")
Back to Journals » Clinical Ophthalmology » Volume 15
Bilateral Implantation of a New Refractive Multi-Segmented Multifocal Intraocular Lens in Cataract or Refractive Lens Exchange Patients
Authors Holzer MP, Nuijts RMMA, Jonker SMR, Mertens ELJG , Sener AB, Cazal JAO, Salvador Playa A, Mesa RR , Thomas BC
Received 28 May 2020
Accepted for publication 3 May 2021
Published 21 May 2021 Volume 2021:15 Pages 2117—2126
DOI https://doi.org/10.2147/OPTH.S261586
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Mike P Holzer,1 Rudy MMA Nuijts,2 Soraya MR Jonker,2 Erik LJG Mertens,3 Asim Bozkurt Sener,4 Jorge AO Cazal,5 Antoni Salvador Playa,5 Ramon Ruiz Mesa,6 Bettina C Thomas1
1Universitäts-Augenklinik Heidelberg, Heidelberg, Germany; 2Academisch Ziekenhuis Maastricht, Maastricht, the Netherlands; 3Medipolis, Antwerp, Belgium; 4Acibadem Maslak Hospital, Istanbul, Turkey; 5Hospital Universitari Mútua Terrassa, Barcelona, Spain; 6Oftalvist CIO Jerez, Cádiz, Spain
Correspondence: Mike P Holzer
Augenzentrum Prof. Dr. Holzer & Prof. Dr. Rabsilber, Bahnhofstrasse 18, Weinheim, 69469, Germany
Tel + 49 0 6201 87 87 24
Email [email protected]
Purpose: To evaluate the safety and efficacy of a new multi-segmented refractive multifocal intraocular lens (IOL) after phacoemulsification and refractive lens exchange (RLE).
Patients and Methods: In this prospective, multicenter clinical trial, 63 presbyopic subjects who had cataract or where RLE candidates were bilaterally implanted with the Precizon Presbyopia IOL (Ophtec BV, Groningen, the Netherlands) after phacoemulsification. The study was conducted at 6 clinical centers in Germany, the Netherlands, Belgium, Turkey and Spain. Subjects were evaluated at baseline and at 1 day, 1 week, 1 and 3 months postoperatively for monocular and binocular uncorrected (UDVA) and corrected distance visual acuity (CDVA), uncorrected (UIVA) and distance-corrected intermediate visual acuity (DCIVA), uncorrected (UNVA), corrected (CNVA) and distance-corrected near visual acuity (DCNVA), contrast sensitivity and quality of vision.
Results: Three months postoperatively, binocular UDVA and CDVA of ≥ 20/40 was achieved in 98.4% (60/61) and 100%, respectively. Binocular UIVA and DCIVA of ≥ 20/40 was achieved in 96.7% (59/61) and 93.4% (57/61) respectively. Binocular UNVA, CNVA and DCNVA of ≥ 20/40 was achieved in 93.4% (57/61), 98.4% (60/61) and 95% (57/60) subjects, respectively. Complete spectacle independence was achieved in 80% (49/61) patients; 93% of patients reported that they were quite or very satisfied with the outcomes of the procedure.
Conclusion: Precizon Presbyopia IOL implantation is a safe and effective method to provide good visual acuity at all distances in presbyopic and cataract patients.
Keywords: presbyopia-correcting IOL, refractive lens exchange, cataract surgery, multifocal IOL
Introduction
The development of multifocal intraocular lenses (MIOL) has been an important breakthrough in the intraocular lens (IOL) technology. The goal is to restore visual function at all distances after cataract surgery. The use of MIOLs has helped improve the quality of life by reducing or eliminating the need for spectacles.1 Due to high rates of patient satisfaction and spectacle independence achieved with MIOL implantation after cataract surgery,1 its use with refractive lens exchange (RLE) is becoming increasingly popular among refractive surgeons for the treatment of presbyopic patients seeking refractive surgery.
MIOLs have been developed using different optical design approaches; of which diffractive and refractive are most common. The optics of both types have concentric circular or annular regions and contain powers suitable for distance, intermediate and/or near correction.2 Diffractive IOLs are based on Huygens–Fresnel principle,2 and have diffractive steps on the IOL that distribute incoming light rays into two or more focal points. By adjusting the width of the rings and the height of steps, multifocality is attained. Refractive IOLs are designed with multiple refractive optical zones, providing various focal points, enabling the patients to see distant, intermediate and near targets.
