")
Back to Journals » Patient Preference and Adherence » Volume 16
Breaking Bad News of a Cancer Diagnosis: A Mixed-Methods Study of Patients’ Perspectives
Authors Al-Johani WM , AlShamlan NA , AlGhamdi MF, AlAbdulkader AM , Aljohani WM, AlGhamdi RF, Alrefae M, Alshehabi M, AlOmar RS , Abdel Wahab MM
Received 20 October 2022
Accepted for publication 13 December 2022
Published 20 December 2022 Volume 2022:16 Pages 3357—3369
DOI https://doi.org/10.2147/PPA.S394170
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Wejdan M Al-Johani,1 Nouf A AlShamlan,1 Manar F AlGhamdi,2 Assim M AlAbdulkader,1 Waleed M Aljohani,3 Rehab F AlGhamdi,2 Munir Alrefae,4 Muna Alshehabi,5 Reem S AlOmar,1 Moataza M Abdel Wahab1
1Department of Family and Community Medicine, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, 34224, Saudi Arabia; 2College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 3Supply Chain Department, Security Forces Hospital, Dammam, Saudi Arabia; 4Department of Internal medicine, King Fahad Hospital of University, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 5Palliative Medicine Department, King Fahad Specialist Hospital, Dammam, Saudi Arabia
Correspondence: Wejdan M Al-Johani, Department of Family and Community Medicine, College of Medicine, Imam Abdulrahman Bin Faisal University, P.O. Box 1982, Dammam, 34224, Saudi Arabia, Tel +966599721175, Email [email protected]
Purpose: A cancer diagnosis is an overwhelming process for both patients and doctors. Many studies have addressed doctors’ opinions and knowledge regarding breaking bad news (BBN). However, scarce knowledge exists regarding patients’ perspectives for communicating bad news. Therefore, the current study aims to assess cancer patient preferences and satisfaction about BBN.
Patients and Methods: This is a mixed methods study consisting of two phases; an in-depth interview and cross-sectional quantitative analysis. Thematic analysis was used for the qualitative data to explore patients’ satisfaction and preferences about BBN. For quantitative analyses, the overall satisfaction was calculated as satisfaction percent. Bivariate analyses were performed, and statistical significance was set as p < 0.05. Quality function deployment was used to effectively define patient requirements of highest priority.
Results: Thematic analysis revealed two main themes. Theme 1; patients’ requirements for BBN and theme 2; patients’ reaction at the time of diagnosis with their categories. For the quantitative part, a total of 222 patients responded to the survey, females made up 70% of the sample. Satisfaction score percent ranged from 25.5 to 100%, with a mean of 82.7± 11.9%. The most preferred items were mainly concerned with the doctor being honest and encouraging, good listener and interacting giving simple smooth explanations without using medical terms, and empathetic (average score 4.8/5). Also, providing the diagnosis in a calm and private environment (4.7/5). Analysis also found that the requirements for improvement included providing a written summary after receiving the diagnosis and patient perception assessed by the doctor before telling the diagnosis.
Conclusion: Communicating bad news effectively is crucial in the management of cancer patients. The process of BBN should be patient-centered, focusing on patients’ needs. Thus, the current study has demonstrated the patients’ preferences and the requirements, which should be incorporated into BBN protocols.
