")
Back to Journals » Vascular Health and Risk Management » Volume 20
Cardiovascular Risk Factors Among First-Degree Relatives of Patients with Premature Cardiovascular Disease in Malta. Baseline Findings from the CRISO Project
Received 13 November 2023
Accepted for publication 29 March 2024
Published 9 April 2024 Volume 2024:20 Pages 167—176
DOI https://doi.org/10.2147/VHRM.S449672
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Mirna N Chahine
Justin Lee Mifsud,1,2 Joseph Galea2
1Department of Nursing, Faculty of Health Sciences, University of Malta, Msida, Malta; 2Department of Medicine, Faculty of Medicine and Surgery, University of Malta, Msida, Malta
Correspondence: Justin Lee Mifsud, Department of Nursing, Faculty of Health Sciences, University of Malta, Msida, Malta, Tel +35623401109, Email [email protected]
Purpose: A family history of premature atherosclerotic cardiovascular disease (ASCVD) confers a greater risk of developing ASCVD. However, the prevalence of ASCVD risk factors among asymptomatic Maltese adults with parental or fraternal history of premature ASCVD is unknown. The study aimed to evaluate and compare their risk with the general population.
Patients and Methods: Posters to market the project were distributed in cardiac rehabilitation areas. Patients with premature cardiovascular disease facilitated recruitment by informing their relatives about the project. Medical doctors and cardiac rehabilitation nurses referred first-degree relatives. Posters were put up in community pharmacies, and an explanatory video clip was shared on social media for interested individuals to contact researchers. Those eligible were enrolled in a preventive cardiology lifestyle intervention. Their data were compared with the risk in the general population.
Results: Many first-degree relatives had a suboptimal risk profile, with 60% (N = 89) having a total cholesterol level of > 5.0 mmol/L; 54% having a low-density lipoprotein-cholesterol level of > 3 mmol/L; 70.5% being overweight/obese, with 62% having a waist circumference greater than the recommended values; 34.8% having hypertension; 56.2% being inadequately adherent to the Mediterranean diet; 62% being underactive, with 18% being sedentary; and 25.8% being smokers. First-degree relatives had significantly higher proportions of underactive lifestyle (p = 0.00016), high body mass index (> 25kg/m2) (p = 0.006), and systolic blood pressure (p = 0.001) than the general population, with 30% having metabolic syndrome.
Conclusion: This study determined the prevalence of lifestyle, biochemical, physiological, and anthropometric cardiovascular risk factors among asymptomatic first-degree relatives of Maltese patients with premature ASCVD. First-degree relatives had considerable prevalences of an underactive lifestyle, hypertension, and obesity, suggesting better screening and early risk factor intervention are needed to modify their risk of ASCVD.
Plain Language Summary: This study was done to evaluate factors that can increase the risk of heart disease in siblings and offspring of Maltese patients who developed atherosclerotic cardiovascular disease (ASCVD) at a young age. Relatives were invited to meetings during which a risk evaluation was performed. The researchers found that relatives had a high prevalence of cardiometabolic risk factors, meaning they were at increased risk of developing the disease.
The researchers have concluded that reducing the risk of ASCVD in individuals at increased risk requires developing and testing potentially sustainable risk factor modification strategies.
Keywords: primary prevention, risk assessment, family history
Introduction
Atherosclerotic cardiovascular disease (ASCVD) is a significant cause of disability and death.1 In Europe, about 3.9 million deaths are attributable to atherosclerotic cardiovascular disease (ASCVD) annually, and 1.8 million are attributable to coronary heart disease (CHD).2 Malta is the smallest country in the European Union, with a population of 500,000. ASCVD is the leading cause of death in Malta, accounting for 38% of all mortalities in 2014, of which 21% (n = 689, 352 males, 337 females) were due to CHD3–5 and 42% were premature (65–75 years: n = 212, 30.8%; <65 years: n = 78, 11.0%).3
The European Society of Cardiology (ESC) guidelines highlight a family history of premature ASCVD as a risk-enhancing factor.6,7 However, no studies have evaluated first-degree relatives of Maltese patients with premature ASCVD, making their prevalence of modifiable risk factors unknown. Therefore, this study aimed to ascertain the prevalence of ASCVD risk factors, including smoking, underactive physical activity, inadequate Mediterranean diet adherence, hyperlipidemia, hypertension, overweight/obesity, central obesity, and low health literacy in a sample of asymptomatic first-degree relatives of Maltese patients with premature CHD and compare them with the general population. In this specific research context in Malta, there is no data available. Thus, this study represents a significant advance in primary prevention from a local perspective, as there is a need for existing literature on the subject.
