")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 16
Biological Depiction of Lipodystrophy and Its Associated Challenges Among HIV AIDS Patients: Literature Review
Authors Lamesa TA
Received 21 November 2023
Accepted for publication 8 March 2024
Published 3 April 2024 Volume 2024:16 Pages 123—132
DOI https://doi.org/10.2147/HIV.S445605
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Tolera Ambisa Lamesa
School of Medical Laboratory Science, Jimma University, Jimma, Ethiopia
Correspondence: Tolera Ambisa Lamesa, Email [email protected]
Abstract: Lipodystrophy syndrome is a medical condition characterized by the absence of adipose tissue without any underlying starvation or macromolecule breakdown. In HIV AIDS patients, the use of highly active antiretroviral therapy (HAART) can lead to an acquired form of lipodystrophy, with a prevalence ranging from 10% to 83% among HIV AIDS patients. It was aimed to review the current understanding of biological depiction and challenges related to lipodystrophy in AIDS patients. Relevant articles published in the English language were searched in PubMed, Google Scholar, and Google. Keywords used for the search were: lipodystrophy, lipodystrophy and HIV, ART and lipodystrophy, HIV treatment, metabolic syndrome and HIV. Articles with full abstract information were read for those that met the objective criteria of the review, then full text of the articles was accessed and used. It was revealed by the literature that patients who developed lipodystrophy are characterized by insulin abnormality, obesity, diabetes mellitus, dyslipidemia, fatty liver disease, and ovarian dysfunction. Anthropometric measurements have been known to change significantly with lipodystrophy. HIV patients suffering from hepatitis C virus, hepatitis B virus, who take a protease inhibitor, are changing treatment or duration of treatment, and are women are the common risk factors for lipodystrophy. The metabolic syndrome seen in HIV patients associated with lipodystrophy can further be complicated to different adverse health effects and can result in increased morbidity and mortality rate if not treated. Existing studies have successfully identified several challenges faced by HIV AIDS patients due to lipodystrophy, including low self-esteem, compromised quality of life, and poor treatment adherence. However, it is crucial to acknowledge that there may be numerous other challenges that have yet to be discovered, emphasizing the need for further studies. It is recommended that managing dyslipidemia, treating diabetes mellitus, modifying lifestyle, and improving the anthropometric measurements have crucial roles to halt further complications associated with lipodystrophy.
Keywords: lipodystrophy, HIV, highly active antiretroviral therapy, dyslipidemia
Introduction
Lipodystrophy syndrome is a collection of disorders manifested as a lack of adipose tissue in the absence of starvation and breakdown of macromolecules. Severe forms of metabolic syndrome can be linked to these disorders because abnormal fat deposition prevents fat from being stored in the appropriate subcutaneous depots.1
Lipodystrophy was first described by Carr et al in 19982 among acquired immune deficiency syndrome (AIDS) patients who were taking highly active antiretroviral therapy (HAART) for a prolonged time. Those HIV-infected patients on HAART develop an acquired type of lipodystrophy syndrome (HALS); these types are characteristically similar to the one seen in obesity.3
A distressing morphologic change in body habitus is evidenced by the accumulation of central fat (lipohypertrophy) as well as an increase in waist to hip ratio, buffalo hump, enlarged breast, arm fat accumulation, and multiple lipomas. Lipodystrophy may also manifest as lipoatrophy of the face, abdomen, arms, legs, or buttocks that results in sunken cheeks, exaggerated muscles, bones, arteries and veins. It occurs most often in patients responding to HAART.2,4
Different studies report about 11% to 83% of HIV AIDS patients have developed lipodystrophy due to the HAART they use.4
The increased risk of lipodystrophy is common in patients who take NRTIs and protease inhibitors.5 The proposed pathogenesis of lipodystrophy for protease inhibitors and nucleoside reverse transcriptase inhibitors (NRTI) is through halting lipid metabolism and causing mitochondrial toxicity.6
Lipodystrophy patients experience increased distress as a result of the cosmetic effects as well as a perception that the obvious facial and extremity wasting represents a disease progression and disclosure of HIV status2 and it also negatively affects the self-esteem of people living with HIV (PLHI), this makes adherence to ART challenging and can result in a sedentary life style.7,8
Several factors may contribute to lipodystrophy, including sex difference, intravenous drug use, age, and the period of antiretroviral therapy usage. Duration of indinavir treatment may further contribute to lipodystrophy with central obesity.6 Female gender, co-infection with hepatitis C, HIV infection status before HAART initiation, NRTI, and protease inhibitors can be risk factors of the condition.9
Method
Relevant articles published in the English-language were searched for in PubMed, Google Scholar and Google. Keywords used for the search were: lipodystrophy, lipodystrophy and HIV, ART and lipodystrophy, HIV treatment, metabolic syndrome and HIV. Articles which contained full abstract information were read; when they met the objective criteria of the review, then the full text of the articles was accessed and used.