Keywords: breaking bad news, cancer, patients’ preferences, patients’ satisfaction
Introduction
Breaking bad news (BBN) is one of the most challenging tasks for any physician. Nevertheless, physicians need to communicate bad news to patients or their families in every medical specialty. Dr. Buckman defined bad news in 1984 as “any information which adversely and seriously affects an individual’s view of his or her future”.1 It has also been defined as news with a feeling of no hope, news affecting a person’s mental or physical well-being, upsetting to their lifestyle, or news that conveys fewer choices in his or her life.2 Delivering bad news in inappropriate ways increases the distress and anger of receivers. Furthermore, it may affect their ability to adapt and adjust to the new situation.3
Literature is rich in studies regarding BBN from physicians’ points of view. However, studies from patients’ perspectives are highly needed.4 In Poland, study showed that doctors’ behaviors impact patients’ decisions to continue medical treatment. This study revealed that less than half (47%) of the patients were satisfied by the way bad news was delivered. Furthermore, it concluded that doctors are more efficient in delivering medical information but have trouble in expressive communication with patients’ emotions.5 Various studies have been carried out to evaluate patients’ preferences and satisfaction regarding BBN utilizing different protocols. One of the most widely used is known as the SPIKES protocol created by Baile et al in 2000. The abbreviation SPIKES represents six steps of BBN: Setting up, Perception, Invitation, Knowledge, Emotions, Strategy, and Summary.6 For example, a study conducted in Germany showed that only 46.2% of cancer patients were completely satisfied with how the bad news was delivered to them.7 Moreover, the satisfaction rate in Ethiopia is lower, where the total satisfaction rate among patients with serious illnesses was only 30.6%.8 In addition, a Canadian study found that patients receiving bad news have additional preferences not included in the SPIKES protocol. These included a referral to a support group, an informational sheet or list of resources, a referral to a counselor, expected timely follow-up, and their physician to bear more determination in assisting them with their condition.9
In Saudi Arabia, many studies have been carried out to assess different aspects of BBN. A study in 2009 showed that all participants rejected the concealment of any information regarding their illness and almost all patients wanted to know the benefits and adverse effects of therapy (98% and 99%, respectively). Similarly, all of them wanted to know about the prognosis of their disease.10 In 2010 Dr. Aljubran published a study on Saudi perspectives about BBN which showed that the supportive attitude of patients’ relatives might progress into a dominating one that takes over the patient’s fundamental right to knowledge and decision-making.11 In 2016 another study revealed that patients desire disclosure of most cancer-related bad news, which contrasts with the views and requests of relatives.12 However, data regarding the preference of cancer patients and satisfaction with the protocol of BBN are limited in Saudi Arabia. Therefore, this study aims to assess the patients’ preferences and satisfaction utilizing the SPIKES protocol.
Materials and Methods
Study Design and Participants
This mixed methods study consists of two phases. The first was an in-depth interview, and the second was a cross-sectional survey. The study was aimed at Saudi cancer patients both males and females above 18 years old. Participants were enrolled from the oncology outpatients’ clinics at the university hospital and the oncology specialist hospital of two of the main cities in the Eastern Province of Saudi Arabia, during the period of July 2020 to November 2021.
Sample Size and Sampling Techniques
The in-depth interview included 19 patients. It was performed until theoretical saturation was achieved. The cross-sectional survey comprised 222 patients. This exceeded the minimum required sample size, which was calculated by STATA 11.0 to be 197, at 95% CL, assuming average satisfaction/ reality percent of 44 ± 25 (Sefart et al, 2014) with a margin of error =of 5%.
Data Collection Tools and Processes
Initially, the study team conducted an in-depth interview using a convenient sampling technique to explore the patient preferences regarding breaking bad news based on the SPIKES protocol. Participants were invited to take part in the study before or after completing their consultations. Data were transcribed and/or recorded (with patients consent to do so).
The interview started with a number of open-ended questions about: How do you perceive a good and a bad way of breaking bad news? Tell us about your experience on first receiving your diagnosis and how did you react to receiving this diagnosis? Interview questions have been obtained from Mirza et al’s study.9 The interviews were carried out by two researchers. Each patient was interviewed individually in a private clinic, each interview lasted around 30 minutes. Interviews were audio recorded with participants’ permission and transcribed verbatim. Translation from Arabic to English and reverse translation into Arabic were done by certified translators.
For the second phase of the study, the investigator constructed a 23-item questionnaire combining the 10 existing SPIKES items obtained from the literature with 13 additional items/requirements for breaking bad news from the in-depth interview. The constructed questionnaire was validated by three experts (face validity) and distributed to 20 patients to calculate reliability of the questionnaire using Cronbach’s Alpha which showed an alpha > 0.9. The questionnaire was distributed to measure the patient preference of each item on a scale of 1–5 (1: least preferred and 5 highest preferred). Moreover, the questionnaire investigated patients’ satisfaction/reality with each item studied (on a scale of 1–5).9
Furthermore, questions on sociodemographic characteristics and medical history including the type of cancer and the place of the original diagnosis were also collected.
Data collectors approached the participants personally at the oncology clinics and admission wards or through phone calls. The purpose of the study was fully explained, and participants were informed that the study results are going to be published anonymously. The consent forms were voluntarily signed, and an electronic version of the survey was shared with them. The survey was customized to accept a single response from each number to avoid duplication of responses.
