")
Back to Journals » Drug, Healthcare and Patient Safety » Volume 14
Clinical Efficacy, Safety, Tolerability, and Real-World Data of Patiromer for the Treatment of Hyperkalemia
Authors Colbert G , Sannapaneni S, Lerma EV
Received 21 March 2022
Accepted for publication 12 July 2022
Published 14 July 2022 Volume 2022:14 Pages 87—96
DOI https://doi.org/10.2147/DHPS.S338579
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rajender R Aparasu
Gates Colbert,1 Shilpa Sannapaneni,1 Edgar V Lerma2
1Department of Internal Medicine, Division of Nephrology, Texas A&M College of Medicine, Dallas, TX, USA; 2Department of Internal Medicine, Division of Nephrology, University of Illinois at Chicago College of Medicine, Chicago, IL, USA
Correspondence: Gates Colbert, 3417 Gaston Ave, Suite 875, Dallas, TX, 75246, Tel +972-388-5970, Fax +972-388-5971, Email [email protected]
Abstract: Hyperkalemia remains one of the most difficult consequences of disease state and treatment for patients with chronic kidney disease, heart failure, and diabetes. Controlling hyperkalemia can be difficult, but has become easier with the introduction of novel oral potassium binders. Patiromer was approved in 2015 for the treatment of hyperkalemia by the FDA in the United States. Several pivotal trials proved its efficacy, safety, and improved tolerability compared with previous hyperkalemia treatments. Additionally, many real-world publications and trials have given deeper insights into the capabilities of patiromer. We discuss improved disease state outcomes with combining patiromer with RAASi. This paper will also highlight new trials forthcoming that are highly anticipated to expand the possibilities in using patiromer to improve outcomes and populations.
Keywords: hyperkalemia, chronic kidney disease, patiromer, proteinuria
Introduction
Hyperkalemia is a common electrolyte abnormality with potentially life-threatening consequences. Known risk factors for the development of hyperkalemia include chronic kidney disease (CKD), heart failure (HF), and diabetes. Hyperkalemia in patients with chronic kidney disease occurs at a rate of 8/100 person-months as defined as an eGFR <60 mL/min/1.72 m2.1 In affected patients who develop hyperkalemia, there is a significant increase in the risk of mortality, cardiovascular morbidity as well as progression of CKD. Interestingly, the medications that have been demonstrated to address these comorbid risks target the renin angiotensin aldosterone system (RAAS), such that their side effect is the development of hyperkalemia.
Although there are several mechanisms by which hyperkalemia develops in high-risk individuals, particularly those with CKD, the most important mechanism is that of decreased secretion of potassium in the distal tubule because of aldosterone resistance.2 Other mechanisms inducing hyperkalemia include altered potassium handling, metabolic acidosis, as well as decreased insulin utility. Hyperkalemia can be episodic or recurrent as a condition. Depending on the cause, temporary such as a medication change or chronic with disease state progression, treatment options and focus may be different. In either clinical scenario, hyperkalemia is a condition that must not be ignored as the life-threatening consequences are real and critical.
History of Oral Potassium Binders
Synthetic ion-exchange resins were first made available to industry in 1935. Potassium (K+) binders used for hyperkalemia management are typically non-absorbed and consist of a counter-ion that is exchanged for potassium, thereby facilitating the elimination of bound K+ via the gastrointestinal route. Sodium polystyrene sulfonate (SPS) is an orally administered sodium-exchange resin, that promotes excretion of potassium in the colon lumen with voluminous stool outputs,3 whereas calcium polystyrene sulfonate (CPS) is a calcium-exchange resin with a similar mechanism. The approval of SPS was based on 2 small trials that demonstrated efficacy4,5 in treating hyperkalemia when administered either orally or rectally.
For several years, SPS was the only oral K+ binder available, and this remains true for several parts of the world today. There are however some known disadvantages to this medication. Aside from issues with palatability, the known effect of diarrhea is significantly undesirable to both patients and caregivers. In addition, there is the problematic cumulative sodium loading (particularly when administered in multiple doses as is frequently required) which can contribute to volume overload as well as difficult to control hypertension. Although uncommon, there have also been case reports of colonic necrosis associated with the use of SPS, with the largest report6 involving 82 cases of colonic necrosis in 2194 in-patients who were prescribed SPS. Current use of SPS is usually episodic and not commonly prescribed over 30 days due to patient tolerability, adherence, and concerns for long-term safety.
Given the challenges associated with SPS described above, newer oral potassium binders were developed to better address hyperkalemia treatment with the goal of better long-term treatment options. In recent years we have seen the advent of novel oral K+ binders, namely sodium zirconium cyclosilicate (SZC),7 which is a cation-exchange agent that primarily exchanges sodium and hydrogen for potassium within the gut lumen; and patiromer, which is a calcium-based polymer suspension, that exchanges calcium in the gut lumen for available K+ cations.8
Mechanism of Action
Potassium is the most abundant cation in the colon, and it stays in the colon longer than any other location within the gastrointestinal tract.9 In patients with CKD and hyperkalemia, secretion of potassium into the colon is compensatory upregulated by two- to eight-fold through the colonic KCNMA1, “big potassium” (BK) channels.10 Patiromer is a spherical, non-absorbable synthetic cation exchange polymer which contains a calcium-sorbitol counter-ion. Patiromer was designed as a high-capacity potassium-binding polymer to be ionized fully at the physiological pH of the colon where the potassium concentration of the gastrointestinal tract is highest, leading to an optimal ion exchange. It acts primarily in the colon, but the potassium binding process can occur in the upper gastrointestinal tract as well. Patiromer binds to potassium in the colonic lumen, creating a concentration gradient which in turn decreases the reabsorption and increases the secretion of potassium through the colonic BK channels. According to a study done in healthy human subjects, patiromer increased fecal potassium and decreased urinary potassium excretion when compared with placebo.11
Safety and Tolerability
Patiromer is not systemically absorbed which is a major contributing factor to its safety and tolerability. When administered with other drugs, few drug-drug interactions due to cytochrome P450 or systemic drug transporter effects are observed. This is the result of its physical stability while passing through the gastrointestinal tract.12 However, patiromer can interact with some drugs in the gastrointestinal tract leading to reduced absorption of certain oral medications when administered concomitantly. For this reason, it is recommended to separate administration of patiromer by 3 hours from the administration of other oral medications. This is similar to the recommendations for the other oral potassium binders, SPS and SZC, available in the United States. A comparative study between a global database and data from a clinical trial program which assessed 45,000 patient years of exposure to patiromer reported that of the adverse events, 26% were serious adverse events (most of which were not attributed to patiromer) and 74% were non-serious adverse events.13 However, this study has some limitations inherent to post marketing data.