Materials and Methods
Study Design and Participants
The Coronary Risk Prevention in Siblings and Offspring of Patients with Premature Coronary Heart Disease (CRISO) project comprises a pilot randomised controlled trial testing a preventive cardiology programme among first-degree relatives of Maltese patients with premature ASCVD (ISRCTN21559170). This trial’s design and procedures have been described previously.8
This study used several inclusion criteria to select the population: (1) first-degree relatives of patients with premature ASCVD, (2) aged ≥30 years, and (3) Maltese ethnicity. Its exclusion criteria were: (1) history of ASCVD, diabetes mellitus, rheumatoid arthritis, or chronic kidney disease; (2) contraindications against physical activities; or (3) pregnancy. The study protocol was approved by the University of Malta Ethics Committee (approval number: 3756_191119) and the Malta Health Ethics Committee (approval number: HEC CT01/20). The primary and secondary endpoints of the protocol were to determine the feasibility and acceptability of a developed preventive cardiology programme and to test for potential risk reduction.
Data Collection
We used data collected at baseline from relatives who consented to participate in the CRISO project between September 2020 and September 2022. Risk factor evaluation took place at the Outpatient Clinic at Mater Dei Hospital, Malta.
Risk Factor Categories
Lifestyle data were collected, including smoking status and dietary and physical activity patterns. Smoking status was answered as ‘yes’ or “no”. Those with carbon monoxide in their exhaled breath >7 parts per million were considered smokers. The Fagerstrom Test for Nicotine Dependence screener was used to assess the level of nicotine dependency.9 The 14-point Mediterranean Diet Adherence Screener (MEDAS)10 was used to assess adherence to the Mediterranean diet. A MEDAS score ≤7 was considered inadequate Mediterranean diet adherence. The Rapid Assessment of Physical Activity (RAPA) questionnaire11 was used to assess physical activity levels. A RAPA score ≤5 was considered underactive.
Biochemical indicators were measured after a 12-hour fasting. Blood indicators (lipids and haemoglobin A1c [HbA1c]) were analysed using the Roche COBAS analyser (Rotkreuz, Switzerland), while the thyroid function test was performed using a Siemens ADVIA Centaur analyser (Erlangen, Germany). Participants were diagnosed with hyperlipidemia if they had already used a lipid-lowering drug and/or had a total cholesterol level of >5 mmol/L.7
Blood pressure was measured after a 10-minute seated rest, repeated 10 minutes after, and then again at the end of the evaluation appointment. Blood pressure was measured in both arms using an Omron™ blood pressure monitor (Kyoto, Japan), measured 2–3 times by auscultation, and an average was taken as the final measurement. Participants were defined as having hypertension if they were already using a blood pressure-lowering drug or had a systolic blood pressure of >140 mmHg or a diastolic blood pressure of >90 mmHg.7
Anthropometric indices were measured using a SECA scale with a height gauge (Hamburg, Germany). Numerous steps were taken to avoid measurement errors. Weight was taken to the nearest 0.1 kg. The waist circumference was measured at the end of expiration while the participant was standing. A non-elastic measuring tape was placed at the midpoint between the iliac crest, the lowest rib, and the umbilicus level. Participants were defined as overweight if their body mass index (BMI) was 25.0–29.9 kg/m2 or obese if their BMI was ≥30.0 kg/m2. A waist circumference >102 cm in men and >88 cm in women was considered central obesity.12
Participants were defined as having metabolic syndrome if they had a clustering of ≥3 cardiometabolic risk factors (elevated blood pressure, triglycerides, waist circumference, and reduced high-density lipoprotein-cholesterol [HDL-C]).13
The Heart-Age and HeartScore2 scores were calculated after obtaining the following parameters: age, sex, systolic blood pressure, cholesterol, smoking status, weight, and height. Participants were defined as having an elevated heart age if their Heart-Age score was >5 years above their chronological age. Using the HeartScore2 thresholds for moderate-risk countries, participants were categorised into three groups: low risk (<1.0%), low to moderate risk (<50 years:1–<2.5%; 50–69 years: 1–<5.0%), and high risk (<50 years: >2.5%; 50–69 years: >5.0%) of developing ASCVD.7
Data Analysis
The Statistical Package for Social Sciences software (version 20) was used to analyse the data. Participants’ characteristics, including demographic information and baseline measurements, were descriptively summarised for the entire cohort. Categorical data are reported as frequencies, valid proportions, and percentages.14 Numerical variables are reported as means ± standard deviations or medians. The study cohort data were compared to secondary data sources representing a sample from the general Maltese population.15 Where data were available (mean; total cholesterol, systolic blood pressure, body mass index), a two-sample t-test was used to compare means between the study cohort and the general Maltese population. Where data were available (%; smoking, underactive physical activity, raised blood pressure, overweight, obese), a z-test for proportions was used to determine whether the prevalence of risk factors differed between the study cohort and the general Maltese population. A p-value of <0.05 was considered statistically significant.
