")
Back to Journals » Drug, Healthcare and Patient Safety » Volume 14
Clinical Utility and Tolerability of Tolvaptan in the Treatment of Autosomal Dominant Polycystic Kidney Disease (ADPKD)
Authors Raina R, Houry A , Rath P, Mangat G, Pandher D, Islam M, Khattab AG, Kalout JK , Bagga S
Received 18 January 2022
Accepted for publication 22 August 2022
Published 8 September 2022 Volume 2022:14 Pages 147—159
DOI https://doi.org/10.2147/DHPS.S338050
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hemalkumar B Mehta
Rupesh Raina,1– 3 Ahmad Houry,1,3 Pratik Rath,1 Guneive Mangat,1 Davinder Pandher,1,4 Muhammad Islam,3 Ala’a Grace Khattab,3 Joseph K Kalout,1 Sumedha Bagga5
1Akron Nephrology Associates/Cleveland Clinic Akron General Medical Center, Akron, OH, USA; 2Department of Nephrology, Akron Children’s Hospital, Akron, OH, USA; 3College of Medicine, Northeast Ohio Medical University, Rootstown, OH, USA; 4Mount Sinai South Nassau, Oceanside, NY, 11570, USA; 5Questrom School of Business, Boston University, Boston, MA, USA
Correspondence: Rupesh Raina, Consultant Nephrologist, Adult-Pediatric Kidney Disease/Hypertension, Akron Nephrology Associates/Cleveland Clinic Akron General Medical Center, Akron, OH, USA, Tel +1 330-543-8950, Fax +1 330-543-3980, Email [email protected]; [email protected]
Abstract: Autosomal dominant polycystic kidney disease, also known as ADPKD, is the most common hereditary kidney disease, affecting different age groups. ADPKD can eventually lead to end-stage renal disease. The etiology of ADPKD is genetic, resulting in the formation of cysts containing fluids on the kidneys. Patients with ADPKD present a range of symptoms following a decline in kidney function. Pain, stones, proteinuria and osteoporosis are few of the many symptoms, resulting from decreased kidney function. Tolvaptan, a selective V2 receptor antagonist, is the etiological treatment used for ADPKD. In this paper, we conducted a systematic review of the literature between 2011 and 2021 to gather data regarding the tolerability and efficacy of tolvaptan use in ADPKD. A total of 22 trials were reviewed. Tolvaptan efficacy in the trials was measured using changes in eGFR or changes in total kidney volume. Results showed that tolvaptan use in ADPKD was associated with a slower decline in kidney function and a decrease in total kidney volume. Side effects of this drug include polyuria, nocturia and polydipsia along with hepatotoxicity. The two biggest trials, TEMPO and REPRISE, change in eGFR from pre-treatment baseline to post-treatment was 1.3 mL/min/1.73 for REPRISE and 1 mL/min/1.73 for TEMPO 3:4. A mean decrease of 49% in total kidney volume from baseline to post-treatment was found in the TEMPO 3:4 study.
Keywords: ADPKD, tolvaptan
Introduction
Autosomal dominant polycystic kidney disease (ADPKD) is a common hereditary kidney disease. The prevalence of ADPKD ranges between 1/1000 and 1/250.1 ADPKD is characterized by several cysts present in the kidneys and has a variable age of onset, with symptoms typically starting around age 30–40 years. ADPKD is a progressive disorder and clinical presentation is variable. Kidney cysts, back pain, and headache are the most common presentations noted in ADPKD. However, in some cases, cysts are also prevalent in other organs like the liver and pancreas. Additionally, urinary tract infections, hypertension, renal stones, and brain aneurysms have been reported in patients with ADPKD. Cyst growth can eventually affect all the kidney functions leading to anemia, cardiovascular risk, secondary hyperparathyroidism, and bone disease. ADPKD is the leading cause of end-stage renal disease (ESRD) and the most common inherited kidney disease in the United States.2 According to the US Renal Data System, 32.9 patients per million citizens in America start dialysis as a result of renal cystic disease. One in 10 patients with ADPKD progress to ESRD.3
Unsatisfactory outcomes for patients with ADPKD have motivated researchers to examine novel tools for diagnosis and treatment. Traditionally, ultrasound was the main investigation to determine cysts of 10 mm in size or greater. In recent times, MRI and CT with contrast are used due to their ability to detect 2- or 3-mm cysts. Therefore, using CT and MRI early on in younger individuals who have atypical kidney presentation can have a drastic impact on future prognosis. Along with the early detection of cysts, different therapies have emerged to control the complications of ADPKD (hypertension, anemia, bone disease) including the vasopressin V2 receptor antagonist, tolvaptan, and oral vasopressin V2-receptor antagonist. Many trials report that the use of tolvaptan in patients with ADPKD has a positive impact on the kidneys by slowing the increase in total kidney volume and reducing the decline of glomerular filtration rate.1 Prospective studies suggest that therapy with tolvaptan in ADPKD prolonged the time to ESKD by 6.5 years, and increased life expectancy by 2.5 years. In this paper, we briefly describe the current understanding of ADPKD, followed by a description of pharmacological characteristics and adverse effects of tolvaptan, and review the results of different studies.
