")
Back to Journals » Clinical Optometry » Volume 16
Baseline Accommodation and Binocular Vision Measures in Malay Schoolchildren Enrolled in the Myopia Control Study Using Spectacle Lenses in Kuala Lumpur
Authors Norazman FNN, Mohd-Ali B , Syed Mohd Dardin SF, Mohamad Shahimin M , Mohamad Fadzil N, Mohd Saman MN, Mohidin N
Received 30 July 2023
Accepted for publication 22 January 2024
Published 20 February 2024 Volume 2024:16 Pages 45—52
DOI https://doi.org/10.2147/OPTO.S432496
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Mr Simon Berry
Fatin Nur Najwa Norazman,1,2,* Bariah Mohd-Ali,1,* Syarifah Faiza Syed Mohd Dardin,1,* Mizhanim Mohamad Shahimin,1,* Norliza Mohamad Fadzil,1,* Mohd Norhafizun Mohd Saman,1,* Norhani Mohidin1,*
1Optometry and Vision Science Program and Research Centre for Community Health (Reach), Faculty of Health Science, Universiti Kebangsaan Malaysia, Kuala Lumpur, Malaysia; 2Centre for Optometry Studies, Faculty of Health Sciences, Universiti Teknologi MARA Cawangan Selangor, Kampus Puncak Alam, Selangor, 42300, Malaysia
*These authors contributed equally to this work
Correspondence: Bariah Mohd-Ali, Optometry and Vision Science Program and Centre for Community Health, Faculty of Health Science, Universiti Kebangsaan Malaysia, Jalan Raja Muda Abdul Aziz, Kuala Lumpur, 50300, Malaysia, Tel +60 39 289 7602, Email [email protected]
Abstract: Myopia control lenses have been shown to modify visual function; however, it is arguable if these changes are short-term or long-term. We investigated the changes in accommodative behaviour and binocular vision functions of Malay myopic children who participated in a myopia control trial utilising spectacle lenses (n = 40). This article presents baseline accommodation and binocular vision measurements. The mean (± SD) age, spherical equivalent measured by cycloplegic autorefraction, and axial length (AL) for the right eyes were 10.00 ± 1.47 years, − 3.02 ± 1.20 D, and 24.42 ± 0.93 mm, respectively. All participants had good distance and near visual acuities with high-contrast charts (100%), which were significantly better than low-contrast charts (10%) (p < 0.001). The mean (± SD) accommodative lag at baseline was 1.14 ± 0.35 D, while monocular and binocular accommodative amplitudes were 15.35 ± 2.07 D and 16.82 ± 2.27 D, respectively. Malay schoolchildren in this study were more esophoric at near compared to distance, with an accommodative-convergence over accommodation (AC/A) ratio of 5.64 ± 0.66 ∆/D. A higher degree of myopia was found to be associated with a longer AL (r = − 0.49, p < 0.05) and higher esophoria at near (r = − 0.46, p < 0.05). These baseline measures are consistent with data from other studies showing that myopic children have a high accommodative lag, an elevated AC/A ratio, a longer AL, and are more esophoric at near. The measures reported herein will serve as a basis for examining changes that occur within 12 months of wearing myopia control spectacle lenses.
Keywords: myopic schoolchildren, myopia control spectacle, accommodation, binocular vision
Introduction
The prevalence of myopia is increasing globally, especially in East Asian countries. Holden et al1 estimate that half of the world’s population will become myopic by 2050. This alarming rate has made myopia a worldwide public health issue. Myopia diagnosed at a young age tends to progress more rapidly to high myopia, and high myopia is associated with sight-threatening diseases such as retinal detachment, glaucoma, and cataract.2
Previous epidemiology studies have shown an association between excessive near work and the onset and progression of myopia.3,4 Subsequently, increased accommodative effort during near work has been proposed to be one of the causative factors for myopia development in young children.3 It is hypothesised that a larger lag of accommodation associated with high accommodative demand produces hyperopic defocus at the fovea, providing a stimulus for the eye to grow and become myopic.5 Nevertheless, evidence from previous studies is contradictory, with few investigators reporting a larger lag of accommodation in myopic than emmetropic eyes,6,7 while other reports showed similar outcomes between both groups.8 In another report, Mutti et al9 stated that increased accommodative lag is unlikely to be a predictive factor for myopia onset but is often present after the onset of myopia. Therefore, there is a justification to evaluate changes in accommodation parameters in myopic children undergoing treatment for myopia control.