Forms of Lipodystrophy Syndromes
Lipodystrophy is a condition that is characterized by body shape abnormalities caused by changes in body fat distribution. It comprises three forms: lipoatrophy, lipohypertrophy and a mixed pattern of both conditions.10 Lipoatrophy is defined as the loss of subcutaneous fat, which is most noticeable on the face, buttocks, and extremities.11 Lipohypertrophy refers to the accumulation of fat in certain body regions, including the abdomen, back of the neck (buffalo hump), breasts, and multiple lipomas. See images in Leow et al.12
HIV AIDS patients who have lipodystrophy are characterized by abnormalities in their body composition, metabolic substance levels, anthropometric measurements, and endocrine metabolic levels.8,13,14 Patients who have developed HIV-associated lipodystrophy syndrome (HALS), may have complications like cardiovascular disease, dyslipidemia, neurological disorders, kidney and liver diseases, bone disorders, and diabetes mellitus type 2; health problems related to abnormality in fat redistribution and metabolic substance level disturbance.13,15,16
Epidemiology
There is no standardized criteria to diagnose lipodystrophy with AIDS disease; therefore, the epidemiological characteristics like prevalence, risk factors, incidence, responses and severity vary significantly from report to report. The prevalence of lipodystrophy varies from 10% to 80% in AIDS patients. The wide variation may also be due to differences in geographical location, age, genetic makeup, lifestyle standard, and methodological approaches.14
Different cross-sectional studies across the world reported the prevalence of lipodystrophy varies as 44%, 32.4%, 69.2%, 30%, and 16.3%2,9,17–19 respectively in all age groups of HIV infected patients (Table 1).
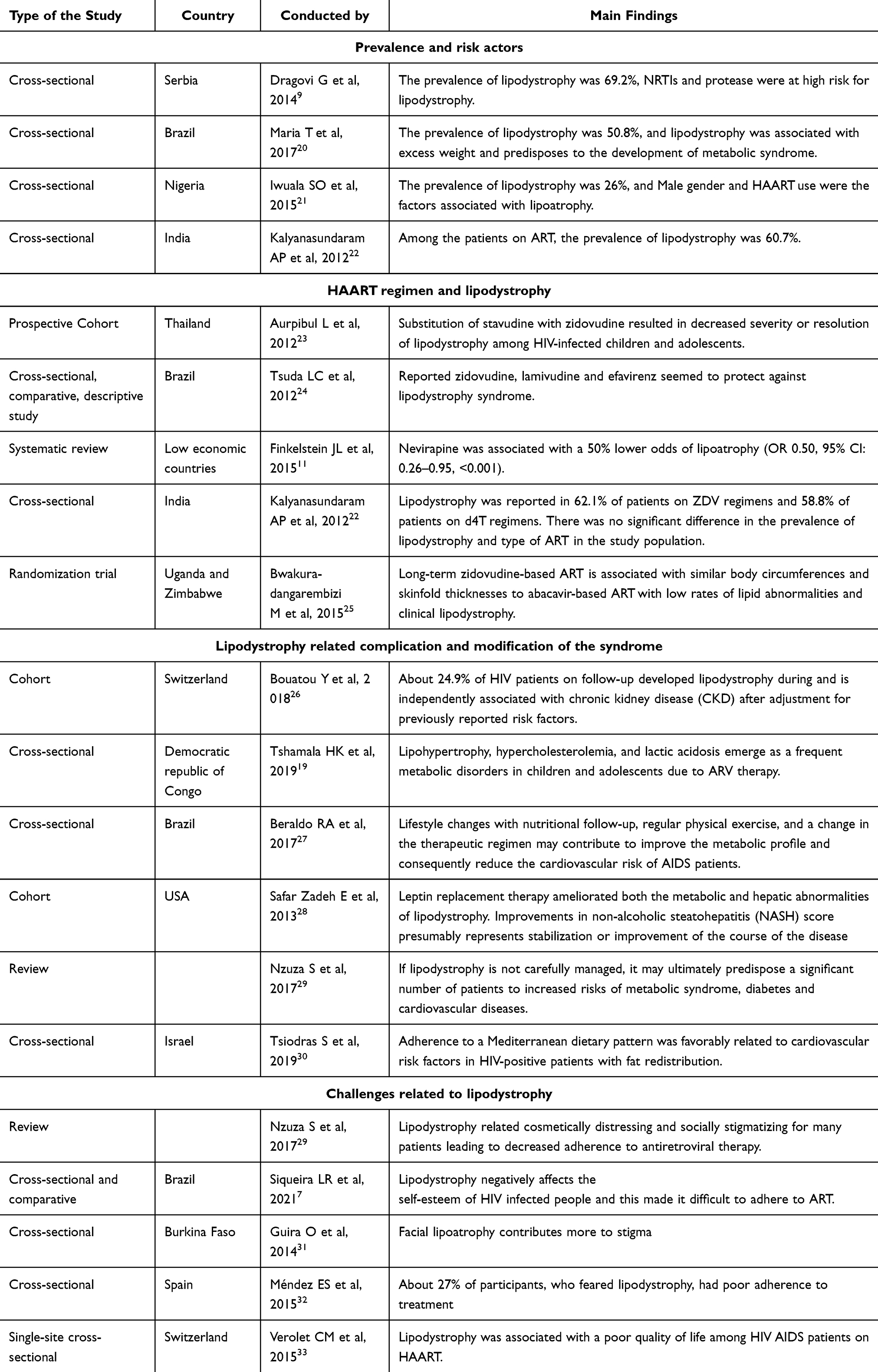 |
Table 1 Studies Finding Showing Biological Depictions and Challenges Related to Lipodystrophy in AIDS Patients |
Pathophysiology
If an antiretroviral is used to treat HIV AIDS, it contributes to lipodystrophy in AIDS patients and the mechanisms are not fully understood.34