ADPKD Genetics
ADPKD is inherited in an autosomal dominant pattern. The most common gene defects are observed in PKD1, which encodes polycystin-1 on chromosome 16, and PKD2, which encodes polycystin-2 on chromosome 4. Although less likely, mutations in GANAB, encoding the glucosidase II alpha subunit, ALG9, or DNAJB11 gene have also been reported.4 PKD1 is more common than PKD2 and, in fact, is more symptomatic and demonstrates faster progression as compared to PKD2.4
Manifestations
There are a host of gross pathophysiologic effects of ADPKD that develop. Hypertension is a common outcome in this group of patients with increased anatomical size bilaterally and decreased kidney function in terms of filtration. The increased kidney size presents both acute and chronic pain. Acute pain can be a result of both infected kidney cysts and kidney stones. The decrease in kidney filtration measured by glomerular filtration rate (GFR) can lead to secondary osteomalacia, secondary osteoporosis, secondary hyperparathyroidism, anemia, cardiovascular disease secondary to hypertension, and valvular heart disease.1
Hematuria, renal stones (uric acid stones are more common because of lower pH), recurrent urinary tract infections, and proteinuria are some of the other renal manifestations seen in ADPKD. Over time, with repeated insults to the kidney and renal cysts increase in size and number, autosomal dominant polycystic kidney disease (ADPKD) progresses to end-stage renal disease (ESRD). In addition to intrarenal pathology, extrarenal cysts can be seen in the pancreas, liver, spleen, and epididymis.
Pathophysiology
The biggest risk factor for the development of autosomal dominant polycystic kidney disease is mutations in the genes PKD1 and PKD2, which encodes polycystin-1 and polycystin-2, respectively.5,6 For ADPKD to manifest, mutations in PKD1 and PKD2 alone are not enough. There must be a second hit involving another mutation causing tubular proliferation and cyst development prior to the symptomatic onset of ADPKD.7 The second hit is thought to occur through somatic mutation on PKD-1 or PKD-2 opposite to the inherited first mutation.8
Polycystin protein’s primary function is to develop vascular and tubular infrastructures in the kidney and other organs by controlling calcium transport across the membrane.6 This process is achieved by a variety of secondary messengers and growth factors, including cAMP, adenosine, epidermal growth factor and insulin growth factor. Extracellular signal regulated kinase (ERK) and mammalian target of rapamycin (mTOR) control and regulate the proliferative stage of the cysts.9,10 The epithelial cell proliferation causing increased cyst size and fluid accumulation are both processes mediated by an increase in cAMP when stimulated by anti-diuretic hormone (ADH).5,6 Eventually, cysts become so large that they become an autonomous unit. Drugs acting on V2 ADH receptors and consequently decreasing cAMP levels are the target treatment mechanism for ADPKD.
Pharmacodynamics and Pharmacokinetics of Tolvaptan
Tolvaptan, a selective V2 receptor antagonist, was developed to reduce cAMP levels and slow down the initiation and progression of ADPKD. Tolvaptan has twice the affinity for the V2 receptor compared with native arginine ADH and is 29 times more attracted to V2 compared to the V1A receptor. It is the only FDA approved drug for the treatment of ADPKD.11
Once in the body, tolvaptan is rapidly absorbed with 40% oral bioavailability. It was shown that tolvaptan is minimally affected by food and is dose dependent. Steady state concentration plateaus at 300 mg after absorption. Tolvaptan binds to plasma protein and undergoes hepatic metabolism through Cytochrome p450. The half-life of tolvaptan is 12 hours and is excreted via the fecal route. Pharmacokinetic and pharmacodynamic properties of tolvaptan are not very well studied. Most studies showed that tolvaptan cannot be used in patients with creatinine values <10 mg/dL. Also, tolvaptan is associated with drug–drug interactions when other drugs use the Cytochrome p450 (CYP 3A4) system at the same time. The use of CYP 3A4 inducers or inhibitors are contraindicated when administering tolvaptan due to their effect on tolvaptan hepatic metabolism.
Once at the level of the kidney, V2 receptor antagonism by tolvaptan in the renal collecting ducts causes a variety of physiological changes, which impact the pathophysiology of the ADPKD. It causes free water excretion resulting in net body fluid loss, increases Na+ concentration in the serum and decreases urine osmolality.11 Furthermore, V2 antagonism decreases cAMP which decreases cyst proliferation and helps to slow down the progression of ADPKD.
Trials and Studies
Tolvaptan is currently FDA-approved for use only in adults. Twenty-two studies have been conducted on the efficacy of tolvaptan between 2011 and 2021. These studies showed that tolvaptan slowed the increase in total kidney volume and decline in estimated glomerular filtration rate in patients with ADPKD. The safety and efficacy of tolvaptan has been studied in the two largest clinical trials done on patients with ADPKD: TEMPO3:4 and REPRISE. Both showed a reduction in the decline of kidney function compared to placebo. In fact, the change in eGFR from pre-treatment baseline to post-treatment was 1.3 mL/min/1.73 for REPRISE and 1 mL/min/1.73 for TEMPO 3:4. A mean decrease of 49% in total kidney volume from baseline to post-treatment was found in the TEMPO 3:4 study.
