")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 15
Children’s Adherence to Antiretroviral Therapy and Associated Factors: Multicenter Cross-Sectional Study
Authors Gemechu GB , Hebo H , Kura Z
Received 22 March 2023
Accepted for publication 11 July 2023
Published 21 July 2023 Volume 2023:15 Pages 423—434
DOI https://doi.org/10.2147/HIV.S407105
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Getahun B Gemechu,1 Habtemu Hebo,2 Zarihun Kura2
1Ilu Woreda Health Office, Shaggar, Oromia Regional State, Ethiopia; 2Epidemiology Department, Jimma University, Jimma, Oromia Regional State, Ethiopia
Correspondence: Getahun B Gemechu, Email [email protected]
Background: Poor adherence to antiretroviral therapy (ART) causes drug resistance, treatment failure and death. Studies conducted among children below 15 years were limited in Ethiopia in general and in the study area. Therefore, this study aimed to assess the status of children’s adherence to ART and associated factors in the study area.
Methods: We conducted a facility-based cross-sectional study from April 1 to May 10, 2020 by including 282 children < 15 years. All children who received ART for at least one month and attend ART clinic during data collection period were consecutively recruited. Face-to-face interview was conducted using a standardized questionnaire. Both bivariate and multivariate logistic regression were performed. Adherence and exposure variables (i.e., sociodemographic and reason for missing) were measured by the caregivers/children’s report of a one-month recall of missed doses.
Results: Among 282 caregivers included with their children, 226 (80.2%) were females (mean age = 38.6 and SD = 12.35) and half (50%) of children were females. Two hundred forty six (87.2%) children were aged between 5– 14 years (mean age = 8.5 and SD = 2.64), and 87.2% were adhered (≥ 95%) to ART in the month prior to the interview. Children whose caregivers were residing in urban were 3.3 (95% CI: 1.17, 9.63) times more adherent to ART than their counterparties. Children whose caregivers were biological parents were 2.37 (95% CI: 1.59, 3.3) times more adherent than children with non-biological parents. Children with knowledgeable caregivers about ART were 4.5 (95% CI: 1.79, 9.8) times more adherent to ART.
Conclusion and Recommendation: Children’s adherence to ART in our study area was sub optimal. Biological caregivers, residing in urban and being knowledgeable about ART facilitate adherence to ART. Adherence counseling targeting non-biological parents and for those who come from rural areas were recommended.
Keywords: adherence, antiretroviral therapy, children, Ethiopia, ART
Background
Globally there were an estimated 37.7 million (35.9 million adults and 1.8 million 0–14 years children) people living with HIV in 2020, over two thirds of whom (25.4 million) are in the WHO African Region.1 At the end of 2019, in Ethiopia, 610,335 people were living with HIV (PLWHIV), in which 62,168 were children under the age of 15.2
In response to HIV/AIDS pandemic, multiple strategies including treatment of patients with Anti-Retro Viral Therapy (ART) have been implemented worldwide to curb the epidemics.3 According to Ethiopian ART guideline, ART should started as early as possible (even the same day with diagnosis of HIV if patient is ready) to all children living with HIV regardless of their WHO clinical stages and CD4 counts/percentage. The preferred first line for all children is AZT or ABC or TDF + 3TC + LPV/r and the preferred 2nd line AZT or ABC or TDF + 3TC + EFV/NVP.4
An important factor in achieving treatment success specially in children is maintaining optimal adherence to ART.3,5,6 Adherence to antiretroviral treatment is defined as taking 95% or more of the prescribed doses on time and in the correct way, either with or without food.3,7 Adherence can be measured using self-report, viral load monitoring, pill count and pharmacy refill records.4 Among these, viral load monitoring is the gold standard for monitoring adherence and confirming treatment response.4,8,9 It introduce as routine activity since 2015/16 in Ethiopia and the national guideline recommended that, every stable PLWHIV receiving ART should monitored using VL every 12 months.4 Even though UNAIDS set a target of 95-95-95,1 currently in Ethiopia, viral load test is 73% and viral suppression is 78.9% among children below 15 years.8
According to a global HIV/AIDS report, the status of adherence to ART among children living with HIV varied from 65% to 90%,10 75% in low and middle income countries11 and 88.8% in Ethiopia.12
Poor adherence to ART will lead to an increased risk of drug resistance, treatment failure and clinical deterioration with increased premature death in children.9,10,12
The causes of poor adherence to ART among pediatric patients are complex and interrelated factors. Total dependency of the child on caregiver, pill burden and dosing frequency, treatment side effects, poor health literacy, limited access to ART,13–15 socioeconomic status of the caregiver, substance use and access to service delivery, non-disclosure16,17 are among some factors. In addition, currently HIV services disrupted and public response is slowed due to COVID-19 restriction and lockdown, resulting in increasing HIV infection, lifting up lost to follow up and becoming barriers to adherence.18
The emergence of drug resistant HIV among children adds an enormous burden.19 It may lead to further spread of resistant virus through vertical and horizontal transmission once the child reaches adolescence and adulthood.19,20
Therefore, designing strategies for maintaining the optimal status of adherence among children, is essential to ensure treatment success. However, the task requires careful assessment of the status of adherence and age specific factors.21 Studies on adherence to ART and associated factors among children below 15 years of age are limited in Ethiopia, in general and in the study area. Additionally, adherence is not static and can vary with time on treatment, making assessing adherence status crucial.17 Moreover, viral load was added as one variable in this study, which has not been researched in previous studies. Therefore, this study aimed to examine the status of adherence and associated factors among children under the age of 15 years in the study area.