HIV-associated lipodystrophy syndrome (HALS) is highly associated with the use of protease inhibitors (PI) and nucleoside reverse transcriptase inhibitors (NRTIs). The mechanisms are: via mitochondrial toxicity that may be caused by abnormally proliferated mitochondria, the structure and DNA makeup of mitochondria. Secondly, via adipocyte cell differentiation disturbance through down regulation of adipocyte forming transcription factors or genes like C/EBPΑ (a gene code for enhancer-binding protein alpha) and peroxisome proliferator-activated receptor gamma (PPARγ). Thirdly, via decreased secretion and release of adiponectin from adipose tissue. Moreover, HAART can increase macrophage recruitment, inhibit glucose delivery, impair insulin signal transmission, and generate reactive oxygen species, as well as enhance the formation of interleukin 6 (IL6) and tumor necrosis factor (TNF).34,35
The other proposed mechanisms are: impairment of adipocyte differentiation and drug-induced lipodystrophy also leads to an increase in lipolysis. Increased free fatty acid (FFAS) in blood, increased intracellular FFAS, increased ectopic FFAS deposition in different organs like visceral, pancreas skeletal muscle, and liver could be due to lipolysis that happens in subcutaneous tissue.34 These are the ways in which metabolic substance de-arrangement may happen.
Adipose tissue distribution may be directly affected by HIV-1 viral proteins. Researchers have shown that HIV-1 viral protein R inhibits gene transcription factor PPARγ, which can cause inhibition of adipocyte differentiation in vivo.34
Anthropometric Characteristics
Anthropometric parameters of HIV AIDS patients who were on HAART are reported by different works of literature. A report from Kenya in 2013 showed that increased abdominal girth was evident in 40.4% of the patients of whom 24% had isolated abdominal fat accumulation.2 Another study reported lipodystrophy in HIV AIDS patients was characterized by increased triceps, subscapular and supra-glacial skin folds, and mid-upper arm and leg circumferences in body appearance.18
According to research conducted in Thailand, substitution of stavudine (d4T) with zidovudine (ZDV) was associated with an increase in weight-for-age z score of children at the time of substitution from −0.91 (SD, 1.0) to −0.76 (SD, 1.1) at 96 weeks (P =0.02), whereas height-for-age z score did not change.23 However, treatment with efavirenz and nevirapine-containing regimens were not anthropometrically differently from the control group in that study.