The most common adverse events related to patiromer are gastrointestinal (GI) side effects and this has been well documented in all the major trials. Constipation, flatulence, and diarrhea are the most common GI side effects, but all are in less than 10% of patients studied. The onset of most GI adverse events occurred within the first 4 weeks of treatment. In addition to lowering serum potassium levels, patiromer is associated with lower magnesium levels and increased serum calcium levels in rare cases.14,15 A potential dose relationship between higher doses of patiromer and higher incidence of hypomagnesemia was reported in the AMETHYST-DN trial.16 A clinical research trial evaluated urine and serum ion concentration changes in healthy volunteers who received patiromer. Serum levels of potassium, sodium, calcium, magnesium, and phosphate were normal and stable while urine potassium, sodium, magnesium, phosphate levels were reduced, and urine calcium levels were modestly increased.17 Hypokalemia, defined as serum potassium < 3.5 mEq/L was rarely observed in pooled studies.12 Other minor side effects such as hypersensitivity reactions, anemia, urinary tract infection, headache can occur with mild to moderate severity.
Patiromer uses calcium instead of sodium as a counter exchange ion, consequently sodium absorption and related consequences of edema and worsening hypertension are not a clinical concern. In the OPAL-HK trial, electrocardiogram findings were assessed, and no abnormal findings were noted.18 In a pooled analysis of AMETHYST-DN and OPAL-HK trials, 8.6% patients had at least one serious adverse event. However, none of these serious adverse events were attributed to patiromer.12 The TOURMALINE study concluded that there was no change in efficacy or tolerability with food consumption versus an empty stomach.19 Summaries of the main trials are available in Tables 1 and 2.
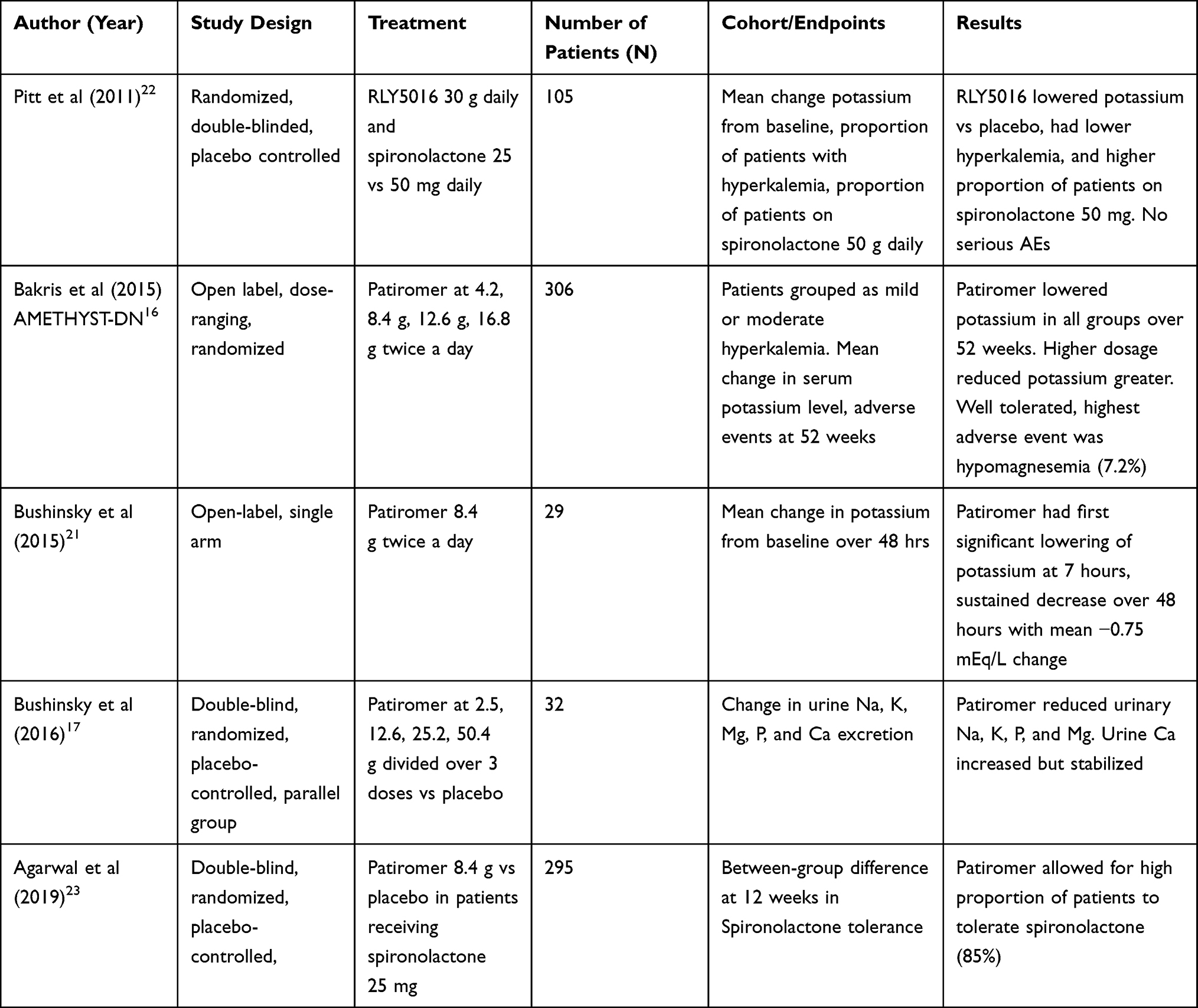 |
Table 1 Summary of Patiromer Phase 1 and 2 Trials |
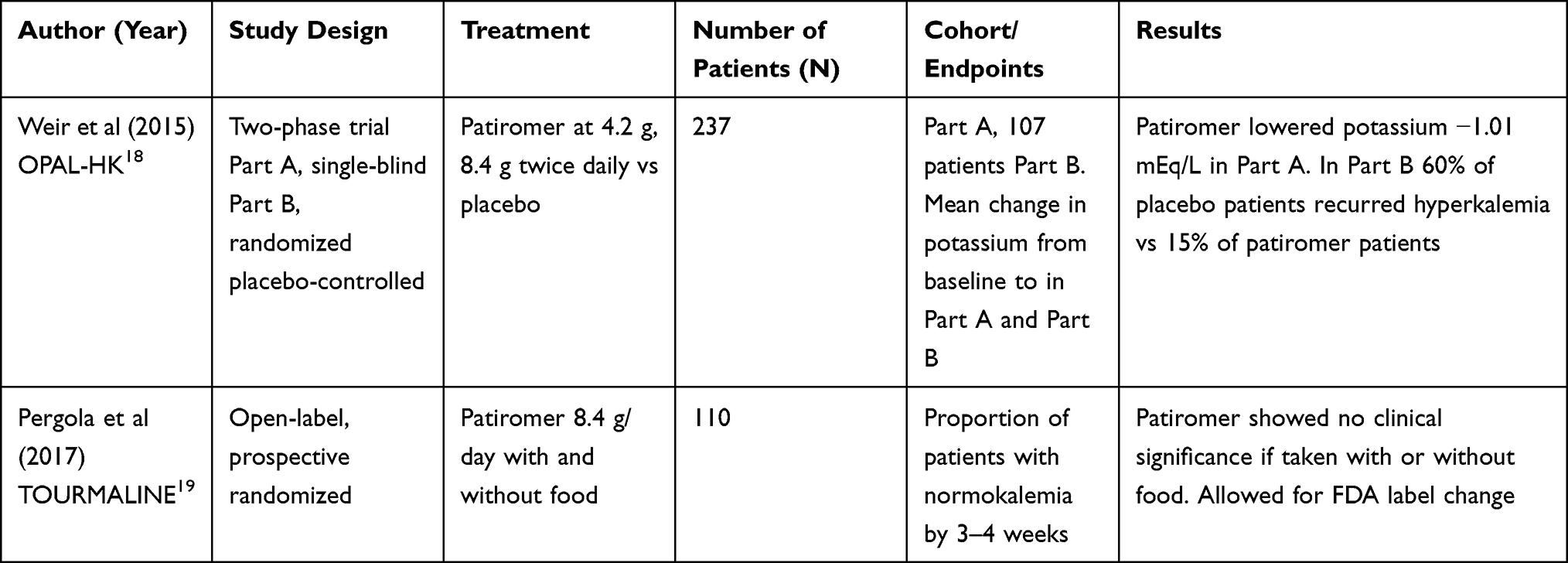 |
Table 2 Summary of Patiromer Phase 3 Trials |
For the introduction of patiromer into clinical use, two simultaneous phase 1 studies were conducted prior to FDA approval. Study 101 looked at dose-related response of lowering potassium levels and the most effective dose for it. Doses of 2.5 g, 12.6 g, 25.2 g or 50 g given three times a day noted significant increases in fecal potassium excretion.20 Study 102 looked at effects of 25.2 g daily dosing vs splitting the same dose over