TEMPO 3:4, was a randomized clinical trial targeting patients aged 18 to 50 years-old with ADPKD. Participants (n = 1445), with total kidney volume of >750 mL and a creatinine clearance >60 mL/min, were randomly assigned to receive either placebo or tolvaptan for 3-years. Tolvaptan was administered at a dose of 45 mg in the morning and 15 mg in the afternoon, followed by dose escalation. The primary outcome was the percent change in total kidney volume. The change in total kidney volume was 9.6% and 18.8% with tolvaptan and placebo, respectively. Patients receiving tolvaptan had fewer episodes of kidney pain as well as a lower rate of worsening of kidney function, as measured by increase in serum creatinine and change in eGFR. Following tolvaptan therapy, the mean increase in serum creatinine was 0.16 mg/dl vs 0.23 mg/dl with placebo. The yearly eGFR slope change was −2.72mL/min/1.73 m2 in the tolvaptan group and −3.70 mL/min/1.73 m2 in those receiving placebo. Patients receiving tolvaptan also showed a significant reduction in albuminuria. TEMPO 4:4 studied the long-term effect of tolvaptan by following 871 patients who completed TEMPO 3:4. The patients received 45, 60, 90 mg doses in the morning and 15 or 30 mg dose 9-hours later, for the next 24 months. The change in the total kidney volume from TEMPO 3:4 to TEMPO 4:4 after 24 months was 29.9% and 31.6% in patients receiving tolvaptan and placebo, respectively (P = not significant). The change in eGFR during TEMPO 4:4 was −3.26% per year with early treatment during TEMPO 3:4 and −3.14% per year with delayed treatment, with no significant eGFR changes following long-term tolvaptan therapy. While therapy with tolvaptan was effective in the short term in slowing the increase in total kidney volume and correcting renal function, the kidney function was maintained in the long term13 (Figures 1–3).
 |
Figure 1 Change in eGFR in tolvaptan vs placebo groups. |
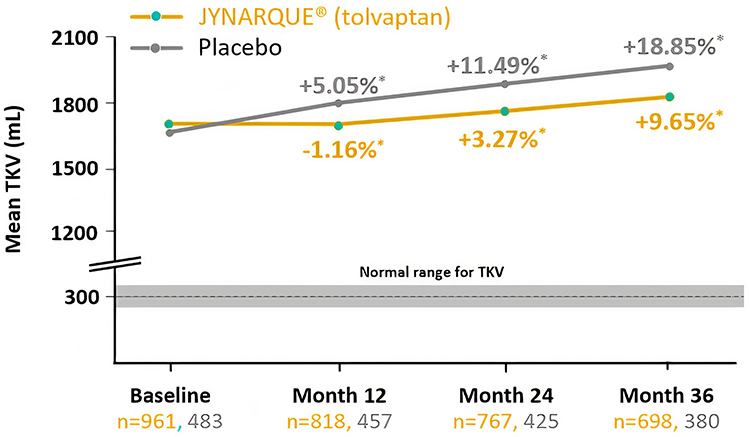 |
Figure 2 Change in total kidney volume (TEMPO 3:4). Note: *Percent change from baseline. |
 |
Figure 3 Summary of tolvaptan efficacy and safety of the 2 largest trials. |
The REPRISE trial included patients 18 to 55 years old with baseline eGFR 25–65 mL/min/1.73 m2 and patients 56 to 65 years-old with eGFR 25–44 mL/min/1.73 m2 and eGFR decline of more than 2 mL/min/1.73 m2 per year. Participants received either tolvaptan or placebo for 12 months; tolvaptan doses were 60 or 90 mg in the morning and 30 mg in the afternoon. At 1-year-follow up, the results showed that the mean change in eGFR was −2.34 mL/min/1.73 m2 in the tolvaptan treated patients, and −3.61 mL/min/1.73 m2 in those administered placebo. The changes were observed in all groups, except in the non-white, more than 55-yr-old or participants with early CKD.13 The use of tolvaptan was found to reduce the decline in kidney function compared to placebo (Figures 1 and 3).
Besides these trials, a number of studies have been conducted on the efficacy and safety of tolvaptan in patients with ADPKD. Irazabal et al followed the progression of ADPKD in 20 participants, 18–60 years old, who were given tolvaptan, 45 mg in the morning and 15 mg 8-hr later 7 days. While there was no significant change in eGFR before and after treatment, total kidney volume and cyst volume were significantly reduced by 3.1% and 1.6%, respectively.14 In another study by Boertien et al, 27 patients with ADPKD received therapy with tolvaptan for 3-weeks, followed by an observation period of 3-weeks. While there was a significant decrease in GFR at 3 weeks following treatment (median −5.4%), this change was not maintained in the 3-weeks following stoppage of medication.15
Horie et al and Muto et al specifically studied the Japanese patients in the TEMPO trial. In the former study, of 92 patients with ADPKD who were administered tolvaptan, 37 responded to the treatment with decrease in total kidney volume (−8.33%) compared to 55 patients with increasing total kidney volume (13.95%). However, for both groups, eGFR decline was significantly slowed.16 Muto et al (n = 118 participants) showed that the change in total kidney volume was 1.3% in patients receiving tolvaptan compared to 5% receiving placebo. The change in was −3.83 mL/min/1.73 m2 in the tolvaptan group vs −5.05 mL/min/1.73 m2 in the placebo groups.17
The next set of studies examined the long-term effects of tolvaptan administration in patients with ADPKD. Administration of tolvaptan had a beneficial long-term outcome by slowing the decrease in eGFR and decreasing total kidney volume. Bennett et al showed that treatment with tolvaptan delayed progression of ADPKD to ESKD by 5-years (57 years in tolvaptan group; 52 years in placebo group).18 Edwards et al (2018) followed 97 patients of ADPKD treated with tolvaptan and followed for an average of 4.6 years (1–11 years). The eGFR decline was lower in patients taking tolvaptan (−1.97 mL/min/1.73 m2) compared to placebo (−3.5 mL/min/1.73 m2).19 Finally, Higashihara et al followed 51 subjects with ADPKD who were administered tolvaptan for 3 years. The kidney total volume was significantly increased in the control group (5.8%) compared to the tolvaptan treated patients (1.7%). The annual eGFR decline was also greater in the placebo group (−2.1 mL/min/1.73 m2) vs tolvaptan (−0.71 mL/min/1.73 m2)20 (Table 1, Figure 1).