This report describes the baseline data on accommodation and binocular vision parameters of Malay myopic children who participated in a myopia control study using spectacle lenses in Kuala Lumpur (MyCOSKL). In this study, changes in accommodative behaviour and binocular vision functions will be evaluated at baseline and after the intervention with spectacle lenses. To our knowledge, there is limited data available in the literature about the accommodation and binocular vision parameters in Malay myopic schoolchildren; hence, the data presented in this report may be used as a reference for clinicians when managing myopic children.
The children in this study wore customised spectacle lenses designed to control myopia by simultaneously introducing myopic defocus and clear vision at all viewing distances. This special lens has a clear optical zone in the middle that is 9 mm wide and is used to correct distance refractive errors. It is surrounded by a 33-mm-diameter annular dual-focal zone made up of small circular lenslets. Each lenslet has a diameter of 1.03 mm and an addition power of +3.50 DS. Past studies on myopia control lenses have demonstrated the existence of changes in binocular vision function following lens wear.10–12 Hence, the current study aimed to examine the changes in accommodation and binocular vision functions that occur before and following the use of this newly designed spectacle lens. Follow-up data will show the changes in these parameters following short-term and long-term of lens wear. The objective of this paper is to describe the demographic data and baseline measures of accommodative and vergence parameters for children enrolled in MyCOSKL. The analysis of these data will provide valuable insights into the visual characteristics and oculomotor functions within this specific population.
Materials and Methods
Participants and Study Design
MyCOSKL is a longitudinal study that was conducted by following Malay primary schoolchildren for 12 months. Malay myopic children from around Kuala Lumpur were invited to participate in this study. Eligible children aged between 7 and 12 years old with a central spherical equivalent between −0.50 D and −5.00 D, astigmatism and anisometropia of less than 1.50 D, and a monocular best-corrected visual acuity (VA) of 6/6 or better were selected. All children were free from any ocular and systemic abnormalities or binocular vision problems, and had no history of myopia control treatment prior to study enrolment.
The sample size calculation was made using G Power software version 3.1.9.4. Based on the type of ANOVA repeated measurement statistical test with an alpha level of 0.05, the minimum number of subjects required to achieve 90% power to detect a 0.25 D difference in visual function measurements was 24. Assuming a dropout rate of about 20%, at least 29 subjects were required for this study.
The Human Subjects Ethics Subcommittee of Universiti Kebangsaan Malaysia (UKM PPI/111/8/JEP-2020-667) approved this study, and it complied with the Declaration of Helsinki’s guidelines for the use of human subjects in scientific research. Informed consents were obtained from the parents or guardians of all participants before the study commenced.
Visual Function Measurement
The following visual parameters were evaluated: spherical equivalent of cycloplegic autorefraction (SER), axial length (AL), high- and low-contrast VA at distance and near, lag of accommodation, stereoacuity, near point of convergence (NPC), monocular and binocular amplitude of accommodation (AA), and distance and near horizontal phoria.
Using a Shin-Nippon NVision-WAM 5500 open-field autorefractor (Ajinomoto Trading Inc., Tokyo, Japan), the refraction was measured 30 minutes after two drops of 1% cyclopentolate were administered 5 minutes apart. The SER (sphere and half-cylinder) was calculated based on the average of five cycloplegic autorefraction measurements. Next, the average of five AL measurements obtained by Lenstar LS900 (Haag-Streit AG, Switzerland) was calculated and recorded.
