Radiother Oncol. 2008;89:180–191. | |
Shaffer R, Nichol AM, Vollans E, et al. A comparison of volumetric modulated arc therapy and conventional intensity-modulated radiotherapy for frontal and temporal high-grade gliomas. Int J Radiat Oncol Biol Phys. 2010;76:1177–1184. | |
Verbakel WF, Cuijpers JP, Hoffmans D, Bieker M, Slotman BJ, Senan S. Volumetric intensity-modulated arc therapy vs. conventional IMRT in head-and-neck cancer: a comparative planning and dosimetric study. Int J Radiat Oncol Biol Phys. 2009;74:252–259. | |
Vanetti E, Clivio A, Nicolini G, et al. Volumetric modulated arc radiotherapy for carcinomas of the oro-pharynx, hypo-pharynx and larynx: a treatment planning comparison with fixed field IMRT. Radiother Oncol. 2009;92:111–117. | |
Murthy V, Gupta T, Kadam A, et al. Time trial: a prospective comparative study of the time-resource burden for three-dimensional conformal radiotherapy and intensity-modulated radiotherapy in head and neck cancers. J Cancer Res Ther. 2009;5:107–112. | |
Miles EA, Clark CH, Urbano MT, et al. The impact of introducing intensity modulated radiotherapy into routine clinical practice. Radiotherapy Oncol. 2005;77:241–246. | |
Hoogeman MS, Nuyttens JJ, Levendag PC, Heijmen BJ. Time dependence of intrafraction patient motion assessed by repeat stereoscopic imaging. Int J Radiat Oncol Biol Phys. 2008;70:609–618. | |
Yang W, Van Ausdal R, Read P, Larner J, Benedict S, Sheng K. The implication of non-cyclic intrafractional longitudinal motion in SBRT by TomoTherapy. Phys Med Biol. 2009;54:2875–2884. | |
Wang JZ, Li XA, D’Souza WD, Stewart RD. Impact of prolonged fraction delivery times on tumor control: a note of caution for intensity-modulated radiation therapy (IMRT). Int J Radiat Oncol Biol Phys. 2003;57:543–552. | |
Fowler JF, Welsh JS, Howard SP. Loss of biological effect in prolonged fraction delivery. Int J Radiat Oncol Biol Phys. 2004;59:242–249. | |
Bewes JM, Suchowerska N, Jackson M, Zhang M, McKenzie DR. The radiobiological effect of intra-fraction dose-rate modulation in intensity modulated radiation therapy (IMRT). Phys Med Biol. 2008;53:3567–3578. | |
Moiseenko V, Duzenli C, Durand RE. In vitro study of cell survival following dynamic MLC intensity-modulated radiation therapy dose delivery. Med Phys. 2007;34:1514–1520. | |
Sterzing F, Münter MW, Schäfer M, et al. Radiobiological investigation of dose-rate effects in intensity-modulated radiation therapy. Strahlenther Onkol. 2005;181:42–48. | |
Verbakel WF, Senan S, Cuijpers JP, Slotman BJ, Lagerwaard FJ. Rapid delivery of stereotactic radiotherapy for peripheral lung tumors using volumetric intensity-modulated arcs. Radiother Oncol. 2009;93:122–124. | |
Wu QJ, Yoo S, Kirkpatrick JP, Thongphiew D, Yin FF. Volumetric arc intensity-modulated therapy for spine body radiotherapy: comparison with static intensity-modulated treatment. Int J Radiat Oncol Biol Phys. 2009;75:1596–1604. | |
Davidson MT, Masucci GL, Follwell M, et al. Single arc volumetric modulated arc therapy for complex brain gliomas: is there an advantage as compared to intensity modulated radiotherapy or by adding a partial arc? Technol Cancer Res Treat. 2012;11:211–220. | |
Fogliata A, Clivio A, Nicolini G, Vanetti E, Cozzi L. Intensity modulation with photons for benign intracranial tumors: a planning comparison of volumetric single arc, helical arc and fixed gantry techniques. Radiother Oncol. 2008;89:254–262. | |