Methods and Materials
Study Design, Area and Period
A facility-based cross sectional study was conducted from April 1 to May 10, 2020 in the Sebeta, Teji, Tullu Bollo and Waliso towns which are located 20 km, 50 km, 65 km and 114 km away from Addis Ababa, respectively (Figure 1). These towns were, in the southwestern direction along the main road from Addis Ababa to Jimma. In total, there are 8 public ART sites included in all 4 towns. Three of the public ART sites are within Sebeta town (Sebeta health center provide ART services for 41 under 15 children, while 21 and 09 are served in Alemgena and Tefki health center respectively. Two public ART sites are found in Tullu Bolo town. Tullu Bolo General Hospital serves 25 children living HIV and Tullu Bolo health center provides services for 17 children living with HIV. Teji town also, has Teji health center who provide services for 18 children under 15. The rest are found in Waliso town (St. Lukes Referral Hospital serves 130 and Waliso health center serves 29 children under 15). In total, 290 children are on ART in those health facilities. These health facilities have case managers and adherence supporters, who promote adherence by giving advice for client on ART.
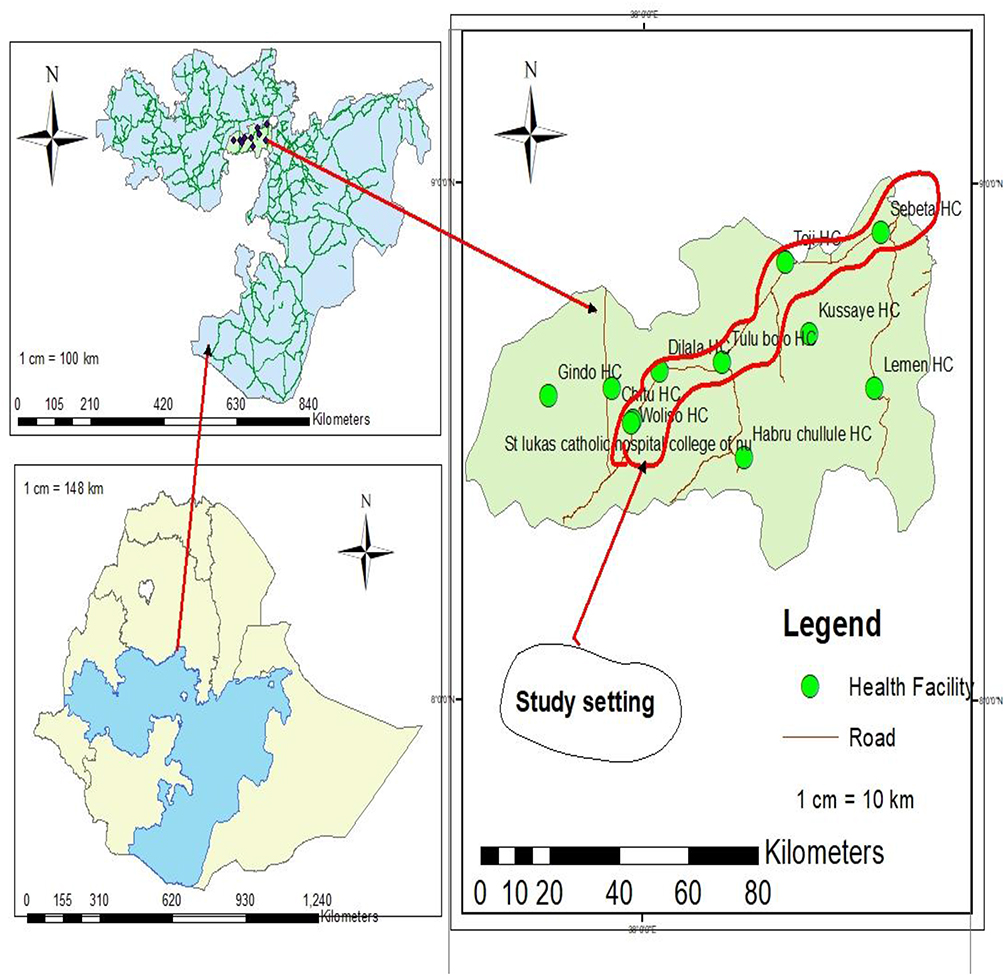 |
Figure 1 Map of study area and study setting of the study conducted at central Ethiopia, 2020. |
Sample Size and Sampling Technique and Inclusion Criteria
Sample size was calculated using STAT CALC of Epi-info by taking disclosed child as associated factors identified by previous study that provide the ratio of unexposed to exposed 0.6, outcome in the exposed group 49%, and outcome in the unexposed group 29.5%.22 And also 95% CI and power 80% was used to calculate sample size and adding 10% nonresponse rate, the total sample size was 254.
However, currently children who are taking ART and being followed up at public ART site of those health facilities were totally 290. Therefore, rather than minimizing 36 extra children, we had included all those children to the study. Therefore, all children/caregivers who fulfill inclusion criteria (who treated with ART at least one month) and attending ART clinic at each facilities were consecutively recruited to the study as they come to refill their medication on the appointment day.
Data Collection Tool and Method
Data were collected by 8 clinical nurses using structured questionnaires and face-to-face interviews, were held with mothers/caregivers. The data collection process was supervised by one health officer and one BSc nurse. Adherence and exposure variables were measured by the caregivers’ or children’s report of a one-month recall of missed doses prior to the date of the interview. Medical records were reviewed to collect clinical data such as WHO clinical stages, regimen type, viral loads (conducted in the last 12 months) and the CD4 counts (done in the last 6 months) of children.
Data Quality Assurance
Pretested and structured questionnaires was used for data collection. The questionnaires were adapted from previously conducted related studies22–24 and some changes were made after reviewing the relevant literature. It was initially prepared in English and translated to Afan Oromo and Amharic, commonly used local languages, using online Google translation. We gave two days training for data collectors and supervisors and a pre-test was done on five percent of the total sample size before the actual data collection in Awash health center. Based on the result of pre-testing, necessary revision like timing, skipping pattern and coherence was conducted.