Statistical Analysis
For the qualitative data, thematic analysis was used to explore patients’ satisfaction and preferences about breaking bad news. Each interview was transcribed by listening to the recordings several times to be familiar with the data. Transcripts were then reviewed and double checked by the other researcher. Subsequently, codes were generated and color-coded using Microsoft Word. Subsequently, all relevant codes were condensed into two themes with categories and subcategories. Themes were considered important if they appeared frequently in the data or if a theme captured an important aspect of the research question.
For quantitative analyses, the overall satisfaction was calculated as satisfaction percent (average scores *100/highest possible score). Using IBM Statistical Package for the Social Sciences (SPSS) Statistics for Windows, version 26.0 program, the different factors related to preferences and satisfaction were tested using independent samples t-test and ANOVA. Statistical significance was considered in p < 0.05.
Quality function deployment (QFD) was used to effectively define patient requirements of highest priority. This was done through calculating the gap of satisfaction of each item (5 – mean satisfaction score of the item) and multiplying it by the mean preference score obtained for this item. Since there was no statistically significant difference between satisfaction at the places of the original diagnosis, we used the total score of each item in the QFD.
Ethical Consideration
The study was conducted according to the Helsinki declaration. Ethical approval was granted by the Institutional Review Board (IRB-2020-01-212) of IAU and Dammam’s King Fahad Specialist Hospital (KFSH) to gain the acceptance for data collection. Informed consent was obtained from all voluntary participants after explanation of the study nature. The participants were reassured that all data will be kept confidential, and they have the right to stop at any time while interviewing them to insure the participants’ rights and welfare.
Results
Qualitative Thematic Analysis
The open-ended responses revealed two main themes (Table 1). Theme 1, patients’ requirements for BBN and its categories, which were preferred doctor characteristics, BBN setting, and preferred method of news delivery. Theme 2, patient’s reaction at the time of diagnosis and its categories which were: shock, acceptance of the diagnosis and that the mode of delivery will not change the reaction.
 |
Table 1 Thematic Analysis for Open Ended Survey |
Most of the participants mentioned good verbal communication skills under the preferred doctor characteristic, followed by giving hope and eliminating worries. Regarding the BBN setting, patients commented on the privacy of the setting as the setting was crowded by several trainees. On the other hand, some patients mentioned their preference of the presence of a family member during the breaking of bad news. Gradual delivery of the news was the preferred method of news delivery followed by simplifying the diagnosis and providing a clear plan. With regards to the second theme, many patients were shocked by the news, others mentioned they were not surprised as they expected the diagnosis. In addition, some patients mentioned that they believed their reaction would not have been affected by the way they received the news.
Quantitative Analysis
Regarding the close-ended survey, of the 222 patients who had responded to the survey, females made up 70% of the sample. The highest percent were breast cancer patients (47%), followed by colon cancer (10.4%). Six patients (2.7%) had more than one type of cancer. Details of socio-demographics and diagnosis-related data are shown in (Table 2).
 |
Table 2 Distribution of Cancer Patients According to the Sociodemographic Characteristics and Medical History |
The Cronbach’s Alpha reliability coefficient for scores of preferences was 0.792 and for scores of satisfactions was 0.898 indicating good reliability. Satisfaction score percent ranged from 25.5 to 100%, with a mean of 82.7±11.9%.
The satisfaction scores showed no statistically significant difference by place of original diagnosis, gender, marital status, educational level, monthly income, duration since diagnosis, type of cancer or family history of cancer (Table 3).
 |
Table 3 Association Between Satisfaction Score Percent, Sociodemographic and Cancer Related Data |
Also, there was no correlation between satisfaction score percent and age (r=0.025, p=0.714) nor was there one with the number of children (r=−0.012, p=0.86).
The mean satisfaction score percent of different types of cancers are shown in Figure 1, yet the differences were not statistically significant (F=0.95, p=0.525).
 |
Figure 1 Mean satisfaction score percent by type of cancer. |
Upon examination of cancer patients’ diagnoses and their preferences, the results found that receiving the diagnosis in a calm environment was more preferred in those with any type of cancer (preference score = 4.5 to 5) compared to those who had more than one type of cancer (3) and the one patient who had pancreatic cancer (2) (p=0.0001). Additionally, bringing a family member or a friend was more preferred among patients with breast cancer (4.1) than bladder cancer (1.8) and more than those patients with more than one type of cancer (3.7) (p=0.009).