Diffractive multifocal IOLs are associated with an 18% to 20% loss of light transmission to higher diffraction orders, causing a reduction in contrast sensitivity.3 On the other hand, refractive MIOLs potentially use 100% of incident light onto the retina,3 thereby having the potential of providing good contrast sensitivity. Recent MIOLs provide excellent visual acuity, but a high incidence of photic phenomena after MIOL implantation can result in patient dissatisfaction even after uneventful cataract surgery.4
IOL decentration is one of the causes associated with photic phenomena reported in previous studies.5 Further, the photic phenomena have been reported to be associated with angle kappa.5 A large angle kappa could contribute to functional decentration if the MIOL is centered on one axis, (pupillary or visual axis) and is not aligned with the other, resulting in glare and decreased visual acuity. It has been documented that decentrations of around 0.75–1.0 mm cause deterioration in optical properties of both refractive and diffractive MIOLs.6,7 As such, large angle kappa combined with IOL decentration can have a cumulative negative impact on vision. Therefore, there is a need to develop such IOL designs that are decentration tolerant.
To overcome such limitations of refractive MIOLs, a multi-segmented IOL that is pupil size independent and decentration tolerant has been developed (Precizon Presbyopia, Ophtec BV, Groningen, the Netherlands). The IOL has 11 segments, 5 for far vision and 6 for near vision, distributed sequentially, such that the ratio between near and far correction remains intact with changing pupil size or when the IOL is decentered to a certain degree. The current study is a clinical trial that examines the outcomes of bilateral implantation of this IOL in cataract and RLE patients.
Methods
Study Design and Subjects
This prospective, open-label, single-arm, multicenter clinical trial (clinicaltrials.gov Identifier: NCT02409771) was conducted at six investigation sites (one each in Germany, Turkey, Belgium and Spain and two in the Netherlands). All procedures were conducted according to the tenets of the Declaration of Helsinki and approval from medical ethics committee and competent authority was obtained for all sites (UZA Antwerpen, Belgium; Ethikkommission Medizinische Fakultät Heidelberg, Germany; METC azM/UM, Netherlands, CEIC Hospital Universitari Mútua de Terrassa, Spain; Comité de Ética de la investigación de Cádiz; Netherlands; Acibadem Universitesi Klinik Arastirmalar Etik Kurulu’num, Turkey). Written informed consent was obtained from all patients. The main objective of the study was to evaluate the ability of the Precizon Presbyopia IOL to provide near, intermediate and distance vision in presbyopic patients. The secondary objectives were to evaluate contrast sensitivity, defocus curve, spectacle independence, quality of vision, patient satisfaction, stability of manifest refraction spherical equivalent (MRSE) and rates of complications.
Seventy presbyopic subjects who had cataract or were RLE candidates and who wished to be spectacle independent for near and far distances were enrolled in this study and were bilaterally implanted with the Precizon Presbyopia IOL. Other inclusion criteria were: age ≥45 years; lifestyle fit with multifocal IOL implantation; qualified for bilateral implantation; had calculated IOL power within the available diopter range of +10.0 to +30.0 D; expected distance corrected visual acuity (CDVA) of 0.5 Snellen decimal or better after IOL implantation; predicted keratometric postoperative astigmatism (calculated with respect to the surgical-induced astigmatism) <1.0 D; no secondary surgical procedure planned during the course of the study; and availability, willingness and sufficient cognitive awareness and physical ability to comply with examination procedures throughout the duration of the study. Subjects who had ocular disease other than cataract that may predispose for future complications or might confound the outcome of the investigation (eg, anterior segment pathology, glaucoma, corneal dystrophy, ocular inflammation, pseudoexfoliation syndrome, retinal disorders); acute or chronic disease or illness or use of medication that could confound the outcome of the study or increase the risk to the subject; endothelial cell count <1500 cells/mm;2 amblyopia; congenital eye abnormalities; previous ocular surgery that might confound the outcome of the investigation or increase risk to patient; concurrent participation or participation during the last 30 days in any other clinical trial; pregnancy or another condition with associated fluctuation of hormones that could lead to refractive changes were excluded from the study.
Of the 70 subjects, seven patients were excluded from the data analysis due to violation of these criteria. The mean age of the remaining subjects (n=63) in the study was 64.1 ± 8.2 years (range 48 to 82 years; 38 females and 25 males). Most subjects (93.7%) were of the Caucasian race and 6.3% were Hispanic. Forty-nine out of 63 (77.8%) subjects were cataract patients; the remaining 14 patients (22.2%) were RLE candidates. Of these 63 subjects, one patient discontinued after 1-week due to COPD exacerbation and one patient discontinued after 1 month due to a stroke.
