")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 15
Bictegravir/Emtricitabine/Tenofovir Alafenamide for HIV-1: What is the Hidden Potential of This Emerging Treatment?
Authors Januszka JE , Drwiega EN, Badowski ME
Received 22 June 2023
Accepted for publication 27 October 2023
Published 29 November 2023 Volume 2023:15 Pages 705—711
DOI https://doi.org/10.2147/HIV.S385877
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Jenna E Januszka, Emily N Drwiega, Melissa E Badowski
University of Illinois at Chicago, College of Pharmacy, Chicago, IL, USA
Correspondence: Melissa E Badowski, Clinical Assistant Professor of Pharmacy Practice, Department of Pharmacy Practice, College of Pharmacy, University of Illinois at Chicago, 833 S. Wood St., Rm 164, M/C 886, Chicago, IL, 60612, USA, Email [email protected]
Abstract: Bictegravir/emtricitabine/tenofovir alafenamide (B/F/TAF) is a single-tablet antiretroviral therapy regimen. B/F/TAF has become a popular treatment choice because of its small tablet size, high barrier to resistance, favorable tolerability, and limited drug–drug interaction profile. Continued research on B/F/TAF has revealed additional potential for this regimen. This review presents recent literature supporting the use of B/F/TAF as an option for consolidating therapy and maintaining virologic suppression in individuals despite M184V/I mutations. Additionally, children are a unique patient population with limited antiviral options. Standard dose B/F/TAF has demonstrated similar drug exposure in children and adolescents as adults, and low-dose B/F/TAF is approved for children living with HIV greater than two years of age and weighing at least 14 kg. Data supporting this recommendation is described in this review. Finally, despite a lack of prospective data, B/F/TAF may have a role in the future of pre- and post-exposure prophylaxis. This review discusses these discoveries and the continued exploration of the hidden potential of B/F/TAF.
Keywords: Biktarvy, bictegravir, INSTI, HIV
Introduction
Co-formulated bictegravir/emtricitabine/tenofovir alafenamide (B/F/TAF) is an integrase inhibitor-based, single-tablet antiretroviral regimen. Integrase inhibitors (INSTIs) are potent, well-tolerated antiretrovirals with high barriers to resistance, and are associated with faster virologic suppression than other antiretroviral classes. Second-generation INSTIs, including bictegravir, are recommended as anchor drugs in all first-line regimens by the United States Department of Health and Human Services (DHHS) guidelines for the treatment of human immunodeficiency virus (HIV) in adult and adolescent patients.1 In clinical trials, B/F/TAF was found to be non-inferior to dolutegravir in combination with either co-formulated emtricitabine/tenofovir alafenamide or co-formulated dolutegravir/abacavir/lamivudine, which is the standard of care.2–5 Owing to its small tablet size, high barrier to resistance, favorable tolerability, and drug–drug interaction profile, B/F/TAF has become the mainstay of modern antiretroviral therapy. Pertinent literature published after 2015 in English was reviewed by the authors for inclusion in this article. This review discusses the latest discoveries in the potential of B/F/TAF, such as its durability against antiretroviral resistance (Table 1),3,4,6–11 its use in pediatric patients, and its emergence as a novel post-exposure prophylaxis (PEP) option.
