")
Back to Journals » International Medical Case Reports Journal » Volume 17
Case Series: Sacubitril/Valsartan Role for Chemotherapy-Induced Cardiotoxicity: An in-Depth Investigation in Saudi Arabia
Authors Alshammari A, Qasem BA, Almatrafi NA, Alharbi LM, Alhuthali AA, Khobrani AA, Alnuhait M
Received 12 November 2023
Accepted for publication 16 January 2024
Published 18 January 2024 Volume 2024:17 Pages 35—41
DOI https://doi.org/10.2147/IMCRJ.S448913
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Abdullah Alshammari,1 Basmah Ahmed Qasem,1 Nouf Ahmed Almatrafi,1 Lujain Mofareh Alharbi,1 Abeer Abdulhadi Alhuthali,2 Attiah Abdulrahman Khobrani,2 Mohammed Alnuhait1
1Clinical Pharmacy Department, College of Pharmacy, Umm Al-Qura University, Makkah, Saudi Arabia; 2Clinical Pharmacy Department, King Abdullah Medical City, Makkah, Saudi Arabia
Correspondence: Mohammed Alnuhait, Clinical Pharmacy Department, College of Pharmacy, Umm Al-Qura University, Makkah, Saudi Arabia, Email [email protected]
Background: Chemotherapy-induced cardiotoxicity is a significant problem, ranking as the second most frequent cause of mortality in cancer patients. This adverse outcome encompasses many cardiovascular problems, such as heart failure. Sacubitril/valsartan has shown potential in the management of heart failure, however, its effectiveness in treating chemotherapy-induced heart failure has not been extensively explored. We performed a case series to investigate the safety and effectiveness of sacubitril/valsartan in treating chemotherapy-induced cardiomyopathy in Saudi Arabia.
Methods: The case series was conducted at a single medical center in Makkah, Saudi Arabia. The data gathered included patient demographics, clinical features, laboratory results, echocardiographic findings, and medication information. The data underwent analysis using descriptive statistics.
Results: Out of the total of eight patients who were part of the investigation, a notable majority of six individuals exhibited substantial enhancements in their ejection fraction (EF) after receiving sacubitril/valsartan medication.
Conclusion: Our case series provides significant insights by revealing improvements in ejection fraction (EF) in six out of eight patients who had chemotherapy-induced cardiomyopathy after receiving sacubitril/valsartan treatment.
Keywords: oncology, sacubitril/valsartan, cardiotoxicity, chemotherapy, Saudi Arabia
Introduction
The primary concern associated with chemotherapy is the occurrence of cardiotoxicity, a serious medical complication. Chemotherapy-induced cardiotoxicity is the second leading cause of mortality among cancer patients.1 There is diversity in the occurrence of chemotherapy-induced cardiotoxicity among various chemotherapeutic drugs. Anthracyclines, for example, are recognized to be associated with a cardiotoxicity development rate of approximately 9%, although this rate can escalate to as much as 30% with certain specific agents.2–4 This adverse effect encompasses a spectrum of cardiovascular problems, including ischemic heart disease, stroke, heart failure, hypertension, and thromboembolic events.5 Several commonly administered chemotherapeutic agents, such as anthracyclines, cisplatin, cyclophosphamide, ifosfamide, and taxanes, have been identified as culprits in inducing cardiotoxicity. The manifestation of these cardiotoxic effects can vary in timing, from early to late after exposure to specific chemotherapy agents. The incidence and impact of cardiotoxicity differ from one chemotherapeutic agent to another, depending on the intensity and mechanism of action of the chemotherapy.6 One such mechanism involved in chemotherapy-induced cardiotoxicities is the generation of reactive oxygen species and subsequent lipid peroxidation of cell membranes, which can lead to irreversible cardiac damage.7 Heart failure is a prevalent and consequential complication that often arises as a result of chemotherapy.6 