Intraocular Lens
The Precizon Presbyopia IOL is made of Hydrophilic Acrylic Benz 25% and can be implanted in the capsular bag to replace the crystalline lens. It has an optic diameter of 6.0 mm with an overall size of 12.50 mm and an open C-loop haptic design for stability. The lens has a +2.75 D power add for improved intermediate and near vision. The optic consists of 11 segments, five for distance vision and 6 for near vision (Figure 1). The segments are distributed in such a way, that pupil size or slight decentration has a minimal effect on the ratio between near and far light distribution.
 |
Figure 1 Schematic diagram of Precizon Presbyopia IOL consisting of 11 optic segments, five for distance vision (red color) and 6 for near vision (blue color). N= near; F= far. |
Pre-Surgical and Surgical Technique
The Sanders–Retzlaff–Kraff (SRK/T) theoretical prediction formula8 was used for the biometrical calculation for eyes with an axial length (AXL) ≥22.0 mm and Hoffer Q was used for eyes with AXL <22.0 mm.
All surgeries were performed using standard phacoemulsification technique with a 2.2–2.4 mm main incision, using the Ophtec DualTec kit for one-piece hydrophilic acrylic IOLs for IOL loading and insertion. Surgery in the second eye was performed within 21 days from surgery in the first eye.
Patient Evaluation
Subjects were evaluated at baseline and postoperative 1 day, 1 week, 1 month and 3 months. A full ophthalmic examination was performed in all subjects and included manifest refraction, measurement of monocular and binocular uncorrected distance visual acuity (UDVA) and CDVA, uncorrected (UIVA) and distance-corrected intermediate visual acuity (DCIVA), uncorrected (UNVA), corrected (CNVA) and distance-corrected near visual acuity (DCNVA), fundus examination, intraocular pressure, slit-lamp examination, specular microscopy, corneal topography, pupillometry and contrast sensitivity with and without glare under photopic (85 cd/m2) and mesopic (3 cd/m2) conditions measured at 4 spatial frequencies (3, 6, 12 and 18 cycles per degree (c/d)), each with 8 levels of contrast. Visual acuities were recorded using the Early Treatment of Diabetic Retinopathy Study (ETDRS) charts for distance vision at 4 m, near vision at 40 cm, and intermediate vision at 80 cm. Preoperative near visual acuity measurements were performed only for RLE patients, as the measurement for the cataract subjects would have been biased. A binocular defocus evaluation was obtained by using the best corrected distance refraction and then adding lenses over the range of +1.5 to −5.0 D in 0.5 D steps.
A quality of vision (QoV) questionnaire9 was used at 3 months postoperatively. The QoV is a validated, Rasch-adjusted questionnaire in which patients are asked to rate 10 photic phenomena items illustrated by standard photographs, scoring each item (0, 1, 2, 3) in relation to how frequent, severe, and bothersome their symptoms are (30 items in total). Patient satisfaction was measured using a questionnaire with 10 items. Patients were asked to grade their level of satisfaction as: not at all, a little, quiet and very satisfied. Spectacle independence was evaluated by asking patients about the need of spectacles as never, occasionally, quite often and very often.
Statistical Analysis
The sample size calculations were performed for the UNVA using the following formula:

where α, the probability of type I error (significance level) is the probability of rejecting the true null hypothesis; β, the probability of type II error (1 – power of the test) is the probability of failing to reject the false null hypothesis; μ – μ0, the value of allowable difference, is the difference value between true mean and reference mean (constant value).
Statistical analyses were performed using Minitab (Minitab, Inc, Pennsylvania USA). Descriptive statistics was used to report demographic variables and the ocular status at baseline. The significance level adopted was 5% (p < 0.05). Quantitative variables were analyzed using a one-sample t-test (for paired differences) for normally distributed variables or a Wilcoxon signed-rank test for skewed distributed variables. For qualitative parameters (categorical or ordered), frequency counts and percentages of each category were calculated.
Results
Table 1 demonstrates the pre-operative parameters.
 |
Table 1 Preoperative Parameters of 126 Eyes of 63 Patients Implanted with Precizon Presbyopia IOL |
Visual Outcomes
Distance Visual Acuity
Table 2 demonstrates the monocular and binocular postoperative mean distance visual acuity. Three months postoperatively, 98.4% (60/61) had a binocular UDVA of 0.3 logMAR or better (≥20/40); 45.9% (28/61) had a binocular UDVA of 0.0 logMAR or better (≥20/20). In RLE patients, postoperative mean UDVA was 0.00 ± 0.08 logMAR (equivalent to 20/20), which was statistically significantly different from preoperative UDVA (0.18 ± 0.29 logMAR equivalent to 20/30; p=0.02) and preoperative CDVA (−0.10 ± 0.12 logMAR equivalent to 20/16, p=0.001).
