")
Back to Journals » Clinical Optometry » Volume 16
Barriers to the Diagnosis and Management of Keratoconus Among Optometrists in Kenya
Authors Rashid ZA , Moodley VR , Mashige KP , Agho KE
Received 25 October 2023
Accepted for publication 11 January 2024
Published 23 February 2024 Volume 2024:16 Pages 71—79
DOI https://doi.org/10.2147/OPTO.S446599
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Mr Simon Berry
Zahra Aly Rashid,1 Vanessa Raquel Moodley,1 Khathutshelo Percy Mashige,1 Kingsley Emwinyore Agho2– 4
1Discipline of Optometry, School of Health Sciences, University of KwaZulu-Natal, Durban, South Africa; 2African Vision Research Institute, University of KwaZulu-Natal, Durban, South Africa; 3School of Health Sciences, Western Sydney University, Penrith, Australia; 4Translational Health Research Institute, Western Sydney University, Penrith, Australia
Correspondence: Zahra Aly Rashid, Email [email protected]
Background: Early diagnosis and management of keratoconus (KC) are important for limiting visual complications of the disease. This study aimed to explore the perspectives of optometrists on the barriers to effective diagnosis and management of KC in Kenya.
Methods: An online questionnaire was distributed to optometrists in Kenya to collect data on barriers to the diagnosis and management of KC.
Results: The majority (60.9%) of optometrists were confident in retinoscopy and subjective refraction. Fewer were confident in the use of keratometers (46.4%) and corneal topographers (24.9%) and in the fitting of rigid gas permeable (RGP) contact lenses (25.0%). The most commonly reported barriers to improving their knowledge and skills were, limited continuous professional development opportunities (87.4%), high costs of conferences (86.1%) and the lack of diagnostic tools (79.5%). Impediments cited to diagnosing and managing KC effectively were a lack of national guidelines (64.9%), patient education material (71.5%), equipment (58.9%) and RGP supply (68.2%) and cost (67.5%). Most commonly reported barriers related to patients were compliance (91.4%), affordability (90.7%), RGP discomfort (89.4%), willingness to pay (88.1%) and the lack of patient education about KC (87.4%).
Conclusion: This study showed that the lack of national guidelines, essential equipment and adequate practitioner knowledge and skills were barriers to KC diagnosis and management. Regulation of optometric education and clinical practice, development of national guidelines for diagnosis and management of KC, up-skilling of practitioners and cost-effective solutions for equipment procurement and maintenance may improve both access to, and quality of, care to patients with KC.
Keywords: keratoconus, optometrist, barriers, Africa, Kenya, optometry education
A Letter to the Editor has been published for this article.
A Response to Letter by Mr Sadeghi has been published for this article.
Introduction
Keratoconus (KC) is characterized by corneal steepening1 usually starting around puberty and rarely progressing after the age of 40 years.2 Caused by genetic and environmental factors,3 it has a reported prevalence of less than 1.2% in Caucasians and ranges from 1.4% to 4.8% in the Middle East.1,4,5 There is a paucity of epidemiological data on the disease in Africa and its prevalence in Kenya is currently unknown. KC is detected using several clinical techniques, such as retinoscopy, slit lamp biomicroscopy, keratometry, pachymetry and diagnosed with corneal topography and tomography. In the early stages of KC, there may be no obvious changes in the corneal structure, resulting in most patients being undiagnosed at disease onset.6 Management is aimed at halting progression with corneal cross-linking (CXL) and vision rehabilitation with spectacles and/or rigid contact lenses (RGP) as well as corneal surgical procedures.3 Anecdotal reports from clinicians in Kenya suggest that most patients with KC are diagnosed late. It is important to diagnose KC early to ensure timely referral for CXL, which is contraindicated in corneas <400µm, and to prevent the need for corneal transplantation.7 As a progressive disease, a delay in diagnosis has a negative impact on the overall vision-related quality of life.8
Optometrists provide comprehensive eye care and hence play an important role in the diagnosis and management of KC. Optometrists in Kenya train at Kenya Medical Training College (KMTC) or Masinde Muliro University of Science and Technology (MMUST). The KMTC program is a 3-year diploma offered since 2006 and MMUST offers a 4-year bachelor’s degree, which started in 2010.9 A milestone event for the profession took place in 2022 when the first ever scope of practice for optometrists in Kenya was published9 and registration of practicing optometrists through a regulatory board – Kenya Health Professions Oversight Authority (KHPOA) was initiated. These suggest that although optometry training in Africa began nearly a century ago,10 in Kenya, the profession is still in its infancy, but evolving. The majority of the optometrists are registered with the Optometry Association of Kenya (OAK), founded in 2009.