Therefore, it is recommended to diligently observe patients receiving chemotherapy by conducting frequent follow-up sessions, performing physical exams, and establishing baseline cardiac function evaluations.6 According to the guidelines set forth by the European Society of Cardiology (ESC), the use of angiotensin converting enzyme inhibitors (ACEI) and beta-blockers (BB) is recommended for patients experiencing chemotherapy-induced cardiomyopathy.5 More recently, the use of sacubitril/valsartan has become more prominent in the management of patients with symptomatic heart failure, as recommended by heart failure guidelines.8 Sacubitril is a pharmacological agent that While valsartan acts by exerting a blocking action on angiotensin II type 1 (AT1) receptors.9 The therapeutic use of sacubitril/valsartan in heart failure has been shown to provide significant advantages, including enhanced left ventricular ejection fraction (LVEF), lower levels of N-terminal pro-brain natriuretic peptide (NT-proBNP) in the bloodstream, and a reduced occurrence of left ventricular remodeling.9 The current body of literature provides limited and inconclusive information pertaining to the efficacy and safety of sacubitril/valsartan in individuals diagnosed with heart failure resulting from chemotherapy treatment.10 A recently reported case series of significance featured two elderly cancer patients who were diagnosed with cardiomyopathy as a result of anthracycline treatment. In these cases, ACEI was replaced with sacubitril/valsartan as a consequence of persistent symptoms. The results revealed a beneficial benefit in terms of minimizing hospitalizations related to heart failure, while also showing minor adverse effects. Similar studies have shown improvements in echocardiographic parameters and an improvement in heart failure symptoms.10,11 Recent investigations that examined people who developed cardiotoxicity as a result of chemotherapy have shown notable improvements in left ventricular ejection fraction. Furthermore, favorable impacts of sacubitril/valsartan were observed to persist regardless of the dosage administered.2,12 To the author’s knowledge, there is a lack of investigation carried out in Saudi Arabia pertaining to studies of this kind. Therefore, the objective of our investigation is to produce a detailed evaluation of the safety and effectiveness of sacubitril/valsartan in individuals who experience heart failure as a result of chemotherapy.
Method
This study was carried out at an institution located in Makkah, Saudi Arabia. The primary objective of this research was to examine a cohort of adult patients, aged over 17 years, who had been diagnosed with chemotherapy-induced cardiotoxicity and were concomitantly using sacubitril/valsartan. The data collection included the acquisition of medical histories, demographic information, clinical features, laboratory measurements (such as NT-proBNP and potassium levels, as indicators of well as renal function), and the recording of echocardiograms with the purpose of finding the left ventricular ejection fraction (LVEF). It’s calculated by comparing the volume of blood in the heart at the end of filling diastole to the volume of blood remaining in the heart after contraction systole. To calculate EF, the following formula is used: EF = ((EDV−ESV) / EDV) × 100%, where EDV is the end-diastolic volume and ESV is the end-systolic volume. These volumes are usually measured in milliliters (mL). The collection of prescribed medications at discharge was also included.
Result
Table 1 presents the main result, which illustrates the ejection fraction (EF) before and after the administration of sacubitril/valsartan. The results indicate that of eight patients, six exhibited improvements after therapy. In the case series we conducted, it was determined that none of the patients featured in the study had any history of alcoholism or a diagnosis of obstructive sleep apnea.