Results
Population Characteristics
The researcher evaluated all 89 participants. Nearly 60.0% (n=53) of participants were women. Their mean age was 45 ± 10 years. Over half (60%, n=53) reported a university education. One-fifth were unemployed (n=18), and 16% lived alone (n=14). Over 93% felt connected with their family and friends (n=83), while 17.0% reported loneliness (n=15), albeit living with someone or connected to family or friends. Among participants, 62.9% had one parent with premature ASCVD (n=56), 20.0% had a parent and a sibling with premature ASCVD (n=18), 14.6% had a sibling with premature ASCVD (n=13), and 2.2% had both parents with premature ASCVD (n=2). Regarding cardioprotective drug use, 23.0% took lipid-lowering drugs (statin therapy) (n=20), and 20.5% took antihypertensives (angiotensin-converting enzyme inhibitors) (n=18).
Lifestyle Factors
Twenty-three participants (26%) smoked cigarettes. Their mean Fagerstrom Test for Nicotine Dependence score was 3.22 ± 2.70.
The participants’ mean MEDAS score was 6.84 ± 2.00 (Table 1). Almost 77% used olive oil (n= 68). However, only 12% used the recommended daily amount (four tablespoons daily) (n= 11). About 50% reported consuming two or more vegetables daily (n=44), and only 32% consumed three or more fruits daily (n=28). Only 18% consumed three or more servings (one serving: 150g) of legumes (soybeans, kidney beans, and fava beans) daily (n=16). Only about 18% reported consuming three servings or more portions of fish weekly (n=16). About 47% reported daily consumption of commercial sweets or pastries (not homemade), such as cakes, biscuits, or custard (n=42), and 52% consumed less than three servings (one serving: 30 g) of nuts weekly (n=46). About 84% reported they preferentially consumed chicken, turkey, or rabbit meat over veal, pork, hamburgers, or sausages (n=75). About 67% used tomato sauce, onion, and garlic simmered with olive oil with pasta or other dishes (n=60). Overall, 56.2% had an inadequate MEDAS (n=50).