two to three times a day and found no differences in potassium excretion.20 Onset of action was evaluated by a phase 1 trial where patiromer 8.4 g BID was given with meals for a total of 4 doses to 29 patients.21 Patients were admitted to a monitoring unit with a controlled diet and had a measured potassium between 5.5–6.5 mEq/L. Change in potassium over 48 hours from baseline was the primary endpoint studied. The mean baseline serum potassium was 5.93 mEq/L at 7 hours and a mean reduction of 0.75 mEq/L was seen at 48 hours, with no serious adverse events or withdrawals.
It was unclear if binding of patiromer to electrolytes such as magnesium or sodium influenced systemic electrolyte balance. This was looked into by a dose finding phase 1 study by Bushinsky et al with a double blind, randomized, placebo controlled, multiple-dose study in healthy volunteers.17 Four groups, each with 8 volunteers were organized; 6 in 8 members received total daily doses of 2.5, 12.6, 25.2 or 50.4 g patiromer for 20 days with the remaining 2 members receiving placebo in each group. Serum sodium (Na), potassium, calcium (Ca), and magnesium (Mg) were within normal ranges and stable. The 24-h urine collection in the treatment group had a dose-dependent decrease in urine K+, Na, Mg, and phosphorus (p<0.01). Urine Ca increased in a dose-dependent fashion but stabilized (p<0.01). Gastrointestinal symptoms were the most common events with no other serious adverse events reported.
Safety of patiromer in patients with comorbidities was looked into by the pivotal PEARL-HF and AMETHYST-DN trials. PEARL-HF, a double-blinded, placebo controlled trial in which 105 patients with HF and CKD, and hyperkalemia were randomized to patiromer 30 g/day vs placebo for 4 weeks.22 Reflecting goal-directed guideline therapy, spironolactone 25 mg was added if potassium levels remained within safe ranges. Change in potassium from baseline being the primary endpoint, proportion of patients with K >5.5 mEq/L and proportion of patients on spironolactone 50 mg/day were the secondary endpoints. The trial showed that patients with hyperkalemia, CKD, and HF could tolerate the addition of spironolactone with patiromer. Findings included lowering of K+ by −0.45 mEq/L (p<0.001), lower incidence of hyperkalemia (7.3% vs 24.5%; drug vs placebo) and higher proportion of patients on spironolactone (91% vs 74%; drug vs placebo). This was the first placebo-controlled study to report patiromer could prevent hyperkalemia in patients with HF and CKD.