 |  |  | 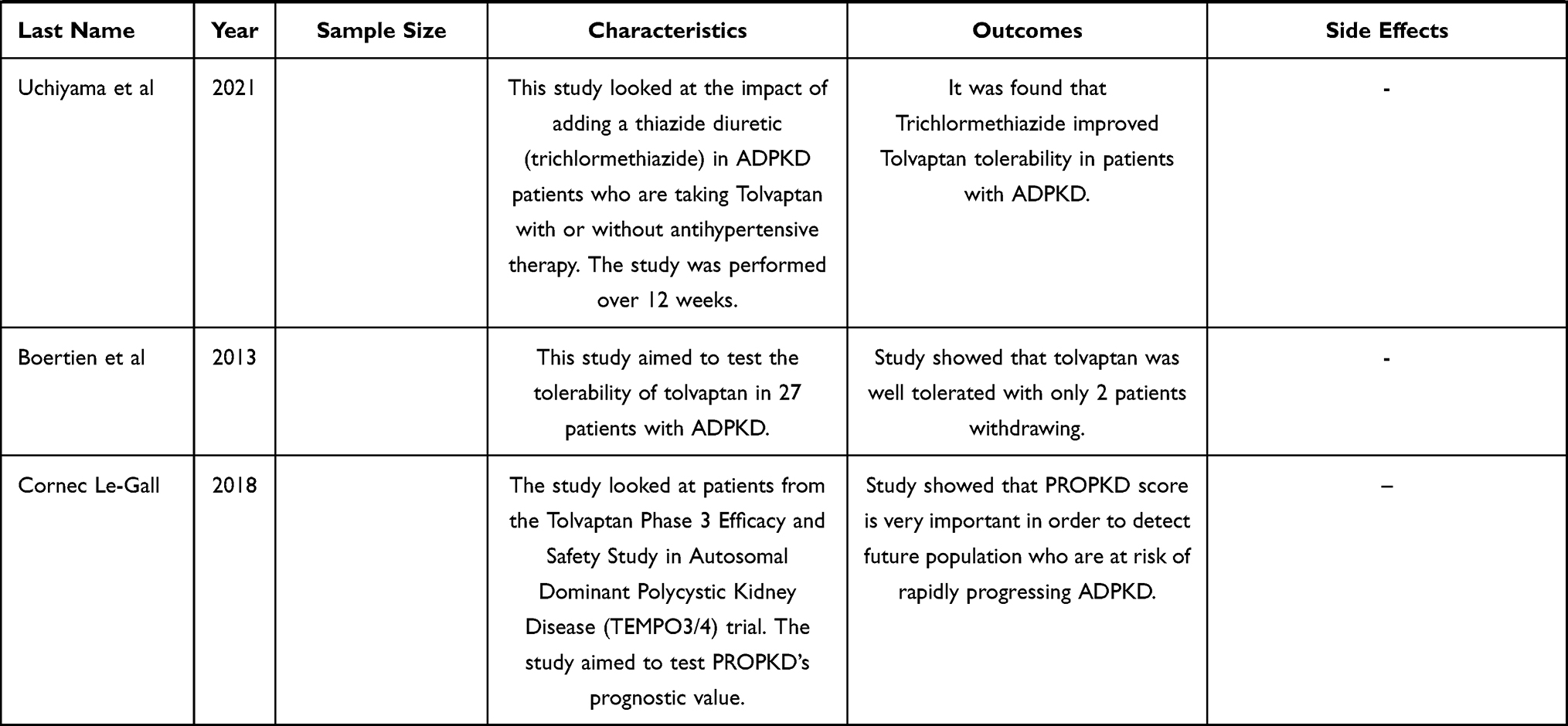 |
Table 1 Outcomes and Side Effects of Tolvaptan Trials |
Different methods are available to calculate the disease progression. As the number of cysts increase in ADPKD the total kidney volume (TKV) is a reliable data point, which helps monitor the disease progression. Renal Function tests which include serum creatinine and glomerular filtration rate (GFR) can also be used to see the disease progression. Of those options, total kidney Volume (TKV) is considered the most reliable (Figure 4). Radiologically measured kidney volume is a good predictor to measure the disease progression.12 Once the disease is diagnosed with ultrasound more sophisticated imaging modalities like CT and MRI are used to measure the TKV to follow the progression of ADPKD.