Several studies have reported challenges that optometrists face regarding the diagnosis and management of KC, which include the cost of corneal topographers, the lack of experience in RGP fitting, the lack of national guidelines and patient-related factors.11–18 In a survey among 39 optometrists with an equal representation from KMTC and MMUST, 68.4% reported having insufficient lecturers.19 Insufficient qualified teaching staff and inadequate teaching and learning resources have been reported in many schools of optometry in Africa.20 The Ministry of Health – Ophthalmic Services Unit (OSU) in Kenya has prioritized the review of refractive error services, the availability of CXL in public hospitals and the accreditation of institutions that train optometrists in the National Eye Health Strategic Plan 2020–2025 (NEHSP).21
Knowledge and skills of optometrists in the diagnosis and management of KC are the cornerstone of preventing vision loss due to the disease. In addition, appropriate equipment to accurately collect key clinical findings is needed to inform the diagnosis and management of KC. There are currently no national guidelines for the diagnosis and management of KC in Kenya. Also, little is known about the barriers that optometrists face to diagnose and manage the condition. This study was conducted to investigate barriers to the diagnosis and management of KC among optometrists in Kenya.
Materials and Methods
This study used a quantitative, cross-sectional, descriptive design. An online survey comprising of 29 questions, based on previous questionnaires11,12 was piloted, modified and distributed via professional associations to 213 ophthalmic clinical officers and 282 registered optometrists over 6 weeks from 13th September to 28th October 2021. The responses from both cadres to questions 1–21 relating to access to equipment, knowledge, practice and referral patterns have been published in a separate paper.22 This paper presents the responses of the optometrists only to questions 24–29 relating to their confidence, perceived barriers and interest in further training in the screening, diagnosis and management of KC (Figure S1). The 151 optometrists who responded were weighted to reflect the total number of 282 registered optometrists.
Statistical Analysis
The data was weighted to reflect the total number of optometrists in Kenya and descriptive analyses were performed using Stata “Svy” (Stata Corp 17.0) commands to allow for adjustments for the sampling weight when estimating the count and percentages of each category. Cross tabulations were generated to describe the frequencies and confidence intervals of association between dependent and independent variables, and the statistical significances were tested using the chi-squared test with a p-value of P<0.05 being considered statistically significant.
Results
Demographic Characteristics
A total of 151 completed responses were received from 282 registered optometrists yielding a response rate of 53.5%. The majority were trained in Kenya with half having a bachelor’s degree or more. Most practiced for less than 10 years, practiced in Nairobi and worked in a hospital setting.
Knowledge, Skills and Interest in Further Training
The majority (60.9%) were confident in performing retinoscopy and subjective refraction. The percentage of optometrists that were confident in performing keratometry, RGP fitting and corneal topography was 46.4%, 25.2% and 24.5% respectively (Figure 1 and Table 1). The majority preferred to update their knowledge and skills using journals and online resources.
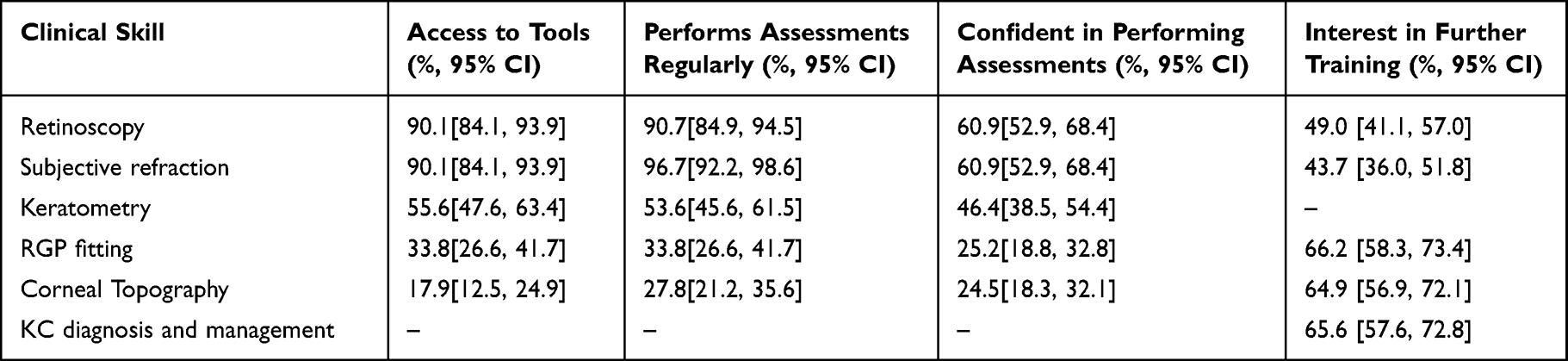 |
Table 1 Proportion and 95% Confidence Intervals (CI) of the Comparison of Access to Equipment, Regular Practice and Confidence Levels of Optometrists (n=282) |
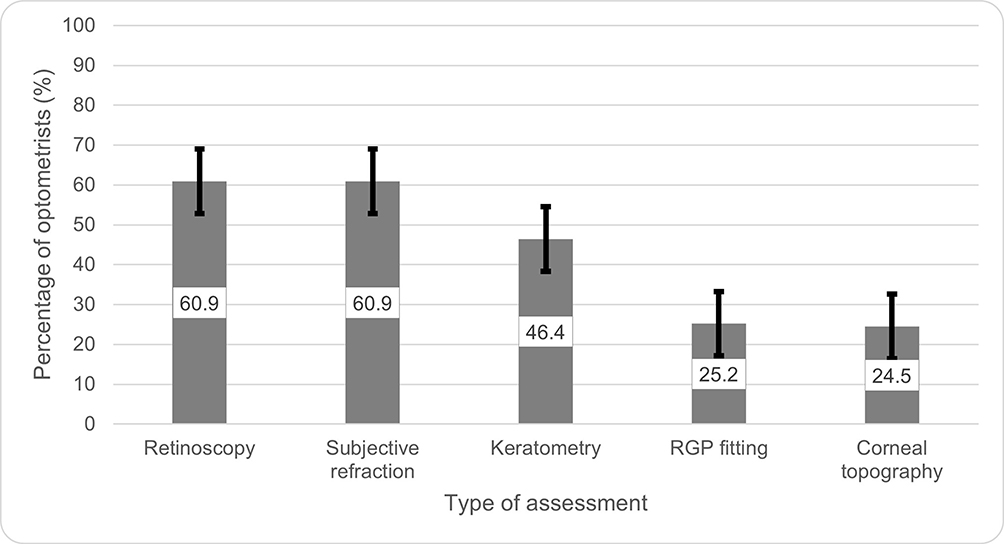 |
Figure 1 The proportion of optometrists confident in performing specific types of assessments. |
Barriers
The most commonly reported barriers to improving knowledge and skills were the lack of continuous professional development (CPD) opportunities, the cost of conferences and the lack of diagnostic tools (Table 2).