The AMETHYST-DN was a long-term safety and efficacy trial in the outpatient setting for patients with diabetes receiving renin angiotensin aldosterone system inhibitors (RAASi) and to set up trial doses for later phase 3 trials.16 An open label, multicenter, dose-ranging, randomized trial was conducted from June 2011 to June 2013 with 306 patients with eGFR between 15–60 mL/min/1.73 m2 and serum potassium level > 5.0 mEq/L. All patients were stratified randomly to one of three starting doses of patiromer twice daily at 4.2 g [n = 74], 8.4 g [n = 74] or 12.6 g [n = 74] for mild hyperkalemia or 8.4 g [n = 26], 12.6 g [n = 28] or 16.8 g [n = 30] for moderate hyperkalemia. The primary endpoint was adverse events over 52 weeks duration. In patients with mild hyperkalemia, the least-squares mean reduction from baseline potassium at week 4- or first-time dose titration was 0.35, 0.51, and 0.55 mEq/L in the 4.2 g, 8.4 g, and 12.6 g twice daily groups, respectively. Reductions were greater in moderate hyperkalemia showing decreases of 0.87, 0.97, and 0.92 mEq/L in the 8.4 g, 12.6 g, and 16.9 twice daily groups respectively. A rise in potassium was noted when patiromer was discontinued at the end of one year. Hypomagnesemia (7.2%) was the most common adverse event and hypokalemia (5.6%), but no patient had K <3.0 mEq/L.
Another phase 2 trial looking at addition and tolerability of spironolactone in patients with CKD eGFR < 45 mL/min/ 1.73 m2 and uncontrolled resistant hypertension on 3 or more anti-hypertensive agents was looked into by Agarwal et al in a study titled AMBER.23 This was a multicenter, double-blind, placebo controlled, randomized trial with 295 participants with potassium <5.1 mEq/L, diabetes, CKD, and hypertension randomized to patiromer 8.4 g daily or placebo with baseline blood pressure medications and spironolactone 25 mg daily. Dose titrations of spironolactone occurred at week 1 for patiromer and week 3. By week 12, 126 (86%) of 147 patients in the patiromer arm and 98 (66%) of 148 patients in the placebo arm remained on spironolactone (p <0.001) which was the primary endpoint. The trial proved that patients with resistant hypertension could tolerate spironolactone while experiencing less hyperkalemia while on patiromer.
Based on the dosage recommendations provided by the AMETHYST-DN trial, a two part single-blind randomized Phase 3 trial, OPAL-HK was performed with goals to determine the efficacy and safety of patiromer while receiving at least one RAASi.18 In total 237 patients with eGFR between 15–60 mL/min/1.73 m2 with potassium levels between 5.1–6.5 mEq/L who were receiving RAAS inhibitors were included. Part A included a single-blind assessment of patiromer dosed at 4.2 g (mild hyperkalemia) or 8.4 g (moderate hyperkalemia) twice daily for 4 weeks. If serum potassium was below 5.1 mEq/L they continued on to Part B, who underwent a randomized, placebo controlled 8-week assessment of withdrawal of patiromer and placement on placebo. Mean change from baseline to week 4 was the primary endpoint of the study. The mean change in potassium for Part A was −1.01 mEq/L (p <0.001). Of the 107 patients included in Part B, recurrence of hyperkalemia occurred in 60% of patients in the placebo group compared with 15% in the patiromer group. Discontinuation of RAASi in the placebo group was over 50% vs only 6% in the patiromer group. This trial showed the benefit of lowering potassium in patients with CKD while allowing for continuation of RAASi agents.
Initial Food and Drug Association (FDA) labeling that required patiromer to be taken with food led to a phase 4 trial titled TOURMALINE which was a prospective, open label, randomized trial which included 110 patients.17 It was a 4 week-long trial and randomized patients to patiromer 8.4 g/day with and without food with the primary endpoint looking at the proportion of patients with normokalemia at the end of 4 weeks. The baseline potassium levels were 5.44 mEq/L (87.3%) vs 5.34 mEq/L (82.5%) in patients without food vs with food, showing equal effectiveness of patiromer with or without food. The least squares mean changes in serum potassium were −0.65 mEq/L and −0.62 mEq/L in patients without food vs with food, respectively. The most common side effects were diarrhea and constipation. As mentioned previously, there were no major differences in outcomes between the groups.
Patiromer Real-World Data and Post-Approval Research
Since patiromer was first introduced into the US market in 2015, there have been several studies and observation cohorts published concerning its effectiveness and safety. No major adverse events have been reported in real-world use requiring an FDA warning statement, “black box” warning, or change in label of the package insert for safety. Some case reports have been published regarding rare side effects, such as hypercalcemia,15 but overall no significant adverse reactions that were not previously discussed have been found.
Patiromer has not been formally studied in the emergency room as of this publication for acute hyperkalemia. But one pilot study has looked at use of patiromer in the emergency room population. This study was open-label and randomized to 30 adults with potassium levels greater than 6.0 mEq/L and compared standard of care or patiromer 25.2 g with standard of care.24 The primary outcome was the difference in potassium levels between these two groups at 6 hours. The study did not find any statistical difference in potassium levels at 6 hours (6.32 mEq/L vs 5.81 mEq/L). But at the 2-hour mark potassium level was lower in the patiromer group (5.9 mEq/L vs 6.51 mEq/L SOC). The need for albuterol in the patiromer group was lower but did not meet a statistical difference. There was no difference in adverse events between patiromer and standard of care without patiromer. Patiromer in previous studies has been shown to have effect at between 4–7 hours, which may not have been fully captured in this small study.