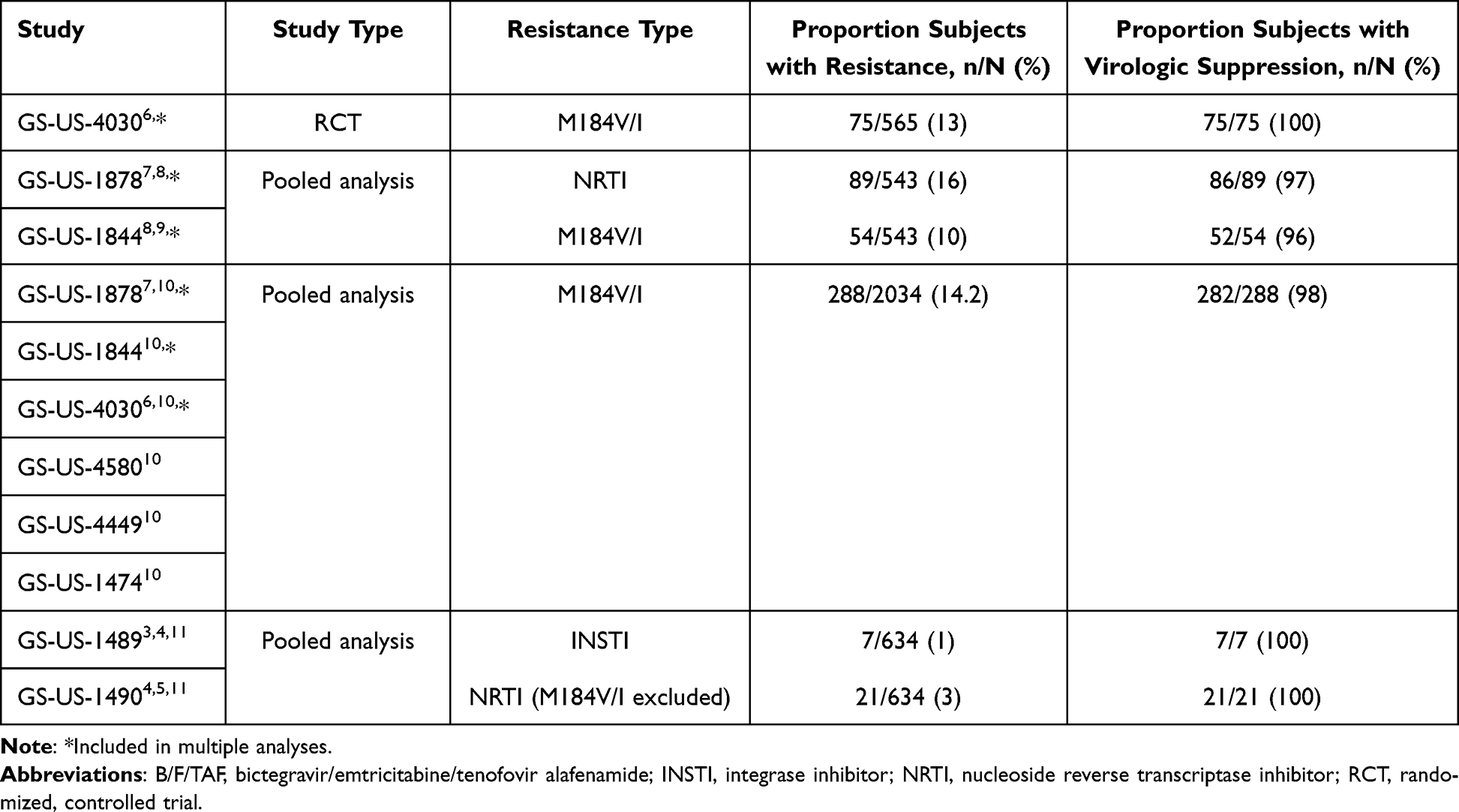 |
Table 1 Summary of Pre-Existing Resistance in B/F/TAF Clinical Trials |
Durability Against M184V/Is and Pre-Existing INSTI Resistance
Both the M184V and M184I mutations confer high-level resistance to emtricitabine but increase susceptibility of the virus to tenofovir; the phenotypic differences between these two mutations lie in their propensity to decrease viral fitness.12 The M184I mutation is typically selected first and produces a greater decrease in viral fitness than the M184V; however, the M184V mutation will often outcompete and replace the M184I. There is increasing evidence that virologically suppressed patients with M184V/I mutations who are switched to B/F/TAF can maintain viral suppression with this regimen. For example, GS-US-1878 and −1844, which were randomized, multicenter trials, found that a switch to B/F/TAF compared to continuation of either a boosted protease inhibitor- or dolutegravir-containing regimen had noninferior efficacy at week 48.7,9 The cumulative pre-existing resistance data from these trials were taken from historical genotypes and retrospective baseline proviral archive DNA genotyping for a subgroup analysis of outcomes in patients with resistance mutations.8 A total of 10% of participants from both studies (54 of 543) treated with B/F/TAF had an M184V/I mutation. Of these participants, 96% maintained viral suppression at week 48 or the last study visit, compared with a 99% suppression rate among patients with wild-type M184 (p > 0.05). Furthermore, the two participants in the B/F/TAF group failed to maintain suppression, with medication adherence rates of 71% and 76%, respectively.8 These findings emphasize the importance of medication adherence in maintaining virologic suppression.