The distance high-contrast (100% contrast) VA (HCVA) and low contrast (10%) VA (LCVA) were measured using the Logarithmic 2000 series Early Treatment Diabetic Retinopathy Charts (Precision Vision Inc., Woodstock, IL, USA) on an illuminated cabinet at a distance of 4 m. The near high-contrast VA (NHCVA) and low-contrast VA (NLCVA) were measured at 40 cm using the Mixed Contrast European-Wide Near Vision Card (Precision Vision Inc., Woodstock, IL, USA). A letter-by-letter logarithm of the minimum angle of resolution (log MAR) was used to record VA, and each letter on the chart represented a score of 0.02 points. The children were requested to read from the biggest to the smallest row of the chart. The testing was stopped when the children missed three or more letters per row or when letters were read incorrectly. All measurements were conducted both monocularly and binocularly under standardised room illumination of 500 cd/m2.
Binocularity and Accommodation
The binocularity and accommodation tests were administered in a predetermined order to preserve data integrity and limit visual system strain. The measurement was taken with the participants’ best corrected VA.
Initially, an open-field autorefractor (Shin-Nippon NVision-WAM 5500 from Ajinomoto Trading Inc., Tokyo, Japan) was used to measure the accommodative response. The test was done with participants viewing the target binocularly at a distance of 40 cm. The children were instructed to ensure that the 20/30 letter target was clear prior to the measurement. The difference between the measured accommodative response (AR) and the accommodative stimulus of 2.50 D (AS) was later subtracted to calculate the lag of accommodation (LoA); LoA = AS – AR.12
Next, stereoacuity was evaluated with the Frisby stereotest (Clement Clarke International Ltd., Haag Streit UK Ltd., Harlow, Essex). This test does not require the use of extra filter glasses to achieve a stereoscopic effect. The children were presented with stereo images on a sequence of three transparent plates with different plate thicknesses of 6, 3, and 1.5 mm. Each plate consists of four squares; however, only one had its central circular area printed from the other side of the plate to create a real-depth image. The children were instructed to locate the square in which the circle appears stereoscopically, and the result was recorded in seconds of arc.
The NPC, monocular, and binocular AA were measured with a Royal Air Force (RAF) ruler. For the NPC, participants were instructed to maintain fixation on the fixation target (a small circle) as the examiner brought it slowly towards their nose. The NPC was recorded (in cm) when participants reported the target becoming double or the examiner observed the participant’s eye deviating. For AA measurement, the children were asked to keep the word target of N5 clear while the examiner slowly moved the chart towards them. The children need to quickly report when a first sustained blur is seen, even after a few blinks. Both NPC and AA measurements were repeated three times, and the average values were reported.
Horizontal distance and near phoria were measured in real space with Howell phoria cards set at 3 m and 33 cm, respectively. The children were asked to report the pointing position of the arrow on the chart after placing the 6-prism dioptre (PD) base down on their right eye to determine the magnitude and direction of the phoria. The odd value in the yellow box represents esophoria, and the even value in the blue box represents exophoria. For the purpose of data analysis, esophoria is recorded as a positive value, while exophoria is recorded as a negative value.
Finally, the AC/A ratio was calculated using the formula derived by Scheiman and Wick:13
AC/A = IPD + NFD (Hn - Hd)
where IPD = interpupillary distance in centimeters, NFD = near fixation distance in meters, Hn = near phoria (esophoria in plus and exophoria in minus), and Hd = distance phoria (esophoria in plus and exophoria in minus).
Statistical Analysis
All statistical analyses were conducted using SPSS version 21.0 (SPSS Inc., Chicago, IL). Descriptive statistics were calculated for each measure, and all data are presented as the mean and standard deviation in this report. Monocular data for the two eyes showed no statistically significant differences (P > 0.05), and the data were highly correlated (r > 0.70). Therefore, only data from the right eye was used for statistical analysis. A p-value of less than 0.05 was set to be statistically significant.
Results
Demographic Data
Sixteen (16) boys and 24 girls were enrolled in this study, with a mean age of 10.00 ± 1.47 years (boys: 10.06 ± 1.44, girls: 9.96 ± 1.52). A total of 47.5% of the participants have at least one parent with myopia, whereas 32.5% of the participants had two myopic parents. Cycloplegic spherical equivalent via open-field autorefraction was −3.02 ± 1.20 D for the right eye and −2.79 ± 1.56 D for the left eye. The cycloplegic refractions for the right and left eyes were highly correlated (r = 0.99, p < 0.05).