Despite being a large population with hyperkalemia risk, transplant patients have also not been formally represented in randomized patiromer trials.25 All transplant patients with calcineurin inhibitor exposure have an increased risk of hyperkalemia due to the decreased secretion of potassium in the nephron. The FDA does not prohibit use of patiromer in transplant patients, as the indication is for hyperkalemia no matter the mechanism of cause. One single-center retrospective study was published in 2019 where 19 transplant patients were receiving patiromer over a 3 year period.26 Sixteen of the transplant patients who received patiromer had potassium levels of 5.2 mEq/L. No patients stopped using patiromer because of GI side effects, and there was no mention of hypercalcemia. A sentinel finding was that immunosuppression levels did not change as a result of patiromer exposure, which is critical to maintain kidney transplant efficacy. Another retrospective study looked at 36 solid organ transplant patients who received patiromer for at least one month.27 They found at 4 weeks that 72% of patients were able to achieve a potassium level < 5.2 mEq/L and maintained that ceiling at 12 weeks. Tacrolimus dose adjustment was variable with 32% decreased in dose, 47% no change, and 21% needing a dose increase. Cyclosporine levels from baseline did not have a significant difference, possibly from small sample size. Overall it appears that transplant patients are able to use patiromer for hyperkalemia, but larger prospective trials are needed.
A Veterans Affairs data study has been published looking at patients with potassium >5.1 mEq/L and use of patiromer.28 A total of 288 patients were included with 32% having heart failure, 83% diabetes, and 95% CKD. Potassium level lowering was on average −1.0 mEq/L (p <0.001). At 6 months, 80% of patients who initiated patiromer and were on RAASi medications were able to maintain their RAASi use. This trial showed in real-world use that patiromer was highly effective in lowering potassium and was tolerable over a 6-month period. As well, with a very high percentage of RAASi continuation, guideline driven medication goals were more likely to be achieved with use of patiromer.
The highest risk group for hyperkalemia are ESKD patients who are on hemodialysis. As part of FDA approval exploratory tests, ESKD patients were excluded from the major randomized trials. Yet there have been more recent trials looking at patiromer use for ESKD groups. A retrospective cohort examined patiromer, SPS, and those without potassium binders in an electronic health record of a large dialysis provider in the USA for 1 year in 2016.29 The study included 527 patients using patiromer, 852 with SPS, and 8747 without use of either. Most patients who received patiromer initiated on the 8.4 g daily dosing (61%) and 60% of total cohort remained on patiromer after 180 days. Patients using patiromer had higher baseline potassium levels and had an average reduction of −0.5 mEq/L in potassium levels. Adverse events were unable to be captured by the electronic record analysis. A small prospective trial was completed by Amdur et al with 27 anuric patients on hemodialysis.30 They received 12 weeks of patiromer at 16.8 g daily and showed a mean potassium fall of −0.6 mEq/L. Stool potassium significantly increased in treatment phase from 4132 to 5923 μg/g. The authors estimated that 16.8 g of patiromer increased fecal potassium by 1880 μg/g. Overall it was well tolerated and provides prospective data, albeit a small cohort. A unique pilot study on patients undergoing hemodialysis twice weekly, as opposed to standard thrice weekly dialysis, also include the use of patiromer.31 Twenty-three patients underwent twice weekly dialysis, of which 17% received patiromer during the median follow up of 281 days. In this group it was significant for better urine outputs and better urea and creatinine clearance. While this patiromer group was extremely small, it may help pave the way for larger multicenter trials for patiromer use in ESKD patients and how it can lead to improved outcomes. As evidenced, the prospective data for ESKD patients and patiromer is highly needed, and should be answered with new clinical trials planned.
The use of hospital and healthcare resources has been positively influenced by patiromer use in the United States. A retrospective study of Medicare Advantage patients was published in 2020.32 The study looked at 610 patients on patiromer, 5556 SPS, and 21,282 without potassium binder exposure who all had a measurable potassium > 5.0 mEq/L. The authors state that patients who remained on RAASi between the groups were 78% on patiromer, 57% SPS, and 57% without either use. Additionally, there were statistically significant reductions in emergency department visits and hospital admissions with patiromer use. Patients without exposure to either oral potassium binder and hyperkalemia had increased hospitalization and emergency department use.
Patiromer Enhancing RAASi Use
We have known for decades through pivotal trials and society guidelines that RAASi utilization is critical to slow CKD progression, reduce mortality, and improve clinical outcomes.33–35 All of these improvements in community health can lower healthcare costs. Yet, the ability to use RAASi at the maximal dosages and in the highest number of patients is hindered by risk of recurrent hyperkalemia.36 Too many patients are started on a RAASI and then it is lowered or removed completely when hyperkalemia occurs. Many patients who experience hyperkalemia and stop RAASi have been shown to suffer adverse long-term outcomes.37 Another recent study by Trevisan et al38 showed that stopping MRA after hyperkalemia had higher risk of death and CV events. When a RAASi medication is stopped, the patients are no longer on guideline driven therapies and likely will have a worse prognosis long term. As such when RAASi modification occurs patients are stuck in a valley of being off treatment recommendations and balancing the adverse outcome of hyperkalemia with RAASi maximization.
A real-world use of patiromer and RAASi was looked at by Kovesdy28 though the US Veteran Healthcare system. In a 6-month post-index follow up 80% of patients on RAASi and patiromer were able to maintain the RAASi at 6 months. The prospective AMBER trial, mentioned earlier, was published looking at hypertension patients and patiromer use.23 Of 295 patients with resistant hypertension and CKD, 86% were able to continue spironolactone therapy compared with only 60% of patients who were on placebo at 12 weeks (p <0.0001). There was not a statistically significant change in blood pressure with spironolactone use, but patients were continued on their baseline medications. Mineralocorticoid receptor antagonists are increasingly showing improved long-term outcomes and may have benefit when combined with other RAASi agents. Unfortunately, dual RAASi agents can lead to hyperkalemia and subsequent stopping of one of the RAASi agents. The AMBER trial was helpful in looking at using dual RAASi agents and the ability to thwart stopping them as a result of hyperkalemia.