Data Analysis
The questionnaires were coded and entered into the EPI Data software and exported to SPSS Windows version 23 for further analysis. Data were summarized and presented using descriptive and analytic statistics. Bivariate and multiple logistic regressions were computed to identify the presence and strength of associations. Variables with a p value <0.25, in binary logistic regression, were subjected to multiple logistic regression for analysis. However, before multiple logistic regression, collinearity diagnostic test was done and no multicollinearity (maximum Variance Inflation Factor [VIF] = 3.883). On the other hand, Breslow-Day test showed, there is significant synergetic interaction between two variables (i.e., child relationship with caregiver vs. caregiver ART history). As a result, the stratum specific odds ratio was considered to measure the strength of the association. At the end, multiple logistic regression (odds ratios with 95% CIs were computed) and variables with p-values less than 0.05 were considered significantly associated with the dependent variable. Finally, the model was fitted using the backward elimination method, and the Hosmer-Lemeshow goodness of fit test indicated a p-value of 0.47). Furthermore, cluster effect was also analyzed using hierarchical cluster analysis classifying into eight cluster. Thus, dendrogram plot result using ward’s method showed that there were higher similarity among each cluster.
Operational Definition
Adherent to ART – when the child has missed ≤1 dose or takes ≥95% of ART in the month prior to the interview.
Non adherent to ART – missing at least two doses or takes <95% of ART in the month prior to interview.
Care givers – Parent/guardian or person in charge of routinely administering antiretroviral drugs to children on ART.
Baseline CD4 count – CD4 count done when a child started ART.7
Current CD count – CD4 count done within 6 months of data collection.7
Knowledge about ART – Those respondents who scored greater than or equal to the mean for the knowledge questions were considered knowledgeable; otherwise, they were not.
Care giver/child substance use – if caregiver/child use either of alcohol, khat, cigarettes or other substance in the month prior to data collection.
Ethical Considerations
Ethical clearance letters were obtained from the Ethical Review Committee, Jimma University, Institute of Health and from Ethical and research committee of Oromia national regional health bureau. The interviews were conducted after informed verbal consent/assent and assurance of confidentiality. This is because the participants in this study were mothers/caregivers in which many of them were carriers of HIV and do not want to give written consent due to suspect that it will take away their privacy as it identified during pretest and, since there is also no any harm procedure. This non-written consent was documented and witnessed according article 26 of Helsinki declaration.