Visual Acuities and Axial Length
The HCVA for distance and near were within 0.0 logMAR. A decrease in LCVA was noted at both distance and near. The findings of binocular HCVA and LCVA tests at both distance and near are summarised in Table 1, while the detailed results of monocular HCVA and LCVA tests are presented in Figure 1. The mean (±SD) AL for the right eyes was 24.42 ± 0.93 mm and 24.34 ± 0.97 mm for the left eyes.
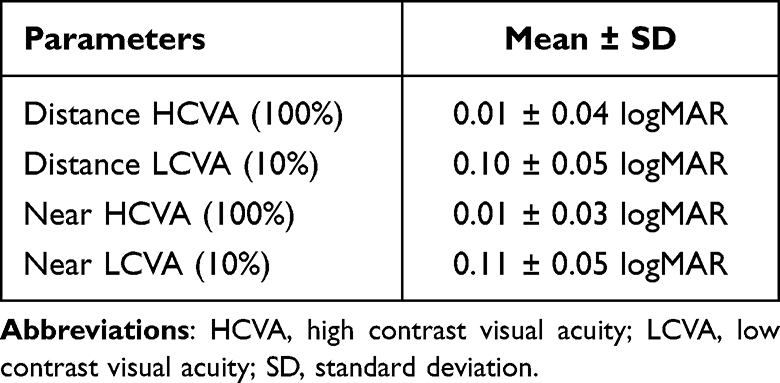 |
Table 1 Binocular Distance and Near Contrast Visual Acuity |
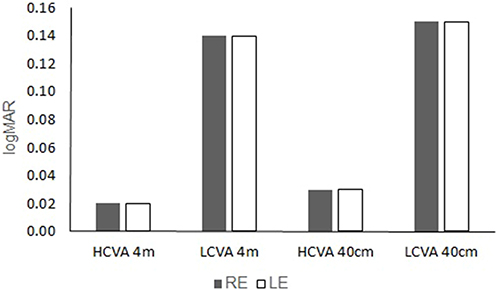 |
Figure 1 Monocular distance and near contrast visual acuity. Abbreviations: HCVA, high contrast visual acuity; LCVA, low contrast visual acuity; RE, right eye; LE, left eye. |
Binocular Vision Function
The mean and standard deviation for lag of accommodation, stereoacuity, NPC, AA, phoria, and the calculated AC/A ratio are summarized in Table 2.
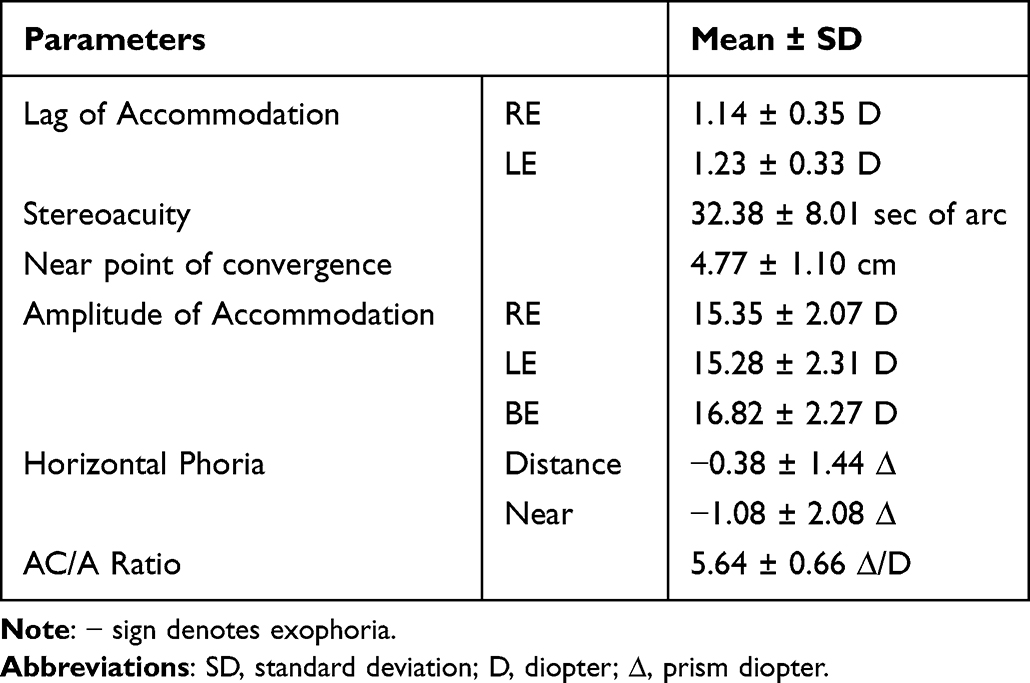 |
Table 2 Binocularity and Accommodation |
Correlations Between Refractive and Binocular Vision Measures
The Pearson correlation coefficient (r) between AL and SER assessed by cycloplegic autorefraction was negatively correlated (r = −0.49, p < 0.05). A similar correlation was observed between near-horizontal phoria and cycloplegic SER (r = −0.46, p < 0.05). This indicates that children with a higher degree of myopia have a longer axial length and are more esophoric at near. Further analysis of the relationship between AL and age also found a moderate but significant correlation (r = 0.49, p = 0.01). It shows that younger children have a shorter axial length than older ones.
Discussion
To our best knowledge, this is the first report about the accommodation and binocular vision of Malay myopic children in Malaysia.
All participants had good distance and near VA with high- and low-contrast. HCVA measures the central visual function under high-contrast conditions, whereas LCVA tests determine the ability to detect objects or details without clear outlines from their background. In this study, it was shown that binocular VA is better than monocular VA for all types of acuity tests. Huang et al14 also reported better acuities with binocular vision in photopic lighting conditions for high- and low-contrast at distance and near. These findings were expected, as subjects could discriminate higher spatial frequencies during binocular viewing than during monocular viewing.15 The mean LCVA (10%) score in our study was significantly lower than the HCVA (100%) score by one line across all chart types (p < 0.001). Our finding was similar to that found by Lam et al.12 They reported a mean difference between HCVA and LCVA of approximately 0.16 logMAR for distance and 0.11 logMAR for near. Meanwhile, Brown and Lovie-Kitchin16 reported that the difference between the high- and low-contrast VA using Bailey-Lovie charts was 2.5 lines. The difference in contrast acuity may not be particularly useful for differential diagnosis or screening for myopia in children, but because it is closely linked to the difficulty of everyday tasks, it has become an important outcome measure for assessing the safety and effectiveness of treatments as well as in any clinical research.