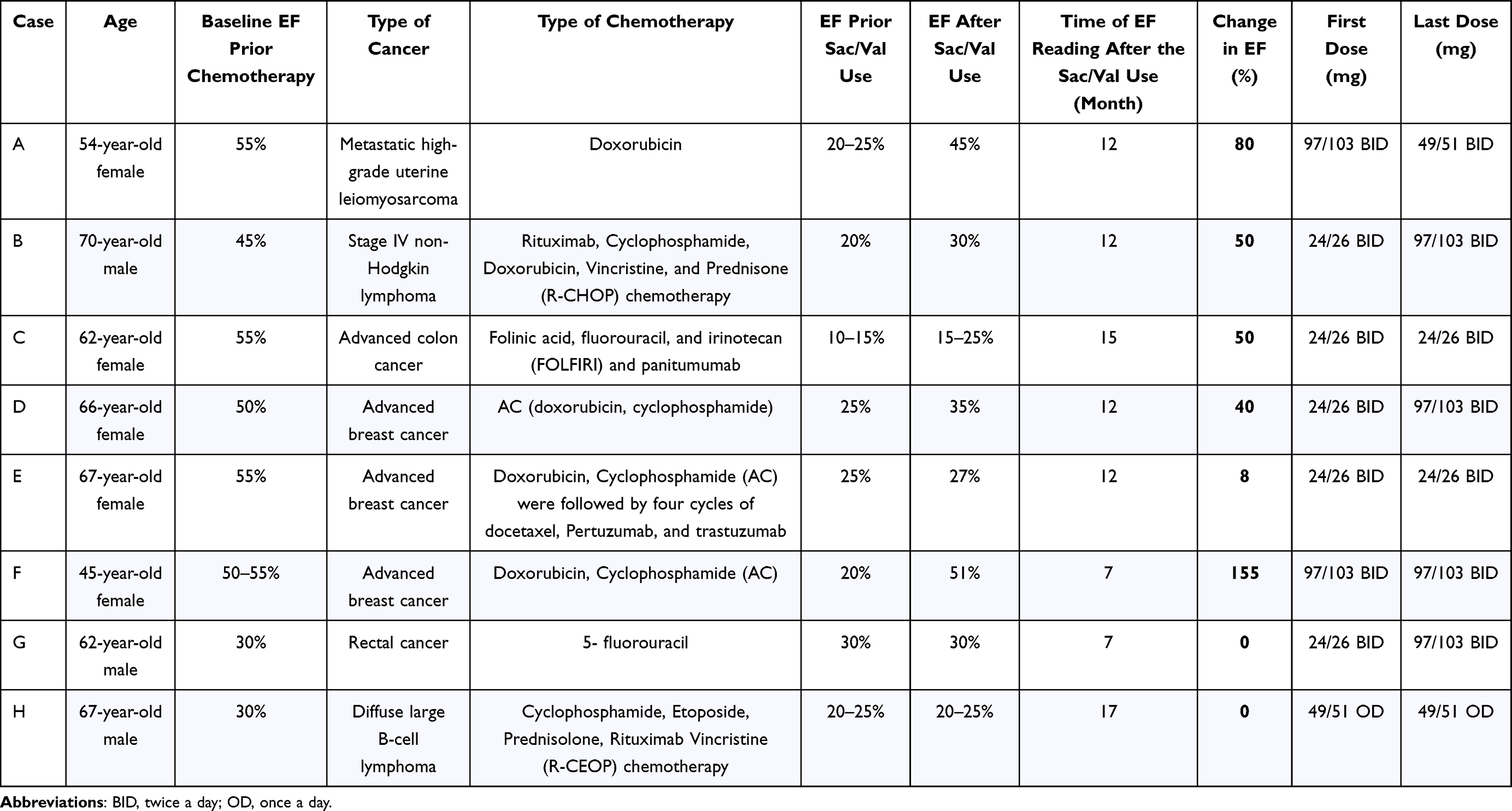 |
Table 1 Primary Outcome of Ejection Fraction (EF) Before and After Receiving Sacubitril / Valsartan (Sac/Val) |
Case A
A 54-year-old woman with high-grade metastatic uterine leiomyosarcoma received doxorubicin-based chemotherapy. Subsequently, her EF dropped precipitously from 55% to 20–25%. This decline in cardiac function prompted cardiology follow-up. Following the diagnosis of chemotherapy-induced cardiomyopathy, the patient was started on sacubitril/valsartan, with a remarkable response. Her EF showed a steady increase over the course of nine months, ultimately reaching 45%. Additionally, the patient was prescribed a tailored combination of medications, including beta-blockers, aldosterone antagonists, anti-coagulants, and diuretics, to optimize her heart function and manage concomitant conditions. Notably, her NT-proBNP levels decreased from 7011 pg/mL to 440 pg/mL, and Troponin-I levels were recorded at 0.29 ng/mL. This case underscores the importance of vigilance in monitoring cardiac function during and after chemotherapy, especially in patients receiving potentially cardiotoxic agents such as doxorubicin. Sacubitril/valsartan has shown promise in improving cardiac outcomes in heart failure patients with reduced EF. Our case demonstrates its potential efficacy in mitigating chemotherapy-induced cardiomyopathy.