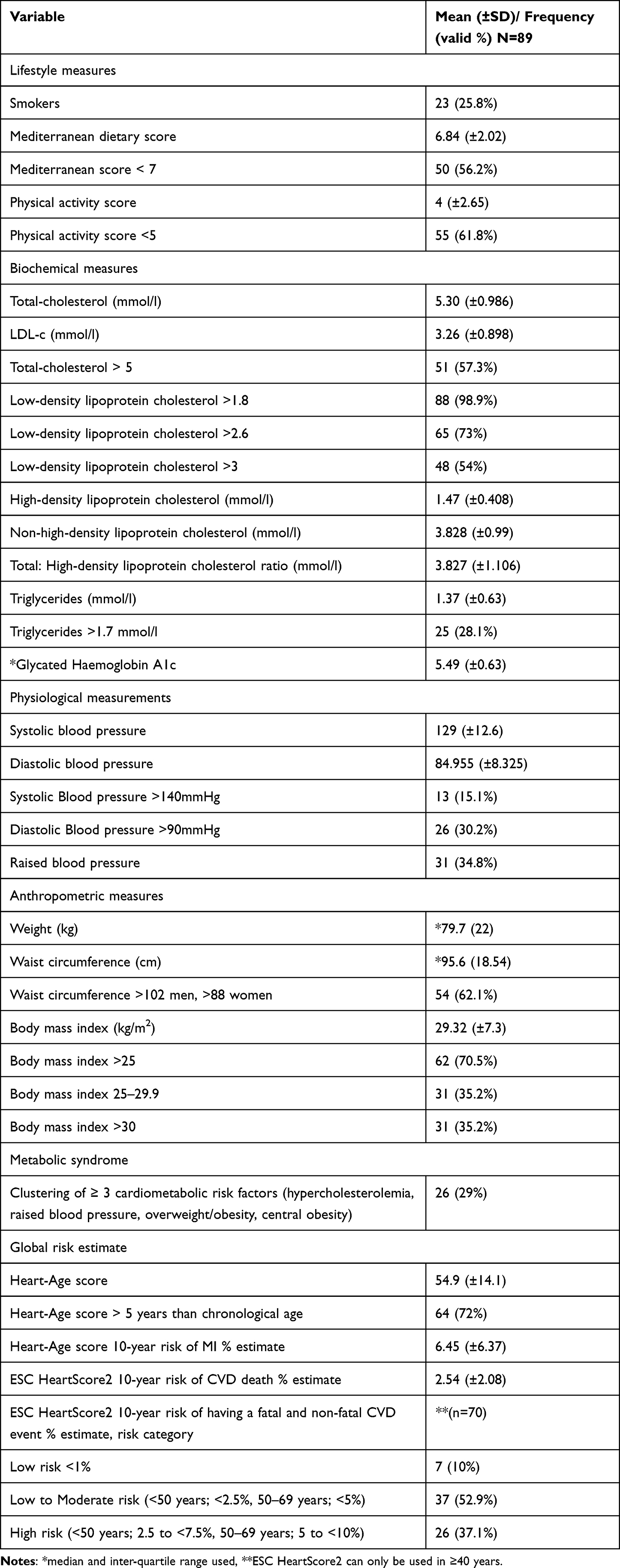 |
Table 1 Lifestyle, Biochemistry, Physiologic, Health Literacy, Anthropometric, Risk Factor Clusters and Global Risk Measures |
The participants’ mean RAPA score was 4.00 ± 2.65 (Table 1). Only about 19% reported performing 30 minutes or more of moderate physical activities at least five days a week (n=17). About 17% reported performing activities to increase muscle strength at least once a week (n=15), and 23% reported performing activities to improve flexibility at least once a week (n=20). Overall, 64% did not achieve a moderate physical activity level (n=57).
Biochemical Factors
Most participants (57.3%, n=51) had an above-average total cholesterol level (>5 mmol/L). Most (98.9%) had a low-density lipoprotein-cholesterol (LDL-C) level of >1.8 mmol/L, 73% had an LDL-C level of >2.6 mmol/L (n=65), and 54% had an LDL-C level of >3 mmol/L (n=48). In addition, 28% had a triglyceride level of >1.70 mmol/L (n=25). The participants’ mean total cholesterol was 5.300 ± 0.986, and the mean LDL-C level was 3.26 mmol/L. The participants’ mean HDL-C level was 1.470 ± 0.408 mmol/L, non-HDL-C level was 3.828 ± 0.990 mmol/L, and total-cholesterol: HDL-C ratio was 3.830 ± 1.106. The participants’ mean HbA1c level was 5.49 ± 0.63 (Table 1).
Physiological Factors
Most participants (65.2%, n=58) had an optimal blood pressure (Blood pressure <140/90 mmHg). Their mean office systolic blood pressure was 129.9 ± 12.6 mmHg and diastolic blood pressure was 84.950 ± 8.325 mmHg. Table 1. provides information on the office systolic and diastolic blood pressure measurements, showing that only 15% had a systolic blood pressure of >140 mmHg (n=13). However, 30.2% had a diastolic blood pressure of >90 mmHg (n=27). Overall, 34.8% had either a high systolic (>140 mmHg) or diastolic (>90 mmHg) blood pressure (n=31).