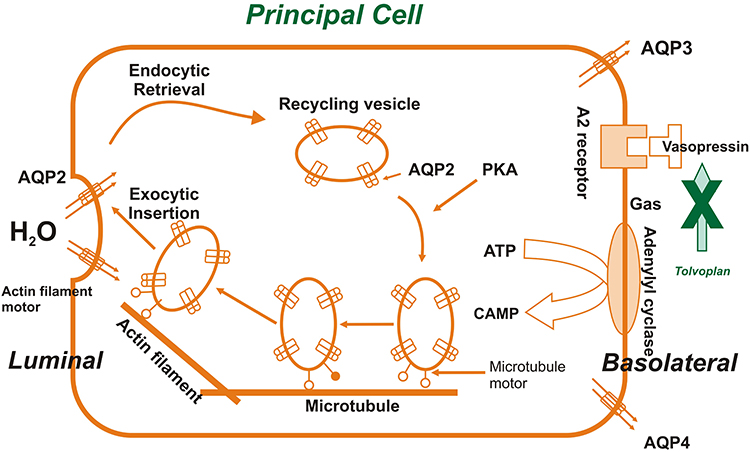 |
Figure 4 Mechanism and site of tolvaptan action. |
Side Effects
The use of tolvaptan has been shown to cause several adverse side effects. Various reports have documented their incidence in patients after treatment initiation for autosomal dominant autosomal polycystic kidney disease (ADPKD). In TEMPO 3:4, the various side effects were compared in the tolvaptan and placebo group.13 Tolvaptan is known to cause aquaretic side effects such as polyuria, nocturia and polydipsia most frequently. Aquaresis is defined as the excretion of water which is free of electrolytes. The aquaretic effects of tolvaptan are not known to decline with time.21 Tolvaptan is a selective vasopressin V2 receptor antagonist. It acts by inhibiting vasopressin from binding to the V2 receptor, thus causing aquaresis (loss of electrolyte-free water). The binding of vasopressin to the V2 receptor normally decreases the free water clearance from the body by aquaporin channel translocation in the collecting duct system. Therefore, tolvaptan usage in patients prevents this process and as result there is loss of free water causing polyuria, nocturia, thirst, dehydration, fatigue, dizziness most commonly22 Supplementary Table .
In the study done by Higashihara in 2011, the side effects of tolvaptan were observed to have a change in incidence with the changing dose of tolvaptan. Adverse effects like nocturia, dizziness, polyuria, fatigue and pollakiuria showed an increased incidence with an increase in dose from 15/15 mg/day to 45/15 mg/day. However, some other side effects like hypertension, renal pain, diarrhea showed a decrease in incidence with the same increase in the dose of tolvaptan20 Supplementary Table.
The TEMPO 3:4 trial also throws light on another serious side effect of tolvaptan: hepatotoxicity.21 This hepatotoxicity is thought to be idiosyncratic in nature. This is accompanied by elevation in the transaminase levels, which may be accompanied by elevated bilirubin levels as well.21 In most of the cases where ALT/AST or bilirubin levels were raised, the levels returned to baseline upon discontinuation of the drug.13 It has been noted that tolvaptan can cause severe liver damage in some patients and in some cases, patients have been required to undergo liver transplantation due to acute liver failure13 (Table 1, Figure 5).
 |
Figure 5 Side effects from the two largest trials. |
The TEMPO 3:4 trial also compared the elevated AST, ALT and bilirubin levels in patients taking tolvaptan and those taking placebo.13 The TEMPO 3:4 trial also compared the elevated AST, ALT and bilirubin levels in patients taking tolvaptan and those taking placebo. The elevations in AST, ALT and bilirubin were compared in tolvaptan and placebo group: 4.4% vs 3.1%, 1.0% vs 0.8% and 0.9% vs 1.9%. (The AST and ALT levels were elevated >3 times the upper limit of normal; the bilirubin levels were elevated >1.5 times the upper limit of normal)13 (Supplementary Table, Figure 5).
Subjects receiving tolvaptan in the REPRISE trial (double blinded study) were noted to develop hepatic side effects as well. In the same trial, subjects receiving placebo also developed hepatic side effects, but the incidence was lower as shown in the table given below.20 In the tolvaptan group 11% of the patients out of 681 total patients developed hepatic side effects and 5% of the patients in the placebo group developed hepatic side effects out of a total of 685 patients (Table 1, Supplementary Table).
According to two largest clinical trials, namely tolvaptan TEMPO 2:4 and tolvaptan TEMPO 3:4, this is the spectrum of side effects seen most in ADPKD patients who have been put on tolvaptan therapy20 (Figure 5).
Complications of Tolvaptan
Tolvaptan causes aquaretic side effects like polyuria, nocturia and polydipsia along with hepatotoxicity, hyperuricemia, fatigue, dehydration, pollakiuria, hypertension, etc. TEMPO 3:4 phase three trial is conducted on subjects between the age of 18–50 years.26 This trial was conducted over a period of three years and was done to show favorable effects of tolvaptan on the growth and function of the kidney.26 In the 18–24 years age group tolvaptan showed a higher TKV, however no hepatotoxicity was detected. In the young population, there was also no risk of hepatotoxicity. This trial prompts the need for further trials and studies in the younger and adolescent population.26
Most of the ADPKD patients have a positive family history with PKD1 mutation being more prevalent than the PKD2 mutation variant.27 ADPKD is usually asymptomatic well into adulthood, therefore efforts are being made to conduct studies to establish whether early initiation of tolvaptan can slow down cyst growth and help contain the renal damage.28 In children with ADPKD, the most common renal manifestations are polyuria, nocturia, hematuria and back/abdominal pain.29 Younger patients frequently develop glomerular hyperfiltration, proteinuria and albuminuria as compared to the adult population. This also leads them to develop more severe disease than patients who do not have proteinuria.30 This brings us to the dilemma whether children who are at a risk of developing ADPKD need screening for early detection of possible disease. Currently, there are no guidelines which recommend any such screening of children who are not symptomatic.