The same authors performed a similar analysis using resistance data from GS-US-4030, a randomized double-blind trial of virologically suppressed patients who switched from a dolutegravir-based regimen to B/F/TAF. Notably, this was the first B/F/TAF switch study to proactively enroll participants with resistance mutations.6 Of the 565 subjects enrolled, 71 had an M184V substitution alone and 4 had M184V/I. The primary endpoint of the study assessed difference in the proportion of patients with an HIV-1 RNA ≥ 50 copies/mL in both groups at week 48 using the US Food and Drug Administration (FDA) snapshot algorithm.13 In this study, all patients with a known M184V/I mutation had a viral load of <50 copies/mL at week 48 or last study visit. This demonstrates the ability of B/F/TAF to effectively maintain viral suppression, despite only two of the three agents, bictegravir and tenofovir alafenamide, being active in participants with known or suspected M184V.6
A pooled analysis of GS-US Studies 4030, 4580, 1844, 1878, 4449, and 1474 was conducted to determine the impact of M184V/I mutations on virologic outcomes in patients treated with B/F/TAF.10 Of 2034 patients treated with B/F/TAF, 288 had pre-existing M184V/I mutations. Most participants with pre-existing resistance had the M184V mutation alone, with the remaining 10% evenly split between patients with M184I alone and those with both M184V/I substitutions. Three participants with pre-existing M184V/I mutations, all within GS-US-1878, failed to maintain virological suppression (HIV-1 RNA < 50 copies/mL). Two of these patients had a viral load of <100 copies/mL and were resuppressed either on B/F/TAF or with boosted atazanavir with emtricitabine/tenofovir disoproxil fumarate (F/TDF). The third patient, without virologic suppression, had documented medication nonadherence with undetectable bictegravir plasma levels and did not develop treatment-emergent resistance. Overall, 98% of patients with an M184V/I mutation maintained virologic suppression compared to 99% of those without an M184V/I mutation.10 The findings of this analysis were consistent with the findings of previous studies that B/F/TAF maintained its effectiveness in patients with pre-existing M184V/I mutations.
Finally, a retrospective analysis of treatment-experienced persons living with HIV (PWH) starting B/F/TAF evaluated the rates of viral suppression in subjects with and without pre-existing nucleoside-reverse transcriptase inhibitor (NRTI) resistance mutations.14 The majority of the included patients (86.6%) were virologically suppressed at baseline. The primary efficacy endpoint was the percentage of participants with HIV-1 RNA levels <50 copies/mL at week 48. A total of 506 were included in the analysis with only 69 subjects (13.6%) with pre-existing NRTI resistance mutations. The most common mutation was M184V/I (N = 57). Additionally, 30 patients had tenofovir resistance. There were no differences in virologic suppression between the patients with and without NRTI resistance (82.2% and 88.4%, respectively). All nine patients with high-level tenofovir resistance and an M184V mutation had HIV-RNA <50 copies/mL at week 48. Overall, these real-world data suggest that B/F/TAF is an effective regimen for PWH with pre-existing NRTI resistance mutations.
B/F/TAF has been shown to be an efficacious switch regimen in patients with a suppressed viral load, with the caveat that maintaining medication adherence is necessary to achieve this outcome. To date, there are no data regarding bictegravir-containing regimens for patients with M184V who are not yet virologically suppressed and because of the level of adherence necessary to maintain a suppressed viral load on this regimen, B/F/TAF may not be an ideal regimen in people with virologic non-suppression who struggle with medication adherence.15 Overall, the use of B/F/TAF as a suppressive regimen is not recommended in patients who have not yet achieved viral suppression.