Checking the patient’s understanding was more preferred in breast cancer and colon cancer patients (4.8 and 4.9, respectively) than in prostate cancer patients (3.3) (p=0.026).
Sociodemographic characteristics and family history were also assessed for any potential correlations with patients’ preference. The results showed that doctor’s empathy had a higher score in those who had a family history (4.9) than those who did not (4.5), p=0.011 and giving hope to the patient was of a higher preference in those with a high school education (4.9) when compared with those with a bachelor’s degree (4.6), p=0.0001. Also, checking patients’ understanding had the lowest preference score among patients diagnosed over 5 years or more (4.2) than those with a more recent diagnoses (4.8) p<0.0001.
Studying the different requirements for BBN, the most preferred items were mainly concerned with the doctor being honest and encouraging, good listener and interacting, gives simple smooth explanation without using medical terms and empathetic (average score 4.8/5). Also, providing the diagnosis in a calm and a private environment (4.7/5).
While the requirements that had a lower preference score were receiving the diagnosis in a direct way not gradually (2.7), using alternative words of cancer by the doctor (3.2), being alone with the doctor (3.3), doctor consoling the patient by patting his/her shoulder, holding hand or hugging the patient during the delivery of the diagnosis (3.3) and providing a psychologist at the time of diagnosis (3.6) (Table 4).
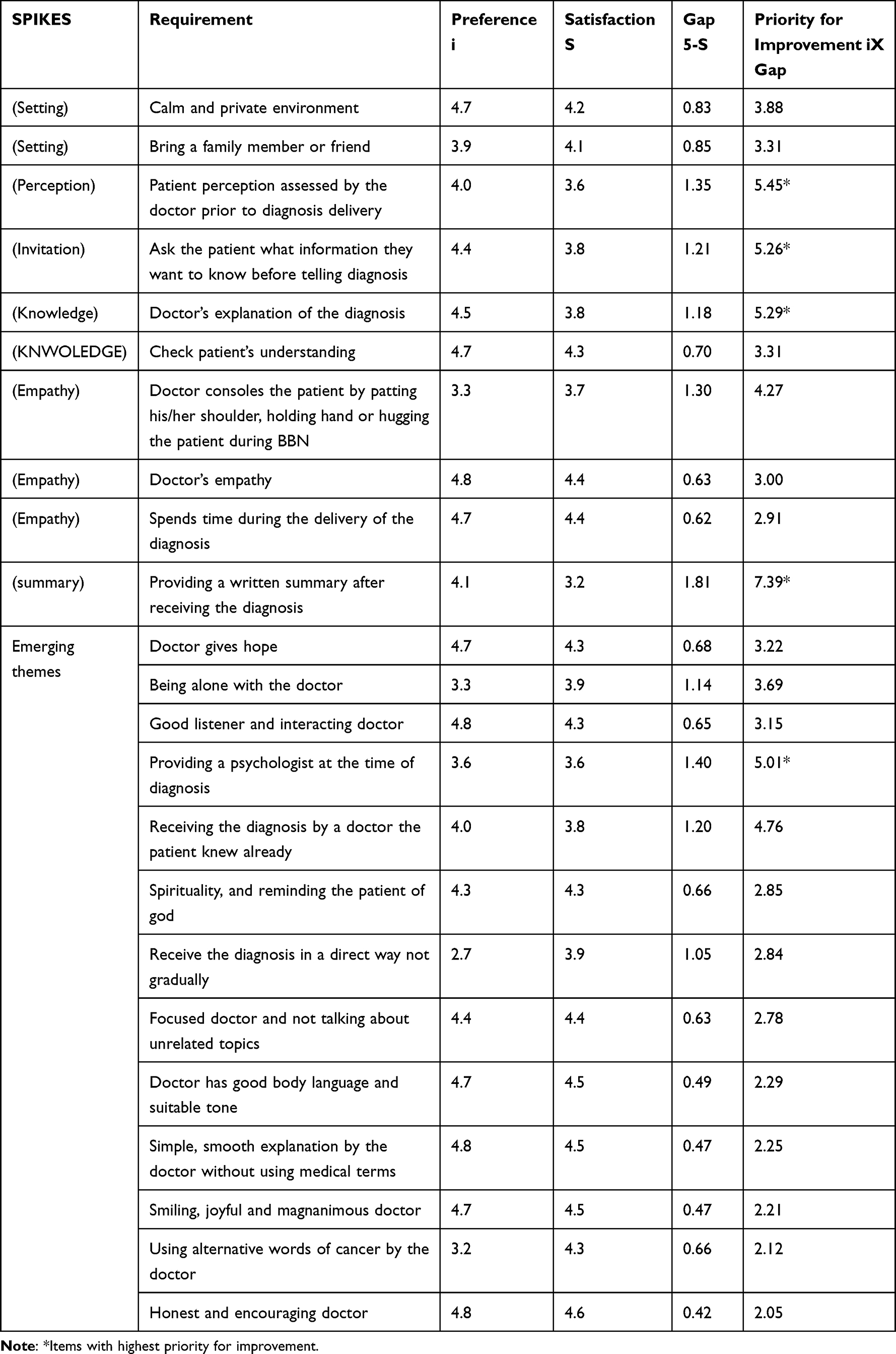 |
Table 4 Priority for Improvement Based on the Gap Between Satisfaction and Preferences of Cancer Patients Based on the SPIKES Model |
Considering the gaps between the highest attainable satisfaction scores weighted by patients ‘preferences, the requirements that should have the priority in improvement were providing a written summary after receiving the diagnosis, patient perception assessed by the doctor before telling the diagnosis (Perception), doctor’s explanation of the diagnosis (knowledge), asking the patient what information they expect to know before informing them of the diagnosis (Invitation), providing a psychologist at the time of diagnosis and receiving the diagnosis by a doctor the patient already knew (Table 4).
Discussion
BBN is a challenge to any physician, and requires proper communication skills.13,14 Various recommendations were designed for consultations that involve the delivery of bad news. However, the utilization of the SPIKES protocol was mostly studied worldwide, especially among cancer patients.7 Understanding the patient’s preferences and satisfaction, from different cultures and backgrounds, on every item in the protocol is crucial to guide the discussion in delivering the bad news. In Saudi Arabia, studies from patients’ perspectives are few, and it is still not known whether and how the SPIKES protocol items meet the patients’ expectations. The qualitative part of the current study suggested the