Hypertension is an important extrarenal manifestation of ADPKD in both children and adults, and it is a strong predictor for determining the prognosis of the patient.31 Owing to the high incidence of proteinuria and hypertension, the International Pediatric Nephrology Association (IPNA) and the European Society of Pediatric Nephrology (ESPN) have put forward the examination of blood pressure and urine in children at risk. The pediatric population at risk of developing ADPKD with any positive family history or with a confirmed diagnosis of ADPKD must be monitored regularly for changes in the blood pressure or albuminuria. Along with surveillance for hypertension, these children are recommended to adhere to a low-salt diet because it is known to keep the blood pressure within normal limits as well. The European Society of Hypertension (ESH) and the American Academy of Pediatrics (AAP) also propose a strict monitoring of blood pressure annually for at-risk children, and they extend this recommendation for healthy children as well.32
Future Perspectives
Reduction in morbidity and mortality associated with the manifestations of ADPKD have been the focus of treatment for many years. Lowering the rate of disease progression remains the main goal in the management of ADPKD, which is currently being done by using tolvaptan. Supportive therapies to reduce the rate of progression include optimization of BP, sufficient fluid intake, low-salt diet, caffeine reduction and avoidance of nephrotoxic agents.
There have been various literature discussions about high fluid intake alone for the treatment of ADPKD but with inconclusive results. Most clinical trials like PREVENT-ADPKD and DRINK (multi-centre, open-label randomized controlled trial) are only exploring an increased water intake, both with a target urine osmolality of ≤270 mOsm/kg.33 Dietary intervention played a key role in patients with ADPKD. Patients with ADPKD who did not follow a diet that focuses on calories, protein, sodium, and phosphate, saw an exacerbation in CKD clinical and metabolic abnormalities. In addition, these patients had a reduced drug therapy effectiveness. Thus, referring patients with ADPKD to a dietician early on can improve the clinical outcomes. No literature yet exists to assess the impact of a specific diet on ADPKD progression. Since drug therapy is not readily available to every patient with ADPKD, looking into dietary option to decrease or control ADPKD clinical presentation, can be an important future perspective. The burdens of ADPKD and CRRT (continuous renal replacement therapy) are serious and should not be disregarded.
Various trials described different medications that could stop the disease progression. Lixivaptan is a new oral V2-receptor-specific antagonist, previously used for SIADH, heart failure, etc., but is now being tested for treatment of ADPKD. Tyrosine Kinase plays a crucial role in the EGFR (epidermal growth factor receptor) pathway that constitutes one of the central stimuli of cystic cell proliferation. Pre-clinical studies have backed the role of tyrosine kinase inhibitors such as Bosutinib. Tesevatinib is a multi-kinase inhibitor that promotes the inhibition of c-Src (a tyrosine kinase closely implicated in EGFR cascade). Sphingolipids play an important role in controlling function, proliferation and apoptosis of cells. An ongoing trial is underway for the drug Venglustat, where the rate of kidney growth and the rate of glomerular filtration change are being studied. Metformin can stimulate the 5′ AMP-activated protein kinase (AMPK), a metabolic sensor that appears to be inhibited in ADPKD and is currently being studied in multiple ongoing clinical trials. 2-deoxy glucose (2DG) is a glucose analog that uses the same plasma membrane carrier as glucose to enter the cells. Once inside, like glucose, 2-deoxy glucose gets phosphorylated. After phosphorylation, the metabolism of 2-deoxy glucose stops here. This will lead to an accumulation inside the cell and thus stopping the glycolytic pathway. By using 2-deoxy glucose, the cell energy demands are targeted, and cystic epithelial proliferation cannot occur anymore in ADPKD. 2DG has been tested in several trials but is not registered as a therapeutic agent.34
Quality of life in patients with ADPKD is affected heavily. Studies on the impact of tolvaptan on the quality of life of patients with ADPKD are absent.35 Although tolvaptan showed a significant impact on the progression of ADPKD, studies showing tolvaptan future effects and whether the results are reproducible over the long term are missing. Monitoring treatment efficacy is a topic, which needs further research. Determination of htTKV (height adjusted total kidney volume) using imaging is at this time the best method to predict disease outcomes and monitor treatment efficacy. In addition, a quantitative image analysis of the kidney can further monitor and predict disease outcomes.
