")
Back to Journals » Clinical Ophthalmology » Volume 17
Botulinum Toxin Injection versus Extraocular Muscle Surgery for Acute Acquired Comitant Esotropia
Authors Suwannaraj S, Rojanasaksothron C, Methapisittikul Y, Wongwai P, Yospaiboon Y
Received 10 December 2022
Accepted for publication 26 January 2023
Published 31 January 2023 Volume 2023:17 Pages 413—420
DOI https://doi.org/10.2147/OPTH.S401019
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Sirinya Suwannaraj, Chawisa Rojanasaksothron, Yanasiri Methapisittikul, Phanthipha Wongwai, Yosanan Yospaiboon
KKU Eye Center, Department of Ophthalmology, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand
Correspondence: Yosanan Yospaiboon, KKU Eye Center, Department of Ophthalmology, Faculty of Medicine, Khon Kaen University, 123 Mitraparb Highway, Khon Kaen, 40002, Thailand, Tel +66-4336-3010, Fax +66-4334-8383, Email [email protected]
Purpose: To compare the success rate of extraocular muscle surgery and botulinum toxin injection for treatment in patients with acute acquired comitant esotropia (AACE).
Patients and Methods: This is a retrospective cohort study in which we treated 34 patients of AACE with botulinum toxin compared with 80 patients who had been treated with surgery. The data included angle of deviation in prism diopter (PD) at baseline and one, three, and six months after treatment. The main outcome was the success rate in each treatment group.
Results: In the surgery group, mean esodeviation angles at baseline and one, three, and six months after treatment were 50.8 ± 18.3 PD, 4.9 ± 8.3 PD, 4.6 ± 9.5 PD, and 5.5 ± 10.3 PD, whereas those in the botulinum toxin group were 51.2 ± 14.3 PD, 13.9 ± 17.4 PD, 22.0 ± 19.3, and 31.3 ± 23.8 PD, respectively. There was a statistically significant difference in the deviation angles between the two groups (p < 0.001). The success rate in the surgery group at one, three, and six months was 81%, 84%, and 79%, whereas that in the botulinum toxin group was 50%, 27%, and 27%.
Conclusion: Botulinum toxin injection was not as effective as conventional extraocular muscle surgery in AACE patients. However, the treatment is safe, fast-acting, and improves both cosmetic appearance and quality of life. This may be considered as a chance for patients not preferring surgery.
Keywords: botulinum toxin, muscle surgery, acute acquired comitant esotropia
Introduction
Esotropia is a common type of strabismus that mostly occurs after infancy or during childhood, but it could appear in adults or even the elderly.1,2 Acute acquired comitant esotropia (AACE) is a subtype of esotropia defined by acute onset, the same deviation angle in all directions of gaze, and normal ocular motility.3 AACE can have various causes such as visual deprivation, refractive error, neurological abnormality, and excessive near work.3–5 The incidence of AACE appears to have risen in recent years, which may be attributable to increased computer and smartphone use. Moreover, the COVID-19 pandemic has led to more people working and studying online, which may aggravate the condition.6,7 AACE may reduce the quality of life, causing diplopia, impaired stereopsis, and/or cosmetic, social, and amblyopic problems, the latter of which may lead to poor vision and blindness in children.
Currently, choices for treatment include horizontal rectus muscle surgery2,8 and botulinum toxin injection.9,11 Due to the increasing number of AACE patients and insufficient hospital resources, the waiting list for surgery can be extremely long. In such cases, botulinum toxin may be employed as an alternative treatment. However, its rate of success remains unclear, as does the duration of its effect. Previous studies have reported botulinum toxin injection as being as effective as conventional rectus muscle surgery.4,9,13 However, the samples in those studies were too small to draw a definitive conclusion. Based on our personal clinical experience, we hypothesize that botulinum toxin may not be as effective as strabismus surgery and the magnitude of deviation may alter the result of treatment. The aim of this study was, therefore, to compare the success rate of strabismus surgery with that of botulinum toxin injection and compare the results in different magnitude of deviation angle in a larger series of AACE patients.