Results
Sociodemographic Characteristics of the Study Participants
Of the 290 study participants, 282 children, along with their caregivers, were included in the analysis, yielding a response rate of 97.2%. Four caregivers were excluded because they did not appear in the health facility during the data collection period. Three questionnaires were discarded as they were not complete (caregivers did not know the dosing history for the past month) and one caregiver was not willing to respond to the questionnaire (did not provide consent). Among the respondents, 226 (80.2%) of the caregivers were females, and the mean age of the respondents was 38.6 years (SD = 12.35). Out of the total respondents, 176 (62.5%) were married. One hundred fifty-eight (56%) of the caregivers attended primary education. Two hundred and nine (74.1%) of the caregivers were urban dwellers. Among the children included in the study, half (50%) were female, 246 (87.2%) were 5–14 years old with the mean age of 8.5 years (SD = 2.64). One hundred and eighty three (64.9%) children are currently attending 1–4 grades (Table 1).
 |
Table 1 Sociodemographic Characteristics of Study Participants, Central Ethiopia, April 1–May 10, 2020 (n=282) |
Clinical Characteristics of Study Participants
Among the children who participated in this study, 102 (36.2%) started ART at WHO clinical stage I and 273 (96.8%) were currently on WHO stage I. At initiation of ART, 142 (50.4%) children had a CD4 count of >500 cells/mm3. During data collection, viral load was done for 206 (73%) children and out of these, high viral load (≥1000 copies/mL) was detected in 55 (19.5%) children (Table 2).
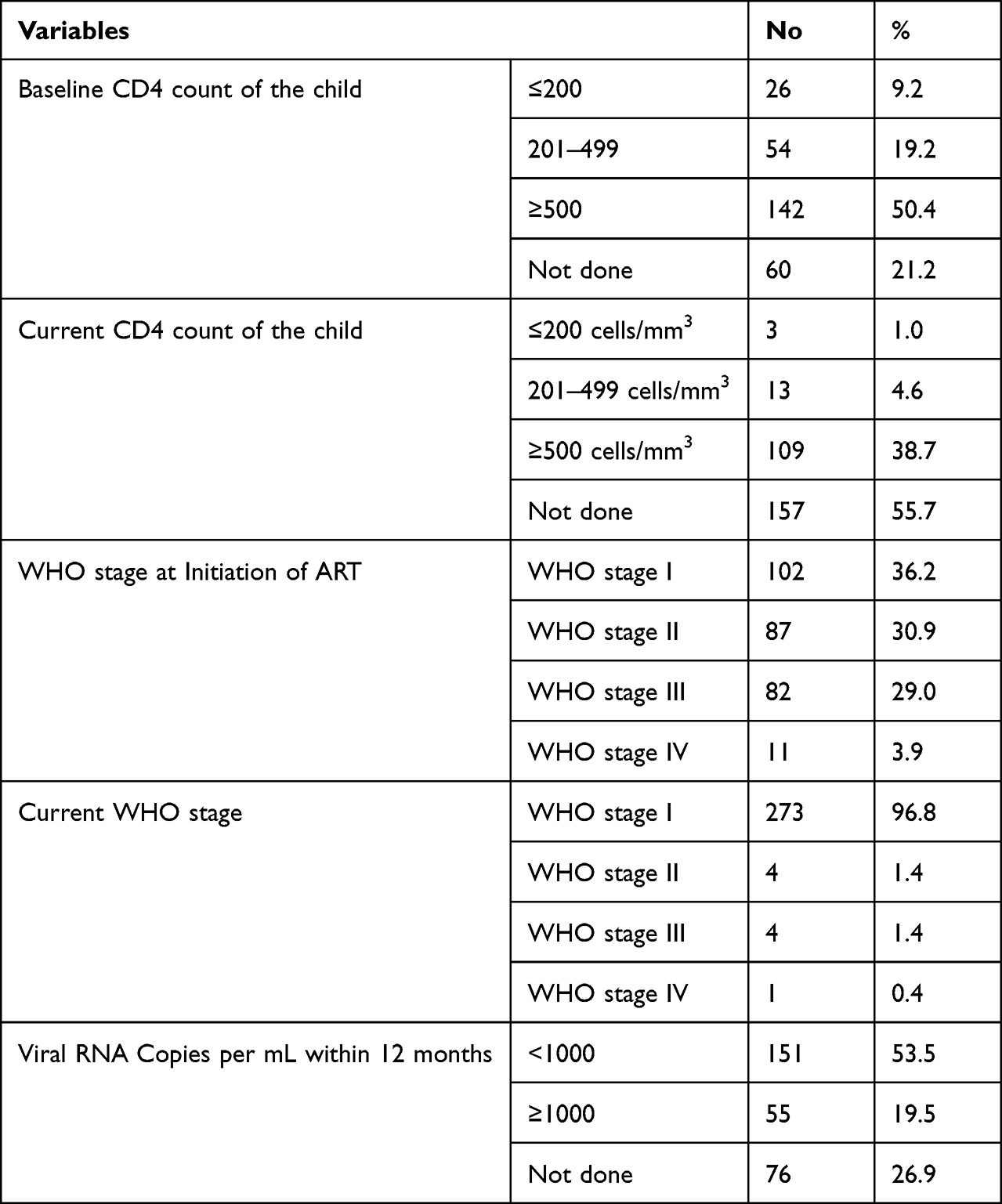 |
Table 2 Clinical Characteristics of Study Participants, in Central Ethiopia, April 1–May 10, 2020 (n=282) |
ART and Other Drug History of the Children
Among the children included in the study, 270 (95.8%) were on 1st line ART medication and 195 (69.2%) of the children were taking 2 pills/day while 38 (13.4%) of the children were taking 3 doses. (Table 3).
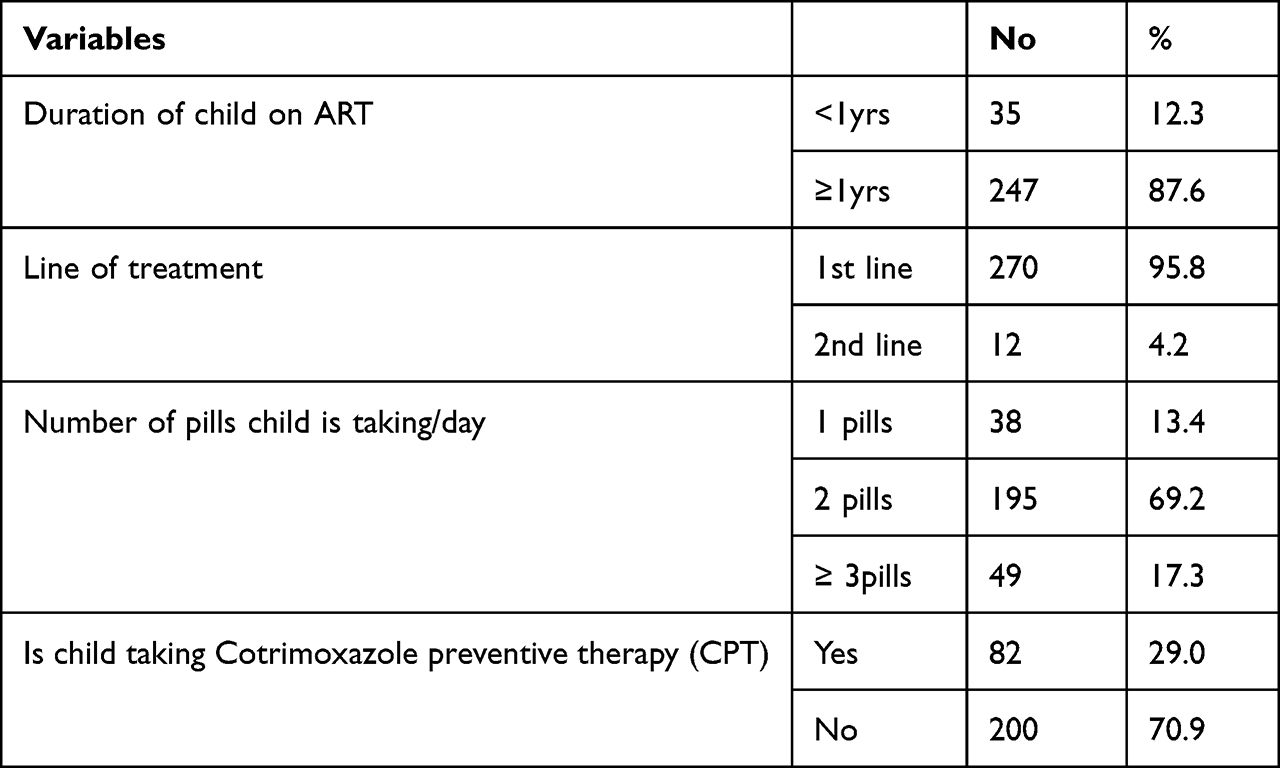 |
Table 3 ART and Other Drug History of Study Participants in Central Ethiopia, April 1–May 10, 2020 (n = 282) |
In addition, according to current, 176 (62.4%) are on AZT-3TC-NVP and 47 (15.6%) are on AZT-3TC-EFV regimen. Only 6 (2%) of the children who are currently on ART have been taking AZT – based LPV/r (boosted drug with Protease inhibitor) (Figure 2).