A recent Kidney Disease Improving Global Outcomes (KDIGO) Controversies Conference has addressed use of potassium binders to enhance RAASi use.39 This group of experts looked at all available data up to 2020 concerning potassium outcomes and treatment options available. Patiromer and other oral potassium lowering agents were recommended to treat hyperkalemia, especially in long-term use to promote maximal use of RAASi. The lower adverse events and side effects of patiromer and SZC were highlighted as a strong reason to consider their use over SPS. The 2021 European Society of Cardiology Guidelines for heart failure management also recommend starting an oral potassium binder when potassium >5.0 mEq/L.40 The guidelines also recommend maintenance use of the binder until an alternative treatment for hyperkalemia is identified. Only once potassium is >6.5 mEq/L is a RAASi dose recommended to be titrated down or stopped completely while taking an oral potassium binder like patiromer.
Additionally, an even more recent retrospective study was published by Leon et al in 2022 looking at CKD patients and hyperkalemia.41 A cohort of almost 80,000 patients with de novo RAASi-related hyperkalemia was evaluated. With a mean potassium of 5.7 mEq/L and eGFR 41 mL/min/1.73 m2, RAASi discontinuation was associated with an increased risk of all-cause mortality, cardiovascular mortality, and dialysis initiation. While these data align with previous studies and knowledge, they continue to add to the data that RAASi make a major difference in mortality in patients with CKD. Stopping RAASi is not without risk long term, and if we can use therapeutic maneuvers and medicine to avoid their discontinuation, we likely will improve overall morbidity and mortality in the long run.
Previously when SPS was the only oral potassium binder available, chronic use was not tolerable by most patients, and many clinicians only used it episodically for hyperkalemia. Now with the novel oral potassium binders such as patiromer, the gastrointestinal side effects and safety data allow for chronic daily use for years. This has created a paradigm shift in thinking of how patiromer can be used to enhance other medications that may induce hyperkalemia risk. Combination of RAASi agents, the reintroduction of variable NSAID use in CKD patients, and even considering high potassium foods with the use of patiromer are being studied and used in the real-world setting. As of writing, the FDA label does not indicate patiromer or any other oral potassium binder as an agent to enhance RAASi use. This is still off label per FDA direction, but major guideline societies are increasingly recommending oral potassium binders as a tool to enhance clinical outcomes. It is the opinion of the authors that oral potassium binders should no longer be thought of as “rescue” medications, but concomitant tools to enhance guideline medication use.
Future
Patiromer has been shown to be safe and effective in patients with hyperkalemia, but there are still many questions to be answered and different populations that need additional data. A Cochrane review looking at 15 studies using 1849 randomized adults with oral potassium binders vs placebo covers these and other data extensively.1 The review pools outcomes and reveals that many questions remain unanswered for oral potassium binder use. There are several clinical trials ongoing that will further determine safety, effectiveness, and tolerability in patient cohorts that were not fully captured in the initial FDA approval trials. One of the largest trials that is nearing publication is the DIAMOND trial by Butler et al.42 This trial will be a prospective, double-blinded, randomized trial of heart failure with reduced ejection fraction (HFrEF) patients who have a potassium level > 5.0 mEq/L while receiving dual RAASi medications. The original endpoint was to study optimization of RAASi therapy on time to CV death or first CV hospitalization, but needed to be amended due to the COVID-19 pandemic and enrollment challenges, as experienced by many prospective trials. The new primary endpoint will be a change in potassium levels from baseline, with secondary endpoints relating to CV outcomes, death, and RAASi modification. While the hard outcomes likely will not be answered in this trial due to enrollment challenges, this will be the largest trial to date to assess impact of patiromer on patients with HFrEF following guideline-directed RAASI medication. This highly anticipated trial regarding patients with advanced HFrEF should be released in 2022.
Several smaller trials are ongoing or actively recruiting regarding patiromer use. A prospective trial is of 40 hemodialysis patients who will receive daily patiromer and thrice-weekly dialysis. The proof-of-concept study will determine if patiromer changes hyperkalemia risk with a goal of a planned large-scale clinical trial (Clinicaltrials.gov: NCT03781089). Another prospective trial TAPCAT will look at kidney transplant patients to determine if immunosuppressive medications have any interaction or involve a change in AUC, a change in magnesium levels, or other unknown outcomes (Clinicaltrials.gov: NCT05029310). A larger-scale trial named PLATINUM is looking at hyperkalemia in emergency departments. Patients will receive emergent medications, either intravenous or inhaled, and be randomized to patiromer or placebo. The study’s aim is to determine use in emergent settings and the need for additional treatments including dialysis (Clinicaltrials.gov NCT: 04443608).
One speculation about using patiromer off label is the ability to resume high potassium, nutritious fruits and vegetables into the diets of patients with CKD and HF. Currently this is not indicated in the patiromer label by the FDA. A small group of 40 adults will be studied over 52 weeks and will be instructed to increase fruit and vegetables in a diet diary while simultaneously taking patiromer daily. Quality of life, kidney function, potassium, magnesium, and other nutrition-focused labs will be assessed (Clinicaltrials.gov: NCT 05050110). A group that has not been formally studied with patiromer are children and adolescents, with further trials forthcoming. The EMERALD trial will study 54 patients less than 18 years old with potassium between 5.1–6.5 mEq/L who will be given patiromer at separate doses to determine change in potassium, safety, and tolerability. This phase 2 study should hopefully open the door to large-scale phase 3 trials with the hopes of extending patiromer use to pediatric populations (Clinicaltrials.gov: NCT03087058). The SONG-CKD trial may be published in 2022–2023 and these consensus outcomes should be incorporated as well.43 The authors anticipate this trial to add value to growing evidence of patient-important outcomes and concerns.
The largest trial on the horizon for patiromer study is the RELIEHF study by the National Health Service in England (ClinicalTrials.gov: NCT04142788). This study will enroll 2000 patients with HFrEF and will investigate whether patiromer allows patients with worsening heart failure to tolerate higher doses of MRAs. These patients will be registered and followed for up to 10 years to determine HF worsening, hospitalization, quality of life, and death. While this study has a long way to go before reporting hard clinical outcomes with the enhancement of MRAs in heart failure patients, these data are desperately needed. The hope is that RELIEHF will give us some of the answers we were looking for in the original DIAMOND protocol. Future studies should focus on patient-reported outcomes, cardiac changes, and mortality. A Cochrane review by Das showed that significant mortality data are still lacking for patiromer, and further hard outcome trials are warranted.44 These relevant outcomes that matter to clinicians and patients would add to further strengthen patiromer use in the real world. As well, we currently do not have any randomized head to head trials of patiromer, SZC, and SPS. This will be important to show both side effect profile, tolerability, and efficacy.