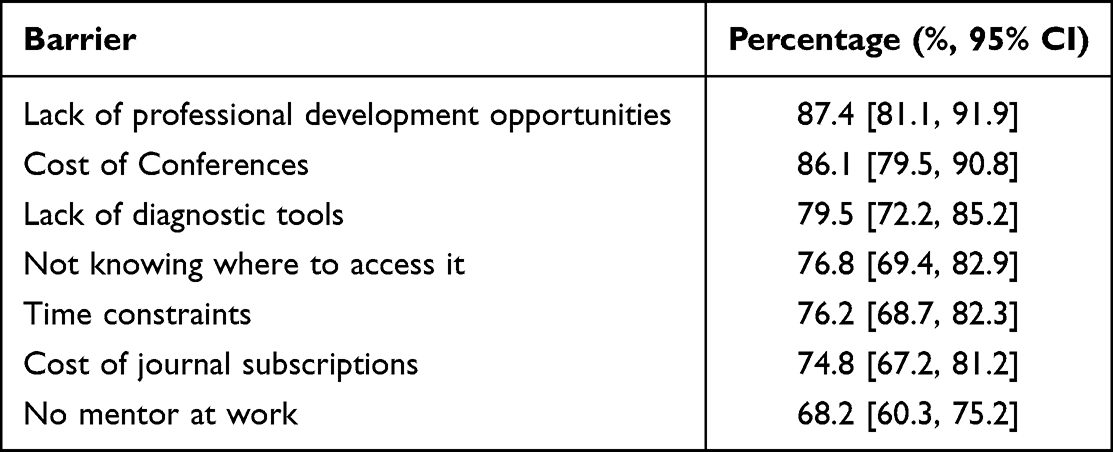 |
Table 2 Proportion and 95% Confidence Intervals (CI) of Barriers That Hinder Optometrists from Increasing Their Knowledge and Skills in Eye Care (n=282) |
The most commonly reported barriers to diagnosing and managing KC effectively were the lack of patient education material, cost of equipment, supply and cost of RGPs, lack of national guidelines and lack of equipment (Table 3).
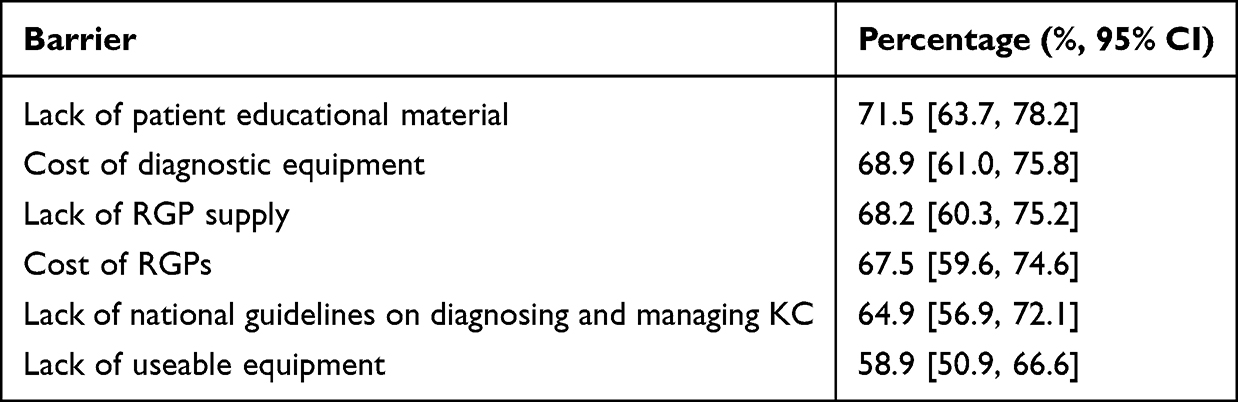 |
Table 3 Proportion and 95% Confidence Intervals (CI) of Barriers That Hinder Optometrists from Diagnosing and Managing KC, (n=282) |
The most commonly reported barriers related to patients were compliance, affordability, RGP discomfort, willingness to pay and lack of patient education about KC (Table 4).