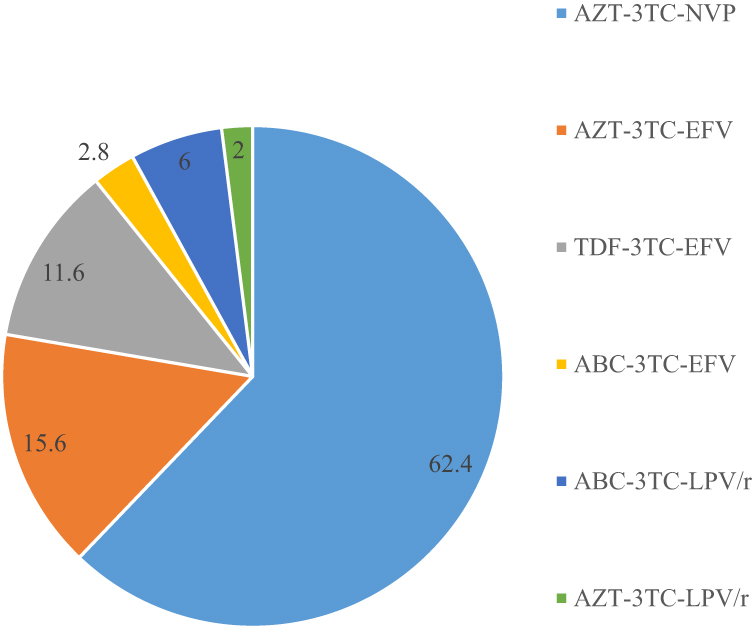 |
Figure 2 Type of ART regimen children currently taking in percent at, central Ethiopia, April 1–May 10, 2020. |
Adherence Status of the Children to ART
Based on the caregivers’ report, a total of 246 (87.2%, [95% CI: 83.3–91.1%]) children had an adherence status of ≥95% in the month prior to interview. The status of adherence to ART among children in the past three and seven days before the interview date was 98.9% and 95.8%, respectively.
Reasons for Non-Adherence
According to the current study, 36 (12.8%) of the children missed at least 2 doses out of their prescribed doses of which, 30 (10.6%) were among in age group of 5–14 years. The commonly mentioned reasons were: fear of stigma (21.3%), caregiver’s forgetfulness (14.2%), child’s refusal to take the drugs (13.8%) and run out of medication (13.8%) (Figure 3).
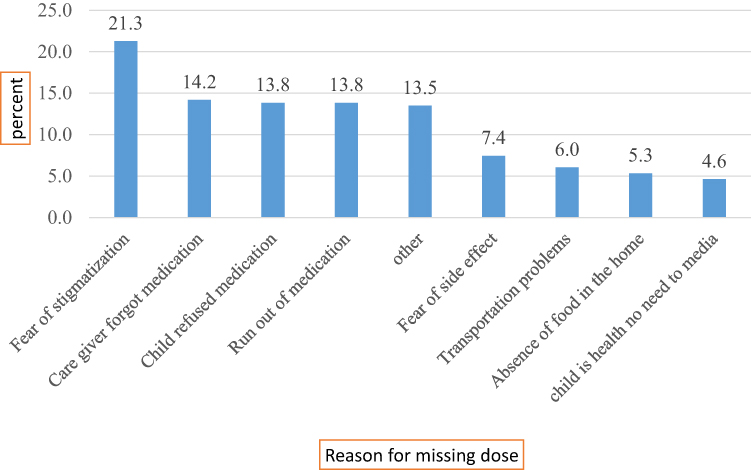 |
Figure 3 Reason for non-adherence to ART drugs among children at study area, central Ethiopia, April 1–May 10, 2020. |
Distance from Health Facility and Mode of Transportation
Out of the total caregivers/children who participated in the study, majority, 219 (77.7%) came from less than 10 km and 113 (40.1%) of the participants came to the health facility on foot (Table 4).
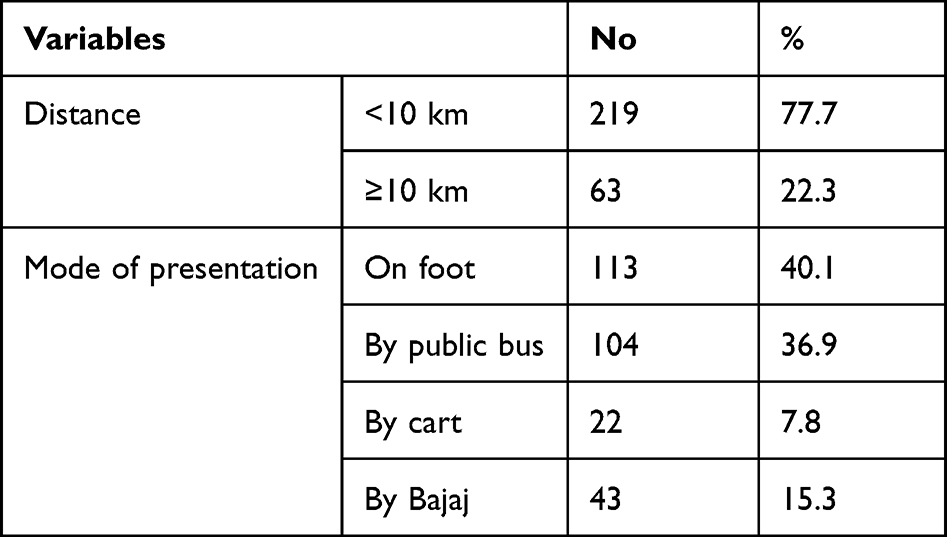 |
Table 4 Distance from Health Facility and Mode of Transportation of Study Participant to Refill Medication, Central Ethiopia, May 10, 2020 (n = 282) |
Factors Associated with Adherence to ART
In multiple logistic regression, the residence area of caregivers, blood relationship between children and caregivers and knowledge of caregivers about ART treatment, were significantly and independently associated with adherence. Children whose caregivers resided in urban areas were 3.3 times more likely adherent to ART than their counterparties (AOR = 3.3 [95% CI: 1.17, 9.63]). Children whose caregivers were biological parents were 2.37 times more likely to be adherent than those whose caregivers were non-biological parents (AOR = 2.37 [95% CI: 1.59, 3.2]). The present study also showed that if the caregiver was knowledgeable about ART treatment, the child was 4.5 times more likely to be adhere to ART (AOR = 4.5 [95% CI: 1.79, 9.8]) (Table 5).