Similarly, another report from Brazil on patients using antiretroviral therapy showed that 34% of overweight and 20% of obesity were observed.36 In another study, lipodystrophy was reported as 18.1% in HIV patients who were underweight compared to 5.5% in HIV-negative controls. In the same report, 3.5% of HIV AIDS patients had severe forms of malnutrition and it was statistically significant (P = 0.00). Another finding of the report was that being male or female resulted in different patterns of lipodystrophy, but prevalence in lipodystrophy and HAART regimen were not shown as significantly associated.22
Moreover, a study conducted at a pediatric HIV outpatient clinic in London, UK, showed about 27.5% patients had BMI ≥91st percentile, 10.0% ≥98th percentile (BMI), 2.5% had a waist circumference ≥90th percentile, 2.5% had a waist hip ratio ≥90th percentile, 22.5% had ≤10th percentile for hip circumference, 37.5% had ≤10th mid-upper arm circumference and 55.0% had at least one abnormal anthropometric measurement, excluding BMI.37
Conversely, other studies did not observe any differences in body habitus like waist/hip circumference ratio, hip circumference, BMI, and waist circumference between HIV infected and non-HIV infected patients on treatment.8
Risk Factors
Demographic, anthropometric, and behavioral factors associated with lipodystrophy were reported differently by different literature.3,6,11
According to a study conducted in Serbia, it was determined that 69.2% of the patients with lipodystrophy, along with HIV also had hepatitis C infection (HCV) and 7.9% were co-infected with hepatitis B virus (HBV).9 Additionally, several other studies demonstrated the association between HCV co-infection with HIV and lipodystrophy.9 In contrast, some other studies did not find a significant difference in the proportion of HCV infection between HIV and non-HIV infected groups.3
According to the Da Silva et al, report, women with HIV AIDS had a 1.87 relative hazard risk of having any kind of lipodystrophy when compared to men.6 In contrast, another study did not show the risk of having lipodystrophy among HIV AIDS patients on treatment and those who were new to treatment was any different according to their gender and age.38
Research conducted in Thailand consisting of 247 HIV-infected adults showed that facial atrophy and abnormally enlarged female breasts were observed in 50% and 42% of patients who were on PI respectively compared to non-PI ART. A study conducted in India has revealed that transitioning HIV patients from NNRTIs to PI upon treatment failure leads to a significant increase in T-cell count. This increase in T-cells has been found to be associated with a 10% annual development of lipodystrophy in these patients. Consistently, using PI treatment among Brazil AIDS patients, was associated with increased self-reported lipodystrophy.6
A similar finding from another study showed that stavudine had about 2.8 to 7.8 greater risk of being associated with lipodystrophy in HIV AIDS when compared to other anti-retroviral treatments.11 Additionally, treatment duration of six month by indinavir was also believed to contribute to the occurrence of a 1.26 greater rate of lipodystrophy with central obesity.6
Characterization of Lipodystrophy in Terms of Laboratory Parameters
As a result of lipodystrophy, metabolic abnormalities such as insulin resistance, steatosis, hypertriglyceridemia and diabetes mellitus often occur in conjunction with the severity of the comorbidities correlated with the level of adiposity.34
A study from Sergipe, Brazil in 2017 showed metabolic syndrome (MS) (mainly lipid and glucose abnormalities) was identified among 59.3% of patients diagnosed with lipodystrophy.20 Similarly, Beraldo et al reported the prevalence of hyperglycemia was 24.8% in HIV AIDS patients.27
A report from Barcelona, Spain showed that AIDS patients who had lipodystrophy, also had increased CD4+ lymphocyte, decreased viral load, and increased triglycerides and cholesterol levels compared with those without lipodystrophy. Furthermore, There was an increased risk of lipodystrophy in patients with a high triglyceride level who had started HAART.6
A cross-sectional study conducted in Melbourne, Australia involved one hundred HIV-positive patients; a multivariate analysis of low-density lipoprotein cholesterol (OR, 2.65; CI, 1.4–4.9) showed an increased risk and current tenofovir or abacavir use with reduced risk of lipodystrophy (OR, 0.096; CI, 0.011–0.83).39
Many other studies showed that lipid parameters abnormally change in HIV-infected individuals. For example, hypercholesterolemia in children on ARV therapy was seen in 7.5%, and 33.3% of two different studies15,19 respectively; hypertriglyceridemia in children on ARV therapy was seen in 16.2% and 7% of children on antiretroviral therapy-naive;19 hypertriglyceridemia and reduced HDL were in 55.7% and 25.9%15,27 of people living with HIV/AIDS respectively.
On the other hand, there were other studies that indicated there were no significant differences in blood lipid parameters, such as HDL-C, total cholesterol, LDL-C, triglyceride, and insulin levels, between individuals with AIDS and ART-related lipodystrophy and those without this condition.3,17
Complications
There is a severe form of the metabolic syndrome in lipodystrophic patients, which consists of dyslipidemia, insulin resistance, diabetes, and ovarian dysfunction.40
Patients with lipodystrophy have insufficient subcutaneous adipose tissue storage capacity, and severe insulin resistance (IR) is also observed, often manifested as acanthosis nigricans, type 2 diabetes mellitus (T2DM), hyperlipidemia, and nonalcoholic fatty liver disease (NAFLD).41
Heart problems were reported in 30.4% of patients with lipodystrophy by the international chart review study and patients with insulin resistance, diabetes, and dyslipidemia may be predisposed to atherosclerotic cardiovascular disease (ASCD).42 Similarly, according to a 7-year surveillance study including patients around the world, darunavir combined with ritonavir increased the risk of cardiovascular disease (CVD) by 1.59%.43
As demonstrated in the replacement therapy of leptin, the complication manifested as NASH was observed in 86% of HIV patients who had the genetical and acquired form of lipodystrophy, but the prevalence of the complication was reduced to 33% upon leptin replacement therapy on average over 25.8 ± 3.7 months (p = 0.0003).28
Current Treatment of Lipodystrophy
Effective treatment options are available to address the body appearance disturbances caused by lipodystrophy in HIV patients. These interventions not only help in resolving the physical changes but also play a crucial role in boosting the patients’ self-esteem and overall satisfaction with the treatment. Furthermore, the utilization of appropriate treatment methods can effectively prevent the occurrence of complications associated with lipodystrophy.35