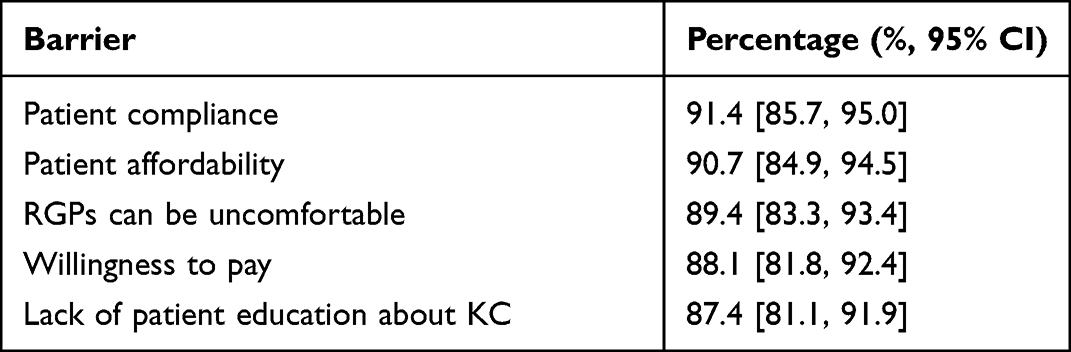 |
Table 4 Proportion and 95% Confidence Intervals (CI) of Patient-Related Barriers to the Diagnosis and Management of KC (n=282) |
Associations
More newly qualified optometrists lacked confidence in retinoscopy, subjective refraction, keratometry, corneal topography and RGP fitting as compared to experienced optometrists (p<0.01). There was no statistically significant difference between the confidence of an optometrist performing the above assessments, their qualification ie diploma or bachelor’s degree and their workplace ie optical shop or hospital. The experienced optometrists were more interested in further training in KC diagnosis and management (p=0.02) and corneal topography (p<0.01). There was no statistically significant difference between the optometrists who work in an optical shop and those who work in a hospital in their interest in further training. The lack of useable equipment was more of a barrier for those working in a hospital than in optical shops (p=0.03) (Table 5).
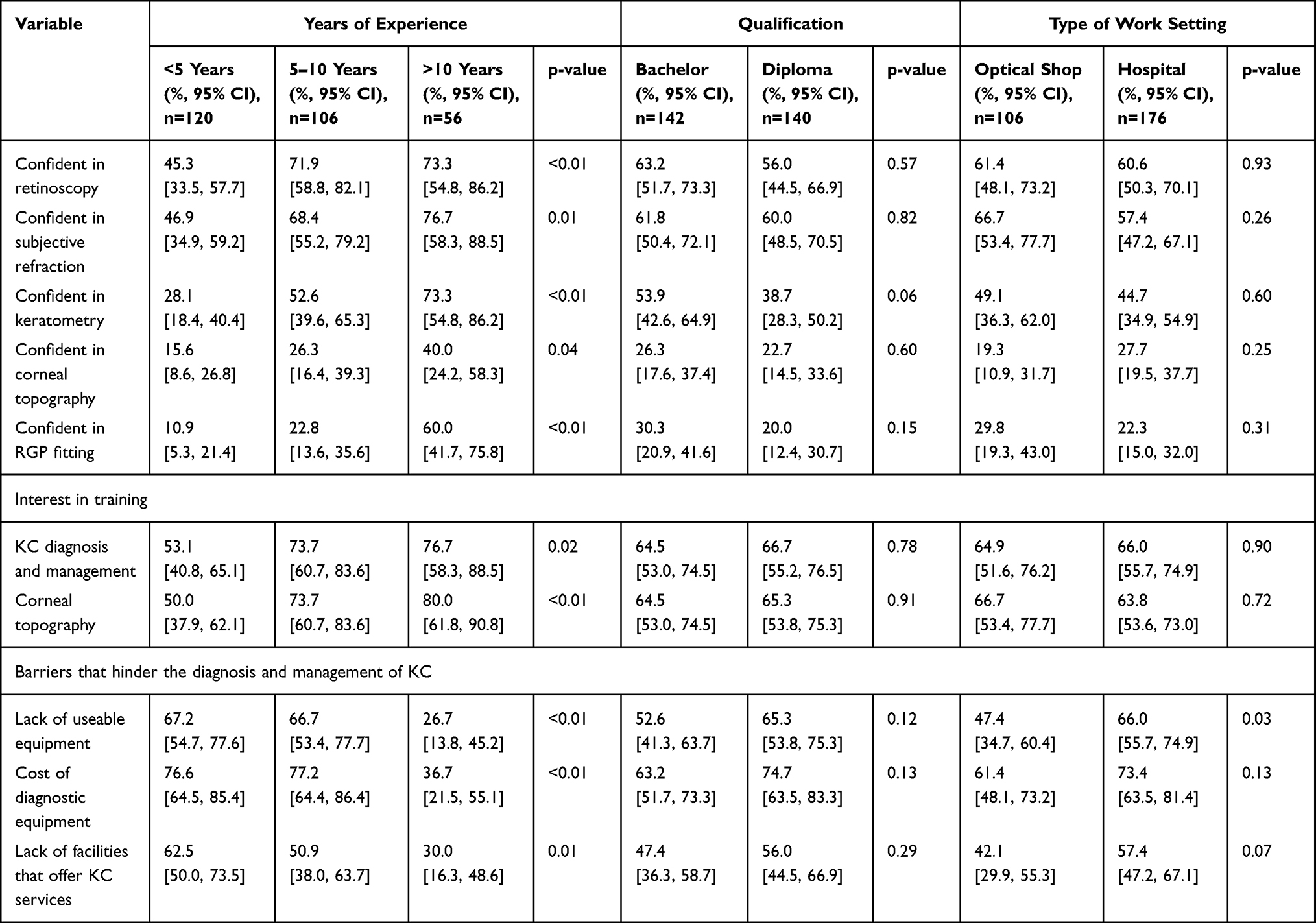 |
Table 5 The Proportion and 95% Confidence Intervals (CI) of Optometrists’ Confidence, Interest and Barriers to Diagnosing and Managing KC, Based on Years of Experience, Qualifications and Type of Work Setting (n=282) |
Discussion
This is the first study to determine the barriers experienced by optometrists in Kenya to the diagnosis and management of KC. The findings showed that the lack of knowledge and skills, diagnostic equipment and national guidelines prevent optometrists from diagnosing KC early and referring them for timely interventions.