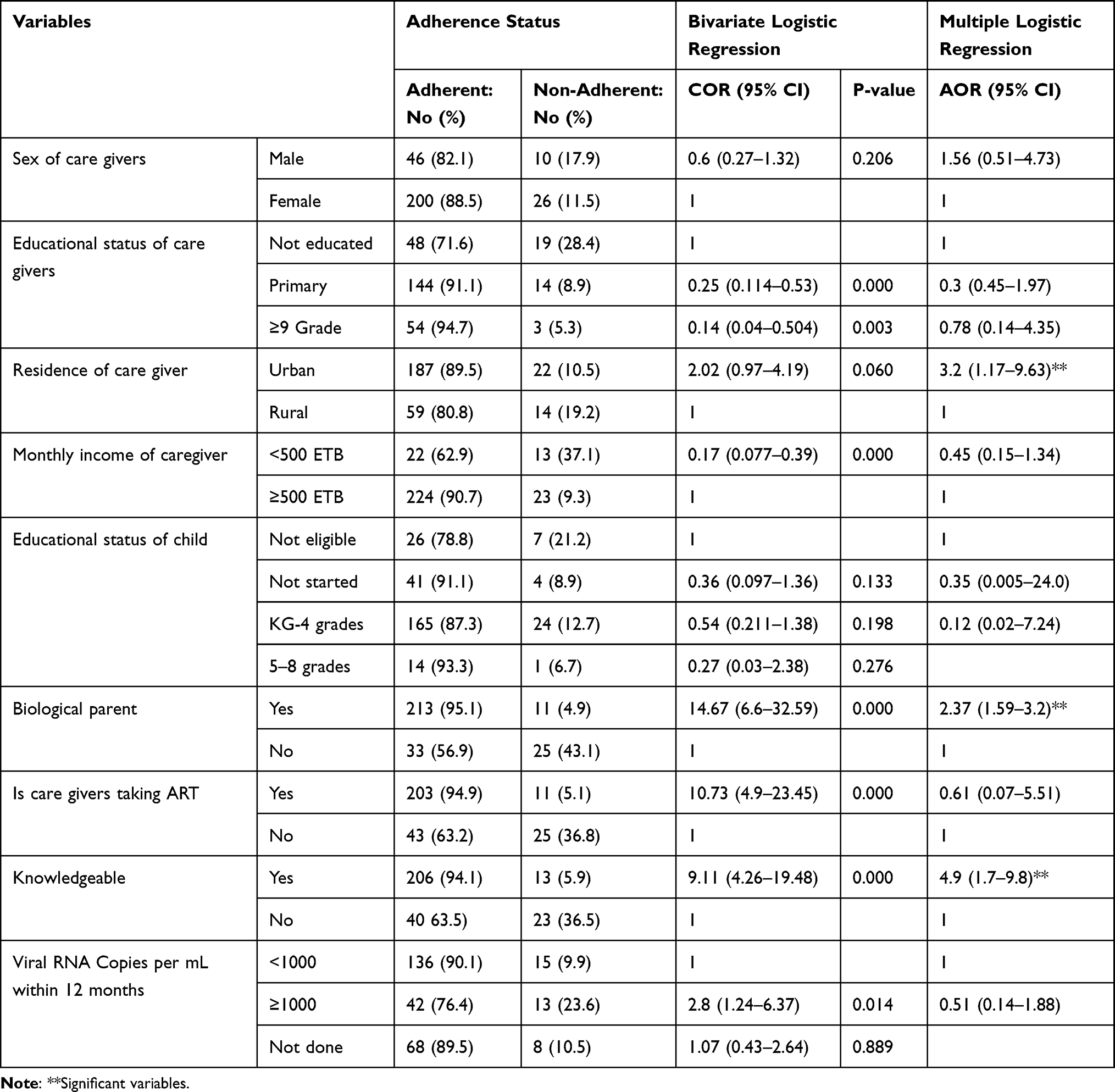 |
Table 5 Crude and Adjusted Odds Ratios and 95% Confidence Intervals (CIs) of Explanatory Variables of Adherence to HAART in the Study Area, Central Ethiopia, April 1–May 10, 2020 (n = 282) |
Discussion
According to this study, 87.2% of children had an adherence status of ≥95% in the month prior to the interview. This is higher than the finding of global pooled estimation, which is 65%−75%.25 This difference could be due to the context of the study area (i.e., specific study area among children living in almost similar sociodemographic characteristics vs. global context). In addition, the global pooled estimate used secondary data. However, our finding was comparable with an studies in East Africa 90%;26 in Southeastern Nigeria, 91%;27 Ethiopian national pooled prevalence of optimal HAART adherence 88.8%;12 Eastern Ethiopia, 90.7%,28 Tigray, Northern Ethiopia, 90.7%;29 in Gondar University Hospital and Gondar Poly Clinic, 90.4%;30 and in Addis Ababa, 86.9%.31 However, the finding of the current study was higher than the finding of study conducted in India, which revealed an overall adherence of 82.1%.32 This difference might be due to the study design (cross-sectional vs. cohort). It was also higher than that in a study in Uganda which reported an overall adherence status of 79.1%),33 North Ethiopia, provided an adherence status of 78.6%,22 and central Ethiopia showed an adherence rate of 74%.24 This difference could be due to the small sample size in central Ethiopia (120 vs. 282). Again, higher adherence rate was observed in our study when compared with finding of study conducted in the ART clinic of Tikur Anbessa Hospital, Addis Ababa (i.e., an adherence rate of children to ART was 34.8%).34 This difference was due to adherence assessment methods (caregiver’s report vs. unannounced home based pill count). This indicates that, self-report have less potential for the assessment of adherence when compared to pill count. In general, the current study finding of the adherence status of children to ART is below the recommendation of the WHO, which recommended that ≥90% of people on ART should be adherent to ART to fully benefit from ART.3 Additionally, among non-adherent children, 10.6% were children in range of 5–14 years old. This is justified by research conducted in Ambo, eastern Ethiopia.12 This is due to the fact that, most of the time older children played outside of the home and also due to schooling, they forget taking medication and this leads to miss a doses.