Patients and Methods
This retrospective cohort study was conducted in accordance with the Declaration of Helsinki and was approved by the Khon Kaen University Ethics Committee for Human Research (HE641629). Medical records of AACE patients who had been treated either by rectus muscle surgery or botulinum toxin injection at the KKU Eye Center, Srinagarind Hospital, Khon Kaen University, Thailand, from January 2014 to October 2021 were comprehensively reviewed. Although patient consent to review their medical records was not required by the ethics committee, the data in case report forms nevertheless had no linkage to the patient identities and the patient data confidentiality was protected. Diagnostic criteria of AACE consisted of acute onset, the same deviation angle in all directions of gaze, and normal ocular motility. Inclusion criteria were patients who met these diagnostic criteria and had at least six-month follow-up period. Exclusion criteria were hyperopia > +2.5 D, an incomitant deviation, nystagmus, sixth cranial nerve palsy, intracranial pathology, restrictive strabismus, and having undergone simultaneous rectus muscle surgery and botulinum toxin injection. Patients who were lost to follow-up or underwent retreatment with surgery or botulinum toxin injection within six months after treatment were also excluded.
The collected data included gender, age at onset and treatment, best-corrected visual acuity (BCVA), history of amblyopia, and treatment complications. Cycloplegic or manifest refraction was recorded and calculated as spherical equivalent. Deviation angle sizes at baseline and one, three, and six months after treatment were assessed using alternate prism cover test at distance. Symptoms of diplopia were also recorded at each time point.
Botulinum toxin injections were performed by a single surgeon (SS) with the patient under either general or local anesthesia, depending on their age, without electromyographic guidance or conjunctival incision. Only the medial rectus muscle in the deviating eye was injected with botulinum toxin. The medial rectus muscle was grasped transconjunctivally with forceps, and 5 IU per 0.1 mL of botulinum toxin A (BOTOX®, Allergan, Inc., Irvine, California, US) was transconjunctivally injected at 10 mm behind the insertion point of the muscle with a 27 G needle on an insulin syringe.
Horizontal rectus muscle surgery was performed by two surgeons (SS and PW). Medial rectus recession and lateral rectus resection in the deviating eye was the procedure of choice.
The primary outcome measure was the comparative success rate of botulinum toxin injection and rectus muscle surgery at six months after treatment. Success was defined as a postoperative horizontal deviation angle <10 prism diopters (PD) and failure as ≥10 PD or consecutive exotropia of any angle. The secondary outcome was to compare the results of treatment between pre-operative small and large deviation angles. Complication of the treatment was also recorded.
Statistical Analysis
All statistical analyses were performed using STATA version 10.1 (StataCorp, College Station, TX, USA). Categorical data were compared by using a Chi-square or Exact probability test. An independent t-test with unequal variances was used to compare continuous data between groups. The success rates of the two groups were analyzed using logistic regression. P-value of less than 0.05 was considered statistically significant.
Results
A total of 114 patients (67 males and 47 females) were included in this study: 80 in the surgery group and 34 in the botulinum toxin group. The mean age of the patients at treatment was 13.9 years (range 5 to 59 years). The mean best-corrected visual acuity (LogMAR) was 0.24 ± 0.47 (range: 0 to 2.3), and spherical equivalent was −0.21 ± 2.79 (range: −6.75 to +6.00) diopter. There were 65 (58%) patients diagnosed with amblyopia. Other baseline characteristics are shown in Table 1.
 |
Table 1 Summary of Patients’ Baseline Characteristics |
The patients were divided into two subgroups by pre-operative deviation angle: small angle (preoperative deviation angle ≤40 PD; n = 32, 28%) and large angle (preoperative deviation angle >40 PD; n = 82, 72%). The overall mean preoperative and postoperative angle of deviation at one, three, and six months is shown in Table 2. Surgery exhibited a better therapeutic effect than botulinum toxin injection at six months in all subgroups (5.5 PD vs 31.3 PD; p<0.001). However, this difference was not statistically significant in the small-angle subgroup (Table 2).
 |
Table 2 Preoperative and Postoperative Angle of Deviation |
The success rate of both groups at one, three, and six months is shown in Table 3. Surgery also showed a better success rate than botulinum toxin injection at six months with statistical significance (78.8% vs 26.5%; p<0.001). The success rate declined over time in both botulinum toxin subgroups, whereas in the surgery group, the postoperative angle of deviation was more stable over the six-month period in both subgroups (Table 3).
 |
Table 3 Success Rate of Surgery and Botulinum Toxin Injection |
In our study, if the first treatment failed, reoperation or a second botulinum toxin injection was scheduled after six months. The decision as to whether to proceed with botulinum toxin or rectus muscle surgery as the second procedure depended on the patient’s preference and their response to botulinum toxin injection. If the patient responded to botulinum toxin injection, a second injection was scheduled. Otherwise, surgery was performed.