As patiromer continues to be used around the world, ongoing real-world data are being collected and analyzed. Patiromer is being used in both on label and off label scenarios, and there is much to be learned about tolerability and long-term outcomes in different clinical situations. As of this publication, SPS remains the dominant oral potassium binder around the world, despite two novel potassium binders available that have more data published on safety and outcomes. As clinicians and prescribers become more comfortable with using patiromer, we may see improvements in potassium safety, RAASi safety, and hard outcomes of CV events and death. These data will be welcomed by the medical community as the optimal use of patiromer remains to be established.
Disclosure
Dr Colbert reports consulting fees paid by Vifor Pharma and AstraZeneca but no funding for this manuscript. Dr Lerma reports Advisory Board fees paid for by Vifor Pharma and AstraZeneca. The authors report no other conflicts of interest in this work.
References
1. Natale P, Palmer SC, Ruospo M, Saglimbene VM, Strippoli GF. Potassium binders for chronic hyperkalaemia in people with chronic kidney disease. Cochrane Database Syst Rev. 2020;6(6):CD013165. doi:10.1002/14651858.CD013165.pub2
2. Palmer BF. A physiologic-based approach to the evaluation of a patient with hyperkalemia. Am J Kidney Diseases. 2010;56:387–393. doi:10.1053/j.ajkd.2010.01.020
3. Kessler C, Ng J, Valdez K, et al. The use of sodium polystyrene sulfonate in the inpatient management of hyperkalemia. J Hosp Med. 2011;6:136–140. doi:10.1002/jhm.834
4. Scherr L, Ogden DA, Mead AW, et al. Management of hyperkalemia with a cation-exchange resin. N Engl J Med. 1961;264:115–119. doi:10.1056/NEJM196101192640303
5. Flinn RB, Merrill JP, Welzant WR. Treatment of the oliguric patient with a new sodium-exchange resin and sorbitol; a preliminary report. N Engl J Med. 1961;264:111–115. doi:10.1056/NEJM196101192640302
6. Watson MA, Baker TP, Nguyen A, et al. Association of prescription of oral sodium polystyrene sulfonate with sorbitol in an inpatient setting with colonic necrosis: a retrospective cohort study. Am J Kidney Dis. 2012;60(3):409–416. doi:10.1053/j.ajkd.2012.04.023
7. Lokelma. Package insert. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/207078s000lbl.pdf.
8. Veltassa. Package insert. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/205739s016lbl.pdf.
9. Fordtran JS, Locklear TW. Ionic constituents and osmolality of gastric and small-intestinal fluids after eating. Am J Dig Dis. 1966;11:503–521. PMID: 5937767. doi:10.1007/BF02233563
10. Sandle GI, Hunter M. Apical potassium (BK) channels and enhanced potassium secretion in human colon. QJM Mon J Assoc Physicians. 2010;103:85–89. PMID: 19892809. doi:10.1093/qjmed/hcp159
11. Li L, Harrison SD, Cope MJ, et al. Mechanism of action and pharmacology of patiromer, a nonabsorbed cross-linked polymer that lowers serum potassium concentration in patients with hyperkalemia. J Cardiovasc Pharmacol Ther. 2016;21:456–465. PMID: 26856345. doi:10.1177/1074248416629549
12. Pitt B, Garza D. The tolerability and safety profile of patiromer: a novel polymer-based potassium binder for the treatment of hyperkalemia. Expert Opin Drug Saf. 2018;17:525–535. PMID: 29667438. doi:10.1080/14740338.2018.1462335
13. Rossignol P, David L, Chan C, Conrad A, Weir MR. Safety and tolerability of the potassium binder patiromer from a global pharmacovigilance database collected over 4 years compared with data from the clinical trial program. Drugs Real World Outcomes. 2021;8:315–323. PMID: 34018121. doi:10.1007/s40801-021-00254-7
14. Bhattarai S, Pupillo S, Man Singh Dangol G, Sarac E. Patiromer acetate induced hypercalcemia: an unreported adverse effect. Case Rep Nephrol. 2019;2019:3507407. PMID: 30863649. doi:10.1155/2019/3507407
15. Wiederkehr MR, Mehta AN, Emmett M. Case report: patiromer-induced hypercalcemia. Clin Nephrol Case Stud. 2019;7:51–53. PMID: 31410346. doi:10.5414/CNCS109782
16. Bakris GL, Pitt B, Weir MR, et al. Effect of patiromer on serum potassium level in patients with hyperkalemia and diabetic kidney disease: the AMETHYST-DN randomized clinical trial. JAMA. 2015;314:151–161. PMID: 26172895. doi:10.1001/jama.2015.7446
17. Bushinsky DA, Spiegel DM, Gross C, et al. Effect of patiromer on urinary ion excretion in healthy adults. Clin J Am Soc Nephrol CJASN. 2016;11:1769–1776. PMID: 27679518. doi:10.2215/CJN.01170216
18. Weir MR, Bakris GL, Bushinsky DA, et al. Patiromer in patients with kidney disease and hyperkalemia receiving RAAS inhibitors. N Engl J Med. 2015;372:211–221. PMID: 25415805. doi:10.1056/NEJMoa1410853
19. Pergola PE, Spiegel DM, Warren S, Yuan J, Weir MR. Patiromer lowers serum potassium when taken without food: comparison to dosing with food from an open-label, randomized, parallel group hyperkalemia study. Am J Nephrol. 2017;46:323–332. PMID: 29017162. doi:10.1159/000481270
20. Ag M, Ma G, Lz G, Mr S. Patiromer: a clinical review. Curr Med Res Opin. 2016;32. PMID: 26456884. doi:10.1185/03007995.2015.1106935
21. Bushinsky DA, Williams GH, Pitt B, et al. Patiromer induces rapid and sustained potassium lowering in patients with chronic kidney disease and hyperkalemia. Kidney Int. 2015;88:1427–1433. PMID: 26376130. doi:10.1038/ki.2015.270