Regarding associated risk factors for non-adherence, the current study showed that children whose caregivers were biological parents were 2.37 times more adherent than those whose caregivers were non-biological parents (AOR = 2.37, 95 CI= [1.59–3.2]). This finding is similar to the cross-sectional study finding conducted in Hiwot Fana and Dil-Chora Referral Hospital in eastern Ethiopia, which revealed that children whose caregivers were biological parents were more adherent.
The other independently associated risk factor for adherence to ART among children identified by this study was caregivers’ knowledge of ART. Accordingly, we found that children with knowledgeable caregivers were 4.5 times more adherent than those children whose caregivers were not knowledgeable (AOR 4.5 95% CI [1.7–9.8]). Our finding is similar to the study finding conducted in Hiwot Fana and Dil-Chora Hospital, which revealed that caregivers of children with good knowledge about the disease were 7.3 times (AOR = 7.3) adherent than their counterparts.28 Again, our finding is also similar to the finding of a study conducted in India that came up with, children whose caregivers had good knowledge about ART treatment were 14.7 times more adherent.32 A similarly study conducted in north Ethiopia, justified our finding (AOR = 2.72).33 Our finding is again in line with the study finding conducted at University of Gondar Hospital and Gondar Poly Clinic, which showed that children of knowledgeable caregivers had 4.7 times more adherent to ART than their counterparts (AOR = 4.7).30 This implies that making caregivers knowledgeable about the importance of ART treatment through ongoing and extensive counseling is mandatory to make children more likely to benefit from good adherence to ART.
The current study also showed that children residing in urban areas were 3.2 times more adherent to ART than those residing in rural (AOR = 3.2 [95% CI 1.17–9.63]). This finding is supported by a study conducted in Tanzania that reported, suboptimal to ART was observed among children in the rural context of the Mwanza region.35 However, our study is contradicts a comparative study conducted between rural and urban children, in South Africa that revealed, rural children were more adherent to ART (93.1% vs. 88%).36 This difference might be due to the study design (cross-sectional vs. cohort). In general, this implies that urban dwellers have more access to information and education when compared with rural dwellers which benefit them to be more adherent to ART.
Our study is not free of limitations. There might be an overestimation of adherence status in our study because of self-report, recall and social desirability bias. Thus, to minimize this bias we used non ART providers as data collectors. Additionally, we did not assess adherence related to the correct timing of ART drug administration. Again, the cross-sectional nature of the study also hinders the causal relationship between adherence status and associated factors.
Conclusion and Recommendations
The adherence status of the children to ART in our study area was sub optimal. Children residing in urban areas, with biological caregivers and children of knowledgeable caregivers were more adherent to ART. Adherence counseling and health information dissemination should be strengthened targeting non-biological parents and for those who come from rural areas. Also other studies should be conducted using multiple and more objective adherence assessment tools (pill count, VL monitoring, etc.).
Acknowledgment
Our heartfelt thanks to Jimma University Institute of Public Health Department of Epidemiology for giving us this opportunity to conduct this study.
Funding
The research was not funded by producing company rather it was funded by the personal efforts of the authors.
Disclosure
The authors declare no competing interest for this work. The product used for this research are commonly and predominantly use products in our area of research and country. There is absolutely no conflict of between authors and producers of the product because we do not intent to use these product as an avenue for litigation but for the advancement of knowledge.
References
1. UNAIDS. Global HIV statistics, Fact Sheet – World AIDS Day 2021; 2021: 1–6.
2. PEPFAR. Ethiopia country operational plan (COP/ROP) 2018 strategic direction summary; 2018.
3. World Health Organization. The Use of Antiretroviral Drugs for Treating and Preventing HIV Infection. World Health Organization; 2016.
4. Republic FD of Ethiopia. National Consolidated Guidelines for Comprehensive HIV Prevention, Care and treatment. Republic FD of ethiopia; 2018:1–238.
5. Federal Democratic Republic of Ethiopia F. National Guidelines for HIV Prevention Treatment and Care National aids and Sti’s Control. Federal Democratic Republic of Ethiopia F; 2016.
6. PEPFAR. Differentiated care in Ethiopia. The way forward; 2017.
7. Federal Democratic republic of Ethiopia F. National Guide Lines for Comprehensive HIV Prevention, Care and Treatment. Federal Democratic republic of Ethiopia F; 2018.
8. FHAPCO. HIV/AIDS National Strategic Plan for Ethiopia, 2021–2025. FHAPCO; 2020:0–175.
9. UNAIDS. Country Factsheets Ethiopia|2021 HIV and AIDS Estimates. UNAIDS; 2021:1–5.
10. Iacob SA, Iacob DG, Jugulete G. Improving the adherence to antiretroviral therapy, a difficult but essential task for a successful HIV treatment—clinical points of view and practical considerations. Front Pharmacol. 2017;8:1–12.
11. Vreeman RC, Wiehe SE, Pearce EC, Nyandiko WM. A systematic review of pediatric adherence to antiretroviral therapy in low- and middle-income countries. Pediatr Infect J. 2008;27(8):686–691.