Case B
A 70-year-old male was diagnosed with stage IV non-Hodgkin lymphoma and underwent six cycles of R-CHOP chemotherapy. Unfortunately, his LVEF deteriorated significantly, dropping from 45% to 20%. Cardiac dysfunction, notably chemotherapy-induced cardiomyopathy, was evident. In response to the cardiomyopathy, sacubitril/valsartan therapy was initiated. Over time, the patient showed a substantial improvement in EF, with a remarkable 50% increase, ultimately reaching 30%. The patient also received a tailored combination of medications, including beta-blockers, aldosterone antagonists, and diuretics, to optimize heart function and manage concurrent conditions like chronic obstructive pulmonary disease (COPD) and right-sided pleural effusion. During his treatment, the patient’s NT-proBNP levels changed from 230 pg/mL to 242 pg/mL, and his Troponin-I level was recorded at 0.016 ng/mL. This case highlights the importance of monitoring cardiac function during and after chemotherapy, especially when using potentially cardiotoxic agents such as anthracyclines. In this case, it demonstrated the potential efficacy of sacubitril/valsartan reversing chemotherapy-induced cardiomyopathy-induced LV systolic dysfunction.
Case C
A 62-year-old female was diagnosed with locally advanced colon cancer in October 2012. She received radiation and neoadjuvant FOLFOX, followed by a left hemicolectomy and adjuvant XELOX chemotherapy. After that, she was diagnosed with dilated cardiomyopathy, which progressed, leading to an EF of 10–15%. The patient started sacubitril/valsartan therapy. Furthermore, the patient received a customized medication regimen that included beta-blockers and aldosterone antagonists. Over 15 months, her EF improved to 15–25%, resulting in a 50% increase. The patient had resumed chemotherapy during this time, and sacubitril/valsartan helped stabilize her cardiac function without further deterioration. This case demonstrates the potential of sacubitril/valsartan in managing chemotherapy-induced cardiomyopathy, allowing cancer patients to continue with potentially life-saving treatments without compromising cardiac function further. It emphasizes the importance of cardiac monitoring during chemotherapy and the need for prompt intervention when cardiotoxicity is detected.
Case D
A 66-year-old woman with a history of heart failure was diagnosed with breast cancer. She received chemotherapy with doxorubicin and cyclophosphamide, leading to a significant decrease in her EF. Chemotherapy was stopped and hormonal therapy was started. The patient had a complex medical history, including obesity, chronic kidney disease, hypertension, hyperlipidemia, ischemic heart disease, and steroid-induced diabetes. The patient underwent a percutaneous coronary intervention (PCI) due to coronary artery disease. Her EF was severely reduced to 25% and sacubitril/valsartan therapy began. Over the following year, the medication was titrated to target doses. Additionally, the patient was put on a specifically designed treatment plan which comprised beta-blockers and aldosterone antagonists. In April 2023, her EF improved to 35%, marking a 40% increase from the initial value after chemotherapy. Moreover, the patient’s treatment outcomes included a notable improvement in biomarkers, with NT-proBNP levels decreasing from 139 pg/mL to 34 pg/mL, and Troponin-I measured at 0.11 ng/mL. This case underscores the potential benefit of sacubitril/valsartan in managing chemotherapy-induced cardiomyopathy and improving EF in breast cancer patients with preexisting heart conditions. The successful outcome allowed for cardiac intervention and better heart function.