Conclusion
Tolvaptan is an approved treatment for use against ADPKD. The results of various clinical trials showed that tolvaptan is the drug of choice in slowing the progressive loss of renal function in patients with ADPKD. Many new treatment approaches are emerging and trying to target different aspects of the disease. Of these emergent approaches, Micheal J. Caplan discussed the importance of the enzyme adenosine monophosphate protein kinase (AMPK) in cellular metabolism and its role in ADPKD. AMPK usually acts by increasing the production mechanism of ATP when AMP levels are high and ATP levels are low. Many processes, which are against cyst formation in kidneys, are normally shut down by AMPK. The author found that AMPK participated in ADPKD pathogenesis, especially when the mutations in ADPKD downregulate AMPK functions, thus allowing cyst formations. Thus, the new drug being researched acts on AMPK either directly (through a chemical compound that mimics AMP) or indirectly (caloric restriction which will increase the need for high energy levels) activating it to counteract the cyst generating factors in ADPKD. By activating AMPK, cellular metabolism will shift to increasing energy expenditure and slowing down cyst developments.36 This new concept is still heavily being tested along with other emergent ones in the future.
Disclosure
Rupesh Raina and Ahmad Houry are co-first authors. The authors declare no conflicts of interest.
References
1. Cornec-Le Gall E, Alam A, Perrone RD. Autosomal dominant polycystic kidney disease. Lancet. 2019;393(10174):919–935. doi:10.1016/S0140-6736(18)32782-X
2. Baur BP, Meaney CJ. Review of tolvaptan for autosomal dominant polycystic kidney disease. Pharmacotherapy. 2014;34(6):605–616. doi:10.1002/phar.1421
3. USRDS, U.S. Renal Data System. USRDS 2012 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Dis- eases: Bethesda, MD; 2012.
4. Pei Y, Watnick T. Autosomal Dominant Polycystic Kidney Disease (ADPKD): genetics of the Disease and Mechanisms of Cyst Growth 2020. Available from: https://www-uptodate-com.auamed.idm.oclc.org/contents/autosomal-dominant-polycystic-kidney-disease-adpkd-genetics-of-the-disease-and-mechanisms-of-cyst-growth?search=ADPKD&topicRef=1678&source=see_link.
5. Grantham JJ. Autosomal dominant polycystic kidney disease. N Engl J Med. 2008;14:1477–1485. doi:10.1056/NEJMcp0804458
6. Torres VE, Harris PC, Pirson Y. Autosomal dominant polycys- tic kidney disease. Lancet. 2007;9569:1287–1301. doi:10.1016/S0140-6736(07)60601-1
7. Arnaout MA. Molecular genetics and pathogenesis of autoso- mal dominant polycystic kidney disease. Annu Rev Med. 2001;52:93–123. doi:10.1146/annurev.med.52.1.93
8. PeiY A. “two-hit”modelofcystogenesisinautosomaldominant polycystic kidney disease? Trends Mol Med. 2001;4:151–156.
9. Yamaguchi T, Wallace DP, Magenheimer BS, Hempson SJ, Grantham JJ, Calvet JP. Calcium restriction allows cAMP activation of the B-Raf/ERK pathway, switching cells to a cAMP-dependent growth-stimulated phenotype. J Biol Chem. 2004;39:40419–40430. doi:10.1074/jbc.M405079200
10. Shillingford JM, Murcia NS, Larson CH, et al. The mTOR pathway is regulated by polycystin-1, and its inhibition reverses renal cystogenesis in polycystic kidney disease. Proc Natl Acad Sci USA. 2006;14:5466–5471. doi:10.1073/pnas.0509694103
11. Miyazaki T, Fujiki H, Yamamura Y, Nakamura S, Mori T. Tolvaptan, an orally active vasopressin V(2)-receptor antago- nist—pharmacology and clinical trials. Cardiovasc Drug Rev. 2007;1:1–13. doi:10.1111/j.1527-3466.2007.00001.x
12. O’Neill WC, Robbin ML, Bae KT, et al. Sonographic assess- ment of the severity and progression of autosomal dominant polycystic kidney disease: the Consortium of Renal Imaging Studies in Polycystic Kidney Disease (CRISP). Am J Kidney Dis. 2005;6:1058–1064. doi:10.1053/j.ajkd.2005.08.026
13. Torres VE, Chapman AB, Devuyst O, et al. Tolvaptan in patients with autosomal dominant polycystic kidney disease. N Engl J Med. 2012;367(25):2407–2418. doi:10.1056/NEJMoa1205511
14. Irazabal MV, Torres VE, Hogan MC, et al. Short-term effects of tolvaptan on renal function and volume in patients with autosomal dominant polycystic kidney disease. Kidney Int. 2011;80(3):295–301. doi:10.1038/ki.2011.119
15. Boertien WE, Meijer E, de Jong PE, et al. Short-term renal hemodynamic effects of tolvaptan in subjects with autosomal dominant polycystic kidney disease at various stages of chronic kidney disease. Kidney Int. 2013;84(6):1278–1286. doi:10.1038/ki.2013.285
16. Horie S, Muto S, Kawano H, et al. Preservation of kidney function irrelevant of total kidney volume growth rate with tolvaptan treatment in patients with autosomal dominant polycystic kidney disease. Clin Exp Nephrol. 2021;25(5):467–478. doi:10.1007/s10157-020-02009-0