According to Scheiman and Wick,13 the normal range for the lag of accommodation is between +0.25 ± 0.50 D. However, a higher lag of accommodation was found in this study, which echoed earlier studies on myopia. For example, Lam et al12 reported a mean accommodative lag among 160 Chinese myopic children in Hong Kong of 1.0 ± 0.4 D, while Berntsen et al17 reported a mean accommodative lag of 1.59 ± 0.63 D among 592 myopic children in the USA. Nevertheless, it has been widely reported that myopes have a higher lag of accommodation compared to emmetropes.18 Seidel, Gray and Heron19 reported that more time was required to change focus from distance to near, which was linked to a reduced ability to relax accommodation in myopic individuals. Chen et al6 also discovered a greater lag of accommodation in myopic Malay schoolchildren when compared to non-myopic eyes, which could be attributed to differences in the crystalline lens and ciliary body properties. It has been found that myopic children have thicker ciliary bodies, which may contribute to accommodative inaccuracies, including accommodative lag.20
A good stereoacuity score is considered to be 40 seconds of arc or better,21 with a lower score indicates finer stereoacuity, allowing for more precise depth perception. Previous studies on children that utilized the Frisby Stereotest to assess stereoacuity, reported scores within the range of 20 to 40 seconds of arc, with a median falling between 20 and 25 seconds of arc.22,23 Our recent findings recorded a mean stereoacuity score of 32.38 ± 8.01 seconds of arc among the participants. This finding aligns with previous research, establishing a consistent range for acceptable stereoacuity levels. The good level of stereoacuity reported in this study might be due to similar VA between both eyes. It has been reported that a large VA difference between two eyes would have resulted in reduced stereopsis.24
The children in this study demonstrated a normal value for NPC and monocular AA.13 A previous study on 6 to 12-year-old children also found a similar result of 5.2 ± 4.4 cm for NPC.25 The AA value in our study was calculated based on the average of three measurements using Hofstetter’s formula: 18.5 - ⅓ (age).26 Most studies have found that AA decreased significantly with age in young children.27,28 In this study, higher AA was found binocularly compared to monocular eyes (16.82 ± 2.27 D binocularly versus 15.35 ± 2.07 D monocularly). Similarly, a study on Chinese myopic children also found higher binocular AA (15.6 ±2.9 D) compared to monocular AA (12.6 ±2.4 D).12 Binocular values of the amplitude of accommodation are usually 1.00 to 2.00 D higher than the monocular values, as the convergence response helps to induce additional accommodation (convergence accommodation) in binocular conditions.29