Wagner D, Christiansen H, Wolff H, Vorwerk H. Radiotherapy of malignant gliomas: comparison of volumetric single arc technique (RapidArc), dynamic intensity-modulated technique and 3D conformal technique. Radiother Oncol. 2009;93:593–596. | |
Lagerwaard FJ, van der Hoorn EA, Verbakel WF, Haasbeek CJ, Slotman BJ, Senan S. Whole-brain radiotherapy with simultaneous integrated boost to multiple brain metastases using volumetric modulated arc therapy. Int J Radiat Oncol Biol Phys. 2009;75:253–259. | |
Clark GM, Popple RA, Young PE, Fiveash JB. Feasibility of single-isocenter volumetric modulated arc radiosurgery for treatment of multiple brain metastases. Int J Radiat Oncol Biol Phys. 2010;76:296–302. | |
Hsu F, Carolan H, Nichol A, et al. Whole brain radiotherapy with hippocampal avoidance and simultaneous integrated boost for 1–3 brain metastases: a feasibility study using volumetric modulated arc therapy. Int J Radiat Oncol Biol Phys. 2010;76:1480–1485. | |
Awad R, Fogarty G, Hong A, et al. Hippocampal avoidance with volumetric modulated arc therapy in melanoma brain metastases – the first Australian experience. Radiat Oncol. 2013;8:62. | |
Bertelsen A, Hansen CR, Johansen J, Brink C. Single arc volumetric modulated arc therapy of head and neck cancer. Radiother Oncol. 2010;95:142–148. | |
Johnston M, Clifford S, Bromley R, Back M, Oliver L, Eade T. Volumetric-modulated arc therapy in head and neck radiotherapy: a planning comparison using simultaneous integrated boost for nasopharynx and oropharynx carcinoma. Clin Oncol (R Coll Radiol). 2011;23:503–511. | |
Stieler F, Wolff D, Schmid H, Welzel G, Wenz F, Lohr F. A comparison of several modulated radiotherapy techniques for head and neck cancer and dosimetric validation of VMAT. Radiother Oncol. 2011;101:388–393. | |
Lu SH, Cheng JC, Kuo SH, et al. Volumetric modulated arc therapy for nasopharyngeal carcinoma: a dosimetric comparison with TomoTherapy and step-and-shoot IMRT. Radiother Oncol. 2012;104:324–330. | |
Neubauer E, Dong L, Followill DS, et al. Assessment of shoulder position variation and its impact on IMRT and VMAT doses for head and neck cancer. Radiat Oncol. 2012;7:19. | |
Oliver M, McConnell D, Romani M, et al. Evaluation of the trade-offs encountered in planning and treating locally advanced head and neck cancer: intensity-modulated radiation therapy vs dual-arc volumetric-modulated arc therapy. Br J Radiol. 2012;85:1539–1545. | |
Murshed H, Liu HH, Liao Z, et al. Dose and volume reduction for normal lung using intensity-modulated radiotherapy for advanced-stage non-small-cell lung cancer. Int J Radiat Oncol Biol Phys. 2004;58:1258–1267. | |
Lee TF, Ting HM, Chao PJ, Fang FM. Dual arc volumetric-modulated arc radiotherapy (VMAT) of nasopharyngeal carcinomas: a simultaneous integrated boost treatment plan comparison with intensity-modulated radiotherapies and single arc VMAT. Clin Oncol (R Coll Radiol). 2012;24:196–207. | |
Chapet O, Khodri M, Jalade P, et al. Potential benefits of using non coplanar field and intensity modulated radiation therapy to preserve the heart in irradiation of lung tumors in the middle and lower lobes. Radiother Oncol. 2006;80:333–340. | |
Keall P. 4-dimensional computed tomography imaging and treatment planning. Semin Radiat Oncol. 2004;14:81–90. | |
McNair HA, Brock J, Symonds-Tayler JR, et al. Feasibility of the use of the Active Breathing Co ordinator (ABC) in patients receiving radical radiotherapy for non-small cell lung cancer (NSCLC). Radiother Oncol. 2009;93:424–429. | |