12. Endalamaw A, Tezera N, Eshetie S, Ambachew S, Dejenie T. Adherence to highly active antiretroviral therapy among children in Ethiopia: a systematic review and meta ‑ analysis. AIDS Behav. 2018;22(8):2513–2523. doi:10.1007/s10461-018-2152-z
13. Teju D, Kumilachew D, Belay A. First-line antiretroviral treatment failure and associated factors in HIV patients at the University of Gondar Teaching Hospital, Gondar, Northwest Ethiopia. HIV/AIDS Res Palliat Care. 2016;8:141–146. doi:10.2147/HIV.S112048
14. Mequanent M, Awoke T, Assefa AT, et al. Incidence and risk factors of first-line antiretroviral treatment failure among human immunodeficiency virus-infected children in Amhara regional state, Ethiopia a retrospective follow-up study. BMJ Open. 2016;10:1–10.
15. Sithole Z, Mbizvo E, Chonzi P, Mungati M, Patience Juru T, Shambira G; Notion Tafara Gombe and MT. Virological failure among adolescents on ART, Harare City, 2017 – a case-control study. BMC Infect Dis. 2018;18. doi:10.1186/s12879-018-3372-6
16. Nichols J, Steinmetz A, Paintsil E. Impact of HIV-status disclosure on adherence to antiretroviral therapy among HIV-infected children in resource-limited settings: a systematic review. AIDS Behav. 2016;20:1–11. doi:10.1007/s10461-015-1193-9
17. Schaecher KL. The importance of treatment adherence in HIV. AJMC. 2019;19(2):2019.
18. UNAIDS. Fact Sheet – global a I DS Update 2019. UNAIDS; 2019: 1–6.
19. USAID/AIDSTAR-One. Implementation of World Health Organization’s 2008 pediatric HIV treatment guidelines technical brief; 2010.
20. World Health Organization. The Consequences of Poor Adherence to Long-Term Therapies are Poor Health Outcomes and Increased Health Care Costs; World Health Organization; 2018.
21. Kassi T, Eboua F, Nouaman M, et al. Factors associated with non-adherence to antiretroviral therapy among HIV-infected adolescents at pediatric department of Yopougon University Hospital, Côte d’ Ivoire. Open J Pediatr. 2018;8:238–248. doi:10.4236/ojped.2018.83025
22. Arage G, Tessema GA, Kassa H. Adherence to antiretroviral therapy and its associated factors among children at South Wollo Zone Hospitals, Northeast Ethiopia: a cross-sectional study. BMC Public Health. 2014;14:1–7.
23. Alemu K, Likisa J, Alebachew M, Temesgen G, Tesfaye G. Adherence to highly active antiretroviral therapy and predictors of non-adherence among pediatrics attending ambo hospital ART clinic, West Ethiopia. HIV/AIDS Infect Dis. 2014;2:1–7.
24. Feyissa A. Magnitude and associated factors of non-adherence to highly active antiretroviral therapy among children in Fiche Hospital, North Shewa, Ethiopia, 2016. J Pharm Care Heal Syst. 2016;(4):170. doi:10.4172/2376-0419.1000170
25. Butler LM, Brickley DB, Kennedy G, Rutherford G, Chan J, Asia E. Rates and determinants of adherence to antiretroviral therapy (ART) in infants, children and adolescents: a systematic review; 2010.
26. Vreeman RC, Ayaya SO, Musick BS, et al. Adherence to antiretroviral therapy in a clinical cohort of HIV-infected children in East Africa. PLoS One. 2018;13(2):e0191848. doi:10.1371/journal.pone.0191848
27. Akahara C, Nwolisa E, Odinaka K, Okolo S. Assessment of antiretroviral treatment adherence among children attending care at a tertiary hospital in Southeastern Nigeria. J Trop Med. 2017;10:1–5. doi:10.1155/2017/3605850
28. Zegeye S, Sendo E. Adherence to antiretroviral therapy among HIV-infected children attending Hiwot Fana and Dil-Chora Art Clinic at referral hospitals in Eastern Ethiopia. J HIV Clin Sci Res. 2015;2(1):8–14.
29. Gultie T, Amlak TG, Sebsibie G. Factors affecting adherence to pediatrics antiretroviral therapy in Mekelle Hospital, Tigray Ethiopia. Int J Public Heal Sci. 2015;4:1–6.
30. Dachew BA, Tesfahunegn TB, Birhanu AM. Adherence to highly active antiretroviral therapy and associated factors among children at the University of Gondar Hospital and Gondar Poly Clinic, Northwest Ethiopia: a cross-sectional institutional based study. BMC Public Health. 2014;14:1–6.
31. Firdu N, Enquselassie F, Jerene D. HIV-infected adolescents have low adherence to antiretroviral therapy a cross-sectional study in Addis Ababa, Ethiopia. Pan Afr Med J. 2017;27. doi:10.11604/pamj.2017.27.80.8544
32. Kendre GM, Gabhale YR, Shah ND, Jadhav VM, Nath K, Manglani MV. Adherence to antiretroviral therapy and factors affecting adherence among paediatric HIV patients. Int J Contemp Pediatr Kendre. 2017;4:1962–1968. doi:10.18203/2349-3291.ijcp20174154
33. Wadunde I, Tuhebwe D, Ediau M, Okure G, Mpimbaza A, Wanyenze RK. Factors associated with adherence to antiretroviral therapy among HIV infected children in Kabale district, Uganda: a cross sectional study. BMC Res Notes. 2018;11:1–6. doi:10.1186/s13104-017-3088-5
34. Biressaw S, Abegaz WE, Abebe M, Taye WA, Belay M. Adherence to Antiretroviral Therapy and associated factors among HIV infected children in Ethiopia: unannounced home-based pill count versus caregivers’ report. BMC Pediatr. 2013;13:1471–2431. doi:10.1186/1471-2431-13-132
35. Id GM, Antonucci R, Mukurasi A, Zepherine H. Adherence to antiretroviral treatment among children and adolescents in Tanzania: comparison between pill count and viral load outcomes in a rural context of Mwanza region. PLoS One. 2019;14(3):1–15.
36. Musiime V, Kayiwa J, Kiconco M, et al. Response to antiretroviral therapy of HIV type 1-infected. AIDS Res Hum. 2017;38:1–13.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.