Anthropometric Factors
The participants’ mean weight was 79.7 ± 22.0 kg. Their mean waist circumference was 95.6 ± 18.54 cm, with almost 62% having an above-average waist circumference (>102 cm for men and >88 cm for women) (n=55). Their mean BMI was 29.32 ± 7.30 kg/m2. Only 29.5% were determined to have a normal BMI (n=26). Almost 71% were overweight (35.2%) or obese (35.2%; Table 1).
Metabolic Syndrome
The proportion of participants with a clustering of ≥ 3 metabolic risk factors was 29% (n=26); the three risk factors were hyperlipidemia, central obesity, and raised blood pressure.
Heart-Age and HeartScore2
The participants’ mean Heart-Age score was 54.9 ± 14.1, with 72% having a Heart-Age score more than five years above their chronological age (n=64). The mean Heart-Age estimated 10-year percentage risk of myocardial infarction was 6.45% ± 6.37%. Their mean ESC HeartScore2 10-year percentage risk of cardiovascular death was 2.54% ± 2.08%. Based on the ESC HeartScore2 score, 10.0% (n=9), 52.9% (n=47), and 37.1% (n=33) fell into the low-, moderate-, and high-risk categories, respectively.
First-Degree Relatives of Patients with Premature ASCVD Compared to the General Population
The study cohort data were compared to secondary data sources representing a sample from the general Maltese population15 (Table 2). Study participants were more likely to smoke than the general population; however, the proportion only differed significantly for female smokers (study cohort: 26.4%; general population: 15.8%; p = 0.040). Study participants were significantly more underactive (61.7%) than the general population (41.7%; p = 0.00016). In contrast, study participants did not differ significantly from the general population in mean total cholesterol levels (MD = 0.053, p = 0.614). However, significantly more study participants (35.0%) had elevated blood pressure than the general population (19.4%) (p = 0.00026), with relatives having a significantly higher mean systolic blood pressure than the general population (MD = 5.55, p = 0.001).
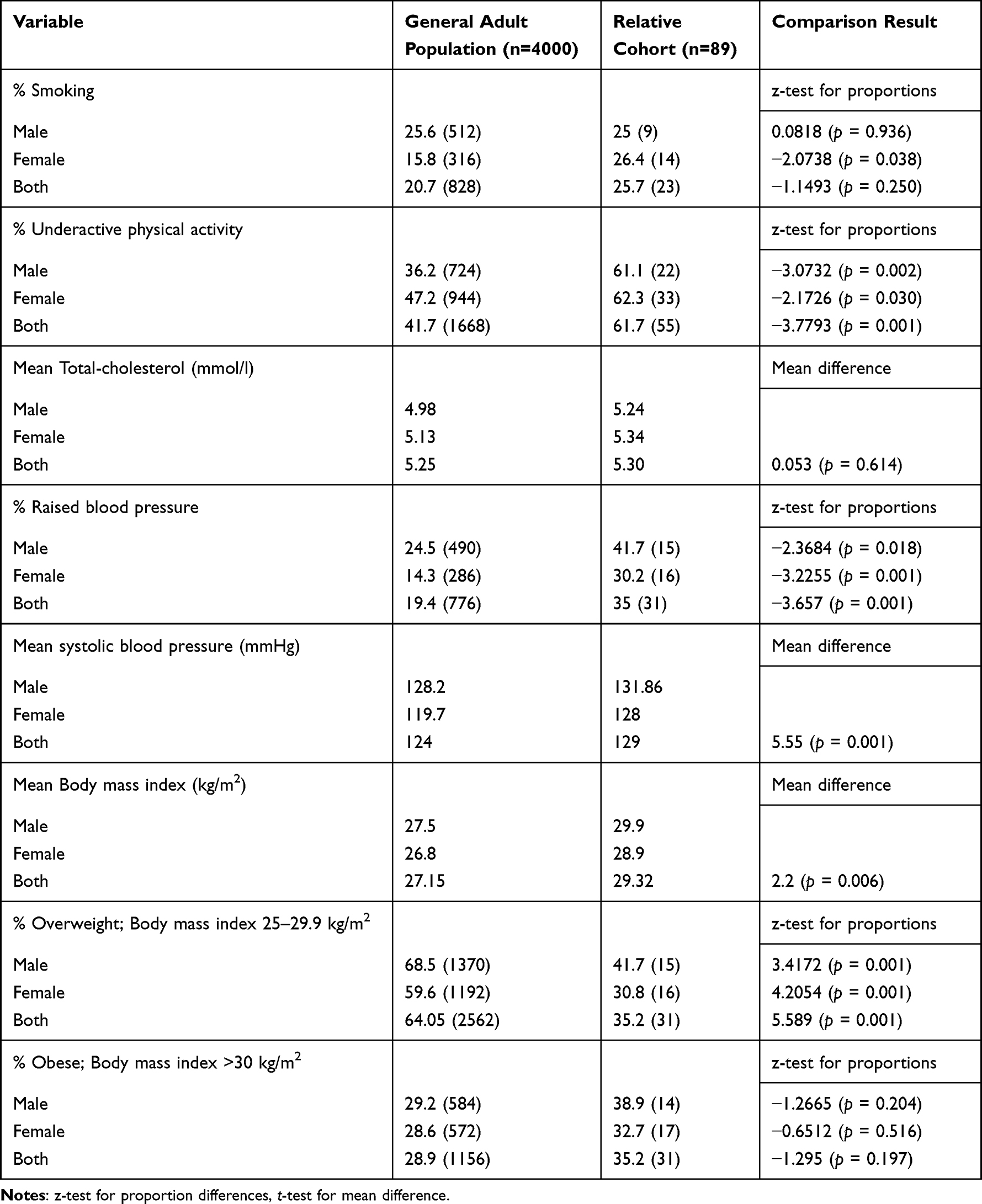 |
Table 2 Relatives of Patients with Premature ASCVD and the General Population Comparison |
The study participants were less overweight than the general population, while at the same time, the study participants were more obese. However, the obesity proportions did not differ significantly between the study participants (35.2%) and the general population (28.9%); albeit the study participants had a significantly higher mean BMI than the general population (p < 0.006).
Discussion
Our results showed that first-degree relatives of Maltese patients with premature ASCVD do not have an optimal risk profile as the European preventive cardiology guidelines recommend.7 Lifestyle factors showed that 56.2% were <50% adherent to the Mediterranean diet. In addition, nearly 62% were underactive, with 18% being sedentary. Moreover, 25.8% were smokers. Furthermore, nearly 60% had hyperlipidemia, and 34.8% had hypertension, with 70.5% overweight or obese and 62% having a waist circumference above the recommended values (≥102 cm in Europid men and ≥88 cm in Europid women).