Case E
A 67-year-old woman with right breast cancer and lymph node metastases underwent chemotherapy, including doxorubicin, cyclophosphamide, docetaxel, pertuzumab, and trastuzumab. The treatments led to a significant decline in her EF, from 55% to 25%. She also had comorbidities, including diabetes mellitus, hypertension, and hypothyroidism. After chemotherapy, the patient developed dilated cardiomyopathy and was also diagnosed with venous thromboembolism (VTE). Sacubitril/valsartan therapy was initiated to address chemotherapy-induced cardiomyopathy. In addition, the patient was placed on a specially tailored treatment regimen that included the use of beta-blockers and aldosterone antagonists. Over time, her EF improved from 25% to 27%, representing an increase of 8%. This case highlights the potential cardioprotective role of sacubitril/valsartan in breast cancer patients with chemotherapy-induced cardiomyopathy and pre-existing comorbidities. Despite the modest improvement in EF, therapy allowed for the continuation of oncological treatments and improved cardiac function.
Case F
A 45-year-old woman with metastatic breast cancer of the liver had a history of left breast cancer. She received adjuvant treatments, including chemotherapy, radiation therapy, and hormonal therapy. However, the recurrence of cancer in her right breast led to further treatment, including AC chemotherapy. During AC chemotherapy, the patient’s EF dropped to 20%, resulting in heart failure. Sacubitril/valsartan therapy was initiated, leading to a remarkable 155% increase in EF. Moreover, the patient was prescribed a therapy plan that encompassed both beta-blockers and aldosterone antagonists. Subsequently, she received paclitaxel, carboplatin, pertuzumab, and trastuzumab, which exacerbated cardiac function. However, the addition of sacubitril/valsartan to her heart failure medications resulted in a significant improvement in cardiac function, with her EF increasing from 30% to 53%. This case demonstrates the potential cardioprotective effects of sacubitril/valsartan in patients with chemotherapy-induced cardiomyopathy, allowing the continuation of oncological treatments. The remarkable improvement in EF suggests that sacubitril/valsartan may be a valuable addition to the treatment of chemotherapy-induced cardiomyopathy in patients with breast cancer.
Case G
A 62-year-old individual with a history of myocardial infarction was diagnosed with rectal cancer and subsequently underwent sigmoidoscopy and colorectal anastomosis and received the adjuvant 5-fluorouracil protocol. The patient’s EF was determined to be 30%, rendering him ineligible for chemotherapy. The patient was also administered a personalized treatment, incorporating beta-blockers and aldosterone antagonists. Given the patient’s compromised cardiac function, ACE inhibitors were discontinued, and sacubitril/valsartan therapy was started. Although no substantial improvements in EF were observed during the treatment period, the patient’s cardiac status remained stable This case highlights the importance of managing chemotherapy-induced cardiomyopathy in cancer patients with preexisting cardiac conditions. While sacubitril/valsartan therapy may not lead to significant improvements in EF, it can help to maintain cardiac stability, allowing patients to receive necessary oncological treatments.
Case H
A 67-year-old man with a history of diabetes mellitus, hypertension, and ischemic heart disease was diagnosed with diffuse large B-cell lymphoma. He received a treatment plan consisting of six cycles of R-CHOP chemotherapy, which led to a decrease in EF from 30% to 20–25%. Due to the previous decline in EF, sacubitril/valsartan were introduced to improve cardiac function. The patient’s treatment incorporated the use of beta-blockers. However, EF remained stable throughout the 17-month follow-up period. NT-proBNP levels were initially recorded at 388 pg/mL and subsequently decreased to 349 pg/mL. This case highlights the challenge of managing chemotherapy-induced cardiomyopathy in lymphoma patients and the use of sacubitril/valsartan to mitigate cardiac dysfunction. Despite the long-term administration of this medication, the patient’s EF did not significantly improve.