Malay schoolchildren in this study were more esophoric at baseline for both distance and near, compared to normative values of 1 exophoria for distance30 and 3 exophoria for near.31 Even though these findings are within the normal range, it can be suggested that this study population exerts more convergence at distance and near, most likely because this study was done during home quarantine, where the classes were mainly conducted online. A previous study discovered that excessive near-work was associated with an increase in esophoria.28
An elevated AC/A ratio (5.64 ± 0.66 ∆/D) was found among Malay myopic schoolchildren in this study. The results are in agreement with previous studies that suggest myopes have higher AC/A ratios than emmetropes. Mutti et al7 reported that the AC/A ratio increased in children who became myopic compared to children who remained emmetropic as early as 4 years prior to myopia onset, with a 3 ∆/D difference between groups at myopia onset. In an earlier study, Mutti et al32 reported that the AC/A ratio was highest in myopes (6.39 ∆/D) compared to emmetropes (3.94 ∆/D), and hyperopes (3.40 ∆/D). This elevated response has been suggested to be due to a reduced accommodative response at near or enhanced accommodation convergence.33 It is possible that the elevated AC/A ratio found in this study was also due to a greater esophoria and a higher lag of accommodation (reduced accommodative response at near).
A longer AL with increasing age was noted in the present study. In the Correction of Myopia Evaluation Trial (COMET) study, Gwiazda et al34 investigated the baseline data of 469 children aged 6 to 11 years with a mean spherical equivalent of −2.38 ± 0.81 D. Their results showed that younger children had significantly shorter ALs than older ones (23.63 ± 0.59 versus 24.23 ± 0.75 mm), which was probably due to a smaller degree of myopia. The results from the present study also showed that children with a higher degree of myopia have a longer AL and are more esophoric at near, which confirm previous findings.35,36 A high level of near-point activity among children in the present study could result in greater ciliary spasm or an accommodative aftereffect, inducing esophoric shift and transient myopia. It was believed that protracted and repeated periods of near work over long periods of time would result in near-work-induced transient myopia that did not completely disappear in some susceptible individuals.37 In addition, the retinal defocus resulting from near-work-induced transient myopia may act as a catalyst for the development of myopia.
Conclusion
In conclusion, the baseline data from this study showed that the myopic Malay schoolchildren had normal stereoacuity, NPC, and AA, even though they had a high lag of accommodation, an elevated AC/A ratio, and being more esophoric at both distance and near. The children with a higher degree of myopia were also found to be more esophoric compared to those with a lower degree of myopia. These findings have important implications for the diagnosis and treatment of myopia, as well as the development of interventions aimed at preventing or slowing the progression of myopia.