 |
Table 2 Visual Outcomes (logMAR) of Patients Implanted with Precizon Presbyopia IOL |
Three months postoperatively, all patients had a binocular CDVA of 0.3 logMAR or better (≥20/40). While the CDVA of 0.0 logMAR (≥20/20) or better was achieved in 60.7% of patients; more than 95% had a CDVA of ≤0.1 logMAR postoperatively. For the RLE patients, binocular CDVA changed from −0.10 ± 0.12 (equivalent to 20/16) preoperatively to −0.06 ± 0.08 logMAR (equivalent to 20/17.4) at postoperative 3 months. Although the difference was statistically significant (p=0.04), it was not clinically relevant.
Intermediate Visual Acuity
Table 2 demonstrates the monocular and binocular postoperative mean intermediate visual acuity. Three months postoperatively, 96.7% (59/61) had a binocular UIVA of 0.3 logMAR or better (≥20/40); 39.3% (24/61) had a binocular UIVA of 0.0 logMAR or better (≥20/20).
Three months postoperatively, 93.4% (57/61) had a binocular DCIVA of 0.3 logMAR or better (≥20/40); 27.9% (17/61) had a binocular DCIVA of 0.0 logMAR or better (≥20/20). Four patients had a binocular DCIVA worse than 0.3 logMAR (20/40). One patient had traces of posterior capsular opacification, the reason for low VA was not found in second patient. While the third and fourth patients had DCIVA of >0.3 logMAR (20/40); defocus curve showed VA of 0.02 logMAR (20/21) and 0.16 logMAR (20/29) respectively at a defocus of −1.5D (66cm) and both these patients were very satisfied with their intermediate vision.
Near Visual Acuity
The preoperative and postoperative 1 and 3 months visual outcomes are presented in Table 2. Three months postoperatively, 93.4% (57/61) patients had a binocular UNVA of 0.3 logMAR or better (≥20/40); 6.8% (4/61) had a binocular UNVA worse than 0.3 logMAR (20/40). The comparison between pre- and postoperative UNVA values was performed for RLE patients only (n=14). In RLE patients, the mean binocular UNVA improved from 0.56 ± 0.19 logMAR (equivalent to 20/73) preoperatively to 0.12 ± 0.13 logMAR (equivalent to 20/26) postoperatively (p<0.01).
Three months postoperatively, 98.4% (60/61) had a binocular CNVA of 0.3 logMAR or better (≥20/40); 32.8% (20/61) had a binocular CNVA of 0.0 logMAR or better (≥20/20). Similarly, at 3 months, 95% (57/60) had a binocular DCNVA of 0.3 logMAR or better (≥20/40); 11.7% (7/60) had a binocular DCNVA of 0.0 logMAR or better (≥20/20).
Refractive Outcomes and Spectacle Independence
Figure 2 shows the stability of MRSE over time. The mean change in MRSE was statistically significantly different between pre-op and Day 1 (p=0.04), Day 1 and Week 1 (p=0.04) and Month 1 and Month 3 (p<0.01). A scatter plot of attempted versus achieved MRSE is shown in Figure 3. Spectacle independence was evaluated at 3 months postoperatively by means of a patient-administered questionnaire. While 98.4% (60/61) patients reported that they never or only occasionally used spectacles, 1.6% (n=1) reported using spectacles quite often (Figure 4).
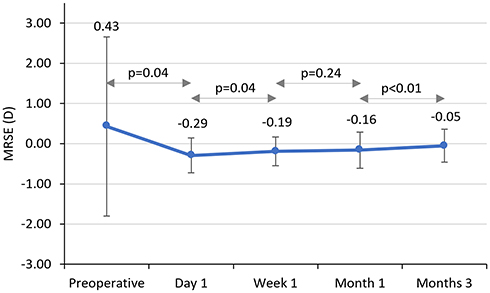 |
Figure 2 Stability of manifest refraction spherical equivalent (MRSE) after Precizon Presbyopia IOL implantation in cataract and refractive lens exchange subjects up to 3 months postoperatively. |
 |
Figure 3 Scatterplot representing attempted versus achieved manifest refraction spherical equivalent (MRSE) at postoperative 3 months following Precizon Presbyopia IOL implantation. |
 |
Figure 4 Overall spectacle independence following Precizon Presbyopia IOL implantation in cataract and refractive lens exchange subjects at postoperative 3 months by means of a questionnaire (how often do you wear spectacles?). |
Photopic and Mesopic Contrast Sensitivity
Contrast sensitivity was tested in a subgroup of 23 patients at three sites. Figure 5 shows the combined post-operative contrast sensitivity scores for the cataract and RLE patients. As can be expected with MIOLs, the post-op mesopic contrast sensitivity scores were lower than the photopic contrast sensitivity scores. The postoperative contrast sensitivity reduced further when measured with glare function activated.