Previous studies have reported similar findings, where the siblings and offspring of patients with ASCVD had a high prevalence of risk factors.16–19 More of our study participants had an underactive lifestyle (61.7%) than the general Maltese population (41.7%; p = 0.00016).
About 24.5% of the adult male population and 14.3% of the adult female population in Malta had elevated blood pressure in 2016.15 The prevalence of elevated blood pressure among male and female study participants was higher than among males and females in the general Maltese population (41.7% vs 24.3% and 30.2% vs 14.3%, respectively; p < 0.05), with a significantly greater difference in mean systolic blood pressure between study participants and the general Maltese population (p < 0.001).
Similarly, previous studies reported that first-degree relatives of patients with premature ASCVD had higher prevalences of central obesity (≥102 cm in Europid men and ≥88 cm in Europid women), hypertension, hypercholesterolemia, and cigarette smoking than the general population.16–19
Almost twice as many study participants had ≥3 cardiometabolic risk factors (30%) compared to the European member states,20 defined as metabolic syndrome.13 The DECODE study found that metabolic syndrome was present in about 15% of adult Europeans without diabetes,20 with the most common metabolic syndrome component being high blood pressure.
The higher prevalence of risk factors among first-degree relatives of patients with premature ASCVD could suggest potential genetic predisposition or shared environmental factors contributing to the clustering of metabolic risk factors, which we observed in our cohort. Even without traditional risk factors, some individuals could have a higher risk of developing disease because of a higher genetic predisposition, making polygenic risk score evaluation a more personalized approach. In our cohort, however, most exhibited a high prevalence of traditional risk factors. This observation is of concern since it can accelerate the development of atherosclerosis and arterial diseases.21,22 It has been reported that siblings of patients with premature CHD have approximately 40% higher risk of developing the disease than the general population, while offspring have 60–75% higher risk.23 Additionally, if the individual has two affected first-degree relatives, the risk can increase by approximately 80%.23,24
Since our results show that first-degree relatives of patients with premature ASCVD have various risk factors associated with ASCVD development, it appears appropriate to develop targeted interventions and preventive strategies to mitigate the impact of risk factors within this at-risk population.8 Once developed and tested, targeted interventions and preventive strategies may benefit the general population with risk cluster factors or other at increased risk populations. However, this needs more resources to be studied further.