A 3-year resistance analysis of two, Phase 3, randomized, double-blind, active controlled studies, GS-US-1489 and GS-US-1490 was conducted to determine the impact of baseline resistance on treatment response to BIC/F/TAF in treatment-naïve participants.11 People with pre-existing M184V mutations were excluded from both studies. In the B/F/TAF arm, 21 participants had primary, or major, NRTI resistance and 7 had primary INSTI-resistance. Secondary INSTI-associated resistance was present in 326 participants at baseline; however, secondary INSTI-resistance mutations rarely confer resistance to INSTIs in the absence of additional mutations. In subjects with pre-treatment resistance of any kind, 98% achieved HIV-1 RNA < 50 copies/mL at week 144 compared to 97% of subjects without pre-existing resistance. Furthermore, all participants identified as having primary INSTI-resistance, including one with Q148H and G140S substitutions in the BIC/F/TAF arm, achieved an HIV-1 RNA of <50 copies/mL at week 144 or at their last visit. None of the participants acquired resistance substitutions during the study period.11
Treatment-Experienced
Pediatrics
Treatment regimens for pediatric PWH are considerably less abundant than those indicated for adolescents and adults; more specifically, there are currently only two fixed-dose combination single-tablet regimens available for pediatric patients weighing less than 25 kg.16 B/F/TAF was approved by the US FDA in October of 2021 for patients at least 2 years of age and weighing at least 14 kg.17
The pharmacokinetics (PK) of antiretrovirals can be used as a surrogate endpoint to predict their efficacy in pediatric patients. The PK of bictegravir 50 mg, emtricitabine 200 mg, and tenofovir alafenamide 25 mg were studied in 100 virologically suppressed children between the ages of 6 and 18 years in a single-arm, open-label trial.18 In Trial 1474, participants were split into two cohorts based on age: cohort one including adolescents aged 12–18 years and cohort two including children aged 6–11 years. Virological suppression of an HIV-1 RNA viral load of <50 copies/mL at weeks 24 and 48, as defined by the FDA-snapshot analysis, was key secondary endpoints. The assumed geometric least squares mean (GLSM) ratio between pediatric and adult areas under the curve (AUC) and plasma concentrations of bictegravir were used to determine that the PK equivalency of bictegravir was 70–143% and the predicted exposure of subjects was comparable to that of adults with HIV who participated in phase 3 studies. Emtricitabine and tenofovir alafenamide (TAF) exposures were also evaluated. Both cohorts met the primary endpoint of PK equivalence, with GLSM ratios of 86.3% (95% confidence interval 80–93%) and 125% (95% confidence interval: 117–134) in cohorts one and two, respectively. The AUCs for emtricitabine and TAF were similar in adolescents and adults; however, children had 43% and 85% higher AUCs than adults for emtricitabine and TAF, respectively. Virologic suppression was maintained in all subjects at week 100 and in 98% of the subjects at week 48. Of the two patients without virologic suppression, one discontinued treatment before week 48, and the other had a viral load >50 copies/mL. Overall, B/F/TAF was effective in maintaining virologic suppression in children and adolescents living with HIV, and had similar exposure to the study drug as adults.
A low-dose formulation of bictegravir 30 mg, emtricitabine 120 mg, and TAF 15 mg was also investigated in children with HIV greater than two years of age and weighing at least 14 kg.19 This as well as in an open-label, single-arm trial with data up to 12 weeks of follow-up presented at CROI 2020 and 24 weeks of follow-up included in the full prescribing information.19,20 Adverse events, virologic suppression at week 12, and bictegravir PK equivalence, with an equivalence boundary of 50–200% were assessed.19 A total of 22 children between the ages of 3 and 9 years and weighing between 14.0 and 24.1 kg were enrolled in the study. Irritability, social avoidant behavior, and neutropenia were reported as adverse effects in one patient each. Ten of the 11 children with HIV-1 RNA data available at week 12 were reported to have a viral load of <50 copies/mL in the preliminary results presented at CROI 2020. At week 24, 20 of 22 patients remained virologically suppressed. The remaining two subjects did not have data available at week 24 due to COVID-19 pandemic-related study disruptions.19 The AUC geometric mean ratio of bictegravir equivalence between children and adults was slightly higher than 100% (exact ratio not reported).19 In this study, low-dose B/F/TAF was well tolerated and highly effective in maintaining virologic suppression in children as young as 3 years of age.19,20
The ability of the children to swallow the low-dose tablet was also assessed in a previous trial; the low-dose tablet was slightly smaller than the full-dose tablet.19 All but one child was able to swallow the tablet. The remaining child split the tablet in half and was able to swallow both halves within 10 minutes of each other. For patients unable to swallow tablets, either halved or whole, B/F/TAF can be dissolved in water and administered orally.21 However, according to the SOLUBIC trial, B/F/TAF should not be crushed and administered in vehicles such as applesauce or yogurt because of decreased exposure to emtricitabine and TAF.21 Dissolving B/F/TAF may be a viable alternative for administration in adults and children with swallowing difficulties.