 |
Figure 5 Postoperative contrast sensitivity for 23 cataract and refractive lens exchange (RLE) patients following Precizon Presbyopia IOL implantation. |
Pre-operative and post-operative contrast sensitivity scores were compared for RLE patients (n=7) (Figure 6A and B). In RLE patients (n=7), contrast sensitivity reduced statistically significantly at postoperative 3 months at all spatial frequencies and for all illumination settings except for the photopic and photopic + glare test at a spatial frequency of 3 c/d (Figure 6A and B).
 |
Figure 6 Preoperative (A) and postoperative (B) contrast sensitivity for 7 refractive lens exchange (RLE) patients following Precizon Presbyopia IOL implantation. |
Defocus Curve
Figure 7 shows the best corrected binocular defocus curve measured 3 months postoperatively. The defocus curve shows a peak at zero D, corresponding to the far focus point. For the intermediate range (ie, −1.5 D, corresponding with 66 cm), VA was 0.11 logMAR whereas optimal near VA was measured at −2.0 D of defocus, corresponding with a distance of 50 cm, and showed a VA of 0.06 logMAR. VA is ≤0.1 logMAR or better over a broad range of defocus, ranging from approximately +0.5 to −2.5 D.
 |
Figure 7 Mean defocus curve at postoperative 3 months after Precizon Presbyopia IOL implantation. |
Patient Satisfaction
Patient satisfaction outcomes are represented in Figure 8A and B. Overall, 93.4% of patients reported that they were “quite” or “very satisfied” with the outcome of the procedure. While 88.5% of patients reported that they were “quite” or “very satisfied” with their overall uncorrected vision, the proportions for satisfaction with distance, intermediate and near vision were 82%, 87% and 92%, respectively. As such, 88.5% patients were “a quite” or “very satisfied” with their choice of the IOL (Figure 8A).
 |
Figure 8 Patient satisfaction outcomes following Precizon Presbyopia IOL implantation – Percentage of patients reporting different levels of satisfaction in response to a directed questionnaire on different aspects of vision, procedure and IOL (A) answers to questions with options, “not at all”, “a little”, “quiet” and “very” (B) answers to questions with options, “No”, “may be”, “quite surely” and “definitely”. |
When asked if they achieved the quality of vision that they expected, 83.6% of patients responded, “quite surely” or “definitely”. Accordingly, ~89% patients reported that they would “quite surely” or “definitely” undergo the same procedure again and 87% would recommend this lens to other people (Figure 8B).
Quality of Vision
Nearly 70 to 90% of the patients either never or occasionally observed photic phenomena like glare, halos and starbursts (Figure 9A). In addition, 77 to 87% of the patients considered these photic phenomena as “not at all” or “a little bothersome” (Figure 9B).
 |
Figure 9 Percentage of patients experiencing photic phenomenon in response to quality of vision questionnaire (A) frequency of glare, halos and starbursts and (B) level of bothersome glare, halos and starbursts following Precizon Presbyopia IOL implantation. |
Surgical Complications and Adverse Events
During surgery, a capsular tension ring was placed in two eyes (1.6%) due to capsular bag laxity and weakened zonular fibers. In three cases (2.4%), traces of capsular fibrosis remained in the capsular bag because they were too difficult to remove. Adverse events (AE) at 3 months included posterior capsule striae (4.9%), posterior capsular opacification (7.4%) and occurrence of halos in 4.9% of patients. These cases did not require medical intervention. Three serious adverse events (SAE) were reported; stroke in one patient and COPD exacerbation in another patient who died later, which was recorded as the third SAE. None of these SAEs were related to the investigational device.
Discussion
The Precizon Presbyopia multifocal IOL is designed to provide patients with good near, intermediate and distance visual acuity with tolerance for misalignment and changes in pupil size. This has previously been studied in an optical bench study (data on file, UNIVERSITAT POLITÈCNICA DE CATALUNYA CD6`, Terrassa, Spain), which demonstrated that Precizon Presbyopia MIOL is only moderately affected by decentration and showed good performance in small pupils or low luminance. The present clinical trial evaluated the outcomes of bilateral implantation of Precizon Presbyopia IOL in cataract and RLE patients for near, intermediate and distance visual acuities, contrast sensitivity, spectacle independence, quality of vision, MRSE, defocus curve and patient satisfaction.