Acknowledgments
This work was supported by GUP-2020-054 grant from Universiti Kebangsaan Malaysia (UKM). We also acknowledge the Optometry & Vision Science Program, UKM, for instruments and facility support.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036–1042. doi:10.1016/j.ophtha.2016.01.006
2. Chen SJ, Lu P, Zhang WF, Lu JH. High myopia as a risk factor in primary open angle glaucoma. Int J Ophthalmol. 2012;5(6):750–753. doi:10.3980/j.issn.2222-3959.2012.06.18
3. Logan NS, Radhakrishnan H, Cruickshank FE, et al. IMI accommodation and binocular vision in myopia development and progression. Investig Ophthalmol Vis Sci. 2021;62(5):4.
4. Saw SM, Chua WH, Hong CY, et al. Nearwork in early-onset myopia. Investig Ophthalmol Vis Sci. 2002;43(2):332–339.
5. Troilo D, Smith EL, Nickla DL, et al. IMI – report on experimental models of emmetropization and myopia. Investig Ophthalmol Vis Sci. 2019;60(3):M31–M88.
6. Chen AH, Ahmad A, Kearney S, Strang N. The influence of age, refractive error, visual demand and lighting conditions on accommodative ability in Malay children and adults. Graefe’s Arch Clin Exp Ophth. 2019;257(9):1997–2004. doi:10.1007/s00417-019-04405-z
7. Mutti DO, Mitchell GL, Jones-Jordan LA, et al. The response AC/A ratio before and after the onset of myopia. Invest Ophthalmol Vis Sci. 2017;58(3):1594–1602. doi:10.1167/iovs.16-19093
8. Yeo ACH, Atchison DA, Schmid KL. Children’s accommodation during reading of Chinese and English texts. Optom Vis Sci. 2013;90(2):156–163.
9. Mutti DO, Mitchell GL, Hayes JR, et al. Accommodative lag before and after the onset of myopia. Invest Ophthalmol Vis Sci. 2006;47(3):837–846. doi:10.1167/iovs.05-0888
10. Berntsen DA, Mutti DO, Zadnik K. The effect of bifocal add on accommodative lag in myopic children with high accommodative lag. Investig Ophthalmol Vis Sci. 2010;51(12):6104.
11. Cheng D, Woo GC, Drobe B, Schmid KL. Effect of bifocal and prismatic bifocal spectacles on myopia progression in children: three-year results of a randomized clinical trial. JAMA Ophthalmol. 2014;132(3):258–264. doi:10.1001/jamaophthalmol.2013.7623
12. Lam CSY, Tang WC, Qi H, et al. Effect of defocus incorporated multiple segments spectacle lens wear on visual function in myopic Chinese children. Transl Vis Sci Technol. 2020;9(9):1–10. doi:10.1167/tvst.9.9.11
13. Scheiman M, Wick B. Clinical Management of Binocular Vision: Heterophoric, Accommodative, and Eye Movement Disorders.
14. Huang Y, Li X, Wang C, et al. Visual acuity, near phoria and accommodation in myopic children using spectacle lenses with aspherical lenslets: results from a randomized clinical trial. Eye Vis. 2022;9(1):1–8. doi:10.1186/s40662-022-00304-3
15. Alberti CF, Bex PJ. Binocular contrast summation and inhibition depends on spatial frequency, eccentricity and binocular disparity. Ophthalmic Physiol Opt. 2018;38(5):525–537. doi:10.1111/opo.12581
16. Brown B, Lovie-Kitchin JE. High and low contrast acuity and clinical contrast sensitivity tested in a normal population. Optom Vis Sci. 1989;66(7):467–473. doi:10.1097/00006324-198907000-00010
17. Berntsen DA, Sinnott LT, Mutti DO, Zadnik K. Accommodative lag and juvenile-onset myopia progression in children wearing refractive correction. Vision Res. 2011;51(9):1039. doi:10.1016/j.visres.2011.02.016
18. Kaphle D, Varnas SR, Schmid KL, Suheimat M, Leube A, Atchison DA. Accommodation lags are higher in myopia than in emmetropia: measurement methods and metrics matter. Ophthalmic Physiol Opt. 2022;42(5):1103–1114. doi:10.1111/opo.13021
19. Seidel D, Gray LS, Heron G. Retinotopic accommodation responses in Myopia. Invest Ophthalmol Vis Sci. 2003;44(3):1035–1041. doi:10.1167/iovs.02-0264
20. Bailey MD, Sinnott LT, Mutti DO. Ciliary body thickness and refractive error in children. Invest Ophthalmol Vis Sci. 2008;49(10):4353–4360. doi:10.1167/iovs.08-2008
21. Frisby J The frisby stereotest: an introduction and review. 2015. Available from: https://www.opticianonline.net/cet-archieve/80.