Lifestyle Modification
Diet and Nutritional Modification Therapy
There is currently no universally accepted nutritional guideline for lipodystrophy syndrome. However, research has indicated that individuals with HIV-associated lipodystrophy syndrome (HALS) may find the Mediterranean diet beneficial. This dietary approach emphasizes the consumption of a variety of vegetables, dairy products, saturated fats, fruits, whole grain cereals, red meat, and fish.34
To attain normalized blood lipid levels, reduced central obesity, corrected body posture, and increased muscle strength, it is advisable to engage in a combination of physical exercise that focus on the cardiovascular system and muscular strengthening activities.35
Managing Underlying Diabetes Mellitus
Metformin
Metformin is a pharmaceutical drug employed in the management of type 2 diabetes mellitus; however, its efficacy does not extend to the treatment of lipodystrophy. A considerable number of individuals afflicted with lipodystrophy also experience diabetes mellitus, leading to the prescription of this medication as a preventive measure against the exacerbation of lipodystrophy, which can be intensified by the presence of diabetes mellitus.34
This medication has been found to have a positive impact on patients with insulin resistance, leading to a decrease in BMI, blood pressure, and blood lipid levels. Additionally, it can improve insulin action resistance in HIV patients with lipodystrophy.35,44
Other Medications for Diabetes Mellitus
Despite not being specifically intended for the treatment of lipodystrophy, rosiglitazone and pioglitazone (thiazolidinedione) are commonly prescribed to manage type 2 diabetes mellitus and mitigate the associated complications of lipodystrophy.34
Management of Dyslipidemia
Statins
Studies have indicated that the administration of pravastatin and rosuvastatin can lead to a reduction in both total and LDL cholesterol levels, while also potentially promoting an increase in subcutaneous adipose tissue in the extremities.34
In a combined analysis of two research studies, tesamorelin demonstrated a significant reduction of visceral adipose tissue (VAT) in individuals with abdominal obesity caused by HIV infection. The treatment resulted in a 15.4% decrease in VAT, while also leading to an increase in insulin-like growth factor one (IGF-1) levels within the normal physiological range. Furthermore, tesamorelin exhibited the ability to lower triglyceride levels and reduce the ratio of total cholesterol to HDL cholesterol in comparison to the placebo group.45
Fibrates, nicotinic acid, ezetimibe are also used for the treatment of blood lipid abnormalities in HALS.34
Leptin Replacement Therapy
Metreleptin, a synthetic form of leptin, is prescribed as a supplementary treatment alongside dietary modifications to address the complications arising from leptin deficiency in individuals diagnosed with congenital generalized lipodystrophy (CGL) and acquired generalized lipodystrophy (AGL). Diker-Cohen et al reported, in a cohort study, the effectiveness of metreleptin was found to be more pronounced in patients with higher baseline metabolic thresholds, including baseline HbA1c levels above 7.0% or 8.0%, triglycerides exceeding 300 or 500 mg/dL, and leptin levels below 4 ng/mL.46
Growth Hormone and Growth Hormone-Releasing Factor
Growth hormone (GH)-releasing factor (GHRF) has demonstrated its ability to reinstate the natural regulation of growth hormone (GH) secretion, upholds the regular negative influence of insulin-like growth factor-1 (IGF1) on GH release, and restricts the adverse effects associated with GH and lipohypertrophy in PLWH.45
Transplantation
Adipose tissue transplantation has been suggested as an alternative treatment for metabolic abnormalities in lipodystrophy. The process involves isolating and culturing pre-adipocytes, followed by repopulating and transplanting adipocytes. However, despite its intriguing concept, this approach has not been extensively studied, and therefore, the metabolic effects of adipose tissue transplantation in lipodystrophy remain largely unknown. In HIV patients with facial lipoatrophy, autologous fat transfer combined with dermal fillers has been tested primarily for aesthetic purposes, yielding promising results. Additionally, it is worth considering that there have been reported cases where hematopoietic stem cell transplantation, used to treat leukemia or neuroblastoma, led to abnormal distribution patterns of adipose tissue resembling APL later in life. This emerging form of lipodystrophy may offer valuable insights into the genetic and pathophysiological processes underlying lipodystrophy.41
Surgical Treatment
Patients who have a chief complaint related to cervicodorsal lipohypertrophy are evaluated for surgery. Excisional lipectomy is the recommended primary treatment due to the limitations of liposuction alone. Liposuction can be used for improved contouring and in subsequent procedures. Although there is a slightly increased risk of complications, adjunctive techniques like quilting sutures and drain placement may be utilized alongside excisional lipectomy.5
Conclusions
Both the HIV virus and the combined antiretroviral therapy used in HIV-infected patients can contribute to the occurrence of lipodystrophy. This metabolic syndrome presents in a severe form, with insulin resistance, ovarian dysfunction, diabetes, and dyslipidemia, being prominent features. These abnormalities can further be complicated to different adverse health states, and can result in increased morbidity and mortality rates if not treated. Different findings associate socio-economic, underlying disease state, treatment regimen, and change in regimen with different forms of lipodystrophy. Any form of lipodystrophy is characterized by different altered laboratory parameters like blood glucose, triglyceride, total cholesterol, LDL-C, CD4 lymphocyte, HDL-C count, viral load and altered anthropometric value. To date, the exact cause of lipodystrophy in HIV AIDS patients remains uncertain, despite numerous studies conducted on the subject. Therefore, it is imperative to conduct additional research that can provide a clear etiological identification and shed light on the precise cause. Existing studies have successfully identified several challenges faced by HIV AIDS patients due to lipodystrophy, including low self-esteem, compromised quality of life, and poor treatment adherence. However, it is crucial to acknowledge that there may be numerous other challenges that have yet to be discovered, emphasizing the need for further studies.