addition of 13 new items to the original SPIKES protocol. Using these new items with the original ones, the overall mean satisfaction score of BBN to patients in this study was 82.7%.9 This was higher than studies from Ethiopia (30.6%), Germany (46.2%), and the United Kingdom (60%).7,8,15 The higher satisfaction score in the current study could reflect the undergraduate and postgraduate training of students and physicians in Saudi Arabia in the doctor-patient relationship, communication skills, and BBN. These skills were administered in the undergraduate and postgraduate curricula in Saudi Arabia.16,17
The current study did not demonstrate an association between patients’ characteristics and their satisfaction with the way they received bad news. A similar insignificant association was found between the satisfaction score and the patient’s type of cancer. However, the one patient with pancreatic cancer had the lowest satisfaction score. This finding could be attributed to the poor prognosis that is usually associated with this type of cancer at the time of diagnosis.18 Nevertheless, this study has reported pancreatic cancer in one patient only, thus further evaluation of such finding is needed.
In the current study some of the new added items to the existing SPIKES protocol had the highest satisfaction and preference scores. Such as an honest and encouraging doctor, a good listener, good body language joyful with a suitable tone. These findings indicate that physicians’ attitude while delivering bad news is essential, parallel to the content of the message, as the patients appreciate these values.7–9,19,20 Moreover, doctors’ empathy and delivering bad news in a calm and private environment also had higher preference scores in the current study. Arrangement of the setting is essential to prepare for the consultation. A cross-sectional study from Germany revealed that having adequate consultation time and avoiding interruptions were important requests by cancer patients while BBN.7 Similarly, Mirza et al revealed that most patients (85%) thought it is necessary to sit in a quiet and private room when receiving bad news.9 Arrangement of the setting is not only a reflection of the physician’s behavior but can also be affected by organizational factors, such as workload and room capacity. Thus, the policymakers in healthcare facilities must be conscious of these patients’ demands.7,21,22
An interesting finding of low patients’ preference for touching, holding hands, or hugging the patient while BBN was consistent with the results reported in a Canadian study.9 This could be attributed to the cultural system in society which usually draws the boundaries of any relationship, including doctor-patient relationship, especially among opposing genders. Additionally, directly receiving the diagnosis, using alternative words of cancer by the physician, being alone with the doctor, and providing a psychologist at the time of diagnosis were also the lowest preferred items by the patients in the present study.