Although the majority of optometrists (60.9%) reported being confident in performing retinoscopy, it is of concern that a significant proportion (39.1%) were not despite owning retinoscopes. This could be because 83.4% reported having access to an auto-refractor. Retinoscopy is a cost-effective, sensitive and reliable procedure to screen for KC.23,24 Optometrists should be encouraged to look for a split or scissor retinoscopy reflex, in all patients under the age of 30 years, especially in countries where there is an increased prevalence of KC. Similar results were reported in Eritrea25 and Mozambique,26,27 where up-skilling and review of the undergraduate curriculum were recommended respectively.
Few optometrists had access to and were confident in performing corneal topography. The lack of local companies to manufacture corneal topographers as well as the costs to import the device may have influenced the results observed. Other African countries such as South Africa and Ghana have reported similar results regarding poor access to corneal topographers.15,16,28 There is therefore a need for African universities to initiate innovations to design cost-effective corneal topographers to improve the diagnosis and management of KC.
Half the number of optometrists had access to and were confident in performing keratometry, this being similar to reports from South Africa and Ghana.15,16,28 Despite keratometry measurements being limited to the central 3 to 4mm of the cornea and the cone in KC decentering as it progresses,29 keratometers are cost-effective with good repeatability up to K-readings of 55D.30 In the absence of corneal topographers practitioners should, at the least, use the keratometer, combined with other clinical signs such as a split/scissor retinoscopy reflex and/or astigmatism of >2.00DC and/or slit lamp signs of KC to screen and monitor for progression. Patients with K-readings of more than 45D and/or oval or distorted mires that are difficult to superimpose should be considered suspicious for KC,31 monitored regularly and referred for corneal imaging.11
The cost and the lack of diagnostic tools were reported as barriers to the diagnosis and management of KC, particularly for those who work in hospitals (Table 5). Similar findings have been reported in South Africa15,16 and other low-and middle-income countries.32 Retinoscopes, slit lamps and keratometers are part of the basic equipment required by hospitals with eye units in Kenya however, 80% of them lacked basic equipment and often when available, were not in working condition.33 This is due to the lack of equipment maintenance officers and budget constraints which the OSU is addressing through the NEHSP.21
A quarter of the respondents were confident in RGP fitting compared to 54.2% to 83.3% of those practicing in South Africa.15,16 The lack of experience in RGP fitting is not unique to Africa and has been reported in Australia, Spain and the UK.11,12 There are no RGP manufacturing companies in sub-Saharan Africa, except in South Africa.34 The limited access to RGP fitting sets possibly results in sub-optimal practical training in RGP fitting in the undergraduate optometry programs in Kenya. The supply and cost of RGPs were among the top barriers hindering optometrists from managing KC. Similar findings were found in South Africa15 and Jordan.17 Most optometrists in Kenya who fit RGPs, order them from the UK or India retailing at $40 to $300 per lens. This is considered expensive in a country where the minimum wage is $126/month.35 In Kenya, RGPs are not fitted in public hospitals, are not covered by the National Health Insurance Fund and their provision has not been included in the NEHSP.21
Whilst the OSU is developing comprehensive refractive error services, it may take some years before these can match that provided by the private sector and possibly longer before the provision of RGPs can be considered. Since, the majority (58.4%) of refractive error services are provided by the private sector36,37 and if optometrists are provided with the necessary training and equipment for RGP fitting, the private sector could provide affordable access whilst specialized eye care services are being developed in public hospitals. Collaboration with other relevant sectors, such as engineering, is advised to investigate the possibilities of local manufacture of RGP lenses and equipment such as topographers.