The monocular and binocular UDVA of 0.10 ± 0.13 logMAR and 0.03 ± 0.12 logMAR and CDVA of 0.04 ± 0.09 logMAR and −0.02 ± 0.08 logMAR found in the current study were compared to the literature-reported corresponding mean values of refractive MIOLs and were found to be either equivalent or better (ranges: monocular UDVA 0.09 to 0.39 logMAR3,10,11 and binocular UDVA −0.01 to 0.23 logMAR);1–3,10,12–14 monocular CDVA 0.03 to 0.17 logMAR3,10,11 and binocular CDVA −0.09 to 0.08 logMAR.1–3,10,12–15 Likewise, the monocular and binocular UDVA and CDVA found in the current study were either equivalent or better than several studies of diffractive MIOLs (ranges: monocular UDVA 0.04 to 0.15 logMAR;16–19 binocular UDVA of 0.00 to 0.17 logMAR;17–25 monocular CDVA of 0.02 logMAR19 and binocular CDVA of −0.06 to 0.0817–23,26). However, there were some studies of diffractive MIOLs that have reported better distance visual acuity outcomes than the current study (ranges: binocular UDVA −0.02 to 0.008 logMAR,16,17,20,27,28 monocular CDVA −0.009 to −0.04 logMAR,16,17,28 and binocular CDVA −0.09 to −0.08 logMAR).16,20,25,26
The monocular and binocular UIVA values of 0.15 ± 0.13 logMAR and 0.06 ± 0.11 logMAR, respectively, in the current study were equivalent to or better than the corresponding values reported for other refractive MIOLs (ranges: monocular UIVA 0.15 to 0.29 logMAR3,10 and binocular UIVA 0.15 to 0.30 logMAR)1–3,10,13 as well as diffractive MIOLs (ranges: monocular UIVA 0.20 logMAR16 and binocular UIVA 0.08 to 0.16 logMAR16,17,20,21,24,27). Likewise, the monocular DCIVA of 0.16 ± 0.14 logMAR found in the current study was better than the corresponding value of 0.22 logMAR reported by one study using a refractive MIOL10 as well as another study reporting values of 0.23 logMAR after implantation of a diffractive MIOL.16 Additionally, the binocular DCIVA of 0.08 ± 0.12 logMAR found in the current study was equivalent to or better than the corresponding values reported in previous studies of refractive MIOLs (range: 0.08 to 0.29 logMAR1,2,10,13), and diffractive MIOLs (range: 0.07 to 0.31 logMAR16,17,20).
The mean monocular and binocular UNVA in the current series were 0.20 ± 0.14 logMAR and 0.14 ± 0.12 logMAR, respectively, at postoperative 3 months. These were either equivalent or better than the literature-reported values of refractive MIOLs, ranging from 0.21 to 0.28 logMAR3,10,15 for monocular UNVA and 0.15 to 0.35 logMAR1–3,10,12,13,15 for binocular UNVA. Likewise, the monocular DCNVA of 0.19 ± 0.13 logMAR and binocular DCNVA of 0.14 ± 0.12 logMAR found in the present study were similar or better than previously reported for refractive MIOLs.1–3,10,12,13 Near visual acuity outcomes of the present study were also equivalent or better than some of the diffractive MIOLs studies;19,21–25 however, other diffractive MIOL publications have reported better monocular and binocular near visual acuity.16–20,27,28 It is important to note that in the present study, we followed the ISO standards of testing near visual acuity at 40 cm. However, the power add of the Precizon Presbyopia MIOL generates a near focal point at 50 cm, translating to suboptimal near visual acuity values at 40 cm. In fact, testing of the near visual acuity at preferred distance or better match between IOL’s near point and distance of near vision measurement could explain the better near visual acuity observed in some of the previous studies.17,19,20,24,28 Since the preferred viewing distance for electronic-paper display or computer displays is approximately 50 cm, the IOLs with near-point at 50 cm, such as the one in current study would be beneficial in the real-world situations.29,30 Additionally, there was a statistically significant increase of ~0.45 logMAR in UNVA (from preoperative mean of 0.56 ± 0.19 LogMAR to postoperative mean 0.12 ± 0.13 LogMAR) and ~0.28 logMAR in DCNVA (from preoperative mean of 0.36 ± 0.13 LogMAR to postoperative mean 0.08 ± 0.12 LogMAR) for the RLE subjects (n=14) when compared with preoperative values. This increase is equivalent to approximately 4–5 lines (UNVA) and about 3 lines (DCNVA) of the ETDRS chart, further proving the effectiveness of the study IOL.