In this regard, several factors influence the patient’s communication preferences regarding BBN. These factors include but are not limited to the patient’s demographics, medical and psychological history, and cultural and spiritual background—besides factors related to the facilitator, content, and environmental settings.21,23 The literature on the association between patients’ preferences in BBN and their cancer type is scarce; hence, we attempted to explore this aspect in our study.
A family member’s role in disclosing a cancer diagnosis varies between cultures and practices. For instance, the eastern “community-oriented” cultures tend to refrain from discussing the cancer diagnosis directly with the patient; instead, they involve the patient’s family in the process. On the other hand, the western “individual-oriented” cultures value patients’ autonomy and honor patients’ preference on whether or not to involve their families in the cancer diagnosis disclosure.24,25 Our study shows an apparent preference for bringing a family member or a friend into the BBN discussion, especially in patients diagnosed with breast cancer compared to other types of cancers. This may be attributed to the sensitivity of the cancer type, especially among women, which emphasizes the importance of patients’ support systems.
Ensuring the patients’ understanding of their cancer diagnosis is an integral part of the SPIKES protocol. We found that patients with breast and colorectal cancer diagnoses prefer that their doctor check their understanding of the diagnosis. This is especially important considering the tendency of physicians to use medical jargon during such conversations. Several studies have described patients’ preference for an understandable conversation devoid of medical terminology.26,27 Furthermore, patients with recent cancer diagnoses reported a higher preference for doctors checking their understanding of their diagnosis than those with earlier diagnoses (more than five years). This comes as no surprise as patients tend to have a better understanding as they go through the diagnosis and treatment process.
The importance of the provider’s emotional support and optimism in the process of BBN cannot be over-emphasized. Physicians’ pessimistic and unsympathetic manner were cited as a primary reason for patients’ dissatisfaction, according to a study at a cancer center in the United Kingdom.15 In our study, giving hope to patients diagnosed with cancer was strongly preferred in those with high school degrees compared to those with bachelors’ degrees. In a Malaysian study of two hundred cancer patients, the skill of offering hope has been rated as an “essential skill” in cancer communication.20 A plausible explanation is that educated people have a rational understanding of their diagnosis and access to facts and information that may influence the expectations of their disease prognosis. While these findings are unique in correlating the patient’s preferences in communication and their cancer diagnosis, we must take these observations with caution given the variability in the prevalence of different cancer types and the small sample size of this study.
Our study revealed that the highest priority for improvement was providing a written summary after diagnosis. The disclosure and discussion of serious health issues can overwhelm patients and doctors alike. Thus, patients may forget or improperly understand the information they are given. Evidence has been established that patients desire more information about their health conditions, treatment, and outcomes.28 Furthermore, providing written information improves patients’ knowledge, attitudes, and behaviors towards their medical condition.29 Patient factors such as age, health literacy, and reading ability must be considered when planning for and delivering such information.
The second top priority for improvement was having their perception assessed by the doctor before being told about the diagnosis. A Sudanese study of 192 participants explored the physicians’ adherence to SPIKES protocol and found that almost all (>90%) of them either “sometimes” or “usually” ask their patients about their perception before telling them the diagnosis.17 While these findings might not be fully generalizable, they show an apparent discrepancy between the reality of patients’ needs and the physicians’ perception of their practices.
The explanation of the diagnosis by the doctor was the third identified priority. While this may seem a prominent element of BBN, getting an explanation of the disease has been previously cited with significant disparity between patients’ preferences and their experiences.7 Moreover, asking the patient what information they wanted to know before telling them their diagnosis was identified as a priority in our study. In a study of 400 patients assessing their perspectives and expectations, participants suggested that the doctor should break the news, check if the information has been understood, and pause to allow for clarifying questions.30 Besides supporting our finding, this highlights the importance of exploring whether the patient needs to know more about their disease and providing additional information about the cancer diagnosis.
Interestingly, involving a psychologist when discussing the diagnosis has emerged as a new theme. A prior work by Alrukban et al in Riyadh, Saudi Arabia, explored this aspect in their cross-sectional study that involved more than 1000 Saudi adults. In contrast to women, who preferred the physician to break the news, men strongly preferred psychologists or social workers.22 Given the scope of medical practice that sets the responsibility of medical diagnosis and treatment on the physician, these findings suggest a unique demand for support by a trained professional (eg, psychologist), besides the doctor, at the time of BBN.