22. Pitt B, Anker SD, Bushinsky DA, et al. Evaluation of the efficacy and safety of RLY5016, a polymeric potassium binder, in a double-blind, placebo-controlled study in patients with chronic heart failure (the PEARL-HF) trial. Eur Heart J. 2011;32:820–828. PMID: 21208974. doi:10.1093/eurheartj/ehq502
23. Agarwal R, Rossignol P, Romero A, et al. Patiromer versus placebo to enable spironolactone use in patients with resistant hypertension and chronic kidney disease (AMBER): a phase 2, randomised, double-blind, placebo-controlled trial. Lancet Lond Engl. 2019;394:1540–1550. PMID: 31533906. doi:10.1016/S0140-6736(19)32135-X
24. Rafique Z, Liu M, Staggers KA, et al. Patiromer for treatment of hyperkalemia in the emergency department: a pilot study. Acad Emerg Med. 2020;27:54–60. doi:10.1111/acem.13868
25. Rattanavich R, Malone AF, Alhamad T. Safety and efficacy of patiromer use with tacrolimus in kidney transplant recipients. Transplant Int. 2019;32:110–111. doi:10.1111/tri.13369
26. Lim MA, Sawinski D, Trofe-Clark J. Safety, effectiveness, and tolerability of patiromer in kidney transplant recipients. Transplantation. 2019;103:e281–e282. doi:10.1097/TP.0000000000002829
27. Schnelle K, Winters H, Pesavento T, Singh P. Largest experience of safety and efficacy of patiromer in solid organ transplant. Transplant Direct. 2020;6(9):e595. doi:10.1097/TXD.0000000000001037
28. Kovesdy CP, Gosmanova EO, Woods SD, et al. Real-world management of hyperkalemia with patiromer among United States Veterans. Postgrad Med. 2020;132(2):176–183. doi:10.1080/00325481.2019.1706920
29. Kovesdy CP, Rowan CG, Conrod A, et al. Real-world evaluation of patiromer for the treatment of hyperkalemia in hemodialysis patients. Kidney Int Rep. 2019;4:301–309. doi:10.1016/j.ekir.2018.10.020
30. Amdur RL, Paul R, Barrows ED, et al. The potassium regulator patiromer affects serum and stool electrolytes in patients receiving hemodialysis. Kidney Int. 2020;98(5):1331–1340. doi:10.1016/j.kint.2020.06.042
31. Murea M, Patel A, Highland BR, et al. Twice-weekly hemodialysis with adjuvant pharmacotherapy and transition to thrice-weekly hemodialysis: a pilot study. Am J Kidney Dis. 2021. doi:10.1053/j.ajkd.2021.12.001
32. Desai NR, Rowan CG, Alvarez PJ, et al. Hyperkalemia treatment modalities: a descriptive observational study focused on medication and healthcare resource utilization. PLoS One. 2020;15:e0226844. doi:10.1371/journal.pone.0226844
33. Lewis EJ, Hunsicker LG, Clarke WR, et al. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med. 2001;345(12):851–860. doi:10.1056/NEJMoa011303
34. Brenner BM, Cooper ME, de Zeeuw D, et al. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med. 2001;345(12):861–869. doi:10.1056/NEJMoa011161
35. CONSENSUS Trial Study Group. Effects of enalapril on mortality in severe congestive heart failure: results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). N Engl J Med. 1987;316(23):1429–1435. doi:10.1056/NEJM198706043162301
36. Epstein M, Alvarez PJ, Reaven NL, et al. Evaluation of clinical outcomes and costs based on prescribed dose level of renin-angiotensin-aldosterone system inhibitors. Am J Manag Care. 2016;22(11 Suppl):s311–s324.
37. Trevisan M, de Deco P, Xu H, et al. Incidence, predictors and clinical management of hyperkalaemia in new users of mineralocorticoid receptor antagonists. Eur J Heart Fail. 2018;20:1217–1226. doi:10.1002/ejhf.1199
38. Trevisan M, Fu EL, Xu Y, et al. Stopping mineralocorticoid receptor antagonists after hyperkalaemia: trial emulation in data from routine care. Eur J Heart Fail. 2021;23:1698–1707. doi:10.1002/ejhf.2287
39. Clase CM, Carrero JJ, Ellison DH, et al. Potassium homeostasis and management of dyskalemia in kidney diseases: conclusions from a kidney disease: improving global outcomes (KDIGO) controversies conference. Kidney Int. 2020;97:42–61. doi:10.1016/j.kint.2019.09.018
40. McDonagh TA, Metra M, Adamo M, et al.; ESC Scientific Document Group. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: developed by the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2022;24(1):4–131. doi:10.1002/ejhf.2333
41. Leon SJ, Whitlock R, Rigatto C, et al. Hyperkalemia-related discontinuation of renin-angiotensin-aldosterone system inhibitors and clinical outcomes in CKD: a population-based cohort study. Am J Kidney Dis. 2022. doi:10.1053/j.ajkd.2022.01.002
42. Butler J, Anker SD, Siddiqi TJ, et al. Patiromer for the management of hyperkalaemia in patients receiving renin-angiotensin-aldosterone system inhibitors for heart failure: design and rationale of the DIAMOND trial. Eur J Heart Fail. 2021. doi:10.1002/ejhf.2386
43. Evangelidis N, Sautenet B, Madero M, et al. Investigators standardised outcomes in nephrology - chronic kidney disease (SONG-CKD): a protocol for establishing a core outcome set for adults with chronic kidney disease who do not require kidney replacement therapy. Trials. 2021;22(1):612. doi:10.1186/s13063-021-05574-1
44. Das S, Dey JK, Sen S, Mukherjee R. Efficacy and safety of patiromer in hyperkalemia: a systematic review and meta-analysis. J Pharm Pract. 2018;31(1):6–17. doi:10.1177/0897190017692921
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.