Recommendation
Even if it is helpful to treat HIV patients with cART, the effect of the drug and the virus itself have huge health impacts on the patients’ health status. Lipodystrophy that happened due to these drugs has disgusting features on the patients which affect both physiological and psychological appearance of the patients. Therefore it is recommended to halt further complications that are associated with this state through management of dyslipidemia, treating diabetes mellitus, life style modification to reduce risk factors and improve the anthropometric measurements.
Abbreviations
AC, abdominal circumference; AIDS, Acquired Immune Deficiency Syndrome; BMI, body mass index; CD4+, cluster of differentiation four, CI, confidence interval; GH, growth hormone; HAART, highly active antiretroviral treatment; HAZ, height for-age z-score; HCV, hepatitis C virus; HIV, human immune virus; MS, metabolic syndrome; NRTI, nucleoside reverse transcriptase inhibitors; OR, odds ratio; PLWH, people living with HIV; PPARγ, peroxisome proliferator activated receptor gamma; VAT, visceral adipose tissue.
Data Sharing Statement
All the literature used to prepare this manuscript can be available upon request.
Funding
No funding was used in this review.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Santini DAVF, Santini F. Diagnosis and treatment of lipodystrophy: a step - by - step approach. J Endocrinol Invest. 2019;42(1):61–73. doi:10.1007/s40618-018-0887-z
2. Awino McLigeyo A, Lule G, Otieno FCF, Joshua Kyateesa Kayima EO. Human immunodeficiency virus (HIV) associated lipodystrophy: the prevalence, severity and phenotypes in patients on highly active anti-retroviral therapy (HAART) in Kenya. J AIDS HIV Res. 2013;5(4):107–114.
3. López-dupla M, Maymó-masip E, Martínez E, Domingo P. HIV-1 / HAART-Related Lipodystrophy Syndrome (HALS) is associated with decreased circulating sTWEAK levels. PLoS One. 2015;10(12):1–13. doi:10.1371/journal.pone.0144789
4. Gomes L, Lana C, Rezende D, Junqueira G, Perini E, Pádua De CM. Lipodystrophy among patients with HIV infection on antiretroviral therapy: a systematic review protocol. BMJ Open. 2014;4:10–13.
5. Barton N, Moore R, Prasad K, Evans G. Excisional lipectomy versus liposuction in HIV-associated lipodystrophy. Arch Plast Surg. 2021;48(6):685–690.