Mean pre- to post-operative improvement in deviation angle at one, three, and six months was 37.3 ± 18.9, 29.2 ± 19.3, and 19.9 ± 21.9 PD in the botulinum toxin group and 45.9 ± 17.2, 45.3 ± 17.4, and 45.3 ± 18.9 in the surgery group (Figure 1). For the small-angle subgroup, mean improvement was 24.7 ± 8.9, 16.7 ± 11.6, and 13.6 ± 13.2 PD in the botulinum toxin group and 27.5 ± 9.3, 27.7 ± 9.0, and 26.7 ± 12.6 in the surgery group (Figure 2). In the large angle subgroup, mean improvement was 40.6 ± 19.6, 32.5 ± 19.7, and 21.6 ± 23.5 PD in the botulinum group and 54.3 ± 12.8, 54.6 ± 13.3, and 53.8 ± 14.8 in the surgery group (Figure 3). Mean deviation angle improvement declined over time in the botulinum toxin group compared to the more stable angle reduction in the surgery group.
 |
Figure 1 Improvement in the angle of deviation after treatment compared between the botulinum toxin and surgery groups. |
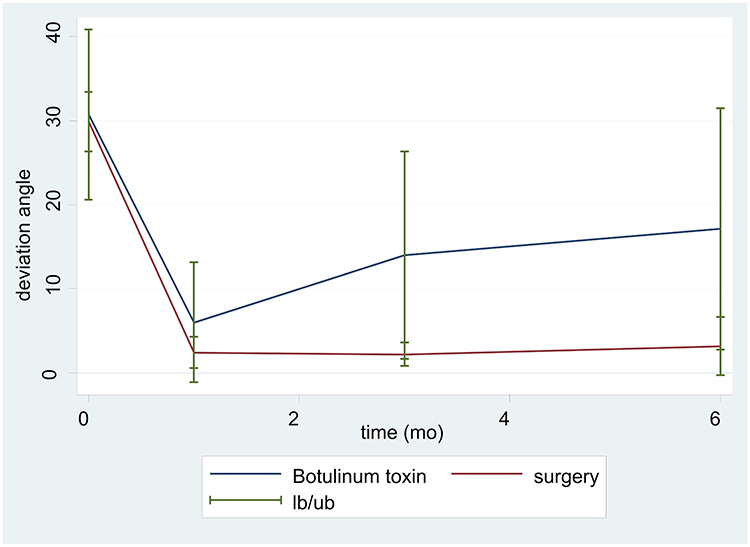 |
Figure 2 Improvement in the angle of deviation after treatment (small-angle subgroup). |
 |
Figure 3 Improvement in the angle of deviation after treatment (large-angle subgroup). |
There were 54 patients in the surgery group and 32 in the botulinum toxin group, who had complete record of diplopia. Thirty-seven patients (68.5%) in the surgery group and 26 (81.3%) in the botulinum toxin group had preoperative diplopia. This number declined in all treatment groups, leaving eight patients (15.1%) in the surgery group and 17 (60.7%) in the botulinum toxin group experiencing residual diplopia at six months.
The most common complication in this study was ptosis, which occurred most frequently in the botulinum toxin group (11/34, 32.4%), but all cases were transient and resulted in full recovery. Consecutive exotropia occurred in two (5.9%) patients in the botulinum toxin group, both of whom recovered spontaneously within six months. In the surgery group, there were three (3.8%) cases of consecutive exotropia, two of which were transient, with the other persisting at six months after surgery. There were no serious complications such as globe perforation, muscle loss or slipping, and postoperative infection in this study.
Discussion
Currently, there are various choices for AACE treatment, two of which are conventional horizontal rectus muscle surgery2,8 and botulinum toxin injection.9–11 The principle of both treatments is to weakening the medial rectus muscle. Common choices of surgery can be either recession of the medial rectus and resection of the lateral rectus muscle in the deviating eye or medial rectus recession in both eyes. Botulinum toxin treatment, in the same manner, can be either injection at medial rectus in deviating eye or medial rectus muscles in both eyes.8 Botulinum toxin was first used to treat strabismus in 197911 and is now regularly used to treat various types of strabismus, including AACE.4,9–13
In this study, patients with AACE received either botulinum toxin injection or horizontal rectus muscle surgery. There were more males than females in both treatment groups and no significant difference in baseline characteristics, with the exception of logMAR visual acuity, which was better in the botulinum toxin group. However, this difference did not impact the primary results of the study.14 Generally, the younger the patient and the smaller the preoperative angle of deviation, the better the treatment effect.9,15,16 However, in our study, age at treatment and preoperative angle of deviation did not differ significantly between the two groups.