As cancer incidence rises, understanding cancer patients’ needs and expectations will help dramatically in managing such cases. To the best of our knowledge, this study is the first Saudi study that addresses patients’ perspectives regarding BBN. Moreover, the study participants were obtained from different levels of care. In addition, the mixed methods design of the study provides an in-depth analysis and a comprehensive understanding of patients’ viewpoints. However, some limitations exist. The study design was cross-sectional; therefore, the temporality and causality cannot be inferred. Furthermore, due to the retrospective nature of the study, the possibility of recall bias could not be eliminated. Additionally, the sample size was small, most of the respondents were females with breast cancer, and the study population was only obtained from a single region, thus it did not represent the general population.
Conclusion
This study illustrated that the mean satisfaction score of cancer patients about the way they received the diagnosis was 82.7. Furthermore, no significant association was found between patients’ sociodemographic factors, type of cancer, and satisfaction scores. Additionally, the study has revealed new preferences which were not addressed by the SPIKES protocol. Most of them focused on doctors’ attitudes and communication skills. Moreover, issues such as providing a written summary after receiving the diagnosis and assessing patient perception prior to BBN needs improvement. Thus, further studies on large-scale populations are recommended to tackle patients’ needs and preferences. Moreover, continuous formal training for doctors should be maintained to meet patients’ needs. In addition, hospitals should ensure that BBN is done professionally.
Acknowledgments
The authors would like to acknowledge the contribution of patients in the study. Also, we thank the patients’ relatives and medical providers who facilitated communication with the patients.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Buckman R. How to Break Bad News: A Guide for Health Care Professionals. JHU Press; 1992.
2. Ptacek JT, Eberhardt TL. Breaking bad news. A review of the literature. JAMA. 1996;276(6):496–502. doi:10.1001/jama.1996.03540060072041
3. Fallowfield L, Jenkins V. Communicating sad, bad, and difficult news in medicine. Lancet. 2004;363(9405):312–319. doi:10.1016/s0140-6736(0315392-5
4. Dean A, Willis S. The use of protocol in breaking bad news: evidence and ethos. Int J Palliat Nurs. 2016;22(6):265–271. doi:10.12968/ijpn.2016.22.6.265
5. Sobczak K, Leoniuk K, Janaszczyk A. Delivering bad news: patient’s perspective and opinions. Patient Prefer Adherence. 2018;12:2397–2404. doi:10.2147/PPA.S183106
6. Baile WF, Buckman R, Lenzi R, Glober G, Beale EA, Kudelka AP. SPIKES—A six-step protocol for delivering bad news: application to the patient with cancer. Oncologist. 2000;5(4):302–311. doi:10.1634/theoncologist.5-4-302
7. Seifart C, Hofmann M, Bär T, Riera Knorrenschild J, Seifart U, Rief W. Breaking bad news–what patients want and what they get: evaluating the SPIKES protocol in Germany. Ann Oncol. 2014;25(3):707–711. doi:10.1093/annonc/mdt582
8. Fisseha H, Mulugeta W, Kassu RA, Geleta T, Desalegn H. Perspectives of protocol based breaking bad news among medical patients and physicians in a teaching hospital, Ethiopia. Ethiop J Health Sci. 2020;30(6):1017–1026. doi:10.4314/ejhs.v30i6.21
9. Mirza RD, Ren M, Agarwal A, Guyatt GH. Assessing patient perspectives on receiving bad news: a survey of 1337 patients with life-changing diagnoses. AJOB Empir Bioeth. 2019;10(1):36–43. doi:10.1080/23294515.2018.1543218
10. Al-Amri AM. Cancer patients’ desire for information: a study in a teaching hospital in Saudi Arabia. East Mediterr Health J. 2009;15(1):19–24. doi:10.26719/2009.15.1.19