Adults
Although single-tablet regimens are routinely combined with other combination products or single agents in clinical practice, there is a paucity of data regarding documented or suspected resistance. A concern with combining combination products is that they may result in higher dosages of medications, as these products cannot be split. A nonrandomized, prospective PK study evaluated the role of B/F/TAF with darunavir/cobicistat (DRV/c) in nine treatment-experienced PWH with a creatinine clearance greater than 30 mL/min.22 Participant age ranged from 54 to 67 years, with a median of 19 years of antiretroviral therapy (range 5.8–30 years). Bictegravir exposure (AUC0-tau) increased by approximately 26% compared to the historical PK data. Using 25 mg of TAF as part of the combination tablet B/F/TAF along with DRV/c produced TAF exposures that were considerably increased by approximately 17%. However, because of TAF’s intracellular metabolism of TAF, the plasma concentrations of the parent drug tenofovir were only modestly increased. The results of this PK study demonstrate that B/F/TAF with DRV/c may be considered an option for treatment-experienced individuals.
An open-label switch study evaluated B/F/TAF in combination with doravirine (DOR) in heavily treatment-experienced men with multidrug resistant HIV who were virologically suppressed on rilpivirine (RPV)/F/TAF plus dolutegravir for at least 6 months.23 Additionally, participants had to be ≥45 years of age with documented resistance to NRTIs, non-nucleoside reverse transcriptase inhibitors (the exceptions being rilpivirine and doravirine resistance), and/or protease inhibitors. In addition, no K65R or T69 insertion mutation was detected. Twenty participants met the eligibility criteria; their ages ranged from 46 to 74 years, with a median of 37 years of antiretroviral therapy (range, 12–42 years). All participants remained virologically suppressed at week 48 with bictegravir and doravirine PK parameters, which is consistent with previously published data. Additionally, this regimen was well tolerated, safe, and effective for the treatment of heavily treatment-experienced men with multidrug-resistant HIV. Although single-tablet regimens are approved as complete regimens for the management of HIV, they may be useful in combination with other agents to reduce the pill burden and promote medication adherence.
PEP/PrEP
No randomized placebo-controlled trials have evaluated the efficacy of HIV PEP after sexual exposure in humans. Performing such a study would require a large cohort and present ethical concerns, leaving us to rely on small observational studies, case reports, non-human studies, and expert opinions.24
For most adults and adolescents at least 13 years of age, the preferred regimen for sexual, injection drug use, or other non-occupational exposure PEP, as listed in the 2016 CDC Guidelines, is a 3-drug combination of F/TDF as a fixed-dose single tablet once daily in combination with raltegravir 400 mg twice daily or in combination with dolutegravir 50 mg once daily.24 Unfortunately, both preferred regimens require at least two pills daily, and a single-tablet regimen would be optimal. Single-dose treatment regimens have been explored for PEP, including elvitegravir/cobicistat/emtricitabine/tenofovir disoproxil fumarate (EVG/c/F/TDF) and B/F/TAF.25–27 The benefits of B/F/TAF over EVG/c/F/TDF include reduced drug–drug interactions because of the lack of necessity for the PK booster, cobicistat, and the lack of food requirements. Additionally, compared to TDF, TAF has fewer adverse effects on bone mineral density and renal toxicity.
Investigators at an HIV/PEP Boston Community Health Center led an open-label Phase 4 clinical trial assessing B/F/TAF for persons exposed to HIV-infected individuals through condomless intercourse.25 Individuals who presented within 72 h of exposure were eligible for PEP, inclusion in the trial, and administered a 28-day supply of B/F/TAF. Fifty-two patients were included in this analysis: 47 (90.4%) completed their course of therapy, which was significantly improved based on completion rates in similar studies with alternative therapies at the same health center, including EVG/c/F/TDF (71.0%, p < 0.05). In this study, none of the participants tested positive for HIV at four weeks or reported seroconversion when interviewed at three months.
Additionally, at the 2022 International AIDS Conference, researchers shared results from a second open-label phase 4 clinical trial.28 Similarly, this study assessed people receiving B/F/TAF in an STD/AIDS clinic in Beijing, China, for PEP for persons with potential sexual exposure to HIV. A larger cohort of 112 participants was enrolled, and adherence was reported to be >98% based on both participant reporting and pill counts. None of the patients acquired HIV infection after 24 weeks.