Our study demonstrated that the horizontal rectus muscle surgery was more effective than botulinum toxin injection in the treatment of AACE in all subgroups and all time periods (one, three, and six months after treatment). The success rate in the surgery group reached 81.3% at one month after surgery and then declined slightly to 78.8% at six months. However, in the botulinum toxin group, it was only 50% at one month after injection and declined to just 26.5% at six months. The success rate of surgery was also higher in both preoperative deviation angle subgroups.
Our results are not consistent with previous studies. A randomized clinical trial by Lang et al13 showed no significant difference in success rate between patients who underwent surgery (n = 16) and those given botulinum toxin (n = 13) at six months (81.3% vs 84.6%; p = 1.00). A study by Wan et al9 with 33 patients in the surgery group and 16 in the botulinum toxin group yielded similar results at six and 18 months (61% vs 81%, p = 0.20, and 58% vs 67%, p = 0.74, respectively). A prospective non-randomized clinical study by Shi et al,4 with 20 cases in the surgery group and 40 in the botulinum toxin group, also found no significant difference. This discrepancy from our study may be attributable to the difference in doses and methods of botulinum toxin injection. Our study used only a single 5 IU dose of botulinum toxin in all cases, whereas Shi study4 administered repeated injections if the patient had not achieved orthotropia or had a deviation angle within 10 PD. In our study, injection was made in only one medial rectus muscle of the deviating eye, whereas both medial rectus muscles were injected with 5 IU dose in the Wan study9 and 2.5 IU dose in the Lang study.13
A retrospective study by Xu et al17 examined 29 AACE patients who received botulinum toxin injection to determine the treatment’s effectiveness. The dose of botulinum toxin used varied by preoperative deviation angle (5 IU, 6 IU, and 7 IU for deviation angles of 20–40 PD, 40–60 PD, and 60–80 PD, respectively), which resulted in a success rate of 86.2% at six months and 82.8% at the final follow-up. The higher success rates than in our study may be explained by the fact that botulinum toxin is dose dependent, so a dose greater than 5 IU may be more effective in patients with a large preoperative deviation angle, as may bilateral injection.16,18 However, Xu et al used 5 IU in patients with a preoperative deviation angle of 20–40 PD, the same amount that was administered in the small-angle subgroup in our study. The difference in success rate may thus have been due to differences in surgical technique and method of injection. The conjunctival microincision technique and 2.5 IU injection in both medial recti may be more effective than 5 IU injected into the medial rectus of the deviating eye in our study. Interestingly, the 5 IU fixed dose in our study reduced the angle of deviation to a greater extent in the large-angle than in the small-angle subgroup.
The effects of botulinum toxin declined over time. However, although the direct effect of botulinum toxin lasted only three months, its effect on eye position can last longer.19 In Xu study, the effects lasted longer than six months,17 and in our study, the deviation angle was smaller at six months than before treatment. This long-lasting effect may be beneficial to patients who refuse conventional surgery or general anesthesia. Moreover, it can improve cosmetic appearance and quality of life, while the patient is waiting to undergo conventional surgery.
The strengths of our study included the larger series of patients compared to previous studies and no missing data. However, there were some limitations including the short follow-up time, and only the motor success rate was interpreted. The sensory results were not presented in this study due to incomplete data on binocular vision and stereopsis. Although the follow-up duration was only six months, it was adequate to determine the effects of both treatments.
Conclusion
Botulinum toxin injection was not as effective as conventional surgery in AACE patients, and its effects were temporary. However, it had some therapeutic effect, and the procedure is simple, rapid in action, and has no serious side effects. This may be considered as a chance for patients not preferring surgery.
Acknowledgments
The authors thank Dr. Kaewjai Thepsuthammarat, Clinical Epidemiology Unit, Faculty of Medicine, Khon Kaen University for statistical analysis, and Dr. Dylan Southard for assistance with the English-language presentation of the manuscript, via the KKU Publication Clinic (Thailand). This study was supported by a research grant (IN 62339) from the Khon Kaen University Faculty of Medicine.
Disclosure
The authors report no conflicts of interest in this work.