As seen in Table 5, the newly qualified optometrists are significantly less confident than the more experienced ones and there was no statistically significant difference in the confidence levels between the diploma and degree holders. A review of education programs to identify the gaps in defined competencies related to knowledge and skills in KC may be initiated. This process may be facilitated by the registration authority and benchmarking could be done against other international institutions with similar health and socio-economic contexts and the World Council of Optometry competency-based scope of practice for optometrists.38 Curricula should be aligned with the defined scope of practice for ophthalmic workers in Kenya.9 Optometrists could engage in CPD activities which offer a voluntary assessment of their competence levels to determine individual needs for further up-skilling and help inform content for up-skilling courses. Assessing the competence of optometrists alongside confidence levels has been found useful in making meaningful recommendations to improve undergraduate training and up-skilling programs.26
Less than half of the optometrists were confident in performing keratometry, corneal topography and RGP fitting, and there was statistically no significant difference in the areas of interest for further training between the optometrists who work in a hospital and those that work in an optical shop (Table 5). One would expect optometrists that work in hospitals to have more experience in the diagnosis and management of KC and fitting of RGPs, similar to that seen in the UK.39 It is possible that the initial focus of training optometrists in Africa was to meet the high burden of refractive errors and hence training institutions focused primarily on producing graduates who could refract and dispense spectacles. The profession in Kenya has however evolved. There are at least 400 qualified optometrists in the country,21 there is now a scope of practice for ophthalmic workers in Kenya and, with the country approaching the World Health Organization’s minimum requirements for eye health workers,40 their role should be extended to disease diagnosis and management. Sub-specialties in contact lenses, low vision and orthoptics have emerged in some African countries to meet the needs of the public and career development for the profession.41
The majority of the optometrists cited the lack of CPD opportunities and the cost of conferences as barriers to improving their knowledge and skills. They preferred journals or online resources to increase their knowledge and skills, which may be influenced by the lower costs associated with them. Online learning has been proven effective in optometry education during the COVID-19 pandemic.42–44 Shah et al26 found up-skilling optometrists post-qualification to be an effective strategy to improve clinical competence. OAK could address the gap in knowledge and skills via cost-effective CPD sessions.
The lack of patient awareness and patient education material hinders optometrists from effectively diagnosing and managing KC. KC literacy has been shown to be low among adults with the disease,45 parents of children with the disease and those from low socioeconomic backgrounds.46 Poor understanding of KC and the different methods of management results in patients seeking eye care services late, not returning for disease monitoring, not getting CXL promptly and poor uptake of spectacles and/or RGPs.15,17 Verbal advice alone may not be successful.18 Patient education leaflets should be developed, adopted by OSU and made available in all eye clinics.
The majority of the optometrists felt the lack of national guidelines hinder them from diagnosing and managing KC effectively. Despite the global consensus on KC and ectatic diseases published in 2015,3 practice patterns differ globally.11–13,47 National guidelines disseminated by OSU would standardize the clinical approach to manage KC across Kenya.
A limitation of this study is that only data from optometrists on self-reported confidence levels in a small range of skills specific to KC diagnosis and management were collected. An independent evaluation of the competencies of the different cohorts to validate self-reported data would give more accurate findings of the gap in knowledge and skills. In addition, we did not include other stakeholders such as the training institutions, the professional associations, the OSU and patients to understand their perspectives. We did not review undergraduate optometry education curricula. A strength of this study is that it is the first to analyze optometric practice in Kenya related to KC. Further studies are required to determine the clinical competence of Kenyan optometrists from students to expert practitioners and patient-related barriers to monitoring and management of KC.
Conclusions
This study provides a snapshot of the barriers to the diagnosis and management of KC among optometrists in Kenya. Consideration of these results in planning will help to improve the early detection of KC and timely interventions to minimize the risk of visual impairment. This study shows the lack of confidence in basic skills required by optometrists to practice such as retinoscopy, subjective refraction and keratometry. Suggestions include the development of up-skilling CPD programs that may include competency assessments of optometrists. This would accurately highlight the gaps in knowledge and skills and would guide undergraduate training institutions and professional associations to enhance their educational programs. National guidelines and patient information leaflets on the diagnosis and management of KC need to be developed and disseminated. Cost-effective solutions to procure equipment and RGPs need to be explored to improve clinical diagnosis and make management options more affordable. This requires a concerted effort among KMTC, MMUST, OAK, OSU, KHPOA, non-governmental organizations and private entities.
Abbreviations
CPD, Continuous professional development; CXL, Corneal cross-linking; KHPOA, Kenya Health Professionals Oversight Authority; KMTC, Kenya Medical Training College; KC, Keratoconus; MMUST, Masinde Muliro University of Science and Technology; NEHSP, National Eye Health Strategic Plan; OAK, Optometry Association of Kenya; RGP, Rigid contact lens; OSU, Ophthalmic Services Unit; Ministry of Health Kenya.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethical Approval and Informed Consent
Ethical approval was obtained from Amref Health Africa, Kenya (ESRC P1918/2021) and the Biomedical Research Ethics Committee at the University of KwaZulu-Natal (BREC/00001226/2020) and was carried out in compliance with the tenets of the Declaration of Helsinki. In the preamble of the online questionnaire where the study purpose was explained, it was stated that “Your return of this anonymous survey implies your consent to participate in this research”. The consenting procedure was approved by Amref Health Africa, Kenya and the Biomedical Research Ethics Committee at the University of KwaZulu-Natal.