Together, these two studies demonstrated excellent patient adherence to B/F/TAF for PEP, which may be due to its once-daily single-tablet regimen, lack of drug–drug interactions, and minimal adverse effects. They also support further exploration of B/F/TAF and its possible hidden potential as a PEP, despite the lack of placebo-controlled, randomized clinical trials.
Intermittent, event-driven pre-exposure prophylaxis (PrEP) is an off-label use of F/TDF for men who have sex with men desiring a non-daily oral regimen, requiring administration of therapy 2–24 hours prior to sex, as well as 24 and 48 hours later (2-1-1).29 Given the timing of HIV DNA integration after reverse transcription, it has been hypothesized that adding an INSTI to an NRTI regimen for 2-1-1 PrEP may increase the window of prevention.30 This was explored in a SHIV macaque study of two-dose, event-driven therapy.30 When administered 2 hours before and 24 hours after, emtricitabine/TAF (F/TAF) and bictegravir 25 mg prevented 100% (6/6) of SHIV seroconversion but this was similar to F/TAF alone (5/6, 83%, 95.2% per-exposure risk reduction). When the same regimen was administered 24 hours apart starting at either 24 or 48 h post-exposure, 1/6 and 0/6 animals, respectively. In six macaques receiving F/TAF in combination with bictegravir 100 mg as PEP, 5/6 (83%, 90.1% per exposure risk reduction) macaques were protected when therapy was initiated 6 h post-exposure, compared to 3/6 (50%, 57.8% risk reduction) with F/TAF alone. When initiated 12-hours post-exposure, this difference did not persist, with 4/6 (67%, 81.7% per-exposure risk reduction) in those receiving F/TAF and bictegravir compared with 4/6 (67%, 78.2% per exposure risk reduction) in F/TAF alone. The pharmacokinetics of these drugs differ in humans and macaques, as do the inhibitory drug concentrations; thus, prediction of the outcomes in humans is challenging.30 However, these results support further exploration of PEP and two-dose schedules of event-driven PrEP with BIC/F/TAF.
Conclusions
B/F/TAF is included in the DHHS guidelines for the treatment of HIV in adults and adolescent patients as a first-line regimen.1 As we have demonstrated throughout this review, continued research of B/F/TAF has exposed additional potential roles of this regimen. Switching to B/F/TAF has demonstrated efficacy despite the presence of an M184V resistance mutation in virologically suppressed patients and may be a useful tool for consolidating therapy in treatment-experienced patients with a large pill burden or in those experiencing adverse effects. The FDA approval of B/F/TAF in children as young as 2 years of age has further expanded its utility. Finally, the ongoing research on B/F/TAF and its role in PEP and PrEP has the potential to lead to B/F/TAF inclusion as an option. B/F/TAF currently remains unavailable or inaccessible in resource limited settings. This is likely due to the availability of a similarly structured, generic, single-tablet formulation of dolutegravir, lamivudine, and TDF and the World Health Organization’s preference of TDF over TAF.31 Other characteristics of B/F/TAF, such as its tolerability and drug–drug interaction profile, contribute to the desire to explore and identify its expanded potential.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Guidelines for the use of antiretroviral agents in adults and adolescents with HIV; 2023. Available from: https://clinicalinfo.hiv.gov/en/guidelines/hiv-clinical-guidelines-adult-and-adolescent-arv/whats-new.