Strengths and Limitations
To our knowledge, this is the first study in Malta focusing on first-degree relatives of patients with premature ASCVD, aiming to develop a programme (CRISO) to support risk factor modification in an increased-risk population. Our study’s preliminary results are significant because they indicate that most of these individuals are at borderline risk despite their young mean age (45.2 ± 10.0 years). As with any study, this study had limitations. First, its small sample might not represent the entire population, potentially impacting the generalisability of its findings. Second, comparing our data with registry-based general population data might not be considered an appropriate comparison with a control group. For example, our sample included individuals aged ≥30 years, whereas the secondary data included a sample of individuals aged ≥18 years, which might have created differences in certain risk factor variables. Third, the observed difference in mean BMI might reflect that study participants comprised individuals who intended to lose weight by participating in a lifestyle intervention trial.
While our study focused on a specific European region, it provides valuable insights into the prevalence of risk factors among Maltese first-degree relatives of patients with premature ASCVD. This data was previously unavailable, and the new findings highlight this group’s high-risk factor prevalence that encourages the implementation of targeted intervention and will test the assumption of whether it has the potential to modify risk. These results also show health authorities the importance of improving access to health screening and healthy lifestyle programmes for potential risk groups in Malta.
Study Implications
Our findings underscore the need to test the assumption about whether a preventive cardiology lifestyle intervention can reduce ASCVD risk in first-degree relatives of Maltese patients with premature ASCVD. Early detection and intervention could lead to better health outcomes and reduce the burden of risk factor clusters within this high-risk group.
Conclusion
First-degree relatives of Maltese patients with premature ASCVD have a high prevalence of risk factors, the most common being high anthropometric indices. Risk factor prevalences were broadly similar between the first-degree relatives and the general population, except for physical activity, blood pressure, and BMI. Risk evaluation and support are required to modify risk among this potential at-risk group.
Key Messages
•The siblings and offspring of Maltese patients with premature atherosclerotic cardiovascular disease (ASCVD) had high prevalences of cardiometabolic risk factors.•To reduce their risk of ASCVD, individuals at increased risk must be provided with and encouraged to use potentially sustainable risk factor modification strategies. These strategies must be developed and tested.
Data Sharing Statement
The authors intend to share the anonymized participant datasets produced and/or examined in the present study via the University of Malta’s institutional open-access data repository at https://www.um.edu.mt/library/oar/. Other study documents will be made available via ISRCTN21559170.
Ethics Statement
The study manuscript complies with the Declaration of Helsinki.
Acknowledgments
We gratefully acknowledge the support from the Cardiac Rehabilitation Unit at Mater Dei Hospital toward this research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Cardiovascular Diseases (CVDs); 2018. Available from: http://www.who.int/mediacentre/factsheets/fs317/en/.
2. Timmis A, Townsend N, Gale CP, et al. European society of cardiology: cardiovascular disease statistics 2019. Eur Heart J. 2019;41(1):12–85. doi:10.1093/eurheartj/ehz859
3. Wilkins E, Wilson L, Wickramasinghe K, et al. European cardiovascular disease statistics 2017. European heart network, Brussels; 2017. Available from: https://ehnheart.org/wp-content/uploads/2023/07/CVD-Statistics.pdf.
4. Malta national statistics office. Malta in figures 2014; 2014. Available from: https://nso.gov.mt/en/publicatons/Publications_by_Unit/Documents/D2_Dissemination_Unit/Malta_in_Figures_2014.pdf.
5. DHIR M World heart day; 2015. Available from: http://health.gov.mt/en/dhir/Pages/Introduction.aspx.
6. Mach F, Baigent C, Catapano A. Task force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS). 2019 ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk [published online ahead of print]. Eur Heart J. 2019;41(1):111–188.