6. Martinez E, Mocroft A, García-viejo MA, et al. Risk of lipodystrophy in HIV-1-infected patients treated with protease inhibitors: a prospective cohort study. Lancet. 2001;357(February 24):592–598. doi:10.1016/S0140-6736(00)04056-3
7. Siqueira LR, Holanda G, Teresinha M, et al. Effect of lipodystrophy on self-esteem and adherence to antiretroviral therapy in people living with HIV. AIDS Care. 2021;1(1):1–10. doi:10.1080/09540121.2021.1936442
8. Grenha I, Oliveira J, Lau E, et al. HIV-Infected Patients With and Without Lipodystrophy Under Combined Antiretroviral Therapy: evaluation of Body Composition. J Clin Densitom. 2018;21(1):75–82. doi:10.1016/j.jocd.2016.07.010
9. Dragovi G, Danilovi D, Dimi A, Jevtovi D. Lipodystrophy induced by combination antiretroviral therapy in HIV / AIDS patients: a Belgrade cohort study. Vojn Pregl. 2014;71(8):746–750. doi:10.2298/VSP121016022D
10. Bouatou Y, Gayet Ageron A, Bernasconi E, et al. Lipodystrophy Increases the Risk of CKD Development in HIV-Positive Patients in Switzerland: the LIPOKID Study. Kidney Int Reports. 2018;3(5):1089–1099. doi:10.1016/j.ekir.2018.04.014
11. Finkelstein JL, Gala P, Rochford R, Glesby MJ, Mehta S. HIV/AIDS and lipodystrophy: implications for clinical management in resource-limited settings. J Int AIDS Soc. 2015;18(1):1–13. doi:10.7448/IAS.18.1.19033
12. Leow MK, Addy CL and Mantzoros CS. (2003). Human immunodeficiency Virus/Highly active antiretroviral therapy-associated metabolic syndrome: clinical presentation, pathophysiology, and therapeutic strategies. J Clin Endocr Metab, 88(5), 1961–1976. 10.1210/jc.2002-021704
13. Sacilotto LB, Papini SJ, Mendes AL, et al. Relationship Between Lipodystrophy, Body Composition, Metabolic Profile, and Serum Levels of Adipocytokines. Front Nutr. 2021;8(December). doi:10.3389/fnut.2021.750721
14. Marcelle D, Sprinz E. HIV-associated lipodystrophy: a review from a Brazilian perspective. Ther Clin Risk Manag. 2014;10:559–566. doi:10.2147/TCRM.S35075
15. Bhutia E, Hemal A, Yadav TP, Ramesh KL. Lipodystrophy syndrome among HIV infected children on highly active antiretroviral therapy in northern India. Afr Health Sci. 2014;14(2):408–413. doi:10.4314/ahs.v14i2.17
16. Araújo-Vilar FS. Diagnosis and treatment of lipodystrophy: a step - by - step approach. J Endocrinol Invest. 2019;42(1):61–73. doi:10.1007/s40618-018-0887-z
17. Della JLB, Luiz MC, Maurici R, Schuelter-Trevisol F. Prevalence and factors associated with lipodystrophy in AIDS patients. Rev Soc Bras Med Trop. 2014;47(1):30–37. doi:10.1590/0037-8682-0240-2013
18. Kinabo GD, Sprengers M, Msuya LJ. Prevalence of Lipodystrophy in HIV-infected Children in Tanzania on Highly Active Antiretroviral Therapy. Pediatr Infect Dis J. 2013;32(1):39–44. doi:10.1097/INF.0b013e3182755a34
19. Tshamala HK, Aketi L, Tshibassu PM, et al. The Lipodystrophy Syndrome in HIV-Infected Children under Antiretroviral Therapy: a First Report from the Central Africa. Int J Pediatr. 2019;2019.
20. Palmeira Dos Santos TM, Barros Da Silva D, Monteiro Franco T, et al. Lipodystrophy and the relationship with cardiovascular risk factors and metabolic syndrome in HIV-infected patients. Nutr Clin y Diet Hosp. 2017;37(2):12–20.
21. Iwuala SO, Lesi OA, Fasanmade OA, Sabir AA, Olamoyegun MA, Okany CC. Prevalence of and Risk Factors for Lipoatrophy in Patients with HIV Infection in Nigeria. AIDS Res Treat. 2015;1–8.
22. Kalyanasundaram AP, Jacob SM, Hemalatha R, Sivakumar MR. Prevalence of lipodystrophy and dyslipidemia among patients with HIV infection on generic ART in rural South India. J Int Assoc Physicians AIDS Care. 2012;11(5):329–334. doi:10.1177/1545109711401750
23. Aurpibul L, Puthanakit T, Taejaroenkul S, Sirisanthana T, Sirisanthana V. Recovery From Lipodystrophy in HIV – infected Children After Substitution of Stavudine With Zidovudine in a Non-nucleoside Reverse Transcriptase Inhibitor – based. Pediatr Infect Dis J. 2012;31(4):384–388. doi:10.1097/INF.0b013e31823f0e11
24. Tsuda LC, Silva MM, Machado AA, Fernandes APM. Body changes: antiretroviral therapy and lipodystrophy syndrome in people living with HIV/AIDS. Rev Lat Am Enfermagem. 2012;20(5):847–853. doi:10.5999/aps.2020.02285
25. Bwakura-dangarembizi M, Musiime V, Szubert AJ, et al. Prevalence of Lipodystrophy and Metabolic Abnormalities in HIV-infected African Children after 3 Years on First-line Antiretroviral Therapy. Int J Med. 2015;34(2):23–31.
26. Bouatou Y, Ageron AG, Bernasconi E, et al. Development in HIV-Positive Patients in Switzerland: the LIPOKID Study. Kidney Int Reports. 2018;3(5):1089–1099. doi:10.1016/j.ekir.2018.04.014
27. Beraldo RA, Dos Santos AP, Guimarães MP, et al. Body fat redistribution and changes in lipid and glucose metabolism in people living with HIV/AIDS. Rev Bras Epidemiol. 2017;20(3):526–536. doi:10.1590/1980-5497201700030014
28. Safar Zadeh E, Lungu AO, Cochran EK, et al. The liver diseases of lipodystrophy: the long-term effect of leptin treatment. J Hepatol. 2013;59(1):131–137. doi:10.1016/j.jhep.2013.02.007
29. Nzuza S, Zondi S, Hurchund R. Highly Active Antiretroviral Therapy-Associated Metabolic Syndrome and Lipodystrophy. Pathophysiology and Current Therapeutic Interventions. 2017;7(4):103–116.