Suh Y, Weiss E, Zhong H, Fatyga M, Siebers JV, Keall PJ. A deliverable four-dimensional intensity-modulated radiation therapy-planning method for dynamic multileaf collimator tumor tracking delivery. Int J Radiat Oncol Biol Phys. 2008;71:1526–1536. | |
Zimmerman J, Korreman S, Persson G, et al. DMLC motion tracking of moving targets for intensity modulated arc therapy treatment: a feasibility study. Acta Oncol. 2009;48:245–250. | |
Bedford JL, Nordmark Hansen V, McNair HA, et al. Treatment of lung cancer using volumetric modulated arc therapy and image guidance: a case study. Acta Oncol. 2008;47:1438–1443. | |
Scorsetti M, Navarria P, Mancosu P, et al. Large volume unresectable locally advanced non-small cell lung cancer: acute toxicity and initial outcome results with rapid arc. Radiat Oncol. 2010;5:94. | |
Brock J, Bedford J, Partridge M, et al. Optimising stereotactic body radiotherapy for non-small cell lung cancer with volumetric intensity-modulated arc therapy – a planning study. Clin Oncol (R Coll Radiol). 2012;24:68–75. | |
McGrath SD, Matuszak MM, Yan D, Kestin LL, Martinez AA, Grills IS. Volumetric modulated arc therapy for delivery of hypofractionated stereotactic lung radiotherapy: a dosimetric and treatment efficiency analysis. Radiother Oncol. 2010;95:153–157. | |
Timmerman R, Paulus R, Galvin J, et al. Stereotactic body radiation therapy for inoperable early stage lung cancer. JAMA. 2010;303:1070–1076. | |
Videtic GM, Stephans K, Reddy C, et al. Intensity-modulated radiotherapy-based stereotactic body radiotherapy for medically inoperable early-stage lung cancer: excellent local control. Int J Radiat Oncol Biol Phys. 2010;77:344–349. | |
Stephans KL, Djemil T, Reddy CA, et al. A comparison of two stereotactic body radiation fractionation schedules for medically inoperable stage I non-small cell lung cancer: the Cleveland Clinic experience. J Thorac Oncol. 2009;4:976–982. | |
Holt A, van Vliet-Vroegindeweij C, Mans A, Belderbos JS, Damen EM. Volumetric-modulated arc therapy for stereotactic body radiotherapy of lung tumors: a comparison with intensity-modulated radiotherapy techniques. Int J Radiat Oncol Biol Phys. 2011;81:1560–1567. | |
Bortfeld T, Jokivarsi K, Goitein M, Kung J, Jiang SB. Effects of intra-fraction motion on IMRT dose delivery: statistical analysis and simulation. Phys Med Biol. 2002;47:2203–2220. | |
de Perrot M, Feld R, Cho BC, et al. Trimodality therapy with induction chemotherapy followed by extrapleural pneumonectomy and adjuvant high-dose hemithoracic radiation for malignant pleural mesothelioma. J Clin Oncol. 2009;27:1413–1418. | |
Scorsetti M, Bignardi M, Clivio A, et al. Volumetric modulation arc radiotherapy compared with static gantry intensity-modulated radiotherapy for malignant pleural mesothelioma tumor: a feasibility study. Int J Radiat Oncol Biol Phys. 2010;77:942–949. | |
Yoo S, Wu QJ, Lee WR, Yin FF. Radiotherapy treatment plans with RapidArc for prostate cancer involving seminal vesicles and lymph nodes. Int J Radiat Oncol Biol Phys. 2010;76:935–942. | |
Zhang P, Happersett L, Hunt M, Jackson A, Zelefsky M, Mageras G. Volumetric modulated arc therapy: planning and evaluation for prostate cancer cases. Int J Radiat Oncol Biol Phys. 2010;76:1456–1462. | |