2. HIV Info Specialist. Guidelines for the use of antiretroviral agents in adults and adolescents with HIV; 2017.
3. Gallant J, Lazzarin A, Mills A, et al. Bictegravir, emtricitabine, and tenofovir alafenamide versus dolutegravir, Abacavir, and lamivudine for initial treatment of HIV-1 infection (GS-US-380-1489): a double-blind, multicentre, phase 3, randomised controlled non-inferiority trial. Lancet. 2017;390(10107):2063–2072. doi:10.1016/S0140-6736(17)32299-7
4. Orkin C, DeJesus E, Sax PE, et al. Fixed-dose combination bictegravir, emtricitabine, and tenofovir alafenamide versus dolutegravir-containing regimens for initial treatment of HIV-1 infection: week 144 results from two randomised, double-blind, multicentre, phase 3, non-inferiority trials. Lancet HIV. 2020;7(6):e389–e400. doi:10.1016/S2352-3018(20)30099-0
5. Sax PE, Pozniak A, Montes ML, et al. Coformulated bictegravir, emtricitabine, and tenofovir alafenamide versus dolutegravir with emtricitabine and tenofovir alafenamide, for initial treatment of HIV-1 infection (GS-US-380–1490): a randomised, double-blind, multicentre, phase 3, non-inferiority trial. Lancet. 2017;390(10107):2073–2082. doi:10.1016/S0140-6736(17)32340-1
6. Acosta RK, Willkom M, Andreatta K, et al. Switching to Bictegravir/Emtricitabine/Tenofovir Alafenamide (B/F/TAF) From Dolutegravir (DTG)+F/TAF or DTG+F/Tenofovir Disoproxil Fumarate (TDF) in the presence of pre-existing NRTI resistance. JAIDS J Acquir Immune Defic Syndr. 2020;85(3):363–371. doi:10.1097/QAI.0000000000002454
7. Daar ES, DeJesus E, Ruane P, et al. Efficacy and safety of switching to fixed-dose bictegravir, emtricitabine, and tenofovir alafenamide from boosted protease inhibitor-based regimens in virologically suppressed adults with HIV-1: 48 week results of a randomised, open-label, multicentre, phase 3, non-inferiority trial. Lancet HIV. 2018;5(7):e347–e356. doi:10.1016/S2352-3018(18)30091-2
8. Andreatta K, Willkom M, Martin R, et al. Switching to bictegravir/emtricitabine/tenofovir alafenamide maintained HIV-1 RNA suppression in participants with archived antiretroviral resistance including M184V/I. J Antimicrob Chemother. 2019;74(12):3555–3564. doi:10.1093/jac/dkz347
9. Molina JM, Ward D, Brar I, et al. Switching to fixed-dose bictegravir, emtricitabine, and tenofovir alafenamide from dolutegravir plus Abacavir and lamivudine in virologically suppressed adults with HIV-1: 48 week results of a randomised, double-blind, multicentre, active-controlled, phase 3, non-inferiority trial. Lancet HIV. 2018;5(7):e357–e365. doi:10.1016/S2352-3018(18)30092-4
10. Andreatta K, Acosta RK, D’Antoni ML, et al. Sustained viral suppression after switch to bictegravir/emtricitabine/tenofovir alafenamide among clinical trial participants with preexisting M184V/I; 2020. Available from: https://hivglasgow.org/wp-content/uploads/2020/11/P123-_Andreatta.pdf.
11. Acosta RK, Chen GQ, Chang S, et al. Three-year study of pre-existing drug resistance substitutions and efficacy of bictegravir/emtricitabine/tenofovir alafenamide in HIV-1 treatment-naive participants. J Antimicrob Chemother. 2021;76(8):2153–2157. doi:10.1093/jac/dkab115
12. Frost SDW, Nijhuis M, Schuurman R, Boucher CAB, Brown AJL. Evolution of lamivudine resistance in human immunodeficiency virus type 1-infected individuals: the relative roles of drift and selection. J Virol. 2000;74(14):6262–6268. doi:10.1128/JVI.74.14.6262-6268.2000
13. Human immunodeficiency virus-1 infection: developing antiretroviral drugs for treatment guidance for industry; 2015 . Available from: https://www.fda.gov/media/86284/download.
14. Micán R, De Gea Grela A, Cadiñanos J, et al. Impact of preexisting nucleos(t)ide reverse transcriptase inhibitor resistance on the effectiveness of bictegravir/emtricitabine/tenofovir alafenamide in treatment experience patients. AIDS. 2022;36(14):1941–1947. doi:10.1097/QAD.0000000000003311
15. Byrd KK, Hou JG, Hazen R, et al. Antiretroviral adherence level necessary for HIV viral suppression using real-world data. JAIDS J Acquir Immune Defic Syndr. 2019;82(3):245–251. doi:10.1097/QAI.0000000000002142
16. NIH. What’s new in the guidelines for the use of antiretroviral agents in pediatric HIV infection; 2023. Available from: https://clinicalinfo.hiv.gov/en/guidelines/pediatric-arv/whats-new.
17. Businesswire. U.S. Food and Drug Administration approves expanded indication of Gilead’s Biktarvy® for treatment of HIV-1 in pediatric populations; 2021. Available from: https://www.businesswire.com/news/home/20211018005505/en/.