The characteristics of the defocus curve (Figure 6) explain the IOL performance of the Precizon Presbyopia IOL. Visual acuity maintained better than ~0.1 logMAR at most distances, except for a little drop at intermediate distances (0.12 logMAR, equivalent to 20/26.5); however, with 98.4% subjects either never needing spectacles or using only occasionally, spectacle independence was not affected. Overall spectacle independence is either in line with or superior than the corresponding values reported in the literature.1,2,10,16
The subjects of the current study did observe photic phenomena like glare, halos and starburst; however, these were described as “not at all” or “a little bothersome” by 77 to 87% of the subjects experiencing these phenomena. It was not possible to compare these results with previous studies because different studies have adopted different methods to report photic phenomenon. For RLE patients (n=7), the comparison of pre- and postoperative contrast sensitivity revealed reduction in contrast sensitivity postoperatively (Figure 6A and B). This may be attributed to the refractive MIOL design; however, it did not affect satisfaction as ~90% of the patients reported that they were satisfied with the outcomes and would undergo the same procedure again or would recommend this lens to others.
Generally, there may be differences between cataract and RLE patients in terms of patient satisfaction. While the cataract patients may yield a high rate of patient satisfaction owing to good improvement in corrected as well as uncorrected visual acuity, patient satisfaction may not be as good in RLE patients due to high expectations of spectacle independence post-surgery. In the present surgery, we did not analyze patient satisfaction for cataract and RLE patients separately. This could be considered as a potential limitation. Other limitations are small sample size in the RLE subgroup and lack of long-term follow-up. Future studies with larger sample size and equivalent distribution of cataract and RLE subjects may validate the current study results.
The outcomes of the present study suggest that the Precizon Presbyopia IOL implantation provides good visual outcomes at all distances following cataract extraction or refractive lens exchange.
Data Sharing Statement
The data that support the findings of this study are available on request from study sponsor OPHTEC BV.
Acknowledgments
Raman Bedi, MD critically reviewed the manuscript and IrisARC – Analytics, Research & Consulting (Chandigarh, India) provided editorial assistance in the preparation of the manuscript.
Funding
This study is funded by Ophtec BV, Groningen, The Netherlands.
Disclosure
Professor Mike Holzer and Dr Bettina Thomas report grants and non-financial support from Ophtec, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Chiam PJT, Chan JH, Haider SI, Karia N, Kasaby H, Aggarwal RK. Functional vision with bilateral ReZoom and ReSTOR intraocular lenses 6 months after cataract surgery. J Cataract Refract Surg. 2007;33(12):2057–2061. doi:10.1016/j.jcrs.2007.07.029
2. Cillino S, Casuccio A, Di Pace F, et al. One-year outcomes with new-generation multifocal intraocular lenses. Ophthalmology. 2008;115(9):1508–1516.
3. Cezon Prieto J, Bautista MJ. Visual outcomes after implantation of a refractive multifocal intraocular lens with a +3.00 D addition. J Cataract Refract Surg. 2010;36(9):1508–1516.
4. de Vries NE, Nuijts RM. Multifocal intraocular lenses in cataract surgery: literature review of benefits and side effects. J Cataract Refract Surg. 2013;39(2):268–278.
5. Agarwal A, Agarwal A, Jacob S. Phacoemulsification.
6. Hayashi K, Hayashi H, Nakao F, Hayashi F. Correlation between pupillary size and intraocular lens decentration and visual acuity of a zonal-progressive multifocal lens and a monofocal lens. Ophthalmology. 2001;108(11):2011–2017.
7. Soda M, Yaguchi S. Effect of decentration on the optical performance in multifocal intraocular lenses. Ophthalmologica. 2012;227(4):197–204.
8. Retzlaff JA, Sanders DR, Kraff MC. Development of the SRK/T intraocular lens implant power calculation formula. J Cataract Refract Surg. 1990;16(3):333–340.
9. McAlinden C, Pesudovs K, Moore JE. The development of an instrument to measure quality of vision: the Quality of Vision (QoV) questionnaire. Invest Ophthalmol Vis Sci. 2010;51(11):5537–5545.
10. Chang DF. Prospective functional and clinical comparison of bilateral ReZoom and ReSTOR intraocular lenses in patients 70 years or younger. J Cataract Refract Surg. 2008;34(6):934–941. doi:10.1016/j.jcrs.2007.12.053
11. Nuzzi R, Tridico F. Comparison of visual outcomes, spectacles dependence and patient satisfaction of multifocal and accommodative intraocular lenses: innovative perspectives for maximal refractive-oriented cataract surgery. BMC Ophthalmol. 2017;17(1):12.