Discussion
Cardiovascular diseases have a large global influence on the mortality rate, while heart failure, a serious cardiovascular disease, plays a considerable role in contributing to morbidity and mortality on a global basis.1 The existence of ventricular dysfunction and heart failure in people with cancer poses considerable obstacles to therapy and has a significant impact on clinical results.1 The combination drug sacubitril / valsartan has shown effectiveness in the management of individuals with ventricular dysfunction and cardiovascular diseases. However, the efficacy of sacubitril/valsartan in the management of chemotherapy-induced cardiomyopathy is still being actively investigated.2
Several studies have been conducted to investigate the possible advantages of sacubitril/valsartan in individuals diagnosed with chemotherapy-induced cardiomyopathy, with a specific emphasis on patients with cancer. Some of these studies and clinical cases have shown improvements in heart function within this specific patient population.2,12 This investigation provides a significant addition to the existing body of literature by assessing the effects of sacubitril/valsartan on the treatment of chemotherapy-induced cardiomyopathy. Although the study sample was limited, the findings provided offer significant evidence to support the effectiveness of sacubitril/valsartan. It is worth mentioning that a considerable improvement in left ventricular ejection fraction (LVEF) was seen in six out of eight patients who had treatment with sacubitril/valsartan, as shown by our study findings. The combination of sacubitril/valsartan is a promising option for the management of chemotherapy-induced cardiomyopathy. This is supported by its ability to alleviate symptoms, improve LVEF and diastolic function, and attenuate cardiac remodeling.12,13 Furthermore, the use of sacubitril/valsartan demonstrated a reduction in chemotherapy-induced cardiac systolic dysfunction and remodelling. This effect was attributed to the improvement of several factors, including oxidative stress, mitochondrial dysfunction, endoplasmic reticulum stress, and the inflammatory response. Those processes have been identified as predictors of toxicity in this context.14 The aforementioned outcomes exhibit a notable distinction from conventional therapy approaches, such as the utilization of beta-blockers and angiotensin-converting enzyme inhibitors (ACEIs) or angiotensin receptor blockers (ARBs).13 Although the current available data mainly comprises descriptive studies with small sample sizes, our work contributes to the expanding body of knowledge in this field. In order to acquire more conclusive results and enhance comprehension about the efficacy of sacubitril/valsartan in the treatment of chemotherapy-induced cardiomyopathy, it is crucial to conduct larger-scale prospective multicenter studies. In conclusion, more research is important to thoroughly examine the effectiveness of sacubitril/valsartan in patients with chemotherapy-induced cardiomyopathy.
Conclusion
The cases presented in our study highlight the need to closely monitor cardiac function during and after chemotherapy treatment, particularly when using potentially cardiotoxic medications. Sacubitril/valsartan has shown promise in alleviating chemotherapy-induced cardiomyopathy, therefore enabling cancer patients to continue crucial oncological therapies. However, more research, including larger multicenter trials, is essential in order to definitely demonstrate the relevance of this intervention in the management of this particular condition.
Data Sharing Statement
Upon reasonable request, the corresponding author is willing to provide the data.
Ethical Approval
The study obtained ethical clearance from the Biomedical Research Ethics Committee at Umm Al Qura University, with the assigned permission number HAPO-02-K-012-2023-03-1488. Stringent measures were used to ensure the preservation of confidentiality and anonymity of participants’ replies throughout the data-gathering procedure. In compliance with ethical standards and to ensure the protection of our participants’ privacy and rights, informed consent for publication was obtained from all individuals included in this case series. This process was conducted in accordance with the ethical guidelines of our institution and aligns with the principles of the Declaration of Helsinki. All personal identifiers have been removed or altered to protect patient privacy.