18. Gaur AH, Cotton MF, Rodriguez CA, et al. Fixed-dose combination bictegravir, emtricitabine, and tenofovir alafenamide in adolescents and children with HIV: week 48 results of a single-arm, open-label, multicentre, Phase 2/3 trial. Lancet Child Adolesc Health. 2021;5(9):642–651. doi:10.1016/S2352-4642(21)00165-6
19. Rodriguez CA, Chokephaibulkit K, Liberty A, et al. Safety, PK, and efficacy of low dose B/F/TAF in children > 2 years old living with HIV; 2020. Available from: https://www.croiconference.org/abstract/safety-pk-and-efficacy-of-low-dose-b-f-taf-in-children-%e2%89%a52-years-old-living-with-hiv/.
20. Highlights of prescribing information. BIKTARVY (bictegravir, emtricitabine, and tenofovir alafenamide) tablets, for oral use; 2021. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/210251s008lbl.pdf.
21. Hocqueloux L, Lefeuvre S, Bois J, et al. Bioavailability of dissolved and crushed single tablets of bictegravir, emtricitabine, tenofovir alafenamide in healthy adults: the SOLUBIC randomized crossover study. J Antimicrob Chemother. 2023;78(1):161–168. doi:10.1093/jac/dkac369
22. Salama E, Hill L, Patel N, Best BM, Momper JD. Brief report: pharmacokinetics of bictegravir and tenofovir in combination with darunavir/cobicistat in treatment-experienced persons with HIV. JAIDS J Acquir Immune Defic Syndr. 2021;88(4):389–392. doi:10.1097/QAI.0000000000002765
23. Sterman FL, Lalezari JP, Kowalczyk UM, et al. Bictegravir/emtricitabine/tenofovir alafenamide plus doravirine in highly treatment-experienced men with multidrug-resistant HIV. AIDS. 2023;37(7):1057–1064. doi:10.1097/QAD.0000000000003513
24. Dominguez KL, Smith DK, Vasavi T, et al. Updated guidelines for antiretroviral postexposure prophylaxis after sexual, injection drug use, or other nonoccupational exposure to HIV—United States; 2016. Available from: https://stacks.cdc.gov/view/cdc/38856.
25. Mayer KH, Gelman M, Holmes J, Kraft J, Melbourne K, Mimiaga MJ. Safety and tolerability of once daily coformulated bictegravir, emtricitabine, and tenofovir alafenamide for postexposure prophylaxis after sexual exposure. J Acquir Immune Defic Syndr. 2022;90(1):27–32. doi:10.1097/QAI.0000000000002912
26. Mayer KH, Jones D, Oldenburg C, et al. Optimal HIV postexposure prophylaxis regimen completion with single tablet daily elvitegravir/cobicistat/tenofovir disoproxil fumarate/emtricitabine compared with more frequent dosing regimens. J Acquir Immune Defic Syndr. 2017;75(5):535–539. doi:10.1097/QAI.0000000000001440
27. Gantner P, Hessamfar M, Souala MF, et al. Elvitegravir-cobicistat-emtricitabine-tenofovir alafenamide single-tablet regimen for human immunodeficiency virus postexposure prophylaxis. Clin Infect Dis off Publ Infect Dis Soc Am. 2020;70(5):943–946. doi:10.1093/cid/ciz577
28. Liu A, Xin R, Zhang H, et al. A Phase IV open-label evaluation of safety and tolerability of coformulated bictegravir/emtricitabine/tenofovir alafenamide for post-exposure prophylaxis following potential exposure to HIV-1; 2022.
29. U.S. Public Health Service., Preexposure prophylaxis for the prevention of HIV infection in the United States - 2021 Update; 2021 Available from: /https://www.cdc.gov/hiv/pdf/risk/prep/cdc-hiv-prep-guidelines-2021.pdf
30. Bekerman E, Cox S, Babusis D, et al. Two-dose emtricitabine/tenofovir alafenamide plus bictegravir prophylaxis protects macaques against SHIV infection. J Antimicrob Chemother. 2021;76(3):692–698. doi:10.1093/jac/dkaa476
31. World Health Organization. Consolidated guidelines on HIV, viral hepatitis and STI prevention, diagnosis, treatment and care for key populations. Geneva: World Health Organization; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK586603/.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.