Acknowledgments
The authors would like to thank all the optometrists who participated in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Santodomingo-Rubido J, Carracedo G, Suzaki A, Villa-Collar C, Vincent SJ, Wolffsohn JS. Keratoconus: an updated review. Cont Lens Anterior Eye. 2022;45(3):101559. doi:10.1016/j.clae.2021.101559
2. Flockerzi E, Xanthopoulou K, Goebels SC, et al. Keratoconus staging by decades: a baseline ABCD classification of 1000 patients in the Homburg Keratoconus Center. Br J Ophthalmol. 2021;105(8):1069–1075. doi:10.1136/bjophthalmol-2020-316789
3. Gomes JAP, Tan D, Rapuano CJ, et al. Global consensus on keratoconus and ectatic diseases. Cornea. 2015;34(4):359–369. doi:10.1097/ICO.0000000000000408
4. Chan E, Chong EW, Lingham G, et al. Prevalence of Keratoconus based on scheimpflug imaging: the raine study. Ophthalmology. 2021;128(4):515–521. doi:10.1016/j.ophtha.2020.08.020
5. Salman A, Darwish T, Ghabra M, et al. Prevalence of Keratoconus in a population-based study in Syria. J Ophthalmol. 2022;2022:6064533. doi:10.1155/2022/6064533
6. Olivo-Payne A, Abdala-Figuerola A, Hernandez-Bogantes E, Pedro-Aguilar L, Chan E, Godefrooij D. Optimal management of pediatric keratoconus: challenges and solutions. Clin Ophthalmol. 2019;13:1183–1191. doi:10.2147/OPTH.S183347
7. Zhu AY, Jun AS, Soiberman US. Combined protocols for corneal collagen cross-linking with photorefractive surgery for refractive management of keratoconus: update on techniques and review of literature. Ophthalmol Ther. 2019;8(Suppl 1):15–31. doi:10.1007/s40123-019-00210-3
8. Panthier C, Moran S, Bourges JL. Evaluation of vision-related quality of life in keratoconus patients, and associated impact of keratoconus severity indicators. Graefes Arch Clin Exp Ophthalmol. 2020;258(7):1459–1468. doi:10.1007/s00417-020-04680-1
9. Ophthalmic Service Unit MoH-RoK. Scope of practice for ophthalmic workers; 2022.
10. Abu SL. The history and current status of optometric education in Africa. Hindsight. 2020;51(4):84–92. doi:10.14434/hindsight.v51i4.31557
11. Hodge C, Chan C, Zantos S, Kokkinakis J, Stapleton F, Sutton G. Therapeutic treatment of keratoconus: a survey of local optometric practice criteria. Clin Exp Optom. 2015;98(4):312–318. doi:10.1111/cxo.12233
12. Ortiz-Toquero S, Martin R. Current optometric practices and attitudes in keratoconus patient management. Cont Lens Anterior Eye. 2017;40(4):253–259. doi:10.1016/j.clae.2017.03.005
13. Rahmani M, Ortiz-Toquero S, Martin R. Referral pattern and co-management of keratoconus patients in primary eye care: a survey of three European countries. Cont Lens Anterior Eye. 2022;45(3):101518. doi:10.1016/j.clae.2021.101518
14. Braga Vieira S, Rivadeneira-Bueno D, Ortiz-Toquero S, Martin R. Optometric practices and attitudes in keratoconus patient management in Latin America. Clin Exp Optometry. 2022;2022:1–9.
15. Gcabashe N, Moodley VR, Hansraj R. Keratoconus management at public sector facilities in KwaZulu-Natal, South Africa: practitioner perspectives. Afr Vision Eye Health. 2022;81:1.
16. Nkoana PM, Moodley VR, Mashige KP. Self-reported knowledge and skills related to diagnosis and management of keratoconus among public sector optometrists in the Limpopo province, South Africa. Afr J Prim Health Care Fam Med. 2022;14(1):e1–e9. doi:10.4102/phcfm.v14i1.3668
17. Bakkar MM, Haddad MF, Qadire MA. Patient-related barriers to Rigid Gas Permeable (RGP) lens wear among keratoconus patients in Jordan. Cont Lens Anterior Eye. 2018;41(3):267–272. doi:10.1016/j.clae.2017.12.007
18. Ikpoh BI, Kunselman A, Stetter C, Chen M. Lost to follow-up: reasons and characteristics of patients undergoing corneal transplantation at Tenwek Hospital in Kenya, East Africa. Pan Afr Med J. 2020;36:95. doi:10.11604/pamj.2020.36.95.19993
19. Muma S, Obonyo S. Study of Kenyan optometrists view on future of optometry and prospective impact on public health; 2020.