References
1. McKean-Cowdin R, Cotter SA, Tarczy-Hornoch K, et al. Prevalence of amblyopia or strabismus in asian and non-Hispanic white preschool children. Ophthalmology. 2013;120(10):2117–2124. doi:10.1016/j.ophtha.2013.03.001
2. Chen J, Deng D, Sun Y, et al. Acute acquired concomitant esotropia: clinical features, classification, and etiology. Medicine. 2015;94(51):e2273. doi:10.1097/MD.0000000000002273
3. Meng Y, Hu X, Huang X, et al. Clinical characteristics and etiology of acute acquired comitant esotropia. Clin Exp Optom. 2022;105(3):293–297. doi:10.1080/08164622.2021.1914510
4. Shi M, Zhou Y, Qin A, Cheng J, Ren H. Treatment of acute acquired concomitant esotropia. BMC Ophthalmol. 2021;21(1):9. doi:10.1186/s12886-020-01787-1
5. Clark AC, Nelson LB, Simon JW, Wagner R, Rubin SE. Acute acquired comitant esotropia. Br J Ophthalmol. 1989;73(8):636–638. doi:10.1136/bjo.73.8.636
6. Vagge A, Giannaccare G, Scarinci F, et al. Acute acquired concomitant esotropia from excessive application of near vision during the COVID-19 lockdown. J Pediatr Ophthalmol Strabismus. 2020;57:e88–e91. doi:10.3928/01913913-20200828-01
7. Mohan A, Sen P, Mujumdar D, Shah C, Jain E. Series of cases of acute acquired comitant esotropia in children associated with excessive online classes on smartphone during COVID-19 pandemic; digital eye strain among kids (DESK) study-3. Strabismus. 2021;29(3):163–167. doi:10.1080/09273972.2021.1948072
8. Lekskul A, Chotkajornkiat N, Wuthisiri W, Tangtammaruk P. Acute acquired comitant esotropia: etiology, clinical course, and management. Clin Ophthalmol. 2021;15:1567–1572. doi:10.2147/OPTH.S307951
9. Wan MJ, Mantagos IS, Shah AS, Kazlas M, Hunter DG. Comparison of botulinum toxin with surgery for the treatment of acute-onset comitant esotropia in children. Am J Ophthalmol. 2017;176:33–39. doi:10.1016/j.ajo.2016.12.024
10. Dawson EL, Marshman WE, Adams GG. The role of botulinum toxin A in acute-onset esotropia. Ophthalmology. 1999;106(9):1727–1730. doi:10.1016/S0161-6420(99)90360-3
11. Scott AB. Botulinum toxin injection into extraocular muscles as an alternative to strabismus surgery. Ophthalmology. 1980;87(10):1044–1049. doi:10.1016/S0161-6420(80)35127-0
12. Wang X, Wu X. The role of botulinum toxin for acute-onset concomitant esotropia: a pilot study. Ophthalmol China. 2010;19:110–112.
13. Lang LJ, Zhu Y, Li ZG, et al. Comparison of botulinum toxin with surgery for the treatment of acute acquired comitant esotropia and its clinical characteristics. Sci Rep. 2019;9(1):13869. doi:10.1038/s41598-019-50383-x
14. Erkan Turan K, Taylan Şekeroğlu H, Şener EC, Sanaç AŞ. Effect of visual acuity on the surgical outcomes of secondary sensory strabismus. Turk J Ophthalmol. 2015;45(6):254–258. doi:10.4274/tjo.67878
15. McNeer KW, Tucker MG. Comparison of botulinum toxin with surgery as primary treatment for infantile esotropia. J AAPOS. 2010;14(6):558. doi:10.1016/j.jaapos.2010.09.003
16. Wan MJ, Gilbert A, Kazlas M, et al. The effect of botulinum toxin augmentation on strabismus surgery for large-angle infantile esotropia. Am J Ophthalmol. 2018;189:160–165. doi:10.1016/j.ajo.2018.02.010
17. Xu H, Sun W, Dai S, et al. Botulinum toxin injection with conjunctival microincision for the treatment of acute acquired comitant esotropia and its effectiveness. J Ophthalmol. 2020;2020:e1702695. doi:10.1155/2020/1702695
18. Abbasoglu OE, Sener EC, Sanac AS. Factors influencing success and dose-effect relation of botulinum a treatment. Eye. 1996;10(3):385–391. doi:10.1038/eye.1996.78
19. Gursoy H, Basmak H, Sahin A, Yildirim N, Aydin Y, Colak E. Long-term follow-up of bilateral botulinum toxin injections versus bilateral recessions of the medial rectus muscles for treatment of infantile esotropia. J AAPOS. 2012;16(3):269–273. doi:10.1016/j.jaapos.2012.01.010
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.