12. Alio JL, Plaza-Puche AB, Javaloy J, Ayala MJ, Moreno LJ, Pinero DP. Comparison of a new refractive multifocal intraocular lens with an inferior segmental near add and a diffractive multifocal intraocular lens. Ophthalmology. 2012;119(3):555–563.
13. Lan J, Huang YS, Dai YH, Wu XM, Sun JJ, Xie LX. Visual performance with accommodating and multifocal intraocular lenses. Int J Ophthalmol. 2017;10(2):235–240.
14. Lin HT, Chen WR, Ding ZF, Chen W, Wu CR. Clinical evaluation of two multifocal intraocular lens implantation patterns. Int J Ophthalmol. 2012;5(1):76–83.
15. Venter JA, Pelouskova M, Collins BM, Schallhorn SC, Hannan SJ. Visual outcomes and patient satisfaction in 9366 eyes using a refractive segmented multifocal intraocular lens. J Cataract Refract Surg. 2013;39(10):1477–1484.
16. Chang DH. Visual acuity and patient satisfaction at varied distances and lighting conditions after implantation of an aspheric diffractive multifocal one-piece intraocular lens. Clin Ophthalmol. 2016;10:1471–1477.
17. de Vries NE, Webers CA, Montes-Mico R, Ferrer-Blasco T, Nuijts RM. Visual outcomes after cataract surgery with implantation of a +3.00 D or +4.00 D aspheric diffractive multifocal intraocular lens: comparative study. J Cataract Refract Surg. 2010;36(8):1316–1322.
18. Friedrich R. Intraocular lens multifocality combined with the compensation for corneal spherical aberration: a new concept of presbyopia-correcting intraocular lens. Case Rep Ophthalmol. 2012;3(3):375–383.
19. Packer M, Chu YR, Waltz KL, et al. Evaluation of the aspheric tecnis multifocal intraocular lens: one-year results from the first cohort of the food and drug administration clinical trial. Am J Ophthalmol. 2010;149(4):577–584e571.
20. Cillino G, Casuccio A, Pasti M, Bono V, Mencucci R, Cillino S. Working-age cataract patients: visual results, reading performance, and quality of life with three diffractive multifocal intraocular lenses. Ophthalmology. 2014;121(1):34–44.
21. Guo X, Sun Y, Zhang B, Zheng D. Medium-term visual outcomes of apodized diffractive multifocal intraocular lens with +3.00 d addition power. J Ophthalmol. 2014;2014:247829.
22. Hutz WW, Jackel R, Hoffman PC. Comparison of visual performance of silicone and acrylic multifocal IOLs utilizing the same diffractive design. Acta Ophthalmol. 2012;90(6):530–533.
23. Schmickler S, Bautista CP, Goes F, Shah S, Wolffsohn JS. Clinical evaluation of a multifocal aspheric diffractive intraocular lens. Br J Ophthalmol. 2013;97(12):1560–1564.
24. Tsaousis KT, Plainis S, Dimitrakos SA, Tsinopoulos IT. Binocularity enhances visual acuity of eyes implanted with multifocal intraocular lenses. J Refract Surg. 2013;29(4):246–250.
25. Yoshino M, Bissen-Miyajima H, Oki S, Minami K, Nakamura K. Two-year follow-up after implantation of diffractive aspheric silicone multifocal intraocular lenses. Acta Ophthalmol. 2011;89(7):617–621.
26. Alfonso JF, Fernandez-Vega L, Puchades C, Montes-Mico R. Intermediate visual function with different multifocal intraocular lens models. J Cataract Refract Surg. 2010;36(5):733–739.
27. Lubinski W, Gronkowska-Serafin J, Podboraczynska-Jodko K. Clinical outcomes after cataract surgery with implantation of the Tecnis ZMB00 multifocal intraocular lens. Med Sci Monit. 2014;20:1220–1226.
28. Mesci C, Erbil HH, Olgun A, Aydin N, Candemir B, Akcakaya AA. Differences in contrast sensitivity between monofocal, multifocal and accommodating intraocular lenses: long-term results. Clin Exp Ophthalmol. 2010;38(8):768–777.
29. Shieh KK, Lee DS. Preferred viewing distance and screen angle of electronic paper displays. Appl Ergon. 2007;38(5):601–608.
30. Shin G, Hegde S. User-preferred position of computer displays: effects of display size. Hum Factors. 2010;52(5):574–585.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.