7. Visseren FL, Mach F, Smulders YM, et al. 2021 ESC guidelines on cardiovascular disease prevention in clinical practice: developed by the task force for cardiovascular disease prevention in clinical practice with representatives of the European society of cardiology and 12 medical societies with the special contribution of the European Association of Preventive Cardiology (EAPC). Eur Heart J. 2021;42(34):3227–3337. doi:10.1093/eurheartj/ehab484
8. Mifsud JL, Stephenson J, Astin F, Galea J. Coronary risk reduction intervention for siblings and offspring of patients with premature coronary heart disease: the CRISO study protocol for a randomised controlled pilot study. Pilot Feasibility Stud. 2021;7(1):1–15. doi:10.1186/s40814-021-00874-4
9. Fagerström K. Determinants of tobacco use and renaming the FTND to the fagerström test for cigarette dependence. Nicotine Tobacco Res. 2011;14(1):75–78. doi:10.1093/ntr/ntr137
10. Martínez-González MA, García-Arellano A, Toledo E, et al. A 14-item Mediterranean diet assessment tool and obesity indexes among high-risk subjects: the PREDIMED trial. PLoS One. 2012;7(8):e43134. doi:10.1371/journal.pone.0043134
11. Ruiz-Comellas A. How can physical activity be measured in primary health care? Ann Sports Med Res. 2014;1(2):1008.
12. WHO. Waist circumference and waist-hip ratio: report of a WHO expert consultation. Geneva. 2008;2008:8–11.
13. Nilsson PM, Tuomilehto J, Rydén L. The metabolic syndrome–what is it and how should it be managed? Eur J Prev Cardiol. 2019;26(2_suppl):33–46. doi:10.1177/2047487319886404
14. Harris T Medical statistics made easy: royal college of general practitioners; 2014.
15. Timmis A, Vardas P, Townsend N, et al. European society of cardiology: cardiovascular disease statistics 2021. Eur Heart J. 2022;43(8):716–799. doi:10.1093/eurheartj/ehab892
16. Soman S, Kar SS, Satheesh S, Ramalingam A. Cardiovascular disease risk profiling among first degree relatives of coronary artery disease patients admitted in cardiology ward of JIPMER, Puducherry. J Cardiovasc Dis Res. 2016;7(3):108–111. doi:10.5530/jcdr.2016.3.2
17. Yanek LR, Moy TF, Blumenthal RS, et al. Hypertension among siblings of persons with premature coronary heart disease. Hypertension. 1998;32(1):123–128. doi:10.1161/01.HYP.32.1.123
18. Hurrell C, Wietlisbach V, Jotterand V, et al. High prevalence of major cardiovascular risk factors in first-degree relatives of individuals with familial premature coronary artery disease—the GENECARD project. Atherosclerosis. 2007;194(1):253–264. doi:10.1016/j.atherosclerosis.2006.08.004
19. Allen JK, Young DR, Blumenthal RS, et al. Prevalence of hypercholesterolemia among siblings of persons with premature coronary heart disease: application of the second adult treatment panel guidelines. Arch Intern Med. 1996;156(15):1654–1660. doi:10.1001/archinte.1996.00440140076007
20. Hu G, Qiao Q, Tuomilehto J, et al. Prevalence of the metabolic syndrome and its relation to all-cause and cardiovascular mortality in nondiabetic European men and women. Arch Intern Med. 2004;164(10):1066–1076. doi:10.1001/archinte.164.10.1066
21. Wahrenberg A, Magnusson PK, Discacciati A, et al. Family history of coronary artery disease is associated with acute coronary syndrome in 28,188 chest pain patients. Eur Heart J Acute Cardiovasc Care. 2020;9(7):741–747. doi:10.1177/2048872619853521
22. Martelli E, Enea I, Zamboni M, et al. Focus on the most common paucisymptomatic vasculopathic population, from diagnosis to secondary prevention of complications. Diagnostics. 2023;13(14):2356. doi:10.3390/diagnostics13142356
23. Kolber MR. Family history of cardiovascular disease. J Colle Physician Can. 2014;60(11):1016.
24. Chow CK, Islam S, Bautista L, et al. Parental history and myocardial infarction risk across the world: the interheart Study. J Am Coll Cardiol. 2011;57(5):619–627. doi:10.1016/j.jacc.2010.07.054
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.