20. Oduntan OA, Mashige KP, Kio FE, Boadi-Kusi SB. Optometric education in Africa: historical perspectives and challenges. Optom Vis Sci. 2014;91(3):359–365. doi:10.1097/OPX.0000000000000153
21. Ophthalmic Service Unit MoH-RoK. National eye health strategic plan 2020–2025; 2020.
22. Rashid ZA, Moodley VR, Mashige KP. Diagnosis and management of keratoconus by eye care practitioners in Kenya. BMC Ophthalmol. 2023;23(1):37. doi:10.1186/s12886-023-02792-w
23. Al-Mahrouqi H, Oraba SB, Al-Habsi S, et al. Retinoscopy as a screening tool for Keratoconus. Cornea. 2019;38(4):442–445. doi:10.1097/ICO.0000000000001843
24. Goebels S, Käsmann-Kellner B, Eppig T, Seitz B, Langenbucher A. Can retinoscopy keep up in keratoconus diagnosis? Cont Lens Anterior Eye. 2015;38(4):234–239. doi:10.1016/j.clae.2015.01.015
25. Gyawali R, Bhayal BK. Practice scope and job confidence of two-year trained optometry technicians in Eritrea. BMC Med Educ. 2019;19(1):303. doi:10.1186/s12909-019-1738-0
26. Shah K, Naidoo K, Chagunda M, Loughman J. Evaluations of refraction competencies of ophthalmic technicians in Mozambique. J Optom. 2016;9(3):148–157. doi:10.1016/j.optom.2015.01.003
27. Shah K, Naidoo K, Bilotto L, Loughman J. Factors affecting the academic performance of optometry students in Mozambique. Optom Vis Sci. 2015;92(6):719–729. doi:10.1097/OPX.0000000000000606
28. Boadi-Kusi SB, Ntodie M, Mashige KP, Owusu-Ansah A, Antwi Osei K. A cross-sectional survey of optometrists and optometric practices in Ghana. Clin Exp Optom. 2015;98(5):473–477. doi:10.1111/cxo.12291
29. Munsamy AJ, Moodley VR. A correlation analysis of cone characteristics and central keratometric readings for the different stages of keratoconus. Indian J Ophthalmol. 2017;65(1):7–11. doi:10.4103/ijo.IJO_980_15
30. Hashemi H, Yekta A, Khabazkhoob M. Effect of keratoconus grades on repeatability of keratometry readings: comparison of 5 devices. J Cataract Refract Surg. 2015;41(5):1065–1072. doi:10.1016/j.jcrs.2014.08.043
31. Zadnik K, Barr JT, Edrington TB, et al. Baseline findings in the collaborative longitudinal evaluation of Keratoconus (CLEK) Study. Invest Ophthalmol Vis Sci. 1998;39(13):2537–2546.
32. Patel D, Mercer E, Mason I. Ophthalmic equipment survey 2010: preliminary results. Community Eye Health. 2010;23(73):22–25.
33. Ophthalmic Service Unit MoH-RoK. Report of the evaluation of the national strategic plan for eye health and blindness prevention 2012 – 2018; 2018.
34. Akowuah PK, Kobia-Acquah E, Donkor R, Adjei-Anang J, Ankamah-Lomotey S. Keratoconus in Africa: a systematic review and meta-analysis. Ophthalmic Physiol Opt. 2021;41(4):736–747. doi:10.1111/opo.12825
35. Kwanyukuri Kakai. Minimum wage gazette notice 2022. Economic papers; 2022. Available from: https://cotu-kenya.org/minimum-wage-gazette-notice/.
36. Morjaria P, Minto H, Ramson P, Naidoo K, Gilbert C. Services for refractive error in Kenya: extent to which human resources and equipment are meeting VISION 2020 targets. J Ophthalmol East Cent South Afr. 2013;17(2):44–49.
37. Kenya Eye Health System Assessment. Sightsavers. Kenya Eye Health System Assessment; 2017.
38. World Council of Optometry. A global competency based-model of scope of practice in optometry; 2015. Available from: https://worldcouncilofoptometry.info/wp-content/uploads/2017/03/wco_global_competency_model_2015.pdf.
39. Gunn PJG, Creer RC, Bowen M, et al. Scope of practice of optometrists working in the UK Hospital Eye Service: second national survey. Ophthalmic Physiol Opt. 2022;42(3):428–439. doi:10.1111/opo.12952
40. Graham R. Facing the crisis in human resources for eye health in sub-Saharan Africa. Community Eye Health. 2017;30(100):85–87.
41. African Council of Optometry BHVI. International association for the prevention of blindness and vision aid overseas. Situat Analy Optom Af. 2016;2016:1.
42. Bullock A, Barnes E, Ryan B, Sheen N. Case-based discussion supporting learning and practice in optometry. Ophthalmic Physiol Opt. 2014;34(5):614–621. doi:10.1111/opo.12151
43. Rajhans V, Memon U, Patil V, Goyal A. Impact of COVID-19 on academic activities and way forward in Indian Optometry. J Optom. 2020;13(4):216–226. doi:10.1016/j.optom.2020.06.002
44. Gupta VK, Gupta VB. Using technology, bioinformatics and health informatics approaches to improve learning experiences in optometry education, research and practice. Healthcare. 2016;4(4). doi:10.3390/healthcare4040086
45. Baenninger PB, Bachmann LM, Ritzmann M, et al. Do patients with keratoconus have minimal disease knowledge? Cornea. 2021;40(5):624–627. doi:10.1097/ICO.0000000000002501
46. Ahmad TR, Turner ML, Hoppe C, et al. Parental Keratoconus Literacy: a Socioeconomic Perspective. Clin Ophthalmol. 2022;16:2505–2511. doi:10.2147/OPTH.S375405
47. Song M, Chen T, Moktar A, et al. Diagnosis and management of keratoconus-a narrative review of clinicians’ perspectives. Children. 2022;9(12). doi:10.3390/children9121973
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.