Author Contributions
Each author made significant contributions to this research, including involvement in conceptualization, study design, data acquisition, analysis, and interpretation. They also contributed to the drafting, revision, and critical review of the manuscript. All authors gave their final approval for the manuscript’s publication, selected the journal for submission, and committed to being accountable for all aspects of the research.
Funding
This research was conducted independently without any external funding or financial support.
Disclosure
The authors have disclosed that they have no conflicts of interest that might potentially influence the research outcomes.
References
1. Okwuosa TM, Anzevino S, Rao R. Cardiovascular disease in cancer survivors. Postgrad Med J. 2017;93(1096):82–90. doi:10.1136/postgradmedj-2016-134417
2. Canale ML, Coviello K, Solarino G, et al. Case Series: recovery of Chemotherapy-Related Acute Heart Failure by the Combined Use of Sacubitril Valsartan and Wearable Cardioverter Defibrillator: a Novel Winning Combination in Cardio-Oncology. Front Cardiovasc Med. 2022;9:801143. doi:10.3389/fcvm.2022.801143
3. Cardinale D, Colombo A, Bacchiani G, et al. Early detection of anthracycline cardiotoxicity and improvement with heart failure therapy. Circulation. 2015;131(22):1981–1988. doi:10.1161/circulationaha.114.013777
4. Iqubal A, Iqubal MK, Sharma S, et al. Molecular mechanism involved in cyclophosphamide-induced cardiotoxicity: old drug with a new vision. Life Sci. 2019;218:112–131. doi:10.1016/j.lfs.2018.12.018
5. Zamorano JL, Lancellotti P, Rodriguez Muñoz D, et al. 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: The Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur Heart J. 2016;37(36):2768–2801. doi:10.1093/eurheartj/ehw211
6. Albini A, Pennesi G, Donatelli F, Cammarota R, De Flora S, Noonan DM. Cardiotoxicity of anticancer drugs: the need for cardio-oncology and cardio-oncological prevention. J Natl Cancer Inst. 2010;102(1):14–25. doi:10.1093/jnci/djp440
7. Ahles TA, Saykin AJ. Candidate mechanisms for chemotherapy-induced cognitive changes. Nat Rev Cancer. 2007;7(3):192–201. doi:10.1038/nrc2073
8. Heidenreich PA, Bozkurt B, Aguilar D. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure. J Card Fail. 2022;28(5):e1–e167. doi:10.1016/j.cardfail.2022.02.010
9. McMurray JJ, Packer M, Desai AS, et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med. 2014;371(11):993–1004. doi:10.1056/NEJMoa1409077
10. De Vecchis R, Paccone A. A case series about the favorable effects of sacubitril/valsartan on anthracycline cardiomyopathy. SAGE Open Med Case Rep. 2020;8:2050313x20952189. doi:10.1177/2050313x20952189
11. Sheppard CE, Anwar M. The use of sacubitril/valsartan in anthracycline-induced cardiomyopathy: a mini case series. J Oncol Pharm Pract. 2019;25(5):1231–1234. doi:10.1177/1078155218783238
12. Gregorietti V, Fernandez TL, Costa D, Chahla EO, Daniele AJ. Use of Sacubitril/valsartan in patients with cardio toxicity and heart failure due to chemotherapy. Cardiooncology. 2020;6(1):24. doi:10.1186/s40959-020-00078-4
13. Pascual-Figal D, Bayés-Genis A, Beltrán-Troncoso P, et al. Sacubitril-Valsartan, Clinical Benefits and Related Mechanisms of Action in Heart Failure With Reduced Ejection Fraction. A Review. Front Cardiovasc Med. 2021;8:754499. doi:10.3389/fcvm.2021.754499
14. Sobiborowicz-Sadowska AM, Kamińska K, Cudnoch-Jędrzejewska A. Neprilysin Inhibition in the Prevention of Anthracycline-Induced Cardiotoxicity. Cancers. 2023;15(1):312. doi:10.3390/cancers15010312
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.