17. Muto S, Kawano H, Higashihara E, et al. The effect of tolvaptan on autosomal dominant polycystic kidney disease patients: a subgroup analysis of the Japanese patient subset from TEMPO 3:4 trial. Clin Exp Nephrol. 2015;19(5):867–877. doi:10.1007/s10157-015-1086-2
18. Bennett H, McEwan P, Hamilton K, O’Reilly K. Modelling the long-term benefits of tolvaptan therapy on renal function decline in autosomal dominant polycystic kidney disease: an exploratory analysis using the ADPKD outcomes model. BMC Nephrol. 2019;20(1):136. doi:10.1186/s12882-019-1290-5
19. Edwards ME, Chebib FT, Irazabal MV, et al. Long-Term Administration of Tolvaptan in Autosomal Dominant Polycystic Kidney Disease. Clin J Am Soc Nephrol. 2019;14(6):910. doi:10.2215/CJN.01520218
20. Higashihara E, Torres VE, Chapman AB, et al. Tolvaptan in autosomal dominant polycystic kidney disease: three years’ experience. Clin J Am Soc Nephrol. 2011;10:2499–2507. doi:10.2215/CJN.03530411
21. Blair HA. Tolvaptan: a Review in Autosomal Dominant Polycystic Kidney Disease. Drugs. 2019;79(3):303–313. doi:10.1007/s40265-019-1056-1
22. Ali Y, Dohi K, Okamoto R, Katayama K, Ito M. Novel molecular mechanisms in the inhibition of adrenal aldosterone synthesis: action of tolvaptan via vasopressin V2 receptor‐independent pathway. Br J Pharmacol. 2019;176:1315–1327. doi:10.1111/bph.14630
23. Torres VE, Chapman AB, Devuyst O, et al. Multicenter, open-label, extension trial to evaluate the long-term efficacy and safety of early versus delayed treatment with tolvaptan in autosomal dominant polycystic kidney disease: the TEMPO 4:4 Trial. Nephrology Dialysis Transplantation. 2017;32(7):1262. doi:10.1093/ndt/gfx043
24. Casteleijn NF, Lianne MA, Bae KT, et al. Polyuria due to vasopressin V2 receptor antagonism is not associated with increased ureter diameter in ADPKD patients. Clin Exp Nephrol. 2017;21(3):375–382. doi:10.1007/s10157-016-1297-1
25. Torres VE, Higashihara E, Devuyst O, et al. Effect of Tolvaptan in Autosomal Dominant Polycystic Kidney Disease by CKD Stage: results from the TEMPO 3:4 Trial. Clin J Am Soc Nephrol. 2016;11(5):803–811. doi:10.2215/CJN.06300615
26. Raina R, Chakraborty R, DeCoy ME, Kline T. Autosomal-dominant polycystic kidney disease: tolvaptan use in adolescents and young adults with rapid progression. Pediatr Res. 2021;89(4):894–899. doi:10.1038/s41390-020-0942-2
27. Iliuta IA, Kalatharan V, Wang K, et al. Polycystic kidney disease without an apparent family history. J Am Soc Nephrol. 2017;28:2768–2776. doi:10.1681/ASN.2016090938
28. Dachy A, Collard L, Krzesinski JM, et al. Polykystose rénale autosomique dominante: perspective pédiatrique [Autosomal dominant polycystic kidney disease: a pediatric perspective]. Rev Med Liege. 2020;75(12):775–780.
29. Fick GM, Duley IT, Johnson AM, Strain JD, Manco-Johnson ML, Gabow PA. The spectrum of autosomal dominant polycystic kidney disease in children. J Am Soc Nephrol. 1994;4(9):1654–1660. doi:10.1681/ASN.V491654
30. Helal I, Reed B, McFann K, Yan XD, Fick-Brosnahan GM, Cadnapaphornchai M. Glomerular Hyperfiltration and Renal Progression in Children with Autosomal Dominant Polycystic Kidney Disease. Clin J Am Soc Nephrol. 2011;6(10):2439–2443. doi:10.2215/CJN.01010211
31. Reddy BV, Chapman AB. The spectrum of autosomal dominant polycystic kidney disease in children and adolescents. Pediatr Nephrol. 2017;32(1):31–42. doi:10.1007/s00467-016-3364-y
32. Gimpel C, Bergmann C, Bockenhauer D, et al. International consensus statement on the diagnosis and management of autosomal dominant polycystic kidney disease in children and young people. Nat Rev Nephrol. 2019;15:713–726. doi:10.1038/s41581-019-0155-2
33. Wong ATY, Mannix C, Grantham JJ, et al. Randomised controlled trial to determine the efficacy and safety of prescribed water intake to prevent kidney failure due to autosomal dominant polycystic kidney disease (PREVENT-ADPKD). BMJ Open. 2018;8(1):e018794. doi:10.1136/bmjopen-2017-018794
34. Testa F, Magistroni R. ADPKD current management and ongoing trials. J Nephrol. 2020;33(2):223–237. doi:10.1007/s40620-019-00679-y
35. Barnawi RA, Attar RZ, Alfaer SS, Safdar OY. Is the light at the end of the tunnel nigh? A review of ADPKD focusing on the burden of disease and tolvaptan as a new treatment. Int J Nephrol Renovasc Dis. 2018;11:53–67. doi:10.2147/IJNRD.S136359
36. Caplan MJ. AMPK and Polycystic Kidney Disease Drug Development: an Interesting Off-Target Target. Front Med. 2022;9:753418. doi:10.3389/fmed.2022.753418
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.