Wolff D, Stieler F, Welzel G, et al. Volumetric modulated arc therapy (VMAT) vs serial tomotherapy, step-and-shoot IMRT and 3D-conformal RT for treatment of prostate cancer. Radiother Oncol. 2009;93:226–233. | |
Pardo-Montero J, Fenwick JD. Tomotherapy-like versus VMAT-like treatments: a multicriteria comparison for a prostate geometry. Med Phys. 2012;39:7418–7429. | |
Myrehaug S, Chan G, Craig T, et al. A treatment planning and acute toxicity comparison of two pelvic nodal volume delineation techniques and delivery comparison of intensity-modulated radiotherapy versus volumetric modulated arc therapy for hypofractionated high-risk prostate cancer radiotherapy. Int J Radiat Oncol Biol Phys. 2012;82:e657–e662. | |
Tsai CL, Wu JK, Chao HL, Tsai YC, Cheng JC. Treatment and dosimetric advantages between VMAT, IMRT, and helical tomotherapy in prostate cancer. Med Dosim. 2011;36:264–271. | |
Rao M, Yang W, Chen F, et al. Comparison of Elekta VMAT with helical tomotherapy and fixed field IMRT: plan quality, delivery efficiency and accuracy. Med Phys. 2010;37:1350–1359. | |
Pesce GA, Clivio A, Cozzi L, et al. Early clinical experience of radiotherapy of prostate cancer with volumetric modulated arc therapy. Radiat Oncol. 2010;5:54. | |
Duthoy W, De Gersem W, Vergote K, et al. Whole abdominopelvic radiotherapy (WAPRT) using intensity-modulated arc therapy (IMAT): first clinical experience. Int J Radiat Oncol Biol Phys. 2003;57:1019–1032. | |
Wong E, D’Souza DP, Chen JZ, et al. Intensity-modulated arc therapy for treatment of high-risk endometrial malignancies. Int J Radiat Oncol Biol Phys. 2005;61:830–841. | |
Mahantshetty U, Jamema S, Engineer R, et al. Whole abdomen radiation therapy in ovarian cancers: a comparison between fixed beam and volumetric arc based intensity modulation. Radiat Oncol. 2010;5:106. | |
Matuszak MM, Yan D, Grills I, Martinez A. Clinical applications of volumetric modulated arc therapy. Int J Radiat Oncol Biol Phys. 2010;77:608–616. | |
Aydogan B, Yeginer M, Kavak GO, Fan J, Radosevich JA, Gwe-Ya K. Total marrow irradiation with RapidArc volumetric arc therapy. Int J Radiat Oncol Biol Phys. 2011;81:592–599. | |
Mancosu P, Navarria P, Castagna L, et al. Anatomy driven optimization strategy for total marrow irradiation with a volumetric modulated arc therapy technique. J Appl Clin Med Phys. 2012;13:3653. | |
Surucu M, Yeginer M, Kavak GO, Fan J, Radosevich JA, Aydogan B. Verification of dose distribution for volumetric modulated arc therapy total marrow irradiation in a humanlike phantom. Med Phys. 2012;39:281–288. | |
Ali AN, Dhabaan AH, Jarrio CS, Siddiqi AK, Landry JC. Dosimetric comparison of volumetric modulated arc therapy and intensity-modulated radiation therapy for pancreatic malignancies. Med Dosim. 2012;37:271–275. | |
Bauman G, Yartsev S, Rodrigues G, et al. A prospective evaluation of helical tomotherapy. Radiat Oncol. 2007;68(2):632–641. | |
Bijdekerke P, Verellen D, Tournel K, et al TomoTherapy: Implications on daily workload and scheduling patients. Radiother Oncol. 2008;86(2):224–230. | |
Cozzarini C, Fiorino C, Di Muzio N, et al. Hypofractionated adjuvant radiotherapy with helical Tomotherapy after radical prostatectomy: Planning data and toxicity results of a Phase I-II study. Radiother Oncol. 2008;88(1):26–33. | |
Fuss M, Shi C, Papanikolaou N. Tomotherapeutic stereotactic body radiation therapy: Techniques and comparison between modalities. Acta Oncologica. 2006;45(7):953–960. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.