30. Tsiodras S, Poulia K, Yannakoulia M, et al. Adherence to Mediterranean diet is favorably associated with metabolic parameters in HIV-positive patients with the highly active antiretroviral therapy – induced metabolic syndrome and lipodystrophy. Metabolism. 2009;58(6):854–859. doi:10.1016/j.metabol.2009.02.012
31. Guira O, Tiéno H, Yaméogo B, et al. Characteristics and factors associated with the clinical forms of lipoatrophy during highly active antiretroviral therapy in Ouagadougou, Burkina Faso. J Int Assoc Provid AIDS Care. 2014;13(2):184–187. doi:10.1177/2325957413503369
32. Méndez ES, Prado AA, José M, Ruiz F. Correlates of perception of HIV-related lipodystrophy: the importance of fears and concerns. Revistamultidiscipliardelsida. 2015;1(4):20–29.
33. Verolet CM, Delhumeau-Cartier C, Sartori M, et al. Lipodystrophy among HIV-infected patients: a cross-sectional study on impact on quality of life and mental health disorders. AIDS Res Ther. 2015;12(1):1–10. doi:10.1186/s12981-015-0061-z
34. Fiorenza CG, Chou SH, Mantzoros CS. Lipodystrophy: pathophysiology and advances in treatment. Nat Rev Endocrinol. 2011;7(3):137–150. doi:10.1038/nrendo.2010.199
35. Nilmaria Guzman VV. HIV-Associated Lipodystrophy. Treasure Island(FL): Stat Pearls; 2022:1–8.
36. Da Silva TAL, Barboza RR, De Andrade RD, et al. Relationship between dietary intake and use of protease inhibitors with anthropometric and biochemical parameters of lipodystrophy in people living with HIV. Nutr Hosp. 2014;30(4):935–940. doi:10.3305/nh.2014.30.4.7638
37. Sacre HP, Chalmers R, Tudor-Williams G, Klassen K, Foster C, Walters RMP. Clinic-based anthropometric measurements of lipodystrophy and associations with antiretroviral therapy in HIV-infected adolescents. HIV Med. 2012;13:78.
38. Iwuala SO, Lesi OA, Fasanmade OA, Sabir AA, Olamoyegun MA, Okany CC. Prevalence of and risk factors for lipoatrophy in patients with HIV infection in Nigeria. AIDS Res Treat. 2015;2015:1–7. doi:10.1155/2015/402638
39. Price J, Hoy J, Ridley E, Nyulasi I, Paul E, Woolley I. Changes in the prevalence of lipodystrophy, metabolic syndrome and cardiovascular disease risk in HIV-infected men. Sex Health. 2015;12(3):240–248. doi:10.1071/SH14084
40. Meehan CA, Cochran E, Kassai A, Brown RJ, Gorden P. Metreleptin for injection to treat the complications of leptin deficiency in patients with congenital or acquired generalized lipodystrophy. Expert Rev Clin Pharmacol. 2016;9(1):59–68. doi:10.1586/17512433.2016.1096772
41. Polyzos SA, Perakakis N, Mantzoros CS. Fatty liver in lipodystrophy: a review with a focus on therapeutic perspectives of adiponectin and/or leptin replacement. Metabolism. 2019;96:66–82. doi:10.1016/j.metabol.2019.05.001
42. Akini G, Merve Celik BA. Complications of lipodystrophy syndromes. Presse Med. 2021;50(3):1–7.
43. Bruder-Nascimento T, Kress TC, Kennard S, De CEJB. HIV Protease Inhibitor Ritonavir Impairs Endothelial Function Via Reduction in Adipose Mass and Endothelial Leptin Receptor-Dependent Increases in NADPH Oxidase 1 (Nox1), C-C Chemokine Receptor Type 5 (CCR5), and Inflammation Thiago. J Am Hear Assoc. 2020;9:1–25.
44. Alves MD, Brites C, Sprinz E. HIV -associated lipodystrophy: a review from a Brazilian perspective. Ther Clin Risk Manag. 2014;10(1):559–566.
45. Koethe JR, Lagathu C, Lake JE, et al. HIV and antiretroviral therapy-related fat alterations. Nat Rev Dis Primers. 2020;6(1). doi:10.1038/s41572-020-0181-1
46. Diker-Cohen T, Cochran E, Gorden P, Brown RJ. Partial and generalized lipodystrophy: comparison of baseline characteristics and response to metreleptin. J Clin Endocrinol Metab. 2015;100(5):1802–1810. doi:10.1210/jc.2014-4491
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.