22. Anketell PM, Saunders KJ, Little JA. Stereoacuity norms for school-age children using the frisby stereotest. J AAPOS. 2013;17(6):582–587. doi:10.1016/j.jaapos.2013.08.012
23. Bohr I, Read JCA. Stereoacuity with frisby and revised FD2 stereo tests. PLoS One. 2013;8(12). doi:10.1371/journal.pone.0082999
24. Chung YW, Park SH, Shin SY. Distant stereoacuity in children with anisometropic amblyopia. Jpn J Ophthalmol. 2017;61(5):402–407. doi:10.1007/s10384-017-0518-9
25. Jiménez R, Pérez MA, García JA, González MD. Statistical normal values of visual parameters that characterize binocular function in children. Ophthalmic Physiol Opt. 2004;24(6):528–542. doi:10.1111/j.1475-1313.2004.00234.x
26. Benjamin WJ, Borish IM. Borish’s Clinical Refraction.
27. Castagno VD, Vilela MAP, Meucci RD, et al. Amplitude of accommodation in schoolchildren. Curr Eye Res. 2017;42(4):604–610. doi:10.1080/02713683.2016.1220586
28. Chen AH, O’Leary DJ, Howell ER. Near visual function in young children. part I: near point of convergence. part II: amplitude of accommodation. part III: near heterophoria. Ophthalmic Physiol Opt. 2000;20(3):185–198. doi:10.1046/j.1475-1313.2000.00498.x
29. Fujikado T, Kanda H, Morimoto T, Hirota M. Difference of accommodative response between binocular and monocular viewing condition measured by binocular wavefront sensor. Invest Ophthalmol Vis Sci. 2019;60(9):1790.
30. Song Y, Zhu S, Yang B, et al. Accommodation and binocular vision changes after wearing orthokeratology lens in 8- to 14-year-old myopic children. Graefe’s Arch Clin Exp Ophth. 2021;259(7):2035–2045. doi:10.1007/s00417-021-05106-2
31. Bao J, Yang A, Huang Y, et al. One-year myopia control efficacy of spectacle lenses with aspherical lenslets. Br J Ophthalmol. 2022;106(8):1171–1176. doi:10.1136/bjophthalmol-2020-318367
32. Mutti DO, Jones LA, Moeschberger ML, Zadnik K. AC/A ratio, age, and refractive error in children. Opt InfoBase Conf Pap. 2000;41:193–196.
33. Gwiazda J, Grice K, Thorn F. Response AC/A ratios are elevated in myopic children. Ophthalmic Physiol Opt. 1999;19(2):173–179. doi:10.1046/j.1475-1313.1999.00437.x
34. Gwiazda J, Marsh-Tootle WL, Hyman L, et al. Baseline refractive and ocular component measures of children enrolled in the Correction of Myopia Evaluation Trial (COMET). Investig Ophthalmol Vis Sci. 2002;43(2):314.
35. Hou W, Norton TT, Hyman L, et al. Axial elongation in myopic children and its association with myopia progression in the Correction of Myopia Evaluation Trial (COMET). Eye Contact Lens. 2018;44(4):248. doi:10.1097/ICL.0000000000000505
36. Chung KM, Chong E. Near esophoria is associated with high myopia. Clin Exp Optom. 2000;83(2):71–75. doi:10.1111/j.1444-0938.2000.tb04895.x
37. Lin Z, Vasudevan B, Yb L, Hj Z, Kj C. The association between nearwork-induced transient myopia and progression of refractive error: a 3-year cohort report from Beijing myopia progression study. J Optom. 2021;14(1):44–49. doi:10.1016/j.optom.2020.05.004
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.