11. Aljubran AH. The attitude towards disclosure of bad news to cancer patients in Saudi Arabia. Ann Saudi Med. 2010;30(2):141–144. doi:10.4103/0256-4947.60520
12. Zekri J, Karim SM. Breaking cancer bad news to patients with cancer: a comprehensive perspective of patients, their relatives, and the public—example from a Middle Eastern country. J Glob Oncol. 2016;2(5):268–274. doi:10.1200/jgo.2015.001925
13. Ferreira da Silveira FJ, Botelho CC, Valadão CC. Breaking bad news: doctors’ skills in communicating with patients. Sao Paulo Med J. 2017;135(4):323–331. doi:10.1590/1516-3180.20160221270117
14. Dafallah MA, Ragab EA, Salih MH, et al. Breaking bad news: awareness and practice among Sudanese doctors. AIMS Public Health. 2020;7(4):758–768. doi:10.3934/publichealth.2020058
15. Brown VA, Parker PA, Furber L, Thomas AL. Patient preferences for the delivery of bad news - the experience of a UK cancer centre. Eur J Cancer Care (Engl). 2011;20(1):56–61. doi:10.1111/j.1365-2354.2009.01156.x
16. Al-Mohaimeed A, Midhet F, Barrimah I, Khan NZ, Sharaf FK, Alnohair S. Students’ perceptions about the family medicine course in Qassim, Saudi Arabia. Med Teach. 2014;36(Suppl 1):S49–S54. doi:10.3109/0142159x.2014.886010
17. Al-Mohaimeed AA, Sharaf FK. Breaking bad news issues: a survey among physicians. Oman Med J. 2013;28(1):20–25. doi:10.5001/omj.2013.05
18. Alghamdi IG, Almadi M, Alsohaibani F, et al. Epidemiology of pancreatic cancer in Saudi Arabia: a retrospective analysis of pancreatic cancer diagnosed in Saudi Arabia between 2004 and 2015. Clin Exp Gastroenterol. 2021;14:45–57. doi:10.2147/ceg.s289269
19. Bumb M, Keefe J, Miller L, Overcash J. Breaking bad news: an evidence-based review of communication models for oncology nurses. Clin J Oncol Nurs. 2017;21(5):573–580. doi:10.1188/17.cjon.573-580
20. Eng TC, Yaakup H, Shah SA, Jaffar A, Omar K. Preferences of Malaysian cancer patients in communication of bad news. Asian Pac J Cancer Prev. 2012;13(6):2749–2752. doi:10.7314/apjcp.2012.13.6.2749
21. von Blanckenburg P, Hofmann M, Rief W, Seifart U, Seifart C. Assessing patients´ preferences for breaking bad news according to the SPIKES-protocol: the MABBAN scale. Patient Educ Couns. 2020;103(8):1623–1629. doi:10.1016/j.pec.2020.02.036
22. Alrukban MO, Albadr BO, Almansour M, et al. Preferences and attitudes of the Saudi population toward receiving medical bad news: a primary study from Riyadh city. J Family Community Med. 2014;21(2):85–92. doi:10.4103/2230-8229.134763
23. Fujimori M, Akechi T, Uchitomi Y. Factors associated with patient preferences for communication of bad news. Palliat Support Care. 2017;15(3):328–335. doi:10.1017/S147895151600078X
24. Mitchell JL. Cross-cultural issues in the disclosure of cancer. Cancer Pract. 1998;6(3):153–160. doi:10.1046/j.1523-5394.1998.006003153.x
25. Chaturvedi SK, Loiselle CG, Chandra PS. Communication with relatives and collusion in palliative care: a cross-cultural perspective. Indian J Palliat Care. 2009;15(1):2–9. doi:10.4103/0973-1075.53485
26. Kim MK, Alvi A. Breaking the bad news of cancer: the patient’s perspective. Laryngoscope. 1999;109(7):1064–1067. doi:10.1097/00005537-199907000-00010
27. Randall TC, Wearn AM. Receiving bad news: patients with haematological cancer reflect upon their experience. Palliat Med. 2005;19(8):594–601. doi:10.1191/0269216305pm1080oa
28. Ley P. Improving patients’ understanding, recall, satisfaction and compliance. Health Psychology. 1989;74–102. doi:10.1007/978-1-4899-3228-0-5
29. Weinman J. Providing written information for patients: psychological considerations. J R Soc Med. 1990;83(5):303–305. doi:10.1177/014107689008300508
30. Ishaque S, Saleem T, Khawaja FB, Qidwai W. Breaking bad news: exploring patient’s perspective and expectations. J Pak Med Assoc. 2010;60(5):407–411.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.